Loss of Control - Collision with Terrain
Piper PA-46-310P, C-GUZZ
Kamsack, Saskatchewan
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The privately operated Piper PA-46-310P Malibu (registration C-GUZZ, serial number 46-8508108) departed Kamsack, on an instrument flight rules flight to Saskatoon, Saskatchewan. The pilot and three passengers were on board. At takeoff from runway 34, the aircraft began rolling to the left. The aircraft initially climbed, then descended in a steep left bank and collided with terrain 200 feet to the left of the runway. A post-impact fire ignited immediately. Two passengers survived the impact with serious injuries and evacuated from the burning wreckage. The pilot and third passenger were fatally injured. The aircraft was destroyed by impact forces and the post-impact fire. The accident occurred during evening civil twilight at 2124 Central Standard Time.
Other Factual Information
History of the Flight
The flight originally departed from Saskatoon during the afternoon of the occurrence, with the pilot and two passengers on board. Before departure, the pilot obtained a weather briefing from a computer terminal, conducted a pre-flight inspection of the aircraft and gave the passengers a safety briefing, including information about exit location and operation. The flight departed Saskatoon at about 1400Footnote 1. The flight was uneventful and arrived in Kamsack at about 1500.
The aircraft party was met by a ground party and, after pushing the aircraft onto a grass parking area, the group departed the aerodrome. During the evening, the pilot obtained a telephone weather briefing and filed an instrument flight rules (IFR) flight plan from Kamsack to Saskatoon with a proposed departure time of 2100 and an estimated fuel endurance of four hours.
The party, with one additional passenger, arrived at Kamsack at about 2100. After conducting a pre-flight aircraft inspection, the pilot taxied the aircraft onto the runway facing southward. With the engine running, the three passengers boarded the aircraft through the door immediately aft of the left wing, after which the pilot closed the door. The pilot continued his pre-flight checks, including loading waypoints into the global positioning system (GPS) and conducting a pre-flight test of the King KFC150 automatic flight control system.
The passengers in the right cockpit seat and the left rear seat were wearing headsets and could hear the pilot on the intercom system. The pilot and all three passengers used the available three-point seat belt/shoulder harness restraint systems.
While the pilot taxied the aircraft to the threshold of runway 34, he broadcast a traffic advisory on the radio. During the takeoff run on runway 34 at Kamsack, the aircraft yawed to the left, remaining on the runway surface until takeoff. During and following the takeoff run, the engine sound did not change.
At takeoff, the aircraft began rolling to the left, and the pilot made aileron control inputs accordingly.
The aircraft climbed to a height of about 50 feet before descending and colliding with the terrain to the left of the runway. Aircraft attitude at impact was estimated to be between 45° and 90° left bank and between 15° and 30° nose-down pitch. A fuel-fed, post-impact fire ignited as the aircraft broke up and came to rest inverted; the fire spread rapidly.
With his clothing on fire, the right seat cockpit passenger freed himself from his restraint belts, determined that the pilot was unresponsive, unsuccessfully ttempted to free him from his restraint belts and then made his way aft. He found the entrance door on the left side of the aircraft open and exited. The left rear passenger unfastened his own restraint belts, determined that the right rear passenger was unresponsive, unsuccessfully attempted to release him from his restraint belts and then also exited through the door.
One member of the ground party immediately called 911 to activate emergency response services. Another member of the ground party drove his vehicle across the runway to the crash site to provide assistance. The ground party member entered the burning aircraft in an attempt to assist the pilot and third passenger. The intense fire prevented him from reaching the cockpit and he was unable to free the third passenger from the restraint belts. The fire further intensified and he withdrew through the door.
The two surviving passengers were transported clear of the crash site in the ground party member's vehicle. Fire, police and ambulance services responded to the site within minutes of the accident.
Pilot Information
The pilot held a private pilot licence with night and multi-engine ratings, as well as a group 3 instrument rating, valid until May 2010. In 2004, he acquired C-GUZZ, received initial PA-46-310P ground and flight training as well as satisfactorily completed an aircraft instrument proficiency check and flight review. He subsequently received annual recurrent ground and flight training on the PA-46-310P. Available records indicate that, at the time of the occurrence, the pilot had accumulated about 1000 hours total flight time, with about 300 hours of that in C-GUZZ.
The pilot held a category 3 medical certificate, valid until July 2010. There was no evidence of any pre-existing conditions or substances that could have affected the pilot's performance.
The pilot was considered to be thorough, cautious and conscientious, cancelling flights in response to adverse weather conditions or aircraft defects. People who flew with him described their experience as comfortable and calm. The pilot was alert and in good health and spirits on the day of the occurrence.
Pilot Spatial Orientation
Vision is the dominant sense enabling pilot spatial orientation.Footnote 2 Peripheral vision is the primary source of spatial orientation, with vestibular organs and kinesthetic sensors also contributing. In the absence of adequate visual cues, vestibular and kinesthetic illusions can occur. This ometimes results in pilot disorientation, which can lead to loss of aircraft control.
The somatogravic illusion is a type of illusion that frequently occurs after takeoff, whereby the pilot incorrectly perceives the aircraft to be pitching nose up. This illusion is corrected by vision when adequate visual cues exist; however, when visual cues are not adequate, the pilot may respond to the illusion by excessively lowering the nose of the aircraft.
In this occurrence, the flight was taking off toward the northwest and, although the sun had set, the sky was still illuminated and the horizon was well-defined. The aircraft rolled rather than pitched, which would have been the case had the pilot been lowering the nose in response to the influence of a somatogravic illusion. It is, therefore, unlikely that the pilot was suffering from disorientation.
Weather
The aviation routine weather report (METAR) for Saskatoon at 1400 was as follows: wind 320° True (T) at 15 knots with gusts to 25 knots and visibility 15 statute miles (sm).
The nearest location providing aviation weather reports is Yorkton, Saskatchewan, located about 28 nautical miles (nm) southwest of Kamsack. The 2100 METAR for Yorkton was as follows: wind 300°T at 12 knots with gusts to 17 knots, visibility 9 sm, clear sky, temperature 21°C and altimeter setting 29.72 inches of mercury (in Hg). Similar conditions prevailed at Kamsack. A photograph taken of the accident scene showed the wind at Kamsack was about 300°T at 10 to 15 knots.
Sunset occurred in Kamsack at 2054, with the end of civil twilight at 2137. A photograph taken at 2120 showed that the sky condition at Kamsack was scattered high clouds with good visibility. Sufficient sky illumination remained to provide a distinct horizon reference through 360°. Weather is not considered a factor in this occurrence.
Aerodrome Information
Kamsack (CJN2) is a registered aerodrome operated by the Town of Kamsack. With an asphalt surface, runway 16/34 is 1510 feet above sea level (asl), 2500 feet long and 75 feet wide. The aerodrome lighting is controlled by Type J aircraft radio control of aerodrome lighting (ARCAL) and was not activated for the takeoff.
Weight and Balance
It could not be determined whether the pilot made any weight and balance calculations for the occurrence flight. The aircraft's maximum allowable takeoff weight was 4100 pounds. Transportation Safety Board (TSB) investigators calculated the Kamsack takeoff weight to be 4097 pounds, with the centre of gravity at 145.24 inches aft of datum. This weight and centre of gravity were within the limits specified in the PA-46-310P Pilot Operating Handbook (POH).
Aircraft Performance
Based on prevailing weather conditions, TSB investigators calculated that the flaps-retracted takeoff would require a ground run of 1800 feet on a paved, level and dry runway.
Flight Duration and Roll Rate
Investigators calculated the duration of the flight, from takeoff to impact, was approximately 7 seconds. The aircraft would have rolled at an average of about 6° per second to reach a bank angle of 45°, and about 13° per second to reach a bank angle of 90°.
Propeller Torque
Propeller-driven aircraft are affected by propeller torque, which is an aerodynamic force in the direction opposite to propeller rotation. The propeller torque effect is greatest at high power settings and low airspeeds. The PA-46-310P will not produce enough propeller torque to roll the aircraft while on the runway. However, the propeller torque produced will cause the left wheel to exert more force on the runway than the right wheel, resulting in some drag. This can induce a yaw to the left while on the ground. The propeller on the PA-46-310P rotates clockwise when viewed from the cockpit and, once the aircraft is airborne, propeller torque will cause the aircraft to roll to the left in the absence of countering aerodynamic control forces, produced by the ailerons in response to pilot control inputs. The aircraft is designed such that aileron controls can easily counter propeller torque throughout the normal operating speed range.
Propeller Slipstream
A propeller produces a helically shaped slipstream of accelerated air. The PA-46-310P propeller slipstream rotates clockwise, looking forward from the tail of the aircraft, striking the left side of the empennage, and will cause the aircraft to yaw to the left in the absence of countering aerodynamic control forces produced by the rudder in response to pilot control inputs. This effect is greatest at high power settings and low airspeeds, such as during takeoff, and is easily countered by the pilot's application of opposite rudder and use of rudder trim.
P-Factor
P-factor results from asymmetric propeller loading, whereby the descending blades have a higher angle of attack and produce more thrust than do the ascending blades, and causes the aircraft to yaw to the left. This effect is greatest at high power settings and high angles of attack, and, at normal operating speeds, is easily countered by the pilot's application of opposite rudder and the use of rudder trim. Aircraft with tricycle landing gear, such as the PA-46-310P, are affected less by P-factor during the takeoff run than are tail-dragger aircraft. However, when the PA-46-310P is rotated for takeoff, the angle of attack and the P-factor effect both increase.
Lateral Stability
The aircraft is designed with 4.5° wing dihedral to provide lateral stability, which will result in the aircraft rolling in response to yaw. While a large yaw angle would be required to produce a roll rate, such as the one that occurred in this accident, the ailerons should provide sufficient authority to counter this roll under normal operating conditions.
Aircraft Information
C-GUZZ was manufactured in 1985 by the Piper Aircraft Corporation. It was modified on 20 March 2001, when a new Continental engine (model TSIO-550-C) was installed, in accordance with Supplemental Type Certificate (STC) SA00380AT. It was again modified on 26 July 2001 with the installation of a new MT-Propeller 4-blade propeller (model MTV-14-D/195-30a), in accordance with STC SA01542AT. The aircraft was manufactured with a hydraulic flap actuator and was later modified with the installation of an electric flap motor-actuator, which was used on later model PA-46-310P aircraft. The aircraft was imported into Canada in August 2004 with 3767 hours total time since new (TTSN).
Examination of the aircraft's maintenance records indicated that the aircraft was being maintained in accordance with approved procedures for a privately-registered aircraft. At the time of the occurrence, there were no reported defects. The aircraft's most recent 100-hour or annual inspection had been conducted on 30 August 2008, at 4059 hours TTSN; the next annual inspection was due on 30 August 2009. The final entry in the airframe technical log was dated 09 January 2009, at 4077 hours TTSN. The date of the final entry in the aircraft journey log was burned away, with 4083 hours TTSN recorded. Based on previous aircraft usage by the pilot, the aircraft TTSN was likely about 4110 hours at the time of the accident.
The aircraft was refuelled with 76 litres of 100LL aviation gasoline before departing Saskatoon. The aircraft was not refuelled in Kamsack. TSB investigators calculated that, at takeoff from Kamsack, the aircraft had about 223 litres of usable fuel. Fuel distribution between the wing tanks could not be determined.
Involved in two known previous occurrences, the aircraft was initially registered in the United States as N26033. The first occurrence was on 11 February 1987 during a flight from Alaska to Europe (TSB report A87W4901). A ferry fuel system had been installed and, during transfer of fuel from the fuselage tank to the wing tanks, the left wing was damaged. The aircraft made a precautionary landing at Mould Bay, Northwest Territories, and remained at Mould Bay until it was repaired and returned to service. The second occurrence was on 16 March 1991, during a flight from Florida to North CarolinaFootnote 3. The aircraft descended out of control from about FL183Footnote 4 to about 3000 feet asl and sustained damage to rivets, the elevator trim tab and the right wheel well door. The aircraft was subsequently repaired and returned to service.
For a normal takeoff, the PA-46-310P POH recommends that the flaps be in the retracted position, with takeoff after accelerating to 77 knots indicated airspeed (KIAS) and landing gear retraction when a straight-ahead landing on the runway is no longer possible. For short or soft field takeoff, the POH recommends flaps be set to 20°, with takeoff after accelerating to 70 KIAS, landing gear retraction after accelerating to 74 KIAS and flap retraction at 110 KIAS, if obstacle clearance is not a factor.
The PA-46-310P is not equipped with control-surface locks. The POH recommends that "the aileron and elevator controls should be secured by looping the safety belt through the control wheel and pulling it snug." While the investigation could not determine whether the occurrence pilot used this method to secure the controls at Kamsack, he was known to regularly use this method. Due to the fact that the pilot and passengers were all wearing their seat belts at the time of the accident, the controls could not have been locked.
The POH states, as part of the before takeoff check, that the pilot must "ensure proper flight control movement and response." The investigation could not determine whether the pilot had conducted this check.
The aircraft manufacturer has issued several service bulletins and letters applicable to PA-46-310P flight control cables and aileron control systems. Compliance with service bulletins and letters is not mandatory, unless they are accompanied by an airworthiness directive.
- On 31 January 1989, Piper issued service bulletin (SB) 863A to mitigate chafing of aileron cables against flap track brackets by installing phenolic fairleads at the flap tracks. Records show that the occurrence aircraft was compliant with this service bulletin on 19 February 1990.
- On 30 November 1994, Piper issued service letter (SL) 1012 recommending the replacement of stainless steel aileron cables with galvanized steel cables to improve service life and increase the time in service between cable replacements. Field reports indicated a high replacement rate of the left and right balance cables and the left and right aft drive cables, which are predominantly located in the wing structure. The left and right forward drive cables, located in the cabin interior, did not show a high replacement rate and were not affected by the service letter. Records show that the occurrence aircraft was compliant with this service letter on 27 December 1995, as a galvanized right balance cable, a galvanized left balance cable and galvanized left and right aft drive cables had all been installed.
- On 03 January 2001, Piper issued SB 1048 applicable to many Piper aircraft types equipped with stainless steel control system cables. While the PA-46-310P was not specifically listed as one of the affected aircraft types, the SB indicated that it is possible that any Piper aircraft, regardless of model year, could have stainless steel control system cables installed. SB 1048 required inspection and lubrication to improve service life of stainless steel control cables on portions of cables passing over a pulley or through a fairlead. The bulletin indicated that the lubrication of stainless steel cables is to be accomplished on the same schedule as that of galvanized cables. However, the PA-46-310P aircraft maintenance manual did not include a lubrication schedule for either stainless steel or galvanized steel cables. SB 1048 indicated that the manufacturer would continue to offer customers a choice of either stainless steel or galvanized steel control cables as service replacements, with the approval of "mix or match" of stainless steel and galvanized steel cables on the same aircraft. The bulletin stated that installation of stainless steel control cables, as standard equipment, would be discontinued. Records show that the occurrence aircraft was compliant with SB 1048 on 26 July 2001 at 3059.1 hours TTSN. The aircraft records did not include any entries indicating subsequent, ongoing compliance with this bulletin after 26 July 2001.
- On 23 September 2008, Piper issued SB 1190, requiring inspection and maintenance of cable guards associated with the left and right aileron quadrants. Compliance with this service bulletin was not required until the next 100-hour or annual inspection, which was due in August 2009. Maintenance records do not include an entry for this service bulletin, which indicates that it had not yet been respected.
On 11 July 2001, the Federal Aviation Administration (FAA) issued special airworthiness information bulletin (SAIB) CE-01-30, alerting owners of specified Piper aircraft with stainless steel control cables about the possibility of corrosion, fraying and/or failure. It also warned of the subsequent loss of control authority that may occur due to a considerably shorter life of the stainless steel cables, as compared to galvanized cables. The SAIB list of affected aircraft types mirrored those listed in Piper SB 1048, and did not include the PA-46-310P as one of the affected aircraft types. The FAA recommended compliance with the contents of Piper SB 1048 at each 100-hour or annual inspection. This SAIB was provided for information purposes only and is not mandatory.
Aircraft records did not include any entries showing replacement of the left forward aileron drive cable, indicating the cable installed during manufacturing was still present. The manufacturer's maintenance program does not specify time limits for cable life. Cable service life is based on the condition of the cable.
Records show the flight control cables, turnbuckles, guides and pulleys were most recently inspected on 25 August 2008 during the 100-hour or annual inspection of the occurrence aircraft. No anomalies were noted. There is no record to indicate that the flight control cables were removed from the aircraft at that time for inspection purposes. A requirement of the 100-hour or annual inspection is to check the aileron system for proper condition and operation.
The Piper Maintenance Manual inspection sheet makes reference to FAA advisory circular AC43-13-1A. Part of this advisory circular provides guidelines for cable lubrication. The inspection involves checking for lost motion between the control wheel and aileron, resistance to control wheel rotation, control wheel synchronization, neutral alignment with the ailerons, proper travel and contact with the control stops. If any of the above criteria are not met, then the control system must be rerigged, which would involve readjusting the cable tension.
The last recorded tensioning of the aileron control system cables was on 08 April 2003 at 3570.6 hours TTSN.
Automatic Flight Control System
The aircraft was equipped with a King KFC150-series 3-axis automatic flight control system (AFCS), in accordance with STC SA1778CE-D. Information regarding the operation of this system is provided in the FAA-approved airplane flight manual supplement, revision 4, dated 14 August 1992. The AFCS autopilot component operates in pitch and roll axes, while the yaw damper component operates in the yaw axis. The supplement includes limitations, which indicate that the autopilot and yaw damper must be off during takeoff and landing and that a pre-flight test of the system must be successfully completed prior to each flight. The latter portion of the test procedure requires that the autopilot and yaw damper be engaged, the flight controls be manually moved in all axes to verify that the autopilot and yaw damper can be overpowered and the autopilot disconnect/trim interrupt switch on the pilot's control wheel be pressed to verify that the autopilot and yaw damper disconnect.
The maximum bank angle commanded by the KFC150 system in the PA-46-310P is 20°. The autopilot was certified so as not to exceed maximum short term forces of 30 pounds in roll and 50 pounds in pitch at the aircraft maximum certified airspeed. Basic aircraft control forces increase with airspeed; therefore, forces required to overpower the autopilot at takeoff speeds would be lower.
While the yaw damper is required to be off for takeoff, the aircraft should still be controllable with the yaw damper on. When it is on, the pilot would likely sense increased rudder pedal forces. If the pilot were to exert sufficient force on the rudder pedals, the yaw servo would disengage, and it is possible the aircraft could then yaw in response to the pilot's rudder input.
Wreckage and Impact Information
The first point of impact was about 200 feet to the left of the runway in an open, level field. The left wing tip collided with the ground first, followed by the propeller and the nose of the aircraft. The axis of the impact trail was 294° Magnetic (M) and extended about 110 feet from the first point of impact to the main portion of the wreckage. The fuselage of the aircraft came to rest inverted on a heading of 030°M about 300 feet to the left of the departure end of runway 34.
The fuel tanks in the left wing were torn open during the impact with the ground. The subsequent fuel-fed fire consumed about 60% of the aircraft, leaving only the empennage and the outer left wing unburned.
Examination of the engine revealed no indications of any pre-impact anomalies. The propeller blade damage indicates that the propeller was rotating at high speed and the engine was developing substantial power at impact.
The left wing separated from the fuselage at the forward and aft spar fittings. The outboard section of the wing separated from the inboard section, just outboard of the main spar wing splice. According to the TSB Laboratory's examination of the spar fittings and fractures of the wing spars, the wing separations resulted from impact-related overstress.
All wing flap surfaces were present at the crash site. Impact and fire damage to the flaps, bell cranks and push-pull rods obscured information regarding the flap position at impact. The flap motor-actuator position was consistent with a flaps-retracted configuration.
The landing gear was in the down and locked position.
Most of the AFCS components were destroyed by the fire, and investigators could not determine whether either the autopilot or yaw damper was engaged at the time of the accident.
Impact and fire damage to the flight control systems was extensive. The cockpit control quadrants were destroyed by fire. All flight control surfaces remained attached to the aircraft; all damage to the surfaces was the result of impact forces and the post-impact fire.
As a result of the post-impact fire, the forward rudder cable attachments separated from the rudder quadrant sector in the cockpit. The rudder cross bar in the cockpit was recovered. Both rudder cables were found loose in the wreckage with their ball-end attachments intact. The rudder cables were intact from the ball-ends to the rudder sector control attachment at the rudder. The inverted aircraft was resting on the rudder horn, and the rudder could not be moved. The yaw servo cables were attached to the yaw servo drum and maintained tension at the rudder sector assembly. The rudder trim bungee and worm/follower assemblies were recovered. The rudder trim was set slightly nose-right of neutral.
The elevator and rudder cables, as well as and the pitch and yaw servo cables, were all intact. The elevator trim actuator was intact, and the elevator trim was set to a neutral position, indicating an electric trim runaway had not occurred. The roll servo was substantially damaged by the fire. The aileron-rudder interconnect was substantially damaged by the fire and surviving steel interconnect components remained loosely assembled over the left forward aileron and left forward rudder drive cables. Resolidified aluminum residue was found in all locations where aluminum components had existed. The interconnect was likely intact and functioning normally during the occurrence flight.
All aileron cable components were present in the wreckage. Fractures in the aileron control cable system were identified at three locations:
- the galvanized steel, left aft aileron drive cable was fractured at the left outboard flap track;
- the galvanized steel, left aileron balance cable was fractured at a point that would have been just inside the fuselage adjacent to the left wing root; and
- the stainless steel, left forward aileron drive cable was almost totally fractured at a point 40 inches from the cable ball-end attachment to the left aileron quadrant assembly (see Appendix A — Aileron Cable System Schematic).
TSB Laboratory examination of the left aft drive cable and left balance cable fractures concluded that they had resulted from impact-related overstress.
Left Forward Aileron Drive Cable
In addition to the fracture at the 40-inch point, the left forward aileron drive cable was found to have some broken wires at the 18, 23 and 27 inch locations, which correspond to pulley locations beneath the instrument panel. Due to cyclic bending stresses, fatigue in cables tends to occur at pulleys.
The 40-inch location was beneath the cockpit floor within a cavity between two bulkheads. The cable passes through lightening holes in the bulkheads, which are equipped with nylon caterpillar grommets that are glued into place for cable protection. The grommets must be checked periodically because, along with the glue, they can become brittle with age and crack or debond. Under proper cable tension, the cable routing is designed to provide sufficient clearance to prevent the cable from contacting the bulkheads or grommets. Cable tension can vary with time and temperature, and must also be checked periodically. The cavity between the bulkheads does not contain any other known components. Control wheel movement from left to right aileron stops causes the cable to move about 2.5 inches.
Displaced away from the fracture location, some cable strands and splayed wires were found at the forward end of the fracture at the 40-inch location. The aft end of the fracture was roughly cone-shaped (see Figure 1).
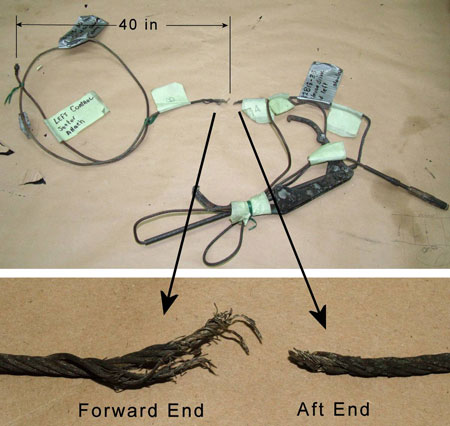
The cable fracture surfaces had deposits of solidified molten material. The forward and aft fracture surfaces were held together by re-solidified metal and a few embrittled wires, which separated during initial handling. Exposure to the post-impact fire had corroded and sooted the cable, destroying all non-ferric material near the cable fracture.
The TSB Laboratory examined the fractured cable ends using a scanning electron microscope. Some wires exhibited localized indentations, suggestive of crushing or pinching. None of the wires had been flattened by abrasion against other objects. Examination of representative solidified molten metal revealed the presence of aluminum and stainless steel, likely from surrounding aluminum aircraft structure and the aileron cable itself. Wire fracture faces included flat square surfaces, indicative of cleavage fracture of embrittled wires during post-occurrence handling, surfaces with dendritic features, indicating they had been subjected to melting, and some flat square surfaces covered in heavy oxidation from the fire, but without dendritic features indicative of melting.
It is highly improbable for a wire to fracture in a brittle manner during a fire, asthe hot metal would flow plastically, resulting in a necked tip. Therefore, it is likely that the wires with the flat square surfaces covered in heavy oxidation were fractured before they were exposed to the fire.
Due to the fact that the wires had been embrittled by the fire, any bending of the wires during wreckage recovery likely would have resulted in their brittle fracture. Therefore, it is improbable that the splaying could have occurred during wreckage recovery. Although this splaying may have occurred during the break-up of the aircraft, it is possible that it was present before the occurrence as a result of progressive damage. The splaying of portions of the forward end of the cable is indicative of cable travel restriction. The presence of flat square fracture surfaces with an oxide layer is considered to be direct evidence that some of the wires had pre-existing progressive fractures. However, the features on the cable fracture surfaces were substantially obliterated by the post-impact fire, and it could not be established that fatigue caused the partial cable fracture.
Analysis
The pilot was healthy and qualified. With 300 hours on C-GUZZ accumulated over 5 years, he would have been familiar with its operation and performance. The aircraft had no known defects and was operating within weight and balance limits. The runway was suitable for a normal takeoff, and weather conditions were benign. The pilot was known to be cautious and thorough; it is unlikely he deliberately operated the aircraft outside normal operating parameters.
The investigation could not identify a reason why the aircraft rolled to the left after takeoff. Consequently, a number of hypotheses were considered and are discussed below.
Yaw Effects
Propeller torque, propeller slipstream and P-factor are all reasons for the aircraft to yaw to the left during the takeoff roll. Such a yaw is a normal aircraft characteristic and can be countered by pilot control inputs.
If the aircraft yaws, lateral stability will result in the aircraft rolling in the direction of the yaw. The investigation considered various factors that could cause the aircraft to yaw, whether the pilot's ability to control various yaw effects might have been impaired as well as whether yaw could induce the roll that occurred.
The aircraft yawed to the left during takeoff from Kamsack. The response to this situation requires the pilot to perceive the yaw and make rudder inputs.
If the pilot inadvertently engages the yaw damper, increased rudder pedal forces could ensue. A sudden and unexpected disengagement of the yaw damper could also cause yaw. However, there was no indication the yaw damper was engaged during the takeoff from Kamsack.
Propeller torque, slipstream and P-factor all occur during normal aircraft operations. Individually or in combination, they could cause the aircraft to yaw to the left on the runway. These factors are easily controlled under normal conditions by using the rudder trim and rudder. If the yaw damper was not engaged and the rudder system operated normally, it is possible the pilot's response slightly lagged the development of the yaw.
While no anomalies were noted on any of the rudder system components found at the site, fire damage limited examination of the yaw damper system. Therefore, no conclusion can be made regarding the functioning of the rudder system. The rudder trim was found set slightly nose-right of neutral, which would counter normal yaw to the left on takeoff.
After takeoff, propeller torque acts in the roll axis and the other factors discussed above continue to act in the yaw axis. It is possible that an aircraft yaw of unknown extent occurred after takeoff. In this situation, lateral stability will induce a rolling moment, which should be controllable with normal aileron authority, even with large yaw angles.
Rudder should provide sufficient ability to counter yaw effects discussed. Under normal conditions, ailerons should provide sufficient ability to counter any yaw-induced roll. It is considered unlikely that a significant yaw occurred to the extent necessary to induce the roll that resulted in this accident.
Flap Asymmetry
The investigation considered whether flap asymmetry during retraction could have caused the aircraft to roll to the left. Had the pilot set the flaps to 20° for a short field takeoff, the normal sequence of events after takeoff would have been to retract the landing gear first, followed by the flaps. However, the landing gear was found in the down and locked position, indicating the pilot had not initiated gear retraction before the impact. The flaps would likely not have been retracted before the landing gear. A normal takeoff is conducted with flaps retracted; the flap actuator was found in a position consistent with the flaps retracted configuration. In all likelihood, the pilot conducted a normal takeoff with the flaps retracted and no flap asymmetry occurred.
Structural Failure
The aircraft had been involved in two known previous occurrences, during which it had been damaged. The investigation considered whether structural failure of the left wing could have caused the aircraft to roll to the left. However, laboratory examination of the left wing spar failures revealed that the failures were all impact-related overstress. There was no indication of any pre-existing fatigue or other damage. It is, therefore, concluded that the aircraft's previous occurrences were not a factor in this accident.
Automatic Flight Control System
There were no known defects of the AFCS. A pre-flight test of this system must be conducted before takeoff, which the pilot did. The test requires that the autopilot and yaw damper be engaged. As such, the investigation considered whether the autopilot could have caused the aircraft to roll uncontrollably to the left if the autopilot was not inadvertently disengaged before takeoff. Yaw damper engagement was not considered to have been capable of inducing a roll of the extent that occurred between takeoff and impact.
The autopilot is designed such that it can be overpowered by the pilot. Part of the pre-flight test procedure is to operate the flight controls in all axes to verify that it can be overpowered. The aircraft is equipped with an autopilot disconnect switch on the pilot's control wheel. Had the autopilot been engaged during the takeoff, the pilot should have been able to both overpower it and quickly disconnect it with the control wheel switch. Additionally, the estimated bank angle at impact was between 45° and 90°, significantly exceeding the 20° maximum bank angle the autopilot is capable of commanding.
Had the autopilot been inadvertently engaged during the takeoff, it would not have caused the aircraft to roll uncontrollably. It is unlikely that this occurrence resulted from the autopilot being engaged before takeoff.
Left Forward Aileron Drive Cable
As the stainless steel, left forward aileron drive cable was not completely fractured, a cable separation could not have caused the accident. TSB Laboratory examination of this cable determined it exhibited signs of pre-existing progressive fractures at four locations in the cable length. Three of these fracture locations were near pulleys, where fatigue is known to occur due to cyclic bending stresses.
The fourth fracture location, at the 40-inch point, was unusual. It occurred in a straight portion of the cable with no cyclic bending stresses and did not show signs of abrasion. The forward end of the fracture included splayed and displaced wires. The splayed wires are indicative of cable wires bunching prior to the post-impact fire; however, it could not be determined whether the wire splaying occurred prior to impact or during the crash sequence.
As the splayed wires were co-located and accompanied with pre-existing progressive wire failures, it is possible that, as the progressive wire failures occurred, they became displaced from the cable. For the splaying to occur, the displaced wires would have to come into contact with a nearby object or structure. The location of the fracture was in an area under the cockpit floor near two fuselage bulkheads with lightening holes, which are equipped with nylon grommets to provide cable protection. The grommets can become brittle with age and detach; however, due to the destruction caused by the post-impact fire, it could not be determined whether such aging and debonding took place. Cable tension can change over time, allowing the cable to contact the grommet or, should the grommets become detached or worn, the bulkhead.
The last recorded tensioning of the aileron control system occurred approximately 6 years, or 540 flight hours, prior to the occurrence. The last inspection of the flight control cables was approximately 11 months, or 51 flight hours, prior to the occurrence. Had the pre-existing progressive fractures in the left forward aileron drive cable, a deteriorated cable grommet or a loose aileron cable existed at the time of the last inspection, it would likely have been identified.
There are no known obstructions in the area between the bulkheads. However, due to the extensive fire damage, it could not be determined if any unidentified obstructions existed.
The aircraft began rolling to the left at takeoff, and the roll continued until the collision with terrain. Such a roll is normally countered by pilot right aileron inputs, but for reasons undetermined, the pilot did not stop or reverse the roll. The roll was likely caused by propeller torque, which could not be countered by opposite aileron inputs.
The cable was splayed at the 40-inch fracture location. Assuming the splaying occurred prior to impact, it is possible that cable movement was restricted such that the pilot could not take effective action to counter a roll.
The POH and KFC150 flight manual supplement both require that control function checks be conducted before takeoff. The investigation could not determine whether the pilot conducted these checks. However, given the pilot's thorough and meticulous nature, it is likely that he would have conducted them. Furthermore, due to the pilot's history of cancelling flights as required for technical reasons, it is likely he would not continue the flight if the pre-takeoff control checks were done and revealed impaired aileron control function.
Service Letters and Bulletins
The manufacturer issued SL 1012, which recommended replacing some stainless steel aileron cables with galvanized steel cables. This would improve the service life and increase the time in service between cable replacements. However, the stainless steel left and right forward aileron drive cables did not show a high field replacement rate, were not affected by the service letter and were not replaced. There was no record of the left forward aileron drive cable having been replaced in the 24 years of service and 4110 hours of aircraft operation. The four pre-existing fracture locations identified on the cable indicate that the cable had reached or was nearing the end of its service life.
The manufacturer issued SB 1048, which recommended lubricating the stainless steel control cables where they pass over a pulley or through a fairlead. This would prevent wear and maintain service life. Additionally, the FAA issued SAIB CE-01-30, recommending compliance with Piper SB 1048 at each 100-hour or annual inspection. The FAA was concerned about the possibility of corrosion, fraying and/or failure, as well as subsequent loss of control authority that may occur due to a considerably shorter life of the stainless steel cables, as opposed to galvanized cables.
However, SB 1048 and CE-01-30 were not associated with an airworthiness directive and compliance with them was not considered mandatory. Additionally, while the bulletins' content makes them relevant to the PA-46-310P, this model was not specifically mentioned in either bulletin's list of affected models.
Consequently, the inspection and cable lubrication recommended by SB 1048 and SAIB CE-01-30 was last carried out on the occurrence aircraft approximately 8 years, or 1050 flight hours, prior to the accident. Seeing as the PA-46-310P is not listed in the affected models and compliance with these two bulletins is not mandatory, it is likely that the maintenance action recommended had not been carried out at the 100-hour or annual inspection of other affected aircraft, as recommended in SAIB CE-01-30.
Survivability
The use of the available three-point restraint systems likely prevented the two survivors from being incapacitated, enabling them to evacuate from the burning wreckage.
The following TSB Laboratory reports were completed:
- LP 099/2009 – BlackBerry Download
- LP 103/2009 – Examination of Wing Failure
- LP 128/2009 – Examination of Aileron Cable
These reports are available from the Transportation Safety Board of Canada upon request.
Finding
Finding as to Causes and Contributing Factors
- The pilot was unable to maintain aircraft control after takeoff for undetermined reasons and the aircraft rolled to the left and collided with terrain.
Finding as to Risk
- The manufacturer issued a service bulletin to regularly inspect and lubricate the stainless steel cables. Due to the fact that the bulletin was not part of an airworthiness directive and was not considered mandatory, it was not carried out on an ongoing basis. It is likely that the recommended maintenance action has not been carried out on other affected aircraft at the 100-hour or annual frequency recommended in FAA SAIB CE-01-30.
Other findings
- Due to the complete destruction of the surrounding structure, restriction to aileron cable movement prior to impact could not be determined.
- The use of the available three-point restraint systems likely prevented the two survivors from being incapacitated, enabling them to evacuate from the burning wreckage.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .
Appendices
Appendix A — Aileron Cable System Schematic