Loss of Control and Collision with Terrain
Forest Protection Limited
Grumman TBM-3E C-GFPL
Miramichi, New Brunswick
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The Forest Protection Limited Grumman TBM-3E fire-fighting aircraft (registration C-GFPL, serial number 86020) departed Miramichi Airport, New Brunswick, for a practice water drop flight at about 1338 Atlantic Daylight Time. Approximately 2 minutes later, the aircraft collided with terrain just south of the airport. Emergency responders and workers from nearby businesses responded immediately. The aircraft was destroyed by the impact forces. There was no reported emergency locator transmitter signal. Medical examination determined that the pilot had suffered a heart attack prior to the aircraft impacting the ground.
Factual information
History of the Flight
The flight departed the Miramichi Airport in conditions suitable for visual flight. After turning toward the practice area to drop a water load, the aircraft levelled off at about 500 feet above ground level. Once levelled off, there was no change in engine speed. The aircraft entered a shallow descent, banked to the right and struck several trees before impacting the ground at approximately 1340. Footnote 1 The aircraft broke apart on impact and came to rest in a wooded area just south of the airport, adjacent to an industrial site. The load of water was expelled on impact. The pilot made no radio transmissions after the aircraft had taken off.
Operator
Forest Protection Limited (FPL) is a private company that conducts operations under subpart 702 of the Canadian Aviation Regulations (CARs). FPL has been operating since 1951 and provides fire suppression, pest management and aerial survey services.
FPL relied on the Transport Canada (TC) medical certificate to determine if a pilot was fit for flight.
Aircraft

The accident aircraft (see Photo 1) was manufactured in 1954 and converted to a fire-fighting aircraft in April 1993 in accordance with a TC approved Limited Supplemental Type Certificate.
At the time of the accident, the aircraft had about 3893 total flight hours since being manufactured. Records indicate that it was certified, equipped, and maintained in accordance with existing regulations and approved procedures, and that there were no known deficiencies before the accident flight. The aircraft was equipped with a 406 Megahertz emergency locator transmitter (ELT). It was not equipped with onboard recorders, nor were they required by regulation. The weight and centre of gravity were within the prescribed limits at the time of the accident.
Accident Site
The aircraft impacted the ground in a 45° nose-down and 45° right wing-low attitude. The aircraft created a 1 metre deep crater before breaking up. The main wreckage trail was oriented at about 300° magnetic and was approximately 110 metres in length. The ELT switch was found in the ON position and the ELT was transmitting. However, the ELT had been ejected from the aircraft during the accident sequence and was no longer connected to its antenna; as a result, no ELT signal was received.
There was no indication of pre-impact structural failure or failure of the flight control system. The landing gear and flaps were in the up position at the time of impact. The damage noted on the propeller blades was consistent with the engine running at the time of impact.
The pilot was ejected from the aircraft. The safety harness and lap belt were not fastened and there was no impact damage noted on the buckle, indicating the harness and belt were not fastened at the time of impact.
Pilot
The pilot held a commercial pilot licence and had approximately 13 530 hours total flight experience with about 260 hours on this type of aircraft. Records indicate that the pilot was certified and qualified for the flight in accordance with existing regulations. The pilot had worked for FPL for approximately 10 years. The pilot's practice was to not use the safety harness's shoulder straps and, on occasion, would not buckle the seat belt portion.
The pilot was over the age of 40. TC requires pilots over the age of 40 years who hold a commercial pilot licence to have a Category 1 medical examination every 6 months and an electrocardiogram (ECG) once yearly. The pilot's last TC Category 1 medical examination was completed on 07 April 2010 and his last ECG was completed in March 2010. The ECG was within normal limits.
In 1991, the pilot's ECG revealed small Q waves. A stress test was carried out and the results were reported as being negative for ischemia and other signs of coronary disease.
The TC Regional Aviation Medical Officer (RAMO) reviewed the pilot's ECGs, which had remained unchanged for 10 years, as well as his medical file each year and determined that there was no need for additional testing.
Pilots are required to report on their TC medical report form all visits to medical professionals and current medications (prescription or over the counter drugs) they are taking. The pilot had a history of hypertension dating from 1998 and he had been taking medication to treat this condition. This information was not reported to TC by the pilot's family physician; however, it was reported by the pilot during his 2008 TC aviation medical examination. Between 1998 and 2008, each of the pilot's TC medical reports recorded that he had not seen a physician during the time between TC medical exams, despite having made numerous visits to his family physician. The pilot had regular cholesterol tests since 1998 and his most recent laboratory tests, conducted in September 2009, 7 months before the occurrence, included both serum lipids, which were in a normal range, and fasting blood sugar, which was above normal. Footnote 2 The pilot did not provide this information to the TC Civil Aviation Medical Examiner (CAME), Footnote 3 nor was he required by the current standard to do so. Footnote 4 The information was therefore not recorded on his medical report.
On the morning of the occurrence flight, the pilot had a grey complexion and was sweating, which can indicate heart problems. Footnote 5 Autopsy results concluded the pilot suffered from ischemic heart disease.
Transport Canada Medical Requirements for Pilots
The primary activity of TC 's Civil Aviation Medicine Branch (CAM) is the performance of medical assessments required for the certification of licensed aviation personnel. CARs Standard 424.17 states that:
The purpose of the medical examination is to determine whether an applicant meets the standards that apply in respect of the issuance of the Medical Certificate that is needed to issue a particular permit, licence or rating.
With aviation medicals, TC is chiefly concerned with managing the risk to aviation over the short term, that is, the validity period of the medical certificate, rather than the long term health of the individual. As such, TC reviews the risk of incapacitation for the period of the licence and, if necessary, may request further medical examination, rather than using the full range of techniques that a family physician might use when looking at the long term health of an individual.
It is the CAME's responsibility to interview and perform a complete examination on all applicants. CARs Standard 424 requires the CAME to examine the applicant in accordance with medical practices recognized by the medical profession, and with the personnel licensing standards. The CAME is usually the only person who physically examines the applicant and makes a recommendation for medical certification. Footnote 6 TC considers the CAME to be the most important link in the medical certification process.
Frequently the CAME is not the applicant's personal physician and must rely, to a large extent, on information disclosed by the applicant. TC recognizes that aviation personnel may not volunteer information that could affect their medical certification, typically because they may fear losing their medical certificate and, in some cases, their employment.
The CAM Handbook for Civil Aviation Medical Examiners (TP13312) Footnote 7 stipulates that, during the medical examination, there is a shared responsibility, with the onus on the applicant, to report any symptoms and a requirement for the CAME to conduct a careful and thorough examination. CARs Standard 424 requires an applicant to sign the Aviation Medical Examination Report, which states that the information provided is complete and correct and that they are aware that it is an offence to knowingly make a false declaration. In addition, they authorize TC to obtain additional medical documentation as necessary for the renewal of the applicant's medical. CARs Standard 424 also requires the applicant to undergo any other examinations or tests that are required by the CAME in order to assess the applicant's medical fitness. Even though TP13312 is a guidance document for professional medical physicians, in practice, many CAMEs and RAMOs believe they are restricted to staying within these guidelines when performing a medical examination. While present legislation provides the CAME with the authority and the means to obtain any additional medical information necessary to determine if a pilot meets the medical requirements of their licence, neither the CAMEs nor the RAMOs are able to require an applicant to undergo medical testing unless:
- CARs Standard 424 requires the test, or
- the test is necessary to determine whether the applicant meets the medical fitness requirements specified in the personnel licensing standards Footnote 8, or
- there are indications of a disease present that must be further examined to establish medical fitness.
Reporting Requirements
The Aeronautics Act 6.5(1)(4) requires physicians to report to TC any holder of a Canadian aviation document who they believe (on reasonable grounds) may, for medical reasons, constitute a risk to aviation safety. Chapter 24 of the Canadian Medical Association (CMA) Driver's Guide, which addresses aviation, states that:
- Before being examined, all pilots must inform the physician that they hold an aviation licence or permit.
- Physicians are required by law to report to regional aviation medical officers of Transport Canada any pilots, air traffic controllers or flight engineers with a medical condition that could affect flight safety.
Section 24.4, Medical Conditions, of the CMA Driver's Guide alerts physicians to aspects of medical fitness that are of unique importance to aircrew and provides a list of common reportable conditions. If the physician is certain that a condition poses a risk to aviation they must report it. If uncertain, the treating physician can contact a RAMO for guidance. Initial treatment of hypertension is specifically highlighted as a mandatory reporting item Footnote 9. The pilot's family physician did not report the initial treatment of hypertension to TC and was not aware of this requirement.
In addition, the Aeronautical Information Manual (AIM), a manual available to flight crews and containing information concerning the rules of the air and procedures for aircraft operation in Canadian airspace addresses the issue of medical reporting. Air Section 3.1.1, Mandatory Medical Reporting, reminds pilots that before they have a medical examination by any physician they must identify themselves as a holder of a pilot's licence. Additionally, the AIM states that the attending physician must notify TC of any finding that may constitute a hazard to aviation safety.
In 2006, TC issued Aviation Safety Letter TP185 which reminded pilots, air traffic controllers and flight engineers that:
… by law, all physicians in Canada must inform a Regional Aviation Medical Officer (RAMO) of any pilot, air traffic controller or flight engineer who has a medical condition that could adversely affect flight safety.
The holder of a Canadian aviation document that imposes standards of medical or optometric fitness shall, prior to any medical or optometric examination of his or her person by a physician or optometrist, advise the physician or optometrist that he is the holder of such a document.
During the investigation, several CAMEs, physicians and pilots were consulted to obtain an understanding about the awareness amongst Canadian general practitioners of the requirement to report a pilot's medical condition that may affect flight safety. With the exception of where the pilot's family physician was also the pilot's CAME, it was determined that some general practitioners may not be aware of the requirement to report.
Cardiovascular Disease
The presence or development of cardiovascular disease in licenced aviation personnel, with the risk of potential clinical manifestations, continues to be a major concern amongst aviation medical practitioners worldwide. The prevalence of ischemic heart disease increases with age and with the presence of major risk factors for ischemic heart disease. The overall population of aviators in Canada is aging and as a consequence the likelihood of a cardiovascular event is increasing. TC has indicated that screening of the aircrew and air traffic controller population to identify cardiovascular disease before sudden incapacitation is a problematic and controversial undertaking. TC has stated that it will not impose a major burden if exercise ECG testing is applied to those who are more likely to have coronary artery disease (CAD), such as those with symptoms of angina, those for whom major risk factors are present and those in older age groups.
The exercise ECG test is useful chiefly in the diagnosis of CAD, blockages in the arteries that supply blood to the heart muscle. If a partial blockage is present, the heart muscle supplied by that partial blockage may be getting all the blood it needs in the resting state. However, if the person with this partial blockage exercises, the artery may not be able to supply all the blood the heart muscle needs to perform at the high level now needed. When a portion of the heart muscle is suddenly not receiving enough blood flow, it becomes oxygen-starved, or ischemic. Ischemic heart muscle often causes chest discomfort (a symptom called angina) and characteristic changes on the ECG. By stressing the heart with exercise, the stress test can bring out abnormalities caused by partial blockages in the coronary arteries. Such abnormalities are often completely unapparent at rest. Footnote 10
According to the International Diabetes Federation, if a male has a body mass index (BMI) greater than 30 kg/m², triglycerides greater than 1.7 mmol/L, and fasting blood sugar greater than 5.6 mmol/L then they meet the criteria for the consensus worldwide definition of metabolic syndrome. Metabolic syndrome is accompanied by a 2-fold increase in the risk of cardiovascular disease. Footnote 11
Based on the pilot's BMI, which was calculated in excess of 30 kg/m², and his triglyceride and fasting blood sugar values, he would fit the definition of having metabolic syndrome.
A study to evaluate the prognostic relevance of metabolic syndrome (MetS) in hypertensive patients at low-medium risk concluded that the presence of MetS increases cardiovascular risk: Footnote 12
Hypertensive patients at low-medium risk with MetS are at higher cardiovascular risk than those without MetS. Metabolic syndrome may be a useful tool for clinicians to identify subjects who are at increased risk when traditional assessment may indicate low-medium risk.
There is currently no reference to the consideration of metabolic syndrome when assessing cardiovascular risk in the current CAM guidelines.
Cardiovascular Guidelines and Risk Assessment
TP13312 addresses the major areas for aeromedical certification, including cardiology. TC has indicated that these guidelines are written such that they allow flexibility, professional judgment and the use of rapidly evolving concepts in medicine. TC reminds CAMEs that these are only guidelines.
Coronary atherosclerosis is a multi-factorial disease, where the risk of early onset increases with the number of risk factors present. The guidelines include a section which provides a means of assessing total risk (see Appendix A) on the basis of risk points for age, total and HDL cholesterol, systolic blood pressure and smoking.Footnote 13 If the 10-year risk score is 20% or greater (9 risk points for men and 15 risk points for women) then a cardiovascular assessment including an exercise treadmill test should be carried out. Additional tests will depend on the risk factor profile.
In a recent article Footnote 14 TC stated:
The standard of care in Canada would suggest that everyone should have their blood lipids tested after the age of 40 to better evaluate their risk for coronary disease. For licensed pilots, fitness assessments are still individualized processes rather than generalized ones based on age.
In this specific case, the information from the pilot's most recent medical examination and his cholesterol test results, when analysed using the Risk Scoring System, showed a risk score of 16% (8 risk points), which is a moderate risk level. Footnote 15
The current standards do not require periodic testing for serum cholesterol (unlike the yearly ECG for pilots over the age of 40 years) even though the cholesterol test results are necessary for accurate use of the Risk Scoring System. If the cholesterol results are not included when using this scoring system, the applicant's overall score will be inaccurate. In this occurrence, neither the CAME nor the RAMO used the Risk Scoring System to assess the risk of a cardiovascular event.
Even though there are different methods Footnote 16 to perform a cardiovascular risk assessment that do not require cholesterol results, the TC guidelines focus on the use of the Risk Scoring System.
Medical Examination Report
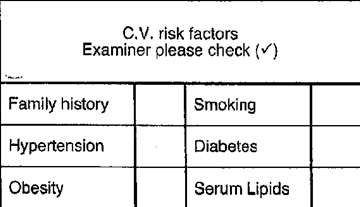
The current TC Civil Aviation Medical Examination Report form contains a cardiovascular risk factors table that can be used by the CAME to consolidate information and to help assess the risk posed by 6 cardiovascular (CV) risk factors (see Figure 1), but the form does not contain or make reference to the Risk Scoring System.
Use of the risk factors table is voluntary and no explicit instructions regarding the use of the table, the meaning of the check marks or the absence thereof are provided. In the occurrence pilot's last 3 medicals, even though the CAME noted elsewhere on the medical report that the pilot had been treated for hypertension and was aware of his obesity and smoking, only the box indicating that the pilot was a smoker had been checked off in the CV risk factors table.
TC Oversight of CAMEs
The RAMOs are responsible for reviewing the medical examination reports and for approving an appropriate medical category for aviation personnel. Oversight of the quality and consistency of the medical examinations performed by CAMEs is primarily limited to the RAMO's review of the completed medical report. If a CAME repeatedly submits reports that are incomplete or have discrepancies, the RAMO contacts the CAME to correct the deficiency. TC does not have documented procedures for providing oversight of CAMEs or for identifying the prevalence of non-reporting by pilots. According to TC CAM website, approximately 55 000 medical examinations are conducted annually by over 950 designated CAMEs across Canada and overseas. Currently, TC has 787 CAMEs in Canada and 5 RAMOs.
Similar Occurrences
For the period between 01 January 1976 and 31 October 2008, the TSB database has 35 occurrences related to cardiovascular issues, of which 28 occurrences involved fatalities. The U.S. National Transportation Safety Board records from 1982 to present identified 13 cardiovascular related events, Footnote 17 involving pilot fatalities.
TSB Report A07P0357, where the cause of the accident was possibly an acute medical event, identified concerns about the use of the cardiovascular risk factor table, the guidelines concerning the use of arisk scoring system, and non-disclosure by pilots of relevant medical information. Additionally, the report discussed the advances in the assessment of risk factors since the 2004 guidelines were published, which included the value of assessing cholesterol levels.
The following TSB Laboratory reports were completed:
- LP061/2010 – Instrument Examination
- LP050/2010 – Video Analysis
These reports are available from the Transportation Safety Board of Canada upon request.
Analysis
Nothing was found to indicate that there was any airframe failure or system malfunction prior to or during the flight. It was also determined that the weather conditions did not play a role in this occurrence. The autopsy determined that the pilot had suffered a heart attack resulting in the aircraft departing controlled flight and impact with the ground. Therefore, the analysis will focus on the medical aspects of the investigation.
The pilot's medical status was being followed by a family physician who originally diagnosed the pilot with hypertension in 1998. The pilot was taking medication to treat this condition. However, this information was not recorded on the Aviation Medical Examination Report until 2008 because the pilot had not disclosed this information to the CAME and the family physician had not reported the relevant condition to TC . Present regulations provide the CAME with the authority and the means to obtain any additional medical information necessary to determine if a pilot meets the medical requirements of their licence. However, if there is no basis to do so because a pilot has not disclosed a symptom/condition to their CAME, an additional medical investigation is not conducted. Non-disclosure of medical symptoms/conditions to a CAME negates some of the safety benefit of examinations and increases the risk that pilots will be allowed to fly with a medical condition that poses a risk to safety.
In addition, although the family physician was aware that the pilot held a pilot's licence, there was a lack of awareness of the requirement to report to TC any medical conditions that may affect flight safety. This is consistent with the results of the TSB's discussions with other CAMEs and personal physicians; there may be a lack of awareness amongst Canadian general practitioners of the requirement to report medical conditions that may affect flight safety. This may result in a CAME not having all the information required to accurately determine a pilot's fitness for flight.
The guidelines contained in TP13312 state that if the 10-year risk score, determined by using the Risk Scoring System, is 20% or greater, a cardiovascular assessment should be carried out. When using the Risk Scoring System, an applicant's 10-year risk score can only be accurately determined if their cholesterol test results are known. However, a cholesterol test is not a required test under the current standards and, therefore, test results are only provided voluntarily, if known. Because CARs Standard 424 does not require an applicant to provide the results of a cholesterol test, there is a risk that CAMEs may not have all of the information needed to accurately determine an applicant's 10-year risk of cardiovascular event.
Use of the Risk Scoring System and the pilot's cholesterol results indicate a medium 16% risk score, which did not require further assessment. Had the pilot reported his elevated fasting blood sugar and serum triglycerides levels to the CAME, current Canadian medical protocol would have suggested a reassessment of the pilot's risk factor profile and additional tests in order to further ascertain his state of health. Additional tests such as an exercise treadmill test, would likely have provided indications of the underlying heart disease. Despite multiple cardiac risk factors, the CAM system in aggregate (i.e. the pilot, the family physician, the CAME and the RAMO) did not identify the pilot's underlying coronary disease.
In this case, neither the CAME nor the RAMO used check boxes on the medical form or the Risk Scoring System contained in the guidelines to consolidate and assess the applicant's risk level. Since TC 's guidelines reference the Risk Scoring System, it would be reasonable to expect that the TC medical examination report form would include a table consistent with what is published in the guidelines and that the guidelines would provide clear direction on its use. Because the Aviation Medical Examination Report form does not include the Risk Scoring System table, there is a risk that cardiovascular risk factor information will not be recorded or used effectively when determining an applicant's risk of cardiovascular event. The risk is exacerbated because the guidelines do not provide clear direction on the use of the table.
A full risk profile of this pilot would have included his age, obesity, BMI, smoking habits, hypertension, elevated triglycerides and blood sugar, as well as prompted further investigations to detect underlying coronary disease. These comprehensive investigations would likely have identified him as high risk for a cardiovascular event.
Findings
Findings as to causes and contributing factors
- The pilot's underlying coronary disease was not identified despite the defences built into the Civil Aviation Medicine system.
- The aircraft departed controlled flight and impacted terrain because the pilot suffered a heart attack.
Findings as to Risk
- A lack of awareness amongst Canadian general practitioners of the requirement to report medical conditions that may affect flight safety may result in Transport Canada (TC ) not having all the information required to accurately determine a pilot's fitness for flight.
- Non-disclosure of medical symptoms /conditions to a Civil Aviation Medical Examiner (CAME) negates the safety benefits of the examination and increases the risk that a pilot will fly with a medical condition that poses a risk to safety.
- TC guidelines for CAMEs do not adequately assess and document all cardiovascular risk factors in pilots, thereby increasing the probability that these risks will go undetected.
- When pilots do not wear their safety harness, they are at greater risk of injury during the operation of the aircraft.
Other Finding
- The ELT became disconnected from its antenna during the impact sequence; as a result no ELT signal was received.
Board Concern
In this occurrence, the pilot had multiple cardiac risk factors. These factors were not reported to TC by the pilot's general practitioner. Further, using the current guidelines, the CAM system did not identify the pilot's underlying coronary disease. This brings into question the adequacy of the current guidelines to assess cardiovascular risk factors in the aviation community.
In 2010, TC CAM held a workshop with cardiovascular specialists to review its cardiovascular assessment guidelines, which are now in the process of being re-written. It is unclear whether the new assessment guidelines will incorporate the lessons learned from TSB investigations, including this investigation and, in particular, whether they will include modern benchmarks and rigorous screening designed to identify aviation personnel at risk of a cardiovascular event.
The Board is concerned that medical practitioners may not always be aware of the need or importance of transmitting reportable medical conditions and, further, that deficiencies exist in the guidelines designed to screen for cardiovascular risks. As a consequence, there continues to be a risk that cardiovascular risk factors will go undetected in aviation personnel.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .