Loss of control and collision with terrain
Kananaskis Mountain Helicopters Ltd.
Bell 206B JetRanger (Helicopter) C-GLQI
Loder Peak, Alberta 0.4 nm NW
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 30 March 2012, the Kananaskis Mountain Helicopters Bell 206B helicopter (registration C GLQI, serial number 1964) departed the Kananaskis/Nakoda base near Kananaskis, Alberta, on a visual-flight-rules day tour flight, with 1 pilot and 4 passengers on board. Approximately 13 minutes after departure, at about 1010 Mountain Daylight Time, the helicopter crashed in a steep, snow-covered avalanche corridor, in a cirque near Loder Peak. About 1 hour and 29 minutes later, the operator was advised by the Joint Rescue Coordination Centre in Trenton, Ontario, that the 406 emergency locator transmitter on C-GLQI was transmitting. A company helicopter was dispatched to search the tour route, and found the wreckage at approximately 1206. All occupants were extracted from the site. The 4 passengers sustained minor injuries; the pilot succumbed to injuries approximately 5 hours after the accident, following removal from the accident site. There was no post-crash fire.
Factual information
The company
Kananaskis Mountain Helicopters (KMH) operates a fleet of 12 helicopters, and holds a valid air operator certificate issued by Transport Canada (TC) under Subparts 702 and 703 of the Canadian Aviation Regulations (CARs). Flight operations are conducted from 2 year-round bases located at Kananaskis/Nakoda (CNK7) and Cline River, Alberta. The CNK7 base is situated east of Canmore, Alberta, adjacent to the eastern slopes of the Rocky Mountains. The services provided include tour flights, oil and gas operations, fire-fighting operations, and general charter. The company had been operating tour flights since 1994. The accident flight was being operated as an air-taxi flight under CARs Subpart 703.
KMH operates in affiliation with Kananaskis Heli Tours, a company that offers mountain sightseeing helicopter flights from either base. The sightseeing flights out of the CNK7 base range in length from 20 to 55 minutes. The accident flight was advertised as the 20-minute Rockies Heritage Tour, and included an optional 1-hour wilderness stop at Brokenleg Lake, Alberta, where passengers could snowshoe for 1 hour.
History of the flight
The Rockies Heritage Tour flight route was a 25- to 27-nautical−mile (nm) circular route. This flight normally proceeded south from the CNK7 base to Barrier Lake, then west to Heart Mountain, and north to the Trans-Canada Highway. After crossing the Trans-Canada Highway, the flight would continue northbound, and would normally track east of Loder Peak (Photo 1). A flight tracking west of Loder Peak would enter the Jura Creek Valley, and then cross a ridge to the north of Loder Peak from west to east, before descending to Brokenleg Lake. The ridges to the north of Loder Peak crested at 7300 to 7400 feet above sea level (asl). The route to the east of Loder Peak paralleled the slopes east and north of Loder Peak, with the Alberta plains immediately to the east. The eastern route could be completed at significantly lower altitudes. Once reaching Brokenleg Lake, with or without a stop, the flight would track directly back to the CNK7 base. The route could be changed at the pilot's discretion due to wind, weather, or time constraints. The accident flight was expected to take 0.3 hours of air time and about 1.3 hours overall, as the passengers had opted for the stop at Brokenleg Lake.

On the accident flight, the pilot entered the Jura Creek Valley northbound, and flew in close proximity to the steep west-facing slopes on the eastern side of the valley (Photo 1). As the helicopter approached the crest of a 7300-foot−high ridge to the north of Loder Peak, in very close proximity to the outcrops and at an altitude below the crest, the helicopter encountered turbulence. Several seconds later, the pilot initiated a left turn toward the valley. Partway through the turn, control was lost, and the helicopter began to spin to the right. Control was not regained, and the helicopter continued to spin rapidly to the right, about the vertical axis, in close proximity to the mountain slope. The helicopter rotated an estimated 6 to 12 times, struck the slope 3 times, and came to rest on snowpack within an avalanche corridor, in a cirque (Photo 2).Footnote 1 The accident occurred at 1010.Footnote 2
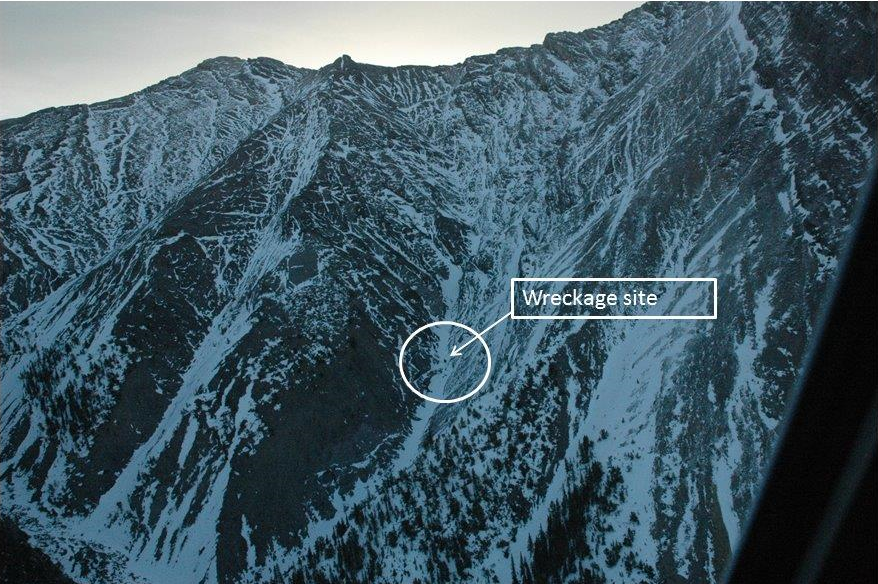
The wreckage came to rest at 6700 feet asl, at 51°06′38.63″ N, 115°09′07.64″ W. The tail boom and main rotor separated during the impact sequence. The fuselage came to rest in snow on its left side, in a nose-low attitude and partially inverted. Investigators were unable to travel to the accident site, due to the risk of rock slides and snowslides; therefore, ground scars associated with the accident were not identified.
Survival aspects
All occupants were secured with a 4-point lap-belt and shoulder-harness restraint system. The use of this restraint system likely reduced the level of injury sustained by the occupants. The 3 passengers seated in the cabin were able to exit the helicopter on their own, through the right cabin door. The passenger in the left cockpit seat was trapped between the left cockpit door, which was resting in snow, and the pilot. The pilot was immobilized, and was in and out of consciousness due to serious head and neck injuries. A passenger released the pilot's harness, and the pilot was removed and laid in snow adjacent to the fuselage. Repositioning of the pilot was minimized, to reduce the risk of exacerbating the injuries. The pilot was not wearing a helmet during the flight.
The temperature at the time of the accident was estimated to be −3°C. The pilot was lightly dressed, and was wearing a long-sleeved cotton sweatshirt, without a jacket. A toque was placed on the pilot's head, and the pilot was covered with lightweight metal survival blankets found in the survival kit. Several snowshoes were placed upright in the snow to form a wind shield around the pilot. The passengers, who were dressed in light winter clothing, subsequently dug a pit in the snow on the upslope side of the wreckage, and used it to reduce their own environmental exposure. The passengers attempted but were unable to establish emergency cellular phone communication.
A rescue helicopter dispatched from Canmore, 7.5 nm west of the site, was delayed for about 70 minutes, due to severe weather that moved through the area between approximately 1245 and 1355. Since it was not possible to land at the site, 2 members of a specialized mountain rescue team were lowered into the accident site by long-line at 1410. Extraction of the occupants from the site was accomplished by lifting them individually in a heli-sling rescue operation. All occupants were long-lined to a safe staging area. The last heli-sling extraction was complete at 1533. The pilot died after extraction from the site, but before transport to a medical facility. An autopsy determined the cause of death to be a combination of head and neck trauma, with hypothermia contributing.
Operational control
KMH used a platform scale to weigh all tour passengers as a group on all tour flights, and the pilot was provided with that weight information before departure. The helicopter's weight at the time of the accident was estimated at 3044 pounds—below the maximum weight of 3200 pounds—and its centre of gravity was within prescribed limits. There was sufficient fuel on board the helicopter for the intended flight.
The company operated under a TC Type D operational control system, and had an active flight-watch system in place. Flight following for a Type D system requires the monitoring of a flight's progress and the notification of appropriate company and search-and-rescue authorities if the flight is overdue or missing.Footnote 3 The KMH Operations Manual stated that most aircraft were equipped with satellite tracking equipment and that, where and when available, this equipment would be used to monitor a flight's progress. The accident helicopter was fitted with a Sky Connect satellite-based tracking system that allowed the operator to track the progress of the flight. The system was programmed to provide a position update, along with altitude and ground speed, once every 2 minutes. This information, as well as pilot reporting, was used to monitor tour flights. On rare occasions in the past, tour pilots either had forgotten to report landing at Brokenleg Lake or had delayed reporting until the helicopter had descended to an altitude that precluded very high frequency (VHF) radio communication with the base, due to terrain blockage. In these cases, the flights had always reported departing Brokenleg Lake about 1 hour later.
The flights were monitored in the Kananaskis Heli Tours office at the CNK7 base. Kananaskis Heli Tours staff members were not assigned exclusively to flight-monitoring duties, and were routinely engaged with numerous customer-care, tour-management, telephone, and receptionist duties while flights were in progress. A flight failing to arrive within 1 hour of the estimated time of arrival was considered overdue, and KMH would be notified. KMH personnel had become aware that the flight was overdue a few minutes before receiving the Joint Rescue Coordination Centre telephone call, and were initiating a response when the call came.
The last Sky Connect tracking return, received at 1005, showed the helicopter crossing the Trans-Canada Highway northbound at 6600 feet asl, at a ground speed of 118 knots, and on a heading of 010° true (T). The last radio communication with the helicopter was a pilot report stating that the flight was passing Loder Peak, bound for Mount Yamnuska. KMH 's flight-following procedures did not identify that the aircraft had stopped transmitting its satellite tracking position and that the pilot had not reported landing at Brokenleg Lake.
Mountain-flying guidelines
Helicopter flying operations in mountainous terrain are particularly demanding, and require specialized knowledge on the part of a pilot. Techniques have been developed to minimize the inherent risk. One hazard is the presence of visual illusions when turning toward rising ground. A pilot turning toward rising ground may perceive that the helicopter's nose is too low, and may intentionally pitch nose-up to maintain a constant sight picture. The result is a decrease in airspeed. This decrease can be more pronounced in cirques or in rapidly rising terrain.
Mountain winds can have either a beneficial or negative effect on helicopter performance, and their impact will depend on pilot techniques and routing used. In combination with high altitude, turbulence and downdrafts can reduce aircraft performance and produce serious consequences in close proximity to terrain. Defenses against mountain-flying hazards include monitoring of helicopter performance, which requires controlling airspeed and vertical speed, and assessing the outside sight picture,Footnote 4 as well as ensuring the availability of a drop-off zone to safely fly away should safe handling conditions and available power requirements be exceeded. The KMH flight-training guidelines called for all ridge crossings to be carried out above 500 feet from any pass, and all passes to be approached at a maximum angle of 45°, in order to provide a good escape route before crossing. KMH pilots were expected to adhere to these guidelines at all times.
Meteorological information
Visual meteorological conditions (VMC) existed at the time of the accident, and the ceiling and visibility conditions were suitable for the intended flight. The nearest aviation weather reporting station was located at the Calgary/Springbank Airport (CYBW) in Alberta, situated 24 nm east of the CNK7 base. Hourly weather for CYBW , taken 10 minutes before the accident, indicated that surface winds were 220°T at 9 knots, and visibility was 30 statute miles, with a few clouds at 6000 feet above ground level (agl), a few clouds at 10 000 feet agl, and a broken layer at 22 000 feet agl. The temperature was 6°C, and the dew point was −3°C, with an altimeter setting of 29.23 inches of mercury (in Hg). The surface winds were light, and the ceiling and visibility were similar to when the helicopter departed the CNK7 base.
The Nakiska Ridgetop remote automated weather-recording station, located approximately 10 nm south of the accident site at 8341 feet asl, indicated that at 1000, surface winds were from 210°T at 10 knots, and the temperature was −5.6°C. At 1100, the same station indicated that surface winds were from 210°T at 13 knots. At about 1315, a front passed through the accident site, leading to reduced visibilities in snow, a wind shift from the north, and a reduction in temperature to about −6°C.
Pilot information
Records indicate that the pilot was qualified and certified for the flight in accordance with existing regulations. The pilot had started flying training in June of 2003, and had received a commercial helicopter pilot licence in April of 2004. Examination of the pilot's personal log book, as well as a personal trip log, determined that, at the time of hiring by KMH on March 11, 2012, the pilot had 425 hours of flight time, including 314 hours as pilot-in-command (PIC) and 193 hours on the Bell 206B. On the application form for employment at KMH , the pilot claimed to have 485 hours of flight time, including 265 hours on the Bell 206. On an insurance application form dated 29 March 2012, after having acquired approximately 6 hours of dual and PIC flight time at KMH , the pilot reported having 500 hours of total flight time, 450 hours of PIC time, and 272 hours of Bell 206 time, including 18 hours within the past 6 months. On the same insurance application, the pilot reported having not had or been involved in any aircraft accidents. However, records indicated that the pilot had previously been involved in an accident in October 2005, when a RotorWay Exec 162F amateur-built helicopter was substantially damaged in a rollover accident.Footnote 5
The pilot had acquired the previous Bell 206 flight experience between September 2008 and June 2010, while employed by a helicopter company based in central British Columbia. There was no record of the pilot having flown in the 21 months between June 2010 and February 2012. In February 2012, the pilot acquired 2.6 hours of flight time on a Robinson R44, toward an endorsement on type.
The pilot had no previous formal mountain-flying training or experience. There is no regulatory requirement for pilots to obtain formal mountain-flying training before undertaking flights in mountainous areas. Generally at KMH , the length and detail of this training varied depending on management confidence in new pilots' abilities, experience, and training performance. Since tour pilots were not normally expected to land in rugged terrain, introductory training did not usually include exposure to a rigorous mountain operational environment. For the accident pilot, the chief pilot had combined the recurrent and emergency training with introductory mountain-flying training. The pilot had demonstrated a strong reluctance to fly in close proximity to mountain slopes during the KMH training flights.
The pilot was on duty daily from 13 March to 29 March, for 10 to 12 hours each day, performing many non-flying duties at the base. Before acting as PIC on tour flights, the pilot was provided with 2.5 hours of recurrent flight training over 3 flights, and a 0.5-hour pilot competency check (PCC) flight by the chief pilot. At the time of the accident, the pilot had acquired 7.8 hours of flight time, including flight-training time and tour-flight time, with KMH.
There was nothing found to indicate that the pilot's performance was degraded by physiological factors. The pilot had experienced a normal sleep-wake pattern in the days before the accident, and there was no evidence that chronic or acute fatigue were factors in the occurrence.
Company pilot-hiring practices
An applicant with no previous flying experience can obtain a commercial helicopter licence after having completed a minimum of 100 hours of commercial pilot flight training in helicopters. The challenge for new commercial helicopter pilots is gaining the flying experience needed to get a flying job, as many helicopter operators require 1000 hours or more of helicopter flight time as a minimum prerequisite for employment, in order to meet insurance and client requirements. New pilots often work in non-flying positions within aviation companies before being hired as pilots. One avenue for low-time pilots to acquire commercial flight experience is to work as tour pilots. Tour flights are typically short and local in nature, and the routes are pre-determined by the operator and flown repetitively, enabling a pilot to build local knowledge. As sightseeing is the primary purpose of the flights, they generally take place in good visual flight rules (VFR) weather conditions. Off-base landings are infrequent. The off-base tour-flight landings at KMH took place in specifically designated, unconfined low-risk areas.
KMH routinely hired newly licensed commercial pilots, some with little more than 100 hours of flying experience, to conduct tour flights. First-year pilots were required to pay their own training costs, which were reimbursed on a pro-rated basis depending on length of employment with the company. As well as providing low-time pilots with an opportunity to build flying experience, this policy ensured that KMH had a pool of pilots to draw from and provided the company with a source of training revenue. The KMH website advertised that KMH has a well-known tour-pilot mentoring program that provides pilots for both KMH and the industry as a whole.
The company employed up to 18 pilots during the tourist season. For approximately one-half of the pilots, their employment at KMH was their first commercial helicopter pilot job. The work was seasonal in nature; there was a high turnover of pilots, either due to seasonal layoff or movement to higher paying jobs; and pilots often left the company once they reached 500 hours of flying experience.
Newly licensed pilots hired without mountain-flying experience were required to take a KMH introductory mountain course, at their own expense, before flying tour flights. In the case of the accident pilot, the company had not confirmed the pilot's previous mountain-flying training or experience. But in view of the pilot's reported flying experience and time, the company did not require formal mountain training.
In addition to flying, new pilots were tasked with many ancillary duties associated with the helicopter operations, tour administration, and base maintenance. These activities occupied a great deal of time between flights, and overall, allowed management to assess an individual's work habits and performance. The pilot was characterized as conscientious, with an excellent work ethic.
Previous flights
KMH allowed new pilots to ride with each other on tour flights if seating space was available and if the tour passengers approved. Low-time pilots often rode with each other, but generally, high-time pilots did not ride along. These flights were encouraged by the company to increase new pilots' knowledge of the tour area.
Passenger photos and video, as well as Sky Connect tracking system information from the pilot's previous flights, indicated that before 27 March 2012, the pilot normally used a routing to the east of Loder Peak. On 27 March 2012, a television film crew had chartered a KMH Bell 206B helicopter for a Rocky Mountain filming flight. The accident pilot accompanied the flight as a passenger seated in the left cockpit seat. Video from that flight shows that on 1 segment, the helicopter was flown close to cliff faces and saddles to the northwest of Loder Peak, and the film crew expressed very positive impressions during the flight.
The pilot completed 13 Rockies Heritage Tour flights before the accident. Tracking information indicated that before the filming flight, the pilot had tracked to the east of Loder Peak 11 times. During the last 2 flights before the accident and on the accident flight, the pilot tracked to the west of Loder Peak. No in-flight photos had been taken during the accident flight.
Helmet Use
The second most frequently injured body region in survivable helicopter crashes is the head.Footnote 6 According to United States military research, the risk of fatal head injuries can be as high as 6 times greater for helicopter occupants not wearing head protection.Footnote 7 The effects of non-fatal head injuries range from momentary confusion and inability to concentrate to full loss of consciousness.Footnote 8 Incapacitation can compromise a pilot's ability to escape quickly from a helicopter and to assist passengers in an emergency evacuation or survival situation. The TSB has documented a number of occurrences in which the use of head protection likely would have reduced or prevented the injuries sustained by the pilot.Footnote 9
In Canada, Aviation Occupational Health and Safety Regulations (SOR/2011-87) are issued pursuant to the Canada Labour Code. These regulations apply with respect to employees employed on board aircraft while in operation and with respect to persons granted access to those aircraft by the employer. Section 6.4 of the Aviation Occupational Health and Safety Regulations states that if there is a risk of head injury, protective headwear shall be used. Although not required by regulation to do so, helicopter operators may conduct a risk assessment to ascertain the level of risk of head injury associated with their operations, to determine if headwear is required.
There is no CARs requirement for helicopter pilots to wear protective headgear. As most pilots flying for KMH voluntarily wore helmets, the company's assessment of risk did not result in a policy requiring mandatory use of helmets. Pilots provided their own helmets, and the accident pilot was considering purchasing a helmet at the time of the accident.
In recognition of the benefits of head protection, a resolution passed by the Helicopter Association of Canada (HAC) Board of Directors on 27 June 2011 stated that:
HAC strongly recommends to its Operator-Members that they should promote the use of helmets for helicopter flight crew members under all operational circumstances which permit their use. HAC also points out, however, that certain pilot/aircraft type configurations may preclude safe helmet use.
Emergency locator transmitter
The helicopter was fitted with an Artex ME406HM emergency locator transmitter (ELT), part number 453-6604, Rev D. The ELT was mounted horizontally on the right side of the left cockpit footwell, and remained secure in the bracket after impact. When activated, this ELT transmits on 406 megahertz (MHz) for satellite detection, and on 121.5 MHz for detection and location identification based on direction finding.
The ELT was fitted with a rod antenna, mounted on the roof deck above the cockpit, and a remote switch assembly, mounted on the console between the 2 cockpit seats. When the ELT is active, a buzzer provides an audible alert, and a light emitting diode (LED) on the remote switch assembly flashes. Immediately following the accident, these indicators were not observed within the wreckage. Three to 5 minutes after the accident, a passenger moved the remote switch from the ARM position to the ON position; a flashing LED on the remote switch assembly and an audible tone were immediately detected.
Before the availability of multi-axis g-switchFootnote 10 modules, ELT manufacturers advised installing ELT s with the sensitive axis pointing approximately 45° downward from the normal forward direction of flight in helicopters. Experience determined that this mounting angle tended to preload the g-switch, and non-emergency nuisance activations could occur as a result of severe manoeuvres and abrupt takeoffs and landings. The ELT is equipped with a 5-axis g-switch module in addition to the usual primary g-switch, which is oriented to the direction of flight. The 6-axis coverage of this ELT design accommodated the flight characteristics of helicopters, while allowing normal installation and significantly reducing nuisance ELT activations. The primary g-switch required 2.3 g to activate; the auxiliary 5-axis g-switch required 12 g to activate.
The ELT was forwarded to the TSB Laboratory to test the operation of the 2 g-switches. TSB Laboratory tests conducted on the ELT showed that, when received, the unit would not function properly in either the ON mode or the ARM mode. While the ELT did function properly when switched to the ON mode a few minutes after the accident, it could not be determined why it did not activate at the time of the crash, even though the mode switch was in the ARM position.
COSPAS-SARSAT, GEO SAR and MEOSAR
COSPAS-SARSAT is an international program that provides distress alert and location data to help search-and-rescue authorities assist persons in distress. COSPAS is a Russian acronym for space system for the search of vessels in distress, while SARSAT stands for search-and-rescue satellite-aided tracking.
The system is composed of:
- distress radio beacons which transmit signals during distress situations;
- instruments on board satellites in geostationary and low-altitude Earth orbits which detect the signals transmitted by distress radio beacons;
- ground receiving stations, referred to as Local Users Terminals (LUTs), which receive and process the satellite downlink signal to generate distress alerts; and
- Mission Control Centres (MCCs) which receive alerts produced by LUTs and forward them to Rescue Coordination Centres (RCCs), Search and Rescue Points Of Contacts (SPOCs) or other MCCs.Footnote 11
COSPAS-SARSAT detects ELT s and other beacons transmitting on 406 MHz. The COSPAS-SARSAT system includes 2 types of satellites: a 6-satellite constellation in low-altitude Earth orbit (LEO), which forms the LEO SAR System, and a 5-satellite constellation in geostationary Earth orbit (GEO), which forms the GEO SAR System. The LEO SAR satellites orbit the poles at approximately 1000 km above earth, and the GEO SAR satellites are stationary over the equator, at approximately 36 000 km above earth. The LEO SAR and GEO SAR capabilities “are complementary. For example, the GEO SAR system can provide almost immediate alerting in the footprint of the GEO SAR satellite,”Footnote 12 whereas the LEO SAR system provides coverage of the polar regions. As well, the LEO SAR system “can calculate the location of distress events using Doppler processing techniques, and is less susceptible to obstructions which may block a beacon signal in a given direction because the satellite is continuously moving with respect to the beacon.”Footnote 13 The COSPAS-SARSAT system first detected the ELT at about 1123.
Currently a third satellite system, the Medium-Earth Orbit Search-and-Rescue (MEOSAR) system, is in the prototype phase. The MEOSAR system is intended to overcome the combined limitations of the LEO and GEO satellites. These limitations, all of which can delay alerting, include periodic or non-continuous coverage of the earth by LEO , limited coverage of the polar regions by GEO SAR, and no locating capability with GEO SAR unless the transmitting beacon has GPS integration. Both systems are subject to reception interference due to terrain blockage. At the time of the accident, the MEOSAR system consisted of 3 satellite constellations, with a total of 11 satellites in orbit. Each constellation will eventually have 24 satellites. The Canadian Mission Control Centre (CMCC) currently does not receive MEOSAR data directly. The developmental next-generation MEOSAR SARSAT system detected the ELT at 1014, based on data out of a Hawaii monitoring station. This system will not be operational until at least 2015.
Aircraft
The helicopter had no known deficiencies before the flight. Records indicated that the helicopter was certified and equipped in accordance with existing regulations and approved procedures.
The helicopter sustained extensive damage from the impact. Approximately 95% of the helicopter, including all critical components, was recovered from the accident site. No mechanical discrepancies that would have contributed to the accident were identified during examination of the wreckage. All flight controls were continuous before the accident, and all damage was attributed to the impact sequence. The main-rotor and tail-rotor systems had sustained extreme damage due to ground contact, indicating that both systems were operating under high power at impact.
The engine torque gauge, altimeter, and annunciator panel were recovered from the wreckage and forwarded to the TSB Laboratory for detailed analysis. It could not be determined what the torque gauge was indicating at impact. The condition of the filaments in the annunciator lamps was consistent with all lamps being OFF at impact.
While the altimeter was found to be functional when received at the TSB Laboratory, it was out of calibration. On average, it was indicating 700 feet (with a standard deviation of 34 feet) lower than it should have been, through an altitude range of zero to 20 000 feet. The calibration error was consistent across the instrument's full range. A microscopic examination of the altimeter's dial face and internal mechanism did not reveal any witness marks that could be used to determine what the unit was indicating at impact. As well, whether the altimeter was out of calibration before or as a result of the accident could not be determined.
The altimeter had last been calibrated on 03 December 2009, and had been installed in the helicopter on 02 March 2010. Altimeters in this type of aircraft must be calibrated at intervals not exceeding 24 months, regardless of the date of installation in an aircraft. The KMH Small Aircraft Maintenance Schedule tolerances were 10% of the specified interval, up to a maximum of 200 hours/3 months/50 cycles. A journey-log entry dated 07 March 2012 indicated that the altimeter calibration had been granted a 1-month extension to 07 April 2012.
The altimeter was set to 29.20 in Hg when the wreckage was recovered. The altimeter setting for CYBW , located 24 nm east of CNK7, was 29.23 in Hg at the time of the accident. KMH helicopter pilots normally set the altimeter to field elevation before departing from CNK7. If the pilot had set the altimeter to field elevation of 4260 feet before departure, and the resulting altimeter setting was 29.20 in Hg, it is probable that the altimeter was accurately calibrated at the time of the flight. If the altimeter was indicating 700 feet low at a given altimeter setting, the helicopter would have been 700 feet higher than indicated in flight.
Performance
At near-maximum gross weight, at the accident-site density altitude of 7600 feet, Bell Helicopter charts for the Bell 206B indicate that climb performance at 47 knots was 1280 feet per minute. Hover out-of-ground-effect was not possible above 5600 feet pressure altitude at ambient temperature. Turbulence and downdraft would further reduce these performance capabilities. Normal cruise speed is approximately 105 knots.
Unanticipated yaw or loss of tail-rotor effectiveness
Federal Aviation Administration (FAA) Advisory Circular AC 90-95, Unanticipated Right Yaw in Helicopters, defines loss of tail-rotor effectiveness (LTE) as a critical low-speed aerodynamic flight characteristic, not related to mechanical malfunction. It can result in an uncommanded rapid yaw rate that does not subside of its own accord and that, if not corrected, can result in loss of aircraft control.
LTE may occur in all single main-rotor helicopters at airspeeds less than 30 knots. On US-manufactured single-rotor helicopters such as the Bell 206, the main rotor rotates counter-clockwise as viewed from above, and the torque produced by the main rotor causes the fuselage of the aircraft to rotate in the opposite direction. In the case of helicopters such as the Bell 206, a tail rotor provides thrust that counteracts main-rotor torque. Any manoeuvre that requires a pilot to operate in a high-power, low-airspeed environment with a left crosswind or tailwind creates an environment where LTE may occur.
Four relative wind azimuth regions can create an environment conducive to LTE:
- Main-rotor disc vortex interference (winds from 285° to 315° relative to the helicopter)
- Weathercock stability (winds from 120° to 240°)
- Tail-rotor vortex ring state (winds from 210° to 330°)
- Loss of translational lift (winds from all azimuths)
Conditions of high gross weight and high-density altitude can significantly influence the severity of the onset of LTE. When operating at air speeds below translational lift,Footnote 14 in areas such as along ridgelines or near buildings, pilots are cautioned to avoid tailwinds and to be alert to changing aircraft flight and wind conditions.Footnote 15 If sudden unanticipated right yaw occurs, recovery should be initiated immediately by applying full left pedal, moving the cyclic forward to increase speed, and, if altitude permits, reducing power. As a recovery takes place, controls are adjusted for normal forward flight.
Flight crew member qualifications
TC CARs 703.88(1)(c)(ii) requires that a PIC on commercially operated single-engine helicopters under VFR successfully complete an annual pilot proficiency check (PPC) on a type operated by the air operator. PPCs must be conducted by TC inspectors or by approved check pilots.
In 2004, a TC risk-assessment team, in anticipation of the implementation of safety management system (SMS) programs in CARs Subpart 703 operators, recommended that the requirement for a PPC be removed and replaced with PCC s. A PCC can be conducted by a chief pilot or designate; however, the chief pilot is not relieved of the responsibility to ensure that the tested operational pilot has fulfilled all training, competency, and currency requirements. TC Policy Letter 178, dated 09 January 2006, enabled this exemption, and KMH operated under this exemption. Although the exemption policy was established in keeping with the principles of SMS, there are no requirements to date for CARs 703 operators to have a SMS.
Safety management system
KMH had a comprehensive, internal, voluntary SMS in place that was designed to identify hazards and eliminate or minimize accident risks within the company, through incident and hazard reporting and risk-management follow-up. The SMS was not required to be approved by TC. CARs Subpart 703 operators were not required to have a SMS, and regulations pertaining to SMS in CARs Subpart 703 organizations did not exist. A review of the reports filed within the year before the accident did not reveal any concerns related to pilot conduct or operational control of tour-flight operations.
Recent Transport Canada inspections
TC Civil Aviation Staff Instruction no. SUR-001 (Surveillance Procedures) defines a TC program validation inspection (PVI) as a process comprised of a documentation review of 1 or more components of a SMS or other regulated areas of a certificate holder. PVI s are conducted on a routine schedule, using risk indicators to adjust the frequency as necessary. While PVI s are intended for review of a company as a whole, they may include examination of a specific item or testing of an individual against established standards.
On 26 January 2011, an evaluation of 13 risk indicators of KMH , covering the period of 01 April 2011 to 31 March 2012, was conducted. This type of evaluation is used as a guide by TC for prioritizing companies that require additional oversight activities. The evaluation scored 9.5. Any score over 10 points indicates that the company should receive immediate attention. This risk evaluation prompted a PVI that was carried out November 21 to 24, 2011.
The PVI resulted in 4 findings: 2 related to deficiencies in operational control, and 2 related to maintenance. The operational control findings were administrative in nature, and related largely to deficiencies in flight duty time records and flight-training records. The company submitted a corrective-action plan, which was accepted by TC. No issues were outstanding at the time of the accident.
Following the accident, in May 2012, TC conducted a process inspection (PI). A PI is a streamlined inspection that may be triggered on short notice by a number of circumstances, including an accident, and that focuses on matters believed to be related specifically to the initiating circumstances. The PI resulted in 6 findings related to operational control, including 2 for which the operations manager and chief pilot bore responsibility. The other 4 findings addressed training deficiencies. In April, May, and October 2011, unqualified pilots had been used for recurrent flight training of company pilots, including the operations manager and chief pilot. Consequently, at the time of the accident, the chief pilot was not considered qualified to conduct PCC s, and the checks that the chief pilot had conducted on staff pilots, including the accident pilot, were considered by TC to be invalid. TC then elected to temporarily remove the exemption under TC Policy Letter 178, and to conduct PPCs on all KMH pilots. Several of the operational control deficiencies that were identified during the post-accident PI were present at the time of the November 2011 PVI; however, they had not been identified during the PVI. They were also present at the time of the accident.
Lightweight flight recording system
The helicopter was not fitted with any sort of flight recorder, and flight and voice recorders are not required by regulation to be installed in commercially operated aircraft of this size. Lightweight flight recording systems with cockpit imaging capability are now available for installation in small aircraft; these lightweight systems are low-cost and do not require extensive modification of the aircraft for installation.
In the case of this accident, a functioning lightweight flight recording system with cockpit imaging capability would have provided the following, otherwise unobtainable, information:
- Forward view of terrain through the cockpit window, which would have identified proximity to terrain
- Flight instrument, engine instrument, and warning indications
- Pilot actions, control inputs, and helicopter response
- Comprehensive altitude, speed, and GPS tracking data
- Helicopter flight attitude data
- Acceleration data
- Ambient sound data
- Other information depending on the data-collection technology offered by individual lightweight flight recording system manufacturers
This information would have allowed investigators to reconstruct the flight sufficiently to validate the factors that led to the accident, thereby providing an improved opportunity to identify safety deficiencies related to the occurrence. At minimum, data from a lightweight flight recorder would have been pivotal in confirming the reason for the loss of control.
As well, given the combined high accident-rate statistics for CARs Subparts 702, 703, and 704 operations, there is a compelling case for industry and the regulator to proactively identify hazards and manage the risks inherent in these operations. To manage risk effectively, they need to know why incidents happen and what the contributing safety deficiencies may be. Moreover, routine monitoring of normal operations can help these operators both improve the efficiency of their operations and identify safety deficiencies before they result in an accident. It is for these reasons that the TSB , following an investigation into the in-flight breakup of a turbine-powered de Havilland DHC-3 Single Otter aircraft,Footnote 16 recommended (in Recommendation A13-01) that
the Department of Transport work with industry to remove obstacles and develop recommended practices for the implementation of flight data monitoring and the installation of lightweight flight recording systems for commercial operators not required to carry these systems.
The circumstances of this accident highlight the need for action on this recommendation.
The following TSB Laboratory report was completed:
- LP065/2012 − Instruments Analysis
Analysis
The investigation found nothing to indicate any airframe failure or system malfunction before or during the flight. The helicopter was being operated within its weight and center-of-gravity limits at the time of the accident. As well, the weather at the time of the accident was suitable for visual flight rules (VFR) flight. Therefore, the analysis will focus on several other factors, including the pilot's experience and training, airmanship, operational control within the company, and environmental factors that likely contributed to the occurrence.
Other than 2.6 hours of flight time obtained in February 2012 toward a Robinson R44 helicopter endorsement, there was no record of the pilot having flown for approximately 21 months when hired by Kananaskis Mountain Helicopters. At the time of hiring, the pilot had little or no mountain-flying training or actual mountain-flying experience.
Based on the pilot's self-reports of having approximately 500 hours of helicopter flight experience in British Columbia and no accidents, the company considered the pilot to have adequate knowledge, skill, and experience to safely conduct mountain tour flights with minimal recurrent flight training and checkout. That the pilot had a previous accident, no prior mountain-flying training, and minimal mountain-flight experience was not identified. As a result, the pilot received very little instruction from Kananaskis Mountain Helicopters (KMH) in mountain-flying techniques, and a minimal evaluation of abilities in that environment. The pilot's reluctance to fly in close proximity to rock outcrops during KMH flight training heightened the company's confidence in the pilot's ability to safely conduct tour flights within the mountainous local area.
Before the filming flight on which the pilot rode along, the pilot flew exclusively on the eastern side of Loder Peak over relatively gentle terrain. The pilot's change of routing to the western side on subsequent flights, and operation in very close proximity to the steep, rugged terrain, were likely influenced by the positive experience on the filming flight, and motivated by a desire to provide the tour passengers with a more thrilling experience. The change in the pilot's routing was unknown to the company. Although this information was available through the Sky Connect system, the company did not have a program in place to monitor the flight profiles of the inexperienced pilots. KMH 's flight-following procedures did not identify that the helicopter had stopped transmitting its satellite tracking position and that the pilot had not reported landing at Brokenleg Lake. This lack of information delayed initiation of search-and-rescue operations.
While flying below the western side of the mountain ridge and climbing toward a saddle leading to the eastern side of the ridge, the helicopter entered a shallow but very steep cirque. The KMH guideline stipulating that ridge crossing was to be carried out above 500 feet from any pass was not followed, increasing the risk of collision with terrain. In attempting to out-climb the terrain, and presented with an illusion resulting from lack of a true horizon while in very close proximity to the rugged rock faces, the pilot may have experienced difficulty in maintaining a constant pitch attitude. There may have been a tendency, when facing the mountain, to raise the nose, with substantial loss of airspeed and climb performance. The illusion may have been compounded by a tailwind, resulting in significant movement across the ground at a low airspeed, and a visual illusion of higher than actual airspeed. The turbulence that was experienced indicates that the helicopter may have entered an area of down-flowing air, or the turbulence may have been the result of loss of translational lift, either of which would have resulted in increased power demands.
It is likely that the pilot recognized the loss of climb performance and attempted to turn left, away from the mountain and into the drop-off area. However, the decision to make this turn was likely made too late to avoid a decrease in airspeed below translational lift speed. Severe damage to the main- and tail-rotor systems indicate the application of high power when the tail-rotor blades struck the rock face. Rapid, multiple rotations to the right indicate a loss of tail-rotor effectiveness, which could be explained with 2 scenarios:
- During an uncoordinated left turn in very close proximity to the rock face and at low airspeed, the tail rotor contacted the ground, with destruction of the rotor and its drive system.
- The high-density altitude (7600 feet) would have required further increase in anti-torque from the tail rotor. An unanticipated right yaw occurred when airspeed deteriorated below translational lift speed, and the pilot initiated a turn to the left. A turn with left pedal input would have placed the relative wind on the left side of the aircraft, where a combination of tail-rotor vortex ring state (210° to 330° relative wind) and main-rotor vortex interference (285° to 315° relative wind) would have reduced tail-rotor effectiveness.
Both of these situations would have resulted in an uncontrolled rotation to the right, and unless the pilot made a substantial reduction in power, rapid rotation would have continued. In close proximity to the terrain, a significant power reduction would not have been possible without the helicopter impacting the steep mountainside at a high rate of descent. The rapid right rotation would have been accompanied by an uncontrolled descent. The helicopter was unable to hover out-of-ground-effect, and rotation would have further reduced this capability.
While the second scenario is considered the more probable reason for loss of tail-rotor effectiveness, it could not be determined conclusively where and when the tail rotor first contacted the ground, due to its severely damaged condition, and because investigators were unable to access the wreckage site. As ground scars associated with the accident were not examined, the possibility of a tail-rotor strike being the initiating event could not be either supported or entirely eliminated. Had the helicopter been fitted with an available crash-protected lightweight flight recording system with cockpit imaging capability, data from the recording system would have allowed superior reconstruction of the flight, permitting a better understanding of the circumstances that led to the accident and confirmation of the reason for the loss of control.
The minimal mountain flying that the pilot received during training and during the pilot competency check (PCC) would not have provided adequate preparation for the challenging situations presented in that environment. In addition, the mentoring provided by riding along with other low-time pilots with limited experience could have instilled wrong perceptions on proper mountain-flying procedures and techniques. These perceptions could have influenced the pilot's decision-making, leading the pilot to place the aircraft in a hazardous situation while not recognizing the hazard. Extraction from the situation was delayed until safe options were not available.
The Transport Canada (TC) post-accident process inspection (PI) of the company in May 2012 revealed deficiencies in pilot training, which existed at the time of the last program validation inspection (PVI) and were active on the day of the accident. This finding resulted in TC inspectors revoking PCC authority and conducting pilot proficiency checks (PPCs) on all company pilots. If adequate surveillance is not maintained by TC , there is an increased risk for operator safety deficiencies to go unidentified.
The helicopter altimeter had not been calibrated within the required calendar time before the flight. While the altimeter was functional following the accident, it was out of calibration by approximately 700 feet low across the full indication range. Although it could not be determined with certainty whether the calibration error predated the flight or whether it resulted from the accident, it is probable that it was a result of the accident. This probability is based on the fact that the displayed altimeter setting was similar to the current altimeter setting at CYBW , and on the presumption that the pilot would have set the altimeter to field elevation before departure. In that case, the altimeter would have been displaying the actual altitude during the flight. If the altimeter was reading 700 feet below actual altitude during the flight, the helicopter would have been 700 feet higher than indicated, which would have provided an increased safety margin. Either way, the out-of-date altimeter calibration was not considered to be a factor in the accident.
The investigation could not determine why the emergency locator transmitter (ELT) did not activate at impact. Action by the surviving passengers to activate the ELT by moving the remote switch to the ON position was instrumental in reducing the time required to locate the wreckage and recover the occupants. Once the ELT was activated, signal detection by the COSPAS-SARSAT system was delayed by terrain influences and satellite geometry. However, the next-generation MEOSAR SARSAT system detected the ELT approximately 1 hour and 29 minutes before the COSPAS-SARSAT system. Until the MEOSAR SARSAT system is operational, protracted search-and-rescue times can place air-accident victims at risk for delayed response.
As flight and voice recorders are not required by regulation to be fitted to commercially operated aircraft of this size, the helicopter was not equipped with a lightweight flight recording system. By not using lightweight flight recording systems, small aircraft commercial operators are less able to effectively monitor flight operations through an internal flight data monitoring program, which precludes proactive identification and correction of safety deficiencies by an operator to reduce accident risk. As well, when flight data from a lightweight flight recording system are not available to an accident investigation, it may preclude the identification and communication of safety deficiencies to advance transportation safety.
Findings
Findings as to causes and contributing factors
- The pilot conducted the tour flight using a route in very close proximity to mountainous terrain, in conditions in which environmental factors resulted in reduced performance margins.
- The visual illusion associated with lack of a true horizon, combined with the illusion of higher-than-actual airspeed, may have resulted in pilot-initiated flight control inputs that further reduced helicopter performance.
- The pilot attempted to cross a mountain ridge at an altitude that did not provide safe terrain clearance, and the pilot did not use the available drop-off zone early enough, which increased the risk of collision with the terrain.
- The helicopter either sustained a tail-rotor strike on terrain or, more likely, entered a condition of aerodynamic loss of tail-rotor effectiveness, resulting in an uncontrolled rotation, loss of control and collision with terrain.
- The pilot had minimal mountain-flying training and experience. As a result, it is likely that the pilot was unable to recognize the hazards associated with flying in mountainous terrain.
- The pilot was not wearing a helmet, which contributed to the level of injury.
- The company's flight-following procedures did not identify that the aircraft had stopped transmitting its satellite tracking position, and that the pilot had not reported landing at Brokenleg Lake. This lack of information delayed initiation of search-and-rescue operations.
Findings as to risk
- By not using lightweight flight recording systems, small aircraft commercial operators are less able to effectively monitor flight operations through an internal flight data monitoring program, which precludes proactive identification and correction of safety deficiencies by an operator to reduce accident risk.
- If adequate surveillance is not maintained by Transport Canada, there is an increased risk that operator safety deficiencies will not be identified.
- The emergency locator transmitter did not activate at impact, and signal detection was delayed due to terrain and satellite geometry. Until improvements in emergency-locator-transmitter detection times arise from inauguration of the developmental MEOSAR SARSAT system, protracted search-and-rescue times can place victims of air accidents at risk for delayed response.
Other Findings
- The aircraft altimeter had not been calibrated within the required 24-month calendar period.
Safety action
Safety action taken
Kanananskis Mountain Helicopters
As a result of this accident, KMH took the following measures to reduce operational risks:
- All KMH pilots are now required to wear helmets while flying.
- Permission is now obtained from KMH pilots at time of hire to inquire into their accident history.
- The KMH pilot-training syllabus has been enhanced to emphasize certain aspects of mountain-flight training.
- Internal KMH indoctrination training forms have been improved.
- A quality assurance program has been put in place to validate that all KMH pilot training has been completed.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on . It was officially released on .