Reduced Power at Take-off and
Collision with Terrain
MK Airlines Limited
Boeing 747-244SF 9G-MKJ
Halifax International Airport, Nova Scotia
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 14 October 2004, an MK Airlines Limited Boeing 747-244SF (registration 9G-MKJ, serial number 22170) was being operated as a non-scheduled international cargo flight from Halifax, Nova Scotia, to Zaragoza, Spain. At about 0654 coordinated universal time, 0354 Atlantic daylight time, MK Airlines Limited Flight 1602 attempted to take off from Runway 24 at the Halifax International Airport. The aircraft overshot the end of the runway for a distance of 825 feet, became airborne for 325 feet, then struck an earthen berm. The aircraft's tail section broke away from the fuselage, and the aircraft remained in the air for another 1200 feet before it struck terrain and burst into flames. The aircraft was destroyed by impact forces and a severe post-crash fire. All seven crew members suffered fatal injuries.
1.0 Factual Information
1.1 History of the Flight
The series of flights for this crew originated at Luxembourg-Findel Airport, Luxembourg, on 13 October 2004, as MK Airlines Limited Flight 1601 (MKA1601),Footnote 1 destined to Bradley International Airport, Windsor Locks, Connecticut, United States. The aircraft operated as MK Airlines Limited Flight 1602 (MKA1602) from Bradley International Airport to Halifax International Airport, Nova Scotia, and was to continue as MKA1602 to Zaragoza, Spain, and return to Luxembourg.
The flights were operating with a heavy crew,Footnote 2 comprised of two captains, one first officer, and two flight engineers. A loadmaster and a ground engineer were also on board. The crew members for MKA1601/MKA1602 arrived at Luxembourg-Findel Airport at different times and dates. The captain and first officer of MKA1601, and flight engineer of MKA1602 operated a flight from Nairobi, Kenya, to Luxembourg-Findel Airport on October 12. The captain of MKA1602 and flight engineer of MKA1601 arrived in Luxembourg from Johannesburg, South Africa, on October 12 as operating crew of their first flight after a two-week period off duty. On October 13, the ground engineer and loadmaster arrived at Luxembourg as crew on the occurrence aircraft.
The planned departure time for MKA1601 was 1000 coordinated universal time (UTC).Footnote 3 At 0848, just before the crew's departure from the hotel in Luxembourg, the MKA1601 captain received a phone call from the MK Airlines Limited station liaison officer in Luxembourg, advising of a delay to the planned departure time due to the late arrival of the aircraft and late preparation of the cargo.
The captain, first officer, and flight engineer of MKA1601 checked out of the hotel at 0925. At 0941, the captain was advised that the aircraft loading was under way, and the captain, first officer, and flight engineer proceeded to the airport. The captain and flight engineer of MKA1602 checked out of the hotel at 1052 and proceeded to the airport.
When the MKA1601 captain arrived at the airport, he received the flight documentation from the Luxembourg station liaison officer. The flight documentation was prepared by the MK Airlines Limited operations centre in Landhurst, East Sussex, United Kingdom. It included the flight brief, the trip schedule, flight routing, weather, flight plan, planned fuel requirements, and planned payload. After the captain reviewed the flight documentation, he requested that 4000 kilograms (kg) of cargo be offloaded to carry additional fuel. The crew made the necessary adjustments to their flight documentation.
Another delay developed when the loadmaster noted that some of the pallets were contaminated with soil and would not be accepted by the authorities at Bradley International Airport. A vacuum cleaner was obtained and the MK Airlines Limited station liaison officer and loadmaster began to clean the pallets. So as not to delay the flight unnecessarily, the loadmaster took the vacuum cleaner on board to finish cleaning the pallets en route. The flight departed at 1556.
The first officer was identified as the pilot communicating with air traffic control (ATC) for the flight from Luxembourg to Bradley, except for a three-hour period during which time the voice communicating with ATC was that of another crew member. MKA1601 landed at Bradley International Airport at 2322.
At Bradley International Airport, all the cargo from Luxembourg-Findel Airport was offloaded. However, the cargo loading at Bradley was prolonged due to unserviceabilities with the aircraft's cargo loading system. With a captain and flight engineer crew change, MKA1602 departed Bradley International Airport for Halifax International Airport at 0403 on October 14, carrying another delay. The MKA1602 captain was the pilot communicating with ATC; the first officer was the pilot flying (PF).
MKA1602 landed on Runway 24 at Halifax International Airport at 0512 and taxied to the ramp. After shutdown, loading of the aircraft was started. During the loading, two MK Airlines Limited crew members were observed sleeping in the upper deck passenger seats. After the fuelling was complete, the ground engineer checked the aircraft fuelling panel and signed the fuel ticket. The aircraft had been uploaded with 72 062 kg of fuel, for a total fuel load of 89 400 kg. The ground engineer then went to the main cargo deck to assist with the loading.
Once the loading was complete, the ramp supervisor for the ground handling agent went to the upper deck to retrieve the MKA1602 cargo and flight documentation. While the loadmaster was completing the documentation, the ramp supervisor visited the cockpit and noted that the first officer was not in his seat. Approximately 10 minutes later, the ramp supervisor, with the documentation, left the aircraft. At 0647, the crew began taxiing the aircraft to position on Runway 24, and at 0653, the aircraft began its take-off roll. See Section 1.11.4 of this report for a detailed sequence of events for the take-off.
During rotation, the aircraft's lower aft fuselage briefly contacted the runway. A few seconds later, the aircraft's lower aft fuselage contacted the runway again but with more force. The aircraft remained in contact with the runway and the ground to a point 825 feet beyond the end of the runway, where it became airborne and flew a distance of 325 feet. The lower aft fuselage then struck an earthen berm supporting an instrument landing system (ILS) localizer antenna. The aircraft's tail separated on impact, and the rest of the aircraft continued in the air for another 1200 feet before it struck terrain and burst into flames. The final impact was at latitude 44°52′51″ N and longitude 063°30′31″ W, approximately 2500 feet past the departure end of Runway 24, at an elevation of 403 feet above sea level (asl). The aircraft was destroyed by impact forces and post-crash fire. All persons on board (seven crew members) were fatally injured.
1.2 Injuries to Persons
| Crew | Passengers | Others | Total | |
|---|---|---|---|---|
| Fatal | 7 | - | - | 7 |
| Serious | - | - | - | - |
| Minor/None | - | - | - | - |
| Total | 7 | - | - | 7 |
1.3 Damage to the Aircraft
The first damage to the aircraft occurred when, on rotation, the aircraft's lower aft fuselage struck the runway twice and remained on the ground to a point 825 feet beyond the end of Runway 24. Severe damage occurred when the aircraft's lower aft fuselage struck the berm and the vertical stabilizer and both horizontal stabilizers separated from the fuselage. The final impact was in a wooded area where impact forces and an extensive post-crash fire destroyed the remaining aircraft structure forward of the aft pressure bulkhead (see Photo 1).

1.4 Other Damage
Grass was uprooted in the area beyond the end of the runway where the aft section of the aircraft fuselage had dragged on the ground; as well, a number of approach lights for Runway 06 were destroyed. The ILS localizer antenna structure sustained significant damage when the aircraft struck the berm. Telephone and power lines adjacent to the main crash site were severed just before final impact. The surrounding wooded area was heavily damaged by the post-crash fire. Unburned fuel contaminated the soil in the immediate area of the crash site, requiring an extensive environmental clean-up.
1.5 Personnel Information
1.5.1 General
The operating flight crew of MKA1602 consisted of one captain, one first officer, and one flight engineer. The captain and flight engineer of MKA1601, a ground engineer, and a loadmaster were also on board.
| Operating Flight Crew | |||
|---|---|---|---|
| Captain | First Officer | Flight Engineer | |
| Licence | Airline Transport | Airline Transport | Flight Engineer |
| Medical Expiry Date | 01 July 2005 | 17 August 2005 | 13 August 2005 |
| Total Flying Hours | 23 200 | 8537 | 2000 |
| Hours Last 90 days | 254 | 245 | 186 |
| Hours on Type Last 90 Days | 254 | 245 | 186 |
| Hours off Duty Prior to Work | 29 | 17 | 17 |
| Non-Operating Crew | ||||
|---|---|---|---|---|
| Captain | Flight Engineer | Ground Engineer | Loadmaster | |
| Licence | Airline Transport | Flight Engineer | Maintenance | Not required |
| Medical Expiry Date | 15 July 2005 | 27 January 2005 | Not required | Not required |
| Total Flying Hours | 6000 | 1991 | Unknown | Unknown |
| Hours Last 90 Days | 171 | 202 | Unknown | 421 |
| Hours on Type Last 90 Days | 171 | 202 | Unknown | Unknown |
1.5.2 Operating Captain
The pilot-in-command (operating captain) of MKA1602 held a Ghanaian airline transport pilot licence (ATPL) with a valid instrument rating. He was qualified and certified in accordance with the Ghana Civil Aviation Regulations (GCARs). His licence was annotated with the remark "holder to wear spectacles which correct for near vision and shall have available a second pair whilst exercising the privileges of the license." Based on a review of the captain's medical records, there was no indication of any pre-existing medical condition or physiological factors that would have adversely affected his performance during the flight.
The captain had been with the company since its inception and started flying the McDonnell Douglas DC-8 with MK Airlines Limited in 1990. He was in one of the first groups of company pilots to transition to the Boeing 747-200 (B747). The captain successfully completed his United States Federal Aviation Administration (FAA) type rating training on the B747 in 1999 at the Pan Am Training Center in Miami, Florida. The captain's total flying time on the B747 was approximately 4000 hours.
In 2000, the company changed its B747 standard operating procedures (SOPs) and required all B747 flight engineers and pilots to undergo additional training. During this additional training, the captain had some difficulties adjusting to the new SOPs and his training was suspended. After two weeks of review and study, the captain returned to training and completed the course without further difficulty. Records indicate that there were instances where supervisory pilots had to counsel the captain regarding non-adherence to SOPs; however, in the period before the accident, he had demonstrated a marked improvement.
The captain trusted other crew members to perform their duties with minimal supervision. He was not comfortable using personal computers and software, such as the Boeing Laptop Tool (BLT) (see Section 1.18.1 of this report). He was more comfortable using manual methods to complete performance calculations, such as using runway analysis chartsFootnote 4 or Volume 2Footnote 5 of the aircraft flight manual (AFM). Generally, those who flew with him reported that he was competent flying the aircraft. He was respected and exercised adequate command authority in the aircraft, although he preferred to work in a casual manner.
1.5.3 Operating First Officer
The first officer held a Ghanaian ATPL with a valid instrument rating. He was qualified and certified in accordance with the GCARs. His last medical was conducted on 17 August 2004 with no annotations on the licence, although the medical records indicated that spectacles were worn for the eye test. The previous medical assessments were annotated with the remark "holder to wear spectacles which correct for distant vision and shall have available a second pair whilst exercising the privileges of the license." Based on a review of the first officer's medical records, there was no indication of any pre-existing medical condition or physiological factors that would have adversely affected his performance during the flight.
The first officer was reported to be a competent pilot and comfortable using personal computers. As the only first officer for the series of flights, he would have had to be an active crew member on duty on the flight deck for all take-offs, departures, arrivals, and landings for the series of flights.
1.5.4 Operating Flight Engineer
The flight engineer's licence was valid until 12 August 2005 and was endorsed for B747 aircraft. He was qualified and certified in accordance with the GCARs. His last medical was completed on 13 August 2004 and, based on a review of his medical records, there was no indication of any pre-existing medical condition or physiological factors that would have adversely affected his performance during the flight.
1.5.5 Loadmaster
The loadmaster was trained and qualified in accordance with company standards. Although a flight medical was not required in a licensing capacity, the loadmaster completed a company medical on 16 September 2000. He was found fit for employment and, based on a review of his medical records, there was no indication of any pre-existing medical condition or physiological factors that would have adversely affected his performance. Records indicate that the loadmaster had flown 421 hours on MK Airlines Limited aircraft during the previous 90 days.
1.5.6 Non-Operating Captain
The non-operating captain held a Ghanaian ATPL with a valid instrument rating. He was qualified and certified in accordance with the GCARs. His licence was annotated with a requirement for corrective lenses. His last medical was conducted on 15 July 2004 and he was found fit for duty. Based on a review of his medical records, there was no indication of any pre existing medical condition or physiological factors that would have adversely affected his performance. The non-operating captain was the pilot-in-command during the flight from Luxembourg-Findel Airport to Bradley International Airport.
1.5.7 Non-Operating Flight Engineer
The non-operating flight engineer's licence was valid until 26 January 2005 and was endorsed for B747 aircraft. He was qualified and certified in accordance with the GCARs. His last medical was completed on 27 January 2004 and, based on a review of his medical records, there was no indication of any pre-existing medical condition or physiological factors that would have adversely affected his performance.
1.5.8 Ground Engineer
The ground engineer held a Ghanaian maintenance licence endorsed for B747 aircraft. The ground engineer was not subject to a medical for licensing purposes. During his last company medical, he was found fit and, based on a review of his medical records, there was no indication of any pre-existing medical condition or physiological factors that would have adversely affected his performance.
1.6 Aircraft Information
1.6.1 General
| Manufacturer | The Boeing Company |
|---|---|
| Type and Model | B747-244SFFootnote 6 |
| Year of Manufacture | 1980 |
| Serial Number | 22170 |
| Certificate of Airworthiness | Issued 03 May 2004; valid until 02 May 2005 |
| Total Airframe Time/Cycles | 80 619 hours/16 368 cycles |
| Engine Type (number of) | Pratt & Whitney JT9D-7Q (4) |
| Maximum Allowable Take-off Weight | 377 842 kg |
| Recommended Fuel Type(s) | Jet A, Jet A-1 |
| Fuel Type Used | Jet A-1 |
On 08 October 2004, the number 2 and number 3 engines were replaced. The throttles for the number 2 and number 3 engines were significantly staggered from the number 1 and number 4 engines at reduced thrust power settings. This defect was written in the aircraft's logbook.
1.6.2 Aircraft Weight and Balance
1.6.2.1 Aircraft Empty Weight
The most recent calculations for the occurrence aircraft's weight and centre of gravity were conducted after a C-check in Jakarta, Indonesia, on 18 September 2004. A review of the 9G-MKJ Aircraft Weight and C.G. Determination document produced by Garuda Maintenance Facilities (GMF) AeroAsia, of the Garuda Indonesia Group, indicated an aircraft basic empty weight of 157 977.5 kg and an empty centre of gravity of 32.50 per cent mean aerodynamic chord (MAC).
A review of a duplicate copy of the BLT software for the occurrence aircraft, weight and balance summary page, indicated that the operating empty weightFootnote 7 was 157 977 kg; this was actually the basic empty weight of the aircraft. The BLT also indicated that the empty centre of gravity arm was 32.3 per cent MAC; this varied slightly from the 9G-MKJ Aircraft Weight and C.G. Determination document produced by GMF AeroAsia, which indicated 32.50 per cent MAC.
The occurrence aircraft carried a spares kit (also known as a fly-away kit) on board at the time of the accident flight. The kit contained spare aircraft parts and tools; MK Airlines Limited estimated the weight of the kit to be 800 kg. The aircraft also carried approximately 50 kg of catering for the crews. MK Airlines Limited used standard weights for the weight of the flight crew in the cockpit, totalling 270 kg. None of these three weights, which totalled 1120 kg, had been included in the operating empty weight in the BLT, or the mass and balance sheet that was used to calculate the aircraft weight for take-off.
1.6.2.2 Bradley International Airport Weight and Balance
The occurrence aircraft had a number of cargo floor power drive units (PDUs) removed from the aircraft and blanked off because they were unserviceable. As part of the cargo load, a large roll of steel was placed on a 20-foot-long pallet for a total weight of 13 206 kg. When the steel was being loaded onto the aircraft, it could only be moved by the cargo loading system as far as the functioning PDUs would permit. Normally, pallets can be manhandled into position if the PDUs are unserviceable, but, because of the weight of this pallet, it could only be loaded into positions LR and MR (see Figure 1).
The weight limits for positions LR and MR are 4264 kg respectively, for a total weight limit of 8528 kg. The weight of the steel and the pallet exceeded the limits by 4678 kg. The MK Airlines Limited operations manual (OM), Part A, Chapter 8, stated in part that "the loadmaster/captain must comply with additional structural limits as specified in the loading manual with regard to the maximum mass per cargo compartment." If all the PDUs had been serviceable, the steel load could have been properly placed in positions HR and JR, where the limit was 13 608 kg.
In addition to the cargo loaded at Bradley International Airport, the aircraft was loaded with 5921 US gallons of Jet A fuel. The take-off mass for Bradley was 239 783 kg, with an MAC of 25 per cent and a stabilizer trim setting of 4.0 units. The lateral imbalance was 18 248 kg, which was within allowable limits. The aircraft was within the centre of gravity limits of 13 to 35 per cent MAC for that weight.
1.6.2.3 Halifax International Airport Weight and Balance
The cargo uploaded in Halifax was comprised of 18 cargo pallets. On 13 October 2004, a local freight forwarder delivered these pallets to the MK Airlines Limited cargo handling agent at Halifax International Airport. Each pallet contained hundreds of individual STYROFOAMTM packages of fresh seafood, supported on wooden skids and secured by a cargo net. The cargo handling agency created a cargo manifest spreadsheet for the flight by taking the gross weight of each pallet, which had been supplied on the cargo manifests by the local freight forwarder. The agency then added 130 kg tare weight for the weight of the pallet and netting, for the total gross weight per pallet. There were 86 wooden skids supporting the fresh seafood on the cargo pallets. The weight of the wooden skids was not accounted for in the cargo pallet gross weight provided by the local freight forwarder, nor in the cargo manifest spreadsheet. Generally, wooden skids weigh between 20 and 25 kg; therefore, approximately 1900 to 2000 kg of extra weight was not accounted for in the cargo manifest. The local freight forwarder did not weigh the built-up pallets nor did the ground handling agent at Halifax International Airport have the facilities to weigh built-up cargo pallets that were provided by others.
In addition to the cargo loaded at Halifax, the aircraft was loaded with 88 637 litres of Jet A-1 fuel. The mass and balance sheet left behind at Halifax by the crew of MKA1602 indicated a total ramp fuel of 90 000 kg, a take-off mass of 350 698 kg with an MAC of 23 per cent, and a stabilizer trim setting of 5.8 units. The lateral imbalance was 88 kg. The aircraft was within the centre of gravity limits for that weight. The company pre-planned flight documentation indicated a minimum of 86 690 kg of fuel and a planned cargo load of 109 920 kg for a planned take-off mass of 353 310 kg.
When the weight of the wooden skids (2000 kg) and the combined weight of the fly-away kit, catering, and the flight crew (1120 kg) were added to the 350 698 kg weight calculated by the crew, the actual aircraft weight would have been approximately 353 800 kg.
1.6.3 Take-off Thrust
The B747-200 was originally certified in 1971 with JT9D-7 engines, which had a maximum thrust of 46 300 pounds (dry) and 47 900 pounds when using water injection (wet)Footnote 8 on take-off. In 1979, the JT9D-7Q engine was certified for use on the B747-200. It had a maximum thrust of 53 000 pounds; the occurrence aircraft was equipped with JT9D-7Q engines.
The maximum thrust available to an engine is dependent on the air density (pressure altitude and temperature of the air) in which the engine is operating. The maximum thrust that can be used for take-off is provided in the approved AFM, and before every take-off, the flight crew must calculate the power setting of the engine to achieve the maximum thrust. To extend engine life, it is common practice to use de-rated or reduced thrust, or a combination of both, for take offs when maximum thrust is not required, such as when taking off from long runways or with light loads.
De-rated thrust is a take-off thrust level less than the maximum take-off thrust for which a separate set of limitations and performance data exists in the AFM. The occurrence aircraft had a de-rated thrust of 46 300 pounds (JT9D-7 dry) and was referred to as "Rating II (RTG II)" in MK Airlines Limited documentation. Reduced take-off thrust is a thrust setting up to 25 per cent less than the maximum or de-rated take-off thrust. A reduced thrust setting is not restrictive in that it allows the flight crew to use maximum thrust at any time during the take off, if desired.
The MK Airlines Limited OM stated that, when setting take-off thrust, the operating crew must advance thrust levers to 1.10 engine pressure ratio (EPR),Footnote 9 check that engine indications are stable and symmetrical, then advance thrust levers to approximately 1.20 EPR and call for "max thrust"Footnote 10 to be set by the flight engineer.
1.6.4 Aircraft Performance Data
According to the B747 AFM, Section 4, Performance, the stall speed for flap 20, at idle power and 353 800 kg, is 133 knots calibrated airspeed (KCAS). The stall speed is based on the aircraft in-flight and out-of-ground effect. The expected minimum unstick speed (Vmu)Footnote 11 for the Halifax International Airport configuration was determined to be approximately 150 ± 2 KCAS. The B747 has an over-rotation stall warning system that activates a control column shaker during take-off when the rate or angle of rotation is excessive. The warning is deactivated when a body landing gear leaves the runway. Two stall warning systems are activated when the nose gear leaves the runway. Control column shaker was not a recorded value on the flight data recorder (FDR).
The B747 AFM indicated that, for the pressure altitude and airport temperature at the Halifax International Airport at the time of the occurrence, an EPR setting of 1.60 was required for maximum thrust, with a maximum reduction of 0.21 EPR for reduced thrust. The de-rated maximum thrust EPR setting was 1.43, with a maximum reduction of 0.14 EPR for reduced thrust.
Climb power for the occurrence flight, derived from the MK Airlines Limited quick reference handbook (QRH), was 1.33 EPR. During a reduced thrust take-off, some pilots at MK Airlines Limited would set climb EPR rather than take-off EPR if the climb EPR was the higher value. Go-around power from the QRH was 1.52 EPR.
1.6.5 Tail Strike Information
According to the aircraft manufacturer, the B747-200 lower aft fuselage will contact the ground at a pitch attitude of 11.1° with static body gear oleo compression, and 13.1° with the body gear fully tilted and the oleos fully extended. The MK Airlines Limited OM indicated that the normal target pitch attitude for rotation is 12° with a rotation rate of 2° to 3° per second; lift-off should occur at approximately 10° pitch attitude. The manufacturer has determined that, for every five knots of airspeed below rotation speed (Vr),Footnote 12 the angle of attack must be increased by 1° to gain the equivalent amount of lift during the rotation.
1.7 Meteorological Information
The 0600 Halifax International Airport weather was as follows: wind 250° true (T) at five knots, visibility 15 statute miles (sm), overcast clouds at 1700 feet above ground level (agl), temperature 10°C, dew point 9°C, and altimeter setting 29.67 inches of mercury (in Hg). The weather issued at 0700 was as follows: wind 260°T at six knots, visibility 15 sm, overcast clouds at 1800 feet agl, temperature 10°C, dew point 9°C, and altimeter setting 29.67 in Hg. The airport's terminal area forecast corresponded to the actual weather.
1.8 Aids to Navigation
At the time of the accident, the crew was using visual references for the take-off and was not relying on ground-based navigation aids. No discrepancies were discovered with the aids to navigation.
1.9 Communications
All communications between the Halifax International Airport air traffic controllers and MKA1602 were normal, and there were no deviations from published procedures. There were, however, some problems with the Aircraft Rescue and Fire Fighting (ARFF) communications (See Section 1.14.3 of this report).
1.10 Aerodrome Information
1.10.1 Introduction
The Halifax International Airport is located at latitude 44°52.85′ N and longitude 063°30.52′ W, at an elevation of 477 feet. It is a certified aerodrome operated by the Halifax International Airport Authority (HIAA) on land leased from Transport Canada (TC). Runway 24 was in use at the time of the accident. It is oriented 234° magnetic (M), constructed of asphalt and concrete, and is 8800 feet long by 200 feet wide. Runway 24 has a published take-off run available of 8800 feet and a clearway of 1000 feet, providing a take-off distance available of 9800 feet.
1.10.2 Airport Electrical Power Supply
Just before impact, the aircraft severed a power cable and several telephone cables supplying the airport. Four diesel generators with auto-start capability, available to provide backup power to the airport power grid, started when the power cable was cut. Three of the generators supplied power to the airport grid; however, a circuit breaker tripped due to a power surge when the aircraft cut through power lines adjacent to the main crash site, preventing the fourth generator from supplying power. Approximately one hour after the accident, power from the fourth generator was restored when technical personnel manually reset the main circuit breaker. The control tower at Halifax International Airport was equipped with a separate stationary uninterruptible power unit and an independent backup power generator; consequently, there was no loss of electrical power to the tower.
The Halifax International Airport fire hall normally would receive backup power from two of the four generators mentioned above. The generator with the tripped circuit breaker should have powered a relay to permit operation of the following fire hall systems: bunkroom lights, vehicle bay lights, and the automatic opening of the vehicle bay doors. Because these systems were not powered, the firefighters had to respond in a darkened environment, and the vehicle bay doors had to be opened by pushing the manual door-open button at each bay. Because the door motors were powered by an operating generator, the doors then opened. The vehicle bay lights in the fire hall were "high-pressure sodium bulbs," which take approximately 10 minutes to reach full brightness; therefore, they would have been ineffective in a quick response scenario.
Had the fourth generator operated as expected, it would have taken 25 to 30 seconds for the bunkroom lights to come on, because of the time it would have taken for the fourth generator to reach full capacity. The fire hall had been equipped with self-contained battery-operated lights; however, when the emergency power generators were installed, these lights were removed.
1.10.3 Runway 24 Slope
In 2002, TC requested that NAV CANADAFootnote 13 publish a slope of 0.17 per cent down for Runway 24 at Halifax International Airport in the Canada Flight Supplement and the Canada Air Pilot. TC's TP 312, Aerodrome Standards and Recommended Practices, Section 3.1.2.1, described how to calculate runway slope. Using TP 312, investigators from the Transportation Safety Board of Canada (TSB) calculated the slope for Runway 24 to be 0.19 per cent up. This error in direction and magnitude was not detected by NAV CANADA personnel before this information was published, nor was the error detected during subsequent reviews of these publications by the airport operator.
There are no standards for publishing slope values or slope changes for runways at Canadian airports, except that NAV CANADA documentation indicates that a slope of less than 0.3 per cent is not to be published.
Runway 24 has several slope changes. The two most significant are from the threshold of Runway 24 to the highpoint of the runway, which is 6975 feet from the threshold. The slope for this section is 0.24 per cent up. The slope for the remaining 1825 feet is 0.55 per cent down. The total absolute change in slope is 0.079 per cent up.
A review of non-Canadian aeronautical publications available to flight crews revealed conflicting information. One of these publications did not indicate any slope information for Runway 24. Another publication had the correct value and direction. A third described the slope for Runway 24 in two segments. The BLT runway information for Runway 24 was imported from a SITAFootnote 14 data file on 19 September 2003 at 0952. It stated that Runway 24 had a slope of 0.08 per cent up and a field length of 8800 feet, plus 150 feet of paved overrun.
International Civil Aviation Organization (ICAO) Annex 15, Aeronautical Information Services, Part 3, specifies that the detailed description of runway physical characteristics for each runway is to include information on the slope of each runway and its associated stopways. Chapter 2 of ICAO Annex 4, Aeronautical Charts, Paragraph 2.17.1, states in part, "States shall insure that established procedures exist in order that aeronautical data at any moment is traceable to its origin so to allow any data anomalies or errors, detected during the production/maintenance phases or in the operational use, to be corrected." The Canadian Aviation Regulations specify that the operator of an airport shall review each issue of each aeronautical information publication on receipt thereof and, immediately after such review, notify the Minister of Transport of any inaccurate information contained therein that pertains to the airport.
1.10.4 Earthen Berm
An earthen berm, with a concrete slab on top to anchor the localizer antenna, was located 1150 feet from the end of Runway 24 on the extended centreline (see photos 2, 3 and 4). This berm was constructed in the fall of 2003 to support a new localizer antenna at a height necessary to meet ICAO localizer signal coverage requirements. The berm was 11.6 feet high, but since the terrain sloped downwards from the end of the runway, the concrete pad on top of the berm was in fact the same elevation as the end of the runway. The localizer antenna projected another 10 feet from the top of the berm. At the same time, a similar berm was constructed off the end of Runway 06 at a distance of 650 feet from the end of the runway. There are similar earthen berms in use at other airports in Canada, including one at Fredericton, New Brunswick, and several at Toronto/Lester B. Pearson International Airport, Ontario.
NAV CANADA submitted an Aeronautical Obstruction Clearance Form to TC on 27 August 2003 for the construction of both berms to support new localizer antennae. Approval was received on 08 September 2003. However, airport personnel raised a number of concerns when the berm on the approach to Runway 24 was first being constructed, primarily because it was thought to be a potential hazard. The HIAA corresponded with TC and requested clarification on whether the berm would affect the airport's certification. Based on an inspection of the berm by TC personnel, TC advised the HIAA in a letter dated 08 October 2003 that the berms for the new localizers on both Runway 06 and Runway 24 were not in conflict with airport certification standards.
In a follow-up letter from TC to the HIAA on 22 October 2003, TC stated, "Based on information supplied by NAV CANADA, we have determined that the subject localizers are in compliance with airport certification standards. Additionally, clearways are not affected and the existing TODAs [take-off distances available] will remain unchanged." The letter concludes, "Thus, from an airport certification perspective, we have no concerns about the installation of the new localizers on Runway 06 or Runway 24."
Airport certification standards are contained in TP 312. Each end of runways 06 and 24 had a clearway to ensure that there was an obstacle-free zone for departing aircraft. An obstacle-free zone comprises the airspace above the approach surface, inner transitional surfaces, and that portion of the strip bounded by these surfaces that is not penetrated by any fixed obstacle other than one that is required for air navigation purposes, is low mass and frangibly mounted. The HIAA did not list any obstacles, as defined in TP 312, for the departure paths for runways 06 and 24. The earthen berm was not considered an obstacle because it did not penetrate into the obstacle-free zone.
TP 312 uses the ICAO phraseology of "standard" or "recommended practice" to identify specifications considered to have a direct impact on the safety of flight from those that affect only operational efficiency. Only the standards contained in TP 312 are mandatory for the certification of Canadian airports; recommended practices are optional and might or might not be implemented. One of the recommended practices in TP 312 is to establish a runway end safety area (RESA). A RESA is defined as an area symmetrical about the extended runway centreline and adjacent to the end of the strip, primarily intended to reduce the risk of damage to an aeroplane undershooting or overrunning the runway.
According to TP 312 recommended practices, a RESA should extend from the end of a runway strip for as great a distance as practicable, but at least 90 m (295 feet). The runway strips for runways 06 and 24 at Halifax extend for 60 m (197 feet) beyond the threshold of each runway. The minimum distance specified for a RESA in the recommendations therefore would be at least 150 m (492 feet) at Halifax International Airport. The berms for the localizers for runways 06 and 24 are both located beyond these minimum recommended distances. There is no RESA published for the Halifax International Airport. ICAO considers a RESA to be a standard (ICAO Annex 14, Section 3.5.1) rather than a recommended practice.
1.10.5 Halifax Automatic Terminal Information Service
The following automatic terminal information service (ATIS) broadcasts were issued during the time MKA1602 arrived and departed Halifax International Airport:
- Halifax International Airport information Victor, weather at 0400 ZuluFootnote 15 - wind 260 [degrees] at 7 [knots], visibility 15 [sm], ceiling 2200 [feet asl] overcast, temperature 10 [°C], dew point 9 [°C], altimeter 2966 in Hg, approach ILS Runway 24, landing and departing Runway 24, inform ATC that you have information Victor.
- Halifax International Airport information Whiskey, weather at 0500 Zulu - wind 260 at 5, visibility 15, ceiling 1800 overcast, temperature 10, dew point 9, altimeter 2967 in Hg, approach ILS Runway 24, landing and departing Runway 24, inform ATC that you have information Whiskey.
- Halifax International Airport information X-Ray, weather at 0600 Zulu - wind 270 at 5, visibility 15, ceiling 1700 overcast, temperature 10, dew point 9, altimeter 2967, approach ILS Runway 24, landing and departing Runway 24, inform ATC that you have information X-Ray.
1.11 Flight Recorders
1.11.1 Cockpit Voice Recorder
The cockpit voice recorder (CVR) was a Collins model 642C-1, part number 522-4057-010, serial number 1660, that was fitted in March 2004. The CVR was found under debris in its mounting bracket near its installed location (see Photo 5), and it had been exposed to fire and extreme heat for an extended period. The recording tape had melted; consequently, no CVR information was available to investigators. Although this model of recorder was not required to meet the more stringent fire test requirements that exist today, the conditions of extreme heat were such that the likelihood of any tape-based recorder surviving in those conditions is considered very low.
1.11.2 Flight Data Recorder
The flight data recorder (FDR) was a Sundstrand, part number 981-6009-011, serial number 2756, that was fitted in April 2004. It had a 25-hour recording capability and recorded a total of 107 parameters. The recording medium was Vicalloy tape. The FDR was found in the main cabin area forward of the wing root (see Photo 5). The FDR suffered impact and heat damage in the crash and the tape broke in two places. The FDR contained information from the previous six flights and good data for the accident flight. A small portion of data for the accident flight was not available because of the necessity to splice the tape where it had broken during the impact sequence.
1.11.3 Flight Data Recorder Data Losses
The FDR data had several areas where data were lost due to signal distortion and dropouts. In some areas, the distortion was such that no recovery could be made. Data cycling causing dropouts was observed during the taxi segment, the initial portion of the take-off and the final 12 seconds of the recording. The data cycling was left as valid data to show this characteristic on the data plots (before and at the start of the take-off roll), even though the recorded data for the affected parameters were not valid. This cycling was tagged as invalid in the last 12-second segment of the flight to remove the dropouts from the data plots.
1.11.4 Halifax Take-off - Flight Data Recorder Recorded Events
After push back, the aircraft began to taxi, the flaps were extended to 20°, and the horizontal stabilizer was set to 6.1 trim units,Footnote 16 where it remained for the duration of the flight. The flight control checks were completed during the taxi. The aircraft entered Runway 24 at Taxiway Delta and backtracked to the threshold. The aircraft then made a 180° turn to the right and, upon lining up with the runway (234°M), the thrust levers were advanced and a rolling take-off was commenced at 0653:22.
At the start of the take-off roll, the thrust levers were smoothly advanced from ground idle thrust (approximately 1.0 EPR) to take-off power with all final EPR settings indicating between 1.3 and 1.33. The aircraft accelerated through 80 KCAS (0653:46) approximately 1800 feet from the threshold.
At 130 KCAS, the control column was moved aft to 8.4° to initiate rotation as the aircraft passed the 5500-foot mark of Runway 24 (3300 feet of runway remaining). The commanded elevator deflection was consistent with the control column input, and the aircraft began to rotate (see Appendix C - Take-off Sequence). The initial rotation rate was approximately 2.2° per second. The pitch attitude stabilized briefly at approximately 9° nose-up, with airspeed at 144 KCAS. The tilt switchFootnote 17 on the FDR continued to record GROUND. The control column was then moved further aft to 10°, and the aircraft responded with a further pitch up to approximately 11°; initial contact of the lower aft fuselage with the runway occurred at this time. The aircraft was approximately at the 8000-foot mark and slightly left of the centreline (see Photo 2). The control column was then relaxed slightly, to 9° aft.
The pitch attitude stabilized in the 11° range for the next four seconds, and the lower aft fuselage contact with the runway ended briefly. With approximately 600 feet of runway remaining, the thrust levers were advanced to 92 per cent (100 per cent is full forward) and the EPRs increased to 1.60. With 420 feet remaining, the lower aft fuselage contacted the runway a second time. As the aircraft passed the end of the runway, the control column was 13.5° aft, pitch attitude was 11.9° nose-up, and airspeed was 152 KCAS. The highest recorded nose-up pitch of 14.5° (0654:24) was recorded after the aircraft passed the end of the runway at a speed of 155 KCAS, during which time the tilt switch discrete changed to AIR. The aircraft became airborne approximately 670 feet beyond the paved surface, the point where the ground scars ended. When the recorded tilt switch position changed to AIR, the airspeed was approximately 155 KCAS, consistent with the Vmu of 150 ± 2 KCAS, indicating that there was sufficient lift to fly. At this point in the FDR data, there were gaps in the recorded information due to data dropouts and data cycling (as described in Section 1.11.3 of this report).
Two additional pitch samples were recorded indicating rapid nose-down pitching to −20° (0654:29). This information was consistent with lower aft fuselage impact with the localizer berm and loss of the tail section, resulting in a subsequent nose-down pitching moment.
1.11.5 Halifax Take-off Compared to the Bradley Take-off
The FDR data for the take-off from Halifax International Airport (calculated aircraft weight of 353 800 kg) was compared with the Bradley International Airport take-off (aircraft weight of 239 783 kg) to determine what similarities, if any, existed between the two flights (see Appendix A - Flight Data Recorder Engine Data Comparison Between Bradley and Halifax and Appendix B - Flight Data Recorder Flight Controls Comparison Between Bradley and Halifax). The comparison focused on the take-off speeds, engine performance, rotation characteristics, and corresponding control inputs and control surface movements.
On both take-offs, the rotation speed was approximately 130 KCAS and 20° of flap was used. During the Bradley take-off, the aircraft reached rotation speed approximately 13 seconds sooner, indicating a higher rate of acceleration compared to the occurrence flight. The engine data were very similar for both take-offs, with the EPRs set in the 1.30 to 1.33 range. In both cases, the engines spooled up normally and stabilized at take-off thrust with no anomalies noted. On the Bradley take-off, the initial pitch rate at rotation was approximately 1.2° per second, and the aircraft climbed away four seconds later as the pitch angle increased through 6°. On the Halifax take-off, the pitch rate was higher at 2.2° per second; however, the aircraft did not lift off the runway as the pitch attitude stabilized near 10°. The pitch attitude subsequently reached the 11° range and eventually at least 14.5°.
1.12 Wreckage and Impact Information
1.12.1 Impact Information
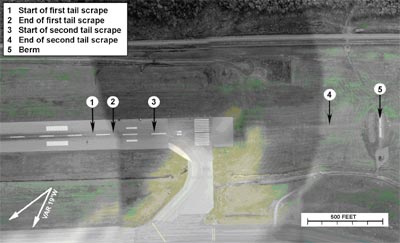
The first indication of aircraft contact with the runway was a scrape mark, which began 830 feet before the end of Runway 24 and was 30 inches left of the runway centreline; it became progressively wider, ending 705 feet from the end of the runway. The scrape mark formed a line approximately one-half degree off the centreline toward the left (see Photo 2).
A second scrape mark began 412 feet from the end of the runway and was initially about 3 inches wide, expanding to about 24 inches wide at the runway threshold. There were aluminum scrapes and shavings all along this scrape mark. It continued through the paved runway overrun area and across the grassy area. On the grassy area, the ground scar was initially about 24 inches wide and 2 inches deep, eventually fanning out to about 30 inches wide (see Photo 3). The ground scar became less pronounced until it disappeared at a point approximately 315 feet before the berm, indicating that the aircraft became airborne. The only indication of aircraft contact with the ground was the ground scar caused by the lower aft fuselage. There was no indication that the tires contacted the ground beyond the paved surface. No primary aircraft structure was found in the debris trail before the berm.

Fuselage structure, comprising the fuselage joint of the aft pressure bulkhead at Station 2360 and some adjacent belly skin, was found embedded in the berm. These pieces were embedded approximately 18 feet to the left of the extended runway centreline, about 30 inches below the top of the concrete pad, and had penetrated about 24 inches into the berm. Black rubber transfer marks, consistent with aircraft tire contact, were on some of the fractured pieces of the ILS antenna, indicating that the tires had struck the antenna (see Photo 4). No similar marks were observed across the concrete pad on top of the berm, indicating that the tires were above the concrete pad as the aircraft passed over it. The pieces of aircraft belly skin found embedded in the berm were identified as coming from the centreline of the aircraft and included roughly the same amount of structure from each side of the centreline. This is consistent with the aircraft having struck the berm in a roughly wings-level attitude. The aircraft pitch was between 15° and 24° at berm impact. If the aircraft was pitched at less than 15°, the wheels would have struck the top of the berm, and if the aircraft was pitched at greater than 24°, the tires would not have struck the antenna.

Immediately beyond the berm, there was extensive debris that included the vertical and horizontal stabilizers, a section of aft pressure bulkhead, the tail cone, the auxiliary power unit, and some pieces of aft fuselage belly skin. In the wooded area beyond the berm, there were numerous smaller pieces of aircraft structure and cargo. The debris trail then diminished until the main impact, suggesting that, following the separation of the empennage, the rest of the aircraft remained relatively intact until impact (see Photo 5).

The aircraft struck a wooded area beyond the airport boundary fence in a downward trajectory of approximately 6° to 16°, in a roughly wings-level attitude. It struck nose-first, with sufficient force that the forward fuselage section separated from the remainder of the fuselage, resulting in severe structural break-up and an intense post-crash fire. The debris trail extended approximately 1000 feet into a quarry. There was no indication of pre-impact fire damage.
1.12.2 Wreckage Examination
The primary flight controls (rudders, elevators, horizontal stabilizers, and ailerons) and secondary flight controls (spoilers, trailing edge flaps, leading edge variable camber, and Krueger flap) were examined, and no discrepancies were noted that would have indicated a pre-existing condition that would have prevented normal operation. Stabilizer position was determined to be between 5.5 and 5.6 unitsFootnote 18 aircraft nose-up based on actuator ballscrew measurements. Three of the four trailing-edge flaps were in the flaps 20 position, and the fourth flap was found in the flaps 10 position, based on ballscrew measurements. However, based on FDR data, it is likely that the fourth flap was in the flaps 20 position during take-off and was repositioned during the impact sequence.
The auto throttle speed indicator was recovered with a reading of 037 through the viewing window. Based on smear and dirt patterns, it was concluded that the likely value of the indicator after impact was 147. The captain's airspeed indicator (ASI) was recovered; the instrument face was missing and there were no plastic bugs on the external ring.
A number of paper documents were recovered from the accident site and examined by TSB investigators. The most significant of these was the voyage report sheet for this series of flights, which contained the MKA1601 captain's comments regarding duty time (see Section 1.18.5.3 of this report). The completed take-off data card used by the crew for the accident take-off was not found.
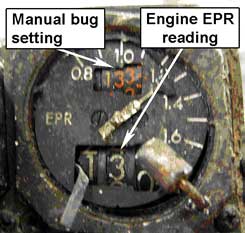
The number 2, number 3 and number 4 EPR gauges were recovered and examined. The number 2 EPR gauge had a manual bug setting of 1.32 and an engine indication reading of 1.01; the number 3 EPR gauge had a manual bug setting of 1.3X (the last digit had broken off at impact) and an engine indication reading of 1.02; and the number 4 EPR gauge (see Photo 6) had a manual bug setting of 1.33 and an engine indication reading of 1.305. The EPR settings on the three recovered instruments were set to 1.32-1.33. These readings were considered to be reliable, with the slight differences attributed to movement during the impact sequence.
FDR recorded data indicated that the engines were operating at a high power setting at the time the aircraft struck the berm; after impact, the data show that the power was reduced before final impact with the terrain. An on-site examination of the engines showed damage consistent with the engines still producing power at the time of final impact. The landing gear was in the down position.
Fuel tests performed on the fuel supplier's fuel storage tanks did not identify any discrepancies.
All the thrust reversers were stowed at the time of the impact. Aircraft records indicated that the thrust reverser system of the number 3 engine was "locked out" (in the stowed position). The FDR data indicated that the thrust reversers had not been deployed before impact.
1.13 Medical Information
All the occupants were identified by DNA testing, and where dental records were available, they were used to verify the identity of the crew members. Forensic examination and toxicology tests did not indicate any physiological conditions or the presence of foreign substances that might have impaired the performance of any flight crew member.
1.14 Fire
1.14.1 General
The Halifax International Airport ARFF met the service standards specified in the Canadian Aviation Regulations, Part III, Section 323, Aerodrome and Airport Standards, which refer to aircraft fire fighting at airports and aerodromes. The ARFF at Halifax International Airport was last inspected by TC on 27 November 2003 and no deficiencies were found.
On 29 July 1997, a Mutual Aid Fire Fighting Agreement was signed between Halifax International Airport ARFF and the Halifax Regional Fire and Emergency Service. This type of agreement is often used by airports and municipal fire departments to outline the responsibilities of the parties involved where one agency requires the other's assistance. Although the agencies had the mutual aid agreement, there had only been limited opportunities for mutual inter-agency training.
On seeing the fireball of the aircraft, the Halifax International Airport tower controller activated the crash alarm. The airport ARFF units responded and arrived at the accident site approximately five minutes after the crash alarm sounded; the site was on airport property, but outside the airport perimeter security fence. The Halifax Regional Municipality (HRM) Fire Department, the Enfield Fire Department, Emergency Health Services and the Royal Canadian Mounted Police (RCMP) all responded within minutes of the accident. The RCMP established a security perimeter and controlled access to the site.
1.14.2 Grid Map
The HIAA Emergency Plan Manual contained a grid map of the Halifax International Airport that depicted the airport runways, taxiways, structures, roads, security fence, and the airport property boundaries. The map was divided into a numbered and lettered grid to permit rapid and clear identification of any response area. Copies of the grid map were posted in the airport fire hall, the ATC tower cab, the security operations centre and the emergency operations centre, and were carried in all airport emergency vehicles.
On hearing the crash alarm, the fire brigade captain in the airport fire hall contacted the air traffic controller over the crash phone to get confirmation that an emergency situation was in progress. The location of the accident site was described to him in general terms of the area and direction, which was normal controller practice; grid map coordinates were not used. When the airport firefighters departed the fire hall, they saw the fire and proceeded to the accident site.
The NAV CANADA air traffic controllers were provided training on how an aerodrome grid map is used to identify areas of an airport. In support of ARFF training at the Halifax International Airport, the air traffic controllers had used the grid map in the past to direct the response of the firefighters to different locations in the airport.
The 911 operator directed the other responding agencies to the accident site by relaying the general location description that was available. This resulted in some confusion as to the exact location of the accident site. There are no regulations, standards or local procedures that require the use of aerodrome grid maps for emergency response and none of the other responding agencies had copies of the Halifax International Airport aerodrome grid map available in their vehicles.
A TSB Safety Advisory was sent to TC following a 1998 accident (TSB report A98Q0192), on the subject of using grid maps for reliable and efficient direction during emergency responses to aircraft accidents. TC replied on 14 August 2000 to advise the TSB that the subject was to be addressed in a Notice of Proposed Amendment to the aerodrome safety regulations and standards. This change has not occurred to date.
1.14.3 Radio Communications
Each ARFF vehicle was equipped with very high frequency, two-way radios, which were used to communicate with the air traffic controller on ground control frequency. The firefighters also had portable ultra high frequency radios that, because of a blind spot at the site, could not be used to communicate with the HIAA Emergency Operations Centre. These radios could have been used at the site for ARFF communication had they used the "simplex" mode, which allows direct communications at short distances.
The ARFF firefighters eventually had to communicate using hand signals until they were supplied with a portable trunk mobile radio from another response agency. The Halifax International Airport ARFF had a portable trunk mobile radio unit that could have been used to communicate with outside agencies such as the Halifax Regional Fire and Emergency Service dispatch facility and the RCMP. However, it had been left at the fire hall. The firefighters also attempted to use their individual cell phones to communicate with the Emergency Operations Centre, but the signal was unreliable.
1.14.4 Site Command
The Halifax International Airport ARFF firefighters were the first on the scene and took command of the situation. Although they were responding outside the airport perimeter security fence, they suspected that the aircraft was still on airport property. The HIAA Emergency Plan Manual stated that the airport's ARFF was to be the lead agency in the event of an aircraft crash "on airport," and the municipal fire department was to be the lead agency in the event of an aircraft crash "off airport." Although the responsibilities for on or off airport crashes were described in the different documents, the actual boundary separating the two areas was not clearly defined. In several locations, the airport property limits extended outside the airport perimeter security fence.
When HRM Fire Department firefighters arrived at the accident site, they observed the aircraft to be outside the airport perimeter security fence; consequently, they assumed that they were the lead agency. A unified command post was established that included the HRM Fire Department, Emergency Health Services, the RCMP and, eventually, Halifax International Airport ARFF. This temporary confusion as to who was in command of the site did not cause significant problems. Some responders noted that there was a need for more inter-agency training.
1.14.5 Persons on Board and Dangerous Goods
Information on the number of persons and dangerous goods carried on board the aircraft was not readily available to air traffic controllers in the Halifax International Airport tower. Shortly after the accident, the air traffic controllers unsuccessfully attempted to contact the ground handling agency at the airport to learn the number of persons and dangerous goods on board MKA1602.
In accordance with ICAO's Technical Instructions for the Safe Transport of Dangerous Goods by Air, shipping documentation must accompany dangerous goods on board an aircraft. The MKA1602 flight crew had copies of the shipping documentation and copies were also available at Bradley International Airport, where the dangerous goods were loaded on the aircraft. Regulations only require that copies of shipping documentation be left at an airport where the dangerous goods have been loaded; therefore, authorities at intermediate airports are not aware of all the dangerous goods that might be on board an aircraft.
Approximately one hour after the accident, MK Airlines Limited operations staff contacted the Halifax International Airport control tower and informed the controller that there were seven crew members on board MKA1602. This information was immediately relayed to ARFF and to the HIAA Emergency Operations Centre. At 0840, MK Airlines Limited informed the ARFF that no dangerous goods had been loaded on MKA1602 at the Halifax International Airport. At 1700, about 10 hours after the accident, MK Airlines Limited sent a 30-page fax listing the dangerous goods that had been loaded on board the aircraft at Bradley International Airport. The goods included medical supplies, adhesives, paint, food flavouring, and motor vehicles.
When an aircraft in flight declares an emergency, controllers get the information regarding the number of persons and dangerous goods on board directly from the flight crew. In the event that it is not possible to communicate with the flight crew, the affected company should be able to provide this information, though it might take some time. However, rarely do controllers have the required contact information for the many airline companies.
1.15 Survival Aspects
The occupants were all located in the cockpit and upper deck rest area behind the cockpit. These areas were severely compromised during the impact and break-up of the aircraft. There was also an intense post-crash fire. The accident was not survivable.
1.16 Tests and Research
The aircraft manufacturer was requested to provide analysis on the aircraft performance characteristics of MKA1602 during the take-off at Halifax International Airport. The manufacturer used two independent software tools to assess the take-off of MKA1602, using the FDR data from the accident and previous flights. The TSB and the United States National Transportation Safety Board (NTSB) reviewed the manufacturer's analysis. It was found that the performance characteristics of MKA1602 were consistent with that expected for normal operation. The simulation EPRs and recorded FDR EPRs were similar, further validating the simulation models for the take-off roll condition. Both software tools provided a consistent result that showed the actual weight of the aircraft to be reasonably near to that calculated by the TSB for the attempted take-off at Halifax International Airport.
The manufacturer's engineering analysis also provided a hypothetical flight path the aircraft would have taken if the berm had not been present. Limitations of the software and the many assumptions required to model such a take-off (where the aircraft lower aft fuselage is dragging) made it difficult to determine a clear result. However, assuming that the performance of the aircraft remained as it was before impact with the berm, it is considered likely that the aircraft would have stayed airborne, possibly contacting tree tops located 2000 feet beyond the end of the runway. The elevation of the top of the berm was the same as the end of the runway, and the tree tops were estimated to be at about the same elevation as the berm or slightly higher (see Photo 3).
1.17 Organizational Information
1.17.1 MK Airlines Limited
1.17.1.1 General
The company began operations with a single DC-8 aircraft in 1990 as Cargo d'Or, using a Ghanaian air operating certificate (AOC). During this same period, the airline established an office in the United Kingdom near Gatwick Airport to facilitate general sales for the company. In 1993, the company invested in another airline in Ghana called Venus Air, and transferred the Cargo d'Or aircraft to the Venus Air AOC. Concurrently with the transfer, the name of the airline was changed to MK Airlines Limited. In November 1993, the commercial offices in Gatwick were moved to the present location at Landhurst, East Sussex. The enhanced communication and infrastructure potential at the new location facilitated improved in-house management functions, flight training, maintenance, crew scheduling, and operational control.
As the company expanded, more DC-8 aircraft were added to the fleet and more employees joined the company. Most of the new flight crew members were from southern Africa, and many had a military background and/or a previous connection with the managing director or other employees of MK Airlines Limited. The company philosophy was to provide people from that geographic area with employment opportunities that would not otherwise exist.
The first B747 aircraft was added to the company's fleet in 1999. At the time of the accident, the company was operating six DC-8 and six B747 aircraft. Over the last several years, the company had increased its fleet by approximately one aircraft each year to accommodate the growing demand for cargo capacity, which was increasing by approximately 30 per cent each year. At the time of the accident, the company employed about 450 people. However, it was reported by several flight crew members that there were crew shortages, especially on the B747. These shortages were due to company expansion, training demands, and crew retention issues (see Section 1.17.1.5 of this report).
At the time of the accident, MK Airlines Limited held a Ghana Civil Aviation Authority (GCAA) AOC (No. 16/18/2003), issued 22 December 2003 and valid until 31 December 2004. The AOC was granted for the purpose of public transport, passengers, mail, cargo, and aerial work with B747 and DC-8 aircraft. The company had an extensive intercontinental route structure with many of the routes being long, triangular patterns to best serve the market demands.
1.17.1.2 Flight Operations Supervision and Oversight
The MK Airlines Limited OM described how the company would manage its flight operations. In anticipation of Ghanaian parliamentary passage of the 2002 GCARs (see Section 1.17.2.2 of this report), the OM also described some programs that were not fully developed or implemented, such as the flight operations quality assurance and flight safety program.
In accordance with the MK Airlines Limited OM, the Operations Manager was responsible for ensuring that an adequate level of flight operations supervision was maintained. For up to two years before the accident, the Operations Manager position was filled by the B747 fleet captain in an acting capacity. In addition to his duties as the acting Operations Manager, his responsibilities as the B747 fleet captain required him to do a considerable amount of line flying. His line flying enabled him to exercise adequate supervision of operations and allowed crews to express their concerns and raise issues directly to him. However, some of the operations management responsibilities were not being fully carried out. For example, the OM was not being kept up to date, the supervision of flight and duty limitations was lacking in some areas, and consistent adherence to SOPs was not being assured.
Many of the MK Airlines Limited flight crew had similar backgrounds. Employees of the company had a familial approach to business, which permeated all levels, including the line crews and supervisory/management personnel. This familial environment resulted in both positive and negative consequences for the company. For example, on the positive side, it provided a strong sense of loyalty and commitment to the success of the company. On the negative side, it created an environment where managers and supervisors could have had difficulty ensuring that their "friends" adhered to company procedures and policies. For example, some supervisory pilots had noted occurrences of non-adherence to SOPs when they were non-operating crew members. These were not brought to the attention of the crew, nor were they reported to the company because of this familial relationship and their status on the flight. It was noted that several supervisory pilots had flown the MKA1601/MKA1602 flights, where the maximum allowable duty hours were exceeded with no action being taken.
Due to the nature of the non-scheduled air cargo operations and the routes that were being flown, there were ongoing, significant challenges faced by management and crews. These included departure delays, schedule changes, aircraft unserviceabilities, inhospitable destinations, and crew flight-time limitations. In this context, both management and crews occasionally felt it was appropriate to deviate from company policy and procedures to accomplish the mission. This was done believing that the risk in doing so was manageable.
1.17.1.3 Flight Operations Quality and Flight Safety Program
The flight operations quality and flight safety program described in the OM was relatively new and had been somewhat slow in developing. The company wanted a program developed in house and one that reflected the company culture, rather than one that was "off the shelf." Company management reported that they had an open approach to flight safety and regarded it as being very important. Safety information was distributed quickly to crews through their computer-generated flight briefs. At the time of the accident, some components of the flight operations quality and flight safety program described in the MK Airlines Limited OM were not actually being carried out, or were only being partially carried out.
Although there was an occurrence investigation system and occurrence tracking software had been acquired, the database was still being developed. There was no confidential reporting system.
There was no flight operations quality assurance audit program in place for flight operations. However, the company had been assessing a number of different systems for the retrieval and analysis of FDR information.
1.17.1.4 Company Aircraft Training and Testing
MK Airlines Limited had been undergoing rapid expansion, especially in the B747 operation. The company had evolved from outsourcing almost all of its training to having a complete in house capability. At the time of the accident, the company was conducting approximately six B747 conversion courses each year. The company operated its own flight simulators, one B747 and one DC-8.
The company also had a comprehensive 40-hour flight crew indoctrination training program that was required for all newly hired flight crew.
The MK Airlines Limited OM, Part D - Training, Appendix A, contained a ground and simulator training course syllabus for the DC-8. There was no equivalent B747 ground and simulator course syllabus in the OM, Part D; however, there was a separate manual describing a ground training syllabus and a simulator training program.
The B747 classroom instruction was supplemented by practical application of the subject matter in the simulator. The simulator flight training syllabus was quite extensive; 14 four-hour sessions were provided with a proficiency check and instrument flight test conducted after these sessions.
A system of tracking the training required by different crew members and the filing of the different training records was in place; however, when TSB investigators requested training files of the occurrence crew, some documents were missing or were difficult to locate.
Training on new technology equipment and software, such as the BLT, was done by self-study and hands-on experience, using training material developed from the manufacturer's software manual. The information was distributed through notices to flight crews but had not been incorporated into the OM. There was no formal documentation to record an assessment of the individual's knowledge and competency using the equipment.
The company had a dedicated, experienced and knowledgeable group of supervisory pilots and flight engineers in its Training Department. One aspect stressed by the Training Department during training sessions and line checks was the strict adherence to SOPs at all times. Generally, most employees felt the training was adequate and the SOPs were appropriate for the operation. The operating philosophy among most flight crew was that SOPs were to be followed unless there were justifiable extenuating circumstances.
1.17.1.5 Crew Pressures
A significant number of MK Airlines Limited employees, particularly flight crew members, lived in southern Africa. Because of the company's business locations and route structure, employees were separated from their families for weeks at a time when on duty. With the political and social unrest in some of these areas, there was the potential for harm to come to their families when the employees were away. There were several examples cited where employees' families had experienced incidents of home invasion and/or personal attack. This was identified as a source of stress within the company.
In an effort to improve working conditions at MK Airlines Limited, the managing director had requested, some time before the accident, that the captain of MKA1602 submit a letter on behalf of the crews, listing some general concerns and suggestions of other flight crew. The letter was submitted shortly before the accident, and the company voluntarily supplied it to the TSB investigators. The letter indicated concern about recent increases in the number of pilots leaving the company and suggested that a new compensation package should be put in place to provide a more stable financial situation for flight crew members. The letter also indicated that there were not enough crews per aircraft. As well, it discussed the uncertainty of life for those living in southern Africa, indicating that the lengthy periods away from home increased stress and contributed to flight crew members looking at other employment options. The letter mentioned that inexperienced operational support personnel, combined with pressure from the Commercial Department, were causing crew scheduling difficulties.
Other company employees reported that there was a consistent shortage of B747 flight crew and they were required to spend lengthy periods away from home. To address a crew shortage in the past, the company had hired flight crew members from Argentina on contract to supplement its DC-8 operation.
1.17.1.6 Company Maintenance Practices
A review of the technical records indicated that all requirements of the approved maintenance program had been completed on the accident aircraft in accordance with the variation/tolerance approved by the GCAA.
1.17.2 Ghana Civil Aviation Authority
1.17.2.1 General
Since 1991, the GCAA has invested in personnel, training and equipment to help ensure conformity with ICAO standards and recommended practices (SARPs). In 1993, the GCAA requested assistance from Canada in the form of a safety review by TC. Following this review, a report was provided to the GCAA that identified areas for improvement, including a rewrite of the regulations and development of oversight guidance for inspectors. Several Canadians were contracted in 1995 to assist the GCAA in this effort. A new set of regulations came into effect in 1995.
1.17.2.2 Ghana Civil Aviation Regulations
The regulations that were in force at the time of the accident were the 1995 GCARs. In 1997, ICAO identified that these regulations needed to be updated.
ICAO conducted an audit of the GCAA in April 2001 and noted in its report that the GCAA's corrective action to the audit findings was generally satisfactory. The audit also determined that the newly drafted GCARs (referred to as the 2002 version) were in compliance with most of the SARPs, but had not yet been approved by the Ghanaian parliament.
An audit follow-up was conducted in May 2003 to determine the progress made on the corrective action. It was noted that some progress had been made, but the GCAA's regulatory efforts were being hampered by the ongoing delay in bringing the new regulations (2002 GCARs) into force. ICAO noted at that time that Ghana had five AOCs issued and there were two approved maintenance organizations. On 11 November 2004, the parliament of the Republic of Ghana approved the Civil Aviation Act, 2004, which brought into law the 2002 version of the regulations.
1.17.2.3 Ghana Civil Aviation Authority Flight Operations Oversight
The GCAA was asked to provide all records of all inspections, audits, and correspondence related to MK Airlines Limited for the two-year period before the accident at Halifax International Airport. The GCAA operations inspection file for MK Airlines Limited was reviewed to determine the actual frequency of inspections and to assess the handling of any safety deficiencies identified by the GCAA. It was concluded that the actual inspections conducted during the two years before the accident were below the minimum frequency of about 20 inspections indicated in the inspector's handbook. The inspection frequency of MK Airlines Limited had been decreased due to increased vigilance and the inspection of another registered Ghanaian operator.
A GCAA base inspection in September 2003 identified areas in the MK Airlines Limited OM that needed revision; however, many other areas were not identified as being out of date, not being followed, or in conflict with the regulations. An example of OM conflict with regulations was the practice of one pilot leaving the cockpit for prolonged periods during a flight. Although this was identified as a deficiency during a GCAA in-flight inspection, and formally recorded, the GCAA inspector was apparently unaware that the MK Airlines Limited OM, Section 8.3.10.1 (revised in 2001), provided for a flight crew member leaving his assigned station for an agreed purpose and period with the permission of the captain. It must be noted that OM, Section 8.3.10.1, contradicted OM, Section 7.4, which prohibited the pilot from leaving his duty station for a prolonged period.
Although the GCAA was asking for compliance with the 2002 GCARs, the company felt that the 1995 version was still in effect, and this might have led to different interpretations. The 1995 version of the GCARs stated that, if the aircraft is required to carry two pilots, the commander shall cause both the pilots to remain at the controls for only the take-off and landing. The GCAA reported that it was not aware of the rest, duty and flight time scheme in use by the company at the time of the accident, even though it had been in use and included in the company OM for two years.
1.17.2.4 Ghana Civil Aviation Authority Airworthiness Oversight
The 1995 GCARs indicated that periodic checks were to be carried out by the GCAA, and that these checks were to be done in conjunction with supervisory visits. These regulations did not specify the frequency or quantity of these checks or visits. The GCAA airworthiness inspectors had participated in the base inspection of MK Airlines Limited Landhurst facilities in September 2003. Additionally, it was reported that the GCAA carried out on-site visits for the annual renewal of each aircraft's Certificate of Airworthiness. During these visits, the GCAA would carry out an inspection that focused on examining the aircraft and reviewing the applicable technical documents. With a fleet of 12 aircraft, the GCAA would be at MK Airlines Limited facilities at least 12 times per year to carry out inspections.
Although some discrepancies were noted during the airworthiness review of MK Airlines Limited, overall, it appeared that the GCAA was providing an adequate level of airworthiness oversight. In a letter from the GCAA to MK Airlines Limited after an airworthiness audit, it was noted that amendments that had been incorporated in the maintenance control manual and the minimum equipment list had not been referred to the authority for prior approval. The GCAA did not receive a corrective action plan promised by MK Airlines Limited from the base inspection in September 2003.
1.17.3 Transport Canada
TC's Foreign Inspection Division conducted a base inspection of MK Airlines Limited operations in the United Kingdom between 15 August and 26 August 2002. The closing paragraph of the base inspection report stated that the company would be issued a Canadian Foreign Air Operators Certificate upon receipt of an acceptable corrective action plan that addressed the findings of the inspection. MK Airlines Limited submitted a corrective action plan in October 2002. On 20 December 2002, TC's Foreign Inspection Division granted MK Airlines Limited Canadian Foreign Air Operators Certificate F 10326. The Division had some concerns about issuing the certificate because of MK Airlines Limited accident history (see Section 1.18.6 of this report). However, the Division was impressed by MK Airlines Limited management, the timeliness and content of the corrective action plan, and the quality of feedback from the United Kingdom Civil Aviation Authority (CAA). Contributing to the confidence of the decision was the FAA's assessment that the GCAA was a Category 1 regulatory authority.
1.17.4 United States Federal Aviation Administration
The FAA established the International Aviation Safety Assessments (IASA) program in August 1992 to assess the ability of foreign civil aviation authorities to ensure compliance with ICAO's SARPs. There are two IASA safety ratings with regard to the SARPs: does comply (Category 1) and does not comply (Category 2). Specifically, the FAA determines whether a foreign civil aviation authority has an adequate infrastructure for international aviation safety oversight as defined by ICAO standards.
The basic elements that the FAA considers necessary include the following:
- laws enabling the appropriate government office to adopt regulations necessary to meet the minimum requirements of ICAO;
- current regulations that meet those requirements;
- procedures to carry out the regulatory requirements;
- air carrier certification, routine inspection, and surveillance programs; and
- organizational and personnel resources to implement and enforce the above.
In 1996, the FAA assessed the GCAA as having a Category 1 safety rating.
On 02 June 2003, the FAA granted MK Airlines Limited authority to operate in the United States by issuing Operations Specification ZM0F869F. As part of the FAA's oversight, periodic ramp inspections were conducted on MK Airlines Limited aircraft. In July 2004, MK Airlines Limited was placed on a special emphasis list. This list is issued semi-annually to identify foreign air carriers that are to be watched. The list also includes countries with a Category 1 Civil Aviation Authority, where the FAA has concerns. In September 2004, a ramp inspection of an MK Airlines Limited aircraft resulted in a decision to increase surveillance of the company's operation. A ramp inspection of an MK Airlines Limited DC-8 in the United States following the accident in Halifax identified several deficiencies, and on 29 October 2004, the FAA informed the company that its Operations Specification was cancelled; no specific reason was stated.
In December 2004, the FAA conducted a reassessment of the GCAA and, on 30 April 2005, it announced publicly that Ghana had failed to comply with ICAO standards. As a result, Ghana's safety rating was lowered to Category 2.
1.17.5 United Kingdom Civil Aviation Authority
Within the United Kingdom, the Department for Transport will issue a permit to a foreign-registered airline to operate into the United Kingdom if the airline has all the relevant approvals from its regulating authority. Where the Department has reason to believe that an airline or aircraft might not comply with international standards, it can arrange for that airline's aircraft to be inspected by the CAA. Where the CAA finds a matter requiring attention, it will be raised with the aircraft crew, airline, and/or foreign authority as appropriate. The Department for Transport relies on the country of registry to carry out effective and ongoing oversight of the company. The Department had issued permits to MK Airlines Limited, and the United Kingdom CAA had conducted a number of ramp inspections on MK Airlines Limited before the accident, without any significant findings.
1.18 Other Relevant Information
1.18.1 Boeing Laptop Tool
1.18.1.1 Introduction
At the time of the accident, MK Airlines Limited was using the Boeing Laptop Tool (BLT) for determining performance calculations. The BLT is a Microsoft Windows®-based software application used to calculate take-off performance data, landing performance data, and weight and balance information (see Figure 2). The performance data in the software are a digitized form of the approved B747 AFM.
The weight and balance data were supplied by and built into the software by MK Airlines Limited, and Boeing provided training to the MK Airlines Limited software administrator. The MK Airlines Limited BLT software administrator was responsible for setting up the weight and balance page for each specific aircraft and for supplying the airport database for the BLT. Boeing did not approve or review the work that the company administrator had done to the BLT weight and balance page. The company administrator had the option to lock out the weight and balance page in the BLT to prevent crews from using it; however, MK Airlines Limited decided not to lock out the weight and balance page in order to leave the page as a cross-check against the loadmaster's manual calculations. MK Airlines Limited had also received a current Boeing Administrator's Guide, with comprehensive instructions and the latest revisions to the software.
The software version in effect at the time of the accident was version 2.69r, effective 24 May 2004. Each B747 in MK Airlines Limited's fleet had been equipped with a laptop computer with a touch screen and printer stored in the upper deck. The BLT software installed on each laptop was aircraft-specific because of the differences in engines and weight and balance among aircraft.
The weight and balance feature of the BLT software allowed a user to perform basic weight and balance functions, including the calculation of the stabilizer trim setting for take-off. This software feature was an option that MK Airlines Limited had activated.
The weight and balance feature was accessed via a dedicated button on the main input dialogue screen, which would bring up a weight and balance summary page. The user could enter passenger weights, cargo zone weights, and fuel for the flight. When that information was entered, the take-off and landing weight, based on those inputs, was updated at the bottom of the summary page. Once updated, the estimated take-off weight would be passed back to the planned weight field on the main input dialogue screen and would automatically overwrite any entry in the planned weight field, without any notification to the user.
1.18.1.2 MK Airlines Limited Crew Training on Boeing Laptop Tool
When the MK Airlines Limited beta versionFootnote 19 of the BLT was ready, the Information Technology Department and the B747 Training Department began in-house testing, comparing the AFM performance section as a cross-check of the BLT using different samples of airports, altitudes, and temperatures. Differences were noted and corrected in conjunction with Boeing. The BLT was then given to the B747 Training Department instructors to begin training crews in its use. Information on the BLT was distributed to flight crews in the form of newsletters and notices to flight crews.
On 09 February 2004, the MK Airlines Limited B747 chief training pilot issued a Notice to Flight Crew to the B747 flight crew (including loadmasters) on the subject of the BLT. It stated the following:
Please find attached the Performance section and relevant QRH pages. Please take the time to study these for when the BLT program is put onto the onboard computers. The BLT will eventually replace the Airport Analysis Charts.Footnote 20
This Notice to Flight Crew had a detailed 46-page manual attached on the use of the BLT to calculate performance data, which was issued as an amendment to the company OM, Part B, for the B747-200 series, Section 4, Performance. The self-study training material was to be read by the pilots, and they were encouraged to practise using the laptop on board each aircraft. If the pilots had questions or comments about the BLT, they were to be sent to the company. Line training captains conducting line checks provided some training, and some crews received BLT training during their regular recurrent aircraft training at Landhurst.
Most of the MK Airlines Limited flight crew members did not receive any formal training on the BLT, and there was no method to evaluate and record if individuals had become competent using the BLT by the end of the self-study training period. Company Training Department and management personnel were aware that some pilots were not comfortable using personal computers. No additional general computer training was offered to the flight crews. However, according to the management of MK Airlines Limited, none was ever requested.
The 46-page BLT manual issued 09 February 2004 had two references to a BLT feature regarding the planned weight dialogue box on the performance page. Whatever weight appeared in the dialogue box would be overwritten automatically with the estimated take-off weight from the weight and balance page, when the user moved from the weight and balance page to the performance page. On 29 March 2004, MK Airlines Limited issued a second Notice to Flight Crew for the B747 fleet, informing the crews that the BLT software had been installed on all aircraft computers and was approved for calculating performance data.
This two-page Notice to Flight Crew asked that the crews use the procedure as written to complete take-off data cards. The first page was an instruction to pilots, while the second page was an instruction to loadmasters. It stated in the loadmaster instructions that, "when closing the weight and balance page, the take-off weight as listed in the weight and balance page will now appear in the planned take-off weight block." There was no mention of this feature in the instructions to pilots.
This Notice to Flight Crew also requested that the flight crew members take time to read the BLT manual. It could not be determined if the occurrence flight crew read the BLT manual issued in February, or the simplified instructions issued in March. Reports from other MK Airlines Limited flight crews indicated that the operating captain was not comfortable using the BLT, while the first officer had been observed using it.
On 12 August 2004, MK Airlines Limited issued a Notice to Flight Crew, which stated the following:
Airport (runway) analysis charts will be removed from all aircraft libraries in the near future. All performance calculations are to be performed using the BLT. In the unlikely event that no BLT computers are working then please revert to Volume 2 for the calculations and make sure a MAX THRUST Take Off Data Card is used.
1.18.1.3 Performance Data from the Boeing Laptop Tool
When the BLT software was opened, the introduction page presented the user with the option of two engine ratings for calculating take-off performance data: maximum take-off power using JT9D-7Q engine performance, identified by the aircraft registration (9G-MKJ), or de-rated power/rating II (RTG II) using the JT9D-7 dry engine certified performance, identified by RTG II.
Once the screen of the appropriate power rating is selected, the user inputs the airport and atmospheric data. The user then selects the "calculate" button and the BLT will indicate the maximum take-off weight for that runway and the EPR setting for maximum thrust for that power rating. The maximum thrust take-off performance data are displayed on the upper right of the screen, and the reduced thrust take-off performance data are displayed in the lower right side of the screen. The performance data on the right of the screen also include the aircraft weight on which the data were based. The user then transfers the appropriate data to a take-off data card (see Figure 3).
1.18.1.4 Maximum Allowable Take-off Weight at Halifax
Based on the atmospheric conditions at Halifax International Airport at the time of the accident and for a take-off on Runway 24, the BLT would have indicated that the maximum weight for a maximum thrust (JT9D-7Q engine) take-off would be 355 230 kg, and the maximum weight for a RTG II take-off would be 321 580 kg. The maximum weight for a reduced thrust take-off using the JT9D-7Q engine would be 346 513 kg, and the maximum weight for a reduced thrust take off using RTG II would be 315 058 kg.
1.18.1.5 Boeing Laptop Tool Take-off Performance Data at Halifax
The BLT take-off performance page would have indicated that, for a take-off weight of 350 698 kg (the weight taken from the mass and balance sheet left behind by the flight crew), using maximum thrust, the EPR setting would have been 1.60 and the take-off speeds, respectively, would have been: V1 (take-off decision speed)=149 knots, Vr (rotation speed)=161 knots, and V2 (take-off safety speed)=171 knots. At that weight, the BLT would not have provided reduced thrust performance data, including an EPR setting.
The BLT take-off performance page would have indicated that, for a take-off weight of 353 800 kg (the estimated actual weight), using maximum thrust, the EPR setting was 1.60 and the take-off speeds, respectively, would have been: V1=150 knots, Vr=162 knots, and V2=172 knots. At that weight, the BLT would not have provided reduced thrust performance data, including an EPR setting. The AFM provided comparable values.
If the RTG II option had been selected, any weight input into the planned weight box greater than 321 580 kg would have given the following warning: "Planned weight exceeds max allowable take-off weight of 321 580 kg."
An EPR setting of 1.33 could have been obtained using the BLT and RTG II, reduced thrust with a minimum weight of 285 000 kg. At that weight, the take-off speeds, respectively, would have been: V1=137 knots, Vr=145 knots, and V2=151 knots.
1.18.1.6 Boeing Laptop Tool Take-off Performance Data at Bradley
Using the atmospheric conditions at the time of take-off on Runway 06 at Bradley International Airport, the BLT take-off performance page would have indicated that, for a take-off weight of 239 783 kg, using RTG II, reduced thrust, the EPR setting would have been 1.30 and the take-off speeds, respectively, would have been: V1=128 knots, Vr=128 knots, and V2=137 knots.
1.18.1.7 Boeing Laptop Tool Take-off Performance Data at Halifax Using Bradley Weight
Using the atmospheric conditions at the time of take-off on Runway 24 at Halifax International Airport and a take-off weight of 239 783 kg, the BLT take-off performance page (see Figure 6) would have indicated the following:
| Engine | Thrust | EPR | V1 | Vr | V2 |
|---|---|---|---|---|---|
| JT9D-7Q | Maximum | 1.60 | 130 | 130 | 145 |
| JT9D-7Q | Reduced | 1.40 | 130 | 130 | 137 |
| JT9D-7 Dry | Maximum | 1.43 | 120 | 124 | 138 |
| JT9D-7 Dry | Reduced | 1.30 | 123 | 129 | 137 |
1.18.1.8 Landing Performance Data at Halifax
The aircraft's landing weight at Halifax International Airport was approximately 227 000 kg. For the atmospheric conditions at the time of landing on Runway 24, the BLT indicated that the aircraft would require a landing reference speed (Vref)Footnote 21 of 133 knots. In accordance with MK Airlines Limited normal flap extension schedule, the airspeed bugs would be set at the following:
| Bug Type | Plastic | Plastic | Plastic | Plastic | Command | 2 Plastic Vref* |
|---|---|---|---|---|---|---|
| Location on airspeed indicator (KIAS) | 213 | 193 | 173 | 153 | Target speed | 133 |
| Flap setting | 0 | 1 | 5 | 10 | N/A | 30 |
* the speed will vary with the landing flap selected
1.18.1.9 Regulatory Approval of Laptop Performance Systems
The 2002 GCARs, Part 9.3.1.13, require that AOC holders have a performance planning manual that contains adequate information to accurately calculate the aircraft performance in all normal phases of operation. The document that was approved by the GCAA was Volume 2 of the B747 AFM. In 2000, MK Airlines Limited elected to use runway analysis charts that were created using Boeing's STAS (Standard Take-off Analysis Software). In 2004, MK Airlines Limited introduced the BLT as the method of determining aircraft take-off performance.
The GCAA did not have any specific regulations or standards with respect to the use of portable or installed electronic flight bag (EFB) aircraft computing devices. The FAA had published an Advisory Circular (AC 120-76A) that set forth an acceptable means for United States operators to obtain certification and approval for the operational use of EFBs. The Joint Aviation Authority used similar guidance material for the approval of EFBs in its member countries and had issued Temporary Guidance Leaflet No. 36: Approval of Electronic Flight Bags (EFBs). MK Airlines Limited had this advisory and guidance material when the BLT and the Jeppesen electronic approach and aerodrome charts (JeppView®) were introduced into the MK Airlines Limited Flight Operations Department. In accordance with the advisory and guidance material above, the BLT and JeppView® were considered Class I and Class II Type B EFBs, respectively.
Also, in accordance with this guidance material, Type B applications did not require design approval, but did require principal inspector approval. These documents stated that, before an operator introduced and used EFBs in the cockpit, regulatory operational approval was required. This requirement included regulatory approval of all operating procedures, pertinent training modules, checklists, OMs, training manuals, maintenance programs, minimum equipment lists, other pertinent documents, and reporting procedures.
The guidance material also stated that a six-month operational evaluation period, using both the EFB system and paper copies, was to be carried out before final approval by the regulator would be considered. MK Airlines Limited did conduct a six-month operational evaluation period using both the BLT and runway analysis charts. The advisory and guidance material recommended that, before final approval is granted, the operator should provide evidence of human factors considerations of the EFB systems to the regulator. The guidance material stated the following:
The human factors/pilot interface characteristics of the EFB system should demonstrate that the EFB operating system and hosted application software meet the criteria for the appropriate intended function and do not provide false or hazardously misleading information. The system should be designed to minimize the occurrence and effects of flight crew error and maximize the identification and resolution of errors, and the effects of undetected errors in all EFB applications should be evaluated for each application. The assessment should also consider the effects of flight crew (procedural) errors determined by comments from the professional pilot community.
There was no GCAA record of operational approval of the BLT, nor was there a revision to the MK Airlines Limited OM, Part A or Part D, describing the BLT. MK Airlines Limited, however, did issue a number of notices to flight crews, providing instructions on the BLT.
1.18.2 Performance Data References
1.18.2.1 Data Cards
MK Airlines Limited has two styles of take off data card, one for maximum thrust take-offs, printed on white paper (see Figure 3), and one for reduced thrust take-offs, printed on yellow paper. The take-off data card includes ATIS information and performance information. The flight crew were required to transcribe the performance data from the BLT onto the take-off data card.
The BLT had an option of printing a standard Boeing "T-card" containing the relevant take-off performance data, which could be used as a take-off data card. MKAirlines Limited management had several meetings to discuss using the Boeing T-card (seeFigure4) as opposed to the standard company take-off data card. The final decision, strongly favoured by the Training Department, was to stay with the company take-off data cards. One point of discussion was the possibility of an error in transcribing the BLT data to the company data card. The Information Technology Department offered to provide pre-printed forms in the style of the MK Airlines Limited take-off data card to have the BLT print the data onto the form; however, this suggestion was rejected.
1.18.2.2 Instrument Bugs
The ASI on both pilot panels had six white plastic indicators (bugs) on the outside of the instrument that could be positioned at various locations of the pilot's choice. The ASI also had an internal bug called the "command airspeed bug" that was set with the auto throttle speed selector knob on the pilot's lightshield panel. The command airspeed bug is set at V2 for take off (see Figure 5), and during an approach, it is used to indicate the current target airspeed.

To remind the pilots of their target EPR settings, a moveable pointer bug is pre-set on each of the four EPR indicators on the pilots' centre instrument panel (seeFigure5). The indicators have two modes, manual and automatic. In manual mode, the knob is pulled out and an Mflag replaces the left digit in the upper window. The bug and upper digital readout respond to the rotation of the knob. In automatic mode, the knob is in, the Mflag is out of view, and the bug and upper digital readout responds to the TAT/EPRL (true air temperature/engine pressure ratio limit) Footnote 22 mode selector. Climb EPR and go around EPR are taken from the MKAirlines Limited QRH and transcribed onto the take-off data card.
1.18.2.3 Gross Error Check
MK Airlines Limited had designed a procedure called a "gross error check." The gross error check was used as a means to double check the correct take-off speeds against the take-off performance data calculated from the BLT. The MK Airlines Limited procedure during the Pilots Panels - Flow Pattern stated, "The pilots must set the Vr and V2 bugs on the ASI with the speeds from the high altitude cruise chart (FL280-FL430). Take-off bugs should be set prior to commencing the flow pattern so it can be completed uninterrupted. (Volume 3, Part 1, page 3.20.24)." The following is an extract from that chart with various Vr/V2 speeds at different flap and thrust settings:
| Thrust | Flap | Vr/V2 | Vr/V2 |
|---|---|---|---|
| 350 tonnes | 240 tonnes | ||
| JT9D-7Q | Flap 10 | 167/179 | 131/151 |
| JT9D-7Q | Flap 20 | 160/172 | 131/151 |
| RTG II | Flap 10 | 171/172 | 129/145 |
| RTG II | Flap 20 | 165/171 | 124/137 |
Using Rating I, Flap 20, for 350 tonnes (closest to planned Halifax International Airport weight) would have given the crew a gross error value of 160 for Vr and 172 for V2. A comparison of these values to the BLT-generated numbers for 350 tonnes of Vr of 161 and V2 of 171 would have shown that these numbers were close enough to confirm their validity.
For a gross error check, the airspeed bugs would be set using the high altitude cruise chart to obtain Vr and V2. Bug 1 is set at 12 o'clock, the next bug on 100, and the next two bugs at the appropriate Vr and V2 positions, as derived from the high altitude cruise chart. For the occurrence flight, the bugs should have been set at 12 o'clock, 100, 160, and 172.
1.18.2.4 Load Planning Sheets
MK Airlines Limited had a company load planning sheet that was to be completed manually for every flight by the loadmasters. The loadmasters received training on how to complete these sheets and learned how to adjust loads to ensure that the aircraft weight and balance were maintained within limits. Some of the MK Airlines Limited loadmasters preferred to use an electronic version that had been developed for another operator and had been modified for the MK Airlines Limited B747 fleet. This electronic version was never officially approved by the company, but the company was aware that it had been in use for approximately 2½ years before the occurrence. The company had many internal discussions on the use and approval of the electronic load planning sheet, but had never officially approved its use.
1.18.3 MK Airlines Limited Operations Manual
The OM was a mixture of information from the Joint Aviation Requirements (JARs) and the AFM volumes, with cross reference to other documents. It was subdivided into four parts: Part A -General/Basics, Part B - Aeroplane Type Operating Procedures, Part C - Flight Guide (Airways and Airports), and Part D - Training. Part B was essentially the AFM tailored to fit the company SOPs. MK Airlines Limited has converted the DC-8 SOPs from the AFM to a Part B; however, the B747 SOPs did not have a Part B and, instead, a version of the AFM volumes was used. The SOPs for the B747 were contained in Volume 3, Part 1 of the AFM, which was the equivalent to a Part B. In October 1999, MK Airlines Limited Training Department issued a newsletter introducing Volume 3, Part 1. The newsletter indicated that at a later date Volume 3, Part 1 would become Part B, to bring the SOPs in line with the JARs. At the time of the accident, this had not been completed.
In February 2004, the company issued a Notice to Flight Crew with an amendment to the company OM, Part B, for the B747-200 series, Section 4, Performance. This 46-page document was a detailed manual on the use of the BLT for calculating performance data. Eight of the pages in this document had an effective date of 22 September 2003, with revision number Original; the remaining 38 pages had an effective date of April 2002,Footnote 23 with revision number 006. The OM was supplemented with notices to flight crews. Each notice was in effect until its published validity period expired, it was cancelled by management, six months had elapsed, or the manual was amended. There were several notices to flight crews in existence longer than six months that should have been, and had not been, incorporated into the OM. There were also cross references in the OM to notices to flight crews and vice versa. For example, in Volume 3, Part 1, Section 4, Performance, the only text stated, "See Notice to Flight Crew BLT Performance Handout," yet that Notice to Flight Crew stated that it was Part B of the OM.
In accordance with Section 9.3.1.2 of the GCARs, each AOC holder shall issue flight crew members an OM acceptable to the GCAA, and keep the OM current. The OM must contain the company's procedures and policies for the use and guidance of its personnel regarding the flight operations it conducts. Section 9.3.1.2 of the GCARs also stated that no person may provide for the use of its personnel in commercial air transport any OM or portion of this manual that has not been reviewed and found acceptable or approved for the AOC holder by the Authority.
In accordance with Part 0.2.1, Section 0, of the OM, whenever the company wanted to amend the document, a proposed amendment would be forwarded to the accountable director of MK Airlines Limited on an Amendment Proposal form. If the amendment was approved internally by the accountable director, it would then be sent out to all manual holders, including the GCAA. All manual holders were required to return a receipt that they had received and incorporated the revision into their manual. When the GCAA returned its receipt to MK Airlines Limited, the amendment was considered by the company to be officially approved by the GCAA.
1.18.4 Procedures for Completing and Verifying Performance Data
The following section describes the normal procedures that would have been required by the crew members during the approach, landing, turnaround, and take-off at Halifax International Airport. They are in accordance with company SOPs, manuals, and notices to flight crews that were in effect at the time of the accident.
During the flight from Bradley International Airport to Halifax International Airport, the loadmaster should have been expected to calculate a load plan for the next leg, Halifax to Zaragoza. The company procedure was to use the load planning worksheet; however, accepted company practice was for the loadmasters to use their personal laptop load planning software to calculate a load plan. The loadmaster should then enter the weight and balance information into the BLT weight and balance summary page. During the descent and approach into Halifax, the pilot not flying should have listened to the ATIS (information Victor) and copied the information onto the landing data card. The landing data card should then have been completed by the flight engineer with the proper landing weight and with a Vref of approximately 133 knots. The captain and first officer should have set the landing bugs on their ASIs.
Once the aircraft was shut down after landing, post-flight duties should have included gathering all the paperwork for the Bradley-to-Halifax flight and placing it into a trip envelope. In preparation for the Halifax-to-Zaragoza flight, the first officer should have taken the latest ATIS information and transcribed it to the take-off data card. The first officer should have then obtained the planned take-off weight from the flight plan (353 310 kg) and transcribed the weight (353) to a white take-off data card. A white card should have been used because maximum thrust was needed for that weight using Runway 24. The first officer should have then extracted the Vmcg (minimum control speed, ground) from the QRH and entered this value on the take-off data card.
The first officer should have then gone to the company laptop computer in the upper deck rest area and opened the BLT program (see Photo 7). Since the BLT defaulted to the previous information used, and the take-off at Bradley International Airport had been a RTG II reduced thrust take-off, that option (RTG II) should have been selected in the window. The first officer should have then used the drop-down menus to insert on the performance page the airport, runway, runway conditions, aircraft bleeds (always defaulted to OFF), anti-ice, and optimum flap. Since there were no aircraft defects and no applicable NOTAMs (notices to airmen) for Halifax, the first officer should have proceeded to the next step. Without a planned weight in the planned weight block, a maximum take-off weight of 321 580 kg should have been generated after "calculate" was selected. Since the maximum take-off weight calculated by the BLT in RTG II would have been less than the planned take-off weight, the first officer would have had to return to the BLT icon and select the maximum thrust (7Q rating).
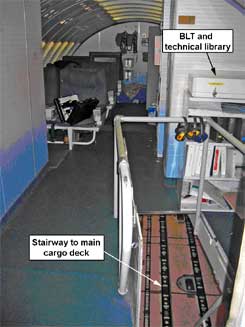
The first officer should then have verified that the ATIS information and data previously entered into the BLT were the same and selected "calculate" again. This should have given a maximum take-off weight of 355 230 kg, which was acceptable because the planned take-off weight was less than the maximum allowable weight for Runway 24. The first officer should then have entered the actual take-off weight of 353 (000 kg) in the planned weight block and selected "calculate" again.
The speeds for the maximum take-off thrust would appear on the right-hand side of the page. Reduced thrust (assumed temperature) speeds would not appear on the right-hand side of the page because the aircraft weight was close to the maximum. The first officer should have transcribed those speeds of V1=151 knots, Vr=162 knots, and V2=173 knots to the take-off data card and deleted the actual take-off weight from the planned weight block. Had the loadmaster entered the load information into the BLT, a stabilizer trim setting of 5 ¾ units would have been visible on the right-hand side of the page.
The first officer should then have given the take-off data card to the captain and the captain should have cross-checked all ATIS and runway conditions entered by the first officer and calculated the maximum take-off weight. The captain should then have entered 353 in the planned weight block and selected "calculate," then cross-checked the speeds entered on the take-off data card by the first officer. The take-off data card should have been taken to the cockpit and left on the throttle quadrant until the flow pattern checks were initiated.
Before starting the cockpit flow checks, the captain or first officer should have used the high altitude cruise data card to obtain the Vr/V2 speeds for the gross error check, and, for the occurrence take-off, set the bugs as follows: V1 bug at 100 knots, Vr bug at 160 knots, and V2 bug (command bug) at 172 knots. While the captain and first officer were conducting their flow pattern checks, the flight engineer should have been performing his pre-flight duties and should have cross-checked the fuel load distribution, individual fuel quantity indicators, and total fuel weight indicator against the load sheet. The flight engineer should have also set the computed gross weight in the total weight indicator on his instrument panel.
After completing the Before Start Checklist and just before completing the Start and Pushback Checklist, the captain would have signed the load sheet and the mass and balance sheet. He should have also verified that the take-off weight and the load distribution were within limits and transcribed the calculated stabilizer trim setting indicated on the mass and balance sheet to the take-off data card. In accordance with company SOPs, since the actual take-off weight would have been within 3000 kg of the estimated take-off weight, it would not have been necessary to rework the take-off speeds.
After, the set bug speeds and EPR setting should have been checked against the speeds on the take-off data card. Gross errors would have been obvious and corrections, if required, would have been made, and the bugs would have been set to the correct take-off (V) speeds and the EPR setting. The first officer should have called the rating (maximum or reduced thrust) being used and noted any surface condition changes since the completion of the take-off data card. A departure briefing should have been accomplished before the engine start and pushback, unless operational factors precluded it at that time.
During the taxi-out procedure, the first officer would have selected the flap lever to 20°, set the stabilizer trim for 5.8 units, and should have confirmed that the take-off data were checked and set. If the take-off data had been previously checked and set, then the captain was to reconfirm the runway in use and V2 when responding to the checklist. If the take-off data had not been previously set, or the data were amended, then all settings would have been called and set at this time.
During the take-off, the thrust levers should have been advanced to 1.10 EPR, engine indications checked stable and symmetrical, then advanced to approximately 1.20 EPR, and "MAX thrust"Footnote 24 called. The flight engineer should have then set maximum thrust of 1.60 EPR before reaching 80 knots. The pilot not flying should have called V1 at 151 knots and Vr at 162 knots. The pilot flying would have initiated a smooth continuous rotation at Vr to the rotation target attitude of approximately 12° pitch attitude. Shortly thereafter, the landing gear would have been retracted and the air conditioning packs selected ON, and the transition to departure and en route climb would have been made.
1.18.5 Rest, Duty and Flight Time Schemes
1.18.5.1 MK Airlines Limited Rest, Duty and Flight Time Schemes
As required by the 1995 GCARs, in force at the time of the accident, the company had established a rest, duty and flight time scheme in its OM. The 2002 version of the GCARs had been drafted but not yet passed into law. The GCAA had asked MK Airlines Limited to comply with the 2002 version but, in fact, the company was only obligated to follow the 1995 regulations.
The 1995 GCARs regarding rest, duty and flight time were much briefer than the 2002 regulations. The 2002 regulations regarding rest, duty and flight time were comprehensive and allowed for special flight duty schemes that could be approved by the GCAA. The MK Airlines Limited OM, Part A, Section 7, contained the rest, duty and flight time scheme, and in this section, it was stated that the rest, duty and flight time scheme was authorized by the authority and that all flights must be planned in accordance with the scheme.
Revision 003 to the MK Airlines Limited OM, Part A, Section 7, effective 11 February 2000, stated that the maximum allowable duty period for a heavy crew was 20 hours, with a maximum of 16 flight hours, conforming to both the 1995 and 2002 version of the GCARs. Revision 003 defined a heavy crew as two captains, two co-pilots and two flight engineers. However, Section 4.1, Crew Composition, of the OM defined a heavy crew as three pilots and two flight engineers, in contradiction to Section 7. The actual practice was to use three pilots, not four.
Revision 011 to the OM, amending the flight and duty time scheme, became effective on 23 September 2002 and was the scheme in effect at the time of the accident. In this revision, the maximum duty time for a heavy crew flying one to four sectors was increased to 24 hours, with a maximum of 18 flight hours. As well, the definition for a heavy crew was revised to include three pilots and two flight engineers. The company indicated that the reduction in pilots was to reflect consistency with Section 4.1 of the OM and the normal company practice. The amendment was sent to all manual holders, including the GCAA. The GCAA could not find any record of having received the amendment. MK Airlines Limited's own electronic records indicated that the GCAA had received the amendment.
1.18.5.2 Rest, Duty and Flight Time Schemes of Other Civil Aviation Authorities
ICAO Annex 6, Part 1, Attachment A, provides guidance on flight time and flight duty period limitations. It states that limitations are established for the sole purpose of reducing the probability of fatigue of flight crew members, which in turn might adversely affect the safety of the flight. It describes two types of fatigue: transient and cumulative. Transient (acuteFootnote 25) fatigue is experienced following a period of work, exertion or excitement and is normally dispelled by a single sufficient period of sleep. Cumulative fatigue might occur after delayed or incomplete recovery from transient fatigue or as the after-effect of too much work or over-exertion without sufficient opportunity for recuperation. Flight time and flight duty period limitations provide safeguards against both kinds of fatigue, because they limit flight time and duty time spent on the ground before a flight or at intermediate points during a series of flights.
The duty time limitations scheme in use by MK Airlines Limited at the time of the accident for a three-pilot augmented crew operating four sectors was 24 hours. For comparison purposes, the following summarizes, for selected jurisdictions, the flight and duty maximum time limitations for an augmented crew (three pilots), cargo operation, on the same itinerary and with similar on-board rest facilities to that of the accident aircraft:
- Canada - the maximum allowable duty period for an augmented crew, consisting of three pilots, would be 20 consecutive hours, in which case the maximum flight deck duty time for any flight crew member shall be 14 hours, and a maximum of three sectors.
- United States - no more than 18 duty hours for a three-pilot crew, and no more than 12 hours aloft are allowed.
- United Kingdom - the maximum allowable duty period for an augmented crew, consisting of three pilots, would be 18 hours.
- Italy - After the accident, an Italian-registered company was found to have an approved duty time limitation scheme with a maximum allowable duty period for an augmented crew, consisting of three pilots (in an aircraft equipped with an inertial navigation system), of 24 hours and a maximum of six sectors.
1.18.5.3 MKA1602 Crew Duty Time
The MKA1602 crew was scheduled for a 24.5-hour duty day.Footnote 26 MK Airlines Limited was in contravention of its OM by planning a flight to exceed 24 hours; similarly, the flight crew was in contravention by accepting a flight planned to exceed the maximum allowable duty period. At the time of the accident, the flight crew (captains, first officer, and flight engineers) had been on duty for almost 19 hours. However, due to the delays that had been experienced at Luxembourg-Findel Airport and Bradley International Airport, the crew would likely have been on duty for approximately 30 hours at their final destination of Luxembourg-Findel Airport, had the remaining flights continued uneventfully. Hotel and telephone records at Luxembourg indicated that some crew members might have been awake since early in the morning. According to the voyage reports, the loadmaster and ground engineer had been on duty for 45.5 hours.
The MK Airlines Limited OM stated, "all flights are planned in accordance with the limitations of the company's approved rest, duty and flight time schemes." Review of the planned duty periods for all the previous MKA1601/MKA1602 flights indicated that approximately 71 per cent of the flights had been planned in excess of 24 hours, averaging 24.37 hours. Company management personnel stated that they were unaware that this was occurring. The GCAA also had not detected these exceedences during its oversight of the company.
The MK Airlines Limited OM also stated, "flights may exceed the prescribed flight/duty limitations due to unforeseen circumstances" and "the company should also monitor these unplanned exceedences on a seasonal quarterly basis and not allow more than 25 per cent of the routes flown for that quarterly season to be exceeded, which will require a re-planning of crewing for that particular route/flight pattern." Review of the actual duty periods flown on the MKA1601/MKA1602 route indicated that they exceeded 24 hours 95 per cent of the time, averaging 26.85 hours. Company management was aware that exceedences were occurring. These exceedences were also not detected by the GCAA during its oversight of the company.
The MKA1601 captain wrote the following on the company voyage report:
According to our brief the duty period required to complete this flight is 24 hrs 30 min. In terms of Part A (7) the max duty period is 24 hrs. The crew were called out to operate starting this duty period at 1200Z only to finally depart at 1600Z. Can anything be done to correct the constant delays experienced in LUX for the Bradley run (re: clean pallets and crew callout when A/C is ready)?
1.18.5.4 Physiological Effects of Fatigue
Fatigue is a physiological state characterized by impaired performance and diminished alertness. Two causes of fatigue are inadequate quantity or quality of sleep and disruption of circadian rhythm. These can result from irregular work schedules, extended duty or altered work/rest schedules and have been identified as contributing factors in many industrial accidents.
Research suggests that it is not possible to store sleep. As a person remains awake, a sleep need develops, notwithstanding how well rested the individual was at the beginning of the wake cycle. Most people need between 7.5 to 8.5 hours of sleep per day. The need for sleep typically recurs after about 15 or 16 hours of being awake, even for someone who is well rested. A person who does not obtain required sleep will develop a sleep debt and will be subject to performance degradation.
Fatigue can lead to forgetting or ignoring normal checks and procedures, reversion to old habits and inaccurate recall of operational events. Fatigue can also reduce attention, the effects of which are that people overlook or misplace sequential task elements, become preoccupied with a single task and are less vigilant. When alertness is impaired, people might fix their focus on a minor problem (even when there was the risk of a major one), they might fail to anticipate danger and they might display automatic behaviour syndrome. Problem solving can also be affected, and flawed logic might culminate in the application of inappropriate actions.
1.18.5.5 Fatigue Management
Under the flight and duty time scheme in use by MK Airlines Limited, three pilots were required in a heavy crew working a maximum 24-hour duty period. The heavy crew would usually consist of one captain and two first officers, or two captains and one first officer. Only training captains who conduct supervised line flying for newly upgraded captains are right-seat qualified; therefore, on most flights, the first officer must occupy the right seat for all take-offs and landings. This results in a situation where there is a critical crew member, the one captain or first officer in the crew, who has to be in his or her respective seat for all landings and take offs. This also results in disrupted rest/sleep patterns for this individual.
The on-board rest facilities on the accident aircraft included a captain's cabin, two bunks, and first-class seats (see Photo 8). The operating captain and the first officer would have had the opportunity to sleep on board the aircraft while transiting from Luxembourg to Bradley. However, other MK Airlines Limited crews indicated that they rarely were able to sleep on the first leg of the MKA1601/MKA1602 route because of the time of day. They also stated that they began to feel the effects of fatigue during the stopover in Halifax and might obtain a nap in Halifax, if the turnaround time permitted. Feeling fatigued at this stage of the flight would be consistent with the expected lowest point of a crew member's circadian rhythm. In the case of the accident flight, which was delayed leaving Luxembourg, the circadian low point would have fallen somewhere between Bradley and Halifax. Other crews also indicated that they normally were able to get several hours of sleep while transiting between Halifax and Zaragoza.

Sleeping on board the aircraft, both in the air and on the ground, was a routine fatigue management practice at MK Airlines Limited. The MK Airlines Limited OM, Section 8.3.10.1, allowed any one flight crew member to leave his or her assigned station for an agreed purpose and period in level cruise with the permission of the captain. During one GCAA in-flight inspection, with a non-augmented crew operating, the first officer left for 1½ hours and the captain left for three hours to sleep during the course of a flight. The fact that crews would commonly sleep or take naps en route and during turnarounds was an indication that crews recognized that they were susceptible to fatigue and did their best to mitigate the risk.
The 2002 GCARs, in effect as of November 2004, require flight crew members to remain at the assigned duty station during all phases of flight unless absence is necessary for the performance of duties; for physiological needs, provided one qualified pilot remains at the controls at all times; or the crew member is taking a rest period and a qualified relief crew member replaces him or her at the duty station.
MK Airlines Limited ground engineers and loadmasters were not subject to any duty time restrictions because there were no company rules, labour laws or aviation regulations pertaining to duty time that applied to them. It was determined that there were times when they could spend up to seven days on board an aircraft. The MKA1601/MKA1602 ground engineer's duty for the month of September 2004 was reviewed, and records indicate that he had worked 24 of the 30 days, with 19 of those days on board an aircraft; the longest stretch was from 06 September 2004 to 13 September 2004. In addition, the ground engineer had some days where he was performing line maintenance duties at the maintenance facilities in Luxembourg and Johannesburg, South Africa. Individuals performing ground engineer and loadmaster tasks are regarded as important members of the crew who could easily contribute adversely to an accident through a fatigue-induced error.
1.18.6 Previous MK Airlines Limited Accidents and Incidents
The MKA1602 accident was the fourth major accident the airline had experienced since 1992. The three previous accidents occurred in Nigeria, and very little information was available with respect to the first two occurrences.
The Federal Republic of Nigeria, Ministry of Aviation, produced a Civil Aviation Accident Report (FMA/AIPB/389) for the company's third accident in Port Harcourt, with one fatality. A review of the report and information obtained from other sources indicated that the pilot flying was following a non-standard autopilot approach, tracking a localizer radial inbound and descending using vertical speed mode; MK Airlines Limited company policy was to not use the autopilot below 2000 feet agl. There were other indications of non-adherence to procedures, including the failure to make appropriate calls between the pilot flying and pilot not flying. A lack of situational awareness due to poor cockpit coordination was apparent, and there was a problem interpreting the visual references on the approach.
The company had also designated Port Harcourt as a Category B airport. According to the MK Airlines Limited OM, Part A, Section 8.1.2.5, a Category B airport is one that requires the captain to fly the approach when there are considerations such as non-standard approach aids and/or approach patterns, unusual local weather, unusual characteristics or performance limitations, other relevant considerations including obstructions, physical layout, lighting, etc. The first officer was flying the approach at the time of the accident.
Also of interest was an incident that occurred on 18 July 2002, when an MK Airlines Limited B747-200 had a take-off performance incident in Sapporo, Japan. The first officer completed the take-off data card using the runway analysis charts for the applicable runway. The captain checked the card and found it to be correct. The take-off weight, as indicated on the card, was written as 258 000 kg, rather than the correct weight of 358 000 kg. Gross error check speeds had also been set using 258 000 kg. The loadmaster presented the load sheet to the captain for checking and he signed it. The load sheet indicated 358 000 kg, but the difference in weight was not detected. The airspeeds and EPRs were set for 258 000 kg. During the early stages of the take-off roll, the flight crew noted that the aircraft was not accelerating normally, and the take off was rejected at approximately 30 to 40 knots. On review of the take-off data card, the error was detected and a new take-off data card was completed using the correct weight. The subsequent take-off was uneventful.
1.18.7 Managing the Risks of an Organization
Managing the Risks of Organizational Accidents by James ReasonFootnote 27 (Ashgate Publishing Limited, 1997) describes the challenges that companies face while trying to balance the priorities of production (flying) versus protection (safety) on a day-to-day basis, and particularly during a period of growth. As an airline expands and its level of production increases, the risks associated with production activities usually increase, requiring the organization to increase the level of protection. This protection comes in many forms, including the development of an adequate company infrastructure, such as logistics, training, facilities, equipment, and quality assurance and safety programs.
During MK Airlines Limited expansion, the management was actively working on improving the company's infrastructure; however, during this same period, there were examples of insufficient management staff, inadequate supervision, routine shortcuts, and procedural non adherences that were taken by employees and supervisors when it was necessary to meet operational demands. Four major accidents in the company history are strong indicators of inadequate protection.
The following is an excerpt from James Reason's book:
Despite frequent protestations to the contrary, the partnership between production and protection is rarely equal, and one of these processes will predominate, depending on the local circumstances. Since production creates the resources that make protection possible, its needs will generally have priority throughout most of an organization's lifetime. This is partly because those who manage the organization possess productive rather than protective skills, and partly because the information relating to production is direct, continuous and readily understood. By contrast, successful protection is indicated by the absence of negative outcomes. The associated information is indirect and discontinuous. The measures involved are hard to interpret and often misleading.
All rational managers accept the need for some degree of protection. Many are committed to the view that production and protection necessarily go hand-in-hand in the long term. It is in the short term that conflicts occur. Almost every day, line managers and supervisors have to choose whether to cut safety corners to meet deadlines or other operational demands. For the most part, such shortcuts bring no bad effects and so can become an habitual part of routine work practices. Unfortunately, this gradual reduction in the system's safety margins renders it increasingly vulnerable to particular combinations of accident-causing factors.
1.18.8 Take-off Accidents - Inadequate Performance
A review of large (above 5700 kg), turbine-powered aircraft accident and incident data has shown that there have been at least 12 major occurrences where take-off performance was significantly different from scheduled performance. Four of the aircraft involved were destroyed and there were 297 fatalities.
Several of these occurrences involved flight crews that attempted a take-off using incorrect performance data, and then did not recognize the inadequate take-off performance of the aircraft. There were other accidents where the take-off performance has been inadequate because of mechanical failures, incorrect aircraft configuration or incorrect instrument indications. These occurrences were not isolated to any particular aircraft type, commercial operation or geographic area.
Underlying most of these occurrences were one or both of the following safety issues:
- the failure or absence of procedural defences to detect an error in the take-off performance data; and
- the failure of the crews to recognize abnormal performance once the take-off had commenced.
The following are some representative accidents taken from the data:
- On 12 March 2003, a Boeing 747-412 suffered a tail strike on take-off in Auckland, New Zealand, and became airborne just above the stall speed (New Zealand Investigation 03 003). The aft pressure bulkhead was severely damaged, but the crew managed to land safely. The cause of the tail strike was a result of the flight crew entering a take-off weight 100 tonnes less than the actual weight into the flight management system, resulting in low take-off speeds being generated. There was no crew cross-checking of the speeds.
- On 11 March 2003, a Boeing 747-300 in Johannesburg had a tail strike on take-off (NTSB report DCA03WA031 refers). The flight engineer had entered the zero fuel weight of 203 580 kg instead of the take-off weight of 324 456 kg into the hand-held performance computer, and then transferred the incorrect computed take-off speeds onto the take-off cards.
- On 14 June 2002, an Airbus A330 had a tail strike on take-off in Frankfurt, Germany, because incorrect take-off data were entered into the flight management system (TSB report A02F0069 refers). The tail strike was undetected by the flight crew, but they were notified by air traffic services during the climb-out. The aircraft sustained substantial structural damage to the underside of the tail.
- On 28 December 2001, a B747-200 cargo aircraft had a tail strike on take-off in Anchorage, Alaska, and sustained substantial damage (NTSB report ANC02LA008 refers). The crew did not account for the weight of the additional fuel (about 45 360 kg) taken on board in Anchorage, and inadvertently used the same performance cards that were used for the previous landing. The crew members were unaware that the tail had struck the runway until after arrival at their destination.
- On 13 January 1982, a Boeing 737-222 was on a scheduled flight from Washington, DC, to Fort Lauderdale, Florida. During take-off, the EPRs were set for 2.04, and on the take-off run, anomalous engine instrument readings were noted; the captain elected to continue the take-off. Approximately 2000 feet and 15 seconds past the normal take-off point, the aircraft became airborne. The aircraft initially climbed, but failed to accelerate. The stall warning stick shaker activated shortly after take-off and continued until the aircraft settled, hit the 14th Street Bridge and several vehicles, then plunged into the frozen Potomac River. The investigation revealed that the engine inlet pressure probes became blocked with ice, resulting in high EPR indications. Of the 79 persons on board, 74 perished, and there were four ground fatalities.
From at least as far back as 1972, there have been safety recommendations and initiatives to ensure that crews have a reliable on-board method of detecting abnormal take-off performance, particularly in situations where performance is less than required or expected. Unfortunately, there is still not a reliable in-cockpit system available for crews to detect and react to abnormal take-off performance in a timely manner.
2.0 Analysis
2.1 Introduction
In this accident, the flight crew's take-off performance calculations resulted in an error that remained undetected until the aircraft reached a point where the crew's response was too late to avert the accident. The analysis will focus on those events, conditions and/or underlying factors that were causal or contributing to the accident. Areas where there were additional and undesirable risks to the system will also be discussed.
2.2 Halifax International Airport - Accident-Related Issues
2.2.1 Electrical Power Supply
The Halifax International Airport fire hall electrical system was configured to provide two separate sources of emergency power (generators) in case of a power failure. However, one failed to provide power because the main circuit breaker had tripped, preventing some of the associated electrical systems in the fire hall from operating as designed. The firefighters, therefore, had to respond in very dim light conditions during their initial response. Aside from creating some confusion, there was an increased risk of injury to the firefighters and the potential for a delayed response. The earlier system of self-contained battery-operated lights, which had been removed following the installation of an emergency power generator, would have provided immediate illumination of the bunk room and vehicle bay.
2.2.2 Grid Map
Grid coordinates were not used to direct the Halifax International Airport ARFF unit or any other responders at any time during the response to this accident. Because the weather conditions and visibility were good, the first responders were able to easily locate the accident site. There was, however, some confusion with other responding units as to the exact location of the accident site.
The air traffic controllers regularly assist the airport firefighters with grid run training, yet the controllers are not required to use grid coordinates when directing ARFF to an accident site. The use of grid coordinates during an emergency would prevent confusion and could reduce critical response time.
2.2.3 Persons and Dangerous Goods On-Board Information
Air traffic controllers were initially unsuccessful in their attempts to get information on the number of persons and dangerous goods on board the aircraft. One hour after the accident, MK Airlines Limited provided information regarding the number of persons on board and indicated that no dangerous goods were loaded in Halifax. Since all the dangerous goods carried on MKA1602 had been loaded at the previous stop, Bradley International Airport, no one in Halifax had any information regarding the dangerous goods. It was not until 10 hours after the accident that ARFF received a listing of the dangerous goods that had been loaded at Bradley. A lack of timely information concerning dangerous goods could have jeopardized the safety of the ARFF personnel and other responding personnel. In the case of a survivable aircraft accident, knowledge of the number of occupants could be critical to successful rescue efforts.
2.2.4 Runway Slope
The slope for Runway 24 was published incorrectly in the Canada Flight Supplement and the Canada Air Pilot as 0.17 per cent down. Slope information is a consideration when calculating aircraft take-off and landing performance. If published slope information is incorrect, aircraft performance data could be incorrectly calculated. It could not be determined how the 0.17 per cent value was determined. The incorrectly published runway slope was not a factor in the take-off performance of MKA1602.
2.2.5 Earthen Berm
NAV CANADA obtained the required approval from TC for construction of the berm at the end of Runway 24. As part of the approval process, the berm was evaluated for obstacle clearance in accordance with TC's TP 312. The berm was not considered an obstacle by definition because it did not penetrate the plane of the obstacle-free zone. Obstacles are only considered hazards if they will affect the climb profile of an aircraft that has met its certification criteria.
There are no specific standards or recommended practices regarding the construction and risk assessment of berms or similar immovable objects in the runway overrun/undershoot areas, except in the case where they constitute an obstacle or they impinge on an established RESA. TC's guidance considers a RESA only to be a recommended practice, yet ICAO considers it to be required standard. There was no RESA published for Runway 06 or Runway 24 at Halifax International Airport. The ILS localizer berms were both located beyond the minimum recommended RESA distances.
2.2.6 Radio Communications
The various communications devices that emergency response personnel tried to use for communication at the crash site and between the crash site and other areas did not provide reliable communications. These communication difficulties complicated coordination during the response, and in other circumstances, could have hampered a rescue attempt or quick evacuation of an injured person.
2.3 Weight and Balance
The aircraft operating empty weight did not include crew and operational equipment carried on board the aircraft. Therefore, every time a mass and balance sheet was completed for the occurrence aircraft, the crew would not be aware that the aircraft was actually 1120 kg heavier than calculated. In some cases, this could have put the aircraft over its maximum allowable take-off or landing weight.
The ground handling agent at Halifax International Airport did not have the facilities to weigh built-up pallets that were provided by others, and because the manifest provided by the freight forwarder was believed to be accurate, an incorrect cargo manifest spreadsheet was created. The unverified cargo weight at Halifax allowed the extra weight of the wooden skids to go unaccounted for and could have also contributed to an overweight condition. As well, the failure to detect an error in the load weight could result in adverse aircraft performance and, potentially, an accident. In this case, the aircraft was still within the allowable weight and balance limits for the take-off at Halifax.
MK Airlines Limited was aware that some loadmasters had been using an unapproved electronic version of the load planning sheet for approximately 2½ years before the accident. The company did not prevent the loadmasters from using this software, even though it had not been verified that the software and database were free from errors. Therefore, there was a risk that an aircraft could have been improperly loaded without the crew's knowledge. This was an example of the company not exercising adequate oversight to correct a known adaptation of company procedures by flight crews.
2.4 MK Airlines Limited
2.4.1 MK Airlines Limited Expansion
MK Airlines Limited had grown significantly during its relatively short history. The company's commercial success and subsequent expansion increased demands on its infrastructure. The addition of the B747 aircraft added significantly to the Training Department's challenge of meeting the demand for qualified flight crews. At the same time, flight crew turnover was increasing as individuals found more attractive employment elsewhere. Also, the company's policy of recruiting from southern Africa limited the pool of new potential crew members. All these factors contributed to a shortage of flight crew required to meet the flying or production demand. This shortage of flight crews increased the potential for increased fatigue and stress among the personnel.
2.4.2 Rest, Duty and Flight Time
Although the OM stated that flights would not be planned beyond 24 hours, the Crewing Department at MK Airlines Limited routinely scheduled flights in excess of that limit. There was no effective program in place to monitor how frequently these planning exceedences occurred, nor was there a program to detect and monitor exceedences beyond the planned duty days. In the absence of adequate company corrective action regarding these exceedences, crews developed risk mitigation strategies that included napping in flight and while on the ground to accommodate the longer scheduled duty days. This routine non-adherence to the OM contributed to an environment where some employees and company management felt that it was acceptable to deviate from company policy and/or procedures when it was considered necessary to complete a flight or a series of flights.
There is a reasonable limit to the time a flight crew can remain on duty before acute fatigue begins to induce unacceptable human performance deficiencies. This is regardless of the crew composition and the adequacy of the rest facilities on board the aircraft. Examination of the occurrence crew's work/rest/sleep and duty history indicated that the operating crew would have been at their lowest levels of performance because of fatigue at, or shortly after, their arrival in Halifax. This state of fatigue would have made them susceptible to taking procedural shortcuts and reduced their situational awareness. This period of low performance would have been present when the take-off performance data were calculated, the before-flight SOPs were not followed, and the inadequate take-off performance was not recognized.
The company's flight and duty scheme allowed flights to be scheduled up to 24 hours with only three pilots required. This meant that there would be either only one captain or one first officer in the crew. Because most crew members were only qualified to occupy either the left or right pilot seat, two of the assigned pilots would have to be present for every take-off, departure, arrival, and landing for the entire route. This resulted in the lone captain or first officer being subjected to a disproportionate amount of flight deck duty and, therefore, more vulnerability to fatigue. For this series of flights, the first officer was the critical crew member in this respect.
The first officer had checked out of the hotel in Luxembourg at 0925 on October 13, but it is known that he was awakened earlier than 0848, perhaps as early as 0630 or 0700. It is probable that he was not in the cockpit for a few hours on the first flight, but it is unlikely that he would have slept or had a good rest because of circadian rhythm effects. As other MK Airlines Limited flight crews indicated, it was not easy to get rest on the flight to Bradley International Airport because of the time of day. The flight from Bradley to Halifax took 1 hour 9 minutes, and the first officer would have been in the cockpit during this flight. Therefore, he would likely have been the most fatigued pilot.
The aircraft was on the ground at Halifax International Airport for 1 hour 42 minutes. Twice during this time, it was noted by ground personnel that the first officer was not in the cockpit, and it was common for flight crew to nap or rest if the turnaround time was long enough. It is likely that he took a nap between the time the take-off performance data were calculated and when he was required to be back in the cockpit to prepare for the departure.
If the first officer had been sleeping while the aircraft was on the ground in Halifax, he would have been susceptible to sleep inertia for 10 to 15 minutes after waking up. As a result, he would have been less alert than usual when he first entered the cockpit, the period when the performance data would have been set from the take-off data card information. In addition, if the captain had carried out some of the first officer's pre-flight duties to allow him to sleep, this would have further removed the first officer from the cockpit environment and decreased his situational awareness.
At the time of the occurrence, MK Airlines Limited rest, duty and flight time scheme was one of the least restrictive among ICAO signatory states. The company's increase of the maximum flight duty time for a heavy crew from 20 to 24 hours also increased the potential for fatigue.
2.4.3 MK Airlines Limited Company Risk Management
MK Airlines Limited flight crews often flew into airports with poor facilities, experienced frequent delays and equipment malfunctions, and were scheduled for lengthy duty periods, often with limited on-board rest facilities. Many of the crews, supervisors and managers were accustomed to difficulty, hardship, and overcoming challenges. The growth and success of the company also had a great deal to do with the familial environment. Unfortunately, some of the strengths that this environment brought also generated weaknesses. These weaknesses were in the form of accepting shortcuts and deviations from procedures when it was deemed appropriate. An example of this was the acceptance of non-adherence to company direction and procedures by both management and line personnel.
Acceptance of non-adherence to company direction and procedures by managers was often tacitly accepted in the belief that it did not generate an unacceptable risk. Although three previous accidents should have been significant risk indicators for the company, there was an overall acceptance that the commercial growth (production) was being managed adequately in terms of risk (protection).
Several of the operating norms that were identified were similar in nature to those in James Reason's book. For example, shortcuts (non-adherence to procedures) had become a habitual part of routine work practices. Reason states, "This gradual reduction in the systems safety margins renders it [the company] increasingly vulnerable to particular combinations of accident-causing factors."
SOPs are established for the safe and efficient operation of an aircraft and are considered to be a critical defence toward ensuring consistent and safe operational outcomes. For this crew, the SOPs were critical for ensuring that the take-off performance data were calculated correctly, and any potential errors in that data were detected before the take-off was attempted. Non-adherence to SOPs, as was shown in this accident, can have catastrophic consequences.
2.4.4 Company Oversight of Operations
The company OM, which had been approved by the GCAA, contained a description of how the company was to conduct flight operations safely and within the regulations. Many areas of the OM were incomplete, out of date or inadequate. Moreover, the Operations Manager was over tasked to a point where adequate supervision and management of day-to-day flight operations was not always possible. The familial nature of the company also interfered at times with ensuring that company personnel consistently adhered to company policies and procedures.
2.4.5 Company Introduction of the Boeing Laptop Tool
The BLT was introduced by MK Airlines Limited without direction, assistance or approval from the GCAA. Although advisory and guidance references of the FAA and Joint Aviation Authority were used, the introduction was without adequate training and evaluation. The crew reference material was self-study and there was little direct training provided. Furthermore, the quick reference information provided in the Notice to Flight Crew of 29 March 2004 did not specifically remind pilots that, when returning from the weight and balance page, the take-off weight as listed in that page would appear in the planned take-off weight block on the performance page. This feature is believed to be a key element in how the incorrect take-off performance data were generated. It is unknown if the user(s) of the BLT in this occurrence was fully conversant with the software, in particular this feature.
2.5 Regulatory Oversight of MK Airlines Limited
In general, the safety oversight the GCAA conducted on MK Airlines Limited was limited. The GCAA's oversight effectiveness was adversely affected by the necessity to maintain a greater amount of scrutiny on another Ghana-registered airline, even though the following significant risk indicators were present at MK Airlines Limited:
- the company had had three previous accidents;
- it had been in a continuous period of growth for some time; and
- there had been deficiencies noted related to non-adherence to OM policy and SOPs identified.
The delay in obtaining Ghana parliamentary approval for new regulations and the diversity of the company's operations also affected the oversight activities. Particularly noteworthy was the undetected, ongoing and substantial exceedences related to crew flight and duty times.
In general, the regulatory oversight of MK Airlines Limited by the GCAA was not adequate to detect serious non-conformances to flight and duty times, or ongoing non-adherence to company directions and procedures.
2.6 Halifax Take-off Performance Data
Without a CVR, it was difficult to determine the exact reasons the flight crew used a low EPR setting and a low rotation speed; however, a comparison of the Bradley take-off performance data against the Halifax take-off performance data was very revealing. The first part of this section will discuss possibilities that were likely not a factor in the take-off performance of the aircraft.
One possibility is that the flight crew did not change the airspeed bugs from their positions after the Halifax landing. If this were true, two white bugs would have been set together at 133 knots, appearing to be a single airspeed bug position. The command speed bug would have been set at 143 knots, appearing to be the second airspeed bug position.Footnote 28 This would have appeared unusual to the flight crew for a take-off because the command speed bug would usually be the third bug in order, not the second. Also, when Vr was called at the second bug, the FDR would have recorded the aircraft rotating after 143 knots. The FDR data showed the aircraft rotating at 130 knots. This scenario is unlikely.
Another possibility is that the flight crew used the Bradley take-off data card since the power settings and rotations were similar. Had the flight crew not completed their post-flight activities in Halifax and not put the Bradley take-off data card in the trip envelope, then it could have been possible to mistakenly use the Bradley take-off data card. However, the card would have had a weight of 240 000 kg written on it, with a stabilizer trim setting of 4.0 units.
It is likely that the captain would have noticed the lower weight and a different trim setting from the one used in Halifax when he compared the mass and balance sheet to the take-off data card. The trim setting that had been determined by the crew in Halifax was appropriate for the aircraft actual take-off weight at Halifax. The correct trim value for Halifax was also confirmed by examination of the FDR data, the trim indicator and the screw jack measurements. If the Bradley data card had been used in Halifax, then a flight crew member would also have had to erase or cross out the Bradley trim value and replace it with the Halifax value. This scenario is unlikely.
If the flight crew had completed a new take-off data card for the Halifax International Airport, they would have had three options to calculate the take-off data: runway analysis charts, Volume 2, or the BLT. Since the runway analysis charts had been removed from all the aircraft, this scenario is only possible if one of the flight crew members had his own personal copies; this is unlikely. The take-off speeds chart of Volume 2 does not provide for obstacle clearance. If the crew had calculated the speeds based on the obstacles by using Volume 2, it would have been time consuming because of the work involved in finding and interpreting all the graphs, tables and charts. If the crew used only the take-off speeds chart of Volume 2, they would have first written the flight planned take-off weight of 353 tonnes onto the take-off data card, then transcribed a V1 of 150 knots, a Vr of 161 knots, and a V2 of 172 knots. Also, if Volume 2 had been used, it would not explain the thrust setting of 1.33 EPR. The BLT had been in use for several months and it was reported that it was being used for take-off performance calculations. Therefore, it is unlikely that Volume 2 was used. The BLT was most likely the source used for the take-off data. Consequently, it is most likely that the performance data error came from the misuse or misunderstanding of the BLT.
There are various scenarios that would have created the erroneous data. Assuming that the user input the correct airport, runway, and atmospheric information, then the only factor that would determine the V speeds and the EPR settings is the weight of the aircraft used in the planned weight box. If the user mistakenly used the zero fuel weight (262 000 kg) or landing weight (281 000 kg), the rotation speeds would be too high compared to what was found on the FDR. Another possibility is that the user input 253 000 kg instead of 353 000 kg by mistake; again, this weight is too high for the rotation speed in Halifax recorded on the FDR. Therefore, the only weight that generates the same rotation speed and EPR settings as found in Halifax is the Bradley weight, 240 000 kg.
The user would likely transcribe the weight of 353 000 kg from the flight plan on a white take off data card. When the BLT program was launched, all the previous settings, data, and information from the last use would have been populated in all the fields. The BLT was last used at Bradley International Airport with RTG II. Therefore, once the user opened the software on the RTG II page, he would have had to change all the fields to the Halifax International Airport, runway and ATIS. If the maximum thrust rating (7Q engines) had been selected, the lowest EPR value that could have been generated by the BLT was 1.40 EPR; therefore, the RTG II page had to have been used. Anytime after that, if the user opened the weight and balance page, for whatever reason, and returned to the take-off performance page, the planned weight dialogue box would be populated with the take-off weight from the weight and balance page, that is Bradley (240 000 kg). If the user did not know about this feature or did not notice the change and selected "calculate," the V speeds and EPR setting would have been identical to those for take-off from Bradley (see Figure 6).
A more comprehensive training program for the BLT that emphasized human factors and the potential for human error as described in the guidance material, combined with a method of ensuring that individuals were competent using the software, would certainly have reduced the possibility of this type of operator error.
If the user then wrote these performance numbers on the take-off data card with the correct planned weight of 353 000 kg for Halifax, it is likely that the error would not be noticed at this point. For this error to proceed to the next level, the other crew member either did not do a cross-check or did a cross-check and made the same error.
It is highly unlikely that both crew members would make the same error. For the incorrect V speeds to be set on the ASIs, it is likely that the gross error check for the planned weight of 353 000 kg was not done, because if it had been, the error would have been detected. Once the bugs were set on both ASIs, any subsequent checks would just validate the erroneous settings. If the weight of 353 000 kg was written on the card, then it would further support the numbers being correct when the captain signed and cross-checked the mass and balance sheet, and when the flight engineer set his total weight indicator.
If the Boeing T-card or a company-amended version of the T-card had been used, the take-off weight used to generate the performance data would have been printed on the T-card and it would not have matched the aircraft weight calculated by the loadmaster and noted on the mass and balance sheet.
2.7 Failure to Recognize Inadequate Take-off Performance
In this accident, the take-off was attempted using a thrust setting and take-off speeds significantly lower than those required to become safely airborne. The company's standard call for "Set MAX POWER" during every take-off would not have provided any additional opportunity to make the crew aware if the power being set was maximum or reduced. Once the take-off began, the flight crew did not recognize that the aircraft's performance was significantly less than the scheduled performance, until they reached a point where their response was insufficient to avert the accident.
Several similar accidents and incidents have shown that there have been other crews throughout the aviation industry that have not recognized inadequate take-off performance. Some of these occurrences have resulted in substantial aircraft damage and, in several cases, substantial loss of life. Notwithstanding over 30 years of effort within the industry, there still does not appear to be an acceptable industry "in-cockpit" defence that would provide crews with timely information when take-off performance is inadequate to become safely airborne.
2.8 Summary
The take-off data card was most likely completed using performance data from the BLT. The FDR data for the Halifax take-off was nearly identical to that of the Bradley take-off, indicating that the Bradley take-off weight was used to generate the performance data in Halifax. The Bradley weight in the weight and balance page was likely unknowingly transferred to the performance page due to a reversion feature of the software. The user subsequently selected "calculate," which resulted in the generation of take-off performance data containing incorrect V speeds and thrust setting for Halifax. The flight crew used the incorrect V speeds and thrust setting during the take-off attempt; however, the settings were too low, especially the thrust setting, to enable the aircraft to take off safely.
Factors that likely contributed to the incorrect take-off data being generated and then not being detected before the take-off attempt were flight crew fatigue, non-adherence to procedures, inadequate training on the BLT, and personal stresses. Once the take-off had commenced, the crew's situational awareness likely was not sufficient to allow them to detect the inadequate acceleration before it was too late to take off safely. Factors that likely contributed to this condition were flight crew fatigue and a dark take-off environment.
3.0 Findings
3.1 Findings as to Causes and Contributing Factors
- The Bradley take-off weight was likely used to generate the Halifax take-off performance data, which resulted in incorrect V speeds and thrust setting being transcribed to the take-off data card.
- The incorrect V speeds and thrust setting were too low to enable the aircraft to take off safely for the actual weight of the aircraft.
- It is likely that the flight crew member who used the Boeing Laptop Tool (BLT) to generate take-off performance data did not recognize that the data were incorrect for the planned take-off weight in Halifax. It is most likely that the crew did not adhere to the operator's procedures for an independent check of the take-off data card.
- The pilots of MKA1602 did not carry out the gross error check in accordance with the company's standard operating procedures (SOPs), and the incorrect take-off performance data were not detected.
- Crew fatigue likely increased the probability of error during calculation of the take off performance data, and degraded the flight crew's ability to detect this error.
- Crew fatigue, combined with the dark take-off environment, likely contributed to a loss of situational awareness during the take-off roll. Consequently, the crew did not recognize the inadequate take-off performance until the aircraft was beyond the point where the take-off could be safely conducted or safely abandoned.
- The aircraft's lower aft fuselage struck a berm supporting a localizer antenna, resulting in the tail separating from the aircraft, rendering the aircraft uncontrollable.
- The company did not have a formal training and testing program on the BLT, and it is likely that the user of the BLT in this occurrence was not fully conversant with the software.
3.2 Findings as to Risk
- Information concerning dangerous goods and the number of persons on board was not readily available, which could have jeopardized the safety of the rescue personnel and aircraft occupants.
- Failure of one of the airport emergency power generators to provide backup power prevented the operation of some automatic functions at the fire hall after the crash alarm was activated, increasing the potential for a delayed response.
- Grid map coordinates were not used to direct units responding to the crash and some responding units did not have copies of the grid map. The non-use of grid coordinates during an emergency could lead to confusion and increase response times.
- Communication difficulties encountered by the emergency response agencies complicated coordination and could have hampered a rescue attempt or quick evacuation of an injured person.
- A faulty aircraft cargo loading system prevented the proper positioning of a roll of steel, resulting in the weight limits of positions LR and MR being exceeded by 4678 kg (50 per cent).
- The company increase of the maximum flight duty time for a heavy crew from 20 to 24 hours increased the potential for fatigue.
- Regulatory oversight of MK Airlines Limited by the Ghana Civil Aviation Authority (GCAA) was not adequate to detect serious non-conformances to flight and duty times, nor ongoing non-adherence to company directions and procedures.
- The delay in passing the new Civil Aviation Act, 2004 hindered the GCAA's ability to exercise effective oversight of MK Airlines Limited.
- Company planning and execution of very long flight crew duty periods substantially increased the potential for fatigue.
- The company expansion, flight crew turnover, and the MK Airlines Limited recruitment policy resulted in a shortage of flight crew; consequently, fewer crews were available to meet operational demands, increasing stress and the potential for fatigue.
- There were no regulations or company rules governing maximum duty periods for loadmasters and ground engineers, resulting in increased potential for fatigue induced errors.
- The MK Airlines Limited flight operations quality and flight safety program was in the early stages of development at the time of the accident; consequently, it had limited effectiveness.
- The berms located at either end of runways 06 and 24 were not evaluated as to whether they were a hazard to aircraft in the runway overrun/undershoot areas.
- The operating empty weight of the aircraft did not include 1120 kg of personnel and equipment; consequently, it was possible that the maximum allowable aircraft weights could be exceeded unknowingly.
- The ground handling agent at Halifax International Airport did not have the facilities to weigh built-up pallets that were provided by others. Incorrect load weights could result in adverse aircraft performance.
- Some MK Airlines Limited flight crew members did not adhere to all company SOPs; company and regulatory oversight did not address this deficiency.
3.3 Other Findings
- An incorrect slope for Runway 24 was published in error and not detected; the effect of this discrepancy was not a significant factor in the operation of MKA1602 at Halifax.
- The occurrence aircraft was within the weight and centre of gravity limits for the occurrence flight, although the allowable cargo weights on positions LR and MR were exceeded.
- Based on engineering simulation, the accident aircraft performance was consistent with that expected for the configuration, weight and conditions for the attempted take-off at Halifax International Airport.
- There have been several examples of incidents and accidents worldwide where non adherence to procedures has led to incorrect take-off data being used, and the associated flight crews have not recognized the inadequate take-off performance.
- No technical fault was found with the aircraft or engines that would have contributed to the accident.
4.0 Safety Action
4.1 Action Taken
4.1.1 Safety Advisory A040058-1
On 20 October 2004, the Transportation Safety Board of Canada (TSB) issued Safety Advisory A040058-1 (Verification of Cargo Weights) to Transport Canada (TC). The Safety Advisory indicated that TC might wish to examine the adequacy of cargo handling procedures, both inside and outside Canada, and, in particular, the adequacy of load weight verification and the regulatory oversight of these issues.
On 09 December 2004, TC responded to Safety Advisory A040058-1. The letter quoted several regulations applicable to commercial operations: International Civil Aviation Organization (ICAO) standards and recommended practices, Canadian Aviation Regulations, Joint Aviation Requirements (JARs), and Federal Aviation Regulations (FARs). TC stated that the intent of the regulations is to ensure that the actual weight of the cargo, including the weight of the contents, the packing material, the packaging, the pallet or unit load device, the strapping, the wrapping, and any other device or material being transported with the cargo is accounted for in the total weight of the cargo. TC further stated that the regulations clearly indicate that it is an operator's responsibility to ensure that proper weighing procedures are in place to support its operations.
It is TC's position that the existing regulations and standards adequately address the issues raised in the Safety Advisory. However, in light of the recent accident in Halifax, Nova Scotia, and to reinforce the absolute necessity for accurate load control, TC published a Commercial and Business Aviation Advisory Circular on this issue on 04 June 2005.
4.1.2 Safety Advisory A040059-1
On 22 October 2004, the TSB issued Safety Advisory A040059-1 (Runway Slope Information - Publication Errors) to TC. The Safety Advisory raised a concern about the accuracy of published runway slope information. The slope datum for Runway 24 at Halifax International Airport published in Canadian aeronautical information publications was incorrectly depicted as 0.17 per cent down, when it should have read 0.17 per cent up. The Safety Advisory suggested that TC might wish to ensure that similar runway slope information errors do not exist for other aerodromes. A review of quality assurance measures regarding the provision and depiction of aerodrome information in Canadian flight information publications was suggested.
On 09 December 2004, TC responded to Safety Advisory A040059-1. TC indicated that a preliminary review has not uncovered further errors in published runway slope data. The error in the Halifax data is the result of a human transposition error. The error in the slope value for Runway 24 was discovered in the course of this accident investigation. TC was advised of the error, and a NOTAM (Notice to Airmen) was issued instructing holders of the Canada Air Pilot to delete the slope information for all runways at the Halifax International Airport.
Subsequently, it was discovered that, in accordance with NAV CANADA's Aeronautical Information Publication (A.I.P. Canada) specifications, only slope values greater than 0.3 per cent are published. Therefore, a second NOTAM was issued, instructing holders of the applicable documents to re-insert the slope value for Runway 33, and delete the value for Runway 24.
Additionally, as a result of this Safety Advisory, an Aerodrome Safety Urgent Bulletin was sent to TC regional offices for distribution to all airports and registered aerodromes. The Urgent Bulletin reminds all airport/aerodrome operators of their responsibility to verify the accuracy of all published data, and to report immediately, via a NOTAM, the corrections to be made to aeronautical information publications. Direction concerning the methodology for the calculation of runway slope data is being reviewed and coordinated with NAV CANADA and other interested stakeholders.
NAV CANADA subsequently advised the TSB that, between 01 January 2004 and 01 October 2004, only two requests were received to amend runway slope information contained in its aeronautical information publications. After the issue of Safety Advisory A040059-1 and up to 01 December 2005, NAV CANADA had received a total of 73 requests to amend or to add runway slope information.
4.1.3 Ghana Civil Aviation Authority
In a letter dated 01 November 2004, the Ghana Civil Aviation Authority (GCAA) instructed MK Airlines Limited to cease use of the Boeing Laptop Tool (BLT) until such time as approval is given by the GCAA. Additionally, the GCAA instructed MK Airlines Limited to comply with the crew rest requirements listed in Section 8.11 of the Ghana Civil Aviation Regulations (GCARs) until the company submits a new schedule for approval; and apply Section 8.11.1.3(a)(4) of the CGARs for loadmaster rest and Section 9.4.1.16 of the CGARs for ground engineer crew rest.
4.1.4 MK Airlines Limited
4.1.4.1 Notices to Flight Crew
On 20 October 2004, MK Airlines Limited issued a Notice to Flight Crew that stated, "Loadmasters and Station Officers are required to query weights on dead-load weight statements when two and/or several pallets are reflected at or near the same weights. Where necessary, a check weight on a suitable calibrated scale must be carried out prior to loading. DO NOT under any circumstances accept freight that has not been weighed over a calibrated and current aircraft pallet scale from a Company approved handling agent/company. Any occurrence of any nature in this regard requires an occurrence report to be completed and submitted to the FSO [Flight Safety Officer]."
On 20 October 2004, MK Airlines Limited issued a Notice to Flight Crew on the above topic that stated, "With immediate effect to avoid any confusion, the weight and index for the total number of people on board (flight deck and all passengers) must be shown in the 'correction' box in both the B747 and DC-8 load sheets. The basic weight does not include 'crew'."
Within two weeks of the accident, MK Airlines Limited issued a Notice to Flight Crew to immediately cease use of the BLT and use alternate procedures. A formal submission has been made to the United Kingdom Civil Aviation Authority (CAA) in accordance with Temporary Guidance Leaflet No. 36: Approval of Electronic Flight Bags (EFBs).
On 03 February 2005, MK Airlines Limited issued a Notice to Flight Crew on the above topic that stated that the EFBs (JeppView® computers) are not to be used until such time as their use has been formally approved in compliance with the JAR guidelines.
4.1.4.2 Operations
At the request of MK Airlines Limited, the United Kingdom government, in cooperation with the GCAA, conducted a full audit for ICAO compliance on 16 November 2004. As a result of the audit, MK Airlines Limited decided to obtain JAR compliance in accordance with the United Kingdom authorities.
The United Kingdom CAA publication entitled Avoidance of Fatigue in Air Crews (CAP 371) lists the regulations for the avoidance of fatigue in aircrew. MK Airlines Limited has asked the GCAA for approval to use this flight time limitation scheme and has amended its operations manual (OM) accordingly. This scheme was approved in May 2005 and has been fully implemented, and United Kingdom CAA inspectors are monitoring compliance. A crew notice was issued concerning the noting of duty times on voyage reports to enable better monitoring of required rest times.
The MK Airlines Limited rostering staff has been briefed on the CAP 371 limitations and will monitor crew scheduling with in-house developed software to prevent exceedences. Crews were briefed on the new flight time limitations and their responsibilities for compliance. Flight documents are subject to close inspection to ensure that captain's discretion reports are completed when required.
A crew notice was issued concerning counselling to reduce fatigue and stress in light of the accident and the continued political and security situation in southern Africa. A new pay scheme introduced in December 2004 improved the financial security of crew members and has been well received.
The audit program of ground service contractors has been enhanced by the qualification of MK Airlines Limited loadmasters to the British Standards Institution (BSI) Lead Assessor standard. More detailed audit procedures have been developed under control of the newly appointed Director, Safety and Quality. The new Safety and Quality Department will coordinate audit activities across the technical, operational, security, and traffic disciplines.
A safety management system was established throughout the company, and a new company safety policy was drafted. A program of flight data monitoring is being implemented as part of the flight operations quality system. This forms part of the safety management system, which integrates safety, quality, and security management of the company. Key staff attended a flight operations quality assurance course from 04 April to 07 April 2005, at Cranfield University, United Kingdom.
A safety culture questionnaire was drafted and included in the latest company safety magazine to acquire employee feedback.
4.1.4.3 Training
There have been extensive revisions to the training manual under United Kingdom CAA guidance to achieve JAR compliance. A new Assistant Training Manager was appointed, who has an extensive background in training management. Training is now compliant with JAR-FCL (flight crew licensing)/JAR-OPS (operations) requirements. Non-JAR-licensed aircrew have commenced study courses for JAR licences.
Numerous companies and consultants were contracted or employed to oversee training standards:
- CTC Crew Training Centre, Bournemouth, United Kingdom - Type Rating Instructor (TRI) training.
- Global Air Training, Cheshire, United Kingdom - Crew Resource Management Instructor (CRMI) and Security Instructor training.
- Consultant - former Flight Operations Training Inspector, United Kingdom CAA. Responsibilities include monitoring instructor training standards.
- Consultant - former British Airways B747 Type Rating Examiner (TRE). Providing expertise in B747 type specific instructor training and standardization.
- Assistant Training Manager - former British Airways Senior Flight Engineer Instructor. Specific responsibilities include ensuring that training documentation and policies under development are of the required standard before submission to authorities.
The company's OM (Part A, Section 8 - Draft for approval by United Kingdom CAA) has been updated with various flight briefings to improve the level of situational awareness. Procedures were developed to ensure continued alignment of company training manuals with current national and international regulations and manufacturer's service bulletins. The training record system for each fleet was reviewed and aligned with the requirements of the training manual. A training expiry database was developed and will be reviewed to ensure that Part D, JAR-FCL requirements are met. Airworthiness directives and manufacturers service bulletins procedures are in Section 2.11 of the maintenance control manual and are being rewritten in the Maintenance Organization Exposition to comply with Section 145 of the JARs. An Information Management Department was established.
A system has been developed to improve the crew qualification system for categories B and C aerodromes. Crew participation in information gathering and updating of aerodrome information has been implemented, incorporating a risk assessment and controlled flight into terrain analysis. Part C of the OM now includes route and aerodrome briefs. In addition to the air operating certificate (AOC) application, MK Airlines Limited will apply for Type Rating Training Organization (TRTO) in accordance with the JARs. MK Airlines Limited is in the process of publishing a TRTO manual for approval, which will contain all the requirements for instructors, instructor training, standards, and facilities.
MK Airlines Limited has initiated a process to ensure that all company instructors and examiners are qualified to JAR-FCL, Subpart I. For example:
- Section 680 of JAR-FCL, Issue 4, has been distributed to all potential TRI and TRE for licensing purposes. Authorization and accreditation for TRIs and TREs will be sought only after licences have been issued and all criteria in sections 1.365 and 1.405 of JAR FCL, and CAA standards document 24, version 4, have been met.
- In respect of the above, 14 instructors have attended the JAR-approved TRI course at the CTC Crew Training Centre in Bournemouth. This training included CRMI (simulator/line) training. Three B747 training personnel have completed a TRI course on the B747 and have received approvals from the United Kingdom CAA. A standardization course is planned for the above instructors as soon as they have gained the necessary experience for approval as TRE.
- United Kingdom CAA-recommended persons will conduct standardization courses when instructors are upgraded from TRI to TRE status.
- Four instructors (two pilots, one flight engineer and one loadmaster) have completed a JAR-approved CRMI (Ground) course at Global Air Training in Cheshire.
The first Boeing 747 training course, in accordance with the new JARs, commenced in May 2005. Work is under way at the company operations centre at Landhurst to add a Training Department wing to the existing structure. The new wing will house the Boeing 747 simulator, the Training Department personnel offices, and the Safety and Quality Department.
Proficiency check rides for each flight crew member have been updated to reflect the requirements of sections 1.240, 1.295 and 4.240 of JAR-CFL, Appendix 2. MK Airlines Limited has initiated a biennial technical ground training program for aircraft systems. Syllabus and course material comply with Subpart N of JAR-OPS. MK Airlines Limited has completed a program of initial and recurrent training for loadmasters to include crew resource management training. The chief loadmaster attended CRMI training from 10 January to 14 January 2005. Eight 3-day courses were conducted for all loadmasters between 16 January and 12 February 2005.
Enhanced ground proximity warning systems (EGPWS) have been added to the ground and simulator training for the B747 fleet. A two-hour EGPWS lecture was programmed for January to June 2005 during recurrent training. An interactive CD ROM was issued to each crew member for home study.
A biennial training requirement for aircraft performance and de-icing was added to the recurrent ground training program. De-icing holdover times in the OM, Part A, Section 8.2.4.8.3, were amended on 21 December 2004 to bring them in accordance with the Association of European Airlines tables (19th edition, September 2004). A Crew Notice was issued on 21 December 2004 to ensure crew awareness and to provide interpretation information.
4.1.4.4 European Aviation Safety Agency Certification
MK Airlines Limited has applied for a United Kingdom AOC.
The company organization has been revised to comply with or surpass the JARs, with the addition of several new, full-time appointments of highly qualified staff. The AOC project plan is managed by the Director, Safety and Quality and was completed in late 2005.
In support of the AOC application, the following activity has been initiated and/or completed:
- The OM was rewritten in compliance with JARs and submitted to the United Kingdom CAA.
- There have been extensive revisions to the training manual to achieve JAR compliance.
- A new JAR-compliant organizational structure has been developed:
- The position of Director, Safety and Quality was created.
- The new Director, Safety and Quality is an airline transport pilot licence holder with extensive aircrew, safety management system and specialized regulatory experience.
- The Flight Safety Officer (Accident Prevention Advisor) is now part of the coordinated safety team.
- An Aircrew Liaison Officer has been appointed as Flight Operations Quality Assurance interface with a confidential safety management function.
- The position of Ground Operations Manager was created and filled.
- The position of Training Manager was created and filled.
- The position of Assistant Training Manager was created and filled.
- Terms of reference in the company OM for these positions were revised for United Kingdom CAA approval.
- Part D, Training, of the OM was re-written to meet the JAR-FCL requirements and was submitted to the United Kingdom CAA for approval. This document has recently been approved.
A revised B747 JAR-compliant minimum equipment list, based on the United Kingdom CAA master minimum equipment list, was submitted for approval. Changes were required and the amended version has been resubmitted as part of the AOC application.
The newly appointed Ground Operations Manager has implemented tighter oversight of contracted ground handling companies.
4.1.4.5 Airworthiness
A full check of aircraft equipment by the United Kingdom CAA was undertaken and confirmed that all aircraft were fully ICAO-compliant. Fuelling and loading procedures were reviewed to ensure standardization across both B747 and DC-8 fleets.
In February 2005, the company commenced the application process for European Aviation Safety Agency (EASA) Part M (maintenance management) and EASA Part 145 approval. In March 2005, MK Airlines Limited started the recruitment of EASA Part 66 licensed staff and introduced training for existing staff to convert licences. In the first six months of 2005, the company undertook or completed several safety actions regarding airworthiness:
- completed response actions to the United Kingdom CAA audit of November 2004;
- received United Kingdom CAA confirmation of MK Airlines Limited compliance with ICAO standards and recommended practices;
- recruited a new Engineering Manager (37 years of experience);
- completed a review of engineering procedures and a restructuring of engineering manuals to ensure compliance with EASA requirements;
- undertook a review of Engineering Quality Department procedures and the recruitment of additional staff;
- undertook an internal audit of all engineering departments and maintenance bases against EASA requirements;
- submitted applications for registration of the B747 fleet in the United Kingdom and EASA Certificate of Airworthiness; and
- completed staff training in human factors and EASA regulatory requirements.
4.1.5 Boeing
On 11 November 2004, Boeing released a BLT Operator Message to all users of the Boeing laptop computer. The message reviewed the built-in feature of the software that automatically overwrites any entry in the planned weight field on the main screen when a user views the weight and balance summary page, and the performance data will be calculated on the weight in that field. The message urged all operators to ensure that their crews were properly trained on that feature.
4.1.6 Halifax International Airport Authority
The Halifax International Airport Authority (HIAA) has indicated that it has made the following change to the Aircraft Rescue and Fire Fighting (ARFF) operation:
- Three extra self-contained battery-operated lighting fixtures have been installed at the fire hall to provide more emergency lighting in the event of a power failure.
The HIAA has also indicated that it plans the following changes to the ARFF operation:
- The lighting system in the fire hall vehicle bay will be modified. The high-pressure sodium bulbs will be replaced with eight-foot fluorescent lights that will come on immediately when emergency power is available.
- An uninterruptible power supply will be installed in the alarm room to ensure a power supply to the relay that activates all the automatic features triggered by the crash alarm.
4.1.7 United Kingdom Civil Aviation Authority
Since the MKA1602 accident, the United Kingdom CAA has continued ramp and in-flight inspections of MK Airlines Limited. The United Kingdom CAA held discussions with management personnel of MK Airlines Limited about the ICAO definition of "principal place of business" and if it was still appropriate for MK Airlines Limited to hold an AOC issued by Ghana. During the last part of November 2005, with the mutual agreement of MK Airlines Limited management, the GCAA and the United Kingdom CAA, the United Kingdom CAA conducted a comprehensive audit of MK Airlines Limited. The audit was conducted by approximately five inspectors over a period of five days. Nothing of an immediate threat to safety was detected, and MK Airlines Limited continued to operate out of the United Kingdom.
4.1.8 United States Federal Aviation Administration
On 30 April 2005, the Federal Aviation Administration (FAA) announced publicly that Ghana was not complying with ICAO international safety standards. As a result, the FAA lowered the safety rating for Ghana from Category 1 to Category 2. The FAA statement said that it will remain engaged with the GCAA and will periodically review the situation with the intention of encouraging improvements that will qualify Ghana for a Category 1 rating.
4.2 Action Required
4.2.1 Take-off Performance Monitoring System
In this accident, the take-off was attempted using a thrust setting and take-off speeds significantly lower than those required to become safely airborne. The company's standard call for "Set MAX POWER" during every take-off would not have provided any additional opportunity to inform the crew if the power being set was maximum or reduced. Once the take off began, the flight crew did not recognize that the aircraft's performance was significantly less than the scheduled performance until they were beyond the point where the take-off could be safely conducted or safely abandoned.
Several similar accidents and incidents have shown that there have been other crews throughout the aviation industry that have also not recognized inadequate take-off performance. Some of these occurrences have resulted in substantial aircraft damage and, in several accidents, substantial loss of life. Although several efforts have been undertaken to develop procedural and technical solutions that would alert crews to inadequate aircraft acceleration performance during take-off, these efforts still have not resulted in a reliable methodology or system being introduced and/or installed in transport category aircraft. Without such a system, there continues to be an unacceptable level of risk to crews and the travelling public.
Therefore, the Board recommends that:
The Department of Transport, in conjunction with the International Civil Aviation Organization, the Federal Aviation Administration, the European Aviation Safety Agency, and other regulatory organizations, establish a requirement for transport category aircraft to be equipped with a take-off performance monitoring system that would provide flight crews with an accurate and timely indication of inadequate take-off performance.
Transportation Safety Recommendation A06-07
4.3 Safety Concerns
4.3.1 Man-Made Objects in Runway Undershoot and Overshoot Areas
Although the berms constructed at Halifax met ICAO and TC required obstacle-clearance standards, the aircraft's lower aft fuselage did strike the berm off the end of Runway 24, causing the tail to separate from the aircraft and rendering the aircraft uncontrollable. Also, there are no specific standards or recommended practices regarding the construction and risk assessment of berms or similar immovable objects in the runway overrun/undershoot areas beyond the established runway end safety area.
The Board is concerned that, because man-made objects, such as the berms off the ends of runways 06 and 24 at Halifax International Airport, are not evaluated in terms of their potential risk to aircraft landing or taking off, there is the potential that an unnecessary hazard may be allowed to exist when mitigation for such risk may be reasonably undertaken.
4.3.2 Persons and Dangerous Goods on Board
Air traffic controllers were unable to get timely information on the number of persons and dangerous goods on board the aircraft. Although MK Airlines Limited was able to provide information regarding the number of persons on board about one hour after the accident, it was not until 10 hours after the accident that rescue and fire-fighting personnel received a listing of the dangerous goods that had been loaded at the previous stop. While there is a requirement for aircraft operators to record both dangerous goods and persons on board, this information is frequently not accessible in a timely manner.
The National Transportation Safety Board (NTSB) has made recommendations for regulatory authorities and operators to address this deficiency, as follows:
- Recommendation A-90-105, issued 03 September 1990: The NTSB recommends that the Federal Aviation Administration: require airlines to provide airport crash/fire rescue personnel accurate and timely numbers of all persons aboard an accident/incident aircraft, and to provide assistance in determining the disposition of persons who have been recovered from the scene of an accident.
- Recommendation A-98-080, issued 12 August 1998: The NTSB recommends that the Federal Aviation Administration: require, within 2 years, that air carriers transporting hazardous materials have the means, 24 hours per day, to quickly retrieve & provide consolidated specific info about the identity (including proper shipping name), hazard class, quantity, number of packages, & location of all hazardous materials on an airplane in a timely manner to emergency responders.
- Recommendation A-05-017, issued 31 May 2005: The NTSB recommends that the Federal Aviation Administration: inform all air traffic control tower controllers of the circumstances of this accident, including the need to ensure that aircraft rescue and firefighting (ARFF) vehicles are not delayed without good cause when en route to an emergency and the need to relay the number of airplane occupants to ARFF responders.
On 13 January 1999, a Douglas DC-3C aircraft crashed on Mayne Island, British Columbia. The accident aircraft was transporting a small amount of dangerous goods. Although personnel involved in the transportation industry were aware of the items, the first responders to the accident site were not. The TSB investigation report contained the Finding as to Risk, "First responders were not aware of the presence of the dangerous goods and were therefore at increased risk during their response activities on the site." (TSB Investigation Report A99P0006)
On 15 September 2000, a Boeing 727 aircraft landed at Ottawa, Ontario, and overran the runway. There was no damage to the aircraft or injury to the nine crew members. There were no passengers on board. The TSB investigation report contained the Finding as to Risk, "The emergency response services (ERS) vehicles approached the aircraft with no knowledge of the number of passengers, the amount of fuel on board, or whether any dangerous goods were on board. The tower controller did not have that information to pass on to the ERS personnel, potentially delaying or slowing ERS operations and therefore jeopardizing ERS and passenger safety." (TSB Investigation Report A00H0004)
Despite the actions taken by the NTSB and the TSB's prompting of regulators to address the safety deficiency, the unsafe condition continues to persist. The Board is concerned that all air carriers do not have a reliable system to provide, in a timely manner, specific information about the number of persons on board an aircraft and the identity, number, and location of all hazardous materials loaded on their aircraft. This lack of accurate information can compromise the effectiveness of the response and potentially put rescue personnel and the aircraft occupants at greater risk than is necessary.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .
5.0 Appendices
- Appendix A - Flight Data Recorder Engine Data Comparison Between Bradley and Halifax
- Appendix B - Flight Data Recorder Flight Controls Comparison Between Bradley and Halifax
- Appendix C - Take-off Sequence
- Appendix D - Sequence of Events
- Appendix E - Glossary
Appendix A - Flight Data Recorder Engine Data Comparison Between Bradley and Halifax

Appendix B - Flight Data Recorder Flight Controls Comparison Between Bradley and Halifax

Appendix C - Take-off Sequence
Appendix D - Sequence of Events
| Time (UTC) | Sequence nts Summary | Indicated Airspeed (knots) | Pitch (degrees) | Distance from Runway 24 threshold (feet) |
|---|---|---|---|---|
| 0647:06 | Flight data recorder (FDR) powers on. All engines are running, parking brake is on, flaps are retracted, horizontal stabilizer is at 3.3 trim units, heading is 337°M, static air temperature is 7.7°C | 50 | −0.9 | |
| 0648:36 | Thrust levers are advanced | 50 | −0.9 | |
| 0648:40 | Aircraft begins to taxi | 50 | −0.9 | |
| 0648:58 | Flap handle position set to 20°. Horizontal stabilizer position briefly moves from 3.28 trim units to 4.9, then briefly decreases to 4.6, followed by further increase to 6.1 trim units (and remains at 6.1 trim units to end of flight) | 50 | −0.4 | |
| 0649:05 | Leading edge flaps extended | 50 | −0.4 | |
| 0649:48 | Aileron control check performed | 50 | −0.4 | |
| 0650:03 | Elevator control check performed | 50 | −0.4 | |
| 0650:14 | Rudder control check performed | 50 | −0.4 | |
| 0651:13 | Starts onto runway | 50 | 0 | |
| 0651:51 | Backtracks Runway 24 | 50 | −0.9 | |
| 0652:49 | Starts right turn at threshold, to line up for take-off Runway 24 | 50 | −0.9 | |
| 0653:18 | Stops right turn on heading 240°, aligned with runway centreline | 50 | −0.4 | 194 |
| 0653:19 | Thrust levers are advanced for rolling take-off | ? | −0.4 | 205 |
| 0653:31 | Split occurs in throttle lever angles | ? | −0.4 | 474 |
| 0653:35 | Recorded airspeed begins to record data above 50 knots indicated airspeed (KIAS) | 51 | −0.5 | 725 |
| 0653:36 | Engines stabilize at take-off power (engine pressure ratios at 1.32 to 1.34; engines 2 & 3 thrust lever angles (TLAs) at 47 per cent and 43 per cent, while engines 1 & 4 TLAs at 30 per cent) | 53 | −0.5 | 801 |
| 0654:08 | Control column moves aft to initiate rotation | 130 | −0.5 | 5483 |
| 0654:10 | Nose-up rotation commences; elevator data mirrors control column movement | 135 | −0.4 | 5907 |
| 0654:13 | Control wheel moves clockwise to 6.1° (6° to 7° clockwise input for next 6 seconds); control column moves aft to 8.4° | 140 | 2.3 | 6571 |
| 0654:15 | Rudder (lower) deflects right to 2.5° | 143 | 6.7 | 7026 |
| 0654:16 | Control column moves to 8.3° aft; pitch briefly stabilizes at 9°; pitch rate approximately 2.2 degrees per second | 143 | 8.5 | 7257 |
| 0654:17 | Control column moves further aft to 10° (data loss due to tape splice) | 145 | ? | 7490 |
| 0654:18 | Control column moves to 9.1° aft; pitch reaches 10.6° (next 4 samples indicate pitch stabilizing in 11° range, consistent with lower aft fuselage/ground contact) | ? | ? | 7726 |
| 0654:19 | Control column at 9.0° aft; pitch reaches 11.1° | ? | 10.7 | 7965 |
| Start of initial runway scrape mark number 1 | 7977 | |||
| End of scrape mark number 1 | 8103 | |||
| 0654:20 | Control wheel moves clockwise to 14.2°; control column moves aft to 12.0°; pitch reaches 11.5°; thrust levers are advanced | 149 | 11.2 | 8207 |
| Start of second runway scrape mark number 2 | 8389 | |||
| 0654:21 | Control column moves aft to 12.6°; pitch at 11.5°; engine pressure ratios of engines 2 & 3 reach 1.6 (maximum commanded thrust); engine pressure ratios of engines 1 & 4 are no longer recorded | 149 | 11.5 | 8449 |
| 0654:22 | Control column moves further aft to 13.5°; rudder (lower) deflects right to peak 8°; pitch reaches 11.9° (data loss likely due to lower aft fuselage contact with runway) | 152 | 11.6 | 8692 |
| End of useable runway | 8800 | |||
| 0654:23 | FDR data loss | ? | ? | 8939 |
| 0654:24 | Control column at 13.4° aft; pitch reaches 14.5°; first tilt switch sample indicating “Air” | ? | 14.5 | 9188 |
| 0654:25 | Data loss likely due to lower aft fuselage impact with localizer berm; localizer berm at 9955 feet; therefore, position discrepancy equates to an error of approximately 5 per cent | 155 | ? | 9438 |
| End of scrape mark number 2 in grass | 9622 | |||
| 0654:26 | Data loss due to localizer berm strike continues for another second | ? | ? | 9691 |
| 0654:27 | Data loss | ? | ? | 9947 |
| Localizer berm position | 9955 | |||
| 0654:28 | Maximum recorded radio altitude is 36 feet; pitch decreases to -5.4° | ? | ? | 10 206 |
| 0654:29 | Final recorded sample of radio altitude at 0 feet; pitch further decreases to -20.9°; horizontal stabilizer position records spurious value of -72.8 trim units following localizer berm impact; FDR stops recording | R | −8.8 | 10 468 |
Appendix E - Glossary
- AC
- Advisory Circular
- A/C
- aircraft
- AFM
- aircraft flight manual
- agl
- above ground level
- AOC
- air operating certificate
- ARFF
- Aircraft Rescue and Fire Fighting
- ASI
- airspeed indicator
- asl
- above sea level
- ATC
- air traffic control
- ATIS
- automatic terminal information service
- ATPL
- airline transport pilot licence
- B747
- Boeing 747-200
- BLT
- Boeing Laptop Tool
- BSI
- British Standards Institution
- CAA
- Civil Aviation Authority
- CAP
- Civil Air Publication
- CAP 371
- United Kingdom Civil Aviation Authority publication entitled Avoidance of Fatigue in Air Crews
- CRMI
- Crew Resource Management Instructor
- CVR
- cockpit voice recorder
- EASA
- European Aviation Safety Agency
- EFB
- electronic flight bag
- EGPWS
- enhanced ground proximity warning system
- EPR
- engine pressure ratio
- ERS
- emergency response services
- FAA
- Federal Aviation Administration (United States)
- FARs
- Federal Aviation Regulations
- FCL
- flight crew licensing
- FDR
- flight data recorder
- FL
- flight level
- FSO
- Flight Safety Officer
- GCAA
- Ghana Civil Aviation Authority
- GCARs
- Ghana Civil Aviation Regulations
- GMF
- Garuda Maintenance Facilities
- HIAA
- Halifax International Airport Authority
- HRM
- Halifax Regional Municipality
- IASA
- International Aviation Safety Assessments
- ICAO
- International Civil Aviation Organization
- ILS
- instrument landing system
- in Hg
- inches of mercury
- JARs
- Joint Aviation Requirements
- KCAS
- knots calibrated airspeed
- kg
- kilograms
- KIAS
- knots indicated airspeed
- LUX
- Luxembourg
- m
- metres
- MAC
- mean aerodynamic chord
- MKA1601
- MK Airlines Limited Flight 1601
- MKA1602
- MK Airlines Limited Flight 1602
- N
- north
- N/A
- not applicable
- NOTAM
- Notice to Airmen
- NTSB
- National Transportation Safety Board (United States)
- OM
- operations manual
- PDUs
- power drive units
- PF
- pilot flying
- QRH
- quick reference handbook
- RCMP
- Royal Canadian Mounted Police
- RESA
- runway end safety area
- RTG II
- Rating II
- SARPs
- standards and recommended practices
- SITA
- Société Internationale de Télécommunications Aéronautiques
- sm
- statute miles
- SOPs
- standard operating procedures
- STAS
- Standard Take-off Analysis Software
- TAT/EPRL
- true air temperature/engine pressure ratio limit
- TC
- Transport Canada
- TLAs
- thrust lever angles
- TODAs
- take-off distances available
- TP
- Transport Publication
- TP 312
- Transport Canada Publication entitled Aerodrome Standards and Recommended Practices
- TRE
- Type Rating Examiner
- TRI
- Type Rating Instructor
- TRTO
- Type Rating Training Organization
- TSB
- Transportation Safety Board of Canada
- UTC
- coordinated universal time
- VAR
- visual-aural range
- V1
- take-off decision speed
- V2
- take-off safety speed
- Vmcg
- minimum control speed, ground
- Vmu
- expected minimum unstick speed
- Vr
- rotation speed
- Vref
- landing reference speed
- W
- west
- Z
- Zulu time (equivalent to UTC)
- ′
- minutes
- ″
- seconds
- °
- degrees
- °C
- degrees Celsius
- °M
- degrees magnetic
- °T
- degrees true