Collision with terrain
Piper PA-30 Twin Comanche C-GLGJ
Kelowna, British Columbia, 18 nm W
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The privately operated Piper PA-30 Twin Comanche (serial number 30-300, registration C-GLGJ) departed Penticton Airport, British Columbia, at 1432 Pacific Daylight Time on a visual flight rules flight plan during daylight hours, to Boundary Bay; 1 pilot and 3 passengers were on board. The aircraft flew northbound over Okanagan Lake for approximately 20 nautical miles, before turning west into a valley; this was about 14 nautical miles further than planned, due to a lower-than-expected rate of climb. At 1454, an overflying airliner received an emergency locator transmitter signal, which the airliner pilot relayed to the area control centre, and the area control centre relayed to the Joint Rescue Coordination Centre. The aircraft wreckage was located about 2½ hours later, in a wooded area near the Brenda Mines site, approximately 18 nautical miles west of Kelowna. There was no fire. All 4 occupants were critically injured; 1 occupant died at the site, and a second died in hospital 2 days later.
Factual information
History of the flight
The first of the 2 flight legs originated at Boundary Bay (CZBB), British Columbia, where the pilot had C-GLGJ's main, auxiliary, and tip tanks filled. Full fuel is 120 U.S. gallons, or 708 pounds, giving the aircraft a flight duration of about 6 hours. The aircraft departed Boundary Bay at 1230Footnote 1 for Penticton Airport (CYYF), British Columbia, on a visual flight rules (VFR) flight plan, with the pilot and 1 passenger on board. It arrived in Penticton, about 140 nautical miles (nm) east of Boundary Bay, at 1343, after an air time of 1.2 hours.
The aircraft was on the ground at Penticton for 49 minutes, during which time the pilot phoned the Kamloops flight information centre (FIC) to file a VFR flight plan for the return flight. The flight plan stated the intended route as Penticton to Boundary Bay via Princeton and Hope. With the headwind component considered, the return flight would have taken approximately 1.4 hours. The FIC. The FIC agent advised of a recent pilot report that described visibility in the Princeton area as 2 nm in haze, and asked the occurrence pilot if visibility on the flight to Penticton had been hazy in that area. The pilot confirmed it had been.
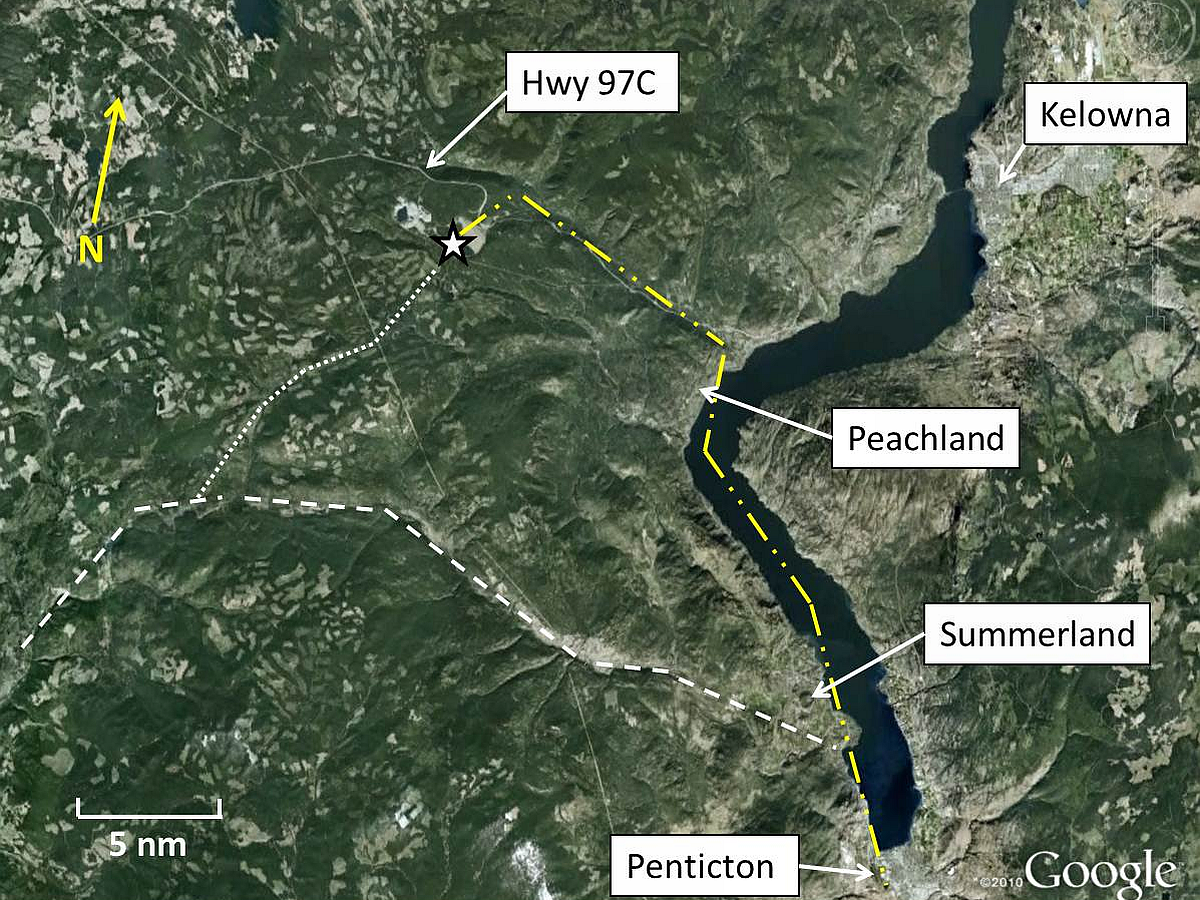
Two more persons boarded the aircraft with their baggage. Immediately before departure, the pilot advised the Penticton Flight Service Station (FSS) of the intention to depart on Runway 34 and climb to 5000 feet above sea level (asl), before turning westbound for Boundary Bay. After take-off from Penticton Airport, the pilot observed that the aircraft's climb rate was significantly lower than it had been 2 days earlier, when it had departed Penticton with only 2 persons on board. Consequently, the pilot did not turn west onto the published VFR route approximately 6 nm north of Penticton (the route taken on the previous flight from Penticton to Boundary Bay), but instead flew approximately 20 nm north, before turning west near Peachland (Figure 1).
It is not known what altitude C-GLGJ reached before it turned west toward rising mountainous terrain, but the aircraft did not appear on radar. Radar had identified other aircraft in that area as low as 4000 feet asl. After turning west, the aircraft proceeded up the Trepanier Creek valley following Highway 97C (also known as the Okanagan Connector) for about 10 nm, before it crashed at 4595 feet asl into a level, treed area on the Brenda Mines tailings dam.
A driver on Highway 97C reported seeing the accident aircraft about 2 nm down-valley from the accident site, climbing slowly toward the tailings dam at roughly the same altitude as the accident site. The driver also reported poor visibility in the area due to smoke.
An airliner flying overhead of the accident site received a 121.5 megahertz (MHz) emergency locator transmitter (ELT) signal, which it reported to the Vancouver Area Control Centre (ACC). The ACC notified Victoria Joint Rescue Coordination Centre, which dispatched search-and-rescue personnel, who air-dropped to the site at 1731. One occupant was found deceased at the accident site. The 3 critically injured occupants were transported by helicopter to hospital, where a second occupant later died.
Accident site
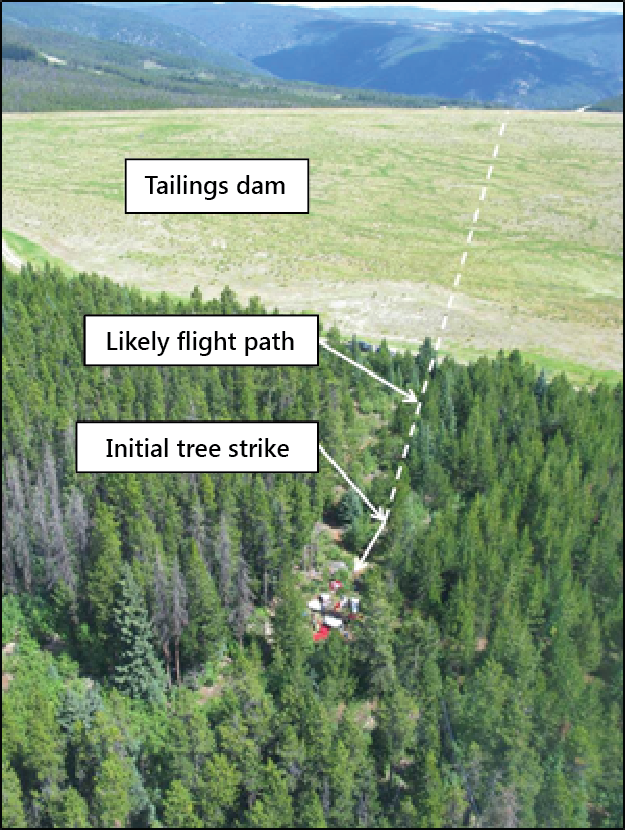
The aircraft crashed on a level, treed portion of the Brenda Mines tailings dam, about 0.7 nm southwest of Highway 97C (Photo 1), at an elevation of 4595 feet asl. Though not a published VFR route, Highway 97C follows the Trepanier Creek Valley and is often used by pilots as a route when flying west from the Okanagan Valley. The Brenda Mines site is about 10 nm north of the published VFR route from Summerland to Princeton, and the valley southwest from the Brenda Mines to the published VFR route is the logical low-ground route between the two (Figure 1).
The terrain before the treed area at the accident site is a level, grass-covered area atop the Brenda Mines tailings dam (Photo 1). Based on the aircraft's path as it struck the trees, its likely flight path took it over about 1600 feet of unobstructed grass and about 200 additional feet of forest, before it contacted the first tree. Trees immediately past the accident site, as well as those to the right of it, were about twice as tall (about 70 feet) as the trees that were overflown (about 35 feet) and struck. A parallel flight path at the same altitude, but about 1000 feet to the left, would have been over ground low enough to clear the trees at this altitude and to then have continued to Princeton.
After striking the first of 5 small trees, the aircraft travelled about 75 feet, before coming to rest. Leading-edge damage indicated that the aircraft struck the trees while banked about 45°, right-wing low. Impact with the trees and ground separated the outboard 6 feet of both wings and broke the fuselage into 3 pieces, but the aircraft remained upright. The flaps and landing gear were found fully retracted. Both propellers sustained light scoring and leading edge damage, as well as heavy bending damage.
Of the 6 thermos-style fuel caps,Footnote 2 5 remained in their respective filler necks. (The right tip-tank fuel cap was not located.) Both tip tanks and the right wing's main and auxiliary fuel tanks were compromised, spilling about 40 imperial gallons of AVGAS at the site. The battery box, located in the aft fuselage, broke free from its mounted position. As a result, the positive cable from the battery detached from the master solenoid, isolating the battery from the aircraft. There was no fire.
Over 140 pounds of baggage (including packs, handbags, air mattress, laptop, food, etc.) and aircraft-related gear (including logbooks, headsets, wheel chocks, tow bar, aircraft cover, baggage tie-down straps, cleaning supplies, survival kit, first-aid kits, spare oil, bottled water, etc.) was recovered from the wreckage.
All 4 occupants were wearing their available lap belts. The aircraft, manufactured in 1964, was not equipped with shoulder belts,Footnote 3 nor was it required to be. All 4 occupants suffered severe head injuries—in 2 cases, fatally. The survivors do not recall the last few minutes of the flight before the crash.
The ELT activated automatically during the impact, and transmitted until manually turned off by rescue personnel.
Weather
The weather reported at the Penticton Airport (elevation 1130 feet asl) at 1400—half an hour before C-GLGJ departed—was wind 360° true (T) at 9 knots, visibility 15 statute miles (sm), clouds few at 18 000 feet above ground level (agl), broken at 25 000 feet agl, temperature 32°C, dew point 10°C, and altimeter setting 29.89 inches of mercury (in. Hg), equating to a density altitude of about 3300 feet asl. The only significant changes to the weather reported 1 hour later (at 1500, about 6 minutes after the aircraft's ELT was reported) were a temperature increase to 34°C, a dew point decrease to 7°C, and a barometric pressure decrease to 29.88 in Hg, equating to a density altitude of about 3500 feet asl.
The weather reported at 1500 at Kelowna Airport (CYLW, elevation 1421 feet asl), 31 nm north of Penticton, included visibility of 9 sm in haze, and a density altitude of 3700 feet. The visibility there had been reported as 2¼ sm in haze at 1302, and as 6 sm in haze at 1400.
Degraded visibility due to forest-fire smoke was reported at 1400 at several airports to the west of Penticton and Kelowna, including Princeton (visibility 3 sm), Merritt (visibility 9 sm), and Hope (visibility 9 sm). Drivers on Highway 97C near Brenda Mines reported poor visibility due to smoke both immediately before and after the accident.
At 1400, a British Columbia Forest Service weather station, 1.5 nm west of and 200 feet higher than the accident site, recorded a temperature of 25.5°C, relative humidity of 12%, and wind 4 knots at 286°T. Calculations show that density altitude at the accident site was over 7000 feet asl.
Pilot
The pilot held a valid Canadian commercial pilot licence (aeroplane) and current medical certificate, and was qualified for the type of flight being conducted. The pilot had accumulated about 338 hours of total flight time, which included about 106 hours of multi-engine time, about 65 hours of which were in the accident aircraft. The pilot was also instrument flight rules (IFR)–rated and endorsed to fly floatplanes. The pilot's total flight time with an instructor in C-GLGJ was 6.9 hours, the most recent of which was 1.5 hours acquired about 5 months before the accident.
It was the pilot's practice to operate the engines of the accident aircraft without using the turbochargers to maintain manifold pressure, and to fly with full fuel tanks.
The pilot had flown C-GLGJ from Boundary Bay to Penticton and back on at least 2 occasions before the accident flight, the most recent of which was 11 August 2012 (2 days before the accident flight). On that occasion, the pilot flew 3 friends to Penticton, dropped off 2 of them, and returned to Boundary Bay with the remaining passenger. Immediately before C-GLGJ departed Penticton on that flight, the CYYF FSS specialist advised the pilot to climb to 5000 feet asl before turning west toward rising terrain. This instruction cannot be found in any of the usual VFR flight-planning sources, such as the VFR Navigation Chart or the Canada Flight Supplement. The only source of this information, besides the informal advisory from the Penticton FSS specialist, was a sign at the Penticton Airport posted on the airside wall beside the door to the pilot information kiosk. This door might not necessarily be used by a pilot to go groundside, and no sign was posted at the pilot information kiosk.
Aircraft
The aircraft was manufactured in the United States by the Piper Aircraft Corporation. It was originally equipped with normally aspirated engines, but had Supplemental-Type-Certificate−approved, turbo-normalizedFootnote 4 Lycoming IO-320-B1A engines and tip tanks installed in 1968. In March 1980, the aircraft was imported to Canada, where it changed ownership 4 times before July 2009.
The aircraft was equipped with a Garmin GNS 430 and a Century 2000 automatic flight system. It was not determined what navigation aids were being used at the time of the accident. However, the heading bug and the course deviation indicator needle on the horizontal situation indicator were both set to a heading that would have taken the aircraft from the Brenda Mines area directly to Hope. It was the pilot's practice to not engage the GNS-coupled autopilot until reaching the cruise portion of flight.
The aircraft was not equipped with shoulder harnesses at manufacture. However, on 18 January 1995, the Piper Aircraft Corporation issued Service Bulletin (SB) no. 980, recommending installation of shoulder-harness kits for several models of Piper aircraft, including the PA-30. Because of a typographic error regarding eligibility of aircraft by serial number, SB no. 980 indicates that a shoulder-harness installation kit is available only for front seat positions for the accident aircraft, when in fact kits are available for front and rear seat positions. Although Piper considers SB no. 980 to be mandatory, SBs are mandatory in Canada only if they are associated with an airworthiness directive (AD), which this SB is not.
Transport Canada indicates that there are 17 ADsFootnote 5 applicable to C-GLGJ that pertain to fuel system problems. (Four of those ADs have been superseded and no longer apply.) At least 2 of the applicable ADs (79-12-08 and 83-10-01) pertain to water contamination in the fuel system. Accident reports from various aircraft-accident investigation authoritiesFootnote 6 suggest that the PA-30 is prone to water contamination of the fuel system. One point of water ingress is reported to be poorly fitting fuel-tank caps.Footnote 7 Significant corrosion was found on the steel portions of the right auxiliary-tank fuel cap. Although the aircraft was normally kept in a hangar, it had been kept outside for several months during wet winter weather in 2011 and in 2012, while waiting for parts and maintenance.
According to the pilot's operating handbook (POH), at maximum gross weight (3725 pounds) and 3300 feet (the density altitude at Penticton at take-off on the accident flight), the PA-30 Twin Comanche turbocharged model will—using maximum continuous power—have a maximum rate of climb (ROC) of about 1250 feet per minute. The POH for the normally aspirated (non-turbocharged) PA-30 indicates that maximum gross weight (3600 pounds) and 3300 feet will also result in a maximum ROC of about 1250 feet per minute. The POHs do not specify what the ROC will be when using reduced power, as recommended once above 1000 feet agl for either model aircraft, but it is reasonable to assume that the rate will be lower than when using maximum continuous power. The POH only gives performance chart information for calculations up to maximum gross weight, as the aircraft is not to be operated beyond this weight.
C-GLGJ's actual ROC after departing Penticton on the accident flight is not known. However, the ROC on the previous leg (Boundary Bay to Penticton), about 2 hours before the accident, was determined from radar data to be about 360 feet per minute. The pilot's practice was to climb using 25 inches of manifold pressure and 2500 revolutions per minute (rpm). During the climb portion of that flight, the aircraft was flying at its best ROC speed and was about 400 pounds lighter than on the accident flight, and the density altitude was about 2700 feet lower than on the accident flight.
Effects of density altitude on aircraft performance
Air density decreases with increased altitude and temperature.Footnote 8 Therefore, the combination of high temperature and high elevation can drastically reduce the aerodynamic and engine performance of the airplane in the following ways:
- The horsepower output of the engine is decreased, because its fuel-air mixture is reduced.
- The propeller develops less thrust, because the blades, as airfoils, are less efficient in the thin air.
- The wings develop less lift, because the thin air exerts less force on the airfoils.
Pressure altitude is the reading on the altimeter when it is set to standard barometric pressure (29.92 in Hg). Density altitude is pressure altitude corrected for temperature when the actual outside temperature is different from the International Civil Aviation Organization (ICAO) standard atmosphere.Footnote 9
Internal combustion engines combine air with fuel to produce power. If less air is available, less fuel can be used, and less power will be produced. Aircraft engine power and flight performance data are based on a standard atmosphere. Any deviation from this will result in a change to the power available from the engines, and a resulting change in the performance of the aircraft.
To overcome the loss of power at higher density altitudes, many engines have a boost system that compresses the air as it enters the engine, so that more air is available for combustion. This system allows an engine to produce its maximum amount of power at higher density altitudes. The boost system on the accident aircraft type is driven by a turbine in the exhaust system that drives a turbo compressor in the engine's intake manifold. At any time that the pilot notices a reduction in manifold pressure as a result of density altitude, a valve can be opened to allow more exhaust gas to the turbo charger, and thus to increase the available power. This is done by turning a control knob that allows for fine adjustment of the turbo.
Maintenance and logbooks
The last 4 flights conducted in C-GLGJ before the accident flight were not recordedFootnote 10 in any logbooks. As well, although log entries show that a typical amount of maintenance (scheduled and unscheduled) had been performed on the aircraft since its importation to Canada, only 5 snags (defects) were recorded during the 32 years between its importation and the accident.Footnote 11 None of the 5 recorded snags pertained to the fuel system or the engines, but several maintenance entries (some during regularly scheduled inspections, some not) show that repairs were done to both the fuel system and engines.
A search of the Transportation Safety Board (TSB) database shows that, on 05 June 2005, a pilot flying C-GLGJ from Victoria to Abbotsford reported to air traffic control that one engine was surging and running rough for some period of time before clearing up on its own.Footnote 12 No record of the event was made in the aircraft's logbooks. However, a logbook entry on 30 October 2005 (just over 8 flight hours later) shows that both the left and right fuel servos and flow dividers were removed and sent for testing and repair.
Notes found in the aircraft wreckage, written following a flight on 11 September 2011 from Qualicum Beach to Boundary Bay, indicate that the right engine had excessive fuel flow and vibration, and that excessive left rudder was required on take-off. The notes also indicate that the right engine's exhaust gas temperature (EGT) dropped to about 700°F, while the left engine's EGT remained about 1400°F.Footnote 13 These defects are not recorded in the logbooks. However, the most recent annual inspection (performed 29 February 2012, about 0.3 flight hours after the 11 September 2011 flight, 18 flight hours before the accident) included replacing the right main fuel-tank bladder, cleaning corrosion from the right engine's fuel servo inlet screen, and cleaning the right engine's number 3 cylinder fuel-injector nozzle.
Photo 2, taken during a flight on 23 March 2012 (12 flight hours before the accident), shows the right engine's fuel-flow indication 45% higher than the left engine's fuel flow for the same throttle setting and manifold pressure. No defect was noted in the logbooks. The systems description section of the POH states that, “It is important to note that an indication of increasing or abnormally high fuel flow is a probable symptom of restricted injector lines or nozzles.”
The fuel-flow gauge, marked in gallons per hour, does not directly measure fuel flow, but rather measures metered fuel pressure to the fuel nozzles. If one nozzle becomes partially or completely obstructed, fuel pressure to the remaining nozzles will increase (showing an increased fuel flow on the gauge), but the total fuel flow to the engine will not. The cylinder with the obstructed nozzle will receive a leaner mixture, while the other cylinders will receive a richer mixture. Engine vibration will increase, and although EGT will vary depending on the fuel/air mixture to each cylinder, any cylinder with a significant fuel nozzle obstruction will have a markedly decreased EGT. Engine power will be reduced. However, on engines equipped with constant speed propellers (such as the accident aircraft), rpm and manifold pressure may indicate near normal.

A 13 July 2012 logbook entry (about 5 flight hours before the accident, following another flight from Qualicum Beach to Boundary Bay) shows the right engine received unscheduled maintenance which included servicing the spark plugs, testing the spark plug leads, and ground-running both engines to check mag drop. There are no defects entered in the logbook to suggest why the maintenance was performed, and the entry made by the maintenance organization notes that no defects were found.
Weight and balance
The pilot did not calculate a weight and balance (W&B) for the accident flight or the previous leg. The journey logbook did not contain the empty W&B information requiredFootnote 14 for a pilot to calculate a loaded W&B. No other W&B information was found in the aircraft.
The W&B section of the POH carried on the aircraft states, in part:
In order to achieve the performance and flying characteristics which are designed into the aircraft, it must be flown with the weight and center of gravity position within the approved operating envelope. Although the airplane offers flexibility of loading, it cannot be flown with the maximum number of adult passengers, full fuel tanks and maximum baggage. With this flexibility comes responsibility. Miss-loading carries consequences for any aircraft. An overloaded airplane will not perform as well, or as safely, as a properly loaded one. The heavier the aircraft is loaded within the approved limit, the less climb performance it will have, and the higher the stall speed will be.
The investigation determined that the aircraft departed Penticton about 150 pounds over its maximum gross weight, and was about 110 pounds over gross at the time of the crash. The aircraft balance remained within allowable limits.
Engine teardown
Both engines were disassembled and inspected following the accident. Indications were found that both engines were operating at impact, although a determination of the amount of power being produced was not made. The turbocharger waste gates on both engines were found to be in the open (bypass) position, meaning that the turbochargers were not being used.
No anomalies were found on the left engine. The spark plugs in 3 cylinders on the right engine showed high carbon buildup (likely indicating a rich mixture), while the spark plugs in the number 2 cylinder showed almost no carbon buildup. A partial obstruction, determined to be rust (TSB Laboratory Report LP242/2012), was found in 1 fuel nozzle (injector) on the right engine. That nozzle was found to flow to about 1/3 that of the other 3 fuel nozzles on that engine. A significant amount of rust was found on and around the steel components in the fuel-flow divider, immediately upstream of the nozzles.
Pilot decision-making
The Transport Canada publication Pilot Decision Making (TP 13897)Footnote 15, includes the following:
Flying is a continuous process of decision making involving the pilot, the aircraft, the environment in which the flight is taking place, the operation itself, and the flight situation…
…While under training, student pilots are constrained and their exposure to risk is controlled by lesson plans and the supervision of the instructor. Once they are licensed, however, pilots are not as constrained and are able to encounter more risks. They will encounter weather they may have never seen before, fly more complex aircraft, and undertake more complex trips that are longer and over quite different terrain than what they encountered in training. In short, they will gain experience, but in the early going they may not recognize some hazards, nor will they have as rich a set of rule-based behaviour patterns as more experienced pilots. Because of their lack of experience, they will not be as well prepared to deal with some situations they may encounter.
Flight recorders
This aircraft was not equipped with any on-board recording devices, such as a cockpit voice recorder or flight data recorder, nor were these devices required by regulation. As well, no other devices, such as a flight-tracking system, handheld global positioning system (GPS), or in-cockpit camera were installed.
TSB laboratory reports
The following TSB Laboratory Reports were completed:
- LP152/2012 – GNS Analysis
- LP242/2012 – Fuel Nozzle Blockage Analysis
Analysis
Aircraft performance
The increased density altitude, from 3300 feet at take-off to over 7000 feet at the accident site, resulted in reduced engine power and aerodynamic performance. In particular, the pilot's decision to not use turbocharger boost resulted in the engines performing like normally-aspirated engines, with continuously decreasing engine performance as the aircraft climbed.
The pilot did not calculate a weight and balance for the accident flight or the previous leg. This was, in part, likely because the information necessary to do so was not readily available to the pilot, in the journey log or elsewhere in the aircraft. On the leg before the accident flight, C-GLGJ departed Boundary Bay with full fuel (about 6 hours in duration), which was substantially more than was necessary to conduct the intended 2 flight legs (about 2.6 hours in total duration). On the accident leg, once the additional passengers and their baggage were boarded in Penticton, the aircraft was about 150 pounds over its maximum gross weight. There were no steps taken to reduce aircraft weight, and this higher weight contributed to reduced climb performance.
The partially obstructed fuel nozzle prevented the right engine from producing as much power as the left engine. The exact amount of power reduction could not be determined, but the aircraft's climb performance on the day of the accident was far lower than the figures stated in the pilot's operating handbook. The fuel-flow indicator showed that the right engine's fuel flow was higher than the left engine's, when in fact it was lower. As a result of that incorrect indication, and of normal revolutions per minute (rpm) and manifold pressure indications, it is likely that the pilot did not recognize the problem or its consequence.
The high density altitude conditions, high aircraft weight, non-use of available turbochargers, and reduced power of the right engine all contributed to a reduced rate of climb.
Likely accident scenario
Although the pilot observed that the aircraft's rate of climb after take-off from Penticton was lower than anticipated, and was aware that climbing to an altitude of 5000 feet before turning west toward high terrain was recommended, the pilot turned west at a lower altitude. The pilot continued flying up the valley toward an area of higher terrain in an aircraft that had reduced performance.
The pilot decided to conduct the flight despite being aware that visibility to the west (the flight planned route) was reduced by smoke. Reduced visibility was almost certainly encountered in the vicinity of Brenda Mines.
Neither survivor recalled the final moments of the flight. There were no other witnesses to the crash, and there were no on-board recording devices. The last time the aircraft was seen by a witness, about 2 nautical miles (nm) from the accident site, it was climbing slowly and was nearly at the same altitude as the accident site. It is not known why the pilot chose the accident flight path instead of a path slightly to its left that would have kept it over lower, unobstructed ground, but it is likely that visibility was reduced so that the pilot was unaware of the safer route.
The small number of trees that were damaged, the short length of the impact swath, and the relative intactness of the wreckage indicate that the aircraft was travelling at slow speed at the time of impact. Damage to the trees and to the wings' leading edges indicates that the aircraft was descending in a 45° right-wing-low bank when it struck the trees. If the aircraft had been descending in this attitude for more than a few seconds, it is likely that the speed at impact would have been higher. It is therefore likely that the aircraft was flying at a relatively low altitude in lowered visibility over the trees just before impact. The low altitude above terrain would not have allowed sufficient room to manoeuver, and the aircraft descended into the trees.
Pilot decision-making
The pilot had earned a commercial pilot's licence and several endorsements, but had relatively little experience. As well, although the accident aircraft was fairly sophisticated—twin engine, turbocharged, with retractable gear and an autopilot—it was privately owned and operated, which meant that the pilot did not have the organizational support that a student or a pilot flying for a commercial operator would have. This support includes resources such as co-workers' experience, copilot or instructor's assistance, managerial supervision, recurrent training, and company maintenance programs.
It is likely that the pilot had previously experienced each of the factors that contributed to the aircraft's low rate of climb—high density altitude, high aircraft gross weight, and degraded engine power—but it is unlikely that the pilot had dealt with all of them at the same time before the accident flight. As stated in the Transport Canada publication Pilot Decision Making (TP 13897), flying is a continuous process of decision-making. The process begins before the flight, when the pilot makes a plan that will result in a safe flight, and it continues throughout the flight, as the pilot monitors the results to determine whether the plan is working as anticipated. If it is not, the pilot needs to be able to revise the plan as necessary, often quickly. If the pilot does not recognize a situation that necessitates a change of plan, or does not have an alternative plan, risk increases.
Logbooks
The occurrence pilot (and previous pilots of C-GLGJ) did not write all defects in the logbooks. Not only is this contrary to Canadian Aviation Regulations (CARs), but it also makes it difficult for pilots and maintenance personnel to recognize trends, understand the significance of defects, and learn what rectifications have been tried (successfully and otherwise). This investigation determined that fuel-nozzle obstruction had been a problem in September 2011 and again in November 2011, and had likely been occurring as far back as 2005, 7 years before the accident. Because recurring symptoms (such as high fuel-flow indication, excessive vibration, unusual exhaust gas temperature (EGT), and left rudder required on take-off) were not properly documented, an opportunity to correctly diagnose and rectify the issue (water ingress into fuel tanks resulting in rust in the fuel system) was lost.
Other
Because the aircraft's battery disconnected from the electrical system during the crash, electrical arcing—one of the main sources of post-crash fire ignition—was eliminated. Despite a large volume of spilled AVGAS, there was no post-crash fire.
The aircraft was not equipped with shoulder harnesses, nor was it required to be. The aircraft owners were not aware that a shoulder-harness kit was available from and recommended by the aircraft manufacturer. All 4 occupants suffered serious head injuries. The severity of these injuries would likely have been reduced had the occupants been wearing shoulder harnesses.
Findings
Findings as to causes and contributing factors
- The high density altitude conditions, high aircraft weight, non-use of available turbochargers, and reduced power of the right engine all contributed to a reduced rate of climb.
- The pilot continued toward an area of higher terrain, and the aircraft was unable to climb rapidly enough to provide adequate terrain clearance.
- The aircraft collided with terrain, likely while in an area of reduced visibility.
Findings as to risk
- There is an increased risk of injury to occupants if the aircraft is not equipped with shoulder harnesses.
- If maintenance activities are not properly documented, an opportunity to correctly diagnose and rectify defects is lost.
Other findings
- The battery disconnected during the crash, which removed an ignition source and may have reduced the risk of a post-crash fire.
Safety action
Safety action taken
Transport Canada and NAV CANADA
NAV CANADA has issued a Canada Flight Supplement amendment for the Penticton, Oliver and Osoyoos Airports in the Okanagan Valley. The following warning has been added to the caution sections of these airports:
“Due to high terrain, it is recommended pilots proceeding E or W under VFR, maintain an alt of 5,000 feet (ASL) min before leaving the Okanagan Valley.”
The next available edition of the NAV CANADA Vancouver visual flight rules (VFR) navigation chart (VNC) includes the new VFR route, as suggested by Transport Canada, between Princeton, Brenda Mines and Highway 97C to Okanagan Lake. An associated caution reads as follows:
−CAUTION−
VFR ROUTE VALLEY FLOOR HAS STEEP GRADIENT TO 4500 FEET ASL WITHIN 10NM OF OKANAGAN LAKE
This edition of the VNC, no. 25, is planned for August 2013.
Penticton Airport
A new sign (Figure 2) was installed at Penticton Airport, advising pilots to climb to 5000 feet before turning west or east when departing the Okanagan Valley.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on . It was officially released on .