Continued visual flight into instrument meteorological conditions - Collision with terrain
Rotorworks Inc.
Bell 206B (helicopter), C-FHTT
Drayton Valley Industrial Airport, Alberta, 1 nm S
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The Rotorworks Inc. Bell 206B (registration C-FHTT, serial number 1042) was on a visual flight rules flight from Whitecourt, Alberta, to Drayton Valley Industrial Airport, Alberta. The flight encountered and continued into instrument meteorological conditions. The aircraft collided with terrain approximately 1 nautical mile south of Drayton Valley Industrial Airport, at 1820 Mountain Daylight Time, during daylight hours. There was no post-crash fire. The pilot, who was the sole occupant, was fatally injured. No emergency locator transmitter signal was received by search and rescue authorities.
Ce rapport est également disponible en français.
Factual information
History of the flight
On 03 October 2011, the occurrence pilot attempted to fly from Drayton Valley Industrial Airport to Whitecourt Airport in order to receive instruction on vertical reference external load operations. While en route, the pilot encountered deteriorating weather (low ceilings and fog) and elected to return to Drayton Valley. A second flight was successfully completed the afternoon of 04 October 2011.
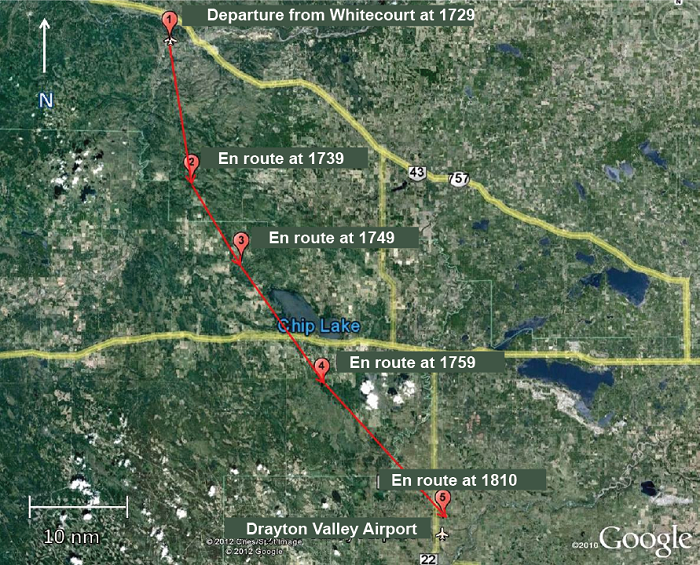
On 05 October 2011, the pilot departed Whitecourt Airport at approximately 1729Footnote 1 (Figure 1). The flight was a visual flight rules (VFR) flight returning to Drayton Valley Industrial Airport (via the McLeod River Valley, Highway 16 and Highway 22), where the pilot resided. The pilot departed Whitecourt Airport with approximately 50 US gallons of fuelFootnote 2 on board. The planned duration of the flight was 1 hour. Assuming a normal fuel consumption of 25 US gallons per hour, C-FHTT left Whitecourt with approximately 2 hours of fuel on board. The pilot checked the weather for Edmonton and Edson, Alberta, and discussed it with the chief pilot/owner prior to departure. They agreed on the routing to be used with the reported weather and that, should the weather deteriorate, an option was to return to Whitecourt, land, and the company would pick up the pilot by vehicle. When located 25 nautical miles (nm) south of Whitecourt Airport, the pilot made a cellular telephone call to a friend in Drayton Valley, indicating that the flight was encountering bad weather and inquiring as to the conditions at Drayton Valley. The pilot reported being at 7000 feet above sea level (asl) on top of the clouds and that there were no holes through which to descend. While the flight departed with a handheld global positioning system (GPS) unit on board, none could be found in the wreckage.
At 1803, the pilot made another telephone call reporting that the aircraft was located 15 miles north of Drayton Valley. The SPOT™ Satellite MessengerFootnote 3 flight tracker data that was retrieved showed its actual position as northwest of the airport.
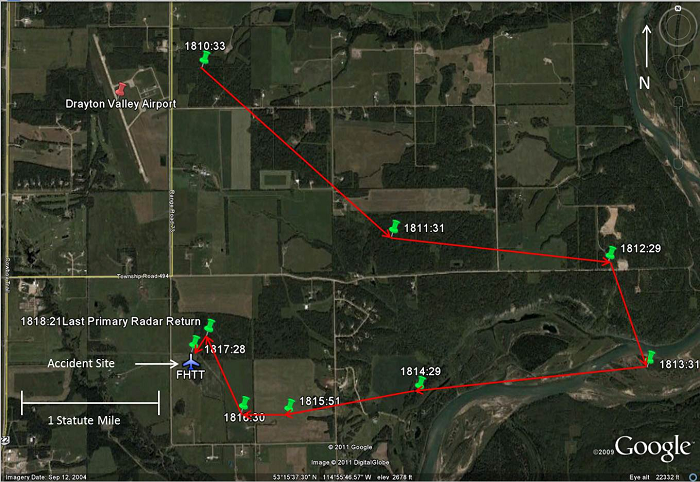
A final call was made at 1807 where the pilot reported slowing down to 20 mph and starting descent. Tracking data showed that the helicopter was located approximately 1 nm north of the airport. The pilot expressed some concern about icing due to the temperature.
The aircraft's track was not displayed on secondary radar; however, a primary target was observed in the area at about the time of the accident. Primary radar does not provide altitude or airspeed information.
The aircraft wreckage was found in a field approximately 1.3 nm south of the airport.
Wreckage information
The accident site was at the edge of a rough ploughed hay field. The fuel cell had ruptured; there was a strong odour of fuel (Jet A1) at the site. There was no post-impact fire. The elevation of the area is very close to that of the Drayton Valley Industrial airport, which is 2776 feet asl.
The aircraft's initial impact marks indicated that it was in a level, but slightly left-side-low, attitude. The parallel impact marks from the landing skids suggested that the helicopter was not rotating about its vertical axis at the time of impact, which in turn indicated that the helicopter's anti-torque rotor was functioning. The wreckage was about 10 feet south of the initial impact. The above description of impact marks indicates directional control. The forward cabin was found on its right side and oriented to 251° magnetic (M). The engine, main transmission, rotor mast, and tail boom were detached, in line with the cabin, lying on their left side. During the impact sequence, an 11-foot-9-inch section of the main rotor blade became detached and was found approximately 520 feet south of the wreckage. The tail rotor blade assembly was detached from the drive shaft and embedded into the ground. There was no indication of rotational damage to the tail rotor blades. There were main rotor blade strike marks immediately to the right of the initial impact location.
The main engine drive shaft was destroyed, with numerous indications of high power having been produced. The main rotor could be rotated slightly by hand, and the engine (Rolls Royce 250-C20) could be rotated in both the N1 and N2 sections.Footnote 4 There were no indications of engine discrepancies prior to impact.
The shoulder harnesses were not attached to the lap belt buckle. The investigation determined that it was the pilot's habit not to wear the shoulder harness. The pilot was not wearing a helmet.
The emergency locator transmitter (ELT) (KANNAD 406 AF-Compact) was located on the left side of the centre console, in the chin-bubble area. When examined by TSB investigators on 06 October 2011, the switch on the ELT was found in the OFF position, and the remote switch located on the instrument panel was found in the armed position. No explanation could be found for this. There was no company-specific procedure (e.g., checklist item) that required the pilot to ensure that the ELT was armed prior to flight. However, it is standard airmanship practice for the pilot to ensure that the ELT is armed prior to flight.Footnote 5
The TSB Laboratory examined the N1 turbine, the N2 turbine, the main rotor tachometers, and the engine torque indicator. Examination of these instruments did not provide any reliable information as to their indications at the time of impact.
In addition, the Laboratory examined the annunciator panel. The condition of the filaments in the annunciators was consistent with lamps that were off (not powered) at impact. This suggests that the helicopter was operating normally at the time of impact.
Aircraft
The Bell 206B helicopter is a single-turbine engine helicopter certified for day or night VFR flight. C-FHTT was equipped with instrumentation that met the requirements for day VFR flight.Footnote 6 Records indicate that the helicopter was certified, equipped, and maintained in accordance with existing regulations and approved procedures. The helicopter had no known deficiencies before the occurrence flight. The weight and centre of gravity were determined to be within the prescribed limits.
Pilot
Records indicate that the pilot was certified and qualified for VFR flight in accordance with existing regulations. The pilot held a commercial pilot licence – helicopter and was endorsed on 3 helicopter types for daylight flying only. As of 05 October 2011, the pilot had accumulated approximately 390 hours of flight time, with 70 hours on the accident aircraft type, of which 43 hours were dual flight time and 27 hours were solo flight time. The flight time accumulated during the previous 90 days was 66.7 hours, within the last 30 days, 17 hours, and within the last 7 days (excluding the accident flight), 2.1 hours. The pilot did not hold an instrument rating. The pilot was an employee of Rotorworks Inc.
The pilot attended a pilot decision-making course and completed the related company exam. The training focused on obtaining approval for flight in reduced visibility. As the regulatory standardsFootnote 7 and the company require pilots to possess 500 hours of flying time before they can operate in reduced visibility, the occurrence pilot, with 390 hours total flying time, would not have been eligible to operate in these conditions.
Rotorworks Inc.
Rotorworks Inc. is a Whitecourt-based helicopter operator that possesses multiple air operator certificates issued by Transport Canada (TC) under the following subparts of the Canadian Aviation Regulations (CARs): 406 – Flight Training Units; 702 – Aerial Work Operations; and 703 – Air Taxi Operations. Its fleet consists of Robinson R22 and R44 piston-powered helicopters and Bell 206 turbine helicopters. Certificates issued under Part VII of the CARs allow for day VFR operations only in any and all of Rotorworks Inc. aircraft.
Rotorworks Inc. uses a pilot self-dispatch system, where the pilot-in-command of any flight is authorized to "make decisions as to initiation, continuation, delay, diversion or rerouting of the flight when conditions are such that operational decisions are necessary."Footnote 8
The occurrence flight was dispatched under the authority of section 2.11(e) of the company operations manual, which states in part:
In uncontrolled airspace below 1000 feet agl the pilot shall have a flight visibility of not less than 1 mile (unless otherwise authorized in the Air Operator Certificate) and clear of cloud. The airspeed must be reduced to an airspeed that will allow the PIC to be able to see other air traffic or obstructions in time to avoid a collision.Footnote 9
Meteorological conditions
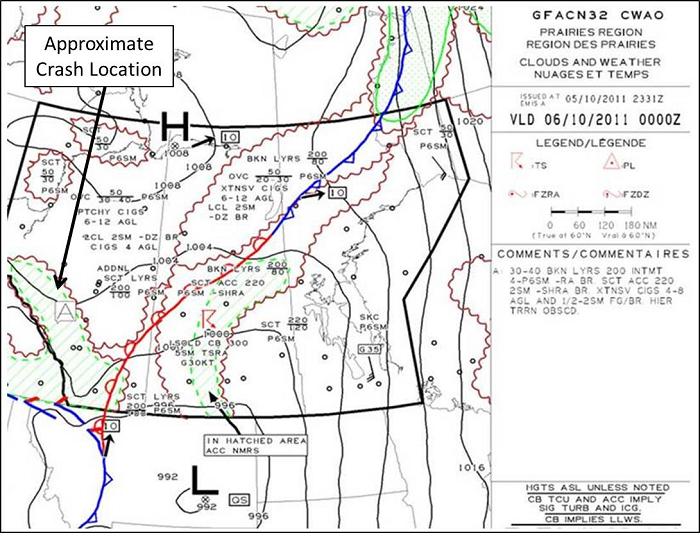
Reported weather conditions upon departure from Whitecourt indicated that ceilings were 600 to 900 feet above ground level (agl) and visibility was 3 statute miles (sm). According to the graphic area forecast (Figure 3), the western part of Alberta, along the Rocky Mountains and along the route to Drayton Valley were forecast to experience broken ceiling from 3000 to 4000 feet asl with layers to 20 000 feet asl. In this area, intermittent visibilities of 4 to 6 sm in light rain and mist were forecast, with scattered altocumulus castellanus clouds to 22 000 feet asl. Also forecast were extensive ceilings of 400 to 800 feet agl and visibilities of ½ - 2 sm in fog and mist. Higher terrain would have been obscured. Patchy moderate mixed icing conditions were forecast between the freezing level (7500 to 10 000 feet asl) and 18 000 feet asl.
Canadian Aviation Regulations
The flight was operating in uncontrolled airspace, that is to say, airspace within which no air traffic control (ATC) services are provided. Section 602.115 of the CARs requires that, for a helicopter flying VFR, flight visibility be at least 1 sm when flying under 1000 feet agl and that the helicopter be operated with visual reference to the ground.
VFR over-the-top is not permitted in commercial operations in Canada.
Pilot decision-making
Pilot decision-making (PDM) is a systematic approach to managing the pilot, the aircraft, the environment and external factors in order to mitigate risk. In the context of an intended flight, the pilot assesses all the elements that are present and develops an effective plan to achieve the desired outcome: a safe flight. For the decision-making process to be successful, however, the pilot must continually re-assess the conditions and determine whether the original plan is still sound, or if a different course of action is required. Accurate and timely interpretation of the information available to the pilot is essential to the success of this process. Failure to understand a changing environment and to act accordingly may have serious consequences. Over-estimating one's skill and knowledge, pushing an aircraft beyond its operating limits, and not understanding the environment and the limits it imposes on the flight are all detrimental to a successful flight. Additionally, external factors can play an adverse role in the decision-making matrix. Pressure placed by company officials and clients/passengers to complete a flight can influence the decision-making process. Likewise, self-imposed pressure to return home can lead a pilot into a situation that is beyond their ability to cope. While the aviation community has made inroads in the field of PDM, continued efforts are required to ensure that effective decision-making skills are taught and used to ensure improvement in flight safety.Footnote 10
Spatial awareness / disorientation
On the ground, spatial orientationFootnote 11 is sensed by a combination of vision, muscle sense, and specialized organs in the inner ear, which sense linear and angular accelerations. Vision is the strongest of the orienting senses, and, in visual flight, the pilot relies on regular visual references with the ground and horizon to control the aircraft attitude and altitude. If a pilot is in cloud, visual references to the ground and horizon are lost. As a result, the available cues (solely from the external forces on the body) often produce spatial disorientation in flight, because the pilot has a false impression of aircraft attitude and motion. Under these conditions, the pilot is completely dependent on flight instruments and learned flying skills for control of the aircraft. Pilots who are not experienced in flying the aircraft solely with reference to instruments are particularly susceptible to spatial disorientation when they are in a situation where no external visual attitude references are available.
A search of the TSB database for the period of January 1992 through May 2011 revealed 24 occurrences involving VFR helicopter flight that resulted in collision with terrain in instrument meteorological conditions. These occurrences resulted in 32 fatalities.
Previous Board recommendations
An investigation into an accident that occurred in 2000 established that the pilot had not received any formal decision-making training, among other types of training, to help formulate decisions. The Board concluded that, without a systemic approach to improving PDM, accidents resulting from ineffective decisions in complex situations would continue to affect commercial operations. At the time, the Board believed and still believes that improved formal PDM training was and is a necessity for all commercial pilots. The Board also believes that an increased emphasis on appropriate decision-making throughout pilot training and during all the pilot's flying-related activities will serve to reduce the occurrence of PDM-related accidents. Therefore, the Board recommended that:
The Department of Transport improve the quality of pilot decision making in commercial air operations through appropriate training standards for crew members.
Transportation Safety Recommendation A00-06
In March 2012, in its annual re-assessment of outstanding recommendations, the TSB reviewed TC's latest response. TC indicated that Notices of Proposed Amendments (NPAs) on PDM had been elevated on its list of regulatory priorities.
In response to TSB recommendations on PDM and crew resource management (CRM), a focus-group recommendation that the ICAO-endorsed Threat and Error Management Model be incorporated into this training was accepted by the Canadian Aviation Regulation Advisory Council (CARC). TC's intent is to address PDM as a component of the review and analysis of the recent CRM Focus Group, cross-referencing existing TSB recommendations as appropriate. TC anticipates the development of new standards for Part VII - Commercial Air Services for both CRM and PDM.
Until all regulatory changes proposed by TC are enacted, the deficiency identified in Recommendation A00-06 will continue to exist. The proposed regulatory changes, if fully implemented, will substantially reduce or eliminate the risks associated with the safety deficiency identified in Recommendation A00-06. Therefore, the Board assessed TC's response to the recommendation as having Satisfactory Intent.
The following TSB Laboratory report was completed:
- LP145/2011 - Instrument and Annunciator Examination.
Analysis
There was no indication that an aircraft system malfunction contributed to this occurrence. This analysis will focus on the decision-making, operational, and environmental factors that contributed to the occurrence.
Two days prior to the occurrence flight, the pilot had decided to terminate a trip and return to base due to deteriorating weather. Regulations, company operational procedures and prior training likely had some influence in that decision-making process. In the case of the occurrence flight, it could not be determined why the pilot chose to deviate from the planned routing.
Once on top, the only recourse was to descend through the cloud to regain visual reference. The pilot did not contact the Edmonton Area Control Centre and request assistance such as vectors to a larger airport. However, had the pilot done so, a descent through cloud would still have been necessary. In addition, there is no indication that the pilot attempted to turn back towards Whitecourt, where the weather was better.
Although the pilot had indicated concern about possible icing, the investigation discounted this possibility, as there likely would have been a loss of control due to the tail rotor icing, which would have resulted in a different impact signature.
During the descent through cloud, the pilot was able to control the rotorcraft, but lost awareness of the aircraft's height above ground, and did not arrest the rate of descent prior to impact with terrain. Disorientation or loss of situational awareness could have played a part to some degree.
The pilot was in the habit of not wearing the available shoulder harnesses. These harnesses serve to maintain occupants in an upright position in order to take full advantage of all the crashworthiness features of the aircraft. To what extent this may have contributed to the injuries sustained could not be determined. The fact that the pilot was not wearing a helmet likely would not have been a factor in survivability due to the severity of impact forces.
Findings
Findings as to causes and contributing factors
- The pilot continued the visual flight rules flight into weather conditions that required descent through cloud to reach destination.
- The pilot did not arrest the rate of descent, resulting in a collision with terrain in which the impact forces were not survivable.
Finding as to risk
- Not wearing the available shoulder harnesses or a helmet increases the risk of severe injury or death.
Other finding
- The emergency locator transmitter switch was found in the off position.
Safety action taken
Rotorworks Inc. pilots have all received human factors training and pilot decision-making training since the accident.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on . It was officially released on .