Stuck elevator control
Exploits Valley Air Services Limited
Hawker Beechcraft 1900D, C-GLHO
Gander, Newfoundland and Labrador
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 10 December 2011, at 1028 Newfoundland and Labrador Standard Time, an Exploits Valley Air Services Hawker Beechcraft 1900D aircraft (registration C-GLHO, serial number UE-266), operating as Air Canada Express flight EV7645, was conducting a scheduled passenger flight from Gander to Goose Bay, Newfoundland and Labrador, with 2 crew members and 13 passengers on board. After the crew began the take-off roll on Runway 21, they noted that the control column was stuck in the full forward position. The take-off was rejected, and the aircraft was taxied back to the terminal. The aircraft was not damaged, and there were no injuries.
1.0 Factual information
1.1 History of the flight
On 08 December 2011, at about 0100Footnote 1, the occurrence aircraft was towed out of the hangar in Gander, Newfoundland and Labrador, by company maintenance personnel and parked with its nose facing east, on the ramp adjacent to the hangar. During the time that the aircraft was parked outside, it was exposed to winds out of the west of greater than 30 knots, with gusts exceeding 50 knots. The aircraft remained there until about 0400 on 10 December 2011, when it was towed back into the hangar for a daily maintenance inspection (DI).
After completing the DI, company maintenance personnel towed the aircraft outside and parked it on the ramp. The recorded winds were not significant at this time. Later that morning, the first officer conducted a pre-flight inspection of the aircraft. The crew carried out the aircraft run-up at the hangar, then taxied to the terminal, where the passengers boarded. The crew then carried out the pre-flight checks. While reading through the checklist, in the After-Start Checks section, they verbally confirmed that the flight controls were checked.Footnote 2
During the take-off roll, upon reaching the rotation speed of 112 knots, the crew could not pull the control column aft from the full forward position. The take-off was rejected at 119 knots, with more than 7000 feet of runway remaining. After the passengers were deplaned, the crew taxied the aircraft back to Exploits Valley Air Services' (EVAS) hangar.
While taxiing, the crew attempted to pull back on the control column, and when using additional force, managed to free it. However, the overall elevator movement was now restricted, such that full nose down could no longer be achieved.
The flight crew were unaware that when difficulties in controlling the aircraft are encountered owing to any aircraft system malfunction, the incident must be reported to the Transportation Safety Board of Canada (TSB). Therefore, they did not disable the applicable circuit breakers to ensure that the data from the cockpit voice recorder (CVR) and flight data recorder (FDR) would be preserved.
1.2 Injuries to persons
| Injuries | Crew | Passengers | Others | Total |
|---|---|---|---|---|
| Fatal | 0 | 0 | 0 | 0 |
| Serious | 0 | 0 | 0 | 0 |
| Minor/None | 2 | 13 | 0 | 15 |
| Total | 2 | 13 | 0 | 15 |
1.3 Damage to aircraft
Damage was noted on the bob-weight, the aft face of the bob-weight bellcrank mounting structure, and the stop-bolt bracket. The face of the stop-bolt bracket was deformed rearward and to the right (see section 1.6.2).
1.4 Other damage
There was no other damage.
1.5 Personnel information
The flight crew members were certified and qualified for the flight in accordance with existing regulations. They were within the required duty periods, and fatigue was not considered a factor. The captain had accumulated approximately 4730 hours of total flying time, which included 3976 hours on the occurrence type. The first officer had accumulated approximately 2360 hours of total flying time, which included 1460 hours on type.
1.6 Aircraft information
1.6.1 General
The Hawker Beechcraft Corporation (HBC) 1900 (B1900) is a 19-passenger, pressurized, twin-engine turboprop aircraft that is designed, and primarily used, as a regional airliner. In Canada, there are 63 B1900D and 28 B1900C modelFootnote 3 aircraft, registered to 18 different operators.Footnote 4
The occurrence aircraft was built in 1997, and had accumulated 29 040.5 flight hours and 33 661 cycles. Records indicate that the aircraft was certified, equipped, and maintained in accordance with existing regulations and approved procedures. There were no known deficiencies before the occurrence flight. No maintenance had been performed on the elevator control system between the last flight and the occurrence flight. The investigation determined that the aircraft's weight and centre of gravity were within the prescribed limits.
1.6.2 Elevator control system
The B1900 elevators are manually controlled through a cable, pulley, bellcrank, and push-rod system, and are operated by conventional control wheels interconnected by a T-shaped control column. The base of the “T” column is connected by a push rod to the forward elevator bellcrank. The elevators are connected to the aft elevator bellcrank by push rods. Cables are installed between the forward and aft elevator bellcranks. A downspring and elevator stabilizing weight (bob-weight) system are incorporated for improved stability.
The primary control stops are located at the elevators; elevator up-travel is limited to 20° +1°/−0, and down-travel is limited to 14° +1°/−0°. Due the combined force of the bob-weight system and the downspring (acting on the aft elevator bellcrank), the elevators of a static aircraft will rest on the primary down-stops.
Secondary control stops are located at the forward elevator bellcrank. Pulling or pushing the control column beyond the primary control stop positions causes the elevator cables to stretch. Continued movement of the control column will result in the secondary stops making contact.
The bob-weight system (Figure 1) incorporates a bob-weight bellcrank assemblyFootnote 5 (item 1), which is connected to the co-pilot's portion of the control column through a link assembly (item 2).
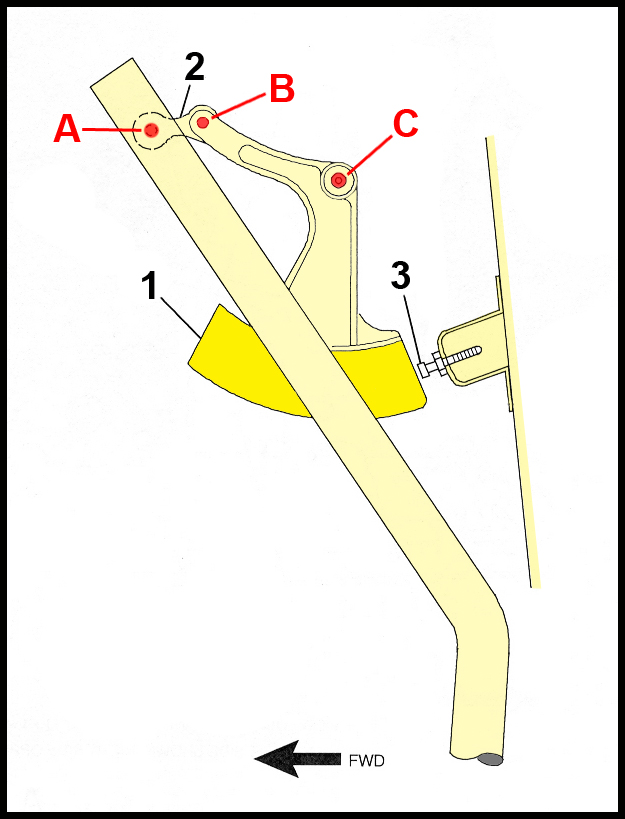
This bellcrank pivots within an enclosed mounting structure (not shown). When the control column is moved forward, the link assembly is pulled forward, causing the bob-weight to pivot rearward. A bob-weight stop bolt (stop bolt; item 3) is installed to limit the bob-weight's rearward travel. HBC has indicated that there are a number of rigging adjustments that affect the extended length of the stop bolt. The maximum extended length is 1.70 inches.Footnote 6 The clearance between the stop bolt and the contact surface of the bob-weight is measured with the elevators resting on the primary down-stops.Footnote 7 As designed, the stop bolt does not align with the centre of the bob-weight; it is offset closer to the left edge.
Under normal operating conditions, with the elevator system rigged as per the manufacturer's instructions, the bob-weight does not come in contact with the stop bolt. Contact between the bob-weight and the stop bolt can occur when the control column is pushed beyond its normal range of travel. Once contact is made with the secondary control stop, continuing to push the column forward causes the vertical portion of the “T” column to flex, and allows further bob-weight movement toward, and including, contact with the stop bolt. This effect was demonstrated by TSB investigators on an exemplar aircraft.
The design of the bob-weight system is such that the further rearward the bob-weight travels, the more aligned the link assembly attachment points (items A and B) become with the bellcrank pivot point (item C). Under normal operating conditions, these 3 points are not aligned, thereby providing an over-centre protection. If completely aligned, then it is possible that the link could go over centre. When the link goes over centre, the geometry of the link assembly attachment points is changed, and elevator travel becomes limited;Footnote 8 full nose-down movement cannot be achieved. FDR data from the occurrence aircraft show that, after the crew freed the elevator controls, the control-column forward movement was restricted to a position corresponding to about 6.7° nose-up.
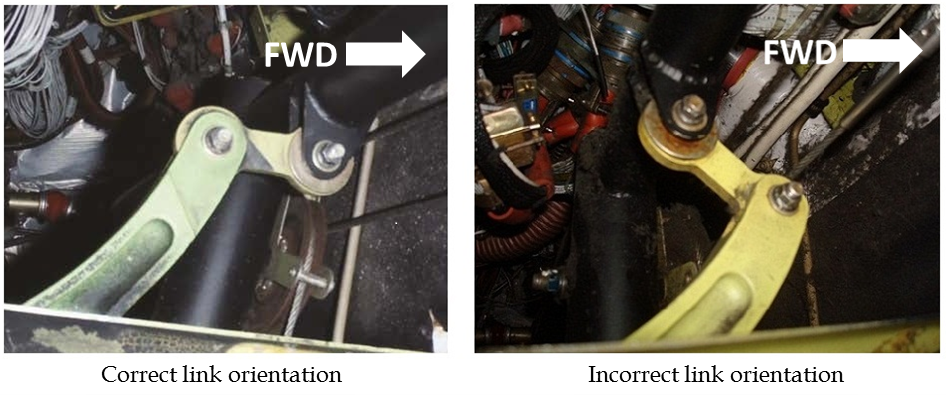
EVAS's maintenance department examined the occurrence aircraft, and noted that the bob-weight system's link had gone over centre (Photo 1). Damage was noted on the bob-weight, the aft face of the bob-weight bellcrank mounting structure, and the stop-bolt bracket. The face of the stop-bolt bracket was deformed rearward and to the right, causing the stop bolt to be deflected to the right. No damage was noted on the elevator primary or secondary control stops, or on any other component of the elevator control system.
EVAS reported that the bob-weight bellcrank pivot bolt holes in the bellcrank mounting structure were elongated. According to HBC, the hole diameter is 0.250 to 0.254 inches. The TSB measured the holes on the occurrence aircraft's bellcrank mounting structure; the left hole's diameter was 0.254 inches, the right hole's diameter ranged from 0.254 to 0.256 inches due to the elongation.
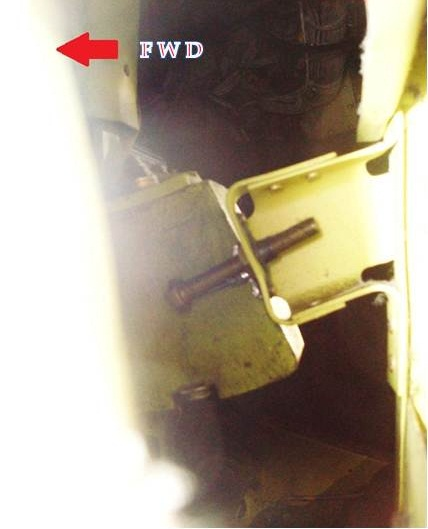
EVAS repositioned the bob-weight by flexing the stop bolt to the left and moving the bob-weight rearward beyond its normal range of travel (Photo 2). Once aligned, the damage was noted to be consistent with the bob-weight scraping the side of the stop bolt.
EVAS filed a service difficulty report (SDR) with Transport Canada (TC); the SDR described the incident, included photographs of the components, and identified that the bob-weight had jammed on the stop bolt before the link had flipped over.Footnote 9 The SDR also stated that the stop-bolt contact point was offset to the left side of the bob-weight, and that if the stop bolt was oriented in the centre of the bob-weight, it would have prevented the weight from travelling beyond its normal range.Footnote 10
EVAS did not recognize this occurrence as a reportable incident;Footnote 11 therefore, it did not notify the TSB. The TSB learned of the occurrence on 13 December 2011, after being contacted by TC. By the time the TSB was notified, repairs had already been undertaken, so it was not possible for TSB investigators to examine the occurrence aircraft's elevator control system in situ.
1.6.3 Bob-weight examination
The B1900 bob-weight material composition is a lead alloy with antimony specifically added to the lead to increase its hardness.Footnote 12
The occurrence aircraft's bob-weight was forwarded to the TSB Laboratory. The weight was found to be slightly lighter than the manufacturer's specification. HBC did not consider the weight difference to be significant.
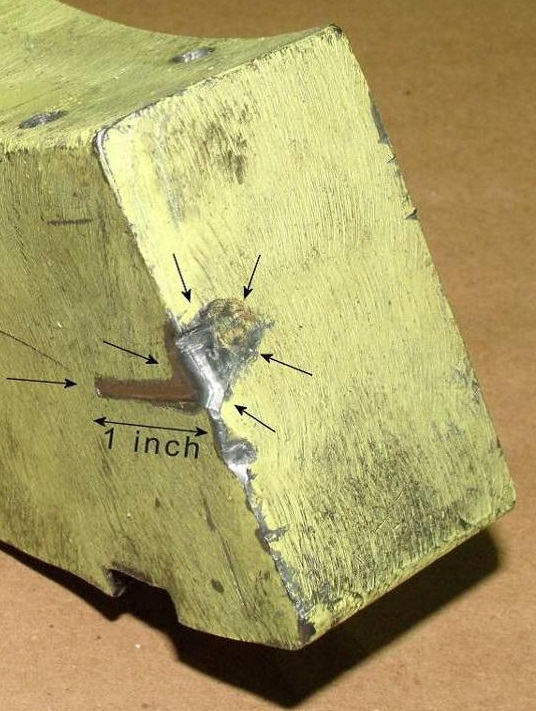
Examination of the bob-weight showed that there were multiple imprints caused by the stop bolt, and these imprints exhibited progressive movement toward the left edge. When the stop bolt contacted the bob-weight at the edge, it was forced over and slid down the side of the bob-weight for approximately 1 inch (Photo 3).
A bob-weight from another operator's aircraftFootnote 13 was also forwarded for examination. This bob-weight had a 0.50-inch-deep imprint, as a result of the bob-weight repeatedly striking the stop bolt. The operator filed a SDR, which indicated that the bob-weight had a groove worn down the side that was caused by the stop bolt.Footnote 14 The bob-weight did not meet the manufacturer's specified values for antimony content or hardness. HBC had previously identified a suspect lot of lead parts, including the B1900 elevator bob-weight, which did not meet the design specification. HBC conducted an engineering analysis, and determined that the suspect B1900 elevator bob-weights did not pose a safety issue; no follow-up action was planned.
1.6.4 Flight controls gust locks
The flight controls gust locksFootnote 15 (control locks) are installed with the pilot's control wheel in the full forward position and rotated approximately 15° to the left.
A review of the Airliner Maintenance Manual (AMM) identifies multiple references to the removal of control locks, requiring that they be fully removed before the aircraft is started, and that the control locks be removed before towing the aircraft to prevent damage to the steering linkage. The AMM also contains multiple references requiring that control locks be installed for flight-ready storage, as well as for mooring in high winds.
In HBC Safety Communiqué No. 1, issued March 2008, Paragraph 2.A and B suggest:
- During pre-flight of your airplane, inspect to be sure the control gust locks are not installed prior to take-off. If installed, remove prior to take-off.
- Prior to take-off roll the ailerons, flaps, elevators and rudders should be activated through their complete travel to insure they are not restricted for any reason. Any cause for restriction should be removed prior to take-off.
EVAS did not have documented maintenance procedures for the removal/installation of the control locks when towing an aircraft. Its practice was to follow the AMM instructions; however, the investigation determined that the control locks were not consistently installed after parking the aircraft.
EVAS's B1900D standard operating procedures (SOP), as well as HBC's Airplane Flight Manual (AFM), requires that the control locks be installed as part of the after-shutdown procedures.
EVAS's practice was to follow the SOP; however, the investigation determined that the control locks were not consistently installed after shutting down the aircraft.
1.7 Meteorological information
Gander weather reported at the time of the occurrence was suitable for the intended flight, and is not considered a factor in this occurrence.
1.8 Aids to navigation
Not Applicable (N/A)
1.9 Communications
N/A
1.10 Aerodrome information
Gander International Airport (CYQX) is a registered aerodrome located in controlled airspace, at an elevation of 496 feet above sea level. The airport has 2 intersecting runways; Runway 31/13 is 8900 feet long, and Runway 21/03 is 10 200 feet long.
1.11 Flight recorders
The aircraft was equipped with a L3 CommunicationsFootnote 16 Model A100S CVR, capable of storing the last 30 minutes of cockpit sounds, and a L3 Communications Model F1000 FDR, capable of storing 115 hours of flight data. The FDR met the applicable requirements of the Canadian Aviation Regulations (CARs) Part VI, Standard 625.33, Schedule I.EVAS maintenance staff removed the CVR and the FDR, and forwarded them to the TSB Laboratory with the occurrence data intact.
The elevator control position is the only primary flight-control datum that is recorded on the FDR. The elevator position data are obtained by a sensor that is attached by a linkage to the base of the control column. The sensor is calibrated so that the position of the control column is associated to an elevator surface position. The sensor is designed to measure beyond the elevator's normal range of travel, and the FDR is capable of recording this movement. At the start of the occurrence flight, with the elevators resting on the primary control stops, the FDR recorded the elevator position as 15.7°. All previous recorded flights recorded the elevator position as 14.6°.
1.12 Wreckage and impact information
N/A
1.13 Medical and pathological information
N/A
1.14 Fire
N/A
1.15 Survival aspects
N/A
1.16 Tests and research
N/A
1.17 Organizational and management information
1.17.1 Company
EVAS is a CARs704 operator.Footnote 17 It is a “Tier III”carrier under a commercial agreement with Air Canada providing propeller aircraft with a maximum seating capacity of 19 seats, and operates as Air Canada Express.Footnote 18 It offers several daily flights within Newfoundland and Labrador, and Quebec.
EVAS began scheduled passenger service in 2004 with one B1900D aircraft. Two more B1900D aircraft were added in 2010, when a courier service from Newfoundland and Labrador to Nova Scotia and New Brunswick was introduced. Two more B1900D aircraft were added in 2011 to support growth as a contractor with Air Canada. Between 2005 and the end of 2011, company staff had increased by over 50%, growing from 33 to 51 employees. At the time of the occurrence, EVAS management was focused on operational priorities,Footnote 19 to meet Air Canada's requirement to increase the number of flights on its existing routes, scheduled to start in February 2012.
1.17.2 Exploits Valley Air Services flight safety program
EVAS utilized a flight safety program (FSP), which combined the components of a FSP with those of a quality assurance program. The Company Operations Manual (COM) describes the FSP as a systematic, explicit, and comprehensive process for the management of safety risks that integrates operations and technical systems with financial and human resource management for all activities related to the air operator's operating certificate. All employees were required to adopt the standards and procedures set forth in the FSP.
The flight safety program manager (FSPM) was responsible for managing the FSP. The FSPM's responsibilities included:
- monitoring and advising on all air-operator flight-safety activities that may have an impact on flight safety;
- establishing a reporting system that provides for a timely and free flow of flight-safety-related information;
- conducting safety surveys and internal safety audits;
- soliciting and processing flight safety improvement suggestions;
- developing and maintaining a safety awareness program;
- monitoring industry flight-safety concerns that may have an impact on air-operator operations;
- maintaining close liaison with aeroplane manufacturers;
- maintaining close liaison with TC Civil Aviation Directorate's System Safety offices and the TSB;
- maintaining close liaison with industry safety associations;
- identifying flight safety deficiencies and making suggestions for corrective action;
- investigating and reporting on incidents/accidents, and making recommendations to preclude a recurrence;
- developing and maintaining a flight safety database to monitor and analyze trends;
- making recommendations to the air operator.
At the time of the incident, the FSPM also held positions as Chief Pilot, Coordinator of Transportation of Dangerous Goods, and Coordinator of Flight /Ground Operations, as well as conducting line pilot duties.
The FSP did not have full-time dedicated employees. A flight safety committee was required to monitor all areas of operation, identify safety concerns and deficiencies, and make recommendations to senior management for corrective actions where applicable.
The Flight Safety Committee consisted of representation from the:
- Flight Safety Program Manager (Chairperson)
- Company Training/Check Pilot (Flight Operations)
- Maintenance Engineer/Apprentice (Maintenance Operations)
- Ground Operations Coordinator (Ground Operations)
- Chief Flight Instructor (Flight School Operations)
- Administrative Assistant (Secretary)
This committee was required to meet at least 4 times per year and to keep minutes detailing all items discussed, decisions and corrective actions to be taken, assignment of tasks, and due-dates of tasks. If an urgent matter arose, any of the committee members could call for a special meeting.
The meetings were referred to as Management/Safety Quarterly meetings, and the minutes kept were brief and reflected a priority on production and operational concerns and on occupational safety and health-related concerns. Operational incident reports were reviewed using an approach to safety management that relied primarily on regulatory compliance and on reacting to undesirable events by identifying the underlying causes and prescribing specific measures to prevent their recurrence.
EVAS carried out 4 Management/Safety Quarterly meetings in 2010 and 2 in 2011. No special meeting was called to review the occurrence flight.
1.18 Additional information
1.18.1 Similar occurrences
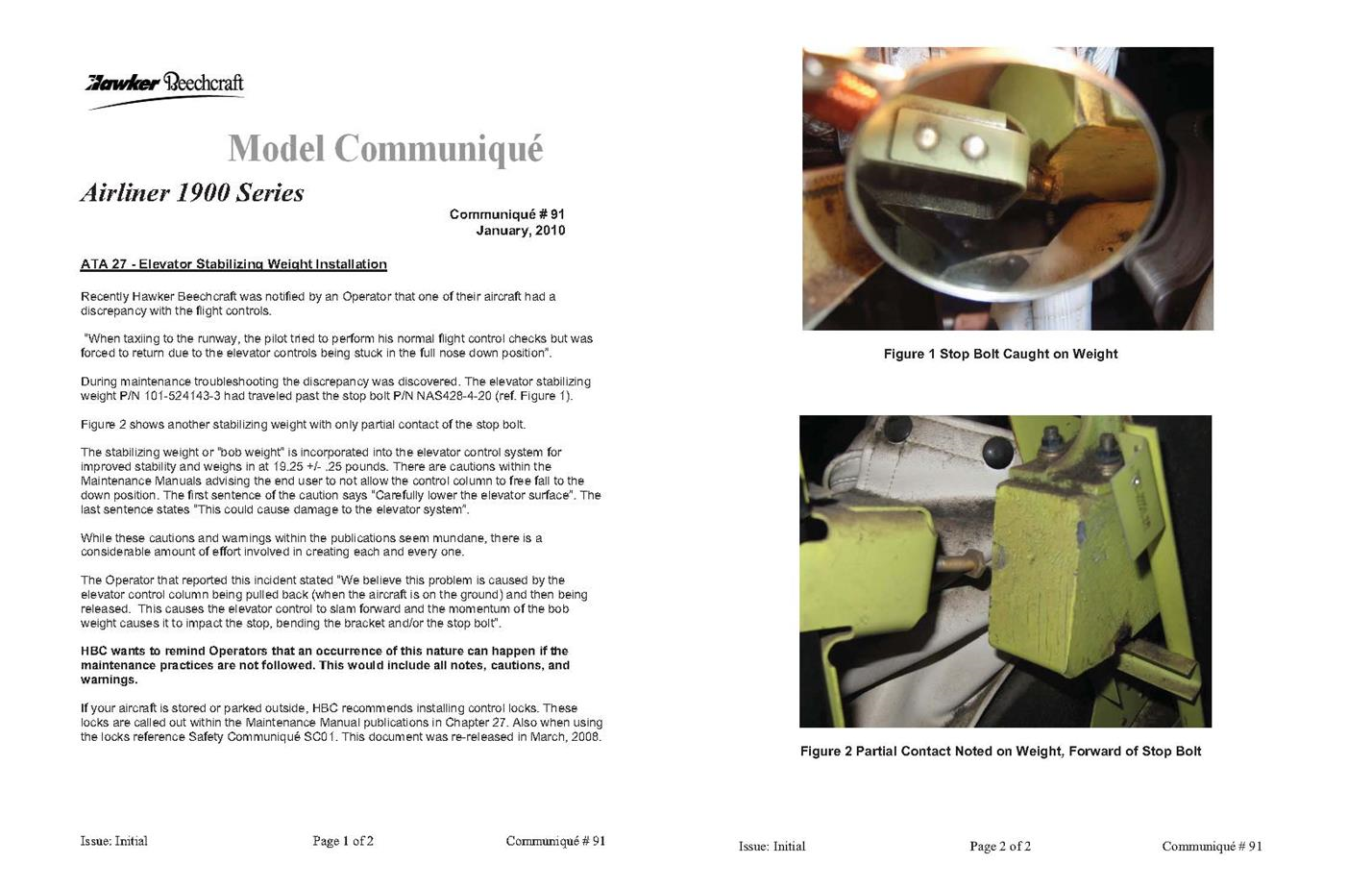
In January 2010, HBC issued Model Communiqué #91 to advise readersFootnote 20 that it had been notified by an operator that one of its aircraft had experienced a discrepancy with the flight controls (Appendix B).Footnote 21 The operator reported:
When taxiing to the runway, the pilot tried to perform his normal flight control checks but was forced to return due to the elevator controls being stuck in the full nose-down position.
Subsequent examination by the operator found that the bob-weight had travelled beyond the stop bolt and become stuck. The operator believed that:
…this problem is caused by the elevator control column being pulled back (when the aircraft is on the ground) and then being released. This causes the elevator control to slam forward and the momentum of the bob weight causes it to impact the stop, bending the bracket and/or stop bolt.
On 11 November 2011, a Pacific Coastal Airlines (Pacific Coastal) B1900C (C-GPCY) was taking off from Runway 08L at Vancouver with 2 crew members and 11 passengers on board.Footnote 22 The first officer was the pilot flying (PF), and the captain was the pilot not flying (PNF). During the take-off roll at about rotation speed, the control column could not be pulled aft from the full forward position. The PF subsequently jerked on the control wheel, which resulted in a loud bang and a significant vibration of the glare shield. The control column could now be moved, and the PF positioned it to establish a normal climb attitude. When the PF moved the column forward to level off, it was noted that forward elevator travel was now restricted to about the neutral position. The PF then passed control to the PNF. With the use of elevator trim and by manipulating the engine power settings, the crew conducted a flapless landing.

This flight was this aircraft's fourth of the day. Between the third flight and the occurrence flight, the aircraft had been parked on the apron, with its tail into the wind, for about 2 hours. During this time, the wind, which was gusting in excess of 40 knots, was blowing the elevators up and down. The aircraft was subsequently repositioned so that it faced into the wind.
When the company examined the aircraft's bob-weight system, it was noted that the left side of the weight had damage that was consistent with the stop bolt scraping along the surface. The aft surface of the bob-weight bellcrank support structure was deformed rearward, and the stop-bolt bracket had been deformed rearward, causing the stop bolt to align closer to the left edge of the bob-weight (Photo 4).
Pacific Coastal filed a SDR, which identified that the position of the bob-weight stop bracket was such that it allowed the bob-weight to periodically slip past the stop bolt.Footnote 23 The company carried out a fleet-wide inspection, and determined that all of its aircraft had the same issue; the stop bolt was aligned such that it only made contact with the left side of the bob-weight. Most of the bob-weights had marks on the left side from making contact with the stop bolt when it travelled beyond its normal range of operation.Footnote 24 This information, as well as the information that on the day of the occurrence flight, the aircraft was exposed to very gusty winds, was provided to HBC on 15 November 2011.
1.18.2 Hawker Beechcraft Corporation's response to occurrences
Model Communiqué #91 included 2 pictures: 1 showing the operator's bob-weight stuck on the stop bolt, and the other showing another bob-weight that had contacted the stop bolt on the left side of the weight (Photo 5). Model Communiqué #91 advised readers that the maintenance manual had numerous cautions advising that the control column should not be allowed to free-fall to the down position, as this free-fall could cause damage to the elevator system. HBC also reminded operators that an occurrence of this nature—the bob-weight becoming stuck on the stop bolt—can happen if the maintenance practices (including the cautions and warnings) are not followed. Although HBC stated that a considerable amount of effort is involved in creating these cautions, they had not performed any testing to determine what, if any, specific system damage(s) would occur if the control column were allowed to free-fall to the down position.

Although not directly related to the elevator control column being pulled back and then being released, Model Communiqué #91 concluded with a reminder about the use of control locks when the aircraft is parked outside.
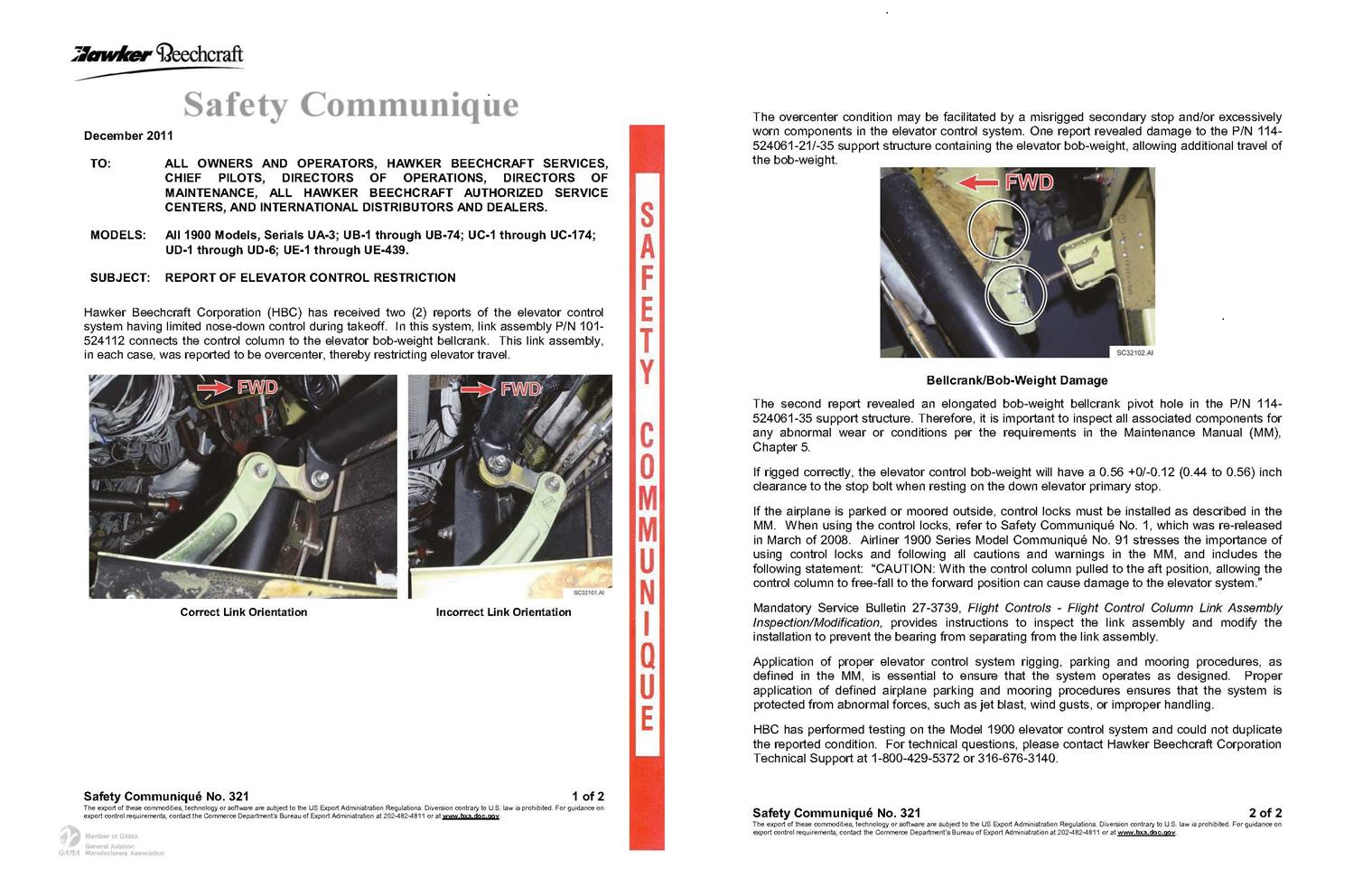
In December 2011, HBC issued Safety Communiqué #321Footnote 25 to advise readersFootnote 26 about its receipt of 2 reports of the elevator control system having limited nose-down control during take-off. In each case, the link was reported to have gone over centre, thereby restricting elevator travel. HBC stated that it had performed testing, but could not duplicate the link going over centre.
Although the safety communiqué referred to the information presented in Model Communiqué #91, it did not clearly state that for the link to go over centre, the bob-weight must travel beyond the stop bolt. The safety communiqué quoted Model Communiqué #91‘s caution regarding not allowing the control column to free-fall to the down position due to the possibility of damage to the elevator system, and provided technical information as to what may have caused the over-centre condition (Appendix C). It also stressed the importance of following the AMM procedures to ensure correct rigging and the importance of inspecting for any abnormal wear or for specific conditions in accordance with the AMM.
The safety communiqué included multiple references to the use of control locks in accordance with AMM procedures, including the following:
If the airplane is parked outside or moored outside, control locks must be installed as described in the MM.Footnote 27
Application of proper elevator control system rigging, parking and mooring procedures, as defined in the MM, is essential to ensure that the system operates as designed. Proper application of defined airplane parking and mooring procedures ensures that the system is protected from abnormal forces, such as jet blast, wind gusts, or improper handling.
Even though Safety Communiqué #321's subject was “Report of elevator control restriction,” the majority of the accompanying text was focused on maintenance-related activities.
After the Pacific Coastal occurrence but before the EVAS occurrence, HBC performed a single test in which the elevators were allowed to free-fall from the full up position. The weight contacted the stop bolt with low force, and no damage or bending of the bob-weight stop bolt was observed.
HBC's follow-up work was focused on reproducing the bob-weight link assembly over-centre condition. Even after removing the complete stop-bolt bracket and deforming the bob-weight bellcrank mounting structure, HBC could not get the link assembly to go over centre by pulling on the control column. Subsequent testing was carried out with the TSB present. When the bob-weight was held in a manner similar to its being retained by the stop bolt, a firm jerk on the control column resulted in the link assembly going over centre. Before this, HBC had not carried out a test by holding the bob-weight and jerking on the control column. Due to the extent of disassembly and the damage done during HBC's testing, it was not practical to reassemble the system and perform a test that would have replicated the initiating event, in which the bob-weight was retained by the stop bolt.
1.18.3 Federal Aviation Administration response
On 23 December 2011, the Federal Aviation Administration (FAA) issued Emergency Airworthiness Directive (AD) 2011-27-51, effective immediately upon receipt.Footnote 28 The FAA issued the AD because it determined that an unsafe condition is likely to exist or develop in other products of the B1900 type design. The AD described the Pacific Coastal and EVAS incidents and identified the unsafe condition as “…the elevator bob-weight (stabilizer weight) travelling past its stop bolt…”, which allowed the attaching linkage to move over centre.
The AD was issued to detect and correct conditions that could result in reduced nose-down elevator control and loss of control of the airplane. A one-time inspection was to be carried out for correct positioning of the bob-weight link, stop bolt to bob-weight clearance, evidence of scraping along the side of the bob-weight, and damage/deformation of the stop-bolt bracket. The AD also required that any discrepancies found in these inspections be reported to HBC and that repairs be completed before further flight.
HBC received reports back from operators of 91 aircraft worldwide; 16 aircraft reported damage on the bob-weight, and 6 aircraft reported damage to the stop-bolt bracket. HBC indicated that Pacific Coastal reported no damage with its aircraft even though they had previously provided photographs showing such damage.
In May 2012, the FAA advised HBC that due to the critical nature of the flight control system involved, a type design change was needed to mitigate the unsafe condition (as stated in AD 2011-27-51) in lieu of relying solely on revised AMM inspection criteria. The design change would have to mitigate the possibility of the bob-weight traveling past its stop.
As of 27 March 2013, HBC has implemented a design change and is working with the FAA to have the certification plan approved.
1.18.4 Bob-weight stop-bolt contact point
After AD 2011-27-51 was issued, the TSB contacted some Canadian B1900 operators to obtain the results of the examinations they carried out and any accompanying photographs. The TSB received information for 49 aircraft from 8 operators, including Pacific Coastal. Stop-bolt impact marks on the bob-weight were noted on 46 of these aircraft, 41 of which occurred left of centre on the bob-weight face.Footnote 29 On 6 of the Pacific Coastal aircraft, damage was noted on the left side of the bob-weight, consistent with the bob-weight going beyond the stop bolt. Some of the stop-bolt brackets had been bent rearward, a few were bent toward the left, and many showed no signs of damage.
Testing was conducted on a B1900D to determine whether the bob-weight would impact the stop bolt when the elevators were allowed to free-fall from the full up position.Footnote 30 The operator conducted the initial test, and noted that the bob-weight impacted the stop bolt, resulting in a small amount of paint being removed from the bob-weight. The TSB carried out a follow-up test on the same aircraft, and observed similar results. With the exception of the small amount of paint removed, no visible imprint was found on the bob-weight.
1.18.5 Hawker Beechcraft Corporation's continued operational safety program
General
In 2007, HBC initiated a continued operational safety (COS) program, which monitors reports of service experience, evaluates whether any such report indicates that operational safety is affected, assesses safety risks, and establishes appropriate resolution of such issues. The various Beechcraft models were integrated into the COS program between 2007 and 2009. Beginning in January 2009, all Beechcraft models, including the Model 1900 series, were included in the COS program. Full use of the COS program by both HBC and the FAA began in January 2010.Footnote 31
Several inputs, such as accident investigation findings, customer reports, quality notifications, and regulator recommendations/notifications, are used to identify hazards. Under the COS program, there is an aircraft-model-specific safety review boardFootnote 32 (SRB) that is responsible for conducting risk assessments, as well as for reviewing and approving issue-resolution proposals. Risk assessment follows the guidelines stated in Appendix VI of the FAA Small Airplane Directorate Airworthiness Directives Manual Supplement (Airworthiness Concern Process Guide).
The SRB evaluates proposed solutions for safety issues, ensuring that the root cause(s) has been determined and that the solution adequately addresses the safety issue.Footnote 33 Once an issue resolution plan has been executed and the issue resolved, the safety issue will be closed. Trend monitoring is carried out for all COS issues that have been closed. If it is found that there is reoccurrence of the issue, the new information will be evaluated, and if the original mitigation plan was not effective, then the issue will be reopened.
In August 2011, HBC began participating in the FAA Manufacturer's Safety Management System (SMS) Pilot Project. In April 2012, HBC successfully completed Level I, and is currently at level II.Footnote 34 As part of HBC's gap analysis for implementation of a SMS, it identified that the current COS program was solely based on reactive safety management; that is, it reacted to reported safety issues.
Initial report of stuck elevator controls
HBC concluded that, based on the information provided by the operator of the aircraft identified in Model Communiqué #91, the cause of the event was improper procedures. Based on this conclusion and on lack of receipt by HBC of any other similar reports, no COS issue was raised, and no formal risk assessment or follow-up was carried out.
Subsequent reports of stuck elevator controls
On 14 November 2011, HBC was notified of the Pacific Coastal occurrence. HBC immediately opened a new COS program issue for the report and began coordinating an investigation. Included in the COS program issue was the information previously identified in Model Communiqué #91. A HBC air safety investigator (ASI) was dispatched to Pacific Coastal's maintenance facility. When the ASI arrived, the aircraft had already been repaired and returned to service. Pacific Coastal advised that no parts had been replaced, and noted that elevator-control secondary stops were not within limits.
On 13 December 2011, HBC was notified of the EVAS occurrence. At this time, the Pacific Coastal COS issue was in the review stage, and HBC's focus was on collecting data to determine how the bob-weight link went over centre. Although the COS program included a requirement for an initial risk assessment, HBC had no record of an initial risk assessment having been performed for this occurrence.
Given that no additional reports of the unsafe condition were reported after HBC's Safety Communiqué # 321, HBC considers that its mitigating strategies have been appropriate and effective in preventing a recurrence of the events reported by Pacific Coastal and EVAS.
1.18.6 Evaluating type certificate holder's recommendations
TC Technical Publication 13094, Civil Aviation Maintenance Schedule Approval Policy and Procedures Manual, states:Footnote 35
It should be noted that the term “type certificate holder's recommendations” is not limited to the basic recommended schedule. Recommendations issued in the form of Instructions for Continued Airworthiness (ICAs) and/or publications issued by the Type Certificate (TC) holder (airframe, engine, or propeller) and the holder of design approvals such as Supplementary Type Certificates (STC), Repair Design Approvals (RDA) or Part Design Approvals (PDA), are instructions that need to be evaluated.
HBC's model communiqués and safety communiqués are publications issued by the type certificate holder; therefore, these documents must be evaluated pursuant to the air operator's operational requirements.
At EVAS, these documents were received through the company's maintenance department. The decision as to whether they would be forwarded on to the flight operations department was typically left up to the individual responsible for the initial review. Unless the contents of the documents were specifically operational in nature, the company's practice was to not forward it on.
1.18.7 Daily inspections
HBC does not require a maintenance DI to be performed.
EVAS developed a DI checklist for the B1900D that included a check of the flight controls for movement and feel. Maintenance personnel were required to complete the DI before the first flight of the day. EVAS did not require maintenance personnel to use the DI checklist, nor did it require a record of the specific checks being carried out or a logbook entry showing that the DI had been completed. The DI was normally conducted from memory, and on occasion, some of the checklist tasks were inadvertently skipped or not completed. If an aircraft was away from base overnight and no maintenance personnel were available, then no DI would be carried out.
Although not required, other operatorsFootnote 36 employ some form of DI. The items included in the DI and the procedures adopted for its completion vary between operators.
1.18.8 Pre-flight inspection
The AFM requires a pre-flight inspection to be carried out before the first flight of the day.Footnote 37 The pre-flight inspection is a check of the exterior and interior of the aircraft, as well as the cockpit. It includes items such as checking the engine oil quantity, checking for brake wear, and draining the fuel sumps. There is no requirement in the AFM pre-flight inspection to carry out a check of the flight control systems.Footnote 38
EVAS's SOP required external checks, cockpit and cabin preliminary checks, and cockpit preparation to be conducted as per the AFM Normal Procedures. A full pre-flight inspection was to be carried out whenever there was a crew change or aircraft change. EVAS did not require the flight crew to record that a pre-flight inspection had been carried out.
Although EVAS's B1900D pilots receive initial and annual recurrent training on aircraft servicing and ground handling, it was not the company's practice to have the crews check the engine oil quantity, open access panels to examine specific areas, or drain the fuel sumps. In general, the crews considered the pre-flight inspection to be a visual check of the aircraft.
The practice of considering the pre-flight inspection as a visual check of the aircraft is generally consistent with the other Canadian operators.
1.18.9 Sterile cockpit
The concept of a sterile cockpit has been in practice for a number of years. The purpose of such a procedure is to avoid non-operational conversations to minimize the risk of distraction to the crew's operational attentiveness.Footnote 39 Although the CARs do not require the implementation of a sterile cockpit, various air operators have included this concept in their daily operations, SOP or COM.
The United States FAA has implemented a Federal Aviation Regulation (FAR 135.100) stating, in part, that:
- No flight crew member may engage in, nor may any pilot in command permit, any activity during a critical phase of flight which could distract any flight crew member from the performance of his or her duties or which could interfere in any way with the proper conduct of those duties. Activities such as eating meals, engaging in non-essential conversations within the cockpit and non-essential communications between the cabin and cockpit crews, and reading publications not related to the proper conduct of the flight are not required for the safe operation of the aircraft.
- For the purposes of this section, critical phase of flight involves all ground operations involving taxi, takeoff and landing, and all other flight operations conducted below 10,000 feet, except cruise flight.
Note: Taxi is defined as “movement of an airplane under its own power on the surface of an airport.”
EVAS required a sterile cockpit for all flight operations below 5000 feet.Footnote 40 During this time, the flight crew was to limit communications and cockpit activities to only what was required to operate the aircraft. There was to be no paperwork completed, idle chat and distracting actions not directly related to the operation of required cockpit duties.
During the occurrence flight, from engine start until the start of the take-off run, about 40% of the crew's conversation was not essential to the operation of the aircraft.
1.18.10 Crew checklists
The National Aeronautics and Space Agency (NASA) report The Human Factors of Flight-Deck Checklists: The Normal Checklist discusses checklist use concepts, stating:
The various ways of conducting a checklist are not only limited to the device in use, but they also pertain to the concept of using a checklist—sometimes referred to as the “checklist philosophy of use.” This philosophy varies between airframe manufacturers, officials of regulatory agencies, and airlines.
[…] In most cases, the checklist philosophy-of-use is the outgrowth of the company's corporate “culture.” This term includes many factors that contribute to the overall operational concept of the organization, including management style, supervision concepts, delegation of responsibilities in the chain of command, punitive actions, etc. The airline's culture is an important factor because it is mirrored in the manner in which flight management and training departments establish, direct, and oversee flight operations and related procedures.Footnote 41
EVAS' SOP requires the aircraft checklist to be executed using a challenge-and-response (C&R) or read-and-do (R&D) method, using normal reading speed, and carried out as read.Footnote 42 Confirmation of the checklist items is mandatory. The PNF is to read the checklist items (challenge), and as each item is read, the PF is to respond (response) with the action to complete (or that has been completed).
The EVAS Normal Procedures Checklist identifies the flight control check in the After-Start Checks section.
FDR data from previous flights indicated that it typically took about 5 seconds to perform a flight control check. During the occurrence flight, the response for the flight control check was about 1 second after the challenge was made, and there was no recorded movement on the FDR. Other checklist items were conducted in a similarly rapid manner. Some challenges were not read in their entirety, and at times, subsequent challenges were read before the previous response was completed.
FDR data for the last 14 flights, including the occurrence flight, showed that no elevator control movement corresponding to a flight control check took place on the occurrence flight or on 11 of the 13 previous flights. These 13 previous flights were conducted by several different flight crew pairings.
1.18.11 Organizational safety culture
Safety culture can be described as “the way we do things around here,”Footnote 43 or “what people at all levels in an organisation do and say when their commitment to safety is not being scrutinized.”Footnote 44 Organizational safety culture sets the boundaries for accepted operational performance in the workplace by establishing the norms and limits, and provides a cornerstone for managerial and employee decision-making. Culture is deeply ingrained, and its impact on safety may not be readily apparent to those working within those cultures.
One of the largest influences on safety culture is management commitment and style. The International Civil Aviation Organization (ICAO) has described the role of management in creating a “good” organizational safety culture as follows:Footnote 45
Those in the best position to effect accident prevention by eliminating unacceptable risks are those who can introduce changes in the organization, its structure, corporate culture, policies and procedures, etc. No one is in a better position to produce these changes than management.
Organizations must strike a balance between safety and production by managing risks present in their operation. The challenge for an organization is to operate efficiently while minimizing safety risks. The reality within many organizations is that production and operational concerns may at times seem more pressing, since they are more measurable and provide immediate feedback in terms of results. Therefore, operational concerns may be more salient in the minds of decision-makers than concerns dealing with safety. In this context, organizations may unwittingly introduce risk into their operations.
Organizations differ considerably in the level of risk they tolerate within their operations. Those organizations which take proactive steps to identify and mitigate risks are considered to have good safety cultures, while other organizations with poor safety cultures knowingly or unknowingly operate with higher levels of risk. An organization that operates with significant risk faces a greater potential for an accident.
The traditional approach to safety management is based on compliance with regulations and a reactive response to incidents and accidents. Follow-up action may generate safety recommendations aimed at the specific, immediate safety concern identified as causing the occurrence. Little emphasis is placed on other hazardous conditions that, although present, are not causal in the occurrence, even though they hold damaging potential for aviation operations under different circumstances.Footnote 46 While this perspective is quite effective in identifying what happened, it is considerably less effective in disclosing why it happened, which is essential to correcting the underlying safety deficiency. Although compliance with safety regulations is fundamental to the development of sound safety practices, organizations that simply comply with the standards set by the regulations are not well situated to identify emerging safety problems.Footnote 47
As global aviation activity and complexity continue to grow, traditional methods for addressing safety risks to an acceptable level become less effective and inefficient. Improved methods for understanding and managing safety risks are necessary.Footnote 48 Modern safety management principles promote a proactive search for hazards, identification of risks, and the best defences to reduce risk to an acceptable level. These principles must be embedded within an organization's management system, so that safety policies, planning, procedures, and performance measurement are integrated into day-to-day operations.Footnote 49 This necessity led to the development of the requirement for formal safety management systems.
1.18.12 Safety management systems
In 2001, TC published Introduction to Safety Management Systems (TP 13739). TP 13739 describes SMS as:
A safety management system is a businesslike approach to safety. It is a systematic, explicit and comprehensive process for managing safety risks. As with all management systems, a safety management system provides for goal setting, planning, and measuring performance. A safety management system is woven into the fabric of an organization. It becomes part of the culture, the way people do their jobs.
Since 2005, Canada's large commercial carriers have been required to have a SMS, but for 702, 703, and 704 operators such as EVAS, implementation has been delayed to provide additional time to refine procedures, guidance material, and training.
Air Canada encourages its Tier III carriers to develop and implement some form of SMS, and provides advice on how to do so when requested. However, Air Canada is of the view that it cannot insist that its Tier III carriers have a SMS in the absence of a regulatory requirement. Air Canada audits all of its Tier III operators using the IATAFootnote 50 Operational Safety Audit (IOSA) and IOSA standards and recommended practices (ISARPs).Footnote 51 Air Canada typically conducts these audits every 2 years; EVAS's IOSA was conducted in June 2010.
The IOSA Standards Manual provides the following information concerning SMS:
The Operator should have a safety management system (SMS) that is implemented and integrated throughout the organization to address the safety of aircraft operations.
Specific SMS requirements for an operator will always be mandated by the State in accordance with its individual State Safety Plan (SSP).
…most SMS provisions are initially presented in the ISARPs as recommended practices (i.e. “should”).
The IOSA audit includes about 30 SMS-related practices. Air Canada reviews these practices when carrying out an audit; however, it does not not require its Tier III carriers to comply with them, as there is no regulatory requirement for CARs 704 operators to have a SMS.
The TSB Watchlist (14 June 2012) identifies the following:
Until SMS are more broadly implemented within the aviation industry, the TSB remains concerned regarding the risks to Canadians, and will continue to monitor progress in this area.
Preservation of aircraft recorded data
On 01 January 2010, TC issued Advisory Circular (AC) 700-013Footnote 52 to provide air operators, flight crew members, and ground personnel with information regarding the training required to disable appropriate circuit breakers for the preservation of recorded data on CVRs and FDRs following an accident or an incident.
Paragraph 724.121(i) of the Commercial Air Service Standard (CASS) requires the inclusion of FDR and CVR procedures in the COM. It is expected that the appropriate steps for disabling of a FDR and/or CVR following an accident or incident will be included in these procedures.
In addition, CARs 704.115(2)(a)(v)(C) requires that an air operator's training program include initial and annual training on emergency procedures. This training should include procedures for disabling the FDR/CVR following an accident or incident, and must be provided to flight crew members and ground personnel.
Current requirements as set out in section GEN 3.4.3 of the Aeronautical Information Manual (AIM) state the following, in part:
Where a reportable incident occurs, the pilot-in-command, operator, owner and any crew member of the aircraft involved shall, as far as possible, preserve and protect the flight data recorders and the information recorded thereon.
The EVAS COM did not include procedures for preserving the FDR/CVR following an accident or incident.
1.19 Useful or effective investigation techniques
N/A
2.0 Analysis
2.1 General
The aircraft had no known deficiencies before the occurrence flight; therefore, this analysis will discuss the conditions that contributed to the occurrence aircraft's elevator control movement becoming restricted, previous occurrences of elevator restriction on B1900 aircraft, the aircraft manufacturer's procedures and publications, and the operator's review of those communications. The analysis will also discuss company procedures and practices that contributed to the restriction not being detected before the take-off attempt.
2.2 Stuck elevator control
The occurrence aircraft had been parked outside, with its tail pointed into gusty winds; Exploits Valley Air Services (EVAS) personnel did not always install the control locks. The Airplane Flight Manual (AFM) indicates that gust locks should be installed after flight and removed before flight. Installing the control locks protects the flight controls from abnormal forces such as gusty winds. Without the control lock installed, gusty winds can cause the elevators to move up and down rapidly. This movement would cause the control column to slam back and forth. The rapid downward movement, in combination with the downspring and bob-weight force, would result in the control-column vertical portion flexing under the strain of the combined forces. In this occurrence, the damage noted on the bob-weight was more severe than what was observed when the elevators were allowed to free-fall or from pushing the control column forward. Therefore, the damage to the occurrence aircraft's bob-weight resulted from the elevators being repeatedly slammed down when the aircraft was parked outside, without the control locks installed, in the gusty wind conditions.
When EVAS examined the aircraft after the occurrence, they had to push the stop bolt to the left to align the damage on the bob-weight with the stop bolt. Once the stop bolt was released, it would have exerted a sideways force on the bob-weight. This force would tend to hold the bob-weight in position. With the bob-weight held beyond its normal range of travel, the vertical portion of the T-shaped column would have been flexed forward. The design of the elevator position sensor system is such that it will read, and the flight data recorder (FDR) will record, movement beyond the normal range of travel. At the start of the occurrence flight, the elevator position indication was 1.1° beyond normal. This position is indicative of the control column travelling beyond its normal range of travel. The control column was stuck forward because the bob-weight became jammed on the stop bolt.
No elevator control check was carried out during the daily maintenance inspection (DI) or the after-start checks, which resulted in the stuck control condition going undetected. The flight crew's first indication of the elevator controls being stuck was at about rotation speed.
2.3 Bob-weight stop-bolt bracket
The design of the stop-bolt bracket is such that the stop bolt is oriented to the left side of the bob-weight. In the occurrence aircraft, as well as the 2 aircraft identified in Model Communiqué #91 and the majority of the aircraft reviewed by the Transportation Safety Board (TSB), the stop bolt was making contact on the left side of the bob-weight. Both Pacific Coastal Airlines (Pacific Coastal) and EVAS had advised Hawker Beechcraft Corporation (HBC) that if the stop bolt had been oriented such that contact was made in the centre of the bob-weight, then it would have prevented this type of occurrence.
In addition to the 3 HBC reported cases, the TSB identified 6 Pacific Coastal aircraft in which the bob-weight went beyond the stop bolt. When the stop bolt is aligned to contact the bob-weight on its left edge, there is a greater risk that, when the elevator control system is acted on by an abnormal force such as wind gusts, the bob-weight will travel beyond its normal range.
2.4 Reporting to the Transportation Safety Board
EVAS was not aware that the incident must be reported to the TSB when difficulties in controlling the aircraft due to any aircraft system malfunction are encountered. EVAS did not notify the TSB of the reportable occurrence, and had already undertaken repairs before the TSB was apprised of the occurrence. Therefore, it was not possible for TSB investigators to examine the occurrence aircraft's elevator control system in situ. When operators are not aware of the TSB's reporting requirements and therefore do not advise the TSB of a reportable accident or incident, potentially valuable information may be lost.
2.5 Flight data recorder parameters
Even though the FDR-recorded parameters met the requirements of the Canadian Aviation Regulations (CARs), only the elevator control position was recorded. Had the FDR recorded the aileron and rudder positions, the investigation team would have had a clearer understanding of what the flight crews were doing during the flight control checks. If the FDR had also recorded the elevator control forces, the investigation team would have had a clearer understanding of the force needed to overcome the bob-weight system's over-centre protection. When an FDR captures only the minimum required parameters as defined by the CARs, potentially valuable information will not be recorded.
2.6 Sterile cockpit
From engine start until the start of the take-off run, 40% of the crew's conversation involved non-essential communication. During this phase of flight, the company standard operating procedures (SOP) require the crew to maintain a sterile cockpit. When crews engage in non-essential communication while a sterile cockpit environment is required, there is an increased risk of distraction that may cause them to make unintentional errors.
2.7 Pre-flight inspection
HBC and EVAS both require a complete pre-flight inspection to be carried out before the first flight of the day. EVAS's SOP requires its flight crews to conduct this inspection in accordance with the HBC AFM. However, EVAS considers the pre-flight inspection to be a visual examination of the aircraft, and therefore, the flight crews do not perform tasks such as checking the engine oil levels and opening access panels. EVAS uses a maintenance DI that includes the pre-flight inspection tasks that the flight crews do not perform. The combination of the DI tasks being carried out by maintenance personnel and the visual examination of the aircraft being carried out by the flight crew typically addresses all of the items identified in the HBC pre-flight inspection. However, at EVAS, both the maintenance DI and the flight crew's pre-flight inspection are done from memory, and on occasion, some tasks are not carried out. When operators do not carry out a complete pre-flight inspection in accordance with the manufacturer's instructions, there is a risk that a critical item may be missed, which could jeopardize the safety of the flight.
2.8 Identifying the underlying unsafe condition
HBC had identified the safety issue as the link assembly over-centre condition. HBC's Continued Operational Safety (COS) program includes identifying the root cause(s) of a specific safety issue. In this occurrence, HBC's follow-up actions, including Safety Communiqué #321, have been focused on how the link assembly went over centre. HBC considered its mitigation strategies to have been effective in assisting operators to maintain and ensure the airworthiness condition of their aircraft. HBC considered that, since there had not been any further reports of the unsafe condition since the release of Safety Communiqué No. 321, its mitigating strategies were appropriate and effective in preventing a recurrence of the events reported by Pacific Coastal and EVAS.
In Model Communiqué #91, HBC recognized the safety issue as the bob-weight going beyond the stop bolt and becoming stuck. In the 3 service difficulty reports (SDRs), all of the operators identified the bob-weight going beyond the stop bolt as a safety issue. This same safety issue was identified as the unsafe condition in Emergency Airworthiness Directive (AD) 2011-27-51. In the Pacific Coastal and EVAS occurrences, the link assemblies had gone over centre as a result of the flight crew's actions to overcome the stuck elevator control.
Even though HBC was aware of the orientation of the stop bolt to the bob-weight, it did not identify this orientation as a root cause or an underlying unsafe condition. The Federal Aviation Administration (FAA) requested that HBC propose a design change to address this underlying unsafe condition. When organizations do not accurately identify underlying unsafe conditions, then it is likely that the resulting mitigation may not be effective in preventing a recurrence of the event.
2.9 Advisory information in the airplane flight manual
In Model Communiqué #91, issued about 2 years before the occurrence flight, the operator concluded that the bob-weight became stuck on the stop bolt because the elevators were allowed to free-fall from the full up position. The primary focus of the communiqué was to remind operators to follow the published maintenance practices. Even though the Airliner Maintenance Manual (AMM) provided cautions related to carefully lowering the elevators to prevent damage to the elevator system, the requirement to not allow the elevators to free-fall is not unique to a maintenance activity. It is possible that the same action can be carried out by flight crews. However, the AFM does not include any cautions similar to what is published in the AMM. When a manufacturer's maintenance documents include cautions/warnings pertaining to actions that may cause damage to aircraft systems and these cautions/warnings are not included in the AFM, there is a risk that flight crews will be unaware of the concerns and inadvertently cause damage to the aircraft system.
2.10 Evaluating type certificate holder's communications
Safety Communiqué #321 was issued as a result of the EVAS and Pacific Coastal incidents. Even though this communiqué was addressed to chief pilots and directors of operations, the majority of the text was related to maintenance practices, implying that the problem may be the result of inadequate maintenance (incorrect rigging or worn component). If manufacturers' communications contain concerns related to both flight operations and maintenance, and the communications' emphasis is maintenance-related, then it is possible that operators will not recognize the need to distribute the communication to their flight operations department for consideration of the operational implications, possibly jeopardizing safety of flight.
2.11 Effectiveness of Hawker Beechcraft Corporation's communications
Model Communiqué #91 indicates that the bob-weight can travel beyond its normal range and become stuck on the stop bolt if maintenance practices are not followed. Safety Communiqué #321 states that the link assembly can go over centre if maintenance practices are not followed. However, there is no mention that, before the link assembly can go over centre, the bob-weight must travel beyond its normal range and become stuck on the stop bolt. Both communiqués include information on the use of control locks when the aircraft is parked outside. HBC has indicated that, by installation of the control locks, the flight control system will be protected from abnormal forces such as gusty winds. However, this information is intertwined with other details, including some implications that the “problem” was a result of incorrect maintenance procedures. Neither of these safety communications clearly conveys the safety-critical information (the bob-weight may travel beyond its normal range and become stuck on the stop bolt) or the consequences (stuck elevator control) if the problem goes undetected. Nor do they clearly state the underlying reason as to why the bob-weight can impact the stop bolt, or what can be done to mitigate the issue (install control locks). When manufacturers do not provide clear and concise information in their communications, operators may not fully understand and appreciate the safety issue and what can be done to mitigate the risk.
2.12 Safety management systems
Organizations respond to operational pressures because these priorities are clearly measurable and provide immediate feedback. Under these pressures, safety concerns may become less prominent, and organizations may unwittingly introduce risk into their operations.
The flight safety program manager (FSPM) had a multitude of other duties, and the safety committee meetings focused on operational concerns. Neither the FSPM nor any of the safety committee members called for a special meeting to review the circumstances surrounding this occurrence, nor was it tabled during the safety meeting in 2012. There was no proactive identification of potential hazards, including the possible impact of an increasing fleet size and the addition of new employees. Although EVAS had a safety program in place, safety management was conducted using a traditional reactive approach.
The traditional approach to safety management has been shown to be ineffective in identifying potential hazards and associated risks. Organizations that comply with the minimum standards and manage safety using the traditional approach are not well situated to identify emerging safety problems. In today's aviation environment, modern safety management practices must be embedded within an organization's management system, so that the management of safety is integrated into day-to-day operations. Even though there are no regulatory requirements for 702, 703, and 704 operators to have a safety management system (SMS), nothing prevents these operators from implementing one. Although Air Canada supports SMS and agrees that SMS would benefit its Tier III operators, it is of the view that it cannot require SMS for its Tier III operators in the absence of a regulatory requirement. When organizations do not use modern safety management practices, there is an increased risk that hazards will not be identified and mitigated.
3.0 Findings
3.1 Findings as to causes and contributing factors
- The aircraft was parked outside, without the control locks installed, in gusty wind conditions, causing damage to the bob-weight from the elevators being repeatedly slammed down.
- The design of the stop-bolt bracket allowed the bob-weight to travel beyond its normal operating range, resulting in the control column being stuck forward because the bob-weight became jammed on the stop bolt.
- No elevator control check was carried out during the daily maintenance inspection, nor as required by the after-start checks, which resulted in the stuck elevator control condition going undetected.
3.2 Findings as to risk
- When manufacturers do not provide clear and concise information in their communications, operators may not fully understand and appreciate the safety issue and what can be done to mitigate the risk.
- When crews engage in non-essential communication while a sterile cockpit environment is required, there is an increased risk of distraction that may cause them to make unintentional errors.
- When operators do not carry out a complete pre-flight inspection in accordance with the manufacturer's instructions, there is a risk that a critical item will get missed, which could jeopardize the safety of flight.
- When organizations don't identify the underlying unsafe condition, then it is likely that the resulting mitigation may not be effective in preventing a recurrence of the event.
- When a manufacturer's maintenance documents include cautions/warnings pertaining to actions that may cause damage to aircraft systems and the cautions/warnings are not included in the Airplane Flight Manual, there is a risk that flight crews will be unaware of these concerns and inadvertently cause damage to the aircraft system.
- When manufacturers' communications contain concerns related to both flight operations and maintenance, and the communications' emphasis is maintenance-related, then it is possible that operators will not recognize the need to distribute the communication to their flight operations department for consideration of the operational implications, possibly jeopardizing safety of flight.
- When organizations do not use modern safety management practices, there is an increased risk that hazards will not be identified and mitigated.
- When operators are not aware of the Transportation Safety Board's reporting requirements and therefore do not advise the Transportation Safety Board of a reportable accident or incident, there is a risk that potentially valuable information will be lost.
- When flight crews do not take precautions to preserve cockpit voice recorder data and flight data recorder data following a reportable occurrence, there is a risk that potentially valuable information may be lost.
3.3 Other findings
- When flight data recorders capture only the minimum required parameters as defined by the Canadian Aviation Regulations, potentially valuable information will not be recorded.
- The bob-weight from aircraft UE-345 did not meet the manufacturer's specified values for antimony content or hardness.
- The Exploits Valley Air Services Company Operations Manual did not include procedures for preserving the flight data recorder / cockpit voice recorder following an accident or incident.
- At Exploits Valley Air Services, Safety Communiqué #321 was not forwarded to flight operations or the chief pilot, although it was addressed to both.
4.0 Safety action
4.1 Safety action taken
4.1.1 Exploits Valley Air Services Limited
Immediately following the occurrence, the company released an instruction to all staff requiring the use of flight control locks at any time when there is not a crew member at the controls of the aircraft. This instruction was also included as an amendment to the company standard operating procedures.
Exploits Valley Air Services flight crew training now incorporates the control lock issue and loss of flight control as a simulated occurrence during all flight crew training.
After receipt of SB 27-4119, Exploits Valley Air Services ordered the associated elevator bob-weight stop kits for its aircraft.
4.1.2 Federal Aviation Administration
On 23 December 2011, the Federal Aviation Administration issued Emergency Airworthiness Directive 2011-27-51, effective immediately upon receipt.
4.1.3 Hawker Beechcraft Corporation
In May 2012, Hawker Beechcraft Corporation issued Model Communiqué #104 to announce newly developed Airliner Maintenance Manual inspection procedures intended to identify and correct noted damage to the stop bolt, the stop-bolt bracket, the bob-weight, and other supporting structures. These procedures require an alignment check of the bob-weight with the stop bolt to ensure that no part of the stop bolt protruded beyond the face of the bob-weight, and a visual examination of the weight for evidence of scraping along the side and for evidence of damage to the stop bolt and stop-bolt bracket.
Subsequently, the third 200-hour and the 5000-hour inspections were revised and became mandatory.
In June 2013, Hawker Beechcraft Corporation issued Mandatory Service Bulletin SB 27-4119. This Service Bulletin introduces Kit 114-5060 (KIT − BOB WEIGHT STOP, ELEVATOR SYSTEM) for Model 1900-series airplanes, and provides parts and instructions to install a second elevator bob-weight stop bolt.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on . It was officially released on .
Appendices
Appendix A – Transportation Safety Board laboratory reports
The following Transportation Safety Board (TSB) Laboratory reports were completed:
- LP 179/2011 – FDR/CVR Analysis
- LP 012/2012 – Examination of Elevator Control Bob-weights
These reports are available from the Transportation Safety Board of Canada upon request.
Appendix B – Hawker Beechcraft Corporation Model Communiqué #91
Appendix C – Hawker Beechcraft Corporation Safety Communiqué #321