Collision with terrain
A.A.L. Air Alps (Glacier Air)
Eurocopter AS350BA (Helicopter) C-GDWF
Squamish, British Columbia, 3 nm W
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
At about 1235 Pacific daylight time on 15 August 1999, a Eurocopter AS350BA helicopter, serial number 2139, departed the airport near Squamish, British Columbia, under visual flight rules with the pilot and four passengers on board. The purpose of the flight was to conduct a 30-minute sightseeing tour in uncontrolled airspace to a glacier and lake, Lake Lovely Water, in high terrain to the west of the airport. After the aircraft had been gone for more than an hour with no communication, company personnel initiated a search. The rescue coordination centre was alerted at 1543, and a ground and aerial search was begun. Search efforts were hampered by low cloud, rain, fog, and darkness.
At 1648 the next day, the wreckage of the helicopter was found about three nautical miles west of Squamish Airport and about one nautical mile northeast of Lake Lovely Water (see Appendix A). The first impact was in a steep ravine, at about 3800 feet above sea level. The aircraft struck the terrain at low speed, broke apart, and fell down the ravine, about 300 feet below the point of impact. The pilot and passengers were fatally injured. There was no fire. The time of the accident could not be determined. The emergency locator transmitter was destroyed by impact forces, and no emergency locator transmitter signal was received at any time.
Factual information
The pilot-in-command (PIC) was the son of the company founder and had been employed in the family business as a pilot since 1986, flying various types of fixed-wing aircraft. He held a Canadian commercial pilot licence (CPL) airplane since 1986, received a CPL helicopter licence in February 1999, held a valid flight medical certificate, and accumulated a total of about 6800 hours flying, about 300 hours of which were on helicopters and 145 hours on the Eurocopter AS350 type. His most recent pilot proficiency check (PPC) was on 15 April 1999 and assessed satisfactory. The PIC had flown 44.7 hours in the last 30 days, 1.9 hours on the previous day, and three tours of about 30 minutes each that morning. His flight and duty times were within the guidelines and regulations established by Transport Canada (TC). A medical examination, limited primarily to toxicology, revealed no indication that incapacitation or physiological factors had affected the pilot's performance.
The accident pilot had conducted his formative helicopter training on a Bell 47, which has the same rotor diameter as the AS350. However, in the AS350, the pilot is further away from the rotor hub, giving a different perspective of distances required to clear obstacles. From the pilot's seat, two more feet are required to clear an obstacle to the left. It was learned that pilots upgrading to the AS350 are often initially surprised by this phenomenon.
There are no ground-based aviation radio navigational aids near Squamish Airport nor in the area over which the accident flight was operating. The accident aircraft was equipped with a global positioning system (GPS); however, the accident pilot had not demonstrated proficiency with the operation of the unit installed in the helicopter. In addition, no routes that would reflect the flights being conducted were stored in the unit; thus, it was unlikely that the GPS was being used.
There is no record of communication from the helicopter during the accident flight; however, communications had been made between aircraft on previous flights that day. Direct communications between the helicopter and the company base could not be established on the day of the accident because the company base radio was being repaired. When the accident helicopter became overdue, company personnel tried to reach the helicopter by using the radio in a Cessna on the ground and by calling the cellular telephone that the pilot was carrying. There was no response.
The weight and balance of the aircraft at take-off from Squamish Airport were within certificated limits. When the aircraft took off, it weighed about 3960 pounds, including 470 pounds of fuel. A review of the aircraft technical records revealed no anomalies. The company's maintenance practices were in accordance with the guidelines set out by TC.
The emergency locator transmitter (ELT) was located in the nose of the helicopter; its location and construction are common for light helicopters. The emergency locator transmitter was destroyed by impact forces, and no emergency locator transmitter signal was received at any time.
Weather information compiled by the Atmospheric Environment Service of Canada (AES) reveals that the weather in the local area was being influenced by a cold front with cloud ceilings at 3000 to 5000 feet above sea level (asl) and frequent precipitation reducing visibility to six miles in light rain and showers. A few ceilings of 800 to 2000 feet asl, with visibility of two to six miles in rain showers and mist were also forecast for the period.
The Squamish Airport's automated weather observation system (AWOS) report for 1200 indicated that the temperature and dew point were both 14 degrees Celsius, the wind was 130 degrees magnetic at seven knots, and it was raining. Ceiling or visibility conditions were not reported.Footnote 1
A company pilot who had conducted a tour that morning from Squamish Airport in the company's Cessna 206 airplane reported the weather as follows: low cloud in rain with a ceiling of about 800 feet above ground level (agl) and a light inflow wind at about five knots from the inlet. The pilot recalled the weather to the north was better and some of the mountain ridges were visible. At that time, the accident helicopter was operating to the west of Squamish, but the Cessna pilot was not conducting tours in that area because the weather was not good enough for fixed-wing operations. She was flying over the airport and over the town of Squamish. While in flight, the pilot of the accident helicopter communicated by radio with the Cessna pilot, discussed the weather, and showed some concern about her flying in the prevailing weather conditions.
The occurrence pilot had flown three flights in the morning and had flown to the glacier each time. However, before the accident flight, he indicated that if he could not reach the glacier, he would go to Lake Lovely Water. Other helicopter operators in the area cancelled operations that day because of poor weather conditions.
It is common practice for helicopter pilots to hover from tree to tree to exit an area of poor weather. If a pilot encounters reduced visibility in inhospitable terrain where it is difficult to land, the pilot slows down and continues as long as reference to the ground can be maintained. This could mean hovering within 10 feet of terrain.
Canadian Aviation Regulations (CARs) for minimum visual meteorological conditions for VFR flight in uncontrolled airspace require that the flight visibility be not less than one mile unless authorized otherwise in an air operating certificate (AOC). In all cases, aircraft are to be operated clear of cloud. The company AOC permitted operations in flight visibility of less than 1.0 mile but not less than 0.5 mile, provided the pilot met the standards set out by TC. The accident pilot did not meet the standard as he had not spent enough time on helicopters.
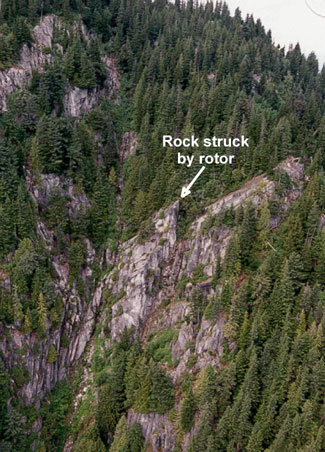
The accident site (latitude 49°47′48″ N, longitude 123°14′36″ W) was not on the normal or expected route for transit to or from the glacier or Lake Lovely Water, nor were there any apparent tourist attractions in the ravine. The initial impact was on a rock formation in a steep, narrow ravine in mountainous terrain below the tree line at about 3800 feet asl. The immediate terrain was too steep to retain the main parts of the wreckage, and the heavier parts tumbled down the ravine, coming to rest about 300 feet below. The mouth of the ravine spans about 300 feet. At the accident location, it spans about 100 feet. The rock formation that the accident helicopter hit protrudes into the ravine; from some angles, the extent of its protrusion is difficult to assess.
The helicopter tumbled down the ravine and sustained impact forces that violated the integrity of the cabin and transmitted intolerable forces to the occupants. The canopy and all the doors were separated from the cabin floor and aft cabin wall. The occupants were found in and close to the wreckage. Prior to departure, all the occupants were wearing properly-secured lap belts and shoulder straps. No details about their restraint in or ejection from the cabin are known; however, there had been stress on the seat belts and the attachment points.
Examination of trees in the vicinity of the initial impact area revealed damage consistent with that made by a hovering helicopter. Wreckage dispersal and reported injuries to the pilot and passengers are consistent with those demonstrated by rotating forces. There was some fuel spillage at the site, but no fire. Debris was spread from 3900 feet asl down to about 3600 feet asl in the ravine.
Following a preliminary examination of the wreckage at the site, the airframe, engine, and ancillary systems were transported to secure facilities and examined in greater detail. Particular attention was given to the engine, the flight controls, and the drive train. The main rotor blades were damaged at initial impact from contact with rock, about two feet from the blade tip. The main rotor blades then contacted the helicopter fuselage and trees in that order. These initial impact forces to the main rotor destroyed the rotor system. Drive component damage is consistent with damage from sudden stoppage while being powered. All component breakage and damage were attributable to the impact forces of the accident. There were no signs of any pre-existing mechanical deficiency or component or system malfunction that might have caused or contributed to the accident.
TSB investigators conducted flights in the accident area in a similar size helicopter. Once in the ravine, ground speed had to be less than 20 knots in order to manoeuvre safely. There was insufficient room to manoeuvre the helicopter much further up the ravine than the accident site. Flying at slow speed abeam the accident site, one can see across the ravine (about 75 feet); a rock formation protrudes up into the ravine. This rock formation is the one that the main rotor blades of the accident helicopter first contacted.
The company is a family-owned business. The accident pilot was the operations manager, as well as the chief pilot of the airplane side of the operation. However, he did not meet the requirements to act as chief pilot for helicopter operation. As a result, a separate chief pilot for helicopter operation was appointed. The helicopter chief pilot was a resident of Nanaimo, on Vancouver Island, about 2.5 hours away by surface transport, and he travelled overseas frequently, flying and consulting for a number of companies.
Helicopter sightseeing tour operations are conducted under Part VII, subpart 703 - Air Taxi. In addition, operations were to be conducted within the limitations of AOC number A/C10263, issued to A.A.L. Air Alps Ltd. by TC. CARs standards for air taxi helicopter operations require a chief pilot to have at least one year of experience within the preceding three years as a helicopter PIC. The chief pilot is responsible for the flight crews' professional standards, developing and maintaining standard operating procedures, and supervising flight crews. In the absence of the chief pilot, all responsibilities for duties were to be delegated to a person with equivalent qualifications. There were no documented company standard operating procedures for tour flights in poor weather, and the appointed chief pilot was not present at the company's base of operations on the days leading up to or on the day of the accident.
The most recent audit of the company conducted by TC was on 6 April 1999. This audit was for the issuance of the company's AOC for helicopters. All requirements were met except that the appointed chief pilot needed to complete a PPC on the Eurocopter AS350. That PPC was completed successfully the following week.
TC inspectors periodically monitor flights by large air carriers but do not normally monitor flights conducted by air taxi operators. TC inspectors from commercial and business and enforcement branches report that it is difficult to determine the level of pilot supervision provided by a chief pilot. Enforcement inspectors also report that it is difficult to enforce the applicable flight visibility regulations.
A TC review of the Safety in Air Taxi Operations (SATOPS) acknowledged that "many controlled flight into terrain (CFIT) accidents have occurred when the visibility was lower than the minimum allowable and the pilot continued to fly into instrument meteorological conditions (IMC). Pilots are still pushing the weather! The decision to continue flight into deteriorating weather conditions may be caused by operational pressures that the air operator or client are imposing on the pilot, because of pressure the pilot is putting on himself, or because flying in marginal VFR conditions, often IMC, has become the accepted way of operating."
Enforcement of regulations is only one option available to TC, and, increasingly, it has been supplemented with efforts to educate this industry in safe recommended practices. CARs do not require safety programs for air taxi operators, but many companies have established in-house safety programs. These programs, not necessarily formalized in the operations manual, normally comprise safety meetings from time to time, the posting of company bulletins about safety, open communication between operating personnel and management, open discussion of problems experienced in day-to-day operations, and, most importantly, management's insistence on safe operating practices. Annual pilot decision-making courses for all pilots, and Safety Officer training for managers and chief pilots, are being promoted for air taxi operators. These initiatives are intended to help pilots conducting VFR operations make the right decisions and not continue flight in deteriorating weather, especially when the visibility is lower than VFR minimums.
Analysis
Accident site scaring and damage to the main rotor blades indicate that the rotor blades struck a rock formation while the helicopter was manoeuvring, likely descending, at slow speed. These indicators also suggest that the initial impact was made as the blades were advancing on the left side of the aircraft. The initial impact forces to the main rotor destroyed the rotor system, making the helicopter uncontrollable. Because no indication was found of any malfunction or pre-existing mechanical defect, further analysis focusses on operational aspects of the accident flight.
The ravine was off the track that joined the lake and the airport, and since there were no apparent tourist attractions in the ravine, it is likely that the pilot flew into the ravine because of low visibility. The pilot did not cross the ravine at its mouth, which would indicate that the visibility at the time was less than the distance that spans the mouth and was probably equal to or less than the distance that spans the ravine in the vicinity of the accident site. When flying up the ravine abeam the accident site, the distance from the pilot's seat to the site is about 75 feet; and, because the helicopter had gone this far up the ravine, it is likely that the flight visibility was 75 feet or less. In this reduced visibility, the pilot would probably have slowed the helicopter to a hover close to terrain and navigated with reference to ground features. When flying a path from the southwest side of the ravine to the northeast side and trying to fly down the ravine back into the valley, the rock formation that was struck, which blends into the background, could initially be disregarded as not obtrusive. This rock formation would be on the pilot's blind side, aft left, as he focussed on the next clump of trees below. It is possible that the pilot, flying this path, descended onto the aforementioned rock formation with little or no sense of how close it was.
It is possible that the pilot was not acutely aware of how much more room was needed to clear obstacles on his left side, since he had limited experience flying the AS350BA.
Generally, there was little direct supervision of the accident pilot's operational activities. He was used to running the operation on his own, as the chief pilot did not live near the company's main operation. Specifically, on the day of the occurrence, the chief pilot was not in Squamish, leaving the pilot to rely on his own judgment and abilities to assess the safety of operating in poor or changing weather conditions.
There are inherent difficulties in enforcing flight visibility regulations for operators of small commercial aircraft.
TC inspectors are not able to determine pilot practices adequately nor the amount or quality of supervision. Also, with current regulations, they have difficulty enforcing flight visibility regulations. Therefore, the accident pilot was operating with ineffective operational supervisory and regulatory defences with regard to poor weather operations.
Findings
Findings as to causes and contributing factors
- At the time of the accident, the visibility at the accident site was concluded to have been about 75 feet.
- The helicopter was being flown in weather below the minimum visibility limits for aerial work (sightseeing) operations.
- While the helicopter was being manoeuvred close to terrain in poor visibility, the helicopter's main rotor struck a rock, making the helicopter uncontrollable.
- The pilot had limited experience in helicopter operations, and he was operating without effective operational supervision and regulatory defences.
Findings as to Risk
- The pilot seat position, relative to the rotor disc, is different in the accident helicopter than in the helicopter in which the pilot received his formative training.
- The emergency locator transmitter was destroyed by impact forces, and no emergency locator transmitter signal was received at any time. The ELT's location and construction are common for light helicopters.
Other findings
- The aircraft loading configuration, with respect to fuel, passengers, and cargo, was appropriate for the flight.
- No indication was found of any malfunction or pre-existing mechanical defect with the helicopter, its engine, or its systems.
Safety action
Safety action taken
Flight Visibility
"Safety Action" from TSB occurrence report A95H0012 states, in part,
Regardless of the prescribed minima, the variability of flight visibility and the subjectivity in assessing it from a moving aircraft make enforcement of visibility requirements implausible in most circumstances. . . The Board believes that many controlled flight into terrain (CFIT) accidents could be prevented if dangerous situations were recognized as conditions deteriorate. Therefore, the Board recommends that:
- The Department of Transport develop and implement a targeted national promotion campaign aimed at raising commercial operators' awareness of the inherent risks associated with flight operations in marginal VFR flight conditions.
In response, TC stated that it conducts Pilot Decision Making (PDM) courses, workshops, and briefings in all regions. A Notice of Proposed Amendment (NPA) for the CARs, issued 05 November 1999, changes the requirement for PDM training from one time to annually.
Emergency Locator Transmitter
Aviation Safety Information letter 950202 (TSB occurrence A95C0197), refers to ELT deficiencies, including the location of ELT installations on helicopters. The letter also refers to occurrence A95W0177: on 19 September 1995, following a collision in flight, Hughes 369D, C-GTZM and C-GXKF crashed and burned. The wreckage of the two helicopters was located about 70 miles east of Yellowknife, Northwest Territories. The ELTs in both helicopters were mounted in the front of the cabin and were destroyed. The tail booms of both helicopters survived the impact with relatively little damage. The TSB is of the opinion that ELTs would be better located in the tail sections of helicopters.
The Board is not aware of any changes in ELT installation practices that would enhance the survivability of ELTs in helicopter accidents.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .
Appendices