Loss of Control
Cessna 305A C-GYHF
Thetis Island, British Columbia
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
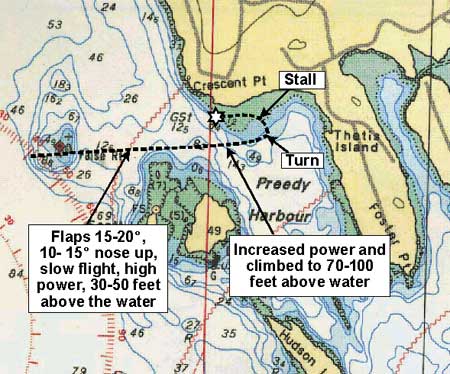
The pilot, flying a privately-owned Cessna 305A float plane (registration C-GYHF, serial number 23260) departed Ganges Harbour on Saltspring Island, British Columbia Footnote 1 at about 0840 Pacific daylight time Footnote 2 (Coordinated Universal Time minus seven hours) and flew to Thetis Island to pick up a passenger. They then took off on a local flight to photograph boats and fleet activities related to an annual regatta at Thetis Island. The passenger was seated in the rear cockpit. Both rear windows of the aircraft were opened inward and secured to permit photography. During low-level manoeuvring near the fleet, just before the accident occurred, the aircraft flew in an easterly direction, south of the fleet (see Appendix A).
The aircraft was being flown in slow flight at a high power setting; the flaps were extended 15 to 20 degrees and the nose of the aircraft was 10 to 15 degrees nose up. During the initial portion of the pass, the aircraft's height was estimated to be 30 to 50 feet above the water. As the aircraft approached Thetis Island, the engine sound increased and the aircraft began to climb in a steep attitude to 70 to 100 feet above the water. The aircraft then banked sharply to the left and the nose dropped abruptly to a steep, nose-down attitude. There was no recovery from the descent, and the aircraft struck the water in a left-wing-down, nose-low attitude. The pilot was fatally injured on impact; the passenger escaped through the left-side rear window and was rescued from the water by nearby boaters. The accident occurred at 1019.
Factual information
Pilot Qualifications and Experience
The pilot held a private pilot licence and valid Category 3 medical certificate at the time of the accident. His total flight experience at the time of his last medical was about 800 hours, and he had been flying at a rate of 100 to 150 hours per year. He had owned and operated the aircraft since July 1998 and was well acquainted with the aircraft's performance. He had flown a similar flight profile with this same photographer on a number of previous occasions.
Aircraft
The aircraft was built by Cessna Aircraft Corporation in 1952 and was initially operated by the military. This aircraft type is approved for civilian operation in Canada under the authority of Type Certificate 5A5. Cessna Aircraft Corporation has sold the rights to this Type Certificate to Regal Air, Inc. of Fort Collins, Colorado, United States.
The aircraft had been flown a total of about 6100 hours since manufacture and about 70 hours over the last calendar year. The most recent annual inspection was completed on 04 August 2003.
The engine was replaced in February 2004. The pilot had noted that several of the engine instruments were not working properly after the installation; however, these problems had been repaired well in advance of the accident flight. The aircraft log books do not record any mechanical problem related to the new engine.
The aircraft's most recent empty weight was documented as 1721.8 pounds; the maximum allowable weight in the seaplane configuration is 2400 pounds. Based on the documented weight of the pilot at his last medical and an estimated weight of the passenger, the aircraft would have been within the certificated weight and balance envelope regardless of the fuel load.
Normally a Cessna 305A aircraft has one access door on the right side of the fuselage. This particular aircraft had been modified with a second access door on the left side of the aircraft. That door could not be opened from outside the aircraft.
The aircraft's airspeed indicator had markings on it to indicate various speeds. However, the following markings were improperly placed:
- The maximum flap speed was placed at 100 knots rather than at 87 knots, as required by the Type Certificate.
- The never-exceed speed was placed at 170 knots rather than at 137 knots, as required by the Type Certificate.
- The normal stall speed (bottom of the green arc) was located at 100 knots; it should have been located at 48 knots, based on the aircraft flight manual.
- The stall speed with flaps extended (bottom of the white arc) was located at 65 knots; it should have been located at 44 knots, based on the aircraft flight manual.
Aircraft Stall Warning System
After removal from military service, the aircraft was equipped with a "Safe Flight" stall warning system, as required by the aircraft's Type Certificate. This system incorporates a vane-type actuator mounted in the leading edge of the left wing with a combination light and horn warning component that is designed for mounting in a standard hole in the aircraft's instrument panel. In the accident aircraft, the warning light and horn component was mounted under the instrument panel to the right of the pilot's right knee. The placement of the instrument in this position rendered the visual warning ineffective because it was outside the pilot's normal field of view.
The stall warning system also generates a tone to provide aural warning of an impending stall. The horn was bench-tested after the accident and found to generate a 93 to 96 decibels-level sound at a distance of 2.5 to 3 feet. The effectiveness of this aural warning will vary depending on ambient sound levels in the cockpit. During a test on a similar aircraft operating under high power with the rear windows open, the ambient noise levels in the cockpit were measured to be as high as 120 to 130 decibels absolute. Under those flight conditions, the audibility of the aural warning was reduced significantly.
Wreckage Examination
A technical examination and analysis of the wreckage following the accident found the following:
- The engine was producing power at impact. This conclusion is supported by the tip curling of the propeller blades and by the impact damage caused to the float system by the propeller rotation.
- It is unlikely that there was any control malfunction. Control continuity was confirmed for aileron, elevator, rudder, and trim control systems. The flaps were found to be selected to between 15 and 20 degrees.
- There was no indication of a structural failure. All flight control surfaces were accounted for, and bending and breakage of structural components was consistent with the crash dynamics. Overload damage to the main spars of the wings was consistent with a steep, left-wing-low impact. Damage to the seat restraint system and the seat structures support this conclusion.
- Although the aircraft was equipped with an entry door on each side of the aircraft, only the door on the right side was operable from outside the aircraft; any rescue attempt from the left side of the aircraft would have been impeded by a lack of external access. Both rear windows were open.
Aerodynamic Stall
Transport Canada's Flight Training Manual states that an aerodynamic stall occurs when the aircraft's wing is no longer capable of providing the lift required to counteract the aircraft's weight. An aircraft may be stalled in practically any attitude and airspeed. When an aircraft stalls at low airspeed with power on, the stall speed will be slightly lower than for a power-off stall; therefore, there will be a decrease in aileron effectiveness. Other factors, such as engine torque, will contribute to the difficulty of controlling a power-on stall. Generally, a power-on stall will be more violent than a power-off stall, and the resultant decrease in controllability will be greater.
Life Jackets
Neither occupant was wearing a life jacket at the time of the accident, and the survivor exited the aircraft without getting one. The TSB has, on several occasions, raised concerns regarding the availability of life jackets for those escaping from float plane accidents. Data show that following a crash, because occupants think only about escaping from the aircraft, they often do not take the time to get the life jackets that are provided for their safety. Once clear of the aircraft, many drown because they lack an appropriate flotation device. To date there is no regulation requiring either crew members or passengers to wear flotation devices while on board a float plane.
Analysis
Various descriptions of the flight are consistent with a power-on, aerodynamic stall. This type of stall will typically result in a more complete loss of control than a power-off stall, and more altitude will be required for recovery. Low-altitude, slow-speed manoeuvring increases the risk of an inadvertent stall and reduces the available recovery time.
Positioning the stall warning system under the instrument panel rendered the visual warning ineffective because it was outside the pilot's normal field of view. High engine power operation with rear windows open raised the ambient noise levels in the cockpit and reduced the effectiveness of the aural stall warning.
The improperly placed airspeed range markings provided no assistance in visually recognizing the normal operating speeds of the aircraft, and could not be used as a defence against either an aerodynamic stall or an aircraft over speed.
Findings as to Causes and Contributing Factors
- The aircraft stalled at an altitude from which there was insufficient time or altitude to recover.
- High ambient sound levels reduced the effectiveness of the aural stall warning system.
- Mounting the stall warning system under the dash placed it outside the pilot's normal field of view and rendered the visual stall warning ineffective.
- Improperly placed airspeed range markings eliminated their effectiveness as visual indicators of the normal safe-flight ranges.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .
Appendices