Decrease in rotor speed followed by collision with terrain
Robinson R44 II (Helicopter) C-GDSF
Montréal, Quebec
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Synopsis
The Robinson R44 II ENG (Electronic News Gathering) helicopter, privately operated by Groupe TVA Inc. (registration C-GDSF, serial number 10750) departed from Montréal (Mirabel) International Airport, Quebec, at approximately 0705 Eastern Standard Time, with the pilot and a reporter onboard for a flight above the Montréal metropolitan area under visual flight rules. At 0724, the helicopter was north of the Champlain Bridge at 1100 feet above sea level flying in a north easterly direction along the St. Lawrence River when its rotor speed dropped below the specified limits. The pilot advised the controller at Montréal (Pierre Elliott Trudeau) International Airport that he was making an emergency landing at Mel's Studios. The helicopter descended rapidly and landed hard in a ditch located between Mel's Studios and the Bonaventure Expressway. The helicopter was found lying on its left side and severely damaged. Both occupants suffered serious injuries.
Factual information
History of the flight
Before takeoff, the pilot completed a walk-around inspection of the helicopter. He checked all systems described in the Pilot Operating Handbook (POH). No anomalies were identified.
Radar dataFootnote 1, voice recordings from Air Traffic Services and a video recording taken from a camera located in the nose of the aircraft were used to recreate the flight path of the helicopter. At 0705Footnote 2 the aircraft took off from Montréal (Mirabel) International Airport, Quebec, with the pilot and a reporter onboard for a routine flight that involved transmitting television images of current news events in the Montréal metropolitan area. The helicopter climbed to 1300Footnote 3 feet above sea level (asl) and headed southeast. At approximately 0712, it entered the Montréal (Pierre Elliott Trudeau) International Airport control zone and was authorized to proceed to the Mercier Bridge. After circling the Mercier Bridge, the aircraft headed in a northeasterly direction at approximately 1100 feet asl following the north shore of the St. Lawrence River.
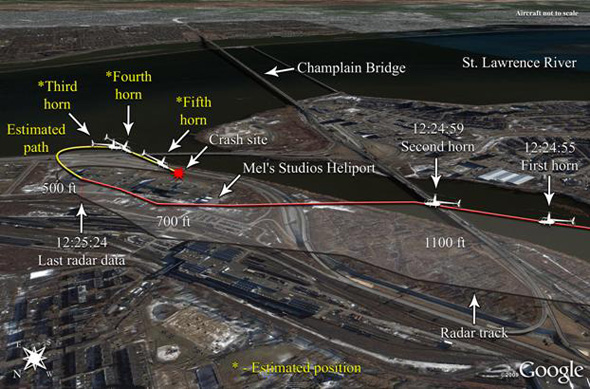
At 0724:55, just east of the Champlain Bridge, the first of 5 low rotor speed warning horns sounded and the engine began to overspeed. At 0725:17, while at an altitude of approximately 650 feet asl, the pilot informed the controller that he was making an emergency landing at Mel's StudiosFootnote 4. The aircraft was then somewhat north of the heliport at Mel's Studios. At approximately 500 feet asl, the pilot executed a 180° turn to the right. During the final moments of the flight, control of the aircraft's pitch and rollFootnote 5 response was sluggish and almost non-existent. The helicopter crashed in a ditch located between Mel's Studios and the Bonaventure Expressway (see Figure 1).
Weather conditions
Visual flight meteorological conditions prevailed during the flight and at the time of the accident. According to the METARFootnote 6 for 0700 issued at Montréal (Pierre Elliott Trudeau) International Airport, Quebec, the wind was blowing from the west at 6 knots, visibility was greater than 15 miles, the ceiling was broken cloud at 11 000 feet above ground level (agl), the outside temperature was −13°C and the dew point was −19°C.
Pilot information
At the time of the accident, the pilot was qualified on the Robinson R22, Robinson R44, Hughes 500, Bell 206, Bell 427, Bell 430 and Eurocopter AS350. He had approximately 2400 hours of total flight time on helicopters, of which about 1000 hours were on the Robinson R44, including 163.5 hours at the controls of C−GDSF. The pilot's most recent pilot proficiency check (PPC) on the Robinson R44 was completed in June 2002 with a Transport Canada inspector.
In March 2006, the pilot received flight training on the Robinson R44 at Passport Hélico in the presence of the chief instructor. The pilot performed autorotations and reviewed emergency procedures. That same month, he became the relief pilot for Groupe TVA Inc. Records do not indicate any additional training. In May 2007, while flying C-GDSF, the pilot was forced to make an emergency landing at the Mel's Studios heliport, owing to a broken engine valve.
In September 2009, he became a regular pilot on C-GDSF, flying the helicopter one day a week and as required to meet business needs. The aircraft log book confirmed that the pilot had flown 37. 3 hours in the 90 days preceding the accident, with 20.5 of the hours flown in the preceding 60 days and 5 hours in the preceding 30 days. This was his first flight in a week.
A review of the pilot's work schedule, flight times, flight duty times and rest periods make it possible to rule out fatigue as a factor in the accident. The investigation revealed that the pilot was well rested before going on duty.
Helicopter information
The Robinson R44 was certified in accordance with Chapter 527 of the Canadian Aviation Regulations (CARs). The C-GDSF was imported into Canada in July 2005, with 35 hours in service. As part of the importation process, it received its certificate of airworthiness on 08 July 2005. At the time of the accident, the helicopter had logged 2103 flying hours.
The Electronic News Gathering (ENG) version of the Robinson R44 is a turnkey aviation platform designed to transmit back to the TV studio video images captured by the helicopter's belly camera (see Photo 1), along with audio from the occupants. The R44 ENG is a three-seater helicopter with a two-bladed single rotor and fuel injected piston engine (Lycoming I0-540-AE1A5). It also features a 28-volt electrical system, a spotlight, a communication system, a gyro−stabilized nose-mounted infrared camera and a main battery located on the underside of the tail boom to offset the weight of the camera.

The helicopter must be overhauled after 2200 hours in service or 12 years. The overhaul involves replacing most major components, including the engine. By 08 June 2009, C−GDSF had accumulated 1900 operating hours and the owner opted to have the overhaul done at a Transport Canada approved aircraft maintenance organization (AMO), which is also an authorized service centre for Robinson. The overhaul took place between June and August 2009.
Although the CARsFootnote 7 do not require the owners of private aircraft to follow the manufacturer's maintenance recommendations for their equipment, Groupe TVA Inc. had decided to maintain its helicopter in accordance with the standards applicable to commercially operated aircraft. The maintenance records and logs show that the helicopter was certified, equipped and maintained in accordance with approved procedures.
No anomalies were recorded in the log books prior to takeoff.
The helicopter was examined on 02 February 2010 in the presence of representatives from Robinson (the manufacturer), Avco Lycoming (the company that built the engine), the helicopter owner, and the Minister of Transport.
After the helicopter was dismantled, certain components were shipped to the manufacturer for examination on test stands. Examination of these components did not reveal any anomalies.
The helicopter was equipped with a Kannad Model 406−AF emergency locator transmitter (ELT). The switch was in the armed position (ARM) and the Rescue Coordination Centre received a signal notification at the time of the accident. The ELT activated upon impact.
C-GDSF was equipped with a Garmin GPSmap 696 GPS that records navigational data such as time, ground speed, and geographic coordinates and aircraft altitude during flight. However, the navigational data recording capability had been deactivated.
Robinson R44 characteristics and emergency procedures
The Robinson R44's main rotor is considered a low-inertia rotor system. This type of rotor has a tendency to deplete its stored energy quickly, leading to the decay of main-rotor RPM (Nr). Engine power is transmitted to the main rotor through a belt system, with the engine and transmission engaged through progressive tensioning of the belts. When the main rotor ceases to be driven by the engine, the pilot must quickly lower the collective to compensate for the rapid decay in Nr and ultimately prevent an aerodynamic stall of the main rotor.
Loss of power
A loss of power can result from engine failure or a failure of the drive system. Normally, this would be indicated by activation of the low Nr warning horn. Indications of a drive system defect include unusual noises or vibrations, right or left yaw or a reduction in Nr concurrent with an increase in engine speed.Footnote 8
Autorotation
Autorotation permits a helicopter to descend in a controlled manner after engine power loss or other catastrophic mechanical failure and still permits the pilot to carry out a safe landing. A critical aspect of autorotation is the entry manoeuvre immediately following the loss of engine power because the pilot must react quickly to conserve rotor RPM. Of the other factors affecting autorotative flight, the existence of sufficient altitude at the time of the loss of engine power is critical to a successful descent and landing. The no-engine landing after an autorotative descent is a challenging manoeuvre for any pilot since it involves skills not frequently practiced.
Following a loss of engine power, the pilot must lower the collective pitch control full down in an effort to prevent loss of Nr and obtain sufficient airflow to turn the main rotor. During flight, the engine provides the power needed to drive the rotors. When the engine fails or the clutch system suffers a mechanical breakdown, some other force must be used to drive the rotors so that the flight can descend safely to the ground. This force, generated when sufficient air flows through the main rotor during descent to overcome blade drag, is provided by the potential energy stored by the helicopter. In other words, as the helicopter's altitude decreases, potential energy in the form of loss in altitude is traded off to place kinetic energy in the rotor system.
The Robinson R44 POH describes, as follows, the recommended procedure for an autorotation at an altitude greater than 500 feet agl:
- lower collective immediately to maintain main rotor RPM and enter normal autorotation;
- establish a steady glide at approximately 70 KIAS;Footnote 9
- adjust collective to keep rotor RPM in the green arc (or lower the collective completely if the weight of the helicopter prevents the pilot from attaining more than 97% RPM);
- select landing area and, if altitude permits, maneuver so landing is into wind;
- at 40 feet agl [above ground level], begin cyclic flare to reduce rate of descent and forward airspeed;
- at 8 feet agl, apply forward cyclic to level the ship and raise collective before touchdown to cushion the landing. Touchdown in a level attitude with the nose straight ahead.
Configuration for maximum glide distance
- Approximate speed: 90 KIAS.
- Approximate Nr: 90%.
- The best glide ratio is approximately 4.7:1 or one nautical mile for 1300 feet agl.
Configuration for minimum rate of descent
- Approximate speed: 55 KIAS.
- Approximate Nr: 90%.
- The minimum rate of descent is approximately 1300 feet/minute. The best glide ratio is approximately 4:1 or one nautical mile for 1500 feet agl.
A warning published in the POH (see Figure 2) requires that the rotor RPM be increased to a minimum of 97% when below 500 feet agl.
Risks associated with a low Nr
During autorotation, the Nr decreases as the collective pitch increases. The increased pitch very temporarily increases the lift and reduces the Nr. The decreased Nr quickly produces a reduction in lift and a faster descent. A low Nr can lead to a loss of control.
A warning published in the POH cautions against the risk of having the rotor RPM drop below 80% (see Figure 3).
To highlight the dangers associated with main rotor stalls, the Robinson Helicopter Company issued Safety Notice SN-24 (see Appendix A) in September 1986. The notice states that a very high percentage of accidents are caused by main rotor stall due to low rotor RPM.
The Robinson R44 has a single warning horn that activates when the rotor RPM is low. The warning horn sounds and a LOW RPM amber caution light (see Photo 2) is illuminated to indicate that rotor RPM has fallen below the established 97% safe limit. The horn stops and the amber caution light is extinguished when:
- rotor RPM reaches safe limits;
- the collective is fully lowered.
During the pre-flight checks on the morning of the occurrence, the warning horn and light were working normally.
The green arc for safe operation of main rotor RPM, with engine stopped is between 90% and 108%. The "danger" area on the RPM gauge is 90% RPM and is indicated by a red line. The danger of low rotor RPM leading to a main-rotor aerodynamic stall during autorotation is covered during ground school.
The throttle is located on the collective lever. When the throttle is rolled to increase engine power, the governor takes over at 80%, advancing automatically until the required power is obtained. During power changes, the throttle moves constantly and therefore pilots learn how to keep minimal pressure on it with two fingers, while the other fingers remain on the collective so as not to interfere with the movement of the governor.
The daily inspection may be carried out by a pilot without the assistance of a licensed maintenance technician. During the daily inspection, the pilot will check the TelaTemp labels found on various major components, among other items. The labels will indicate if any of the components have overheated and provide the pilot with advance warning of future defects. During the daily inspection of 16 December 2009, as well as when the components were dismantled, all the TelaTemp labels indicated temperatures were within the specified ranges.
Clutch system
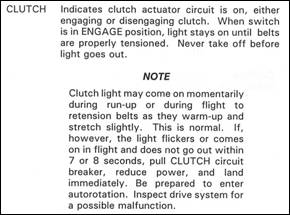
Engine power is transmitted to the main rotor through a belt system, with the engine and transmission engaged by progressive tensioning of the belts. After engine start-up, the belts are tensioned by an actuator motor that automatically stops at a pre-set value. An amber CLUTCH warning light, located on the instrument panel (see Photo 2), comes on when the actuator is running, that is when the belts are being tensioned or are no longer tensioned. If the light comes on during flight, this indicates that the actuator is running because the belts are under−tensioned, which may result from the belts heating up. A fuse located in the test switch compartment Footnote 10 protects the clutch and prevents the breaker from tripping, which would deactivate the warning light during actuator overload.

It is normal for the warning light to come on during flight. However, if it remains on for more than 7 or 8 seconds, the POH recommends pulling the CLUTCH circuit breaker (see Photo 3), reducing power and landing immediately. The breaker is marked with a red ring to facilitate identification and manual activation. As well, the pilot is warned to be prepared to enter autorotation and inspect the drive system (see Figure 4).

Electrical circuits
The Robinson R44 ENG is fitted with two circuit breaker panels mounted on the helicopter floor. The first breaker panel, located on the right side, in front of the pilot's seat, controls the specialized communications equipment. The second breaker panel, located on the floor in front of the left-hand seat, controls the helicopter's electrical system (see Photo 4). The left breaker panel is difficult to see from the pilot's seat. The R44 is not equipped with a warning light in the event that a breaker trips.

At the accident site, the Clutch/Start breaker, which is located on the left panel, was found in the open position. The breaker feeds the belt-tension actuator via the actuator switch. The CLUTCH warning light doesn't illuminate if power to the actuator is cut. When the breaker is opened, the actuator and the warning light stop working. An examination of the Clutch/Start breaker did not reveal any anomalies.
The Clutch/Start breaker is not exclusive to the actuator; it also powers the electrical circuits for the helicopter's main blade brakes and a lock-out signal to the starter system. CARs Section 527.1357Footnote 11 (Circuit Protective Devices) states that “a protective device for a circuit essential to flight safety may not be used to protect any other circuit”.
The R44 is equipped with 2 red warning lights (engine fire and engine oil) and 13 amber warning lights. Microscopic examination of the warning light and alarm filaments confirmed that none of the lights were illuminated at the time of impact.Footnote 12
The illumination frequency of the CLUTCH warning light varies from one R44 to another. The hours of operation, wear and outside temperature can affect the frequency of illumination during a flight. Since the belts on the occurrence helicopter had accumulated few hoursFootnote 13 of operation, they stretched normally and the CLUTCH light came on momentarily in the normal manner.
Section 4 of the POH includes a checklist for breaker inspection. The pilot must ensure that all breakers are positioned normally (i.e. not tripped), carrying out this inspection procedure before starting up the engine.
Operations
General
The helicopter was operated by Groupe TVA Inc. During the day and when required at night, it transmitted live images of media events taking place in the Greater Montréal area. On weekdays, the aircraft would take off at around 0630 from its base at Mirabel Airport, with a pilot and a reporter on board, for an initial patrol of approximately 2 hours in duration. Subsequently, the crew remained on call at the base until 1900 to make other flights, depending on events. The helicopter flew approximately 450 hours per year. According to available information, Groupe TVA Inc. did not pressure its pilots in any way and their authority was never challenged when it came to covering special media events.
Agreement with NAV CANADA
A few months prior to the start of aerial operations, Groupe TVA Inc. and Nav Canada signed an agreementFootnote 14 whose purpose was, among other things, to establish procedures governing the helicopter's patrol flights. The parties agreed that the aircraft would use preferential routes at 1300 feet asl to facilitate navigation and air traffic control. These routes are intended to facilitate flights over urban areas, while providing suitable landing sites in case of emergency. Notwithstanding this, the helicopter could leave the routes in accordance with air traffic control standards and procedures to overfly any media event taking place in the Greater Montréal area. It had also been agreed that patrols would be flown with a cloud ceiling of at least 1600 feet agl and a minimum visibility of 4 miles.
Private/Commercial
A meeting between Groupe TVA Inc. and Transport Canada took place before the start of helicopter operations. Its purpose was to inform the Minister about the type of operation that Groupe TVA Inc. intended to run and to confirm with them whether a private operation was acceptable from a regulatory standpoint. Other than a letter of intent from Groupe TVA Inc., no other meeting and/or request was specified by Transport Canada. In addition, the investigation revealed that no risk assessment was done by Transport Canada since the operation was private in nature. Consequently, no inspections or operational/maintenance follow-ups were conducted by Transport Canada inspectors following the start of operations in 2005.
As Groupe TVA Inc. did not request or collect any compensation, either direct or indirect , for the use of its helicopter, the aircraft was operated in accordance with CARs Part VI (General Operating and Flight Rules). Moreover, since Groupe TVA Inc. was not operating a commercial air service and use of the helicopter was strictly for its own business purposes, Transport Canada did not require that operation of C-GDSF be subjected to the requirements of Part VII (Commercial Air Services). As a private aircraft, C−GDSF was operating under less restrictive rules than those in CARs Part VII. Among other aspects, the regulatory requirements relating to qualifications for flight crew members and commercial air services operators stipulated in Part VII differ significantly from those in Part VI (see Table 1).
| CARs, Part VII | CARs, Part VI |
|---|---|
Flight crew members must:
|
Every two years, pilots must complete a recurrent training activity. They can choose one of the following seven activities:
|
|
|
|
|
|
|
|
|
|
|
Among other differences, a pilot flying a private aircraft is not required to pass a pilot proficiency check (PPC)Footnote 15 each year, as would a pilot flying the same type of aircraft and doing the same type of aerial work in commercial operation.
Although not required by regulations, operation of the helicopter was conducted under the limited supervision of a person who was also serving as the senior pilot. The company could count on other pilots to replace the senior pilot as required. The latter was responsible for scheduling. When other pilots were hired, the senior pilot ensured that they possessed a valid pilot's licence. The senior pilot received annual flight training at Passport Helicopter – a helicopter flight training unit - paid for by Groupe TVA Inc.
Groupe TVA Inc. recordings
During the flight, the reporter's audio commentary and images from the aircraft's camera were transmitted live to Groupe TVA Inc.'s control room. However, the data were transmitted intermittently; obstacles interfering with the signal's line of sight and the inclination of the aircraft resulted in the microwave transmissions to the Groupe TVA Inc. building breaking up. According to available information, signal interruption was normal, considering the position of the antenna in relation to the helicopter.
The Groupe TVA Inc. tape was analyzed at the TSB Laboratory. The noise of the engine could not be heard. However, the analysis detected a change in the Nr just before the low rotor RPM warning horn sounded. As the signal was weak and short in duration, the Nr could not be determined. The last three alarms were recorded in the moments before the crash; they broke up as a result of the interrupted transmission to the Groupe TVA Inc. control room.
Flight altitude above a built-up area
CARs Section 602.14 is a general prohibition. It forbids operating an aircraft over a built-up area unless it is operated at an altitude from which it would be possible to land without creating a hazard to persons or property on the surface. In any case, that altitude for helicopters is not to be lower than 1000 feet above the highest obstacle located within a horizontal distance of 500 feet or less from the aircraft. In all other circumstances, the aircraft is not to be operated at a distance of less than 500 feet from a person, vessel, vehicle or structure. CARs Section 602.12 deems a helicopter to be over a built-up area when it is within 500 feet horizontally of it.
The Robinson R44 was flying just east of Highway 15 at approximately 1100 feet asl and some 2700 feet west of the Mel's Studios heliport when the low rotor RPM warning horn sounded for the first time. The aircraft continued flying east at a rate of descent of approximately 1200 feet per minute.Footnote 16
When the low rotor RPM horn sounded, the helicopter was flying over an industrial area with a scattering of sites conducive to a safe emergency landing. These sites included parking lots, access roads, vacant lots and fields, as well as the heliport at Mel's Studios. At the time of the occurrence, the ground was covered in snow and the sky overcast. Under such conditions, it is difficult to evaluate height above terrain.
Information about the crash site
The heliport at Mel's Studios is a private facility not certified by Transport Canada. It is located just west of the studios between the St. Lawrence River to the south and a railway shop to the north. It has a surface area measuring 150 feet by 150 feet and is bound on the east by two hangars. The helicopter crashed in a ditch 70 feet north of the Bonaventure Expressway and approximately 800 feet from the heliport. The ditch was bound on each side by a flat parcel of land approximately 35 feet in length.
The helicopter came to rest on its left side. There was a strong fuel odour. Emergency services personnel had to use the Jaws of Life to extricate the passenger, who was in the left rear seat. The cabin was partially destroyed. Following impact with the ground, one of the main rotor blades broke off and became detached from the hub; it was found south of the expressway approximately 200 feet from the wreckage. The two blades on the tail rotor were only slightly damaged and remained attached to the tail boom. The right skid initially contacted the snow-covered surface and, because of the forward speed, the helicopter landed in a ditch to the left of the initial point of impact. The angle of the ditch was steep and the helicopter came to a stop alongside a fence. The helicopter hit the ground hard, causing the two skids to collapse under the force of impact. The cabin was cut in two, between the front and rear seats. Both the pilot and passenger were wearing their safety harnesses.
The fuel drain valve was damaged on impact. When the helicopter was raised, the fuel leaked onto the snow through the valve normally used to drain water and debris from the tanks during the pre-flight inspection. The shaft connecting the transmission and tail rotor was still in place because, when the main rotor blades were rotated, the tail rotor blades moved along with them. The engine had shifted to the rear and upward, which explains why one of the tail drive belts was no longer in place.
The helicopter was examined to the extent possible at the crash site before being transported to the TSB Engineering Laboratory in Ottawa. Given the condition of the helicopter and the extent of its mechanical destruction, it wasn't possible to establish control continuity. However, all fractures occurred as the result of an overload condition. There was no indication that any anomaly or flight control failure had preceded the accident or could have contributed to it.
TSB Laboratory Reports
The following TSB Engineering Laboratory reports were completed:
- LP002/2010 – Instruments and Circuit Breaker Analysis
- LP003/2010 – DVD Analysis
- LP049/ 2009 – Airframe and Engine Analysis
Analysis
The accident occurred following a reduction in Nr concurrent with an increase in engine speed. Since the examination of the wreckage did not reveal any anomalies, it is reasonable to think that the belt system tension reduced in flight. Belt slippage produces an increase in the speed of the engine, since the latter is no longer engaged with the clutch system. In addition, since the main rotor is no longer driven by the engine, the Nr drops. Consequently, it can be concluded that the helicopter sustained a drive system malfunction. This analysis will deal with the failure that likely caused the reduction in Nr and with the emergency landing executed by the pilot.
Plausible scenarios
No defects were observed upon examination of the helicopter. However, it was noted at the accident site that the Clutch/Start breaker had tripped. Three scenarios that could explain the breaker tripping were examined.
Breaker pulled in flight
This scenario was determined to be highly unlikely. The investigation did not find any indication to suggest that the pilot had pulled the breaker following illumination of the CLUTCH light. If this had occurred, the pilot, knowing he had to execute a precautionary landing as quickly as possible, would have notified the controller of his intention before the low rotor RPM horn had sounded. The pilot did not indicate his intention to land at Mel's Studios until after the low rotor RPM horn had sounded.
Breaker tripped upon impact with the ground
The hypothesis that the breaker would have tripped upon impact cannot be completely ruled out. Given that the force of the collision with the ground was sufficiently great to cause significant damage to the aircraft and seriously injure its occupants, it is conceivable that the force of the impact could have triggered the breakers located on the floor. If the breaker had been engaged prior to the accident, the CLUTCH warning light would have gone on in flight and the pilot would have seen it before the low rotor RPM horn had sounded.
Breaker tripped in flight following a temporary overvoltage
The clutch system was working normally prior to the flight.Footnote 17 In addition, the laboratory tests did not reveal any defects. Therefore, the belt-tensioning actuator should have been running and the CLUTCH warning light illuminated when the belts lost tension, prior to the low rotor RPM horn sounding. It follows that, had the breaker not tripped, the pilot would likely have noticed that the CLUTCH warning light had come on. In these circumstances, it can be assumed that the Clutch/Start breaker was tripped before the reduction in Nr. According to this hypothesis, the breaker could have tripped without the pilot's knowledge since it is located outside his normal field of visionFootnote 18 and no visual or auditory warning is provided when the breaker trips. Consequently, the helicopter was able to continue flying with the clutch system not engaged. The investigation was unable to determine why the Clutch/Start breaker tripped.
Clutch/Start breaker
Since the Clutch/Start breaker is not exclusive to the clutch system, it can be tripped by a defective component in a related non-essential electrical system.Footnote 19 Once tripped, the breaker no longer powers the actuator and warning light. As a result, the actuator is no longer able to tighten the belts. According to CARs Section 527.1357, the electrical system of a system essential to flight should be exclusive to that system. Although the R44's clutch system is essential to the safety of the helicopter's flight, its Clutch/Start breaker powers other electrical circuits belonging to non-essential systems.
The checklist in Section 4 of the POH requires that the breakers be inspected prior to engine start-up. In the event that an electrical problem arises during start-up and the breaker trips, an additional verification of the breaker panel must be included in the checklist procedure immediately prior to takeoff.
Emergency landing
The helicopter was in the vicinity of the Champlain Bridge at 1100 feet asl, when the low rotor RPM horn sounded indicating that the Nr had dropped below 97%. The engine was producing power with no other associated caution or warning lights. Although the pilot recognized the low rotor horn, it is likely the pilot believed that some power was still being delivered to the main rotor system. Therefore, the clutch failure went undetected and the pilot did not enter autorotation. As a result the main rotor rpm decreased to the point where control authority had been significantly reduced preventing a normal autorotative landing.
Clutch malfunction symptoms are not replicated during training flights; therefore, the pilot could not fall back on any related experience to quickly evaluate the situation.
Autorotation, which involves completely lowering the collective pitch lever, is critical to preventing the loss of Nr. Any delay in entering autorotation or the partial lowering of the collective can result in significant Nr decay and cause control problems that could affect the landing. The analysis of Groupe TVA Inc.'s tape revealed that the low rotor RPM warning signal was recorded four times after it first sounded. It was also noted that the last three low RPM alarms were recorded in the moments preceding the crash and that they were broken up by the interruption in transmissions to Groupe TVA Inc.'s control room. It is conceivable that the last three alarms were in fact one continuous alarm divided by transmission interruptions. In view of the preceding and the escalating loss of control response in the last moments of the flight, it can be concluded that the Nr decayed during autorotation to the point where control of the aircraft was compromised.
Autorotation is a manoeuvre that demands skills rarely put into practice, other than during recurrent training sessions. When the low rotor RPM horn sounded, the pilot had little time in which to select a site conducive to a forced landing. Although several sites permitting a safe landing were available in the flight area, few of them were conducive to an autorotation landing. The choice of an appropriate site for a forced landing is related to the altitude of the helicopter at the time of failure, the site's position in relation to the helicopter, its surface characteristics and obstacles in the surrounding area.
The location of the heliport at Mel's Studios presented a more serious challenge than the other available sites right in front of the helicopter. Indeed, the hangars on the east side made any approach from the east difficult and the location of the site with respect to the helicopter required that the pilot initiate a turn of at least 180° at an altitude of 700 feet agl. These two factors complicated the pilot's task by limiting the approach track and increasing the rate of descent during the turn.
The fact that Groupe TVA Inc.'s single-engine helicopter was flying over an urban area in accordance with the criteria for private operation is in no way linked to the failure that resulted in a forced landing. Nevertheless, it would be reasonable to think that sustained low-level aerial operationsFootnote 20 with a single-engine helicopter over a built-up area during the day and at night increases the likelihood of adverse consequences when the aircraft operation is not regulated to commercial standards .It should be noted in this regard that Groupe TVA Inc. had decided when it purchased the helicopter that its maintenance would be performed in accordance with commercial standards. However, Groupe TVA Inc. had decided that the helicopter would be operated in accordance with the less stringent standards in CARs Part VI.
It is conceivable that the requirements governing the operation of a commercial company and its pilot training would reduce the probability that a hazardous condition would lead to adverse consequences and the gravity of such consequences (see Table 1). It is interesting that Transport Canada does not perform any risk assessment in the case of a private operation . The number of flight hours over an urban area, the number of engines (single or twin-engine), scheduling (night or day), recurrent pilot training and the type of flight are not taken into consideration by Transport Canada when it comes to private operations. However, in terms of the nature of the work, the operation of Groupe TVA Inc.'s helicopter involved a level of risk that was more significant than if it had been operated in accordance with commercial standards.
In the case at hand, the pilot held a commercial licence. However, his last PPC on the R44 was in 2002 and his last in-flight test on type had taken place 2.5 years prior to the accident. It can be concluded that his skills for dealing with the situation were not as highly developed as would have been the case if his recurrent training had been carried out in accordance with the requirements for a commercial operation. It cannot be stated categorically that the pilot would have successfully completed the forced landing if he had participated in the training program required under CARs Part VII. However, such training would have increased the likelihood of his executing the autorotation successfully.
Findings
Findings as to causes and contributing factors
- The clutch system ceased operating when its circuit breaker tripped for undetermined reasons resulting in a reduction in rotor speed. The malfunction took place at a low altitude leaving the pilot with very little time to react.
Findings as to risks
- Sustained low level aerial operations with single-engine aircraft over a built-up area that are not regulated to commercial standards represent an added risk.
- Regulations do not require continuous recurrent flight training for private pilots. Consequently, they can fly in difficult conditions without demonstrating their proficiency, as is required of commercial pilots flying in the same operational conditions.
- The lack of an annunciator panel or auditory warning system indicating an electrical malfunction on a critical system increases the risk that a pilot may not correctly identify and react to a system failure.
Other findings
- The clutch system electrical circuit breaker was found to be connected with other electrical systems onboard the helicopter.
This report concludes the Transportation Safety Board's investigation into this occurrence. The Board authorized the release of this report on .
Appendices
Appendix A - Safety Notice SN-24
ROBINSON HELICOPTER COMPANY
Safety Notice SN-24
Issued: Sep 86 Rev: Jun 94
Low RPM Rotor Stall can be Fatal
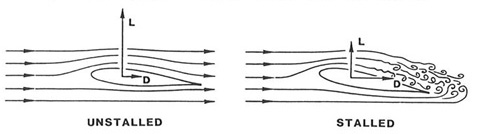
Rotor stall due to low RPM causes a very high percentage of helicopter accidents, both fatal and non-fatal. Frequently misunderstood, rotor stall is not to be confused with retreating tip stall which occurs only at high forward speeds when stall occurs over a small portion of the retreating blade tip. Retreating tip stall causes vibration and control problems, but the rotor is still very capable of providing sufficient lift to support the weight of the helicopter.
Rotor stall, on the other hand, can occur at any airspeed and when it does, the rotor stops producing the lift required to support the helicopter and the aircraft literally falls out of the sky. Fortunately, rotor stall accidents most often occur close to the ground during takeoff or landing and the helicopter falls only four or five feet. The helicopter is wrecked but the occupants survive. However, rotor stall also occurs at higher altitudes and when it happens at heights above 40 or 50 feet AGL it is most likely to be fatal.
Rotor stall is very similar to the stall of an airplane wing at low airspeeds. As the airspeed of an airplane gets lower, the nose-up angle, or angle-of-attack, of the wing must be higher for the wind to produce the lift required to support the weight of the airplane. At a critical angle (about 15 degrees), the airflow over the wing will separate and stall, causing a sudden loss of lift and a very large increase in drag. The airplane pilot recovers by lowering the nose of the airplane to reduce the wing angle-of-attack below stall and adds power to recover the lost airspeed.
The same thing happens during rotor stall with a helicopter except it occurs due to low rotor RPM instead of low airspeed. As the RPM of the rotor gets lower, the angle-of-attack of the rotor blades must be higher to generate the lift required to support the weight of the helicopter. Even if the collective is not raised by the pilot to provide the higher blade angle, the helicopter will start to descend until the upward movement of air to the rotor provides the necessary increase in blade angle-of-attack. As with the airplane wing, the blade airfoil will stall at a critical angle, resulting in a sudden loss of lift and a large increase in drag. The increased drag on the blades acts like a huge rotor brake causing the rotor RPM to rapidly decrease, further increasing the rotor stall. As the helicopter begins to fall, the upward rushing air continues to increase the angle-of-attack on the slowly rotating blades, making recovery virtually impossible, even with full down collective.
When the rotor stalls, it does not do so symmetrically because any forward airspeed of the helicopter will produce a higher airflow on the advancing blade than on the retreating blade. This causes the retreating blade to stall first, allowing it to dive as it goes aft while the advancing blade is still climbing as it goes forward. The resulting low aft blade and high forward blade become a rapid aft tilting of the rotor disc sometimes referred to as "rotor blow-back". Also, as the helicopter begins to fall, the upward flow of air under the tail surfaces tends to pitch the aircraft nose-down. These two effects, combined with aft cyclic by the pilot attempting to keep the nose from dropping, will frequently allow the rotor blades to blow back and chop off the tailboom as the stalled helicopter falls. Due to the magnitude of the forces involved and the flexibility of rotor blades, rotor teeter stops will not prevent the boom chop. The resulting boom chop, however, is academic, as the aircraft and its occupants are already doomed by the stalled rotor before the chop occurs.