Loss of control – collision with water
Transwest Air Limited Partnership
de Havilland DHC-3 Otter, C-FSGD
Ivanhoe Lake, Northwest Territories, 7 nm S
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
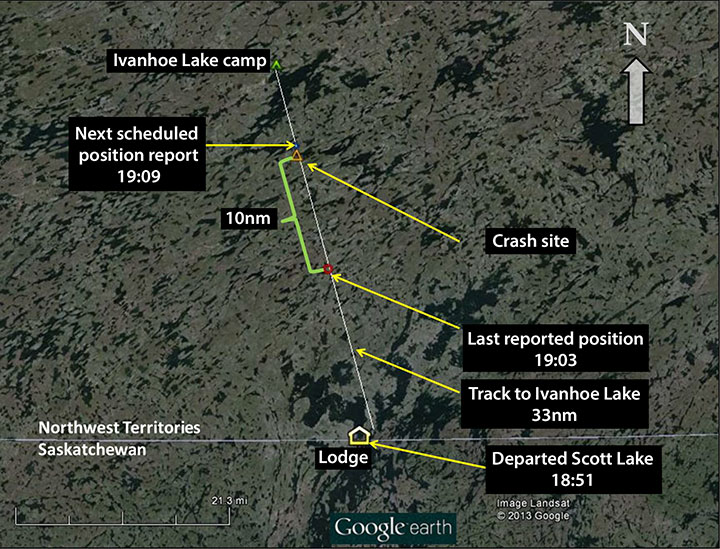
The float-equipped Transwest Air Limited Partnership DHC-3 turbine Otter (registration C-FSGD, serial number 316) departed Scott Lake, Northwest Territories, at approximately 1850 Central Standard Time on a 33-nautical mile, day, visual flight rules flight to Ivanhoe Lake, Northwest Territories. The aircraft did not arrive at its destination, and was reported overdue at approximately 2100. The Joint Rescue Coordination Centre Trenton was notified by the company. There was no emergency locator transmitter signal. A search and rescue C-130 Hercules aircraft was dispatched; the aircraft wreckage was located on 23 August 2013, in an unnamed lake, 10 nautical miles north of the last reported position. The pilot, who was the sole occupant of the aircraft, sustained fatal injuries.
1.0 Factual information
1.1 History of the flight
At approximately 0645Footnote 1 on the day of the occurrence, C-FSGD departed the Transwest Air Limited Partnership (Transwest Air) water base in Stony Rapids, Saskatchewan. The itinerary for the day was for approximately 15 flights and included a series of fly-out trips to various outpost camps for a lodge on Scott Lake, Northwest Territories.
The aircraft departed Stony Rapids for the final time at 1637 en route to Desmarais Lake, Northwest Territories, and Sandy Lake, Northwest Territories, to pick up guests and guides and return them to Scott Lake.
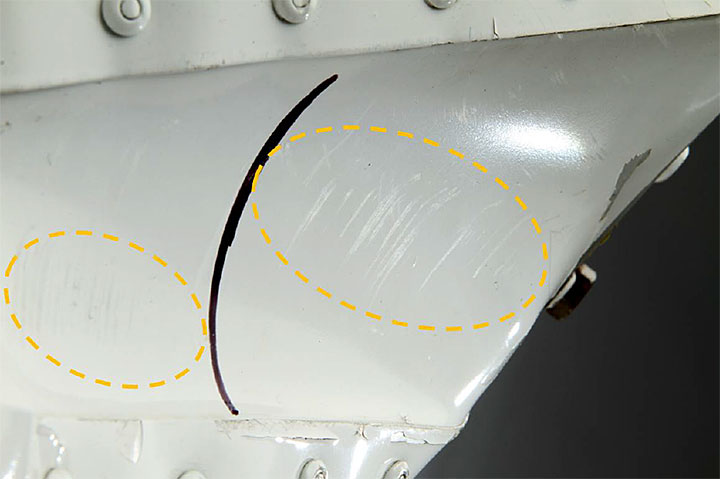
During the approach to land at Scott Lake, the aircraft made a low-altitude turn to the right around the south end of an island onto the final approach toward the lodge. While in a right bank, the right wing tip struck a stand of trees on the point of the island. There was a loud bang, and the aircraft swung to the right. The pilot maintained control and touched down on the water several seconds later. After taxiing to the lodge, the pilot made 2 attempts to dock, after which the pilot brusquely ordered a passenger to vacate the right seat. The pilot then moved from the left seat into the right seat and docked the aircraft with the right wing over the dock. Damage to the right-wing leading edge and fibreglass wing tip was evident and was pointed out to the pilot, but the comment was dismissed (Photo 1). When the unloading was complete, the pilot immediately called for the lines to be cast off, and taxied away from the dock.

The aircraft, with only the pilot on board, departed for Ivanhoe Lake, Northwest Territories at 1850. The take-off appeared normal, and the aircraft was observed climbing to the north. The aircraft was expected back at Scott Lake by 2030. Shortly before the aircraft was due to return, the lodge manager contacted Transwest Air flight-following personnel in Stony Rapids and requested a position report. The aircraft was equipped with a tracking device that sends automated position information on a programmed schedule. After several calls, it was apparent that the flight tracking system had not received any position reports after the 1903 uplink. When the aircraft was 30 minutes overdue, it was reported to Transwest Air, and the overdue aircraft emergency response, as detailed in Transwest Air's Emergency Response Manual (ERM), was initiated. This included a call to the Joint Rescue Coordination Centre (JRCC) Trenton at 2215.
There was no emergency locator transmitter (ELT) signal from the aircraft. The C-130 Hercules tasked by the JRCC commenced a search pattern toward Ivanhoe Lake from the last reported position. The wreckage was discovered on 23 August 2013 at 0526 on track between Scott Lake and Ivanhoe Lake, 10 nautical miles (nm) north of the last position report in the 1903 data package (Figure 1).
1.2 Injuries to persons
The pilot, who was the sole occupant of the aircraft, was fatally injured.
1.3 Damage to aircraft
The aircraft was destroyed due to impact with water.
1.4 Other damage
The aircraft contained an unknown quantity of Jet A fuel, which was released into the lake. Damage sustained by the airframe and engine resulted in the release of some hydraulic fluid and engine oil into the lake.
1.5 Personnel information
1.5.1 Pilot-in-command
The pilot held a Canadian commercial pilot licence and was certified for single and multi-engine aircraft land and seaplane operations. The pilot held a valid category 1 medical certificate. The pilot had accumulated approximately 1600 total flight hours, of which 248 were on the DHC-3 turbine Otter aircraft, and was qualified to act as pilot-in-command (PIC) of C-FSGD on the day of the occurrence.
The training for pilots employed by Transwest Air included pilot decision making (PDM) and crew resource management (CRM). Testing on Transwest Air's Flight Operations Manual was also included.
The pilot had recently transitioned onto the DHC-3 turbine Otter from the DHC-2 Beaver. The Otter is a physically demanding aircraft to fly and to control on the water in strong wind and currents. It can carry a larger load than the Beaver, and pilots are sometimes left to unload the aircraft on their own. During the previous year, the pilot had flown the Beaver in support of the same lodge and was familiar with the area. The pilot was characterized as capable, careful, and reluctant to take unnecessary risks.
The pilot had returned to work on 21 August after 5 days of leave and had slept approximately 6.5 hours in each of the 2 nights that preceded the crash. On the evening prior to the accident, the pilot and several others socialized at the Transwest crew house in Stony Rapids. The pilot shared a meal with a fellow pilot and then went to bed at approximately 2330. The following morning, both pilots experienced stomach cramps and were feeling unwell.
Transwest's policy provides that if pilots feel unfit to fly due to illness, they are expected to contact the base manager, chief pilot or director of flight operations and remove themselves from flight duty. The pilot would still be paid for a sick day. There is no indication that the occurrence pilot attempted to call in sick.
The pilot had been encountering operational problems throughout the day of the accident. The wind was making it difficult to manoeuvre the aircraft to the various docks and unloading points. On one of the flights, a water rudder was damaged. The water rudder was repaired at Stony Rapids prior to a flight to Pinkham Lake, Northwest Territories. On arrival at Pinkham Lake, the pilot made approximately 8 attempts to manoeuvre to the unloading spot. Later in the day, while trying to depart Desmarais Lake, the aircraft became stuck near the beach, and the pilot had to use substantial power several times to free the aircraft from sandbars.
While at Stony Rapids for maintenance, the pilot complained of an upset stomach. The pilot turned down offers of some lunch and ate a few crackers instead. Although normally described as happy and relaxed, throughout the day of the accident, the pilot had appeared increasingly agitated, withdrawn and short-tempered.
1.5.2 Flight duty time
The Canadian Aviation Regulations (CARs) specify flight time limitationsFootnote 2 that flight crew must observe. The pilot had returned to work on 21 August after a 5-day leave. A review of the pilot's accumulated flight time showed that it was within the allowable limits. The CARs also limit flight duty timeFootnote 3 to 14 consecutive hours in any 24-hour period.Footnote 4 If, during those 14 consecutive hours, the flight duty time includes a rest period of at least 4 hours, the maximum flight duty time can be extended by an amount equal to one-half the duration of the rest period.
The day before, the pilot was on duty for 14.6 hours and flew approximately 6.5 hours. Between 1206 and 1636, the pilot was able to observe a rest period. As a result of the rest period, the allowable flight duty time would have been 16 hours. That night, the pilot went to bed at approximately 2330. The next morning, the pilot commenced flight duties and was airborne at 0647. At most, the pilot obtained 6.5 hours of sleep.
| Depart | Time | Arrive | Time |
|---|---|---|---|
| Stony Rapids (base) | 6:47 | Scott Lake Lodge | 7:17 |
| Scott Lake Lodge | 8:06 | Desmarais Lake | 8:30 |
| Desmarais Lake | 8:57 | Sandy Lake | 9:09 |
| Sandy Lake | 9:35 | Scott Lake Lodge | 10:05 |
| Scott Lake Lodge | 10:33 | Ivanhoe Lake | 10:57 |
| Ivanhoe Lake | 11:12 | Gardiner Lake | 11:24 |
| Gardiner Lake | 11:49 | Stony Rapids (base) | 12:37 |
| Stony Rapids (base) | 13:30 | Pinkham Lake | 14:06 |
| Pinkham Lake | 14:50 | Stony Rapids (base) | 15:26 |
| Stony Rapids (base) | 16:37 | Desmarais Lake | 17:19 |
| Desmarais Lake | 17:31 | Sandy Lake | 17:37 |
| Sandy Lake | 18:01 | Scott Lake Lodge | 18:37 |
| Scott Lake Lodge | 18:51 | Accident site | 19:08 |
At the time of the crash, the pilot had been on duty for almost 12 hours and was on the 13th flight of 15 that were planned for the day. Approximately 7 hours of flight time were accumulated during this time. Except for 2 brief periods at Stony Rapids throughout the day, the flying duties had been continuous and did not include a rest period (Table 1). In the afternoon, lodge personnel had suggested to Transwest Air operations personnel that the pilot could spend the night at the lodge at Scott Lake. After doing a fly-out trip in the morning, the aircraft could return to Stony Rapids. Although this was approved, the pilot turned down this offer and was intent on returning to Stony Rapids that night after the Ivanhoe Lake trip. The planned last leg back to the waterdrome at Stony Rapids had to be completed under day visual flight rules (VFR) before the end of civil twilight at 2119. The investigation did not determine the reason why the pilot was intent on returning to Stony Rapids.
1.6 Aircraft information
1.6.1 General
The aircraft was manufactured in 1959. In 1997, the originally-fitted radial engine was replaced with a Pratt & Whitney PT6-135A turbine engine in accordance with Supplemental Type Certificate (STC) SA89-32. The take-off and maximum continuous torque rating of the PT6-135A is 59.1 pounds per square inch (psi) (2080 foot-pounds). The wing leading edges and wing tips were modified in 2002 by the incorporation of a short take-off and landing (STOL) kit, in accordance with STC SA94-114. At the same time, the gross weight of the aircraft was also increased by 400 pounds to 8367 pounds with the incorporation of STC SA95-32.
The STOL kit modified the wing by installing cuffed leading edges over the original leading edge skins. The original wing tips were removed and replaced by drooped wing tips made of fiberglass.
A feature of the Otter is the incorporation of the ailerons into the full-span flap system. As the flaps deploy, the ailerons droop down and move aft past the wing tip. The flap system utilizes push-pull tubes connected to bellcranks and links driven by a hydraulic cylinder located in the fuselage. Extension of the hydraulic cylinder pulls the tubes inboard and deploys the flaps.
Records indicate that the aircraft was certified, equipped and maintained in accordance with existing regulations and approved procedures. The Transwest Air Operator Certificate approved the operation of C-FSGD under day VFR only.
1.6.2 Weight and balance
On the flight to Ivanhoe Lake, the aircraft was not carrying any payload. Using data from load control forms for a similar configuration from the previous day, TSB investigators calculated that the centre of gravity was likely close to, but within, the seaplane forward limit.
1.7 Meteorological information
There are no routine weather observations at Ivanhoe Lake. The nearest weather observation was recorded by an automatic weather observation system (AWOS) at Stony Rapids, 72 nm southeast of the accident site. The 2000 weather for Stony Rapids was recorded as: wind 270° True (T) at 8 knots; visibility 9 statute miles (sm); sky clear; temperature 19°C. Earlier in the day, the wind had been from a southwesterly direction and gusting as high as 23 knots. Light mechanical turbulence had been forecast for the area north of Ivanhoe Lake. At Scott Lake and Stony Rapids, civil twilight ended at 2125 and 2119, respectively.
1.8 Aids to navigation
The accident flight was a VFR flight in visual meteorological conditions (VMC). It is probable that the pilot was using a handheld global positioning system (GPS) mounted in a holder to assist navigation to the remote camp on Ivanhoe Lake.
1.9 Communications
There was no record of any communications with the aircraft following the take-off from Scott Lake.
Most Transwest Air aircraft dedicated to serving the lodge are equipped with a frequency modulation (FM) radio to enable communication with the lodge. However, due to the temporary assignment of C-FSGD for this series of flights, it was not equipped with an FM radio, and lodge personnel were unable to contact the aircraft once it moved away from the dock.
1.10 Aerodrome information
Not applicable.
1.11 Flight recorders
The aircraft was not equipped with a flight data recorder (FDR) or a cockpit voice recorder (CVR), nor was either required by regulation.
Given the combined accident statistics for operations under CARs subparts 702, 703, and 704, the TSB has previously stated that there is a compelling case for industry and the regulator to proactively identify hazards and manage the risks inherent to these operations.
| Commercial Air Services category | Accidents | Fatal injuries |
|---|---|---|
| 702 − Aerial Work | 245 | 51 |
| 703 − Air Taxi Operations | 485 | 176 |
| 704 − Commuter Operations | 47 | 29 |
| Total | 777 | 256 |
In order to manage risk effectively, they need to know why incidents happen and what the contributing safety deficiencies may be. Moreover, routine monitoring of normal operations can help these operators both improve the efficiency of their operations and identify safety deficiencies before they result in an accident. In the event that an accident does occur, recordings from lightweight flight recording systems will provide useful information to enhance the identification of safety deficiencies in the investigation. Based on this, the TSB recommended that:
The Department of Transport work with industry to remove obstacles and develop recommended practices for the implementation of flight data monitoring and the installation of lightweight flight recording systems by commercial operators not currently required to carry these systems.
Transportation Safety Recommendation A13-01
On 02 April 2014, the TSB issued the following Board Assessment of Response to A13-01:Footnote 5
The Board [TSB] notes Transport Canada's commitment to proceed with the development of an Advisory Circular and to consider adding FDM principles in future regulatory initiatives/amendments. However, TC is silent on the issues of removing obstacles around the installation of lightweight flight data recording systems. Further, TC has not indicated how it will work with industry on these issues.
Given the paucity of information received from TC, the Board is Unable to Assess TC's response.
To assist the company in performing flight following, Transwest Air aircraft are equipped with a flight tracking unit that provides periodic position reports via satellite. This information is accessed by Transwest Air flight-following personnel via a web-based utility. The upload frequency of the reports is determined by the operator of the aircraft as part of the subscription agreement. In this case, the system recorded the aircraft's position every 2 minutes and transferred the data (3 position reports) every 6 minutes. The last data package was transmitted at 1903, and indicated that the aircraft was at 1000 feet above ground level (agl) and at a normal cruising airspeed of approximately 110 knots. TSB investigators estimated that the crash occurred less than 1 minute before the next data package was due to be transmitted at 1909. In the absence of an ELT signal, the data available from the flight tracking website was the best information on which to base the search plan.
1.12 Wreckage and impact information
The site of the initial tree strike at Scott Lake was examined. Four closely grouped trees near the water's edge had been severed at a point approximately 12 feet from the ground. Each of the tree trunks were approximately 2 to 3 inches in diameter. Blue paint and fibreglass chips were embedded in one trunk.
At the crash site, the aircraft wreckage was located in a shallow lake, submerged in approximately 6 feet of water (Photo 2). The lake bottom consisted of deep mud and silt. Depressions in the mud indicated that the aircraft had impacted almost vertically and that the floats and left wing impacted first. All major components were located within an area not much larger than the aircraft itself. The left and right wings were separated from the fuselage, although they remained connected to each other by the rear-spar fuselage carry-through structure (hoop). The fuselage was broken into several major pieces.

The engine and cockpit were located to the right of the fuselage and submerged in mud up to the first row of cabin windows. The propeller and reduction gearbox had separated from the engine at the B flange and were not recovered. The exhaust duct portion of the engine was bent and compressed hydraulically almost 90 degrees to the right. The output spline portion of the first-stage reduction-gear planetary carrier had failed due to torsion loads. Several engine instruments and lamps were recovered.
The ELT was recovered, and had suffered impact damage. A handheld GPS and a flight track reporting unit were also recovered.
All of the flight control cables were examined; all discontinuities were due to overload failures or cuts made during the wreckage recovery. The left side of the horizontal stabilizer was broken outboard of the fairing. The flaps, ailerons and elevators were bent or broken in half. The control surface and horizontal stabilizer fracture surfaces were overload in nature. The right aileron mass balance was trapped within the crushed fore-flap cavity and there was off-axis scrubbing of the mass-balance against the sides of the cavity. The right, outboard aileron hinge bracket on the fore flap was worn from uneven side-load contact with the aileron hinge. The flap actuator was in the UP position. The flap actuating tubes had failed in overload due to tension forces developed when the wings broke away. These forces had partially, and unevenly, deployed the flaps. The ailerons and fore-flaps were compressed together such that the ailerons were positioned to produce a roll to the left. The control column was bent and collapsed. The aileron chains and cables were trapped inside the collapsed column, locking both control wheels, which were fully rotated to the left.
The outboard rib of the right aileron displayed a chord-wise dent (Photo 3) coincident with blue paint transfer as well as marks scratched into the paint in an arc from the hinge point (Photo 4). Blue paint had also transferred from the wing tip to the adjacent fore flap, hinge hanger and the top skin of the aileron. The left-wing aileron and flap components did not exhibit any paint transfer. The wreckage was recovered to shore before being transported to Stony Rapids. TSB investigators examined the wreckage at the crash site and in Stony Rapids as well as at the final storage site in Prince Albert, Saskatchewan. Selected items were sent to the TSB Laboratory for further examination.

1.13 Medical and pathological information
Autopsy and toxicological tests did not detect the presence of drugs or indicate the consumption of alcohol, and did not identify any underlying physiological factors.
1.14 Fire
There was no in-flight or post-impact fire.
1.15 Survival aspects
The nature of the crash was such that the forces generated by the impact with the water surface were not survivable.
1.16 Tests and research
A number of tests were conducted at the TSB Laboratory. Fuselage-former fracture surfaces revealed a small area of fatigue and an overstress fracture. The fatigue was relatively short and pre-dated the impact with water. The overstress fracture was not exactly in line with the fatigue crack.
A microscopic examination of the engine torque indicator dial face revealed several white marks that were determined to be paint that had been transferred from the instrument's pointer at impact. Aligning the pointer with these marks provided an indication of approximately 40 psi. Information from the engine manufacturer suggests that 40 psi is equivalent to 1409 foot-pounds of torque or approximately 68% of take-off, or maximum continuous, torque.
Lamp filament analysis indicated that the stall warning annunciator was not illuminated at the moment of impact.
The flight track reporting unit was examined by the manufacturer under the supervision of the TSB. Although position reports were being transmitted periodically, the unit was also recording position, altitude, heading and ground speed data every 10 seconds. The data was retained in non-volatile memory. The data covered the entire flight and consisted of 108 data points. The initial climb and cruise portion of the flight was unremarkable. The aircraft was cruising at about 1000 feet agl. At data point (DP) 93, the aircraft's altitude began to decrease by about 250 feet before recovering slightly by DP 105. From DP 107, the aircraft descended 430 feet in 10 seconds to DP 108, which would have required a rate of descent of over 2500 feet per minute (fpm).
DP 108 was about 275 feet south of the crash site at approximately 610 feet agl. The direct descent angle and distance from DP 108 to the crash site was 66 degrees and 670 feet, respectively. Taking the spacing between previous DPs into account, it was calculated that a direct descent from DP 108 to the crash site would have taken about 4 seconds and would have required a descent rate of roughly 10 000 fpm.
However, the data did not indicate whether the aircraft descended directly to the crash site or performed some form of manoeuvre during descent. Since the crash occurred before the next DP could be recorded, the final descent occurred in less than 10 seconds. Therefore, although the exact track could not be calculated, the rate of descent from DP 108 to the crash site, using 10 seconds, would have required a descent rate of 3650 fpm.
The following TSB Laboratory reports were completed and are available on request:
- LP 231/2013 – Examination of Wing Components
- LP 171/2013 – Instrument, Annunciator and NVM Analysis
1.17 Organizational and management information
1.17.1 Safety management systems
The TSB has recognized that, implemented properly, a safety management system (SMS) allows aviation companies to identify hazards, manage risks, and develop and follow effective safety processes.
The aircraft was being operated in accordance with CARs subsection 703; however, Transwest Air is also a CARs subsection 705 operator and has an SMS in place. Subsection 2.4.6, item 5, of the Transwest Safety Management Program Manual requires line personnel to “[b]e accountable by reporting any hazards, incidents and accidents to the Manager, Safety & Quality Systems and/or Safety Officer (or Line Manager when applicable).”
Transwest Air has a non-punitive reporting policy. Disciplinary actions may be taken under several conditions, such as wilful negligence or violation of the CARs, criminal intent or use of illicit substances. Actions taken by the company can range from a verbal warning or letter to a monetary fine or termination.
Safety information generated by the SMS is distributed to employees by various means such as Safety Directives (SD), safety meetings, bulletin boards and incident summary binders as well as verbally. SDs can also be accessed from the employee area of Transwest Air's website.
The indoctrination program for new Transwest Air employees includes training on the SMS. Employees also undergo annual recurrent training. A review of several incident reports indicates that, this occurrence notwithstanding, employees are reporting hazards, incidents and accidents as intended by the SMS.
1.17.2 Transwest Air dispatch system
The Flight Operations Manual (FOM), Section 4.2.1, indicates that flight authorization for operations originating from Transwest Air bases, such as La Ronge and Stony Rapids, is delegated to the base manager. The Director of Flight Operations delegates operational control of each flight to the PIC; however, the Director retains responsibility for the day-to-day conduct of flight operations. This type of operational control system is known as pilot self-dispatch.Footnote 6
Section 4.2.1 of the FOM states:
A flight release will deem to have been given when the PIC has determined that:
- the flight can be conducted in compliance with the company Air Operator Certificate and Operations Specifications, the company Flight Operations Manual and the Canadian Aviation Regulations and Standards;
- all required licenses, permits, certificates are valid;
- the aircraft is airworthy:
- all required aircraft maintenance work has been completed;
- a technical dispatch authority has been issued; and
- sufficient flight time to complete the intended flight remains before the next required maintenance.
The itinerary can be modified throughout the day according to changing conditions or customer requirements. Itinerary revisions are communicated to the crews by various means such as satellite phone and VHF (very high frequency) or FM (frequency modulating) radio as well as through air traffic control or flight service stations facilities. Email and cell phone communications are also available at some locations.
The following excerpt from the FOM, Section 4.2.1, refers to the PIC's authority in such cases:
If a new requirement for a flight develops while operating away from base, the PIC is authorized to release the aircraft subject to the following conditions:
- the requirement for the new flight must be reviewed with the Director of Flight Operations or his delegate unless the PIC has been delegated by the Director of Flight Operations to assess the requirement; and
- the conditions of the flight release have been fulfilled.
The pilot self-dispatch system delegates sole responsibility for flight watch to the PIC. To facilitate this, the PIC must communicate pertinent details of the flight to the dispatcher/flight follower. If flight-following is not available at the point of departure, this information may be left with a responsible person. The PIC is responsible to provide flight-following personnel with departures and arrivals via any available means of communication. The dispatcher/flight follower shall confirm that all flights have reached their destinations.Footnote 7 The flight tracking system installed in Transwest Air aircraft enables flight-following personnel to query a particular aircraft's location via a web-based utility on an ad-hoc basis or, as was the case in this accident, prompted by the lodge manager's report of a deviation from the flight information provided by the PIC.
1.18 Additional information
1.18.1 Decision making
Pilots in remote self-dispatch operations are at risk to commit plan continuation errorsFootnote 8 due to factors that influence them toward unsafe behaviour (goal seduction) and away from safe behaviour (situation aversion).Footnote 9 These factors can include organizational, situational, social and psychological pressures.Footnote 10 A pilot must systematically consider complete information on those factors in order to maintain awareness of the positive and negative aspects of decision alternatives. Pilots are trained to use mnemonics (memory aids) to identify hazards, assess personal fitness, and manage associated risks during preflight planning and inflight decision making. For example, mnemonics discussed during Human Factors training at Transwest Air include PAVE (Pilot-in-command, Aircraft, EnVironment, External pressures) and IMSAFE (Illness, Medication, Stress, Alcohol, Fatigue, Emotion). PAVE is designed to help pilots make safe decisions through systematic or deliberative processingFootnote 11 of all relevant information, and avoid using heuristic information-processing strategies that may yield unsafe and error-prone decisions. IMSAFE is designed to enable pilots to determine their physical and mental readiness for flying and provide an overall assessment of their well being.Footnote 12 Systematic use of mnemonics aside, pilots also have a regulatory obligation to ground themselves when suffering from an illness, injury or disability.Footnote 13
These mnemonics are designed to help pilots make safe decisions through self evaluation and systematic processingFootnote 14 of all relevant information. Human decision making is not naturally based on considering all factors and all possible outcomes, but rather on assessing what has been successful in similar situations. Pilots may also use mnemonics in order to avoid using error-prone heuristic,Footnote 15 information-processing strategies.
Systematic processing is careful and complete, although mentally challenging. Heuristic processing involves shortcuts to reduce mental workload. It is usually applied to incomplete information, and is subject to numerous biases. When performance-affecting factors such as fatigue, illness, stress, time pressure and heavy workload are present and mnemonics are not used, there is a greater likelihood that poor heuristic decisions will be made.
The TSB has investigated several single-pilot self-dispatch air taxi operations where pilot decision making was a factor, and has identified the need for improved risk mitigation strategies such as decision-making training, mnemonics, and management of customer pressure.Footnote 16
1.18.2 Fatigue
The consumption of a hard-to-digest meal within 2 hours of sleeping and possible onset of upset stomach and cramps during sleep may cause a disruption of sleep quality. The normal sleep requirement to avoid sleep debt (fatigue) is an hour of sleep for every 2 hours awake, calculated from the start of a prior sleep period over a cycle of at least 2 or 3 periods prior. Calculations applied to the pilot's prior duty day and 2 sleep periods of approximately 6.5 hours each indicate a sleep debt of approximately 2 hours. This amount of sleep debt would not necessarily be sufficient to cause performance decrements in the absence of other factors. However, illness such as gastric upset and cramps will disrupt sleep and reduce its restorative function, increasing the acute sleep debt. Fatigue reduces a person's problem-solving ability, making it difficult to revise an ongoing planFootnote 17, and is associated with angerFootnote 18 and risky decision making.Footnote 19
1.18.3 Stress
The response to stress has 3 stages: alarm, adaptation, and exhaustion. After the initial alarm, stability is maintained in the continuing presence of stressors through the expenditure of adaptation energy. Depletion of this finite resource eventually leads to exhaustion and the loss of adaptability.Footnote 20
As adaptive resources are used up, stressed individuals tend to switch from systematic processing to more error-prone heuristic processing of information.Footnote 21, Footnote 22
Stressors affect decision-making and risk management in several ways. Illness reduces overall pilot performance and safetyFootnote 23 and may reduce the capacity to adapt to other stressors and make appropriate decisions.
1.18.4 Workload
Decision-making under time pressure and heavy workload is characterized by the use of mental shortcuts (i.e., heuristics) in information processing, and reduced levels of mental effort.Footnote 24
Time pressure increases the likelihood of risky decision making.Footnote 25 Long periods of continuous time-pressured decision making may actually lead to depletion of cognitive resources.Footnote 26, Footnote 27 Individuals become particularly stressed when they realize that they have insufficient time to meet a deadline.Footnote 28 In addition, time pressure amplifies anger associated with delay, and that anger tends to persist.Footnote 29 Anger increases the likelihood of risky, heuristic decision making,Footnote 30, Footnote 31, Footnote 32 in part because anger gives rise to more optimistic risk assessments and higher-risk choices.Footnote 33
1.19 Useful or effective investigation techniques
The data retained in the on-board component of the position reporting system enabled a reconstruction of the accident flight in 10 second intervals. Altitude, heading, groundspeed and position data was then transposed onto Google Earth to create a representation of the flight profile.
2.0 Analysis
2.1 General
The pilot was certified and experienced for the flight and was familiar with the area of operation. The aircraft was maintained and equipped in accordance with existing regulations. Examination of the torque indicator and damage sustained by the engine indicates that the engine was operating and producing power at the moment of impact with the water. The aircraft was operating within acceptable centre of gravity limits, and there were no un-actioned defects reported prior to the landing at Scott Lake, Northwest Territories. Examination of the wreckage did not reveal any defects that pre-dated the tree strike at Scott Lake.
The recovered flight track data indicates a relatively normal flight profile until altitude fluctuations begin to appear after DP 93 and progress to an increasingly rapid rate of descent after DP 107. These factors, when combined with the nature of the impact with the water, indicate that the aircraft had departed controlled flight.
Because the emergency locator transmitter (ELT) did not activate, the aircraft was located by searching along the aircraft's track from the last reported position. Although the sample rate and up-link interval configured into the flight tracking system increased the possible search area, the crash site was located relatively quickly because the aircraft was on track to the destination.
The analysis will discuss possible scenarios, the pilot's decision-making process and the significance of the tree strike at Scott Lake.
2.2 Possible scenarios ruled out
2.2.1 Incapacitation
Pilot incapacitation was considered. The flight was relatively short, and the aircraft had only been airborne for about 17 minutes. The Otter is a noisy aircraft that has to be hand flown. Light turbulence was forecast en-route and the pilot would be preparing to make the descent and approach to Ivanhoe Lake, Northwest Territories. The pilot was likely feeling stress and mounting frustration after the tree strike. It is unlikely, therefore, that the loss of control was due to the pilot falling asleep. Autopsy and toxicological results do not indicate that the pilot's performance was degraded by pre-existing medical or physiological factors; as a result, incapacitation was considered unlikely.
2.2.2 Precautionary landing
The possibility that the pilot was attempting a precautionary landing was considered. The flap actuator was in the UP position, which indicates that the aircraft was not configured for a landing. The crash scenario is not consistent with an upset on the water resulting from a failed landing attempt.
2.3 Decision making
Pilot decision making may be affected by factors such as fatigue, illness, stress, time pressure and heavy workload. When these factors are present and mnemonics are not used, there is an increased likelihood that unsafe decisions will be made. The 2-hour sleep reduction and poor quality sleep due to stomach upset would have resulted in an acute sleep debt and fatigue. The pilot had not been feeling well earlier that day.
The pilot had been on duty for about 12 hours and had accumulated approximately 7 hours of flight time while flying 13 of 15 planned flights. The pilot had experienced a number of stressors as the day progressed. The weather conditions were acceptable; however, the difficulty taxiing the aircraft in the gusty wind conditions caused heavy workload and further stress. The pilot was appearing increasingly withdrawn and agitated throughout the day. The pilot was determined to return the guests and guides to Scott Lake and finish the day at Stony Rapids, Saskatchewan.
The delays caused by the difficulties in docking and getting stuck were incrementally increasing the time pressure to return to Stony Rapids before the end of civil twilight. These cumulative stressors were conducive to risky decision making, as indicated by the unusual approach for the landing at Scott Lake. The approach path chosen would likely have limited the exposure to crosswinds while taxiing the aircraft to the dock. However, the resultant tree strike probably increased the pilot's level of stress, anger and frustration, as indicated by the uncharacteristic manner in which the pilot ordered the guest to vacate the right seat while attempting to dock.
A number of situations occurred during the day that were potential stressors, and while these may not necessarily cause unmanageable stress, the pilot's reactions to them demonstrates that he was progressively less able to cope with them. A number of factors were present that would have reduced the pilot's ability to cope with the stressors and also to make safe decisions. Specifically, the pilot's fatigue, in combination with illness, anger, heavy workload, time pressure, and the tree strike, reduced the resources available to gather and systematically process safety-critical information, resulting in a decision to depart with a damaged, uninspected aircraft.
2.4 Tree strike
The pilot was aware that the wing had struck the stand of trees and with only a cursory glance at the wing, may have decided that the damage was minor in nature. A detailed inspection by a qualified person, as required by company policy, would have been required to determine the full extent of the damage to the wing, wing tip and wing attachment points. The impact with the water obliterated the damage caused by the tree strike, and this complicated the differentiation of damage caused by the 2 events.
2.4.1 Effects of the tree strike
When the aircraft departed Scott Lake, it was seen to take off and climb normally. Flight tracking unit data indicates that the climb and cruise portions of the flight were initially normal. It is therefore unlikely that aerodynamic effects of the distorted wing leading edge resulting from the tree strike caused a loss of control.
Aileron flutter induced by the disturbed airflow over the distorted wing leading edge was considered. The hinge points and control rods displayed no signs of pre-existing looseness. The aircraft was being operated within allowable airspeed parameters. All of the flight controls were accounted for at the crash site, and were found in roughly the correct orientation. Damage to the elevators and some off-axis scrubbing of the right aileron mass balance horn indicates that the aircraft had likely begun to break up before the impact with the water. There was no indication however that the ailerons had been damaged by a flutter event. The departure from controlled flight likely preceded any subsequent damage to the flight control surfaces.
The energy absorbed by the wing as it struck the trees at Scott Lake initiated a swing, or yaw, to the right. The force applied at the wing tip would have been multiplied at the point where the rear wing spar is connected to the fuselage. The short fatigue crack in an aft-spar fuselage former indicates that some damage was sustained when the wing struck the trees. The final overstress failure of the fuselage formers was not in line with the fatigue crack, however, and indicates that the subsequent in-flight failure of the aft wing-attachment point was unlikely.
The wing tip was damaged during the tree strike at Scott Lake. On the subsequent flight, the aircraft flew for approximately 17 minutes and indicates that the factors that led to the apparent loss of control took a period of time to develop. The broken edges of the fibreglass wing tip would have been exposed to the airstream. The wing tip was also subjected to a rise in internal pressure due to ram air entering through the breaks in the fibreglass. The wing tip was likely breaking apart under the combination of these forces. The chord-wise dent and scratch marks on the outboard aileron rib as well as the transfer of blue paint from the wing tip to adjacent aileron components indicates that parts of the wing tip were being pressed against the aileron in flight. Air loads may have forced the remaining aft portions of the wing tip under, or over, the aileron. The blue paint transfer to the top surface of the aileron skin indicates that some wing tip parts moved over the aileron.
When the aircraft struck the trees at Scott Lake the flaps were down and when the wings broke away during the crash the flaps were pulled toward deployment. The only time that the chord-wise blue paint transfer line and dent in the aileron rib would have been aligned with the wing tip was in flight, with the flaps up, and ailerons nearly neutral.
It is likely that parts of the failing wing tip, acting under air load, interfered with the right hand aileron. The degree of interference could not be conclusively established but it likely would have been sufficient to affect the pilot's ability to control the aircraft. The uneven, side-loaded wear at the outboard aileron hinge and off-axis scrubbing of the mass balance indicate that the right aileron had likely begun to twist and oscillate over its full travel prior to the impact with the water. It is not known whether the twisting was caused by air-loads that developed after the loss of control or by attempts by the pilot to free the aileron.
3.0 Findings
3.1 Findings as to causes and contributing factors
- During approach to landing on the previous flight, the right-wing leading-edge and wing tip were damaged by impact with several trees.
- The damage to the aircraft was not evaluated or inspected by qualified personnel prior to take-off.
- Cumulative unmanaged stressors disrupted the pilot's processing of safety-critical information, and likely contributed to an unsafe decision to depart with a damaged, uninspected aircraft.
- The aircraft was operated in a damaged condition and departed controlled flight likely due to interference between parts of the failing wing tip, acting under air loads, and the right aileron.
3.2 Findings as to risk
Not applicable.
3.3 Other findings
- The emergency locator transmitter did not activate, due to crash damage and submersion in water.
- The aircraft was not fitted with FM radio equipment that is usually carried by aircraft servicing the lodge. Lodge personnel did not have a means to contact the pilot once the aircraft moved away from the dock.
4.0 Safety action
4.1 Safety action taken
4.1.1 Transwest Air
On 30 September 2013, Transwest Air Safety Directive issued SD13-10 (Appendix A), which was circulated to all employees. The directive expands on Transwest Air 's expectation of compliance with section 605.06 of the Canadian Aviation Regulations (CARs).
In October 2013, pilot meetings were held at each of Transwest Air's bases. A portion of a discussion on human factors concerned Transwest Air's expectations with respect to pilots' responsibility to remove themselves from flight duty if they do not feel fit to fly. The following excerpt is from the minutes of one of those meetings.
- Flight crews reminded that if they do not feel fit to fly, they are to call dispatch and/or [Chief Pilot or Director of Flight Operations] and remove themselves from flight duty.
- Reasons for you to not feel “fit” to fly and being unable to focus on safety and the task at hand may include, but are not limited to:
- Going through personal difficulties such as separation, divorce, financial difficulties
- Feeling physically ill due to cold/flu, food poisoning, being “hung over”
- Being emotionally distraught due to an illness or death of someone close to you
- Being too exhausted to fly
- Transwest Air will still pay you for sick days. You will not be financially penalized for being sick and/or being unavailable to fly. We will either find another pilot to complete the flight or cancel the flight. Safety is our first priority.
Everyone was reminded that we have short-term and long-term disability benefits available.Footnote 34
On 10 October 2014, Transwest Air issued SD13-10 Revised (Appendix B), and it was circulated to all employees. The directive expands on Transwest Air 's expectation of compliance with CARs subsection 605.03(1).
This report concludes the Transportation Safety Board's investigation into this occurrence. the Board authorized the release of this report on . It was officially released on .