Collision with Terrain
Robinson R22 Alpha (Helicopter) N97CP
Huttonville, Ontario
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The Robinson R22 Alpha helicopter (registration N97CP, serial number 0421) departed Toronto City Centre Airport, Ontario, on a short flight to the pilot's private helipad in the rural town of Norval, Ontario. At 2000 Eastern Daylight Time, in the hours of darkness, the helicopter crashed 1.8 nautical miles northeast of the final destination. The helicopter erupted into flames at impact and was partially consumed by a post-crash fire. The pilot was fatally injured.
Other Factual Information
History of Flight
On the evening of the occurrence, the helicopter departed Toronto City Centre Airport (CYTZ), Ontario, at 1942,Footnote 1 for a 20-minute visual flight rules (VFR) flight to the owner/pilot's residence. The pilot routinely flew this route. Recorded air traffic control radar data indicate that the helicopter departed toward the west and initially climbed to approximately 1300 feet above sea level (asl) and continued along the lake shore of Lake Ontario. It then climbed to 1500 to 1600 feet asl, approximately 1000 feet above ground level (agl), turned right and continued in a northwesterly direction toward its intended destination.
At 1958:51, the helicopter started a right turn, which was followed by a tight left climbing turn. The helicopter reached a maximum altitude of 1800 feet asl (1150 feet agl) at 1959:15 and then began to descend rapidly while continuing the left turn. Radar data ends at 1959:29, when the helicopter was at 1300 feet asl (650 feet agl).
Moments before the crash, the helicopter was heading in an easterly direction then abruptly pitched nose down and crashed into the treed swampy area one nautical mile (nm) south of Huttonville, Ontario, a small rural community within the city of Brampton, Ontario.
Helicopter Information
The Robinson R22 Alpha is a two-seat helicopter manufactured by the Robinson Helicopter Company and was certified for VFR operations only. N97CP was manufactured in 1984. The pilot had purchased and registered the helicopter in the United States in February 2009. The pilot then brought the helicopter into Canada and, although required by regulations, it had not been registered in Canada. It was insured in the United States in February 2009; however, that policy was cancelled in March 2009 by the insurer when it discovered that the helicopter was no longer based in the United States. While paragraph 606.02(8)(a) of the Canadian Aviation Regulations prohibits an aircraft owner to operate an aircraft without liability insurance, insurance was never obtained following the cancellation of the original policy.
Records indicate that the helicopter was equipped and maintained in accordance with existing United States Federal Aviation Regulations (FARs) and approved procedures. The helicopter's journey logbook was not located. Technical logbook records indicate that an annual inspection had been completed on 22 May 2009, in the United States. At that time, it had a total airframe time of 3555 hours and 1115 hours since the last overhaul. Nothing unusual was found during the inspection.
The helicopter was operated using 91 octane automotive gasoline (MOGAS). According to the aircraft type certificate, this was not a fuel approved for use in the helicopter. Supplemental type certificate (STC) SH760NE allows the use of MOGAS. There are no records at the United States Federal Aviation Administration (FAA) indicating that the STC was installed on the accident helicopter; however, aircraft records indicate that the STC was installed on 08 August 2003 and that the appropriate placards were in place indicating that the helicopter could be fuelled with MOGAS.
The helicopter was used regularly by the pilot to commute between his residence located in Norval and Toronto in the previous eight months. The number of hours flown in that period was approximately 100 hours with most flights being approximately 20 minutes in duration.
The helicopter had no known deficiencies before the flight and was being operated within its load and centre of gravity limits. The aircraft was not equipped with on-board recorders and these were not required by regulation.
Pilot Information
The pilot held a valid United States private pilot licence issued on 08 December 2008, with the rotorcraft-helicopter rating valid for day and night VFR flight. Records indicate that the pilot was certified and qualified for the flight in accordance with existing FARss. He had accumulated approximately 210 hours of total flying time, including 110 hours as pilot in command. All flying was done on Robinson R22 helicopters.
There was no indication of any physiological issues that might have contributed to the accident.
Weather
There is no official weather reporting station in Huttonville. Sunset was at 1918, the end of civil twilight at 1947, and the moon had not risen. Due to the overcast sky and limited ground lighting, the area was in total darkness. At 2000, the time of the occurrence, the aviation routine weather report for Toronto/Lester B. Pearson International Airport (CYYZ), located 8 nm east of Huttonville, was as follows: wind 130° true (T) at 4 knots, visibility 5 statute miles, mist, scattered clouds at 3800 feet agl, overcast clouds at 8500 feet agl, temperature 19°C, dew point 18°C, altimeter setting 30.11 inches of mercury.
Wreckage Examination
The crash site was located in a swampy clearing surrounded by a mixture of mature deciduous and coniferous trees ranging in height from 30 to 70 feet. The helicopter struck some of the upper branches of the taller trees during descent, consistent with a 50° descent angle. The helicopter struck the ground in an estimated 50° nose-down attitude and came to rest approximately nine feet from the initial impact point. The helicopter was substantially damaged during the impact and post-crash fire, which partially destroyed the front of the helicopter.
There were no signs of any pre-impact mechanical failure or system malfunction that could have contributed to this accident. Examination of the engine and drivetrain indicates that they were not turning at impact. Furthermore, examination of the low rotor revolutions per minute (rpm) warning lamp showed signs of stretch in the filament consistent with the lamp being illuminated at the time of impact. There was no evidence of rotor mast bumping, excessive blade coning, or main rotor blade contact with the tail boom.
The fuel mixture and carburetor heat controls are located on the centre pedestal in close proximity to each other. To aid in identification, the control knobs are shaped differently. Furthermore, the fuel mixture control knob is red while the carburetor heat control knob is black (see Photo 1). To prevent the inadvertent deployment in flight, the manufacturer's checklist directs the pilot to place a removable cylindrical plastic guard over the mixture control knob before starting the engine (see Photo 2). This guard is not to be removed until engine shutdown when the mixture control knob is pulled to the idle cut-off position (see Photo 3). This plastic guard is not permanently attached to the control panel. While the plastic guard was found at the crash site, it could not be determined whether it was used at the time of the occurrence.



The engine and fuel controls were found as follows:
- The mixture control knob was pulled out and bent back. The mixture control is a push/pull control with a push button locking feature and therefore most likely did not move at impact.
- The carburetor heat control knob was fully in (cold). The carburetor heat control is a standard push/pull control with no locking feature and may have moved at impact.
- The throttle position (connecting rod) was found in the full open position.
- The fuel selector located on the rear cabin bulkhead above and behind the left passenger seat was found in the OFF position. This likely moved to the OFF position during impact.
- The mixture arm position on the carburetor was full rich and the carburetor heat slider was partially open. Both of these likely moved during impact.
The pilot was flying from the right seat and was ejected at impact. The pilot was found approximately 26 feet from the initial impact point. The pilot's lap belt buckle was found secured. The lap belt attachments were torn out of the airframe at impact and the lap belt was found on the ground between the pilot and the wreckage. A helmet was found at the scene, but the pilot was not wearing it at the time of the occurrence.
Robinson Helicopter Company Safety Notices
Following previous accidents and incidents, the Robinson Helicopter Company had taken safety actions, issuing several safety notices (SN) to its operators to reduce the likelihood of recurrence. These are published on its website and at the back of the pilot's operating handbook (POH). Of particular relevance are the following SNs, all of which document issues that may have contributed to this accident (see Appendix A to Appendix G — Safety Notices):
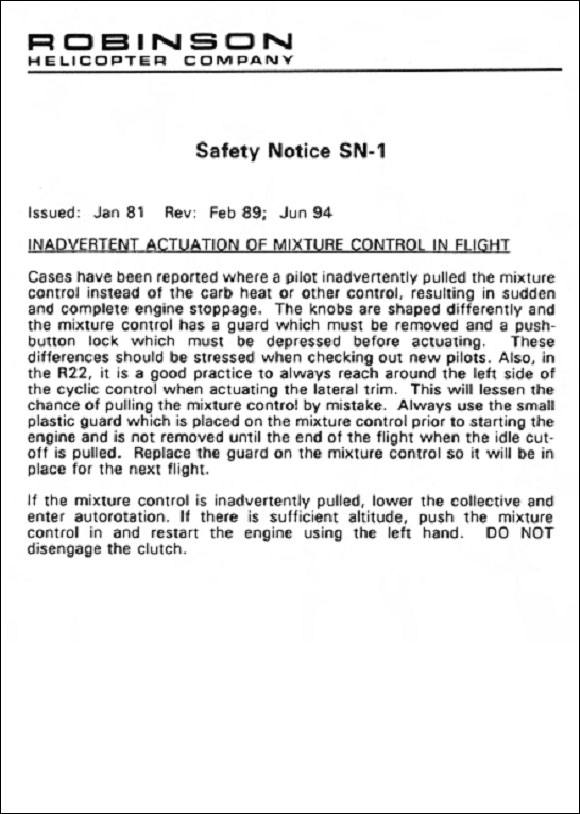
- SN-1 — Inadvertent Actuation of Mixture Control in Flight
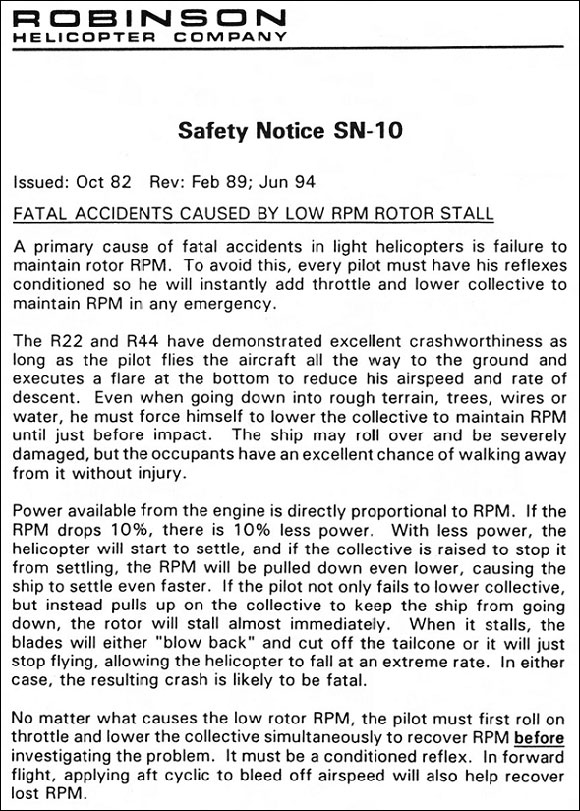
- SN-10 — Fatal Accidents Caused by Low RPM Rotor Stall
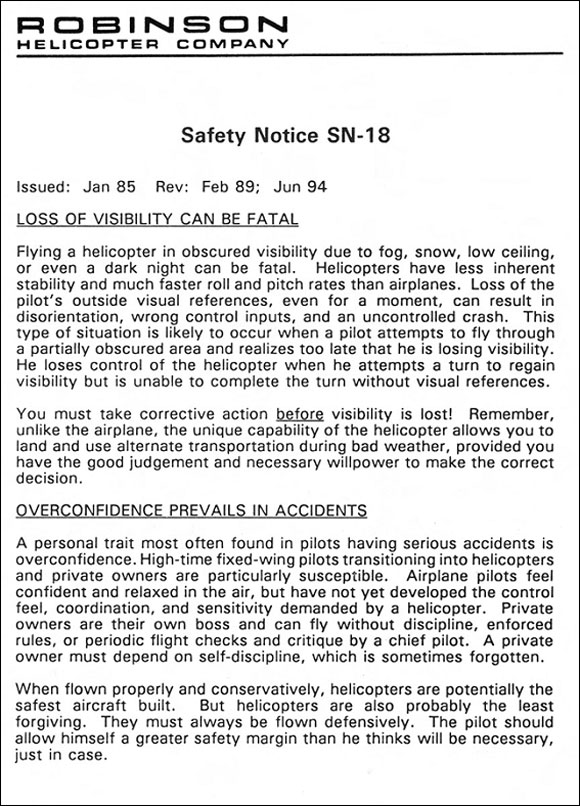
- SN-18 — Loss of Visibility Can Be Fatal and Overconfidence Prevails in Accidents
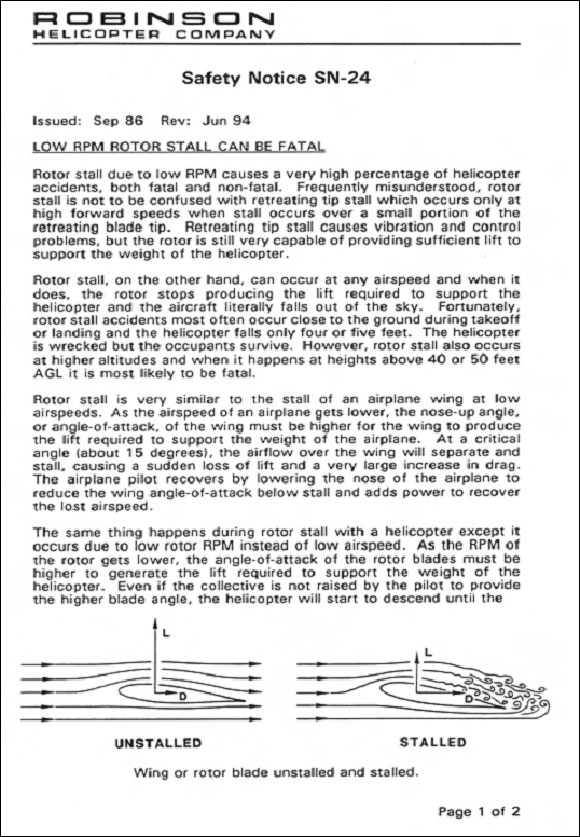
- SN-24 — Low RPM Rotor Stall can be Fatal
- SN-25 — Carburetor Ice
- SN-26 — Night Flight Plus Bad Weather Can Be Deadly
- SN-31 — Governor Can Mask Carb Ice
Emergency Procedures
The POH prescribes the following emergency procedure for a power failure above 500 feet:
- Lower collective immediately to maintain RPM and enter normal autorotation.
- Establish a steady glide at approximately 65 KIAS.
- Adjust collective to keep RPM in green arc or apply full down collective if light weight prevents attaining above 97%.
- Select landing spot and, if altitude permits, manoeuvre so landing will be into wind.
- A restart may be attempted at pilot's discretion if sufficient time is available.
- If unable to restart, turn off unnecessary switches and shut off fuel.
- At about 40 feet agl, begin cyclic flare to reduce rate of descent and forward speed.
- At about 8 feet agl, apply forward cyclic to level ship and raise collective just before touchdown to cushion landing. Touchdown in level attitude with nose straight ahead.
Carburetor Icing
Carburetor icing is a phenomenon where water vapour in the air freezes as it passes through the carburetor. When the throttle is open and the relative humidity is high, ice can form in the venturi, restricting air flow. Unchecked, this could result in either a reduction or a complete loss of power. If enough ice forms, the venturi throat can be completely blocked, causing total engine failure. When the throttle valve is closed to lower the power during a descent, ice will form at the edge of the throttle valve in the area of reduced pressure and fuel vaporization. To overcome carburetor icing, the airframe manufacturer provided a system to heat the incoming air and to prevent water condensation.
To help determine whether a flight is more or less susceptible to carburetor ice, charts based on knowledge of dry (ambient) air and wet (dew point) air temperatures have been produced. Depending on the level of severity, pilots would make use of carburetor heat more or less often to prevent ice from accumulating. These charts, however, are based on the use of aviation grades of fuel and may not apply to aircraft using MOGAS. MOGAS is more likely to cause carburetor ice because of its lower vapour point.
Unlike aeroplanes, which take off at wide open throttle, helicopters take off using only power as required, making them vulnerable to carburetor ice, especially when the engine and induction system are still cold. The Robinson R22 governor can easily mask carburetor icing by automatically increasing the throttle to maintain engine rpm, which will also result in a constant manifold pressure. Robinson Helicopter Company recommends the following:
- During takeoff, use full carburetor heat during warm-up to preheat the induction system and then apply carburetor heat as required during hover and takeoff to keep the Carburetor Air Temperature (CAT) gauge out of the yellow arc.
- During climb or cruise, apply carburetor heat as required to keep CAT gauge out the yellow arc.
- During descent or autorotation, below 18 inches manifold pressure, ignore the CAT gauge and apply full carburetor heat.
At the time of the occurrence, the meteorological conditions were conducive to moderate carburetor icing during cruise and descent on aircraft using aviation grade 100 low lead fuel.
Spatial Disorientation
All humans are susceptible to spatial disorientation. In aviation, spatial disorientation can be defined as the failure of aviators to sense correctly the position, motion, or attitude of their aircraft or themselves with respect to the earth's surface and gravity.
According to FAA documentation,Footnote 2 spatial orientation defines our natural ability to maintain our body orientation and/or posture in relation to the surrounding environment (physical space) at rest and during motion. Humans generally maintain spatial orientation on the ground. The three-dimensional environment of flight is unfamiliar to the human body, creating sensory conflicts and illusions that make spatial orientation difficult, and sometimes impossible to achieve. Statistics show that, between 5 and 10 per cent of all general aviation accidents can be attributed to spatial disorientation, 90 per cent of which are fatal.
Analysis
The sole occupant of the helicopter was fatally injured in the accident. There were no witnesses to the final moments of the flight and there were no on-board recording devices to assist investigators. Examination of the helicopter engine indicates that it was not running at impact and that the helicopter struck the ground in a 50-degree nose-down attitude suggesting an in-flight loss of control. Although the helicopter was extensively damaged, there were no signs of any pre-impact mechanical failure or system malfunction that could have contributed to this accident. As a result, this analysis focuses on possible scenarios for what caused the engine to stop running and why the helicopter departed controlled flight and collided with terrain.
While it was not possible to determine accurately the position of the carburetor heat control before impact, the mixture control knob was found out and bent. With the push button locking feature, it is unlikely that the mixture control moved during the impact. It was, therefore, likely in the idle cut-off position at impact.
Two scenarios were considered why the pilot inadvertently pulled the mixture control to the idle cut-off position, causing the engine to shut down:
- On approaching destination and in preparation for descent, the pilot attempted to apply carburetor heat.
- The meteorological conditions were conducive to moderate carburetor icing during cruise and descent. The Robinson R22 governor can easily mask carburetor icing by automatically increasing the throttle to maintain engine rpm, which will also result in a constant manifold pressure. It is possible that the helicopter's engine developed carburetor ice en route, causing performance degradation or a total power loss. To correct this situation, the pilot would have attempted to apply carburetor heat.
The mixture control knob is shaped differently than the carburetor heat knob. To reposition the mixture control, the pilot needs to action the push button locking feature. In addition, to prevent its inadvertent actuation, the manufacturer also requires that a cylindrical plastic guard be placed over the mixture control knob, from the time the engine is started until such time as the engine is shut down. This plastic guard would make it difficult to inadvertently action the mixture control and would also provide tactile feedback that the pilot was attempting to move the wrong control knob. In order for the pilot to be able to pull the mixture control knob to the idle-cut off position, it is likely that the plastic guard had not been placed over the mixture control knob as required.
In the Robinson R22, the pilot must take immediate action following a loss of power to ensure that rotor rpm is maintained. Failure to do this can lead to a low rotor rpm and rotor stall from which recovery may not be possible. The Robinson R22 POH emergency procedures for a power loss above 500 feet in part instructs the pilot to immediately lower the collective to maintain rotor rpm and enter a normal autorotation. A restart may be attempted at the pilot's discretion if sufficient time is available. If unable to restart, the pilot should turn off unnecessary switches and shut off the fuel.
Approximately 40 seconds before the crash, the helicopter started to turn to the right, then immediately started turning sharply to the left and climbed 300 feet. Approximately 20 seconds before the crash, the helicopter began a rapid descent from 1800 feet asl to the crash site at 650 feet asl; this equates to a descent rate of approximately 3450 feet per minute. According to Robinson Helicopter Company Safety Notices SN-18 and SN-26, helicopters have less inherent stability and much faster roll rates than aeroplanes. Loss of the pilot's outside visual references, even for a moment, can result in spatial disorientation, wrong control inputs and an uncontrolled crash.
With a lack of visual reference at night, limited visibility due to weather and the pilot's relative inexperience, the pilot likely became spatially disoriented while dealing with the power loss emergency. Unable to determine the correct attitude of the helicopter without visual reference, the pilot lost control, resulting in uncontrolled flight into the terrain.
The following TSB Laboratory reports were completed:
- LP 144/2009 – Instrument Examination
- LP 145/2009 – Radar Data Analysis
These reports are available from the Transportation Safety Board of Canada upon request.
Findings as to Causes and Contributing Factors
Findings as to causes and contributing factors
- It is likely that, while attempting to apply carburetor heat, the pilot inadvertently pulled the mixture control knob to the idle cut-off position, causing the engine to shut down.
- It is likely that the plastic guard had not been placed over the mixture control knob, resulting in the pilot being able to pull the control to the cut-off position.
- Following the engine shutdown, the rotor rpm was allowed to decay, resulting in a loss of control and uncontrolled flight into the terrain.
- With few visual references, the pilot likely became spatially disoriented, contributing to the inability to maintain control.
Other findings
- The helicopter was being operated in Canada without liability insurance, as required by Canadian Aviation Regulations (CARs).
- The helicopter had not been registered in Canada as required by CARs.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .
Appendices