Loss of control – In-flight breakup
Black Sheep Aviation & Cattle Co. Ltd.
de Havilland DHC-3 Otter C-GMCW
Mayo, Yukon, 38 nm NE
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The Black Sheep Aviation and Cattle Co. Ltd. turbine powered de Havilland DHC-3 Otter (registration C-GMCW, serial number 108) departed Mayo on a 94 statute mile day visual flight rules flight to the Rackla Airstrip, Yukon. At 1507 Pacific Daylight Time, approximately 19 minutes after the aircraft had left Mayo, a 406 MHz emergency locator transmitter alert was received by the Canadian Mission Control Centre. The Joint Rescue Co-ordination Centre Victoria was notified and a commercial helicopter was dispatched from Ross River, Yukon. Aircraft wreckage was located on a hillside 38 nautical miles northeast of Mayo at 1833 Pacific Daylight Time. The wheel-ski equipped aircraft had experienced a catastrophic in-flight breakup and the pilot, who was the sole occupant, had sustained fatal injuries. There was no post-impact fire.
1.0 Factual information
1.1 History of the flight
The aircraft was being utilized in support of mineral exploration activities, to transport building materials, fuel, and winter camp supplies from Mayo, Yukon, to winter airstrips located at Withers Lake and Rackla River, Yukon. Withers Lake is located 113 statute miles (sm) east of Mayo, and Rackla Airstrip is located 94 sm northeast of Mayo (Appendix B). On the accident flight, the aircraft was transporting a load of twelve 6-inch by 6-inch wood timbers, each 16 feet long, and 2 barrels of jet fuel.
The pilot had arrived at the Mayo Airport at about 0630 Footnote 1 on the morning of the accident. The pilot's first trip of the day was to Withers Lake, departing Mayo at 0834. The pilot completed 2 trips to Withers Lake and 1 trip to Rackla prior to the accident flight. The accident flight departed Mayo at 1448 under visual flight rules (VFR) on a company itinerary. At 1507 the Canadian Mission Control Centre (CMCC) received a 406-MHz emergency locater transmitter (ELT) alert. Joint Rescue Co-ordination Centre Victoria (JRCC Victoria) was notified at 1522. Aircraft operating in the area were alerted, and a commercial helicopter was dispatched from Ross River, Yukon, approximately 1 hour later to search for the aircraft. The helicopter crew located the aircraft wreckage at 1833 at about 4300 feet above sea level (asl), on a remote, snow-covered hillside 38 nautical miles (nm) northeast of Mayo.
1.2 Injuries to persons
The pilot was the sole occupant and was fatally injured; no persons on the ground sustained injuries.
1.3 Damage to aircraft
The aircraft was substantially damaged due to the in-flight breakup and ground impact. The empennage, all flight controls, and both wings had separated during flight.
1.4 Other damage
The aircraft fuel tanks and 2 barrels containing Jet A fuel ruptured at impact, releasing approximately 770 litres of jet fuel into the environment. Environmental damage was confined to the main impact site. There was no other property damage.
1.5 Personnel information
1.5.1 Pilot-in-command
The pilot was certified and qualified for flight in accordance with existing regulations. The pilot held a medically valid commercial pilot licence endorsed for single- and multi-engine land and seaplanes. The pilot had previously held a class 4 instructor rating, valid to 01 September 2003, and a group 1 instrument rating, valid to 01 April 2004. The pilot's personal log books were not found during the investigation; however, information from other sources indicated the pilot had accumulated approximately 5000 hours of flying experience, mostly as pilot-in-command, with an estimated 3000 hours on turbine-powered DHC-3 Otters. The pilot also held an E‑category aircraft maintenance engineer (AME) licence.
The pilot had flown Pratt and Whitney PT 6–powered DHC-3 Otters on the West Coast of British Columbia for 3 years before being hired by Black Sheep Aviation. The pilot had flown for Black Sheep Aviation for all of the 2010 float season, and had flown winter operations for the company from 10 January to 03 February 2011. The pilot had returned to Mayo to participate in a second winter flying campaign that was to last several weeks, beginning 21 March 2011.
The pilot was paid solely on a per-mile-flown basis. An examination of the flight records from 21 March to 31 March identified that the pilot was regularly flying 6 to 7 trips (12 to 14 flights) and 1200 to 1400 miles per day. It is an industry standard to pay small aircraft charter pilots partially or fully on a per-mile-flown basis.
Transport Canada published the Safety of Air Taxi Operations (SATOPS) report in 1998. The report contained 71 recommendations to improve safety in air taxi operations. According to the report, paying a pilot by the mile or hours flown, or paying a pilot only for completed flights, may have a direct and negative effect on the pilot's decision-making, especially in seasonal operations where there are only a few weeks or months to work. The report made 2 recommendations to address this concern:
- SATOPS Recommendation (SR) 37 recommended that Transport Canada investigate a means of requiring air operators to remunerate pilots in a way that eliminates the operating pressures associated with the method of payment.
- SATOPS Industry Action (IA) 37 recommended that air operators and pilots acknowledge the negative effect that the “pay-by-the-mile” method of payment can have on safe operational decision making. It recommended that air operators and pilots make decisions based on safety, not remuneration, and that air operators consider other methods of remunerating pilots.
There is no known follow-up action on SR 37 or IA 37.
The pilot was characterized as an extremely hard worker who was willing to put in long days and fly at every opportunity when trips were offered. The pilot was physically strong and had a reputation for loading and unloading the aircraft rapidly during turnarounds. On trips from Mayo to Rackla and Withers Lake, Black Sheep Aviation's turbine-powered DHC-3 Otters typically transported 2400 pounds of mixed cargo, including lumber, barrels of fuel, and camp supplies. In addition to flying, company pilots worked with ground personnel to load aircraft, secure loads, and unload aircraft for each flight. After the last flight of each day, the normal routine included helping to load and refuel the aircraft, install engine covers and heaters, and tow the aircraft to a safe parking area at the Mayo airport in order to prepare the aircraft for an early departure the next morning. These end-of-day duties were estimated to take 45 minutes. Company personnel were available to help pilots with end-of-day duties.
Mayo is a central Yukon village with a winter population of fewer than 500 people. The pilot's accommodation, which was provided by the company, was a kitchenette room in a small motel in the village. The motel room was being shared with another company employee; both employees were given the opportunity by the company to have separate rooms, but they chose not to. The quality of sleep that the pilot was experiencing each night could not be determined.
Restaurant facilities in Mayo were limited. The pilot normally ate a light breakfast in the motel room before leaving for the airport in the morning; the pilot's normal lunch and dinner routines were not determined.
1.5.2 Flight duty time and minimum rest period
Canadian Aviation Regulations (CARs) 101.01(1) defines the following terms:
“flight duty time” - means the period that starts when a flight crew member reports for a flight, or reports as a flight crew member on standby, and finishes at engines off or rotors stopped at the end of the final flight….
“minimum rest period” - means a period during which a flight crew member is free from all duties, is not interrupted by the air operator or private operator, and is provided with an opportunity to obtain not less than eight consecutive hours of sleep in suitable accommodation, time to travel to and from that accommodation and time for personal hygiene and meals.
CARs 700.16 (1) permits flight duty time of 14 consecutive hours in any 24 consecutive hours in normal circumstances.The Black Sheep Aviation & Cattle Co. Ltd. Air Operator Certificate authorized an increase in flight duty time under Operations Specification Number 93. The Operations Specification was valid as long as the operator complied with the requirements of section 720.16 of the Commercial Air Service Standards, which provides that where a flight is conducted under Subpart 3 of Part VII of the CARs, the maximum flight duty time may be extended to 15 consecutive hours if the minimum rest period is increased by 1 hour or the maximum flight time does not exceed 8 hours in any 24 consecutive hours.
The investigation determined that the pilot's actual flight times had exceeded 8 hours in any 24 consecutive hours for the 8 consecutive days before the accident (Appendix D). Compliance with Operations Specification Number 93 would have required that the minimum rest period be increased by 1 hour. On days when the flight duty time exceeded 14 hours and the flight time exceeded 8 hours, the minimum rest periods had not been extended as required by regulation.
CARs 700.14(1) requires every air operator to have a system that monitors the flight time, flight duty time, and rest periods of each of its flight crew members. While the operator and the pilot share the responsibilities of making sure they are operating within the flight time, flight duty time, and rest period regulations before a flight is dispatched, it is the responsibility of the operator to ensure the system that is in place to track these items is adequate to validate compliance with CARs at any time. Under CARs 723.07, the responsibilities of the operations manager include crew scheduling, ensuring that the air operator's operations are conducted in accordance with current regulations, and ensuring that crew scheduling complies with flight and duty time regulations.
Black Sheep Aviation flight time, flight duty time and rest period tracking records were based on transcriptions of the pilot's own journey log entries. The company operations manual (COM) required pilots to inform the operations manager of their daily flying times, asa well as the length of—and reasons for—duty-time extensions. The COM also required a flight duty–time form showing days off, rest periods, and a running total of flight times to be maintained in the company office by the operations manager. At the time of the accident pilots were noting their duty-day start and stop times in the “Remarks” column of the aircraft journey logs, and were forwarding duplicate sheets of the completed journey log pages to Whitehorse from Mayo by ground transportation on a weekly basis. The operator was reconciling pilot flight hours and flight duty times on the company Flight Time/Duty Time/Rest Period form on a monthly basis at the time of the accident.
Company records completed after the accident and recovered from the operator's flight duty tracking system indicated that the pilot had not exceeded a 14.0-hour duty day at any time from 21 March to 30 March inclusive. The records indicated the pilot had accrued a total flight duty time of 122.2 hours from 21 March to 30 March inclusive, and 92.6 hours for the 7-day period 24 March to 30 March inclusive. Examination of these records in concert with records from other sources identified that the pilot's actual flight duty time from 21 March to 30 March inclusive was 132.6 hours, and the pilot's actual flight duty time for the 7-day period 24 March to 30 March inclusive was 99.6 hours (Appendix D).
The pilot had finished the previous day's duty day at approximately 2100 and had arrived at the airport on the day of the accident at about 0630. That signified a 9.5 hour rest period in which the pilot would have travelled from the airport to the accommodation, eaten dinner, slept and taken care of personal hygiene, eaten breakfast, and travelled back to the airport. The drive time between the pilot's accommodation and the airport was approximately 5 minutes. The pilot had been awake for 9.1 hours and on duty for 8.6 hours at the time of the accident.
1.5.3 Air times and flight times
CARs 101.01 defines air time “as the time from the moment an aircraft leaves the surface until it comes into contact with the surface at the next point of landing.”
CARs 605.94 requires the air time of each flight or series of flights and the cumulative total air time to be entered in the aircraft journey log daily on completion of each flight or series of flights by the pilot-in-command of the aircraft or a person designated by an air operator. Section 7.3 (1) of the Aeronautics Act states, “no person shall make or cause to be made any false entry in a record required under this Part to be kept with intent to mislead or wilfully omit to make an entry in any such record.”
CARs 101.01(1) defines flight time as “the time from the moment an aircraft first moves under its own power for the purpose of taking off until the moment it comes to rest at the end of the flight.” Flight time includes taxi time. To account for this, it is usual to add 0.1 hours to air time to calculate flight time for journey log entries.
The accident aircraft was equipped with a panel-mounted Bendix-King KMD150 global positioning system (GPS) that had captured 7 data parameters, including date and time, once each 30 seconds for the last 25 flights the aircraft had made, including the accident flight (Appendix E). The GPS began recording data when the aircraft reached a GPS ground speed of approximately 23 mph, and it stopped recording data when the GPS ground speed dropped below approximately 3 mph. The investigation therefore considered the GPS data as a reasonably accurate source of air times.
The GPS data identified that, from 29 March to 31 March, the 94-sm flights from Mayo to Rackla and return had consistently taken from 0.6 hours to 0.7 hours air time, and the 113-sm flights from Mayo to Withers Lake and return had consistently taken from 0.7 hours to 0.8 hours air time. Based on the GPS times and actual distances, and without consideration for winds, the average ground speeds would have ranged from approximately 134 mph to 161 mph. These flights had all been recorded in the aircraft journey log as 0.5 hours air time. Based on the logged times, the average ground speeds would have ranged from approximately 188 mph to 226 mph.
The pilot had flown every day from 21 March to 31 March inclusive, and had conducted 121 flights, including the accident flight, during that period. With the exception of 4 flights on 21 March, all of the flights were from Mayo to Rackla and return, or Mayo to Withers Lake and return. The pilot had logged 112 of the flights in the appropriate aircraft journey log; all flights to or from Rackla or Withers Lake had been recorded as 0.5 hours air time and 0.6 hours flight time. Two flights, from Mayo to Withers Lake and return, on 30 March recorded in both the GPS data and on the Mayo Community Aerodrome Radio Station (CARS) records, as well as all the flights flown on 31 March, had not been logged in the aircraft journey log.
Another company pilot had been consistently logging flights from Mayo to Rackla return and to Withers Lake and return as 0.5 hours air time and 0.7 hours flight time in the journey log for the second company turbine-powered DHC-3 Otter.
Journey-log records and company flight-duty records indicated the pilot had accrued 69.4 hours of flight time from 21 March to 30 March inclusive, and 53.4 hours flight time for the 7-day period from 24 March to 30 March inclusive. By adjusting the journey-log flight times conservatively upward by 0.1 hours for each flight between Mayo and Rackla and return and by 0.2 hours for each flight between Mayo and Withers Lake and return to represent more accurately actual flight times as indicated by the GPS date and time data, it was determined that the pilot had actually accrued 88.6 hours flight time from 21 March to 30 March inclusive and 68.2 hours flight time for the 7-day period from 24 March to 30 March inclusive (Appendix D). The cumulative increase in the total air and flight times was significant due to the number of flights involved. Black Sheep Aviation had not reconciled the pilot's recent flight times, and was therefore unaware of the underreporting of air and flight times. The pilot's flight time for the day of the accident was estimated to have been 4.9 hours.
The Black Sheep Aviation & Cattle Co. Ltd. Air Operator Certificate authorized an increase in flight time under Operations Specification Number 92. The Operations Specification was valid if the air operator complied with the requirements of section 720.15 of the Commercial Air Service Standards. Section 720.15 provides that where a flight is conducted under Subpart 3 of Part VII of the CARs, the maximum flight time in any aircraft shall not exceed 60 hours in any 7 consecutive days.
| Reported and/or logged | Actual | |
|---|---|---|
| Flight time | 53.4 hours (reported and from journey log) | 68.2 hours |
| Air time | 43.0 hours (from journey log) | 59.4 hours |
| Number of flights | 86 (logged) | 88 |
| Flight duty time | 92.6 hours (reported) | 99.6 hours |
Note: Actual air and flight times include a conservative 0.1-hour increase over journey log times for Rackla flights and a 0.2-hour increase over journey log times for Withers Lake flights.
1.6 Aircraft information
1.6.1 General
The de Havilland DHC-3 Otter had been approved under Type Certificate No. A-27, which was originally held by de Havilland Canada, on 07 November 1952. At the time of the accident, the type certificate holder was Viking Air Limited of Sydney, British Columbia. The current type certificate data sheet identifies the maximum weight as 8000 pounds and the maximum number of occupants, including the pilot, as 16.
A total of 466 DHC-3 Otters were manufactured by de Havilland Canada (the accident aircraft was manufactured in 1956). At the time of manufacture all were fitted with a Pratt & Whitney R-1340 geared radial piston engine, rated at 600 horsepower for take-off and 550 horsepower maximum continuous.
The accident aircraft was fitted with a Honeywell (Garrett) TPE331-10-511C turboprop engine, flat-rated at 900 shaft horsepower, and a 4-blade Hartzell propeller in accordance with Transport Canada Supplemental Type Certificate (STC) SA02-15. The STC holder was Texas Turbine Conversions, Inc., and the conversion was known as the Texas Turbine Conversions Super Otter. The turboprop conversion significantly increased the climb and cruise performance of the aircraft compared with that of the Pratt & Whitney R 1340–engined DHC-3 Otter, as shown in the following comparison of performance specifications:Footnote 2
| Specification | Standard DHC-3 Otter | Texas Turbine Conversions Super Otter |
|---|---|---|
| Engine | Pratt & Whitney R1340 | Honeywell (Garrett) TPE331-10/-12JR |
| Horsepower | 600 horsepower | 900 horsepower flat-rated |
| Climb (ISA-g.w. wheels) | 850 feet/minute | 1700 feet/minute |
| Climb (ISA-g.w. floats) | 450 feet/minute | 1600 feet/minute |
| Cruise (10 000 feet, wheels) | 105 knots | 155 knots (airframe limited) Footnote 3 |
| Cruise (10 000 feet, floats) | 100 knots | 145 knots (airframe limited) |
The Texas Turbine Conversions Airplane Flight Manual Supplement (TTC-FMS-1) states, “The information contained in the document supplements or supersedes the Airplane Flight Manual only in those areas listed herein. For limitations, procedures, and performance not contained in this supplement, consult the Airplane Flight Manual.” Because the limitations section of TTC-FMS-1 does not address airspeed limits, the airspeed limits in the DHC-3 Otter Flight Manual(DHC-3 AFM) apply. Paragraph 4.5.2 of Chapter IV, Operating Limits, of the DHC-3 AFM states that the normal operating limit speed for the landplane and skiplane is 144 mph indicated airspeed (IAS). The normal operating limit speed for the DHC-3 seaplane is 134 mph IAS.
Records indicated the aircraft was certified, equipped, and maintained in accordance with existing regulations and approved procedures. The aircraft was being maintained in accordance with the periodic inspection schedules published in the Allied Signal Garrett TPE331-10 maintenance manual, the Garrett Otter maintenance manual supplement, and Appendix IV of the DHC-3 Otter maintenance manual. The inspection cycle required the airframe and engine to be inspected to varying degrees each 100 flying hours.
A 700-hour inspection had been completed on the aircraft on 22 March, at 16 369 airframe hours, and the airframe would have been due for an 800-hour inspection at 16 469 hours. Based on journey log entries, the airframe time would have been approximately 16 415 hours at the time of the accident. Based on actual air times since the last inspection, however, the airframe time would have been about 16 431.5 hours at the time of the accident, a difference of 16.5 hours near the midpoint of the inspection cycle.
Aircraft maintenance programs—including inspection schedules, engine, propeller, and other component overhaul times—and service bulletin (SB) and airworthiness directive (AD) compliance times are normally based on aircraft air time hours as recorded in aircraft journey logs or calendar times, whichever comes first.
Limit load factors are the maximum values to which the airframe may safely be subjected in flight. The DHC-3 AFM identifies the limit load factors as −1 g Footnote 4 and +3.5 g. Footnote 5 These limits did not change and were not required to change with the incorporation of STC SA02-15.
The aircraft was not equipped with an autopilot. The DHC-3 AFM states that the inherent stability of the aircraft is good about all axes and the aircraft is easy to fly and docile.
1.6.2 Aircraft weight and balance
All cargo loads were being assembled and weighed on pallets by expeditors in Mayo prior to being loaded on the aircraft. The aircraft had departed Mayo at or near the certified gross weight of 8000 pounds on the accident flight. The centre of gravity (c of g) was 145.8 inches aft of datum, within the allowable limits of 135.8 inches to 151.4 inches.
1.6.3 Texas Turbine Conversions Supplemental Type Certificate
The Honeywell (Garrett) TPE331-10-511C turboprop engine had been installed in the aircraft in 2002. Aircraft records indicated the engine had accumulated approximately 4600 hours since the date of the installation.
The Texas Turbine Conversions Honeywell (Garrett) STC had originally been certified by the Federal Aviation Administration (FAA) under STC number SA09866SC, in 2001. The United States was considered the Country of Design for the STC. The STC was familiarized Footnote 6 and approved by Transport Canada as STC SA02-15 on 25 January 2002.
The certification basis for the STC was Part 3 of the Civil Air Regulations, as amended to 1 November 1949, plus Federal Aviation Regulations (FAR) 23 requirements applicable to power plant installation. FAA Advisory Circular (AC) 23-14, issued 30 September 1993, provides guidance on the type certification basis for conversion from reciprocating engine to turbine-powered FAR 23 airplanes. Section 6 of the document discusses modification considerations. Paragraph 6 b. states,
The applicant should be particularly aware that in the absence of structural substantiation, FAR 23.1505(c) requires the airspeed indicator red line (VMO/MMO) not exceed VC (usually top of the old green arc). This may limit operational usefulness of the airplane.
A certification plan was prepared to identify the regulatory requirements with which Texas Turbine Conversions had to show compliance in order to receive STC approval. The certification plan, dated 21 January 2001, was agreed to by the FAA and Texas Turbines Conversions. The certification plan made no reference to FAR 23.1505(c). The original flight test aircraft had been dive-tested on wheels to 202 mph IAS for a minimum of 3 seconds in smooth air, in accordance with FAR 23.251, during the FAA STC flight test certification program, with no unacceptable vibration or buffeting observed. The aircraft has also been flight tested on floats. The piston DHC-3 Otter was approved for operation on de Havilland wheel-skis; the Texas Turbine Conversions Super Otter had not been flight tested on wheel-skis during the FAA STC flight test program.
| Never-exceed speed (VNE) and design diving speed (VD) | Maximum operating speed (VMO) | |
|---|---|---|
| Land/ski plane | 192 mph IAS | 144 mph IAS |
| Sea plane | 183 mph IAS | 134 mph IAS |
The DHC-3 AFM stated that the range of speed between the maximum operating limit speed and the design diving speed should be intentionally entered only with due regard to prevailing flight and atmospheric conditions, turbulence in particular. That speed range was marked by the standardized yellow arc on the airspeed indicator (Appendix F). Based on the results of the Texas Turbine Conversions STC flight test program, no changes were made to any of the airspeed limits that applied to the original piston-engine DHC-3 Otter.
At least 2 other DHC-3 Otter turbine-engine STC conversions are popular with DHC-3 Otter operators:
- TC STC SA01-111, FAA STC SA09857SC: conversion to Walters M601E-11 turbine engine;
- TC STC SA89-32, FAA STC SA3777NM: conversion to PT6A-34 or -135 or -135A turbine engine.
In both of these conversions, the aircraft were speed-restricted to the top of the original green arc on the airspeed indicator (144 mph) in accordance with FAR 23.1505 (c), as part of the STC requirements (Appendix F).
The FAA issued AD 2011-12-02 following the accident; it applied to Viking Air Limited Model DHC-3 Otter airplanes equipped with a Honeywell TPE331-10 or -12JR turboprop engine installed per FAA STC SA09866SC (Texas Turbines Conversions, Inc.). The AD did not refer to Transport Canada STC SA02-15, and Transport Canada did not issue an equivalent AD. The FAA AD was prompted by analysis that showed that airspeed limitations for the affected airplanes had not been adjusted for the installation of the turboprop engine, and was issued to prevent the loss of airplane structural integrity due to the affected airplanes being able to operate at speeds that exceed those determined to be safe by the FAA. Footnote 7 The AD restricted the maximum certificated operating speed (VMO) for the land/ski plane to 144 mph and for the seaplane to 134 mph.
This was the fourth in-flight breakup of a DHC-3 Otter. Two had occurred in the 1950s and a third had occurred in 1970. All previous break-ups involved aircraft fitted with the Pratt & Whitney R-1340 radial engine.
1.6.4 Aircraft examination
An estimated 98% or more of the wreckage was recovered from the accident site. All of the recovered wreckage except for the engine was transported to the TSB Laboratory for detailed examination.
1.6.5 Engine examination
The Honeywell (Garrett) TPE331-10-511C turboprop engine was disassembled and examined in detail at the Honeywell Product Integrity Teardown Laboratory in Phoenix, Arizona, with TSB oversight. The engine, while generally intact, had sustained significant impact damage. Examination identified no evidence of catastrophic engine failure, and no mechanical discrepancies that would have precluded normal operation of the engine were identified.
1.6.6 Fuel control unit examination
The engine was fitted with a Woodward hydromechanical fuel control unit (FCU). The FCU was bench-tested, disassembled, and examined in detail at the Woodward Governor Company facility in Rockford, Illinois, with US National Transportation Safety Board (NTSB) oversight. The FCU had sustained impact damage; however, it was able to be repaired sufficiently, without disturbance to critical settings, to allow bench testing. Several high fuel flow anomalies were identified during bench testing; no discrepancies that could account for the observed high fuel flow readings were identified. Component records indicated the FCU had been overhauled in 2001, and function-tested and installed on the engine in 2002. There was no record of the FCU having been removed from the engine, repaired, or function-tested since 2002, and no record or report of recent engine operating deficiencies. The P2T2 loading spring assembly contained incorrect parts from an unknown source. When the unit is shipped from Woodward, the cover on the P2T2 loading spring assembly is secured with two screws, which are lockwired; lead clips or seals are not normally installed on the lockwire. There was no record of the P2T2 loading spring assembly having been replaced. These parts were replaced with the correct parts for additional bench-testing, but no change to the high fuel flow bench-test results was observed.
1.6.7 Propeller examination
The aircraft was equipped with a Hartzell propeller, model number HC-B4TN-5N/LT. This propeller is a 4-bladed, single acting, hydraulically operated, constant-speed model with feathering and reversing capability. No discrepancies that would preclude normal operation of the propeller prior to impact were identified during examination of the propeller at the TSB Laboratory. The position of the blades, counterweights, and piston,indicated the blades were at a high blade angle, but not completely feathered, when the spinner was crushed at impact. Three of the 4 blades remained attached to the hub following impact; the lack of damage to the 3 attached blades indicated the propeller was not rotating or under power at the time of impact. The fourth blade appeared to have struck the ground first, causing it to bend and fail in the area of the blade retention shoulder and associated blade clamp.
1.6.8 Airframe structural examination
Both wings and the empennage had broken into several sections during the breakup sequence (Appendix G). The wreckage was laid out on a shop floor with the fuselage, wings, empennage, landing gear, and all flight controls geographically positioned to replicate an intact and assembled aircraft condition. Structural examination determined that the aircraft was operating beyond its maximum allowable speed when the breakup occurred, and that the breakup was initiated by both wings failing downwards in a negative overstress loading due to high speed.
There were several indicators of the wings having failed in a downwards direction. Aerodynamic torsion loads progressively build up across the span of the wing as the speed increases and reach their peak at the wing root. Both wings exhibited leading edge down torsional deformation, which was progressively more severe towards the inboard direction. Additional indicators of leading edge–down torsion were diagonal (forward-swept) buckles on both upper wing skins and a leading edge–down twist in the left rear wing attachment fitting. As well, both wing struts had failed in compression in multiple locations, which was consistent with the wings having failed in a downwards direction.
Damage and paint transfer evidence identified that the right wing had rolled under the fuselage after failure and had struck the leading edge of the left horizontal stabilizer during the breakup sequence. This indicated the horizontal stabilizer assembly was intact and attached to the fuselage when it was struck by the separating right wing. There was no evidence that airframe fatigue, corrosion, or any other pre-existing damage had contributed to any of the structural separations.
Aircraft flutter is a phenomenon in which the flying or control surfaces of an aircraft begin to vibrate in an unstable manner at progressively greater amplitude, which can lead to in-flight breakup. Factors commonly contributing to the onset of flutter include high speed, change in structural mass distribution, and reduction of structural stiffness. The DHC-3 Otter has a history of tailplane flutter; however in previously documented cases of DHC-3 Otter tailplane flutter, a reduction of power and airspeed at the moment of onset of flutter vibration prevented further flutter vibrations and had allowed a precautionary landing to be successfully completed.
Examination identified that it was improbable that the aircraft had experienced stabilizer and/or elevator flutter. All elevator balance weights were the correct weight and were securely attached in position. Damage to the elevator tabs and hinges was minimal and inconsistent with the tab and hinge damage seen in previous cases of tab flutter. Both elevators were broken in half, and their fractured spars were plastically deformed, indicating bi-directional bending. In addition, the skins of the left elevator had split along their trailing edge. While these were signatures of flutter, no reason was found why the stabilizer/elevator might have begun to flutter while the aircraft was being operated within the allowable flight envelope.
The pitch trim system on a DHC-3 Single Otter is a variable incidence tailplane system, whereby the incidence of the tailplane is adjusted in flight by rotating the TAILPLANE TRIM handwheel in the cockpit. Two hinged control tabs are fitted to the trailing edge of the DHC-3 Otter elevator. The hinged tab on the trailing edge of the left elevator is interconnected to the flaps, so as to reduce the amount of trim input required when the flap setting is changed; the hinged tab on the trailing edge of the right elevator is a servo tab.
The DHC-3 Otter had previously experienced occurrences of elevator tab flutter, and on 30 July 1968 Transport Canada issued Airworthiness Directive (AD) CF-68-13. The AD mandated the installation of a mass balance to the left elevator tab, in accordance with de Havilland Service Bulletin 3/6. C-GMCW was in compliance with this AD. Later in the aircraft's design life, when turbine conversions began to appear, occurrences of right elevator tab flutter began to occur. These flutter occurrences were a result of the right elevator tab control rod separating from the tab, allowing the tab to flap freely. A new right elevator servo tab and redundant control linkage had been installed on C-GMCW on 24 May 2006, at 14 214.7 airframe hours and almost 5 years before the accident, in accordance with Transport Canada STC SA 03-99 and AD CF-2006-02R1.
Detailed examination of the elevator, elevator tab, and rudder systems found no evidence of excessive free-play in the hinges or linkages and no other evidence of a pre-occurrence discrepancy that would have contributed to a loss of control. While there was partial evidence of tailplane excitation, it could not be determined if the excitation had induced a loss of control or was a result of high speed that occurred following a loss of control. All discontinuities were overload in nature, and were considered to be a result of the in-flight breakup.
The right tailplane hinge assembly (part number C3FS472-7, which secured the forward right side of the horizontal stabilizer to the fuselage, had fractured. The fracture surface exhibited shear lips and plastic deformation consistent with failure by overstress. One small thumbnail-shaped region of fatigue was observed on the hinge assembly; the region of fatigue was considered too small to affect the strength of the part. It was considered likely that the pre-existing fatigue crack served only to localize the failure.
The wheel-skis on the DHC-3 Otter are equipped with a trim unit that maintains the skis in a horizontal position during flight and prevents extreme up-and-down movements of the ski tips. The system includes check cables that extend from the front and rear ski tips and attach to the airframe. The check cables serve as a backup to the trim unit, and prevent extreme movement of the ski tips during landing on snowdrifts, which protects the trim unit from damage. Both trim units as well as both forward check cables had failed in overload. It was therefore considered probable that these components had failed during the breakup or ground impact.
The aircraft had a placard on the instrument panel that limited indicated airspeed to 150 mph. The placard was not associated with the Texas Turbine conversion, however, and was believed to have been inadvertently left over from the temporary airspeed limitation imposed by AD CF-68-13 in 1968.
The last GPS recording indicated that the aircraft was travelling at approximately 203 mph calibrated airspeed (CAS) (Appendix E). Analysis of the breakup and debris trail indicated the aircraft was travelling at 203 to 226 mph equivalent airspeed (EAS) at the point of breakup. It is probable that the aircraft exceeded one, if not both, of the limiting speeds of 192 mph IAS (VNE) Footnote 8 and 217 mph EAS (VD). Footnote 9
The aircraft may have entered an unusual attitude, such as nose-low inverted flight, during the final seconds of flight prior to the breakup; however, this could not be determined by structural analysis. Depending on the aircraft and the position of the nose relative to the ground, airspeed can build much more rapidly in inverted flight than in upright flight, and can reach or exceed red-line speed very quickly. If a nose-low inverted attitude is entered and recognized, the required immediate response would be to roll the aircraft upright and ease out of the ensuing dive.
1.6.9 Systems examination
The aircraft systems were examined, and no evidence of a malfunction was found. All flight controls were accounted for within the debris field, and pre-accident engine control and flight control continuity were confirmed. All flight control–system discontinuities were overload in nature and were considered the result of the in-flight breakup. Pre-accident flight control rigging and cable tensions could not be determined. Examination of the hydraulic flap-actuator extension identified that the flapsh were in the up position at impact.
The pitch trim system on the DHC-3 Otter is a variable-incidence tailplane system. The horizontal stabilizer is hinged at the front, and tailplane incidence is adjusted through a cable-operated screw jack actuator mounted to the rear of the stabilizer. Extension on the pitch trim actuator corresponded to a cruise or cruise descent setting with an aft c of g loading. This was consistent with the forward mid-range position of the pointer on the trim control index that was adjacent to the trim handwheel in the cockpit.
The aircraft was fitted with an emergency fuel shutoff/feather lever on the far right side of the engine control pedestal. The lever moves fore and aft between 2 locked positions. When the lever is locked forward, the engine fuel valve can be electrically opened and the feathering valve is closed, allowing the engine and propeller to operate normally. When the lever is locked aft, the fuel valve is manually shut off and the feathering valve is open, which shuts down the engine and feathers the propeller. The lever is normally in the locked-forward position at all times, including when the aircraft is parked on the ground. The lever would be locked aft only if activated by the pilot to address an emergency that required the engine to be shut down and the propeller to be feathered. Post-accident examination of the emergency lever indicated the lever was in the locked aft position at impact. It was considered unlikely that the lever had been forced into that position as a result of the impact.
An aircraft turnbuckle is a device that is used to adjust cable tensions in a cable-operated flight control system. Aircraft turnbuckles are adjusted so no more than 3 threads on each end terminal are visible on either end of the threaded barrel when the cable is adjusted to the correct tension. As well, aircraft turnbuckles are required to be safetied using lockwire or locking devices once the correct cable tension is achieved, to ensure tension is not lost due to rotation of the threaded barrel. Wreckage examination identified that while the aileron flight control system was continuous, the threaded barrel on the aileron balance cable was missing the required lockwire. No threads were visible on either end terminal, which indicated the threaded barrel had not backed off in service. CARs Standard 571.10 requires work that disturbs engine or flight controls to be inspected by at least 2 persons, often referred to as a dual inspection, to ensure correct locking of any parts disturbed by the maintenance performed.
1.6.10 Instrument examination
The attitude indicator, directional gyro, and turn-and-slip indicator were examined at the TSB Laboratory. All 3 instruments had significant impact damage. The directional gyroscope had a pneumatically-driven gyroscopic mass. An examination of the outer edge of the gyro mass and of the inside wall of the mass housing revealed circumferential scrape marks, indicating that the mass was spinning with high rotational energy at impact and that the vacuum system was serviceable at the time of the occurrence. Microscopic examination of the gyroscopic mechanisms of the remaining instruments did not provide any reliable information that could be used to determine if these gyroscopes were or were not spinning at impact.
1.6.11 Effect of turbine conversions
The conversion of piston-engine aircraft to turbine-engine aircraft allows an aircraft such as the DHC-3 Otter to routinely cruise at much higher speeds. Since gust loads Footnote 10 are proportional to speed, higher speeds result in higher gust loads. In addition, the different engine and propeller will result in different propeller wash patterns and airframe vibration harmonics. Vibrations and loadings will differ from one turbine conversion to another due to different engine rotation speeds, the number of propeller blades, and the direction of propeller rotation. All of these factors can combine to result in dissimilar and accelerated wear patterns on a converted aircraft. Accelerated wear could manifest itself as flight control rod-end and hinge looseness, and fatigue cracking. No indications were found on the occurrence aircraft to suggest that the precipitating event was a structural failure caused by looseness, fatigue cracking, or wear.
1.6.12 Incident at Withers Lake
The aircraft had been involved in a minor incident at the staging area on the Withers Lake ice strip on the second flight to Withers Lake on the morning of the accident. After landing, as the pilot was taxiing to position the aircraft for unloading, the aircraft struck a pile of lumber. The contact point was the left side of the fuselage, about 2 feet above ground immediately forward of the tail wheel. Following the incident, the pilot , with the help of an expeditor at the site, pushed on the tail of the aircraft to reposition the aircraft for taxi:the expeditor pushed on the right side of the aft fuselage, immediately below the right horizontal stabilizer, while the pilot pushed on the rudder. As the pilot was pushing on the rudder, a loud bang came from the aft fuselage.
The aircraft was unloaded and flown back to Mayo. Efforts during the investigation to determine the source of the abnormal bang were unsuccessful. The incident had not been reported to Black Sheep Aviation maintenance staff, and the empennage had not been inspected for associated damage by maintenance personnel before the accident. Detailed post-accident examination of the wreckage did not identify any damage that could be associated with the incident. The aircraft flew approximately 2.2 hours after the incident, prior to the accident.
1.6.12 Requirement to de-ice the aircraft on the morning of the accident
The pilot's first trip on the day of the accident was delayed for approximately 2 hours, because the aircraft had to be de-iced. No de-icing fluid was available at Mayo, so tarps and a forced-air heater had been used to remove the surface contamination. The pilot had helped with the work. The aircraft was considered to be free of ice or frost that had accumulated overnight, given that the accident occurred on the 7th flight of the day following the morning de-icing.
1.7 Meteorological information
The weather was suitable for VFR flight. Twelve minutes after the aircraft departed Mayo, the aviation routine weather report (METAR) recorded the Mayo weather as surface winds 070° true (T) at 5 knots and surface visibility as 20 sm. The cloud layer types and opacity were towering cumulus 2/8 based at 4500 feet agl, alto cumulus 1/8 based at 12 000 feet agl, and cirrus 1/8 based at 22 000 feet agl. Snow showers were occasionally moving through the area (Appendix C).
Weather analysis for the accident site area at the time of the accident identified no signs of icing, turbulence, or cloud cover to explain the chain of events in the accident. Cloud cover increased within a few hours of the accident, with towering cumulus and cumulonimbus developing across the region. It could not be determined with certainty if the pilot had flown into cloud at any time during the flight; however, weather analysis indicated the pilot would have most likely been able to remain VFR for the duration of the flight. The GPS data indicated the aircraft had tracked in a straight line to Rackla, except for a diversion to the left immediately before the breakup.
1.8 Aids to navigation
The accident flight was a VFR flight in VFR conditions; it is probable that the pilot was using the on-board GPS as the primary navigation aid.
1.9 Communications
There was no record of communications with the aircraft following take-off from Mayo.
1.10 Aerodrome information
The Mayo aerodrome is located at 63°36′59″N, 135°52′06″W, at 1653 feet asl. It has 1 gravel-surfaced runway that is oriented 240° and 060°, and is 4856 feet long and 100 feet wide.
The Rackla airstrip is located at 64°13′20″N, 133°12′26″W at 2825 feet asl. The airstrip was built in about 1966. It is a cleared gravel area that was bulldozed on the edge of the river to create an airstrip. The original usable length was 5000 feet. The current usable length is 3000 feet because the approaches have not been brushed out. The summer surface is pebbly gravel, and the winter surface is snow. No maintenance of the surface is conducted at any time.
1.11 Flight recorders
1.11.1 General
The aircraft was not fitted with—and was not required by regulation to be fitted with—a cockpit voice recorder (CVR) or a flight data recorder (FDR). The requirements for CVR and FDR equipment to be installed in aircraft are similar throughout the world, and are based primarily on the number and type of engines, and on the number of passengers seats in the aircraft. Canadian Aviation Regulations (CARs) 605.33 requires the following Canadian registered multi-engined turbine-powered aircraft to be fitted with an FDR:
- a type-certificated aircraft authorized to transport 30 or fewer passengers, configured for 10 or more passsenger seats and manufactured after 11 October 1991.
- a type-certificated aircraft authorized to transport 30 or fewer passengers and configured for 20 to 30 passenger seats.
- a type-certificated aircraft authorized to transport more than 30 passengers.
- a type-certificated aircraft authorized to transport cargo only and operated under Subpart 5 of CARs Part VII.
CARs 605.33 also stipulates that Canadian-registered multi-engined turbine-powered aircraft configured for 6 or more passenger seats and requiring 2 pilots must be fitted with a CVR.
1.11.2 Benefits of CVRs and FDRs
The benefits of recorded flight data in aircraft accident investigations are well known and documented. Flight recorders have been considered primary tools in large aircraft accident investigations for decades. Currently, CVRs and FDRs are considered the most comprehensive methods of capturing large amounts of flight data for accident investigtion purposes. Investigation reports involving aircraft not equipped with flight recorders occasionally contain data downloaded from GPS, engine monitors, or other non crash–protected non-volatile memory sources in lieu of flight recorder data, and radar data. Investigation reports that are able to use data from flight recorders as well as from non flight–recorder sources that contain non-volitile memory are higher quality and more likely to identify safety deficiencies than reports that do not.
1.11.3 Alternatives to conventional CVRs and FDRs currently available
Commercially operated aircraft weighing less than 5700 kg are usually not fitted at manufacture with the system infrastructure required to support an FDR, and conventional FDRs would require expensive modifications in order to be installed in this category of aircraft. Several affordable, stand-alone, lightweight flight recording systems that can record combined cockpit image, cockpit audio, aircraft parametric data, and/or data-link messages, and that require minimal modification to the aircraft to install, are currently being manufactured. ED-155 Minimum Operational Performance Specification (MOPS) for Lightweight Recording Systems published by the European Organization for Civil Aviation Equipment (EUROCAE) Footnote 11 defines the minimum specifications for lightweight flight recording systems.
Several helicopter operators have already embraced this type of technology as a basis for the Flight Operational Quality Assurance (FOQA) Footnote 12 program recommended by the FAA. At least 1 operator has recognized that the presence of a lightweight flight recorder system has had a positive influence on flight crew decision making.
1.11.4 Number of aircraft on the Canadian Civil Aircraft Register
In June of 2012, there were 35 264 aircraft listed on the Canadian Civil Aircraft Register. Commercial registered aircraft accounted for 6957 of that total; of these, 5453 weighed less than 5700 kg. Most commercial aircraft weighing less than 5700 kg are operated under Subparts 702 and/or 703 of the CARs. Canadian aircraft operated commercially under these subparts are typically single- or multi-engined piston-powered aircraft, or single- or multi-engined turbine-powered aircraft carrying 9 passengers or fewer. Most of these aircraft are not governed by the provisions of Section 605.33, and are therefore not required to be fitted with any type of flight recorder.
1.11.5 TSB accident statistics
Between 01 January 2002 and 05 July 2012 there were 932 accidents involving Canadian-registered commercial aircraft. Approximately 88% of these accidents involved aircraft operating under Subparts 702 or 703 and accounted for 82% of all serious injuries and 87% of all fatalities in accidents involving Canadian commercial aircraft.
| Commercial Air Services category | Accidents | Fatal injuries | Serious injuries |
|---|---|---|---|
| 702-Aerial Work | 285 | 57 | 48 |
| 703-Air Taxi Operations | 539 | 179 | 111 |
| 704-Commuter Operations | 56 | 23 | 18 |
| 705-Airline Operations | 52 | 12 | 17 |
| Total | 932 | 271 | 194 |
Numerous TSB aviation investigation reports have referred to investigators being unable to determine the reasons why an accident occurred, due to the lack of on-board recording devices; these include reports A01W0261, A02W0173, A03H0002, A05W0137, A05C0187, A06W0139, A07Q0063, A07W0150, A09A0036, A09P0187 and A10P0244, which are available on the TSB website.
Data recovered from the onboard KMD150 GPS was very limited due to the small number of parameters and the large 30‑second time interval between consecutive data points. Additional critical data was not available through other sources in this investigation.
ED 155–compliant flight recorders can record image, audio, parametric, and data-link data in one recording medium. A functioning lightweight ED 155–compliant flight recording system with cockpit-imaging capability can provide the following information at a recording interval of 2 seconds or less between consecutive data points:
- actual weather as recorded through the cockpit windows;
- flight instrument, engine instrument, and warning indications;
- pilot actions, control inputs, and aircraft response;
- engine control positions;
- comprehensive altitude, speed, and GPS tracking data;
- aircraft flight attitude data;
- acceleration data;
- ambient sound; andperhaps more information depending on the data collection technology offered by individual lightweight flight recording system manufacturers.
In order to identify causal/contributory/risk findings and safety deficiencies, investigators need to determine reliably the events, circumstances, and factors that led to an accident. Often in the case of small aircraft not fitted with traditional flight and voice recorder technology, as in this investigation, facts critical to the investigation, including actual weather, ambient sound, pilot actions, and aircraft response, are never recovered. As a lightweight flight recorder system can capture these types of information, the presence of one increases the opportunity to understand fully why an accident occurred and to identify potentially significant safety deficiencies.
1.11.6 International examples
There are numerous examples of accident investigations involving small aircraft that were hampered by the lack of flight recorder data.
The Unites States NTSB has issued numerous recommendations (A-99-060, A-99-069, A-99-074, A-03-062, A-03-064, A-03-065, A-09-009, A-09-10, A-09-11, A-09-90, A-09-99, A-09-106, and A-10-168) calling for the installation of crash-protected video and other recording devices in aircraft not otherwise fitted with CVRs and FDRs.
The NTSB recently investigated another accident involving a turbine-powered de Havilland DHC-3 Otter. The accident occurred in Alaska; 5 occupants including the pilot sustained fatal injuries, and 4 sustained serious injuries. The final report stated that the lack of a cockpit recorder system with the ability to capture audio, images, and parametric data contributed to the investigation's inability to determine exactly what occurred in the final minutes of the flight. NTSB recommendation numbers A-09-10 and A-09-11 were reissued on 09 June 2011 as a result of this accident.
In February 2006 the Australian Transportation Safety Bureau (ATSB) issued Safety Recommendation R20060004, recommending that the Australian Civil Aviation Safety Authority (CASA) review the requirements for the carriage of on-board recording devices in Australian registered aircraft as a consequence of technological developments.
In 2010 the UK Air Accidents Investigation Branch (AAIB) issued Safety Recommendation 2010‑016, recommending that the International Civil Aviation Organisation (ICAO) adopt the proposals of its Flight Recorder Panel that the installation of flight recorders be required on turbineengine–powered aeroplanes of a maximum certified takeoff mass of 5700 kg or less.
1.11.7 ICAO Annex 6 Small Aircraft Flight Recorder Standard and Recommendation
ICAO has published a standard for flight recorders in small aircraft in the 9th edition of ICAO Annex 6, dated July 2010. Paragraph 6.3.1.2.1 in Annex 6 states:
All turbine-engined aeroplanes of a maximum certificated take-off mass of 5 700 kg or less for which the application for type certification is submitted to a Contracting State on or after 1 January 2016 shall be equipped with:
- a Type II FDR; or
- a Class C AIR capable of recording flight path and speed parameters displayed to the pilot(s); or
- an ADRS capable of recording the essential parameters defined in Table A9-3 of Appendix 9.
Paragraph 6.3.1.2.2 in Annex 6 states:
Recommendation.— All turbine-engined aeroplanes of a maximum certificated take-off mass of 5 700 kg or less for which the individual certificate of airworthiness is first issued on or after 1 January 2016 should be equipped with:
- a Type II FDR; or
- a Class C AIR capable of recording flight path and speed parameters displayed to the pilot(s); or
- an ADRS capable of recording the essential parameters defined in Table A9-3 of Appendix 9.
Contracting ICAO states are required to notify ICAO of any differences between their regulations and practices and the standards contained in Annex 6 (ICAO states are not required to file differences pertaining to recommendations, however). It is unknown if Transport Canada has filed or will be filing a difference to para 6.3.1.2.1. The standard and the recommendation will apply initially to a very limited number of Canadian commercial aircraft, and no aircraft in the existing fleet.
In 2009, EUROCAE published ED-155, which defines the minimum specification to be met for aircraft required to carry lightweight flight recording systems, which may record image, audio, parametric, and data-link data in one recording medium. The aircraft modification required to support lightweight flight recording systems is minimal. Besides incident and accident investigation, and where the information is not privileged or protected by law, as is the case in certain countries, ED-155 recorders can also be used for purposes such as flight training and flight data monitoring, which may confer a significant additional safety benefit. Footnote 13
A Technical Standard Order (TSO) is a minimum performance standard for specified materials, parts, and appliances used on civil aircraft (FAA definition).
- The FAA issued TSO-C176 on 28 July 2007 to address minimum performance standards for aircraft cockpit image recorder systems; it applies to equipment intended to record aircraft flight images and store the data in crash-protected memory to assist in accident or incident investigations. TSO-C176 products are required to meet the minimum performance standards in EUROCAE ED-112 MOPS for Crash Protected Airborne Recorder Systems, dated March 2003.
- The FAA also issued TSO-C197 to provide minimum performance standards for information collection and monitoring systems. TSO-C197 products are required to meet the minimum performance standard qualification and documentation requirements in EUROCAE ED-155.
1.11.8 GPS flight data
The GPS had recorded 36 units of data for the occurrence flight. Each 30-second data point included a date, time, latitude, longitude, GPS speed in knots, Footnote 14 GPS track in degrees true (°T) and GPS altitude in feet asl. The GPS speeds represented speed through space, and were based on the vector sum of the aircraft's horizontal speed and vertical speed with respect to the ground.
Based on these data, it was determined that the aircraft had reached an altitude of approximately 11 500 feet asl about 13.5 minutes after take-off on the accident flight. The aircraft had remained on track to Rackla at that altitude for approximately 2 minutes, and had then commenced a descent at a slightly increased speed. Over the final 2 minutes of the flight, the aircraft entered a shallow left turn, and the track changed from 66°T through 360°T to 286°T, over a total distance of approximately 4.4 sm. The GPS data did not indicate that the aircraft had entered a spiral dive. Between the last two 30-second data points, the GPS altitude decreased by 2392 feet and the GPS speed through space increased from 177 to 241 mph calibrated airspeed (CAS), indicating a loss of control. Due to the capability of the GPS, the GPS data were insufficient to determine the aircraft attitudes and movements leading up to the apparent loss of control, the pilot's actions, and the functioning of the aircraft systems (Appendix E).
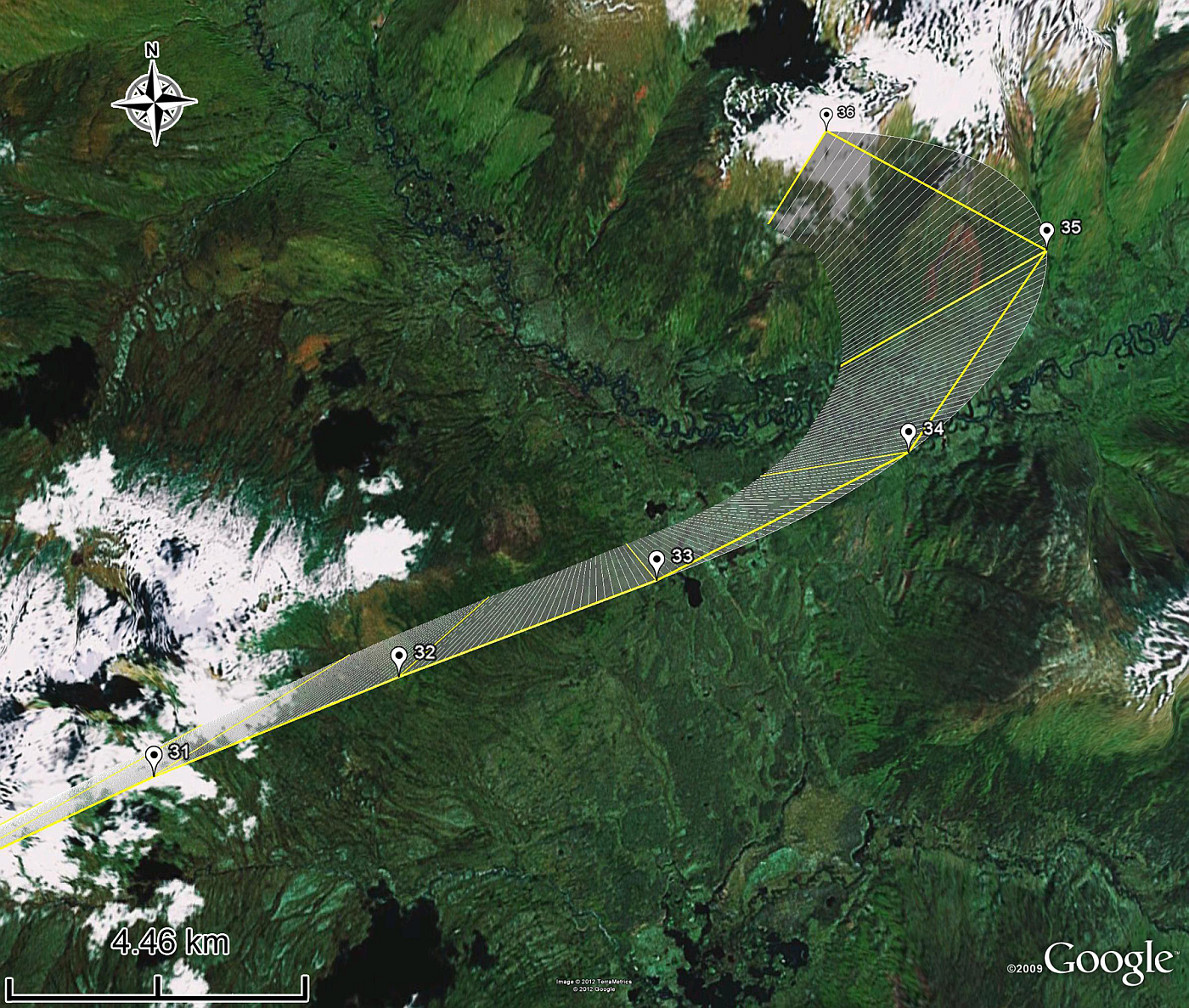
| Data point | GPS track (°M) | GPS altitude (feet asl) | Calibrated airspeed (mph) |
|---|---|---|---|
| 31 | 64.7 | 11 337 | 150 |
| 32 | 71.1 | 11 342 | 147 |
| 33 | 66.1 | 11 177 | 153 |
| 34 | 58 | 10 984 | 154 |
| 35 | 9.1 | 10 652 | 152 |
| 36 | 286 | 8 262 | 203 |
Note: The data points are spaced 30 seconds apart. In the 30 seconds between the last 2 data points, the aircraft descended approximately 2000 feet and accelerated approximately 50 mph. The breakup must have occurred within 30 seconds of the last data point.
The GPS speeds in all 2000 units of recorded data, representing 24 flights that had taken place within 3 days of the accident plus the accident flight , were converted to CAS in mph, using a computer-sourced algorithm model that considered the forecast upper wind speed and direction; the forecast temperature at altitude; the GPS-derived altitude for each data point; and an nm-to-sm conversion. The results were considered accurate to within plus or minus 6 mph IAS. The difference between IAS and CAS for the DHC-3 Otter is small—in the neighbourhood of +3 mph at cruising speeds.
Analysis of the GPS speeds indicated the pilot was operating the aircraft at or above 144 mph IAS, which was the top of the green arc on the Honeywell (Garrett)-powered DHC-3 Otter airspeed indicator, for a significant percentage of time. This speed was exceeded at some point in all flights, and was exceeded for the entire cruise portion in 6 flights, and for over 50% of the cruise portion in 2 flights. The analysis indicated that on the occurrence flight the aircraft was being operated at or slightly above an indicated airspeed of 144 pmh IAS when it began to track left.
1.12 Wreckage and impact information
The wreckage was spread over a debris field approximately 800 feet wide and 1300 feet long (Appendix H) at between 4200 and 4600 feet asl on a remote treed hillside in the central Yukon. Ground scars and damage to trees suggested that the wreckage, including the fuselage, had no significant horizontal velocity at impact. The engine remained attached to the firewall following impact.
There was 4 to 5 feet of snow on the ground at the accident site, which precluded recovery of all wreckage during the initial recovery phase. The accident site was revisited in early June, after the snow had melted, to complete the wreckage recovery. All flight controls, all engine and propeller components, and all major structural components, including the wings, fuselage, empennage, and landing gear were found within the debris field and were recovered for examination. Initial examination of the wreckage took place in Whitehorse; the wreckage was subsequently transported to the TSB Laboratory for detailed examination.
A trajectory analysis of 71 separated components following the in-flight breakup indicated that the breakup had occurred at between 6742 and 8257 feet asl (2450 and 4000 agl), at a groundspeed of between 224 and 256 mph, and a flight path angle of approximately −73°.
| Parameter | Minimum | Nominal | Maximum | Change from nominal |
|---|---|---|---|---|
| Wind speed | 1.5 knots | 3 knots | 4.5 knots | 50% |
| Wind direction | 175 °T | 185 °T | 195 °T | 5% |
| Ground speed | 224 mph | 240 mph | 256 mph | 6.7% |
| Altitude | 6742 feet | 7500 feet | 8257 feet | 10% |
| Flight path angle | -72.9 ° | -72.5 ° | -72.1 ° | 0.5% |
| Ground track | 281 °M | 283 °M | 285 °M | 0.5% |
1.13 Medical and pathological information
The pilot had been diagnosed with a faint systolic heart murmur during an annual Transport Canada pilot medical on 15 March 2011, and had been instructed to submit an echocardiogram to the examining doctor and Transport Canada before the end of April 2011. The echocardiogram had not been submitted prior to the accident; however, based on autopsy, toxicology, and other medical records, there was no information to indicate that the pilot's performance was degraded by physiological factors or a sudden medical event.
Due to the amount of flying the pilot had done in the days preceding the accident (Appendix D), a human factors analysis of the pilot's sleep–wake history was performed to assess his level of fatigue at the time of the accident.
Because it was not possible to obtain information on the pilot's normal sleep patterns and actual sleep times in the period leading up to the occurrence,, his sleep was estimated using available data.
The pilot likely had between 9 and 15.25 hours off between duties. The approximate start and finish times of the pilot's duty days are listed below.
| Date | Time off before starting this duty | Start time | Finish time |
|---|---|---|---|
| 21 Mar 11 | >20 days | 0915 | 1700 |
| 22 Mar 11 | 15.25 hours | 0815 | 2000 |
| 23 Mar 11 | 12 hours | 0800 | 2130 |
| 24 Mar 11 | 9 hours | 0630 | 2015 |
| 25 Mar 11 | 10.5 hours | 0645 | 2130 |
| 26 Mar 11 | 9.25 hours | 0645 | 1945 |
| 27 Mar 11 | 10.75 hours | 0630 | 1945 |
| 28 Mar 11 | 10.5 hours | 0615 | 1945 |
| 29 Mar 11 | 10.5 hours | 0615 | 2045 |
| 30 Mar 11 | 9.5 hours | 0615 | 2100 |
| 31 Mar 11 | 9.5 hours | 0630 | Accident at 1515 |
Given that the pilot had at least 9 hours off between shifts, there would likely have been enough time for the 5-minute commute, meals, and personal hygiene as well as between 7 and 8 hours of sleep per night. The TSB did not find any information suggesting that the pilot engaged in social activities at the base.
Telephone records indicated the pilot had sent 2 text messages, one at 0036 and one at 0041, 2 nights prior to the accident on March 30. There are at least 3 possible effects on the pilot's sleep from the texting:
- First, the pilot may have stayed awake later than normal to text, which would have significantly reduced total sleep time for that night.
- Second, the pilot may have woken up briefly to texti. This would have reduced total sleep time by only about 30 minutes.
- Third, the pilot may have started sleeping earlier that evening, spontaneously woke up and decided to spend a short time texting.
According to the duty periods listed above, the pilot could have started to sleep anytime after 2045 on 29 March. With a 5-minute interruption to sleep, there was still over 9.25 hours available for sleep and other activities. This possibility would have had no negative effect on the pilot's total sleep time. Furthermore, the pilot's total sleep time was not reduced by texting the night before the accident. This last period of sleep could have offset any reduction in sleep quantity from the previous night.
In addition, the investigation determined that the pilot was physically fit; was able to maintain vigilance for long periods of time while driving to and from remote locations; and was regularly sleeping between 2200 and 0530 or 0600 (i.e., 7.5 to 8 hours) for the 10 days leading up to the accident.
The human factors analysis above was validated using the Fatigue Avoidance Scheduling Tool (FAST). The FAST analysis confirmed the conclusion that fatigue was not likely.
The following factors were also considered as potentially contributing to fatigue: difficult meal scheduling; limited quality of diet; cumulative exposure to a loud cockpit environment; and wintry work conditions.
Given this data, and in the absence of contradictory information—and in spite of the high number of work hours—the TSB estimated that the pilot had obtained enough sleep on the 10 nights preceding the accident. Therefore, the pilot was likely not fatigued enough to fall asleep at the time of the accident.
People who are mildly fatigued fall asleep within 10 to 15 minutes if they are left alone in a dark room and instructed to try to sleep. Footnote 15 In the same situation, people who are moderately fatigued fall asleep within 5 to 10 minutes; people who are severely fatigued fall asleep in less than 5 minutes.
It is very unlikely that the pilot was severely fatigued. This diagnosis is normally reserved for people suffering from sleep disorders such as obstructive sleep apnea and narcolepsy. There was no information to suggest that the pilot was suffering from a sleep disorder. If the pilot was moderately fatigued, it would have taken him at least 5 minutes to fall asleep and he would have had to have been trying to sleep rather than resisting it.
GPS data indicated that the aircraft entered a shallow descent after 16 minutes of flight (a 13-minute climb followed by 3 minutes at altitude). The shallow descent lasted approximately 3 minutes. Although a shallow descent may be consistent with the pilot falling asleep and ceasing to control the aircraft, it is unlikely that the pilot fell asleep that quickly.
As mentioned above, the aircraft was not fitted with an autopilot. This means that the pilot would have been awake for 16 minutes while manually controlling the aircraft through take off, climbing to altitude, and maintaining altitude. It could be argued that level flight could be maintained by a fatigued person and, given that very few control inputs would be required, the fatigue could lead to falling asleep. However, level flight was maintained for only 3 minutes. Falling asleep and ceasing to control the aircraft within 3 minutes is highly unlikely for a person who is not severely fatigued.
1.14 Fire
There was no in-flight or post-impact fire.
1.15 Survival aspects
The accident was not survivable due to the severity of impact forces.
1.16 Tests and research
A number of tests and research was conducted at the TSB Laboratory (Appendix A).
1.17 Organizational and management information
The aircraft was being operated under Canadian Aviation Regulations Part 703. Black Sheep Aviation operated 4 aircraft types in day VFR operations, all under CARs 702 and 703. The Company Operations Manual stated:
Operational Control is delegated to the Pilot-in-Command of a flight by the Operations Manager, who retains responsibility for the day-to-day conduct of flight operations. Flights operated under this system are self-dispatched and released by the pilot-in-command.
1.18 Additional information
1.18.1 Use of oxygen
CARs 605.32(1) governing the use of oxygen during flight states, “where an aircraft is operated at cabin-pressure-altitudes above 10 000 feet asl but not exceeding 13 000 feet asl, each crew member shall wear an oxygen mask and use supplemental oxygen for any part of the flight at those altitudes that is more that 30 minutes in duration.” CARs 605.32 (2) states, “where an aircraft is operated at cabin-pressure-altitudes above 13 000 feet asl, each person on board the aircraft shall wear an oxygen mask and use supplemental oxygen for the duration of the flight at those altitudes.” Black Sheep Aviation pilots often flew the turbine-powered DHC-3 Otters at altitudes of 10 500 to 12 500 feet for less than 30 minutes per flight. The aircraft were unpressurized and were not equipped with supplemental oxygen.
Review of the GPS data identified that the pilot had flown above GPS altitudes of 10 000 feet on 12 of 25 recorded flights. On 1 flight, the aircraft reached a maximum GPS altitude of 16 228 feet and was above 13 000 feet for 16 minutes. On the day of the accident the pilot was above 10 000 feet and below 11 800 feet, without oxygen, during 6 flights. Flight times above 10 000 feet ranged from 7.5 minutes to 18 minutes per flight; the total time above 10 000 feet was 89 minutes over a period of 6.5 hours. As the pilot was below 10 000 feet for about 77% of the time on the day of the accident, and hypoxia is remedied when oxygen levels improve, hypoxia is not considered to have affected the pilot's peformance.
1.18.2 Transport Canada process validation inspection
A post-accident process validation inspection was conducted by 2 Transport Canada inspectors approximately 2 weeks after the accident. This inspection consisted of a review of Black Sheep Aviation records to look for immediate company issues and confirm regulatory compliance. Unless significant deficiencies are identified by a review of company records, no further investigation is normally undertaken by Transport Canada. Seven minor record keeping deficiencies were identified in this case; none was considered to be a factor in the occurrence. During that inspection, the review of the existing company flight and flight duty-time records indicated that the accident pilot had been complying with regulatory requirements for flight time and flight duty time.
2.0 Analysis
2.1 General
The GPS data indicated that the flight to Rackla had progressed normally until approximately 3 minutes before the accident. The aircraft had climbed on track to about 11 500 feet asl in approximately 13 minutes after departure from Mayo, and had remained at that altitude for approximately 3 minutes, before entering a shallow descent. Over the final 2 minutes of flight the aircraft tracked left through approximately 145°, although the initial speed, altitude, and track changes during that time were not indicative of a sudden loss of control. This deviation from the normal flight path suggests that something had occurred. Over the final 30 seconds of flight the aircraft lost nearly 2400 feet in altitude and the GPS speed through space increased from 177 mph to 241 mph. This data was indicative of a loss of control and it is presumed the aircraft broke up immediately after the last GPS data unit was recorded. Due to the GPS capability, the GPS data were insufficient to determine the aircraft attitudes and movements leading up to the loss of control; the flight path between the 30-second data points; the pilot's actions; and the functioning of the aircraft systems.
The pilot was experienced on the aircraft type, and was flying a familiar route with a familiar load in a familiar aircraft on the fourth trip and seventh flight of the day. There was no radar information for the accident flight; no communication record with the aircraft after the aircraft departed Mayo; no witnesses to the accident, no survivor; and the aircraft was not fitted with a flight data recorder (FDR) or a cockpit voice recorder (CVR). The aircraft departed controlled flight for reasons which could not be determined, and broke up due to high speed. The analysis will therefore focus on several possible scenarios considered during the investigation in an effort to identify, through a process of elimination, the events and unsafe conditions that could have led to the accident.
2.2 Overspeed operation
TSB analysis of the GPS data indicated the pilot had been operating the aircraft at or above the normal operating limit speed of 144 mph IAS, which was the top of the old green arc on the airspeed indicator dial, for a significant percentage of the time in the period 29 March to 31 March 2011. However, because FAR 23.1505 (c) had not been referenced on the Texas Turbine Conversions de Havilland DHC-3ST Otter certification plan and had been inadvertently missed as being applicable, the airspeed limits were not reduced as part of the FAA STC certification program. This discrepancy was not identified during the Transport Canada familiarization of the STC. As the Texas Turbines DHC-3ST Otter Flight Manual Supplement made no reference to maximum airspeed limits, the airspeed limits stated in the original DHC-3 AFM applied. Therefore, at the time of the accident, the airspeed limits and the speed range markings on the airspeed indicator were the same as those approved for the piston-powered version of the DHC-3 Otter, and there were no AFM limitations, other than with due regard for turbulence, to prevent intentional operation at speeds within the yellow caution arc on the ASI. While it was apparent that the pilot had been operating the aircraft intermittently at speeds above 144 mph IAS, there was no physical evidence that this had contributed to the accident.
Although operation at speeds above 144 mph IAS did not appear to have been a factor in the occurrence, the FAA issued AD 2011-12-02 after the accident, mandating reduced airspeed limitations and marking of the airspeed indicator accordingly on DHC-3 Otter aircraft equipped with a Honeywell TPE331-10 or -12JR engine installed per FAA STC SA09866SC. The AD did not apply to aircraft converted under Transport Canada STC SA02-15, and Transport Canada did not issue an equivalent AD.
If owners of a DHC-3 Otter converted in accordance with STC SA02-15 are not aware of or have not complied with AD 2011-12-02, those aircraft may be at risk of loss of structural integrity due to operation at speeds in excess of those determined to be safe by the FAA.
2.3 Tailplane flutter/structural failure
There had been 3 previous in-flight breakups of piston-powered DHC-3 Otter aircraft. The DHC-3 Otter had a lengthy history of tailplane problems, including failures of the left and right elevator tab systems that resulted in elevator flutter. As well, the requirement to move the red line on the dial face of the airspeed indicator back to the top of the old green arc had been overlooked during the FAA STC flight test and approval program for the Honeywell(Garrett) turbine-powered DHC-3 Otter. The reason for this requirement would have been to ensure the design cruising speed (VC) of 144 mph IAS on wheels and skis or 134 mph on floats was not exceeded in flight, which could easily occur with the significantly more powerful Honeywell (Garrett) turbine engine. Considering this history, tailplane flutter and structural failure of the aircraft within the structural design limits posed 2 potential accident scenarios.
Extensive examination and analysis of the wreckage did not identify any structural or mechanical discrepancies likely to have contributed to an in-flight loss of control and high-speed descent, or any discrepancies that would have prevented normal operation of the aircraft. Pre-accident flight control continuity was confirmed during the wreckage examination; there was no evidence of excessive freeplay in the flight control hinges or linkages; no evidence that flutter had induced a loss of control; and no evidence of significant corrosion in the airframe. Structural analysis determined that, at the time of the breakup, the flight loads had exceeded the design limit due to high speed. While some evidence of tailplane excitation was observed during the wreckage examination, it could not be determined whether the excitation had precipitated an apparent loss of control or was the result of a loss of control. As it appeared the aircraft was operating within its allowable envelope when it first started to deviate from the intended flight track, there was no identified reason for stabilizer/elevator flutter to be the initiating event.
Detailed examination of the wreckage did not reveal the source of the noise associated with the pilot pushing on the rudder during the Withers Lake incident, and did not identify any damage that could be attributed to the incident. The Withers Lake incident was therefore discounted as a factor in the occurrence.
2.4 Pilot disorientation
Loss of control in instrument meteorological conditions (IMC) and entry into an unusual attitude, such as a spiral dive or inverted flight, was also considered as a possible scenario. Although there were snow showers moving through the area on the day of the accident, the weather was suitable for VFR flight. At worst, the pilot would have had to divert around the occasional localized snow shower in order to remain under VFR. Weather analysis for the accident site area at the time of the accident identified no signs of icing, turbulence, or cloud cover to explain the chain of events in the accident. It was not determined if the aircraft had entered cloud or flown above cloud during any portion of the flight; however, given the existing weather conditions, entry into cloud would have been deliberate rather than inadvertent. As well, there was no evidence to support a flight instrument failure. The GPS data identified that a significant loss of altitude and a rapid increase in speed had occurred between the last two 30 second data points. This would indicate the aircraft had entered either a steep, nose-down but upright flight attitude, or a nose-down and inverted flight attitude; however, the flight attitude of the aircraft at the point of breakup could not be determined. The distance covered between successive data points, and the track changes indicated by the last 60 seconds of GPS data, were not consistent with the aircraft having entered a spiral dive prior to breakup. The wings having failed in negative loading suggested the pilot was not attempting a dive recovery at the time of the accident.
2.5 Pilot incapacitation
Pilot incapacitation was considered as a fourth possible scenario, because there were several indications that the pilot had not responded when the aircraft entered an apparent loss of control situation. As well, the pilot had recently been diagnosed with a faint systolic heart murmur. There had been no emergency radio call from the aircraft following departure from Mayo, and the aircraft had sufficient altitude for a call to have been heard by other aircraft in the area and by the Mayo community aerodrome radio station (CARS). Given that the aircraft deviated from the intended flight path approximately 3 minutes prior to the accident, there should have been sufficient time for an emergency radio call. In addition, the aircraft speed increased rather than decreased over the final minutes of flight, and the aircraft had not been re-trimmed from a normal cruise or cruise descent trim position. Had the pilot experienced a nose-down pitch-control problem, it is expected that the pilot would have attempted to re-trim the aircraft to a nose-up position. Furthermore, the negative wing loading at breakup indicated the pilot had not initiated an effective dive recovery prior to the breakup. As well, the locked aft position of the emergency fuel shutoff/feather lever and the near feather–position of the propeller blades at impact indicated the pilot had attempted to respond to whatever was occurring by shutting down the engine at or near the point of breakup.
Nothing was found in autopsy, toxicology, and other available medical records to indicate that the pilot's performance was degraded by physiological factors. Without further tests such as an echocardiogram when the pilot was alive, confirmation of and the significance of the heart murmur could not be determined.
2.6 Pilot fatigue
Performance and judgment degradation due to fatigue were also considered possible contributing factors, as the pilot was functioning in a high-tempo work environment, the pilot's duty days had exceeded 14 hours several times in the previous 10 days, and the requirement for 1 extra hour of rest time per day was not being met. The pilot had also exceeded the 7-day 60-hour flight time limit imposed by regulations. Although it was estimated that the pilot's sleep/work cycles were sufficiently regular to avoid fatigue, he was helping unload or attend to the aircraft during the day—physically demanding tasks that left him no opportunity for rest breaks during the duty days.
Because the aircraft was not fitted with an autopilot, the pilot was hand flying and, even though the inherent stability of the aircraft was good, he had to be vigilant at all times. The accident took place after the aircraft had been airborne only 19 minutes; for the pilot to have fallen asleep in the 3 minutes of level flight that followed the 13-minute climb, he would have had to have been severely fatigued, a level of fatigue that the data did not support.
2.7 Regulatory issues
Regulatory compliance is one measure of individual and organizational attitudes to safety; several regulatory violations which constituted a risk to flight safety were identified. On at least 1 flight 2 days before the accident, the pilot had flown to 16 000 feet and had remained above 13 000 feet for approximately 16 minutes without oxygen. On this flight the pilot was not in compliance with CARs 605.32, which governs the requirements for and the use of oxygen by flight crew. Although the investigation did not consider the occurrence pilot to be affected by hypoxia on the day of the occurrence, the operation of unpressurized aircraft at higher altitudes without supplementary oxygen may increase the risk of adverse effect on reaction time and judgment.
The pilot had averaged 14.2 hours flight duty time per day in the 7 days prior to the accident and it is probable that the duration of the pilot's sleep the night before the accident was less than 8 hours. Based on regulation, and having accrued 68.2 hours of actual flight time in the 7 days prior to the day of the accident, the pilot should have been on a day off on the day of the accident, in order to reset the 7 day/60 hours flight time limit.
Compliance with flight time and flight duty time regulations is a responsibility shared by the operator and the pilot. Considering the distances flown (the distance from Mayo to Rackla was 94 sm, and the distance from Mayo to Withers Lake was 113 sm), the normal cruise speed of the aircraft, the air times indicated by the GPS data, and the regularity in the entries, company DHC-3 Otter pilots had, from 22 March to 30 March inclusive, routinely recorded journey log times inaccurately—by 0.1 to 0.3 hours less per flight. Because the flights were both numerous and short, the overall difference between the actual times and the recorded journey log times was significant. Pilots were being paid on the basis of per mile flown, so flying 1 or 2 more trips per day significantly increased a pilot's income. A downward adjustment of times recorded in aircraft journey log and flight duty records would have deferred flight interruptions due to scheduled maintenance and duty day limitations, increasing the pilot's opportunity to fly. The more flying the pilot did, the greater the pilot's income was, and the sooner the pilot could return to family life. The 1998 TC SATOPS report highlighted the risk of poor operational decision making by pilots paid by the mile or the flight hour.
At the time of the accident, the journey log entries were being transcribed to the company flight time and duty day records on a monthly basis. This system was inadequate for monitoring flight time, flight duty time, and rest periods daily, and contributed to the company not being aware that company pilots were not complying with applicable regulations during the Mayo campaign.
Inaccurate journey log entries constitute a risk to flight safety. In this case, one consequence of inaccurate journey log entries was errors in company flight and duty time records, which further diminished the effectiveness of the flight and duty time monitoring program in use by the company, and which misled Transport Canada inspectors. Incorrect journey log times ultimately could have contributed to a reduction in pilot performance due to fatigue. As well, the aircraft was being maintained under a program that required the aircraft to be inspected each 100 flight hours, and inaccurate air times could have had an adverse effect on the continued airworthiness of the aircraft.
The threaded barrel on the aileron balance cable turnbuckle had not been lockwired, indicating either that a dual inspection had not been carried out, or that it had been carried out incorrectly at some time in the past. The P2T2 loading spring assembly in the FCU contained incorrect parts from an unknown source, but there was no evidence to indicate this was a factor in the occurrence.
2.8 Requirement for lightweight flight recorder system in commercially operated aircraft not governed by CARs 605.33
The factual information that was gathered during the investigation was insufficient to determine what precipitated the probable loss of control. The aircraft was not fitted with, and was not required by regulation to be fitted with, a CVR or an FDR under CARs 605.33. If cockpit or data recordings are not available to an investigation, the identification and communication of safety deficiencies to advance transportation safety may be precluded.
Aerial work (CAR subpart 702) and air taxi operations (CAR subpart 703) have accounted for 88% of all accidents, 87% of all fatalities and 82% of all serious injuries involving Canadian registered commercial aircraft in the past 10 years. While the accident risks and rates remain high for aircraft operating in these categories, facts critical to determining the events, circumstances, and factors that lead to accidents involving these aircraft are often never recovered, due to the lack of a requirement for lightweight flight recording systems on these aircraft.
Several stand-alone lightweight flight recording systems which can record combined aircraft parametric data, cockpit audio data, airborne images and/or data-link messages are currently being manufactured. EUROCAE ED-155 MOPS for Lightweight Recording Systemsdefines the minimum specifications for lightweight flight recording systems. While performance standards and technical standard orders (TSOs) exist, there is no requirement for aircraft not governed by CARs 605.33 to be fitted with any type of flight recorder, and Transport Canada does not intend to extend those requirements to smaller aircraft.
Had the aircraft been fitted with a lightweight flight recording system, investigators would have been able to understand better the circumstances and events that led to the break-up, particularly the actions of the pilot. The data from a lightweight flight recording system would have become a primary tool in the investigation.
Flight data monitoring has been implemented in many countries, and it is widely recognized as a cost-effective tool for improving safety. In the United States and Europe—thanks to ICAO—many carriers have had the program for years. Some helicopter operators have it already, and the FAA has recommended it.
The use of recorders in the context of flight data monitoring has proven to benefit safety by giving operators the means to look carefully at the operation of their fleets over time; it allows for a review of objective data, which leads in turn to proactive identification and correction of safety deficiencies.
In Canada, some companies have decided to move in advance of regulatory requirements and to fit their aircraft with lightweight flight recording systems, which can record voice, video and other data. While the TSB believes this is a positive industry development, it should be noted that the Canadian Accident Investigation and Safety Board (CTAISB) Act protects on-board recordings and does not currently allow for their use outside a TSB investigation. Footnote 16 In the absence of a regulatory requirement, if the wider use of flight recording systems is to be encouraged for Canada's commuter, air taxi, and flight school operations, the law protecting on-board recordings would have to be modified to allow for the use of these systems by operators for safety purposes.
3.0 Findings
3.1 Findings as to causes and contributing factors
- The aircraft departed controlled flight for reasons which could not be determined, and broke up due to high speed.
3.2 Findings as to risk
- Inaccurate journey log time entries by pilots may have a negative bearing on pilot duty time monitoring and aircraft maintenance schedules.
- Pilot exceedance of duty time, such as the 60 hours flight time allowed by regulation for the 7-day period, may increase the risk of fatigue.
- Non-adherence to Federal Aviation Administration (FAA) Advisory Circular (AC) 23-14 during both the supplemental type certificate (STC) approval process and the familiarization of the STC by Transport Canada may have reduced the safety margins envisaged by AC 23-14, in turn increasing risk for loss of aircraft structural integrity.
- The operation of unpressurized aircraft at higher altitudes without supplementary oxygen may increase the risk of adverse effect on reaction time and judgment.
- If owners of a DHC-3 Otter converted in accordance with STC SA02-15 are unaware of or have not complied with AD 2011-12-02, the aircraft may be at risk for loss of structural integrity due to operation at speeds in excess of those determined to be safe by the FAA.
- The company practice of reconciling flight time and flight duty times on a monthly rather than a daily basis was inadequate to ensure compliance with CARs flight time and flight duty time limitations and rest period requirements.
- If cockpit or data recordings are not available to an investigation, the identification and communication of safety deficiencies to advance transportation safety may be precluded.
- If companies do not proactively monitor flight data, the identification and correction of safety deficiencies may be precluded.
- Identifying human factors is critical to understanding why accidents happen. If companies cannot use voice and video recordings proactively for safety purposes, they are deprived of opportunities to reduce risk and improve safety before an accident occurs.
3.3 Other findings
- While not considered a factor in the occurrence, the threaded barrel on the aileron balance cable turnbuckle was not lockwired.
- While not considered a factor in the occurrence, the P2T2 loading spring assembly in the FCU contained incorrect parts from an unknown source.
4.0 Safety action
4.1 Safety action taken
4.1.1 The Federal Aviation Administration
On 25 May 2011 the Federal Aviation Administration (FAA) issued Airworthiness Directive (AD) 2011-12-02. Effective on 02 June 2011, the AD applied to Viking Air Limited Model DHC-3 Otter airplanes (all serial numbers) that were equipped with a Honeywell TPE331-10 or -12JR turboprop engine installed per Supplemental Type Certificate (STC) SA09866SC (Texas Turbines Conversions, Inc.) and certified in any category.
The AD was prompted by analysis that showed airspeed limitations for the affected airplanes were not adjusted for the installation of a turboprop engine as stated in the regulations. The AD was issued to prevent the loss of airplane structural integrity due to the affected airplanes being able to operate at speeds exceeding those determined to be safe by the FAA.
The AD imposed a maximum operating speed (VMO) of 144 mph for DHC-3 Otter land/ski aircraft and 134 mph (VMO) for DHC-3 Otter seaplanes. Footnote 17
On 19 August 2011 the FAA issued AD 2011-18-11, which became effective on 03 October 2011. The AD applied to all Viking Air Limited Model DHC-3 Otter airplanes that were certified in any category. The AD resulted from an evaluation of revisions to the manufacturer's maintenance manual that added new repetitive inspections to the elevator control tabs. The AD stated that if these inspections were not done, excessive free-play in the elevator control tabs could develop. That condition could lead to loss of tab control linkage and severe elevator flutter, which could lead to a loss of control. Footnote 18
4.1.2 Black Sheep Aviation & Cattle Co. Ltd.
As a result of this accident Black Sheep Aviation established a system that correlates flight duty times to flight ticket invoice numbers. The information is entered on a new flight duty form which is delivered to company dispatch daily and and entered into company Flight Time/Duty Time/Rest Period records daily.
4.2 Safety action required
In June 2012, there were 6957 commercially registered aircraft listed on the Canadian Civil Aircraft Register, of which 5453 (78.4%) weighed less than 5700 kg. Most commercial aircraft weighing less than 5700 kg are operated under CARs subpart 702 Aerial Work and CARs subpart 703 Air Taxi Operations. These operations accounted for 88% of all accidents, 87% of all fatalities, and 82% of all serious injuries involving Canadian registered commercial aircraft in the past 10 years. If accidents involving commuter operations under CAR subpart 704 are added, the number of commercial air accidents jumps to 94% and the number of commercial air fatalities to 95%. Many of the aircraft operated by these companies are not required to be fitted with any type of flight recorder.
These smaller operators face challenging conditions, such as difficult terrain, and typically operate into smaller, more remote airports with less infrastructure. They often fly smaller, older aircraft with less sophisticated navigation and warning systems, which cause higher workloads for crew. Flight crews working for these operators are often working their way up in the system; they may have less training and experience, and often do not benefit from mentors able to pass on their experience.
In contrast, from 2001 to 2012, Canada's large carriers operating under CARs Subpart 705 have had only 1 fatal accident on home soil. Footnote 19 These large commercial carriers are required to have safety management systems (SMS), cockpit voice recorders (CVR), and flight data recorders (FDR). Many of these operators routinely download their flight data to conduct flight data monitoring (FDM) of normal operations. Air carriers with flight data monitoring programs have used flight data to identify problems such as unstabilized approaches and rushed approaches; exceedance of flap limit speeds; excessive bank angles after take-off; engine over-temperature events; exceedance of recommended speed thresholds; ground-proximity warning systems (GPWS)/terrain awareness and warning system (TAWS) warnings; onset of stall conditions; excessive rates of rotation; glide path excursions; and vertical acceleration. Footnote 20
Flight data monitoring has been implemented in many countries, and it is widely recognized as a cost-effective tool for improving safety. In the United States and Europe—thanks to ICAO—many carriers have had the program for years. Some helicopter operators have it already, and the FAA has recommended it.
Worldwide, FDM has proven to benefit safety by giving operators the tools to look carefully at individual flights and ultimately at the operation of their fleets over time. This review of objective data, especially as an integral component of a company safety management system, has proven beneficial in the proactive identification and correction of safety deficiencies and the prevention of accidents.
Several stand-alone lightweight flight recording systems which can record combined aircraft parametric data, cockpit audio data, airborne images and/or data-link messages are currently being manufactured. ED-155 MOPS for Lightweight Recording Systemspublished by the European Organization for Civil Aviation Equipment (EUROCAE) defines the minimum specifications for lightweight flight recording systems. While performance standards and TSOs exist, there is no requirement for aircraft not governed by CARs 605.33 to be fitted with any type of flight recorder, and Transport Canada does not intend to extend those requirements to smaller aircraft.
The development of lightweight flight recording system technology presents an opportunity to extend FDM approaches to smaller operations. Using this technology and FDM, these operations will be able to monitor, among other things, standard operating procedure compliance, pilot decision making, and adherence to operational limitations. Review of this information will allow operators to identify problems in their operations and initiate corrective actions before an accident takes place. In short, a whole new and promising avenue is now available to improve operational control and safety beyond CARs subpart 705 operations. In Canada, some companies have already decided to fit their aircraft with lightweight flight recording systems.
The Board acknowledges that there are issues that will need to be resolved to facilitate the effective use of recordings from lightweight flight recording systems, including questions about the integration of this equipment in an aircraft, human resource management, and legal issues such as the restriction on the use of cockpit voice and video recordings. Nevertheless, given the potential of this technology combined with FDM to significantly improve safety, the Board believes that no effort should be spared to overcome these obstacles.
Given the combined accident statistics for CARs Subparts 702, 703, and 704 operations, there is a compelling case for industry and the regulator to proactively identify hazards and manage the risks inherent in these operations. In order to manage risk effectively, they need to know why incidents happen and what the contributing safety deficiencies may be. Moreover, routine monitoring of normal operations can help these operators both improve the efficiency of their operations and identify safety deficiencies before they result in an accident. In the event that an accident does occur, recordings from lightweight flight recording systems will provide useful information to enhance the identification of safety deficiencies in the investigation.
Therefore the Board recommends that:
The Department of Transport work with industry to remove obstacles and develop recommended practices for the implementation of flight data monitoring and the installation of lightweight flight recording systems for commercial operators not required to carry these systems.
Transportation Safety Recommendation A13-01
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on . It was officially released on .
Correction
In the period 1 January 2002 to 5 July 2012, accidents involving aircraft operating under CARs subpart 704 (commuter operations), 702 (aerial work) and 703 (air taxi operations) together accounted for 94% of all commercial air accidents and 95% of commercial air fatalities. These were reported incorrectly as 91% and 93% respectively in the report when it was initially released, and have been corrected in this version.
5.0 Appendices
Appendix A – TSB Laboratory reports
The following TSB Laboratory reports were completed:
- LP043/2011 – GPS & Instruments Analysis
- LP 044/2011 – Analysis of Fibre Samples
- LP045/2011 – Trajectory Analysis
- LP047/2011 – Aircraft Structural Analysis
- LP051/2011 – Propeller Analysis
- LP050/2011 – Pitch Trim Actuator & Control Cable Analysis
- LP173/2011 – Indicated Airspeed Analysis
Appendix B – Mayo area VFR route map (1:500 000)
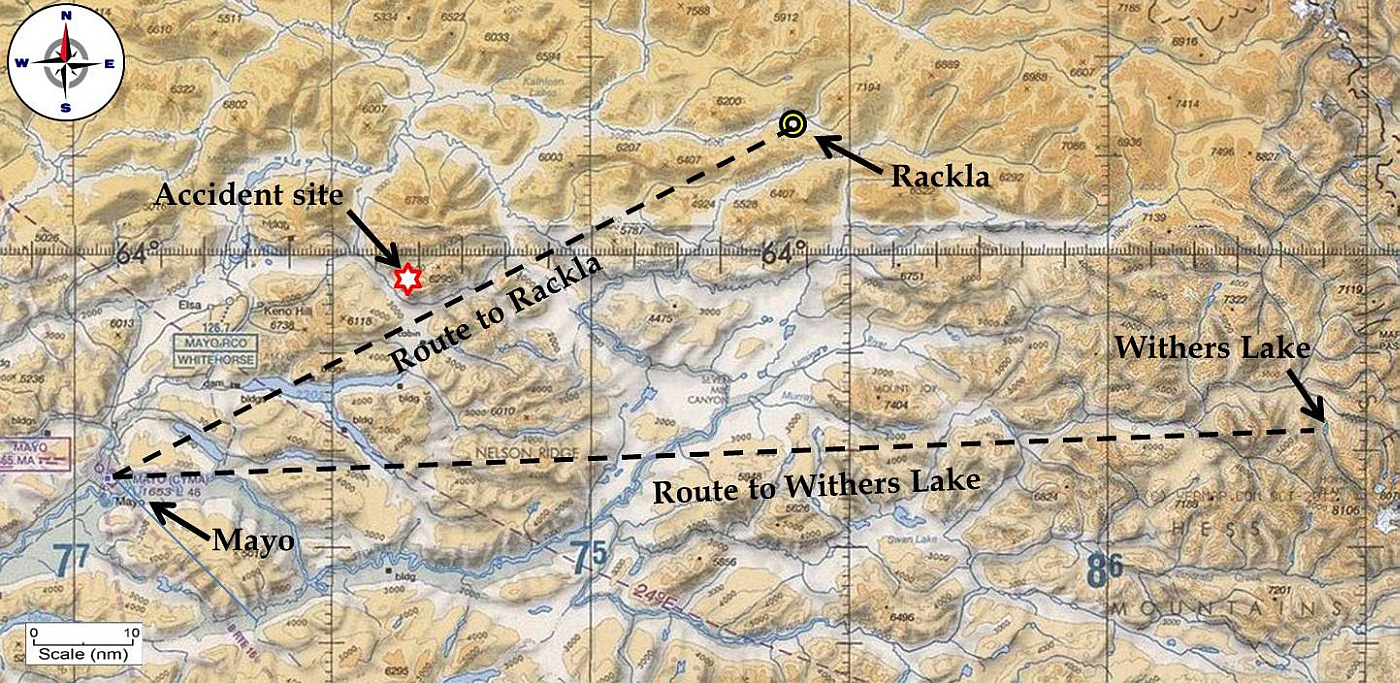
Appendix C – Mayo, Yukon, and area weather
METAR:
CYMA 312200Z 07005KT 20SM FEW045TCU SCT120 BKN220 6.1/-4.7 A2945 RMK TCU2AC1CI1 SLP997 SKY47=
CYMA 312300Z 00000KT 20SM FEW045TCU BKN220 6.7/-5.5 A2945 RMK TCU2CI2 SLP999
SKY58=
TAF:
CYMA 311738Z 3118/0106 VRB03KT P6SM FEW006 SCT080 TEMPO 3118/3121 BKN020
FM312100 VRB03KT P6SM SCT060 TEMPO 3121/0104 BKN060 BECMG 0104/0106 OVC030
RMK NXT FCST BY 010000Z=
FD (Kts to nearest 10°T):
Valid 00:00 Apr 01 2011 Issued 12:00 Mar 31 2011 for use 21-06Z
3000 6000 9000 12000 18000 24000 30000 34000 39000 45000
YMA 9900-06 2405-13 2410-20 2511-36 2317-47 990057 240955 232350 222746
Appendix D – Pilot-reported flight duty times, flight times and actual times
| Date | Reported time on duty1 | Reported time off duty | Reported flight duty time (hours) | Reported flight time (hours) | Number of flights | CARS departure time (time off) for first flight of day2 | CARS arrival time on last flight of day | Actual flight duty time3 (hours) | Actual flight time4 (hours) | Rest time |
|---|---|---|---|---|---|---|---|---|---|---|
| 21-Mar | 920 | 1600 | 6.7 | 2.8 | 4 | 1018 | 1619 | 7.7 | 2.8 (n/a, trips not to Rackla or Withers) | 1704 to 0815 |
| 22-Mar | 815 | 1810 | 9.9 | 6 | 10 | 917 | 1921 | 11.8 | 8 | 2006 to 0755 |
| 23-Mar | 755 | 2055 | 13 | 7.2 | 12 | 853 | 2042 | 13.5 | 9.6 | 2127 to 0620 |
| 24-Mar | 620 | 1955 | 13.6 | 9 | 12 | 725 | 1932 | 14 | 9.6 | 2017 to 0705 |
| 25-Mar | 705 | 1940 | 12.6 | 7.2 | 12 | 709 | 2049 | 14.5 | 9.6 | 2134 to 0610 |
| 26-Mar | 610 | 1920 | 13.2 | 7.2 | 12 | 708 | 1900 | 13.6 | 9.6 | 1945 to 0600 |
| 27-Mar | 600 | 1910 | 13.2 | 7.2 | 12 | 644 | 1921 | 14.1 | 9.6 | 2006 to 0605 |
| 28-Mar | 605 | 1930 | 13.4 | 7.2 | 12 | 653 | 1914 | 13.9 | 9.4 | 1959 to 0605 |
| 29-Mar | 605 | 1950 | 13.8 | 8.4 | 14 | 644 | 1953 | 14.5 | 10.2 | 2038 to 0600 |
| 30-Mar | 600 | 1845 | 12.8 | 7.2 | 14 | 653 | 2013 | 15 | 10.2 | 2058 to 0630 |
| 31-Mar | 630 | N/A | N/A | N/A | 7 | 834 | 15.07 (accident) | 8.6 | 4.9 | None |
| Total | 122.2 | 69.4 | 121 | 141.2 (132.6 prior to 31 Mar) | 93.5 | |||||
| Total last 7 days (Mar 24 to 30) | 92.6 | 53.4 | 99.6 | 68.2 |
Notes
- All times Pacific Daylight Time (GMT -7 hours)
- From community aerodrome radio station (CARS) daily records
- Time from pilot`s reported on-duty time for the day through to CARS arrival time for last flight of day plus 45 minutes
- Journey log flight time plus 0.1 hours for trips to Rackla airstrip, and 0.2 hours for trips to Withers Lake
Appendix E - Bendix/King KMD 150 GPS flight data
| Date (ddmmyy) | UTC time (hhmmss) | Latitude (ddmm.mm) | Longitude (ddmm.mm) | Speed through space (mph) | Calibrated airspeed (mph) Footnote 21 | GPS track (° true) | GPS altitude (feet) |
|---|---|---|---|---|---|---|---|
| 310311 | 214722 | N6337.00 | W13552.56 | 23 | 19 | 90 | 1695 |
| 310311 | 214752 | N6337.00 | W13551.25 | 120 | 113 | 90.3 | 1754 |
| 310311 | 214822 | N6337.32 | W13549.21 | 138 | 129 | 59.3 | 2144 |
| 310311 | 214853 | N6337.84 | W13547.31 | 128 | 117 | 59 | 2809 |
| 310311 | 214922 | N6338.29 | W13545.62 | 124 | 113 | 58.4 | 3391 |
| 310311 | 214953 | N6338.85 | W13543.87 | 135 | 122 | 53.3 | 3952 |
| 310311 | 215023 | N6339.47 | W13542.00 | 144 | 135 | 55.9 | 4343 |
| 310311 | 215053 | N6339.98 | W13540.05 | 142 | 132 | 60.7 | 4894 |
| 310311 | 215123 | N6340.48 | W13538.06 | 137 | 126 | 60.1 | 5470 |
| 310311 | 215153 | N6341.02 | W13536.08 | 146 | 134 | 60 | 5901 |
| 310311 | 215223 | N6341.55 | W13534.00 | 147 | 134 | 59.3 | 6366 |
| 310311 | 215253 | N6342.14 | W13531.97 | 147 | 133 | 57.9 | 6803 |
| 310311 | 215323 | N6342.68 | W13529.94 | 144 | 136 | 59.9 | 7303 |
| 310311 | 215353 | N6343.19 | W13527.93 | 140 | 131 | 59.7 | 7802 |
| 310311 | 215422 | N6343.69 | W13525.98 | 143 | 133 | 59.6 | 8166 |
| 310311 | 215453 | N6344.24 | W13523.91 | 143 | 131 | 56.2 | 8600 |
| 310311 | 215523 | N6344.80 | W13521.94 | 144 | 132 | 58.9 | 9007 |
| 310311 | 215553 | N6345.36 | W13519.87 | 153 | 139 | 60.1 | 9313 |
| 310311 | 215622 | N6345.88 | W13517.73 | 157 | 142 | 60.7 | 9606 |
| 310311 | 215653 | N6346.47 | W13515.40 | 160 | 144 | 58.6 | 9903 |
| 310311 | 215723 | N6347.10 | W13513.17 | 162 | 145 | 56.8 | 10156 |
| 310311 | 215753 | N6347.80 | W13510.96 | 167 | 148 | 53.1 | 10338 |
| 310311 | 215823 | N6348.52 | W13508.85 | 158 | 140 | 56.7 | 10693 |
| 310311 | 215853 | N6349.10 | W13506.67 | 157 | 139 | 62.4 | 11041 |
| 310311 | 215923 | N6349.63 | W13504.28 | 167 | 147 | 63.6 | 11188 |
| 310311 | 215953 | N6350.20 | W13501.84 | 163 | 144 | 62.1 | 11419 |
| 310311 | 220023 | N6350.77 | W13459.44 | 173 | 151 | 61.7 | 11489 |
| 310311 | 220053 | N6351.38 | W13456.84 | 182 | 159 | 62.2 | 11432 |
| 310311 | 220123 | N6351.99 | W13454.27 | 176 | 154 | 62.6 | 11390 |
| 310311 | 220153 | N6352.54 | W13451.69 | 174 | 153 | 65.6 | 11368 |
| 310311 | 220223 | N6353.07 | W13449.15 | 170 | 150 | 64.7 | 11337 |
| 310311 | 220252 | N6353.52 | W13446.66 | 167 | 147 | 71.1 | 11342 |
| 310311 | 220322 | N6353.95 | W13444.03 | 174 | 153 | 66.1 | 11177 |
| 310311 | 220353 | N6354.54 | W13441.36 | 175 | 154 | 58 | 10984 |
| 310311 | 220423 | N6355.52 | W13439.74 | 177 | 152 | 9.1 | 10652 |
| 310311 | 220453 | N6356.52 | W13441.55 | 241 | 203 | 286 | 8262 |
Appendix F – Markings on original DHC-3 vs. FAR 1505(c) compliant DHC-3T airspeed indicators


Appendix G – Three-view sketch of the occurrence aircraft
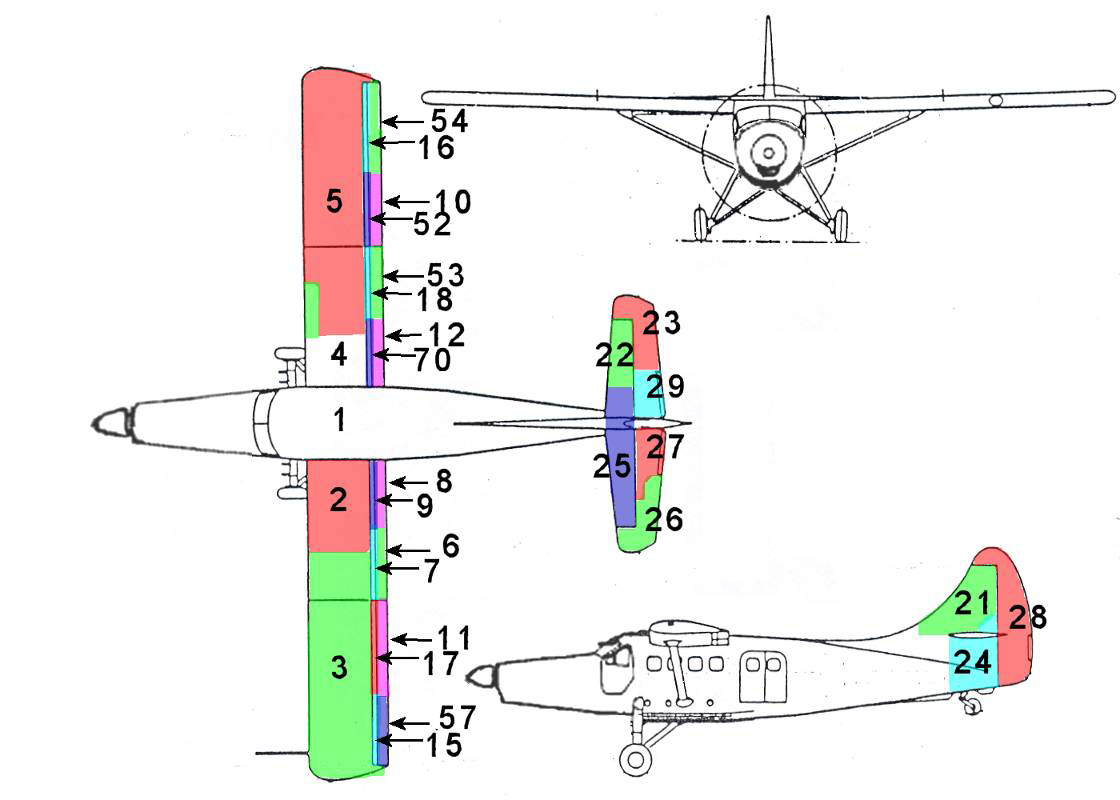
Appendix H – Wreckage distribution
Scale drawing of the contents of the debris trail produced from the on-site GPS survey of the debris trail (key to numbered items below)
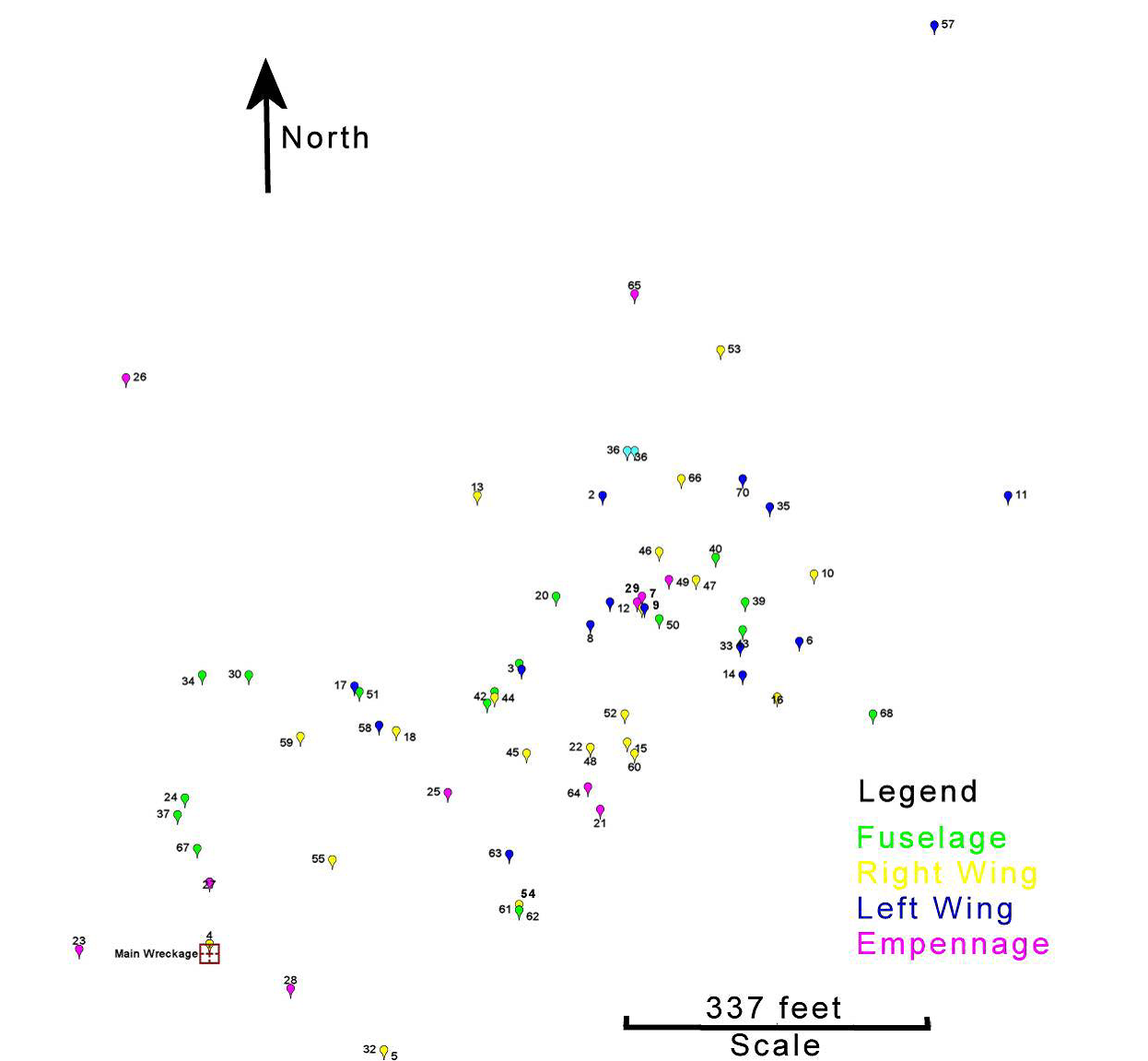
Key to numbered items in wreckage distribution diagram
- Main wreckage
- Left-hand wing inboard section
- Left-hand wing outboard section
- Right hand wing inboard section
- RH wing outboard section
- Left-hand trailing edge flap outboard section
- Left-hand wing inboard fore flap, outboard section
- Left-hand trailing edge flap inboard section
- Left-hand wing inboard fore flap, inboard section
- Right-hand aileron inboard section
- Left-hand wing aileron, inboard Section
- Right-hand wing inboard trailing edge Flap, inboard section
- Right-hand wing trailing edge inboard section
- Left-hand wing trailing edge C3w 1-11
- Left-hand wing outboard fore flap, outboard section
- Right-hand wing outboard flore flap, outboard section
- Left-hand wing outboard fore flap, inboard section
- Right-hand wing inboard fore flap, outboard section
- Aft fuselage piece left-hand side
- Aft fuselage piece left-hand side
- Tail fin with registation markings
- Right-hand horizontal stab, outboard section
- Right-hand elevator, outboard section
- Aft fuselage adjacent to rudder trim actuator
- Left-hand horizontal stab
- Left-hand elevator, outboard section
- Left-hand elevator, inboard section
- Rudder
- Right-hand elevator, inboard section
- Left-hand forward cargo door
- Left-hand aft cargo door
- Right-hand wing fence
- Left-hand wing fence
- Skin piece
- Wing skin
- Aircraft chart
- Left-hand fuselage skin
- Small piece of fuselage skin
- Right-hand aft fuselage “Zer Trim” decal
- Right-hand fus adj tail blue paint transfer
- Right-hand elevator (?) internal piece
- Right-hand wingtip fibreglass piece
- Small skin piece
- Rear fuselage skin piece
- Right-hand wing tip (large fibreglass piece)
- Right-hand wing tip small piece
- Right-hand wing tip small piece
- Right-hand wing tip small piece
- Right-hand elevator outboard skin piece
- Internal rear fuselage piece
- Small piece cabin window
- Right-hand wing outboard fore flap inboard section
- Right-hand wing inboard trailing edge flap outboard section
- Right-hand wing aileron outboard section
- Right-hand wing hinge from wing to joint of inboard/outboard fore flap section
- Left-hand aileron OB piece
- Left-hand wing strut centre station (clean)
- Right-hand wing strut centre section (sooty)
- Pitot tube
- Right-hand cargo door
- Fuselage skin piece
- Aileron hinge and counterweight
- Flap/elevator servo tab control rod, bellcrank and skin piece
- Right-hand elevator bottom skin piece
- Right-hand wing fairing piece (small)
- Fuselage skin piece (small) with red paint streaks
- Control cable quadrant with 2 broken cables attached
- Aircraft chart
- Right-hand wing inboard fore flap inboard section
- Propeller blade
Appendix I – Glossary
- AD
- airworthiness directive
- agl
- above ground level
- AME
- aircraft maintenance engineer
- asl
- above sea level
- CARs
- Canadian Aviation Regulations
- CARS
- community aerodrome radio stations
- CAS
- calibrated airspeed
- CMCC
- Canadian Mission Control Centre
- CVR
- cockpit voice recorder
- EAS
- equivalent airspeed
- ELT
- emergency locator transmitter
- EUROCAE
- European Organization for Civil Aviation Equipment
- FAA
- Federal Aviation Administration
- FAR
- Federal Aviation Regulations
- FAST
- Fatigue Avoidance Scheduling Tool
- FCU
- Fuel control unit
- FDR
- flight data recorder
- FOQA
- Flight Operational Quality Assurance
- GPS
- global positioning system
- IAS
- indicated airspeed
- ICAO
- International Civil Aviation Organization
- JRCC
- Joint Rescue Co-ordination Centre
- MHz
- megahertz
- Mmo
- maximum operating Mach
- MOPS
- Minimum Operational Performance Specification
- mph
- miles per hour
- nm
- nautical mile
- NTSB
- National Transportation Safety Board
- SB
- service bulletin
- sm
- statute mile
- STC
- Supplemental Type Certificate
- TC
- Transport Canada
- TSB
- Transportation Safety Board
- VC
- design cruise speed
- VD
- design diving speed
- VFR
- visual flight rules
- VMO
- maximum operating speed
- VNE
- never-exceed speed