Loss of Control and Collision with Terrain
Nordair Québec 2000 Inc.
de Havilland DHC-2 Mk. 1 C-FGYK
La Grande-Rivière Airport, Quebec
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
At approximately 1053 Eastern Daylight Time, de Havilland DHC–2 Mk. 1 amphibious floatplane (registration C–FGYK, serial number 123), operated by Nordair Québec 2000 Inc., took off from runway 31 at La Grande–Rivière Airport, Quebec, for a visual flight rules flight to l'Eau Claire Lake, Quebec, about 190 nautical miles to the north. The take–off run was longer than usual. The aircraft became airborne but was unable to gain altitude. At the runway end, at approximately 50 feet above ground level, the aircraft pitched up and banked left. It then nosed down and crashed in a small shallow lake. The pilot and 1 front–seat passenger were fatally injured and the 3 rear–seat passengers sustained serious injuries. The aircraft broke up on impact, and the forward part of the cockpit was partly submerged. The emergency locator transmitter activated on impact.
Other Factual Information
During the afternoon of 23 July 2010, the day before the flight, the passengers went to the office of Nordair Québec 2000 Inc. in Radisson, Quebec. The passengers' baggage was transported in 2 cars. The pilot checked it, and it was agreed that there would be no problem loading it all on the aircraft. The passengers were being flown to l'Eau Claire Lake to join a canoe expedition.
On the day of the accident, the aircraft was fuelled from the facilities at La Grande–Rivière Airport. It was determined that the aircraft took on a total of 374 litres of fuel, including the 3 full belly tanks and 2 more 20–litre containers. Four other 20 L containers were filled with automotive fuel. Two containers were placed in the forward float compartments and the other 4 were placed immediately behind the rear passenger seat in the cabin. Also, a canoe, 18 feet long and 32 inches wide, was tied directly to the right float struts.
The aircraft had 2 forward seats and 1 triple seat aft. The pilot loaded and placed the baggage items behind the triple seat, but did not weigh them beforehand. The pilot let the passengers choose their own seats.
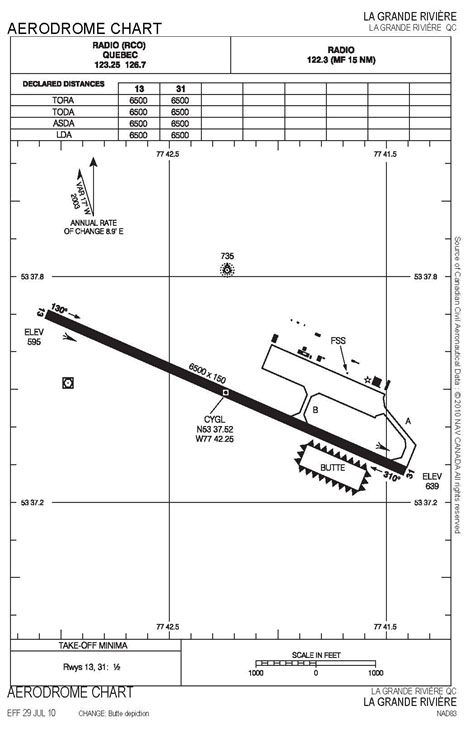
At 1051, Footnote 1 the pilot informed the Flight Services Specialist (FSS) that he was ready to taxi for runway 31. In accordance with the Flight Services Manual of Operations (FS MANOPS) procedures, the FSS informed the pilot that runway 13 would be better, due to the wind speed and direction. The pilot acknowledged and advised the FSS that he was taking off from runway 31. He used the full length, which was unusual because he normally took off from the intersection of taxiway Bravo (Appendix A). The aircraft took off at 1053.
The take–off run was longer than usual. Once airborne, the aircraft was unable to gain altitude. The engine noise was constant and it seemed to be operating normally. When the aircraft was approximately 50 feet above ground level (agl) at the runway end, it pitched up and banked left. It then nosed down and crashed in a lake approximately 900 m from the end of runway 31, to the left of the runway centre line. At 1054:30, the emergency locator transmitter (ELT) signal is received.
Although the FSS could not see where the aircraft crashed from his position, he immediately activated the crash alarm. Twenty–three seconds later, he tried calling 911 but a misdial occurred. Afterwards, the FSS was busy communicating by radio with other aircraft and also with the rescue team in charge. As a result, the call to 911 was made about 10 minutes after the crash.
Rescue Information
When the crash alarm was activated, the prevention officer on duty drove the airport fire truck to the runway 13 threshold and saw the aircraft in the lake. However, the truck could not get any closer to the wreckage. An Air Inuit Hawker Siddeley 748 (HS748) flew over the accident site and confirmed that it saw no movement around the aircraft. Two airport employees reached the wreckage by following a trail and wading into the lake. The pilot was still conscious when they arrived at the site. They got one of the rear–seat passengers out and took him to shore. Then, they held the heads of the other 2 rear–seat passengers above water until the rescuers arrived. When the first responders arrived at the airport, they were transported to the accident site by helicopter. A short time later, a second helicopter transported one of the injured to Chisasibi. That evening, the 3 rear–seat passengers were flown to 2 hospitals in the Montreal area.
Information on Airport and Fire Service
La Grande–Rivière Airport is in the Municipality of Radisson. The airport is operated by the Société de Développement de la Baie–James, which holds the Transport Canada (TC) operating certificate.
TC approved the existing emergency measures plan on 17 March 2003. Since 1 January 1997, there was only 1 rescue truck available at the airport. The area under airport responsibility is restricted to airport property only. It covers an imaginary rectangle extending 1000 m beyond each runway end and 150 m either side of the runway centre line. Any response required outside this boundary is the responsibility of the Municipality of Radisson, located 32 km away. The estimated response time for the regular crew is approximately 45 minutes.
Wreckage Information
The aircraft broke into 3 parts on impact. The cockpit part rested on its right side, on the bottom of the lake, in about 1 m of water. The substantial damage to the front of the aircraft showed that it struck the surface of the lake in a vertical attitude, with left bank. The engine compartment was pushed upward and to the right. All float attachment fittings failed due to the force of the impact. Both wings separated forward due to strong forces. The left side of the aircraft was more severely damaged than the right side. The left float sustained substantial compression damage and the nose wheel separated due to the force of the impact.
The cabin floor was not severely damaged. However, the aluminum legs of the triple seat were broken and the seat was completely separated from its attachment fittings, propelling the passengers forward. The seatbelts were anchored directly to the seats. Although baggage tie–down fittings were installed in the aircraft, the baggage was not secured to the floor, and it shifted forward (photo 1).

The 2 front seats were fitted with shoulder harnesses, while the rear triple seat had lap belts anchored directly to the seat. It could not be determined whether or not the pilot and front passenger were wearing their shoulder harness at the time of impact. All 3 rear passengers were wearing their lap belts when the crash occurred.
The damage to the propeller and engine show that the P&W R985–14B engine was developing power at the time of impact. The flap position was measured from the flap actuator cylinder. An impact mark was found on the cylinder ram, indicating that the flaps were lowered at 24.5 °. Normally the flap position on take–off is 35 °.
The landing gear selector mounted on the floor, to the right of the pilot, was in 'UP' position, but at the accident site, the wheels were found in the down and locked position. The Flight Supplement states that the normal landing gear retraction cycle takes about 20 to 30 seconds after the selector is placed in the ‘UP’
position.
Weather
At 1000, the weather conditions were as follows: temperature 14.5°C, dew point 13.9°C, winds from the east–northeast, 080° magnetic at 7 knots, broken clouds at 4000 feet agl, overcast at 8000 feet agl, visibility 8 statute miles in rain showers and altimeter setting 29.65 inHg. Due to his increased workload, and higher priorities immediately following the accident, the FSS was unable to make a weather observation at 1100.
Pilot Information
The pilot was certified and qualified for the flight in accordance with existing regulations. He held a valid Canadian commercial pilot – aeroplane licence. In total, he had approximately 3800 flying hours, including about 1000 hours on DHC–2. On 18 July 2009, the pilot had his annual in–flight training on the amphibious DHC–2. Also, this training was to be renewed before 1 August 2010.
The pilot held the following positions in Nordair Québec 2000 Inc.: operations manager, chief pilot, maintenance control system manager and maintenance coordinator.
There was no evidence that incapacitation, physiological or psychological factors affected the pilot's performance.
Carrier Information
Nordair Québec 2000 Inc. holds a valid operating certificate. The carrier's base of operations was La Grande–Rivière Airport. At the time of the occurrence, it was operating a fleet of 3 aircraft: a DHC–2 Beaver, a DHC–3T Turbo Otter and a Piper Navajo PA–31. The aircraft were operated under Part VII, Subparts 2 and 3 of the Canadian Aviation Regulations (CARs). At the time of this occurrence, the aircraft was being operated under Subpart 3. Footnote 2
Aircraft Information
The DHC–2 Mk. 1 is a single–engine piston aircraft used widely in bush flying operations. It can be used on wheels, skis or floats or in amphibious configuration (wheels/floats). The C–FGYK was purchased by the carrier in February 2009. It was built in 1951, and the log book indicated that as of 22 July 2010, it had accumulated 23 886.9 airframe hours since new. The last 100–hour inspection was completed on 5 July 2010, when the aircraft had 23 808.3 hours. After that date, there were no deficiencies reported in the log book.
The aircraft was not equipped with on–board recorders, nor were they required by regulation. Without recorders, it was difficult to establish the sequence of events that led to the accident.
Weight and Balance Report
On 29 May 2009, Wipline model 6000A amphibious floats were installed. Also, airframe modifications Footnote 3 were made to increase the maximum allowable take–off weight to 5600 pounds. A new weight and balance report was done, resulting in a dry weight of 3778.10 pounds. According to the Aircraft Flight Manual Supplement Footnote 4 issued with this modification, the centre of gravity (CG) should be between −2.6 inches and −6.11 inches from datum. Footnote 5
The carrier's weight and balance report form was not amended after the new amphibious floats were installed, and it contained an error in the forward CG limit, which was −1.25 inches for amphibious float configuration. Footnote 6 The aft CG was the same in both float configurations, i.e., −6.11 inches.
Subsection 703.37(1) of the CARs states that no person shall operate an aircraft unless, during every phase of the flight, the load restrictions, weight and CG of the aircraft conform to the limitations specified in the aircraft flight manual. Nordair Québec 2000 Inc. used an approved pilot self–dispatch system. Under this system, pilots are required to do weight and balance calculations before every flight. Where possible, the pilot should leave a copy of the weight and balance report at the point of departure. No report was found for this flight.
The carrier operations manual Footnote 7 states that the aircraft take–off weight must be reduced to 5300 pounds when carrying a canoe as external cargo, and that the total take–off weight of the aircraft must be reduced by twice the total weight of that external payload. Since the canoe being transported weighed 70 pounds, the maximum allowable take–off weight of 5300 pounds should have been reduced by 140 pounds. Consequently, the maximum allowable take–off weight for this particular flight was 5160 pounds.
To determine as accurately as possible the weight of the aircraft on take–off, the baggage was recovered on the evening of the accident and left under supervision in a dry place. The baggage was weighed during the afternoon of the following day. Together, the baggage and the 6 containers of fuel weighed approximately 900 pounds. The weight of the canoe, 70 pounds, must be added to that figure.
Based on the actual weight of the passengers, and considering the quantity of fuel, the baggage and the canoe on departure, the overall weight of the aircraft was determined to be 6162 pounds, which means it was 1002 pounds overweight. As for the CG, it was at 111.80 inches, or 5.69 inches beyond the CG aft limit (Appendix B).
Information on Triple Seat
The rear triple seat was secured to the floor structure by 6 attachment fittings, 4 at the front and 2 at the rear. Three of the 4 fittings at the front failed, while the 2 rear fittings did not fail but separated from their floor–mounted receptacles. On impact, most of the inertial forces acted in the forward direction and laterally due to the left angle of impact. The rear leg fittings for the triple seat were subjected to tension forces, while the front leg fittings were subjected to compression forces. When the accident occurred, the seat pivoted forward, causing the front fittings to fail in tension. The occupants were propelled forward.
Comparison of the construction of the triple seat with the original drawings, obtained by the owner of the type certificate, Footnote 8 revealed that it met the construction standards, except for the welds and the addition of sheet metal to the rear of the seat back. These deviations from the original drawings did not contribute to the separation of the seat from the floor. The types of materials used, as well as the dimension and thickness of the tube stock, the attachment fittings and the nuts and washers were essentially consistent with the original drawings. Since the seat had no nameplate, it is possible that it was not an original de Havilland seat or that it had undergone substantial repairs over the years.
On original certification of the triple seat, it was designed to hold 3 occupants each weighing 170 pounds, for a total of 510 pounds. When the impact occurred, the 828 pounds of items, not tied down to the floor, shifted forward and pushed against the seat. As a result, the seat would have had to withstand the weight of the passengers in addition to 828 pounds of baggage, for a total of 1435 pounds. The forward shifting of the unsecured baggage considerably diminished the capacity of the seat to remain anchored.
Take–off Performance
The take–off performance of the aircraft was calculated in the conditions that existed at the time of this take–off based on the following elements:
- wind 080° at 7 knots, Footnote 9 resulting in a tail wind component
- certified maximum take–off weight of 5600 pounds in accordance with STC no SA01324CH
- temperature during take–off at 15°C
- elevation of La Grande–Rivière Airport of 640 asl.
The calculations indicate a take–off distance of 1263 feet plus tail wind take–off distance of 918 feet, for a total of 2181 feet, to clear a 50–foot obstruction. Instead of calculating the total weight of the aircraft at the time of the accident, the figures used in the performance calculations were the maximum weight allowable according to Wipaire STC SA01324CH, which is 5600 pounds.
DHC–2 Stall Characteristics
The DHC–2 was built and certificated according to British Civil Airworthiness Requirements (BCAR), as amended on 1 June 1947. When the DHC–2 was certificated in 1948, certification requirements were less stringent than they are today. More recent single–engine aircraft are certificated according to CARs, Part V, Standard 523 or equivalent. CARs require that aircraft be equipped with a stall–warning device to give the pilot a clear and distinctive warning of the impending stall. The DHC–2 is not equipped with a visual or audible stall–warning device, nor was it required for certification at the time.
The DHC–2 flight manual provisions Footnote 10 relating to flight characteristics, and specifically to stall characteristics, state that the aircraft is easy to fly and controllable all the way to the stall. Stalling is gentle in all normal conditions of load and flap configuration, and it is preceded by a slight vibration that increases when the flaps are extended. Aircraft pitch changes if there is no yaw. If the yaw is not controlled, the aircraft tends to roll. Corrective action must be taken quickly to prevent the roll from developing.
Aeronautical Testing Service Inc. (ATS), in Washington, U.S.A., is an aviation consulting and manufacturing firm mainly involved in designing, developing and manufacturing modifications for general aviation aircraft. ATS did flight tests with an unmodified DHC‑2 Mk. 1 as part of the design process for a vortex generator for this aircraft type. The aim of the tests was to evaluate the stall characteristics, stall warnings and stall control in accordance with the BCAR.
The flight test report indicates that the test aircraft's stall characteristics were acceptable with a forward CG. However, with an aft CG and power, incipient stalls with 60° of roll, 30° to 40° of yaw, and 30° of pitch occurred often on these flight tests. The ATS flight test report indicates that, with flaps set for the climb, take–off or landing, the ailerons and rudder were effective until the aircraft stalled but were not effective in controlling abrupt roll or yaw after the stall occurred.
Carrying External Loads
Carriage of external cargo by a commercial carrier in Canada must be evaluated and approved by Transport Canada (TC). On 9 June 2009, to allow the in–flight assessment to be done, TC issued a permit for experiment flights over a period of 30 days. Flight Test Plan 093023 from JCM Aerodesign Ltd. was used. One of the restrictions stipulated in the experiment flight permit was that the canoe could not exceed 150 pounds in weight, 14 feet in length and 42 inches in width.
Further, in accordance with TC's Advisory Circular 500–004, Footnote 11 the maximum allowable take–off weight should be reduced to 5300 pounds when a canoe is carried or to 5000 pounds when 2 canoes are carried.
Section 703.25 of the CARs provides as follows: “except where carriage of an external load has been authorized in a type certificate or supplemental type certificate (STC), no air operator shall operate an aircraft to carry an external load with passengers on board.”
The Minister issued an exemption to CARs 703.25, which was to be in effect until 31 December 2010 at 2359 hours.
To be eligible for this exemption, the air operator must first register their intended use of the exemption, prior to engaging in the carriage of external loads under the authority of this exemption, by providing specified information. Even though the carrier had conducted the flight tests, it had not submitted any documents for approval.
Consequently, it was not authorized to carry external loads. However, the operations manual Footnote 12 states that DHC–2 aircraft C–FGYK is approved under a limited STC to carry canoes as external cargo. This amendment was approved by TC on 1 March 2010, despite the fact that no STC had been issued for this aircraft.
Transport Canada Regulatory Oversight
TC's Commercial and Business Aviation (CBA) Division is responsible for the oversight of commercial air operations that fall under CARs 700. The CBA has an Air Operator Certification Standards Unit (AOCSU) responsible for handling applications for new operations and for changes to existing operations. It also ensures that air operators meet the required standards according to the Commercial Air Service Standards Unit (CASSU).
The AOCSU monitors day–to–day operations to ensure that the company is conducting business in accordance with its Air Operator Certificate (AOC). It also exchanges information on related issues, as required. Also, the AOCSU ensures that commercial air operators comply with the Commercial Air Service Standards (CASS).
Also, the CASSU ensures compliance oversight through formal audits, inspections and pilot proficiency checks. Each air operator has an assigned principal operations inspector (POI) who monitors the company's operations. The activities of the POI are governed by the Air Carrier Inspector Manual (ACIM), TP 3783.
In 2003, TC's CASSU assigned Nordair Québec 2000 Inc. a POI who carried out the regulatory oversight of the company through e–mails, telephone conversations, and routine visits to the air operator's La Grande–Rivière and Radisson facilities.
One of the various types of audits performed by TC is the program validation inspection (PVI), which is a process comprising a targeted inspection of one or more aspects of an organization that is, or is not, required to have a safety management system (SMS) and another one that targets inspections of an organization that is in the process of introducing an SMS.
Program validation inspections are carried out at regular intervals and take into account risk indicators to adjust the frequency, if necessary. The PVI may include an examination of one item in particular or an evaluation of one person according to established standards. A TC inspection can result in major consequences, including the cancellation of an air operator certificate.
Following a PVI, a score from 1 to 5 is assigned. Two PVIs took place: a maintenance PVI in 2009 and an operation PVI in 2010. During the maintenance PVI in 2009, the air operator was given a score of 2 because its quality assurance system was deemed ineffective.
It was up to the convening authority to decide what type of monitoring to apply. Subsequently, the decision–maker selected enhanced monitoring.
When a score lower than 3 is assigned, or if there are major findings of non–conformance, TC manages the risk associated with the findings by asking the certificate holder to submit a detailed corrective action plan that addresses these findings.
Since 2003, Nordair Québec 2000 Inc. has been audited several times by TC, which conducted
- 2 regulatory audits of operations;
- 2 regulatory audits of maintenance;
- 4 operations ramp inspections;
- 3 maintenance ramp inspections;
- 1 maintenance PVI; and
- 1 operations PVI.
Conducted over a period of 7 years, these audits revealed the following: 20 cases of operations non–conformance, 16 cases of maintenance non–conformance, and 38 cases of non–conformance with respect to aircraft condition. It should be noted that the 38 cases of non–conformance observed by TC inspectors included
- personnel training;
- flying with uncorrected mechanical deficiencies;
- absence of baggage tie–down devices (4 times);
- non–compliance related to log–book entries;
- aircraft maintenance status;
- non–compliance with Maintenance Control Manual procedures; and
- ineffective quality assurance system.
Each time, a corrective action plan was submitted to TC, and each time the plans were approved. Nevertheless, subsequent inspections revealed that similar anomalies were recurring.
Aviation Enforcement Philosophy
TC's aviation enforcement policy recognizes that "voluntary compliance" with the regulations is the most progressive and effective approach in achieving aviation safety. It is assumed that members of the aviation community share an interest, commitment and responsibility with regard to aviation safety, and that they will perform their activities showing common sense, responsibility and respect for others.
However, TC believes that there are individuals in the aviation community who are less motivated by common sense, personal and civil responsibility, pride and professionalism, and especially safety. It is these individuals who are the focus of enforcement action.
TC is committed to enforcing the regulations fairly and firmly, while encouraging communication between the alleged offenders. Also, TC offers "oral counselling" for minor violations where there is no threat to aviation safety, and it also informs offenders of their right to have penalties reviewed by the Transportation Appeal Tribunal of Canada (TATC). TC also ensures that strict measures are taken against repeat offenders and those displaying flagrant disregard for aviation safety.
Since 2003, the Enforcement Section has received 3 Detection Notices concerning Nordair Québec 2000 Inc., all of which have resulted in financial penalties.
The following laboratory reports were completed:
- LP127/2010 – Flight instruments analysis
- LP128/2010 – Flap actuator analysis
- LP177/2010 – Triple seat analysis
- LP178/2010 – Propeller analysis.
Analysis
Although the winds favoured runway 13, the pilot elected to take off from runway 31. While a tail wind component increased the take–off distance, the runway length available was sufficient for a take–off at the maximum allowable weight, even from intersection Bravo. It was unusual for C–FGYK to use the full length of runway 31 for a take–off. It is likely that the pilot allowed for the effect of the tail wind component on the take–off distance, and that he knew he was overweight. Not having weighed the baggage, the pilot could not know the precise weight and balance status of the aircraft on take–off.
It is not known why the pilot did not weigh or secure the baggage. Weight and balance calculations confirm that the aircraft was overweight on take–off and that its centre of gravity (CG) was aft of the limit prescribed in the STC on the installation of new amphibious floats. In such a case, the stall speed was higher and the stall characteristics caused changes of altitude which are hard to counteract, making recovery difficult.
Further, the aft CG reduced the distance between the CG and the centre of pressure of the vertical stabilizer, thereby decreasing the effectiveness of the rudder and making recovery more difficult. Although a stall warning device would have alerted the pilot to the impending stall, with the CG beyond the aft limit, the aircraft pitched up quickly. When the aircraft was out of the ground effect, it stalled at an altitude that did not allow the pilot to execute the recovery manoeuvre.
Although the carrier did flight tests in order to apply for authorization to carry external loads, it did not file the required documents for approval. Thus, the carrier did not have approval to carry a canoe, although the section of its operations manual relating to external loads was approved by TC. Moreover, as stated in the flight test documents, the dimensions of the canoe exceeded the limits specified in the approval document. The aerodynamic effects of carrying a canoe longer than the limit allowed by the experiment flight permit are unknown. Operating an aircraft outside the limits and conditions under which a permit is issued can increase the risk of an accident.
The construction and installation of the triple seat was, with few exceptions, consistent with the manufacturer's original drawings and allowed it to withstand some impact forces. However, the forward shift of the unsecured baggage was a major contributing factor in the injuries sustained by the 3 rear–seat passengers, who were propelled towards the cockpit when their seat pivoted forward.
Since 2003, TC has performed inspections and audits of the company's facilities and the results indicated several findings of non–conformance. Although in each of these cases, a corrective action plan was submitted to and approved by TC. However, the same anomalies were again observed in subsequent inspections, in spite of previous monetary penalties. For example, TC inspectors have noted on 4 occasions that the baggage tie–down system was not installed or not used, as was the case in this accident.
Given Nordair Québec 2000 Inc.'s latest evaluation score and the 3 previous Detection Notices, it is obvious that enhanced monitoring would have resulted in an in–depth analysis of their management, in addition to targeting repeated deficiencies. The action taken by TC did not have the desired outcomes to ensure regulatory compliance; consequently, unsafe practices persisted.
Although the flight services specialist activated the crash alarm upon receiving the ELT signal, and the prevention officer on duty immediately headed for the site, the officer could not get close to the wreckage. Because the aircraft crashed outside the airport property limits, the Municipality of Radisson was responsible for responding. Given that the regular rescue crew's response time was about 45 minutes, and that the 911 call was made about 10 minutes after the crash, it is estimated that it took at least 55 minutes for the first responders to arrive. Like the airport prevention officer, the first responders were unable to get close to the wreckage with their vehicle. It was necessary to use a helicopter. The assistance provided to the 3 rear–seat passengers by the 2 persons who went to the site before the arrival of the first responders probably saved them from drowning.
Findings as to Causes and Contributing Factors
- The aircraft was overloaded and its centre of gravity was beyond the aft limit. The aircraft pitched up and stalled at an altitude that did not allow the pilot to execute the stall recovery manoeuvre.
- The baggage was not secured. Shifting of the baggage caused the triple seat to pivot forward, propelling the 3 rear–seat passengers against the pilot and front–seat passenger during impact.
- Although the design of the triple seat met aviation standards, it separated from the floor at the time of impact, principally due to the fact that the heavy cargo shifted.
- The action taken by TC did not have the desired outcomes to ensure regulatory compliance; consequently, unsafe practices persisted.
Finding as to risk
- Operating an aircraft outside the limits and conditions under which a permit is issued can increase the risk of an accident.
Other Finding
- The carrier's operations manual had been approved by Transport Canada for the carriage of external loads despite, despite the fact that the carrier did not have the required supplemental type certificate (STC).
Safety Action Taken
NAV Canada
Following the accident, unit staff received updated procedures and checklists to follow in the event of a crash. Emphasis was placed on calling 911 as soon as possible, as well as performing meteorological observations after an accident. In addition, the button assigned to 911 on all unit telephones was coloured red to facilitate and expedite calling 911.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on . It was officially released on .
Appendices