Runway excursion
Canair Cargo Ltd. Convair 580 C-GQHB
Tofino, British Columbia
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The aircraft, a Convair 580, was on a flight from Vancouver, British Columbia, to Tofino with four crew members and 47 passengers on board. When the aircraft landed at Tofino, it touched down about midway down the 5,000-foot runway. The aircraft ran off the end of the runway and came to rest 150 feet past the runway end. There were no injuries; however, the aircraft sustained substantial damage.
The Board determined that the descent profile flown during the approach procedure resulted in the aircraft not being in a position to land safely; the captain elected to continue rather than conduct a missed approach, and the aircraft touched down with insufficient runway remaining in which to stop. Contributing to the occurrence were inadequate monitoring, by both the air carrier and Transport Canada, of aircraft operations remote from the company's main base.
OCCURRENCE NUMBER: A93P0131
TYPE OF OCCURRENCE: Runway Excursion (Accident)
DATE OF OCCURRENCE: 21 July 1993
LOCAL TIME: 1740 PDT
LOCATION: Tofino, British Columbia
TYPE OF AIRCRAFT: Convair 580
REGISTRATION: C-GQHB
TYPE OF OPERATOR: Air Carrier
TYPE OF OPERATION: Domestic Charter
DAMAGE CATEGORY: Substantial
PILOT LICENCE: Airline Transport - Aeroplane
Pilot-In-Command
| PILOT HOURS | Last 90 Days | Total |
|---|---|---|
| All Types | 120 | 5,700 |
| On Type | 120 | 2,700 |
Co-Pilot
| PILOT HOURS | Last 90 Days | Total |
|---|---|---|
| All Types | 124 | 2,528 |
| On Type | 124 | 452 |
| INJURIES | Crew | Passengers |
|---|---|---|
| Fatal | - | - |
| Serious | - | - |
| Minor | - | - |
| None | 4 | 47 |
- All times are PDT (Coordinated Universal Time (UTC) minus seven hours) unless otherwise indicated.
- See Glossary for all abbreviations and acronyms.
1.0 Factual Information
1.1 History of the Flight
Canair Cargo Flight 801, C-GQHB, a Convair 580, departed from Vancouver, British Columbia, at 1705 Pacific daylight time (PDT1) on a charter flight to Tofino. The aircraft carried two pilots, two flight attendants, 47 passengers, and approximately 1,200 pounds of baggage.
The flight proceeded initially via radar vectors, and then direct to the Tofino non- directional beacon (NDB2). At approximately 1728 PDT, the aircraft was cleared for an approach to the Tofino Airport. The flight crew elected to fly the NDB A instrument approach procedure to Tofino, and radioed their intentions to Nanaimo Flight Service Station (FSS) through the Tofino remote communications outlet (RCO). The crew made the required blind radio transmission on the aerodrome traffic frequency (ATF) at Tofino.
After completing the instrument approach procedure, the crew proceeded with a landing on runway 28. The aircraft touched down near the midpoint of the 5,000-foot long runway, and the crew was unable to bring the aircraft to a stop; it ran 150 feet off the end of the runway. The crew shut down both engines, and, after determining that the passengers could safely exit the aircraft, lowered the airstair door and evacuated the passengers. There were no injuries.
1.2 Flight Crew Qualifications
1.2.1 Captain
The captain obtained his private and commercial licences in 1984. Prior to 1989, he was employed outside of Canada on heavy turbine aircraft types. In 1989, he was employed on SA- 226 aircraft with a company operating from Toronto, Ontario, and received a type endorsement on Convair 580 aircraft in 1990, including an upgrade to captain status in July 1990. He joined Canair Cargo Ltd. in July 1990 as a Convair 580 first officer, and was upgraded to captain in June 1991. His most recent flight check on the Convair 580 was 18 January 1993, when all items were listed as satisfactory.
The occurrence flight was the captain's second flight into Tofino. His first was earlier in the day, when the first officer had performed a landing on runway 15 using the same flap setting (flap 28). Flap 40, the other landing flap setting available, gives improved landing distance performance.
1.2.2 First Officer
The first officer obtained her private licence in 1986, commercial licence in 1987, and multi- engine and instrument ratings in 1988. She had been employed as a pilot in British Columbia since 1989, having flown a number of aircraft types including the Convair 580, and was familiar with the Tofino Airport. She began her employment with Canair Cargo Ltd. as a first officer in April 1993.
The first officer's most recent aircraft flight check on the Convair 580 was in May 1993, when the check pilot noted that it was a generally well-handled pilot proficiency check and instrument flight rules renewal check.
1.2.3 Route and Airport Qualifications
Air Navigation Order (ANO) Series VII, No. 2, the Air Carriers Using Large Aeroplanes Order, Section 56, refers to "Route and Airport Qualifications" and requires that an air carrier ensure that a pilot is not assigned to act as pilot-in-command of an aeroplane unless he is qualified for the route to be flown and the airports to be used.
The qualifications listed in the ANO state that a pilot has to have conducted an approach under supervision into each airport or have been suitably briefed. The captain in this occurrence had not flown into Tofino prior to the occurrence date. Company personnel conducted a briefing with the pilot two days prior to the occurrence date.
1.2.4 Cockpit/Crew Resource Management (CRM) Training
The flight crew members had not received a separate course of instruction in cockpit/crew resource management, nor was a separate course of instruction required by regulation.
Crew coordination training was included as part of the company flight training and line checks.
1.3 Aircraft Technical Information
The aircraft was certified and maintained in accordance with existing regulations and approved procedures. The aircraft was not equipped with an optional anti-skid braking system. Nor was it equipped with an intercom communication system between the pilot and first officer. Ambient noise made cockpit communication between the captain and first officer difficult. Neither system was required by regulation.
1.4 Aircraft Loading
The aircraft weight and centre of gravity were within the prescribed limits. A copy of the weight and balance, along with the passenger manifest, was left at the Vancouver dispatch base.
The estimated take-off weight for the occurrence flight was 52,405 pounds. The forecast landing weight, as calculated by the first officer prior to departure, was 50,905 pounds.
1.5 Environmental Conditions
The accident occurred at 1740 PDT, during the hours of daylight. The actual weather report (SA) at Tofino, recorded by Environment Canada at 1700 PDT, reported the conditions to be as follows: cloud ceiling estimated 3,000 feet broken (7/10 stratocumulus), 9,000 feet broken (2/10 altocumulus), 12,000 feet overcast (1/10 altostratus), visibility greater than 15 miles, temperature 16 degrees Celsius, dew point 10 degrees Celsius, wind from 150 degrees true at 3 knots, altimeter setting 29.92 inches of mercury.
Witness reports indicate that the wind at the airport at the time the aircraft was landing may have been as high as 15 knots, in a direction favouring a landing on runway 15.
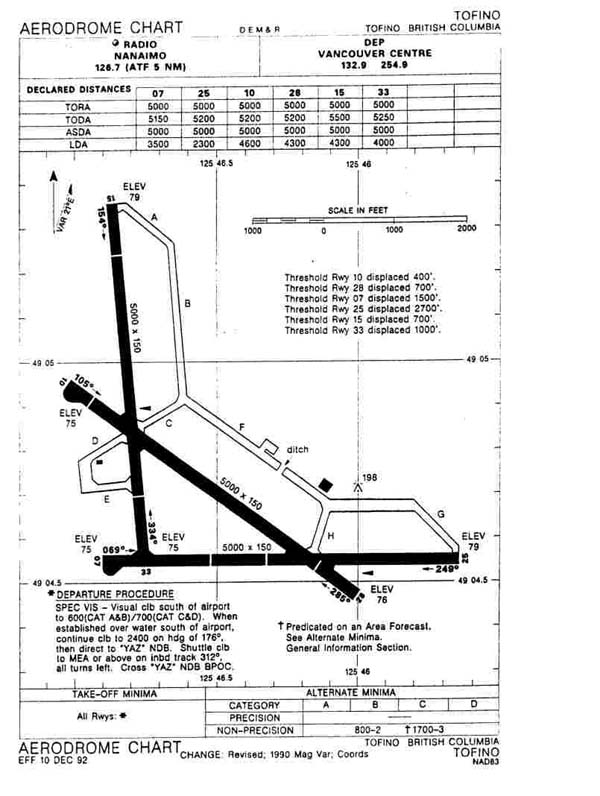
1.6 Tofino Airport
The Tofino Airport is situated on the west coast of Vancouver Island, at an elevation of 79 feet above sea level (asl). Three runways, each 5,000 feet long, are arranged in a triangular pattern.
(See Appendix C.)
All runways have displaced thresholds due to high terrain on the approach. The threshold of runway 28 is displaced 700 feet, reducing the usable runway length to 4,300 feet. The Aeronautical Information Publication, section 3.3.1, "Aerodromes," states that "the displaced threshold portion of the runway may be used for landing; however, it is the pilot's responsibility to ensure that the descent path can be safely adjusted to clear all obstacles."
The sole navigation facility associated with the airport is the Tofino NDB and it is located 2.8 nautical miles (nm) from the threshold of runway 28.
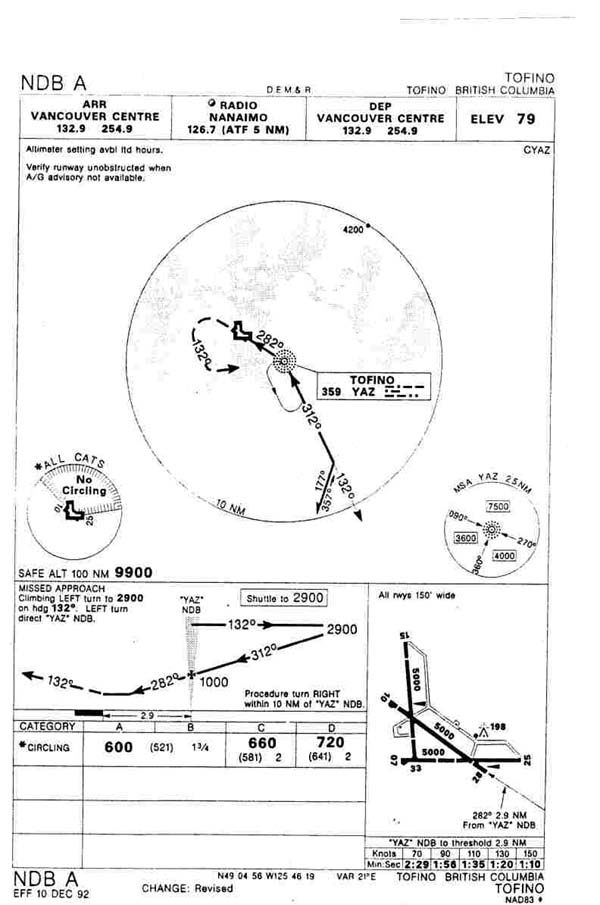
1.7 Approach Procedure - Tofino
A 7,500-foot asl safe quadrantal altitude is located within 25 nm of the Tofino NDB. A non- standard shuttle pattern at the Tofino NDB is used to descend to the procedure turn altitude of 2,900 feet asl.
NDB A (Appendix B) is the sole approach procedure specified for the Tofino Airport. The procedure specifies that, descending from a minimum sector altitude of 7,500 feet asl, the aircraft should be established in the procedure turn altitude of 2,900 feet prior to intercepting the initial inbound approach track of 312 degrees magnetic (inbound to the Tofino NDB). Upon track interception, the aircraft can descend further to 1,000 feet asl. After crossing the beacon inbound to the airport, a partial left turn is required, and the aircraft can descend to 600 feet asl, where a circling approach to land is permitted. Circling in the quadrant north of the airport is not permitted unless visual flight rules (VFR) conditions prevail.
1.8 Track and Approach - Occurrence Flight
The captain was performing "pilot flying" duties, and the first officer, "pilot not flying" duties. The first officer was in contact with Vancouver Centre during the en route portion of flight, and she contacted Nanaimo FSS at 1718 PDT to obtain the 1700 PDT weather and current airport information.
The aircraft reached the Tofino NDB at approximately 1733 PDT, at 7,500 feet asl, and the crew began the descent to the procedure turn altitude of 2,900 feet asl. The captain had briefed the first officer that he would fly a modified racetrack procedure turn, planning to descend to the procedure turn altitude. The crew proceeded outbound on the procedure turn to a distance of approximately 10 nm before turning inbound.
At 1738 PDT, the first officer reported on the Tofino traffic frequency that the aircraft had crossed the Tofino NDB (inbound), at an altitude of 1,500 feet asl (500 feet above the published altitude). Data from the flight data recorder indicate that the aircraft was at an airspeed of approximately 150 knots. The crew then aligned the aircraft with runway 28, and flew a straight-in approach to touch down on runway 28.
Evidence obtained from the cockpit voice recorder (CVR) indicates that the aircraft had only descended to 1,500 feet asl at the final approach fix, and that the final approach speed was consistently above the target speed. The airspeed deviation was called twice by the first officer and acknowledged by the captain. The tail wind was evident to both crew members, although neither proposed abandoning the approach.
1.9 Runway Overrun
After touchdown, the captain realized that the aircraft would not stop on the remaining runway. He intentionally turned the aircraft to the right as the aircraft rolled off the end of the runway so that both engines would not be damaged in a manner that would interfere with passenger egress.
Tire marks on the runway show that the aircraft moved left of the runway centre line prior to exiting the runway. The aircraft came to rest on a heading which was 90 degrees to the right of the runway heading.
1.10 Wreckage Examination
The left propeller struck the ground, and the propeller and reduction gearbox separated from the aircraft. One blade separated from the propeller hub and was later located some distance from the aircraft.
There was a vertical propeller slice, approximately two feet long, in the fuselage adjacent to the left propeller. There was a hole in the airstair door, about midway up and near the aft edge, probably made by a gear (from the ruptured gearbox) which was found on the ground below. There was also a hole below and aft of the left cockpit window with another section of gear embedded in it. All fuselage damage was confined to the outside aircraft skin.
Both nose-wheel tires and the rim of the left nose-wheel sustained substantial damage.
There was no damage inside the aircraft. Cabin blankets and pillows were stowed in the open overhead racks, and the galley equipment was stowed normally.
After the occurrence, the wing flaps were cycled to full extension, and operated normally.
When the aircraft was pulled back onto the runway, the brake discs were very noisy because of gravel picked up during the overrun. When the gravel was blown out of the discs with compressed air, the brakes were quiet while the aircraft was towed to a parking spot. When the brakes were applied, the discs were observed to be firmly held.
The right propeller had cut through low bushes, but there was no other evidence of power on the right engine. No damage to the right engine or propeller occurred.
1.11 Flight Recorders
The aircraft was equipped with a Sundstrand FA-542 five-parameter foil-type flight data recorder (FDR) and a Sundstrand V-557 CVR.
The five parameters available on the FDR were as follows: pressure altitude, airspeed, heading, vertical acceleration, and time. Transport Canada had issued a waiver, through a grandfather clause, that allowed the company to use such a recorder. Current legislation would require the aircraft to have a digital FDR with a minimum of 17 parameters.
When the FDR was recovered, heading, airspeed and vertical acceleration traces were readable, but the altitude trace was not. Data indicated that the aircraft touched down at a speed of approximately 111 knots indicated airspeed (KIAS). A decrease in vertical acceleration to approximately 0.8 g for 3.5 seconds and a slight decrease in speed during that time were consistent with the aircraft bouncing on touchdown. Integration of derived groundspeed over the time of the bounce indicated a float after the bounce of approximately 550 to 700 feet, taking into account the reported tail wind conditions.
The airspeed data from the FDR was not considered to be valid below 100 KIAS, so that the actual touchdown point on the runway could not be determined.
The CVR recording was of fair quality, with some sound obscured by engine background noise. Crew conversation was recorded by a cockpit area microphone since no intercom was installed.
1.12 Flight Planning
The company had conducted charter flights to Tofino since May 1993. A company-issued route manual listed phone numbers and operational procedures. Included in the route manual listing for Tofino was the statement that "Best runway for landing is runway 28."
Canair Standard Operating Procedures, Section 6.5.3, "Unfamiliar Airports," states "The minimum runway length to be used [for landing] is that set down in the Aircraft Operations Manual."
1.13 Landing Performance Information
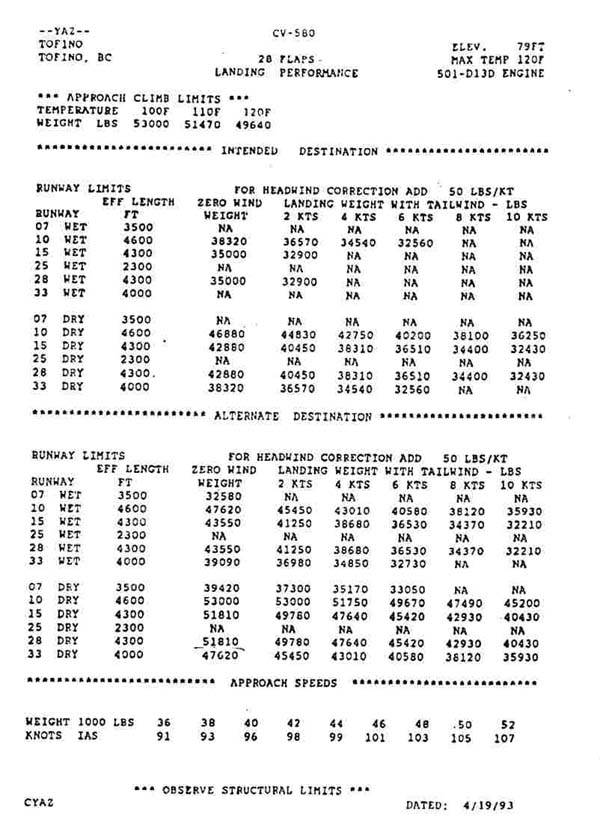
There were three sources of landing performance information available to the flight crew, as follows:
- Runway analysis charts (Appendix A) prepared by Jeppesen for the operator; these charts are calculated using aircraft performance data, temperature, wind and obstacle information in the airport area;
- Performance tables in the company Convair 580 Aircraft Operating Manual (AOM);
- Performance graphs in the Convair 580 Airplane Flight Manual (AFM).
Accepted company practice was to use the runway analysis charts for determining take- off and landing distances. Company standard operating procedures (SOPs) refer to the use of runway analysis charts for determining the maximum take-off weight for a particular runway at an airport; the SOPs do not refer to these charts for obtaining landing information.
The company aircraft operating manual also provided a landing distance reference table. This table, which was reportedly not normally referred to by the company flight crews, is an extrapolation of aircraft performance data and is a conservative summary of that data for use in "normal" operations. It does not account for anomalies such as obstacles or adverse runway conditions.
Company personnel stated that 28-flap landing performance for an equivalent length runway at another airport of the same altitude above sea level (Campbell River, British Columbia) could be used to establish a landing performance reference.
The crew did not specifically calculate, by any of the means available, the landing distance required or the maximum allowable weight for landing on runway 28 with either a 28- flap or 40-flap setting. Calculations made from the available sources would have shown that, using the full runway length of 5,000 feet, the required landing distance for a flap 28 landing would be just within limits; with a two-knot tail wind, there would not be sufficient runway available.
There was no discussion in the cockpit when the captain briefed that the landing configuration was to be 28-degree flap. Company SOPs did not include landing performance data as an item to be briefed prior to landing.
1.14 Crew Coordination/
Company Standard Operating Procedures
Review of the CVR information showed that the flight crew discussed the approach procedure in an abbreviated fashion, and that all required briefing elements (as per the SOP) were not completed. That briefing omitted required items, including approach timing and minimum descent altitudes.
An item shown in the Transport Canada Instrument Procedures Manual.(TP2076) as an essential planning element when preparing for an approach is "the rates of descent required during various stages of the approach." These were not briefed during the occurrence approach.
Company SOPs require that the activities of the pilot flying (PF) be monitored by the pilot not flying (PNF) during the approach and landing phase of flight. Deviations from normal flight profiles are to be announced to the PF. Although the first officer noted deviations to the required approach profile and reference speeds, and communicated them to the captain, the approach continued unchanged.
1.15 Passenger Safety
The cabin crew consisted of two persons, a purser and a 1st flight attendant. The purser was seated in the flight attendant jumpseat at the rear of the cabin near the rear service door exit. She stated that she was not aware of a problem until shortly before the aircraft departed the runway. After the aircraft came to rest, she began a 15-second silent count, as specified in the flight attendant procedures, before initiating emergency actions. She stated that, part way into that silent count, she heard the "remain seated, remain seated" instruction on the cabin public- address (PA) system from the first officer, then heard four chimes and saw the pilot light on the intercom, which indicated to her that the flight crew was attempting to contact the cabin crew. She then used the interphone to contact the flight crew, but got no response. Shortly thereafter, the captain appeared in the cabin, opened the airstair door, and instructed her to lead the passengers out.
The captain had determined that there was no fire before allowing the passengers to descend. Passenger evacuation proceeded in an orderly manner, and there were no injuries. The flight attendants then led the passengers away from the aircraft.
The 1st flight attendant was seated near the centre of the cabin. After the order to evacuate the passengers was given, she proceeded to the rear of the cabin to follow the passengers off.
1.16 Transport Canada Monitoring
Transport Canada Ontario Region, the region in which the company was based, is responsible for supervising and monitoring the operation of the carrier. The company was described by Transport Canada Ontario Region staff as being cooperative in all aspects of regulatory monitoring, and overall a respected operator.
When the company began operations in Vancouver, in the Transport Canada Pacific region, the Transport Canada Ontario Region office did not request that Transport Canada Pacific Region monitor the company's operations in Vancouver on their behalf. Transport Canada Ontario Region staff indicated that there was some difficulty in requesting another region to assist with their monitoring function, due to limited resources.
1.17 Pilot Decision Making
A fundamental element in making correct decisions when flying an aircraft is maintaining adequate situational awareness--that is, knowing what is happening around you. Situational awareness is the starting point in the decision-making process; appropriate action or correct decisions cannot be expected unless the information the decisions are based upon is reasonably complete and accurate. In general, breakdowns in situational awareness are caused by faulty acquisition and processing of this information.
When a pilot is performing a task with which he or she is familiar, such as landing, there is a natural tendency to refrain from using all the cues available. Because certain cues are anticipated, an unconscious filter will tend to select those cues which quickly reinforce the pilot's perception of his or her ability to accomplish that particular task. Not only may this assessment be flawed, but there is significant resistance to changing that assessment, even in the presence of what would objectively appear to be very compelling evidence.
2.0 Analysis
2.1 Introduction
The investigation identified that certain operating practices established by management were not being effectively transmitted to the operating personnel, and that the regulatory agency (Transport Canada) did not effectively monitor the company operations when the company was operating at bases remote from the supervising regional office.
Operating irregularities that allowed this aircraft accident to occur include the crew's use of an aircraft configuration that did not allow for adequate margins for landing performance (stopping distance) and the captain's inadequate handling of the aircraft during the approach.
2.2 Company Management
The operating practices of the company, as directed at the management level of Director of Flight Operations and Chief Pilot, were not effectively transmitted to the flight crews. Policies distributed by the company in the form of Standard Operating Procedures and other manuals were not put into effect at the operating level at the Vancouver base.
Specifically, the pilots did not use the runway analysis charts for calculation of landing distance. The result was repeated company operations into airports where the runway length available for landing was marginally acceptable or insufficient according to the required runway length indicated by the charts.
2.3 Transport Canada Monitoring
Because Transport Canada did not monitor the operations of Canair Cargo at their Vancouver base with the same frequency that they would have in the Ontario region, they were not able to ensure that all company operations were being performed to the required standard.
2.4 Aircraft Configuration/Use of Runway Analysis Charts
The landing performance charts for Tofino indicated that a safe landing could only be conducted with a flap 40 setting, yet there was no discussion in the cockpit when the captain briefed that the landing configuration was to be 28-degree flap. Company SOPs did not include landing performance data as an item to be briefed prior to landing.
Thus, the flight crew used an aircraft configuration that may not have allowed for adequate margins for landing performance (stopping distance).
2.5 Approach Effectiveness
The weather at the time of the approach was suitable for a visual approach to the airport, after the aircraft had completed the procedure turn and was established inbound to the airport. The crew conducted a visual approach, but the captain did not maintain the required descent profile to ensure a safe touchdown near the runway threshold and stop the aircraft in the distance available.
The published approach procedure calls for a descent to minimum descent altitude and then a circling procedure for landing; however, the captain elected to fly a visual straight-in procedure to runway 28.
The crew's lack of appreciation of the situation was exacerbated by the absence of the final approach descent planning information. If the required descent rates had been briefed prior to the approach, there might have been more indication to the crew that the approach was not proceeding normally.
The combination of excessive altitude to be lost on final approach, a higher than target airspeed on final approach, and a tail wind component led to the aircraft not being in the required position to execute the straight-in landing on runway 28.
Both crew members were qualified and experienced on the aircraft type. The captain had not, however, flown on this operation or into this airport prior to the day of the occurrence. The first officer had fewer flying hours on type and in total, but was familiar with the Tofino Airport.
2.6 Pilot Decision Making
Throughout the approach, the captain received, and acknowledged, information from the first officer which indicated that the aircraft was above the optimum descent profile and desired speed. Further, comments about the significant tail wind encountered on the approach were made by both crew members. Notwithstanding these cues, and the perspective provided from the cockpit, the captain continued with the approach.
The first officer could have been more assertive in expressing her discomfort with the approach profile. However, neither crew member had CRM training; the lack of assertiveness and the lack of corrective action by the captain were responses which could have been expected from a crew without such training.
The incorrect descent profile, higher than normal approach speed, and tail wind should have dictated a missed approach; the captain, however, elected to continue with a landing, which resulted in a long touchdown and insufficient runway remaining on which to stop the aircraft.
The following laboratory reports were completed:
- LP 086/93 - Flight Data Recorder Report; and
- LP 087/93 - Cockpit Voice Recorder Repor.
3.0 Findings
- The aircraft's weight and centre of gravity position were within limits.
- The aircraft was certified in accordance with existing regulations and approved procedures.
- There was no evidence found of any airframe failure or system malfunction prior to or during the flight.
- A five-parameter foil-type FDR was installed on the aircraft. The company had been granted a waiver to permit the installation.
- The captain's aircraft handling during the approach procedure resulted in the aircraft not being in a position to carry out a safe landing.
- The captain elected to continue the landing attempt after an unsatisfactory approach, and the aircraft touched down about midway along the runway at a speed of approximately 111 knots indicated airspeed (KIAS).
- The aircraft touched down at a point on the runway which left insufficient distance remaining in which to stop.
- This was the second time that the captain had flown in to Tofino Airport, and the first time he had been there while performing the "pilot flying" duties.
- The captain had not received specific company training on landing performance requirements at the Tofino Airport, although he had been briefed.
- The flight crew used an aircraft configuration that may not have allowed for adequate margins for landing performance (stopping distance).
- The captain's approach briefing did not conform to the requirements specified in the company SOPs.
- The operating practices of the company at the management level were not effectively translated to the operating personnel.
- The regulatory agency (Transport Canada) did not effectively monitor the company operations when the company was operating at bases remote from the supervising regional office.
- The company did not provide a separate course of instruction in cockpit/crew resource management or pilot decision making, nor was such training required by regulations.
3.1 Causes
The descent profile flown during the approach procedure resulted in the aircraft not being in a position to land safely; the captain elected to continue rather than conduct a missed approach, and the aircraft touched down with insufficient runway remaining in which to stop.
Contributing to the occurrence were inadequate monitoring, by both the air carrier and Transport Canada, of aircraft operations remote from the company's main base.
4.0 Safety Action
4.1 Action Taken
4.1.1 Regulatory Audits and Surveillance
Analysis and information from this investigation and 18 others led to the identification of shortcomings in the regulatory audit process of air carriers. In particular, it was found that Transport Canada's (TC) audits lacked depth, and that the verification of corrective action following the audits was inadequate. Therefore, the Board recommended that:
The Department of Transport amend the Manual of Regulatory Audits.to provide for more in-depth audits of those air carriers demonstrating an adverse trend in its risk management indicators;
Transportation Safety Recommendation A94-23
The Department of Transport ensure that its inspectors involved in the audit process are able to apply risk management methods in identifying carriers warranting increased audit attention;
Transportation Safety Recommendation A94-24
The Department of Transport develop, as a priority, a system to track audit follow-up actions;
Transportation Safety Recommendation A94-25
The Department of Transport implement both short and long term actions to place greater emphasis on verification of required audit follow-up action and on enforcement action in cases of non-compliance.
Transportation Safety Recommendation A94-26
4.1.2 Flight Recorder Legislation
Over the years, the Board has made several recommendations concerning deficiencies in the retrieval and quality of flight recorded data and in the lengthy process required to update flight recorder legislation. Notwithstanding the emphasis that the Board has put on the importance of flight recorders for investigation and accident prevention purposes, there has not been significant progress in addressing these flight recorder deficiencies. Therefore, the Board recommended, inter alia, that:
The Departments of Justice and Transport promulgate the new Orders on flight recorders without further delay; and
Transportation Safety Recommendation A94-03
The Department of Transport streamline its processes to facilitate the timely Canadian implementation of updated flight recorder requirements.
Transportation Safety Recommendation A94-04
In response, TC has indicated that it intends to issue two interim circulars to facilitate industry adjustment to the new flight recorder regulation expected to come into law in early 1995. Also, TC stated that new regulations will refer to associated standards, which should facilitate amendment action in a timely way. The Department of Justice has advised that it is prepared to carry out its regulatory functions as quickly as possible to ensure that the regulations proposed by TC can be promulgated with the least possible delay.
4.2 Action Required
4.2.1 Crew Resource Management and Decision Making
Several factors led to the accident aircraft not being in the required position on final approach from which a safe landing could be executed. However, the accident could have been prevented if a decision had been made to discontinue the landing.
The Board has investigated several recent occurrences3 where inappropriate decisions have been made by aircrew, although cues were available which should have alerted them to potentially dangerous situations. While this occurrence at Tofino hinged upon a pilot decision at a critical point in the approach and landing phase, inappropriate decisions occur in almost all aspects of flight operations. (See Appendix D for some examples of aviation occurrences with probable decision-making implications.)
3 TSB occurrences A90P0337, A91A0198, A91C0083, A92P0015, A93H0023, A94H0001, A94W0026, and A94A0078
The Board recognizes that there are pressures in commercial aviation to "get the job done" and that these pressures undoubtedly affect decision making. Nevertheless, informed operators and trained aircrew should be able to handle these day-to-day operational decisions safely. In this vein, it is understood that crew training under real-world decision-making situations increases the likelihood of safe operational decisions. Subsequent to a DC-8 runway excursion at Moncton, New Brunswick (A91A0198), the involved carrier undertook several corrective measures, including the use of simulator training to assist crews in the decision-making process during approaches in reduced visibilities (such as the conditions encountered in the occurrence). In its final report on the occurrence, the Board encouraged such preventive action taken by the aviation community independent of regulatory requirements. However, the Board also expressed concern that other operators and aircrew without benefit of similar training programs and guidelines on the handling of critical decisions might continue to place their aircraft in unsafe situations.
Like the Convair 580 aircrew involved in the Tofino occurrence, most of the aircrew involved in the other incidents/accidents had not received formal crew resource management (CRM) or pilot decision-making (PDM) training. (The operators and aircrew involved in the occurrences listed in Appendix D may have subsequently taken action with respect to CRM and PDM training.) In its Commercial Pilot Survey (1991), Levels III to VI Air Carrier Operations, the TSB found that only 22 per cent of the respondents indicated that CRM training was provided by their employer and that decision-making training was available to only 27 per cent. Other countries have recognized the merits of this type of training; reportedly, the Federal Aviation Administration in the United States will require, by late 1995, resource management training for airlines to improve communication and co-ordination among crew members.
In its Safety Study of VFR Flight into Adverse Weather.(1990), the Board supported TC's initiative to evaluate pilot decision-making skills in the Private Pilot Licence flight test, and recommended that the Minister of Transport devise and implement a means of regularly evaluating the practical decision-making skills of commercially employed pilots in small air carrier operations (TSB A90-86). TC responded that Pilot Proficiency Checks would provide an assessment of a pilot's ability to make reasoned and timely decisions when faced with a simulated emergency situation. TC also indicated that it would keep abreast of developments in the field of decision-making training and assessment, and would not hesitate to introduce improvements.
The eight referenced occurrences and the one at Tofino involved a total of 188 crew and passengers on board nine aircraft; eighteen fatalities resulted. The potential for more serious consequences was high. All of these occurrences were after the issuance of TSB recommendation A90-86 and for the most part involved small air carriers. The "inappropriate decisions" taken in these occurrences were not linked to emergency situations that would normally be tested on Pilot Proficiency Checks. Furthermore, the Board understands that there are still no requirements or established guidelines for ongoing training and evaluation of decision-making skills in the routine situations that commercial pilots face day-to-day.
While the commercial aviation community has broadly embraced the concepts of CRM and PDM training, formal programs are only being administered on a voluntary, ad hoc basis. Consequently, ineffective resource management and faulty decision making continue to contribute to unsafe situations in commercial air transportation. Notwithstanding the many pressures in the commercial flying environment that come to bear on operators and aircrew, the Board believes that, with the correct tools and skills, the likelihood of inappropriate decisions can be reduced. While some large air carriers can develop the necessary training on their own, other operators will require direction and assistance in setting up meaningful training programs. Therefore, to ensure that all operators and aircrew involved in commercial aviation have access to training for better coping with day-to-day operating decisions, the Board recommends that:
The Department of Transport establish guidelines for crew resource management (CRM) and decision-making training for all operators and aircrew involved in commercial aviation;
Transportation Safety Recommendation A95-11
The Department of Transport establish procedures for evaluating crew resource management (CRM) and pilot decision-making (PDM) skills on a recurrent basis for all aircrew involved in commercial aviation.
Transportation Safety Recommendation A95-12
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board, consisting of Chairperson, John W. Stants, and members Gerald E. Bennett, Zita Brunet, the Hon. Wilfred R. DuPont and Hugh MacNeil, authorized the release of this report on .
Appendices
Appendix A - Runway Analysis Charts
Appendix B - Approach Procedure for Tofino Airport
Appendix C - Aerodrome Chart for Tofino Airport
Appendix D - Some Occurrences in which Decision Making was a Factor
A90P0337: It was found that the crew of a B-737 attempted a second approach in marginal weather at an intended destination prior to proceeding to an alternate airport even though the fuel for the second approach had not been calculated in the fuel load.
A91C0083: Although there were several pre-flight indications of a hydraulic system malfunction on a HS 748, the captain elected to conduct the flight.
A91A0198: The crew of a DC-8 continued with a landing in marginal weather, although adequate visual references had not been acquired by the pilot flying.
A92P0015: The operator scheduled a flight of a float-equipped Beech 18 in unfavourable conditions and an inexperienced pilot attempted a heavy weight take-off in the marginal weather.
A93H0023: A night flight in a HS-748 with electrical problems was initiated from Sandy Lake, Ontario, and the aircraft struck the ground shortly after take-off.
A94H0001 (investigation ongoing): A VFR chartered helicopter struck a ridge in mountainous terrain during a flight in known poor weather.
A94W0026 (investigation ongoing): At Calgary, Alberta, the take-off of a charter DC-8 with 83 persons on board was continued with two failed tires.
A94A0078 (investigation ongoing): The crew of a Swearingen SA226-AT on a courier flight nearly collided with a building while on approach for landing at Sydney, Nova Scotia.
Appendix E - Glossary
- AFM
- Airplane Flight Manual
- ANO
- Air Navigation Order
- AOM
- Aircraft Operating Manual
- asl
- above sea level
- ATF
- aerodrome traffic frequency
- CRM
- cockpit/crew resource management
- CVR
- cockpit voice recorder
- FDR
- flight data recorder
- FSS
- Flight Service Station
- KIAS
- knots indicated airspeed
- NDB
- non - directional beacon
- nm
- nautical mile(s)
- PA
- public address system
- PDM
- pilot decision making
- PDT
- Pacific daylight time
- PF
- pilot flying
- PNF
- pilot not flying
- RCO
- remote communications outlet
- SA
- actual weather report
- SOP
- standard operating procedure
- TC
- Transport Canada
- TSB
- Transportation Safety Board of Canada
- UTC
- Coordinated Universal Time
- VFR
- visual flight rules