Controlled flight into terrain
7506406 Canada Inc.
Sikorsky S-76A (helicopter), C-GIMY
Moosonee, Ontario
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
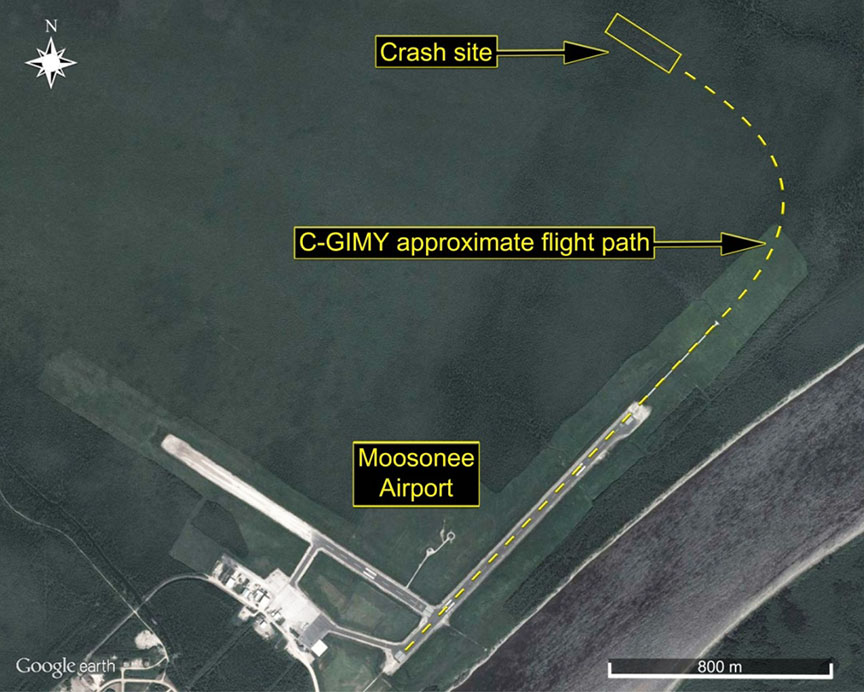
On 31 May 2013, at approximately 0011 Eastern Daylight Time, the Sikorsky S-76A helicopter (registration C-GIMY, serial number 760055), operated as Lifeflight 8, departed at night from Runway 06 at the Moosonee Airport, Ontario, on a visual flight rules flight to the Attawapiskat Airport, Ontario, with 2 pilots and 2 paramedics on board. As the helicopter climbed through 300 feet above the ground toward its planned cruising altitude of 1000 feet above sea level, the pilot flying commenced a left-hand turn toward the Attawapiskat Airport, approximately 119 nautical miles to the northwest of the Moosonee Airport. Twenty-three seconds later, the helicopter impacted trees and then struck the ground in an area of dense bush and swampy terrain. The aircraft was destroyed by impact forces and the ensuing post-crash fire. The helicopter’s satellite tracking system reported a takeoff message and then went inactive. The search-and-rescue satellite system did not detect a signal from the emergency locator transmitter. At approximately 0543, a search-and-rescue aircraft located the crash site approximately 1 nautical mile northeast of Runway 06, and deployed search-and-rescue technicians. However, there were no survivors.
1.0 Factual information
The International Civil Aviation Organization’s (ICAO’s) Annex 13 requires states conducting accident investigations to protect cockpit voice recordings.Footnote 1 Canada complies with this requirement by making all on-board recordings —including cockpit voice recorders (CVR)— privileged in the Canadian Transportation Accident Investigation and Safety Board Act. While the TSB may make use of any on-board recording in the interests of transportation safety, it is not permitted to knowingly communicate any portion of an on-board recording that is unrelated to the causes or contributing factors of an accident or to the identification of safety deficiencies.
The reason for protecting CVR material lies in the premise that these protections help ensure that pilots will continue to express themselves freely and that this essential material is available for the benefit of safety investigations. The TSB has always taken its obligations in this area very seriously and has vigorously restricted the use of CVR data in its reports. Unless the CVR material is required to both support a finding and identify a substantive safety deficiency, it will not be included in the TSB’s report.
To validate the safety issues raised in this investigation, the TSB has made use of the available CVR information in its report. In each instance, the material has been carefully examined in order to ensure that it is required to advance transportation safety.
1.1 History of the flight
On 30 May 2013, at 1845,Footnote 2 the Operations Control Centre (OCC)Footnote 3 of Ornge received a request to medevac a pediatric patient from Attawapiskat, Ontario, to Moose Factory, Ontario. The patient's medical condition was classified by the sending physician as an emergency. According to the Ontario Regulation 257/00 under the Ambulance Act, an emergency is defined as “a situation where a delay in responding to a call for services could endanger the life, limb or function of a person.”Footnote 4 Since the day crew were to finish at 1900, Ornge's OCC decided to dispatch the night crew at 1900. At 1918, the captain, who had completed a weather check, declined the trip due to poor weather conditions. At 2009, following the release of a new weather sequence for the area, the OCC contacted the captain for another weather check. The captain again declined the trip due to poor weather. At 2319, the captain contacted the OCC, advised that weather conditions had improved, and accepted the trip. The flight crew proceeded to the Moosonee Airport (CYMO), Ontario, and had the helicopter readied, including fuelling, for the 1-hour-and-48-minute visual flight rules (VFR) flight to the Attawapiskat Airport.Footnote 5 Two paramedics were on board in addition to the captain and first officer.
At approximately 0000, the occurrence pilots commenced the pre-start checklist. The first officer, seated in the right-hand seat, was the pilot flying (PF). The captain, seated in the left-hand seat, was the pilot monitoring (PM). In the S-76, the captain would normally operate from the right seat; however, under certain circumstances, a first officer could be permitted to fly from the right seat. These circumstances will be discussed later in the report.
After starting the first engine and engaging the main rotor, the flight crew obtained the weather report from the automated weather observation system (AWOS) located at CYMO. The first officer then commenced the start sequence for the second engine. As the speed of the second engine was increasing to idle, the captain verbalized that he was initially having difficulty locating the flight instrument light-intensity rotary switch, which was located on the centre console between the pilot seats. The captain then advised the first officer that he had a flashlight in case he had any further difficulty locating a switch.
As the engine start checks continued, the first officer called “150”, which is a radio altimeter decision-height setting (often referred to as a radio altimeter low-height bug) commonly used by S-76A pilots at 7506406 Canada Inc. (hereinafter referred to as Ornge Rotor-Wing [RW]). The captain did not acknowledge the first officer's call of “150”. Shortly thereafter, the first officer advanced the engine/fuel levers to the fly position as per the checklist.
The first officer then briefed the captain that the departure would be from Runway 06, with a left-hand turn toward Attawapiskat. He did not mention a planned turnout altitude or planned actions in the event of an emergency during the takeoff portion of the flight, as is required under the company standard operating procedures (SOPs). The captain indicated his concurrence with the first officer's briefing.
Moments later, the first officer called for the taxi checks and began to taxi toward Runway 06, completing the taxi checks along the way. The flight crew then carried out the takeoff check. When the captain called for altimeters and radio altimeter, the first officer indicated that he had an altimeter setting of 30.00 inches of mercury (in. Hg), and that the altimeter indicated 20 feet above sea level (asl). The first officer also indicated that he had 150 feet set on the radio altimeter low-height bug. The captain did not read back any of this information; instead, he continued with the next step in the checklist. Moments later, the captain called for the compass and heading. The first officer replied, stating that these were 137 and 140. The captain did not read back the compass settings on his side of the cockpit. The first officer then completed his takeoff briefing, indicating that it would be a takeoff from Runway 06, with routine calls as per SOPs, and with a left-hand turnout to Attawapiskat. After a brief pause, the first officer indicated that the flight to Attawapiskat would be conducted at 1000 feet. As the flight crew prepared for takeoff, the captain again momentarily experienced difficulty locating the rotary switch used to control the helicopter's flight instrument lights.
At approximately 0011, the first officer applied power, and the helicopter lifted into the hover. The first officer indicated that the centre of gravity felt fine, and the captain advised that they were pulling approximately 80% torque in the hover. After verifying that the engine instruments were fine, the first officer initiated the departure along Runway 06. During the initial transition to forward flight, the captain called torque at 85%, at 90%, and then at 95%. Immediately after calling 95%, the captain indicated that the airspeed had increased through 35 knots. The first officer then indicated that he was commencing the climb-out. The captain called 52 knots, then 74 knots, and then confirmed that the aircraft had a positive rate of climb and that they were climbing at approximately 400 feet per minute.
Approximately 10 seconds later, the first officer called for the post-takeoff check. The captain advised that they were climbing through 300 feet above ground level (agl). Immediately afterward, the first officer advised the captain that he was commencing a left-hand turn. The captain acknowledged the statement and began the post-takeoff checklist, verbalizing that the gear was in transit, the aircraft's emergency flotation system was off, and the compasses were slaved. The captain also offered to turn off the landing light for the first officer. Approximately 5 seconds later, the captain again indicated that he would turn the landing light off; 2 seconds after that, the captain called out “30 degrees of bank.” The first officer acknowledged the callout, indicated that it was too much bank, and apologized. One second later, the landing-gear warning horn sounded; the captain advised that they were descending and said, “Let's climb.” The aircraft struck terrain less than 1 second later, on a heading of approximately 318° magnetic (M). Twenty-three seconds had elapsed from the time the first officer advised the captain that he was commencing the left-hand turn to the point of impact.
The occurrence aircraft was equipped with a satellite tracking system, which reports takeoffs, landings, and position updates every 2 minutes. The system reported a takeoff message at 0011 and then went inactive 2 minutes later. At approximately 0033, suspecting a problem, the duty flight follower attempted to contact the occurrence flight crew by calling the standby pilot cellular phone normally carried by one of the standby pilots, calling the base, and then calling the satellite phone carried on board the aircraft. These steps were repeated a couple of times. At 0047, the flight follower briefed the manager of flight operations on the situation, and London Flight Information Centre (FIC) was advised. A communication search, in which attempts were made to reach the occurrence flight crew over the radio, was then initiated by London FIC. Shortly after 0100, it was confirmed that the aircraft was no longer at CYMO, and there were reports of a fire in the trees a few miles northeast of CYMO. The local Ontario Provincial Police (OPP) detachment was advised, and at 0112, the Joint Rescue Coordination Centre was contacted. A CC130 Hercules and a CH146 Griffon stationed in Trenton, Ontario, were tasked to search for the missing aircraft. At 0125, Ornge initiated its emergency response plan. At 0543, the CC130 located the crash site, and the search-and-rescue technicians (SAR TECHs) parachuted into the location. Once on scene, the SAR TECHs reported that there were no survivors.
1.2 Injuries to persons
| Injury | Crew | Passengers | Others | Total |
|---|---|---|---|---|
| Fatal | 2 | 2 | – | 4 |
| Serious | – | – | – | – |
| Minor/None | – | – | – | – |
| Total | 2 | 2 | – | 4 |
1.3 Damage to aircraft
The helicopter was destroyed by impact forces and post-crash fire.
1.4 Other damage
The accident occurred in a densely wooded area, away from any built-up areas.
1.5 Personnel information
1.5.1 General
| Captain | First officer | |
|---|---|---|
| Licence | Airline Transport Pilot Licence–Helicopter |
Commercial Pilot Licence–Helicopter |
| Medical expiry date | 01 July 2013 | 01 December 2013 |
| Total flying hours | 11 500 | 3706 |
| Total hours, pilot-in-command | 10 430 | 3369 |
| Total hours, pilot-in-command on S-76A | 150 | 0 |
| Total instrument (actual/simulated) flight hours | 244 | 33 |
| Total simulator flight hours | 82 | 51 |
| Total night hours | 650 | 140 |
| Total flying hours, helicopter | 10 800 | 3706 |
| Hours on type | 500 | 158 |
| Hours in the last 7 days | 6.2 | 4.9 |
| Hours in the last 30 days | 14.8 | 19.3 |
| Hours in the last 90 days | 66.2 | 61.3 |
| Hours in the last 365 days | 170.8 | 281 |
| Hours off duty prior to work | 24 | 12 |
1.5.2 Captain
1.5.2.1 General
The captain held a Canadian Airline Transport Pilot Licence (ATPL)–Helicopter, with type ratings on the Bell 206, 212, 222, 47, Eurocopter 135 and AS350, Messerschmitt–Bolkow–Blohm BK117, Robinson R44, and Sikorsky S-76. His licence was endorsed with a Group 4 instrument rating, valid until 01 April 2015. The captain was also a licensed aircraft maintenance engineer.
1.5.2.2 Chief Pilot, Ontario Ministry of Natural Resources
At the time of the occurrence, the captain was working as a part-time captain for Ornge RW while on vacation from his full-time employment as chief pilot (CP) of the Ontario Ministry of Natural Resources (MNR) Rotor-Wing division. The investigation determined that the captain was highly respected by subordinates, peers, and superiors.
At the MNR, rotor-wing flights are conducted under day and night VFR; however, the operation is predominantly a day VFR operation. In 2005, the MNR transitioned to using night-vision goggles (NVG) for its night VFR operations. While not mandatory that all MNR night VFR flights be conducted using NVGs, all planned night VFR operations for MNR clients are done with NVGs. For other night VFR flights, NVGs are employed when they are available and the pilots are trained and current on NVG operations. The occurrence captain was instrumental in implementing NVGs at the MNR.
MNR pilots receive some instrument flight training during annual recurrent simulator training, and they are permitted to conduct instrument flight training while operating in visual meteorological conditions (VMC) if a safety pilot is on board the aircraft.
Prior to joining Ornge RW in March 2013, the captain had made a few positioning flights into and out of CYMO over the years while employed with the MNR. All of these flights were conducted during daylight hours. According to his logbook, the last time that the captain had been to CYMO prior to commencing employment with Ornge RW was in the summer of 2012.
1.5.2.3 Captain's previous emergency medical services experience
In December 2001, the captain completed his S-76A initial aircraft type course. For the next year, he flew on a casual part-time basis for the previous operator that had been contracted to provide helicopter air ambulance services for Ontario. The captain allowed his pilot proficiency check (PPC) on the S-76A to expire in 2003. Then, in March 2007, he conducted 3 training flights with the previous helicopter emergency medical services (HEMS) operator. Shortly thereafter, the captain sought and received approval from the MNR to engage in additional part-time employment as an emergency medical services (EMS) captain. In its approval letter of 20 August 2007, the MNR stated “You must continue to maintain the flight duty time and minimum rest periods in accordance with Transport Canada and MNR regulations.”Footnote 6 Although it was the captain's intention to serve as a part-time EMS captain in 2007, he was not involved in any operational flights for the remainder of that year.
In April 2008, the captain completed a PPC on the S-76A. During the PPC, he received a mark of 2 (on a 4-point marking scale) for pilot-not-flying (PNF) duties, resulting from difficulties associated with setting up the radios and aids to navigation as per the SOPs. Transport Canada's (TC's) Pilot Proficiency Check and Aircraft Type Rating Flight Test Guide (Helicopter) (TP 14728) specifies that a mark of 2 on a PPC means that the pilot has met the “basic standard” and is assigned as a mark when “major deviations from the qualification standards occur, which may include momentary excursions beyond prescribed limits but these are recognized and corrected in a timely manner.”Footnote 7 A candidate who has 5 or more sequences or items assessed as 2 during a PPC will receive a general assessment of “failed”.
During the summer of 2008, the captain again sought approval from the MNR to fill occasional EMS shifts throughout the summer. He indicated to MNR management that the EMS operator was aware of the conditions of the MNR's previous approval. Once again, MNR management approved the captain's request, with the caveat that this work not interfere with his MNR duties. In addition, he was advised not to do both jobs at the same time, due to duty-time regulations. The captain made it clear that he understood that he was required to comply with crew duty-day regulations and indicated that he would not over-commit.
The captain's next PPC on the S-76A was completed on 10 March 2009. During that PPC, the captain received a mark of 2 for the go-around portion of the flight, as a result of being slow to acquire, and then having difficulty maintaining, the correct missed-approach track. On 12 April 2010, the captain completed another PPC on the S-76A. During that PPC, the captain received a mark of 2 for the initial climb, resulting from momentarily allowing the rate of climb to decrease during the departure. According to the captain's logbook, his last flight in the S-76A before joining Ornge RW was on 21 February 2011.
The vast majority of the captain's flights as an EMS pilot prior to joining Ornge RW were out of Sudbury, Ontario, where he had been hired. While employed with the previous EMS operator, the captain had flown a couple of flights into and out of CYMO. As well, he had conducted 3 night flights, totalling 4 hours, as first officer on the S-76A out of CYMO in December 2008. He also acted as the pilot-in-command (PIC) during 4 day shifts at CYMO in July 2010, accumulating 11.7 flight hours during those 4 shifts. Although it is possible that the captain had at some point in the past flown out of CYMO as PIC on a night VFR flight, there is no record of the captain having flown as PIC during a night VFR flight from CYMO since at least 2001 when he first began flying as an EMS pilot.
1.5.2.4 Hiring of the captain by Ornge Rotor-Wing
In mid-January 2013, the captain contacted Ornge RW's Operations Manager (OM)/Director of Flight Operations (DFO) about doing some part-time work for Ornge RW. During communications with the OM/DFO, hereafter referred to as the OM, the captain indicated that his S-76 PPC had expired in May 2011. No arrangements were made at that time for the captain to join Ornge RW. Then, in early March 2013, the OM asked the captain whether he would be available to commence training later that month, indicating that he would like to pair him with 1 of 3 new hires on an upcoming initial S-76 course, and that the captain's mentoring on the course would be invaluable to the 3 new hires.
Although the original plan was to send the captain on an initial S-76 course, the company hired a fourth new first officer who needed an initial S-76 course, and there was a last-minute opening on one of the upcoming recurrent S-76 courses. As a result, a decision was made to send the captain on the S-76 recurrent course from 24 to 31 March (including travel time) at the CAE Inc. training facility in Whippany, New Jersey. According to Commercial Air Service Standards (CASS) 723.91 and 724.111, if a flight crew member's PPC has been expired for 24 months or more, that crew member shall complete the air operator's initial helicopter-type ground school and flight training program, and then successfully complete a PPC on the helicopter type. Since the captain's most recent PPC on the S-76A had expired on 01 May 2011 (22 months previously), he was not required by regulation to complete a full initial S-76 course prior to his PPC.
As he had done previously, the captain approached MNR management about his potential employment at Ornge RW. As justification, the captain indicated that doing part-time EMS work would allow him to gain more experience in the instrument and night environments. He also advised the MNR that he would use his leave to cover shifts for Ornge RW. As previously, the captain was told that the MNR did not object, as long as this work did not interfere with his MNR duties. The captain then advised the MNR that he would complete the S-76 recurrent course at some point in the near future. However, he never advised MNR management that he had begun holding standby shifts with Ornge RW. Consequently, very few people, including MNR management, were aware that the captain had begun working for Ornge RW on a part-time basis at the time of the accident.
1.5.2.5 Captain's recurrent S-76 course
The captain's S-76 recurrent training, conducted by CAE, consisted of ground school on 25 and 26 March 2013, then simulator training from 27 to 29 March, followed by a PPC on 30 March 2013. Before his PPC, the captain completed 2 VFR simulator sessions and 1 instrument flight rules (IFR) simulator session as PIC. According to the captain's simulator training records, he underwent a total of 1 hour of night VFR training during the first recurrent VFR session, during which he completed 5 night takeoffs and 5 night landings.
There is no record, on Ornge RW's pilot training records, of the captain having completed practical controlled flight into terrain (CFIT) training while at the simulator, in accordance with the company's TC-approved Training Manual. According to CAE, CFIT-avoidance training is carried out in conjunction with a black-hole scenario in which candidates are required to depart from a helipad on a sheer cliff in New Jersey and then cross the Hudson River toward Manhattan, where they would receive a ground proximity warning system (GPWS) warning of approaching obstacles (i.e., the city skyscrapers). During the training, the occurrence captain and his training partner refused to carry out the black-hole training scenario presented by the CAE instructor because they considered it lacked operational realism. As a result, neither pilot completed the black-hole takeoff and the practical CFIT-avoidance portion of the recurrent S-76 training program. Despite this, the “Ground & Flight Training Summary & PPC Letter of Recommendation” form was signed by the instructor, and the captain was recommended for his PPC. The signoff and recommendation section of that form contains the following statement, “I have reviewed the candidate's training documentation and hereby certify that the ground and flight training requirements have been met in accordance with the approved training program as outlined in the Company Operations Manual.”
The captain was paired with an experienced Ornge RW S-76A captain from a different base. Two other Ornge RW S-76A pilots were undergoing recurrent training in Whippany at the same time. On multiple occasions during the recurrent course, the occurrence captain expressed concerns about working at CYMO as a captain due to his lack of recent IFR and night experience and his lack of preparation for the recurrent training.
On 30 March 2013, a company approved check pilot (ACP) conducted the PPCs for the captain and his partner. These PPCs, which lasted 2 hours, were monitored by the TC principal operations inspector (POI) responsible for Ornge RW, as part of routine ACP monitoring activities. Before starting the occurrence captain's PPC, the ACP, who noticed that the captain's IFR had expired in April 2012, discussed with him his employment at Ornge and his recent experience in night/IFR environments. Based on that discussion, the ACP believed that the captain should initially be given an opportunity to get comfortable in the job as a first officer before assuming captain duties. The captain concurred with the ACP's suggestion. Accordingly, the ACP advised the captain that he would fill in the “First Officer” dot in the Crew Status section of the Flight Test Report Pilot Proficiency Check (form 26-0249/0279).Footnote 8 However, according to TC, the crew status blocks on the PPC “have no significance for helicopters” and TC qualifies pilots as PIC. TC also indicated that a company can employ a pilot as captain regardless of what crew status box is selected on the PPC form.
The captain passed his PPC/IFR. He received a mark of 2 for his technical skills and knowledge as a result of momentary excursions from company SOPs and limited proficiency in these procedures. He was also marked 2 for aircraft handling, resulting from momentary deviations from specified limits when intercepting and tracking the non-directional beacon (NDB). The PPC form indicates that both of these issues were corrected in an acceptable time frame.
On 30 March 2013, while still in Whippany, the ACP sent an email to the OM and the Assistant CP advising them that his monitor ride went well. The ACP also indicated in that email that he had completed PPCs for the captain and his training partner, reporting that each had received 2 marks of 2. The ACP also advised the OM and the Assistant CP that the POI commented that the captain “needs to receive some training with our SOPs.”
On 01 April 2013, the ACP advised the TC POI that he would “address the issues we encountered during the rides” with the OM and the Assistant CP as soon as possible. On 10 April 2013, the ACP reported to Ornge's head office for some ACP-related work. During that visit, the ACP advised the OM and the Assistant CP that, due to difficulties encountered during the PPC/IFR, especially with respect to IFR and multi-crew operations, the captain should be employed as a first officer until he gained some additional experience.
The OM and the Assistant CP were aware that the captain's signed PPC form indicated “First Officer”, and that the TC POI had suggested the captain needed to receive additional training on company SOPs. According to the OM and the Assistant CP, it was their understanding that since the PPC standard for Ornge RW helicopter pilots was identical for captains and first officers, it was permissible to employ the captain, as originally intended, in a PIC capacity immediately. No restrictions were placed on the captain at that time, nor was anything done to flag the captain for additional supervision.
At the time of the occurrence, the company did not have a process in place to ensure close monitoring of pilots who experienced difficulties during their PPCs, nor was such a process required by regulation. The company's approach was that a captain holding a valid PPC was allowed to carry out PIC duties without restrictions.
1.5.2.6 Company indoctrination training
On 03 April 2013, Ornge's scheduling manager contacted the captain to inquire whether he would be interested in filling some empty shifts at CYMO. The captain advised the scheduling manager that he was unable to do so since he had not yet completed the required company indoctrination training.
The captain completed indoctrination training during the third week of April 2013. During that time, he completed the examinations on company indoctrination, safety management systems (SMS), and CFIT avoidance. On 22 April 2013, the captain participated in the company's aeromedical resource management (AMRM) training, taught by a contracted provider, and on 24 April 2013, he completed the S-76 Type examination and A-Model Variant examination.
1.5.2.7 Line indoctrination and aerodrome and area of operation qualification training
Under the Canadian Aviation Regulations (CARs), Subpart 705 operators and Subpart 704 operators that conduct IFR operations are required to conduct line indoctrination training. There is no such requirement for Subpart 703 operators.
In addition to line indoctrination training, Subpart 704 operators are required to provide pilots with aerodrome and area of operation qualification training. This training is done to “ensure that pilots-in-command are qualified for the areas of operation to which they are assigned and have received training, as applicable, to ensure safe operations are conducted.”Footnote 9 At Ornge RW, the company's TC-approved Training Manual states that its Agusta Aerospace Corporation 139 (AW139) and S-76 pilots shall receive aerodrome and area of operation qualification training. Ornge RW uses a combined line indoctrination and aerodrome and area of operation qualification training record to capture both training requirements. However, the line indoctrination portion of the record is normally not completed for S-76A pilots, since the company's S-76 pilots are not subject to the same Subpart 704 requirements as Ornge RW's AW139 pilots. The captain did not complete line indoctrination, nor was it required by regulation.
On 24 April 2013, the captain completed his aerodrome and area of operation qualification training at the Moosonee base. The training consisted of a verbal briefing of some of the different aspects of operations at the base, and was provided by one of the S-76A line captains at CYMO, who had been asked to do so by the Assistant CP. During discussion, the captain indicated that he had not done any black-hole training during his recurrent course in March 2013. As a result, on the captain's record of line indoctrination and training in aerodrome and area of operation qualification training, the line captain who provided the training annotated the “Black Hole Operations” portion of the form with “No training to date.”
The investigation determined that the OM and the CP were aware that the captain's form had been annotated to indicate that he had received no black-hole training. However, the OM believed that this unusual annotation had been investigated and that clarification had been sought through the CP's office. Although aware of the unusual annotation on the captain's form, the CP did not investigate it because he believed that the training had been completed in the simulator.
1.5.2.8 Captain's shift rotation history with Ornge Rotor-Wing
The captain's first rotation of shifts was from 25 April to 04 May 2013. These were all-day shifts (0700 to 1900), and were conducted with the first officer involved in the occurrence. The captain then returned for a second rotation of shifts starting 23 May 2013. From 23 to 29 May 2013, the captain was on day shift at CYMO. The captain and the first officer were paired from 23 to 27 May 2013 for day shifts. On 28 and 29 May 2013, the captain was paired with a different first officer on day shift. Then, on 30 May 2013, the pilots involved in the occurrence were scheduled together for a night shift (1900 to 0700). This was their first night shift together, and aside from the 5 night takeoffs and night landings completed during simulator training at the end of March 2013, it was the captain's first night flight at Ornge RW. At the time of the occurrence, the captain had flown approximately 28 hours on the S-76A since joining Ornge RW in March 2013.
On 22 May 2013, at approximately 1830, the captain arrived at CYMO for his final shift rotation. During his rotations in Moosonee, the captain had been heavily involved with MNR business. During the afternoon of his day shift on 28 May 2013, the captain sent several emails related to MNR business. During his day shift the following day (29 May 2013), he participated via telephone in a weekly MNR managers' meeting that lasted approximately 45 minutes. As well, he sent more than 50 emails between the 4 flights that he flew that day, many of which were related to MNR business.
On the day of the occurrence night shift (30 May 2013), the captain spent most of the morning and early afternoon corresponding via email on a number of MNR-related topics. From 0614 to 1332, the captain sent a total of 49 emails.Footnote 10 From 1332 to 1830, he did not send any emails. Between 1830 and 1907, he sent 5 emails, 3 of which were related to an email he had sent at 1307, earlier that day. That same day, the captain also participated in an MNR teleconference, which lasted from 0900 to just after 1215. The MNR employees involved in the teleconference were unaware that the captain was participating from CYMO.
The TSB conducted a fatigue analysis to determine what, if any, role fatigue may have played in the occurrence. The fatigue analysis examined sleep disruption, continuous wakefulness, circadian rhythms, medical conditions, and levels of arousal (i.e., stress). It was determined that the captain was awake by 0614 on the morning of the occurrence night shift, but that afternoon naps were a regular part of his daily routine when he was scheduled for night shifts. To maximize the quality of sleep obtained, he wore ear plugs and an eye shield at night and/or when napping. While it was not possible to confirm that the captain slept between 1332 and 1830, it is highly likely that he did so based on his history and the 5-hour gap in his email records. Based on the results of the fatigue analysis and a rigorous analysis of crew communications during the occurrence flight, there was no indication that fatigue played a role in this occurrence.
1.5.2.9 Captain's night flight and instrument flight rules experience/recency
According to the captain's logbook, he flew 1 night flight in 2011. That 3.5-hour flight, which occurred on 08 November 2011, was conducted using NVGs. In 2012, the captain logged 3 night flights in May and June, totalling 7.7 flight hours. All 3 flights were conducted using NVGs. In 2013, the captain completed 4 night flights totalling 7.9 flight hours. The first 2 night flights took place on 16 February 2013. No night training was conducted on either of these flights, and the captain, who occupied the left seat, acted only in a pilot-not-flying (PNF) capacity. The third and fourth night flights were training flights completed on 17 April 2013. All 4 flights were conducted using NVGs.
The captain's logbook showed no record of any actual or simulated instrument flight hours between 2011 and 2013; however, there were PPC/IFR entries in December 2012 and April 2013. In 2013, 3 flights were identified in the captain's logbook as being IFR training. Those flights occurred between the end of February and the beginning of March 2013. Aside from the IFR portion of the captain's recurrent S-76 course in March, he had not conducted any IFR flights or undergone any IFR training while with Ornge RW, nor was it required under regulations.
1.5.3 First officer
1.5.3.1 General
The first officer acquired his commercial helicopter pilot licence in March 1997. He had endorsements for the Bell 206 and 407, Robinson R22 and R44, and Sikorsky S-76 helicopters, and was endorsed with a Group 4 instrument rating that was valid until 01 April 2015. Prior to joining Ornge RW, he had been involved in some executive and bush flying, and also had some experience conducting spraying and firefighting operations. He was interviewed by Ornge RW on 21 June 2012, and officially joined the company on 05 August 2012.
1.5.3.2 Initial S-76 training
The first officer completed S-76 initial ground school from 06 to 10 August 2012 at a certified training facility in West Palm Beach, Florida. Following ground school, he returned to flying for another company, engaging in a spraying operation. The first officer's flying schedule had been very busy in the weeks leading up to the simulator portion of his initial training, and he was unable to study before the simulator training. Moreover, the first officer, who was new to the multi-crew environment, had not received a copy of the company SOPs before the simulator training.
From 01 to 08 September 2012, the first officer completed his training on a Sikorsky S-76C++ simulator in Vancouver, British Columbia, using an Ornge RW training pilot and Ornge RW SOPs and checklists. Just prior to this, the first officer had received 2 hours of on-aircraft differences training in one of the company's S-76As. The simulator complied with Level B qualification standards and criteria as per TC's Aeroplane and Rotorcraft Simulator Manual.Footnote 11 However, according to Appendices 8-D and 8-E in TP 9685, and confirmed by TC, a Level B simulator cannot be used for a PPC without additional time on the aircraft. When Ornge RW's POI became aware in November 2012 that the first officer's training and PPC had been completed exclusively using a Level B simulator, the validity of the first officer's PPC was brought into question. Following internal review, TC decided that the first officer's PPC would be accepted.
During his time in Vancouver, the first officer completed the examination covering IFR, night, global positioning system (GPS), CFIT, and minimum equipment list training; the S-76A type examination; and the S-76A SOP examination. However, the investigation learned that, before the simulator training, one of the company pilots had sent the answers to these 3 examinations to all 4 of the company pilots who were undergoing simulator training during that time frame. Investigators also determined that the CP was aware that answers to the examinations were in circulation; however, timely action was not taken to re-establish the integrity of the examinations. At the time of the accident, Ornge RW had not revised its S-76A examinations. One of the examinations was subsequently revised in July 2013, and the other 2 were revised in November 2013.
Simulator training records indicated that the first officer experienced some difficulties with unusual attitude recoveries, basic instrument air work, standard night operations, multi-crew IFR operations, and company-approved landing sites. Comments on the first officer's training records indicated that he had experienced slow but steady progress. However, when it was time for his final simulator training session, the training captain requested, and was granted permission to carry out, an additional 8 hours of simulator training for the first officer and his partner (4 hours as PF and 4 hours as PNF) due to motion sickness and below-average IFR skills. In total, the first officer received 16 hours of flight time as PF and 16 hours as PNF. He received practical CFIT-avoidance training during the simulator sessions.
Upon completion of his initial simulator training, the first officer successfully completed a PPC on the S‑76. During that PPC, the first officer obtained 3 different ratings of 2 for different sequences:
- enroute climb—for being slow to correct airspeed and rate of climb deviations;
- very high frequency omnidirectional radio range (VOR) approaches—for being slow to maintain accurate altitude at the minimum descent altitude (MDA); and
- a simulated tail-rotor cable failure—resulting from slowness by the first officer to follow the procedure.
1.5.3.3 Company indoctrination training
As part of his company indoctrination training, the first officer completed company in-house AMRM training on 12 September 2012. This training was instructed by the DFO of Ornge's fixed-wing (FW) division, who was running an AMRM course for the fixed-wing pilots. The following day, the first officer completed the written company indoctrination examination and SMS examination, followed on 14 September 2012 by completion of the dangerous goods exam.
1.5.3.4 Line indoctrination and aerodrome and area of operation qualification training
The first officer's training file showed that his line indoctrination and aerodrome and area of operation qualification training record had only been signed off on 11 January 2013, despite his commencement of operational duties at CYMO in September 2012. According to Ornge, this deficiency was due to an administrative oversight and was picked up during an internal audit in January 2013. As with the captain's aerodrome and area of operation qualification training, it was completed as a short ground briefing session. As with the captain, the first officer did not complete line indoctrination training, and it was not required by regulation.
1.5.3.5 First officer progression
The first officer was motivated and eager to become a captain in order to build his multi-engine PIC time. During the first officer's employment, Ornge did not have a formal process in place to document a first officer's progression and authorization to fly from the right seat. In the case of some first officers, including the occurrence first officer, there was no supporting documentation to show that they had completed Ornge RW's in-house requirements for right-seat approval (section 1.17.5.3 ), as per the TC-approved Company Operations Manual (COM). In other cases, records consisted of an email sent from the training pilot that did not include detailed information about the sequences flown. As well, the onus was on the first officer to advise his captain that he was permitted to fly from the right seat. There was no ready means for a captain to confirm this. If a captain was unsure or had concerns, the recourse was to call company headquarters (HQ) to verify whether or not a first officer was authorized to fly from the right seat.
1.5.3.6 First officer's night flight and instrument flight rules experience/recency
Prior to joining Ornge RW, the first officer had acquired very little night flight and IFR flight experience. He had begun flight training in June 1996, and by the end of that year had accumulated approximately 10 hours of simulated instrument flight hours and no night experience. He did not log any actual or simulated instrument flight from January 1997 to September 2008, at which time he logged 4.3 hours of simulated instrument flight time. He later conducted a series of instrument flights during March 2010, in order to earn his Group 4 instrument rating. Between March 2010 and April 2012, he logged approximately 3 hours of simulated instrument flight time. After April 2012, there are no actual or simulated instrument flight hours logged in the first officer's personal logbook. In that logbook, he logged all of his S-76 simulator course time (34.6 hours) as “simulator” and also logged it as 16.3 hours of multi-engine night PIC time and 16.8 hours of multi-engine night co-pilot time. As well, he logged 1 hour each of multi-engine day PIC time and co-pilot time. Under CARs, simulator time may be used for credit in certain circumstances, but does not count toward a pilot's total flight hours.Footnote 12 The first officer had no actual instrument flight hours logged. Aside from the simulated instrument time he obtained during the initial S-76 conversion course, the first officer had not conducted any IFR flights with Ornge.
Over the period of his employment at Ornge RW, the first officer accumulated 12.5 hours of night flying. During his last 6 months with the company, he completed 5 night takeoffs and 6 night landings, meeting the requirement of 5 night takeoffs and 5 night landings stipulated by regulation to carry passengers. Ornge RW flight records, compiled from the company's Aviation All In One (AvAIO) software programFootnote 13 shortly after the accident, indicated that the first officer had completed only 2 night takeoffs and 4 night landings in the previous 6 months. At the time of the accident, Ornge RW was not actively monitoring its pilots to ensure that they were meeting their minimum takeoff and landing currency requirements. It was later determined that AvAIO was not tracking takeoffs and landings at Moose Factory before 01 January 2013, due to a typographical error in the coordinates for that location. As a result, none of the takeoffs or landings made at Moose Factory were counted before 01 January 2013, when the problem was corrected.
A review of the first officer's corrected flight records revealed that he had not completed a night takeoff and landing in the previous 60 days, and had done only 2 night takeoffs and 2 night landings in the previous 90 days. Since becoming operational at Ornge RW in September 2012, he had completed a total of 10 night takeoffs and 11 night landings.
| Date | Night takeoffs | Night landings |
|---|---|---|
| 07 November 2012 | 1 | 1 |
| 16 November 2012 | 2 | 2 |
| 17 November 2012 | 2 | 2 |
| 05 December 2012 | 1 | 1 |
| 13 December 2012 | 2 | 2 |
| 09 January 2013 | 0 | 1 |
| 07 March 2013 | 1 | 1 |
| 08 March 2013 | 1 | 1 |
| Total | 10 | 11 |
His most recent night takeoff was on 08 March 2013, 85 days before the accident. The investigation revealed that the first officer often did not do much of the flying during the night flights he logged while at the company. Due to his lack of night flight experience, the Ornge RW captains normally did the flying, while the first officer performed the PM duties.
Shortly after completing his initial S-76 course, the first officer began to routinely swap his night shifts for day shifts with another Moosonee-based pilot. The first officer, who was eager to increase his total flight hours, preferred the day shift over the night shift because more flying was typically done during the day shifts compared to the night shifts. The first officer first began swapping his night shifts in September 2012 and held day standby exclusively until January 2013. At that point, he was advised by Ornge that he would have to return to night shift rotation for a while, because he was accumulating overtime due to the additional hours that he flew while only holding day standby.
He held night standby shifts in February and March 2013, and then swapped his night shifts in April and early May 2013 for day shifts. On 28 May, he started a night shift rotation, logging just over 30 minutes of night flight time on 28 May and none on 29 May. The first officer's flight- and duty-time limits were not exceeded, and there was no indication that fatigue played a role in the occurrence.
Company employees considered the first officer to be highly proficient in daytime VFR operations. However, he had previously encountered some difficulties at night, which were considered to be due to his lack of experience in night VFR operations. During a night departure into a black hole in early March 2013, the first officer began turning at 300 feet agl. The captain intervened, applied collective thrust and directed the first officer to continue climbing straight ahead up to at least 500 feet agl. Once passing through 500 feet agl, the first officer entered the turn. During the turn, he allowed the aircraft angle of bank to increase beyond the accepted rate-1 turn.Footnote 14 As the aircraft bank angle passed through 20 degrees, the captain provided verbal corrections, and the first officer reduced the bank angle. The captain of the flight had anticipated that the first officer would have difficulties because of his inexperience in night black-hole operations, and therefore did not consider it necessary to report this.
1.6 Aircraft information
1.6.1 General
The Sikorsky S-76A helicopter was designed and manufactured by Sikorsky Aircraft United Technologies as a medium-sized utility/corporate helicopter in the mid-1970s, with the first production flight in 1977. It has a maximum take-off weight of 4763 kg (10 500 pounds), a maximum cruising speed of 155 knots, and a range of approximately 404 nautical miles. The S‑76As at Ornge RW are IFR-equipped and operated by 2 pilots.
The occurrence aircraft was manufactured in 1980 and imported into Canada in 1999. On 13 July 2012, it was registered as a commercial helicopter to Ornge RW. At the time of the occurrence, C-GIMY had accumulated approximately 15 600 hours of air time and 48 400 landings. Records indicate that the aircraft was certified, equipped, and maintained in accordance with existing regulations and approved procedures. The helicopter had no known deficiencies before the occurrence flight and was being operated within its load and centre-of-gravity limits. Nothing was found to indicate that the aircraft encountered any type of system malfunction during the flight.
1.6.2 Description
The S-76A has a crew door on each side of the fuselage, allowing access to the cockpit, and 2 swing doors hinged to 135 degrees used to access the cabin area. It has retractable landing gear and is equipped with emergency flotation bags for use in the event of an emergency landing on water. The helicopter is outfitted with 2 Rolls-Royce 250-C30A turboshaft engines. Each of the engines is capable of producing 650 shaft horsepower.
The aircraft has a 4-bladed main rotor, with a diameter of 44 feet. The main-rotor blades are strengthened by titanium spars, which are the primary structural members of each blade on the main rotor, and the leading edge of each blade is protected by a titanium nosepiece. The blade tips are tapered and swept back. The anti-torque tail-rotor system also incorporates a 4-bladed rotor. The total length of the helicopter from the tip of the main rotor to the tip of the tail rotor is just over 56 feet.
To accommodate medical staff, the cabin had 2 forward-facing seats at the rear and 2 back-facing seats located just aft of the cockpit. All 4 seats were located toward the outer section of the cabin to allow for a patient stretcher to be installed in a longitudinal orientation in the middle of the cabin.
1.6.3 S-76A flight controls
The aircraft is equipped with conventional helicopter flight controls, which are hydraulically actuated. Collective and cyclic trim and a force-gradient system permit trimming of the controls in the cockpit to the desired position and provide cyclic control stick (cyclic stick) feel.
1.6.4 S-76A fleet differences at Ornge Rotor-Wing
Since its introduction into service, the S-76 has undergone a number of changes, many of which are associated with developments in technology. Ornge RW has a diverse fleet of S-76A helicopters, with many differences among their respective airframes (Appendix A). At times, these differences created challenges for Ornge RW's pilots. Some pilots were uncomfortable switching, on short notice, to an unfamiliar S-76A in the fleet. In some cases, pilots refused to fly at night in unfamiliar S-76As because they deemed it to be unsafe. In other instances, concerns were raised by pilots regarding the lack of modern GPSs and autopilots in some of the company's S-76As to help reduce pilot workload.
1.6.4.1 Automatic flight control systems / autopilots
There are a number of different automatic flight control systems (AFCS) available on the S-76A. At Ornge RW, some of the company's S-76As have upgraded AFCSs and autopilots that are capable of full four-axis coupled hands-off operation. The occurrence aircraft was equipped with a rudimentary AFCS, designed to provide basic attitude retention functions about the pitch, roll, and yaw axes. Due to the limited authority of these systems, the pilot may easily override AFCS inputs.
1.6.4.2 Global positioning system
At the time of the occurrence, 3 different GPSs were employed across Ornge RW's S-76A fleet. The Trimble 2100 GPS was installed in one of the 11 aircraft. Five of the other helicopters, including the occurrence helicopter, were equipped with the Bendix KLN 900 GPS. The KLN 900 is certified for IFR non-precision approaches. However, it provides little in the way of visual guidance or cues to pilots, and it is not tied into other aircraft systems.
The 5 remaining S-76As in Ornge RW's fleet are equipped with the Garmin 530 GPS, which is an all-in-one IFR GPS, communication, navigation, and in-colour moving map unit designed to enhance situational awareness by presenting the pilot with information that is easy to read and interpret. The unit can be upgraded to also include a terrain awareness and warning system (TAWS) and traffic information services alerts that identify surrounding air traffic.
1.6.4.3 Enhanced ground proximity warning system
At the time of the accident, 5 of Ornge RW's 11 S-76A helicopters were equipped with the Honeywell MK XXI enhanced ground proximity warning systems (EGPWS). Of the 3 S-76As that were in service on the day of the accident, only one had an EGPWS. The occurrence helicopter was not equipped with an EGPWS, nor was this system required by regulation.
The MK XXI has both look-down and look-ahead functionality, to predict potential conflicts that may be approaching and give the pilot additional time to take corrective action before it is too late, through a combination of annunciator lights, colour displays, and aural alerts.
All 10 of Ornge RW's AW139s are equipped with the Honeywell MK XXII EGPWS, which is the successor to the Honeywell MK XXI EGPWS.
1.6.4.4 Landing gear “up” warning horn
On the S-76A, the landing gear warning system is designed to warn the pilot that the landing gear is up and that the aircraft is entering a flight regime typically associated with the landing phase. Due to the vast differences within the S-76A fleet, this system is not the same in all aircraft. All of Ornge RW's S-76As were equipped with a 60-knot airspeed switch. Some of the company's S-76As were wired so that the landing gear warning would also activate if the aircraft descended below 300 feet agl and the landing gear was still in the up position. Yet another aircraft was wired so that the landing gear warning was tied to the radio altimeter low-height bug setting.
However, in the case of the occurrence aircraft, the landing gear warning system was not connected to the radio altimeter. Based on an evaluation of the cockpit voice recorder (CVR), discussions with the manufacturer, and examination of the wreckage field, it was determined that the landing gear warning horn sounded just before impact, and was most likely activated as a result of erroneous pitot-static readings caused by impact with the trees.
1.7 Meteorological information
The weather conditions reported by the AWOS at the time of the occurrence were: winds at 040°M at 5 knots, visibility greater than 9 statute miles (sm), a scattered cloud layer based at 4600 feet asl, an overcast ceiling based at 9000 feet asl, temperature 3°C, dewpoint 2°C, and altimeter 30.00 in. Hg.
In the hours before the accident, the weather had gradually improved from IFR conditions, due to low ceilings and visibilities, to VFR conditions.
At the time of the occurrence, approximately 50% of the moon was illuminated. However, ambient lighting would have been reduced due to the high overcast condition.
1.8 Aids to navigation
There was no indication of problems with the available aids to navigation.
1.9 Communications
No difficulties with the quality of radio transmissions were noted.
1.10 Aerodrome information
1.10.1 General
The Moosonee Airport (CYMO) has 2 runways: Runway 06/24, which is asphalt and measures 4000 feet long and 100 feet wide, and Runway 14/32, which consists of 1600 feet of asphalt and 1900 feet of gravel, and measures 100 feet wide. The elevation of CYMO is 30 feet asl.
Runway 06/24 parallels the Moose River, and Runway 06 heads away from the town of Moosonee. Beyond the approach lights at the departure end of Runway 06, there are virtually no sources of cultural lighting. The terrain to the northeast of Runway 06 is dense brush and bog. For the most part, the terrain increases very gradually to the northeast as one moves farther from the river's shore.
1.10.2 Weather camera
The airport is equipped with 2 weather cameras that take still images every 10 minutes. One of the cameras points to the northeast and the other points to the southwest. The camera pointing to the northeast is oriented in the general direction of Runway 06, paralleling it to the north. In the daylight image from this camera, it is possible to see a lit tower on the airfield and the treeline to the north of Runway 06. Images taken hours before the occurrence clearly show the tower and the treeline (Photo 1). In contrast, the only thing visible in a photograph from approximately the same time as the accident is the single light from the tower located on the airfield (Photo 2). No other cultural lighting, or ambient lighting from stars, is visible in the image.


1.11 Flight recorders
The occurrence aircraft was equipped with a solid-state Penny and Giles multi-purpose flight recorder (MPFR) configured as a CVR (part number D51615-102, serial number 323005-001) with a recording capacity of 2 hours. Although the MPFR was damaged by fire, the TSB laboratory was able to download the CVR data. The occurrence flight was captured within the last 11 minutes of the recording. The recording stopped upon impact.
The CVR was instrumental in determining the events leading up to the accident. In addition to the CVR data, the TSB laboratory recovered a supplemental flight information file from the MPFR containing main-rotor revolutions per minute (rpm) data. This information showed that the rotor rpm increased to and stabilized at approximately 104% during the flight.Footnote 15 The final value was 104.99%, recorded just before impact.
1.12 Wreckage and impact information
1.12.1 General
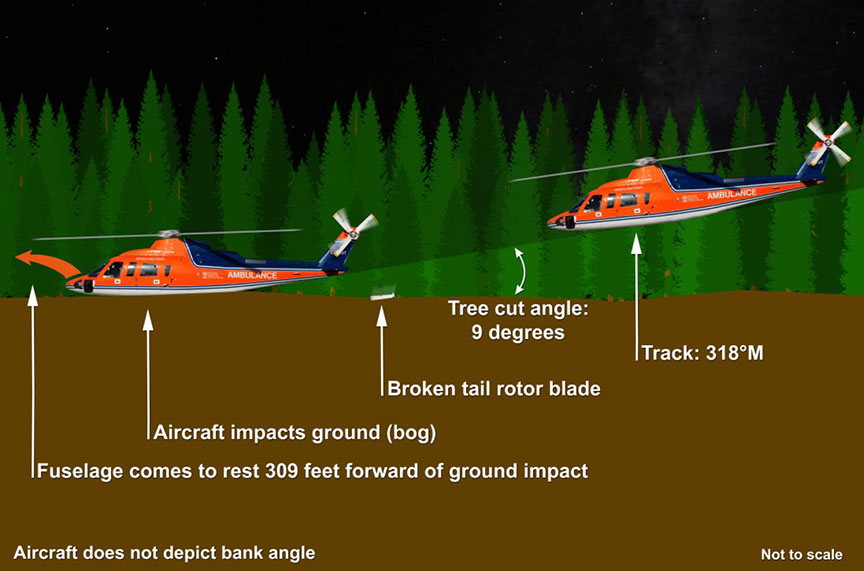
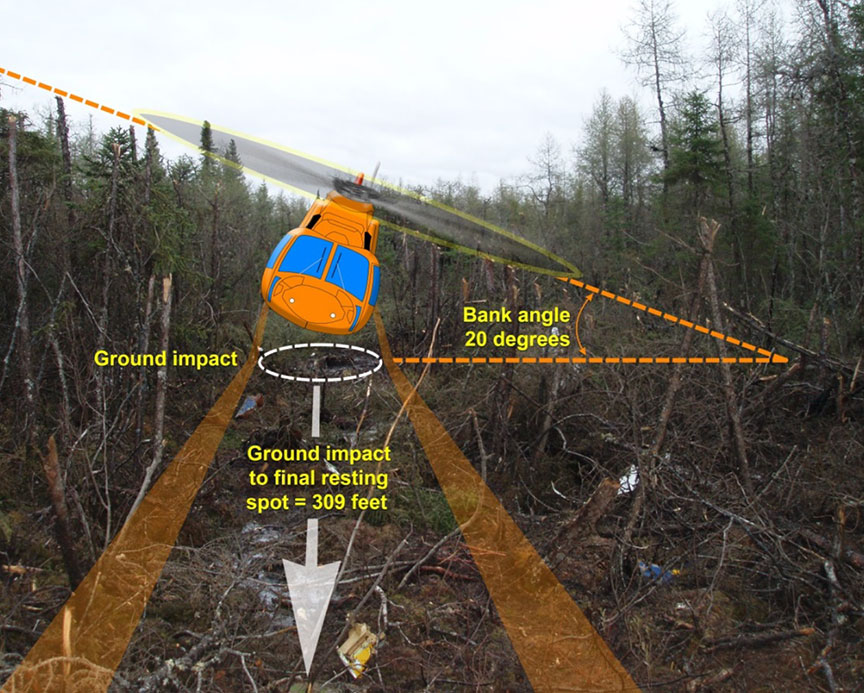
The wreckage was located in densely wooded, swampy terrain approximately 0.8 sm from the end of Runway 06, on a bearing of 020°M (Figure 1). Based on damage to surrounding trees and ground scars, investigators determined that the aircraft collided with the ground in a steady, shallow descent angle (approximately 9 degrees), in a left-banked (approximately 20 degrees) attitude (Figure 2 and Figure 3). Although it was not possible to determine the exact speed of the helicopter at the time of the accident, the damage to the surrounding terrain and trees, length of the wreckage trail, and extent of aircraft breakup during the impact sequence indicated a high-energy state (consistent with the helicopter being at or near cruise speed) upon impact with the ground.
The length of the crash swath path, from the first indication of contact with the trees to the location of the main wreckage, was approximately 405 feet. At the point of ground impact, the swath path was approximately 40 feet wide, gradually narrowing to approximately 20 feet, and then widening out again to form a circular, burned-out area approximately 35 feet in diameter (Figure 4).
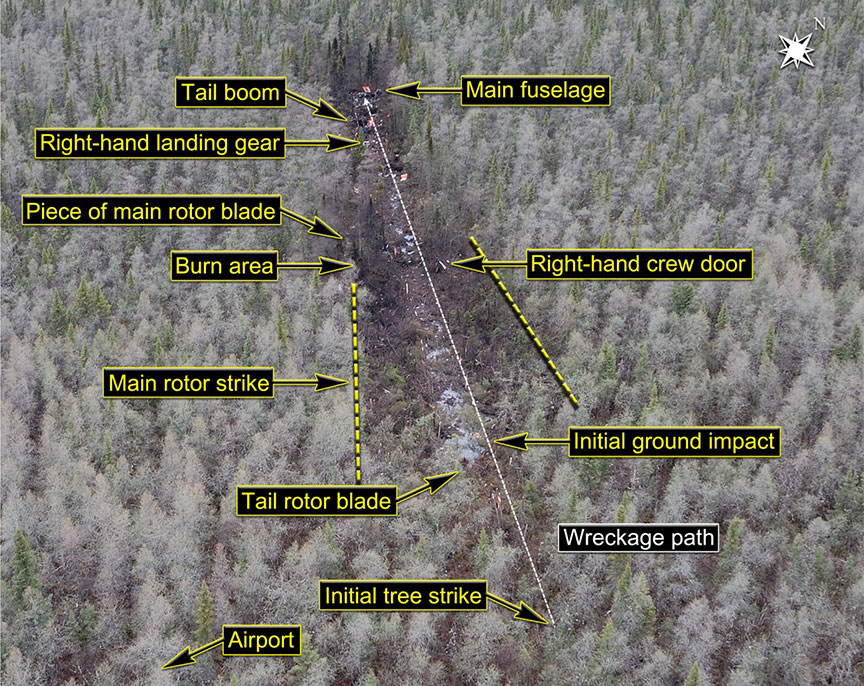
The point of initial impact was approximately 96 feet past the first indication of damage to the tops of the trees. Between the first indication of damage to the trees and the impact point, there is a definitive pattern of cut trees. The trees are cut to within 3 feet at the lowest point, corresponding with a left-bank attitude as the aircraft descended into the trees and the fuselage made contact with the ground.
At the location of the initial ground impact, a visible crater in the swampy terrain was evident, and the area was heavily saturated with fuel. In the crater and surrounding area were pieces of the fuel tanks and some of the fuel system components. As the fuel tanks and associated hardware are located in the belly of an S-76A helicopter, these observations indicate that the structure of the helicopter was compromised at that point. One of the helicopter's 4 tail-rotor blades was discovered just before the main impact location. The tail-rotor blade had broken off at the root. The loss of an S-76A tail-rotor blade would have introduced a yawing moment, causing the helicopter to rotate to the right.
The severed tailboom was located approximately 90 feet beyond the large burned area, almost perpendicular to the orientation of the impact trail. The tailboom had come to rest lying on the ground in its proper orientation. The top of the tailboom and the exposed tail-rotor drive shafts were covered in dirt and vegetation, which is consistent with tumbling during the impact sequence. A large portion of the tailboom, originating close to the point where the tailboom attaches to the fuselage, was found wrapped around a tree located just before the severed main portion of the tailboom, indicating that impact with that tree likely caused the tailboom to separate from the fuselage. Only 1 tail-rotor blade remained attached to the hub, and it exhibited damage to the trailing edge near the end of the blade. The remainder of the tailboom was not affected by fire damage. The external emergency locator transmitter (ELT) antenna, located on the tailboom, was found broken off at the base of the antenna.
One of the helicopter's 2 pitot tubes, normally located on each side of the nose near the front of the helicopter, was located approximately 20 feet outside of the main cut-out area, adjacent to the severed tailboom. The pitot tube had broken off at the base where it joins the helicopter's fuselage. The other pitot tube was not located.
The right main landing gear was located just before the severed tailboom. The left main landing gear was located just before the main wreckage. It was determined that both landing gear actuators were in the up position, indicating that the aircraft's landing gear was retracted at the time of the accident.
Approximately 60 feet beyond the severed tailboom was the main wreckage of the helicopter. The main wreckage was damaged extensively due to impact forces and a post-impact fire. The wreckage had come to rest almost perpendicular to the direction of the impact sequence. The main gearbox was found resting on its right side, and the 2 engines were found inverted behind it. The cockpit was also found in the inverted position. Because of the damage resulting from the post-crash fire, very little information could be obtained from the main wreckage, and the position of the engine controls prior to impact could not be verified.
1.13 Medical and pathological information
A post-mortem medical examination was conducted on all of the occupants of the helicopter. In all cases, the occupants had suffered from significant impact and thermal damage due to high impact forces and the post-crash fire.
It was determined that the captain and one of the medics survived the impact forces; however, they likely succumbed quickly to their injuries before significant inhalation of the fire combustion products. The medical examiner determined that the survival interval for these 2 individuals was in the order of seconds to minutes. In both cases, this survival interval may not have involved a level of consciousness.
In the case of the first officer, the medical examiner found no evidence of a survival interval, suggesting that the first officer died as a result of the impact forces. The autopsy also revealed significant coronary artery disease; however, there was no evidence to suggest that the first officer experienced an acute coronary event at the time of the accident, which is consistent with information obtained from the CVR.
As with the first officer, the medical examiner determined that the second paramedic died as a result of impact forces and there was no evidence of a survival interval.
1.14 Fire
The aircraft was destroyed by impact forces and an intense post-crash fire. There were indications that a large fire and/or an explosion had occurred approximately 50 feet beyond the point of initial impact with the ground. This burned-out area coincided with a large amount of debris, likely resulting from a significant impact to the trees in the surrounding area and a subsequent explosion.
1.15 Survival aspects
1.15.1 Helmets
The TSB has previously identified the risk to helicopter pilots who do not wear helmets, and has documented a number of occurrences in which the use of head protection likely would have reduced or prevented the injuries sustained by the pilots involved.Footnote 16
There is no regulatory requirement, nor was there a company requirement, for helicopter pilots at Ornge RW to wear helmets. The medics, on the other hand, fall under different collective bargaining agreements than the company's pilots and are provided with, and required to wear a helmet.
A large percentage of the company's pilots wore flight helmets; however, several pilots did not. The company had a cost-sharing program in place; however, it was not actively promoted within the company, so many pilots were unaware of the specifics of the program.
The investigation determined that both medics and the first officer were wearing helmets at the time of the occurrence. However, only the helmets of the first officer and one of the medics were recovered. The second medic's helmet was not recovered and was likely destroyed by the post-crash fire. Both of the recovered helmets were sent to the TSB laboratory for detailed examination.
The first officer was wearing an MSA Gallet LH 250 helicopter flight helmet (serial number 10458). The helmet was located on the ground, along the direction of travel, approximately 45 feet before the main wreckage. The shell of the helmet had cracks and small flaked-off areas on the back and right side consistent with impact damage. The chinstrap and the locking lever were not recovered with the helmet. No damage was observed on the permanently mounted chinstrap support and buckle on the left side of the helmet. The right side chinstrap support was also intact. No fire damage was observed on the exterior or interior of the helmet.
A white helmet, which had belonged to one of the medics and was a Gentex SPH-5 model, was located approximately 10 feet before the main wreckage. The front and left side of this helmet showed extensive fire damage. The helmet shell was burned, exposing its fiberglass reinforcement, and most of the chinstrap retention system was extensively fire-damaged. The chinstrap was constructed of Kevlar-reinforced nylon webbing, with a double D-ring for adjustment, and a single snap release for connection and disconnection. It was in good condition, with no sign of fraying or other damage.
In both cases, examination by the TSB laboratory determined that there were no signs of pre-existing or impact-related damage to explain why the helmets were not found on the victims, and it was not possible to determine whether they had been properly secured before the occurrence.
The captain did not wear a helmet while flying at Ornge RW. Instead, he wore aviation headphones while in the S-76A. However, the captain was required to, and did, wear a flight helmet when flying with the MNR. It is unknown why the captain did not wear a helmet while flying with Ornge RW.
1.15.2 Seat belts and crew harnesses
According to Ornge RW's COM, flight crew members are required to wear their seat belts and shoulder harnesses while seated at their respective stations while the rotors are turning. Due to the extent of the damage to the aircraft, it was not possible to determine whether all of the occupants were wearing their seat belts and shoulder harnesses at the time of impact.
1.15.3 Emergency locator transmitter
1.15.3.1 General
The occurrence aircraft was equipped with a Kannad 406-megahertz (MHz) automatic fixed helicopter (AF-H) emergency locator transmitter (ELT) (part number S1822502-02, serial number 2620766-0020). The ELT and the programming dongle (part number S1820514-01, serial number 2620955-0136) were installed on a shelf in the tailboom at station 341.3. There was an external antenna (part number 1327-82, serial number 8320) installed on top of the tailboom at station 373.8, and a remote control head installed in the cockpit on the centre console.
The Kannad 406 MHz AF-H ELT has a 3-position switch on the body of the ELT that allows for selection of “arm”, “off”, and “on”. The ELT switch was found at the accident site in the “arm” position. The ELT unit, which was held in position by a hook-and-loop retaining strap, was found hanging by its wire harness by search-and-rescue (SAR) personnel. The strap was ripped near the bottom of the tray, allowing the unit to hang freely (Figure 5).

In addition to the detachment of the unit from its mounting tray, the external antenna located on the tailboom had been severed due to ground impact forces (Figure 6).

The Kannad 406 MHz AF-H ELT exhibited minor damage to its case. Functional tests were performed to determine the serviceability of the ELT. Using the internal battery, the ELT did not provide a status indication, nor did the device produce any transmissions. However, when an external power supply was used, the ELT's status light flashed repeatedly, indicating that the ELT was transmitting, and it transmitted a 121.5 MHz signal and a 243.0 MHz signal along with a 406 MHz data burst approximately every 50 seconds.
Additional testing of the ELT confirmed that it would be activated when subjected to impact forces that were within the specified “g” range of the unit. This confirmation, in conjunction with the fact that the ELT's battery pack was depleted, strongly suggests that the device did activate on impact and did transmit a signal. However, no signal was received due to the damaged antenna.
1.15.3.2 Hook-and-loop fasteners for emergency locator transmitter retention
This is not the first TSB investigation in which a Kannad 406 MHz ELT has come free from its hook-and-loop mounting strap. There have been several accidents in which an ELT antenna broke off during the impact sequence or the wire to an antenna was damaged, and no signal was received by SAR personnel.Footnote 17 In TSB Aviation Investigation A11W0151, a Kannad 406 MHz AF-H ELT was ejected from its mounting tray during the impact sequence, and the external antenna was broken off due to ground impact. That investigation identified the importance of ensuring that the hook-and-loop retaining strap is tight; otherwise, the ELT can easily slide out of the tray if enough force is applied to it.
In the aftermath of its Aviation Investigation A11W0151, the TSB issued Safety Advisories to TC and to ELT manufacturers that use hook-and-loop retention systems. In addition, the United States National Transportation Safety Board (NTSB) issued safety recommendations to the Federal Aviation Administration (FAA) regarding hook-and-loop fastening systems. In response to the TSB's and NTSB's safety communications, TC and the FAA issued guidance to manufacturers, installers, and maintenance facilities. Kannad produced detailed guidance on how to properly secure an ELT using the hook-and-loop style of fasteners. Appendix B provides a more in-depth discussion of the safety communications issued following TSB Aviation Investigation A11W0151 that were related to hook-and-loop fasteners.
Acting on a previous NTSB recommendation, on 26 November 2012, the FAA issued Technical Standard Order (TSO) C126b: 406 MHz Emergency Locator Transmitter, which stated that “the use of hook and loop fasteners is not an acceptable means of attachment” for automatic fixed (AF) and automatic portable (AP) ELTs.Footnote 18 However, C126b was not retroactive, so it did not apply to previously installed ELTs. The NTSB therefore stated that “the problem of unintentional detachment during accidents will likely persist.”Footnote 19 In TC's Aviation Safety Letter Issue 2/2013, TC indicated that it planned to adopt TSO-C126b in its Airworthiness Manual (AWM) as a design standard. On 11 June 2015, a Preliminary Issue and Consultation Assessment (PICA) was published on the TC Canadian Aviation Regulation Advisory Council (CARAC) activity website. The PICA identifies that TSO-C126b has been adopted by the FAA. According to the PICA, “Transport Canada recognizes TSO-C126 or subsequent revisions as appropriate for aviation use in Canada. AWM Section 551.104 does not reflect this and requires amendment.”Footnote 20 However, at time of report writing, the standard had not been updated by TC. The Department has indicated that 406 MHz ELT installation approvals obtained before the adoption of the new standard will remain valid, even if those installations incorporate a hook-and-loop fastener. As a result, a large number of ELTs using hook-and-loop fasteners will remain in service in Canada for the foreseeable future.
1.15.3.3 Emergency locator transmitter performance studies
In a 2009 Defence Research and Development Canada (DRDC) report, Emergency Locator Transmitter (ELT) Performance in Canada from 2003 to 2008: Statistics and Human Factors Issues, DRDC examined impact-related and human factors–related reasons for ELT system failures during aircraft incidents.
In the DRDC study, which examined 27 instances in which no ELT signal was received, DRDC determined that fire damage, general impact to the ELT, breaking or disconnection of the ELT antenna, and water damage accounted for 55% of the reasons why no signal had been received. In total, the study determined that impact-related damage accounted for 92% of all failures among the occurrences that were examined. The report therefore concluded that the “greatest opportunity for improvement is to address ELT system failure due to crash impact.”Footnote 21 In particular, the report identified the following as possible areas for improvement:
- Crash impact survivability;
- Fire survivability;
- Survivability of connecting coaxial cable;
- Survivability of antenna; and
- Survivability and operation on submersion in water.Footnote 22
The Canadian Mission Control Centre (CMCC)Footnote 23 and the Australian Transport Safety Bureau (ATSB) have also found that impact-related damage (i.e., fire damage, impact damage, broken/disconnected antenna, and water damage) is responsible for the vast majority of non-activations.Footnote 24, Footnote 25 This conclusion is consistent with earlier research conducted in the late 1980s by the United States National Aeronautics and Space Administration (NASA), in which NASA concluded that the high percentage (88%) of crash-related ELT failures “reflects a requirement for ELTs and antennas which are more crash damage resistant.”Footnote 26
In 2005, the International Civil Aviation Organization (ICAO) ELT Task Force highlighted the need to pay particular regard to evidence concerning the survivability of ELT systems subject to crash forces.Footnote 27
1.15.3.4 Emergency locator transmitter regulatory requirements
As a member-state of ICAO, Canada is required to follow ICAO standards, unless TC formally notifies ICAO, in accordance with Article 38 of the Convention on International Civil Aviation, “of the differences between its own practice and that established by the international standard.”Footnote 28 The intent of filing a difference is to enable foreign operators to make informed decisions when considering whether or not to operate in a particular country.Footnote 29
In November 1999, ICAO released Amendment 74 to Annex 10 of the International Standards and Recommended Practices (SARP), Volume III. That amendment included the following standards related to ELTs:
5.1.1 Until 1 January 2005, emergency locator transmitters shall operate either on both 406 MHz and 121.5 MHz or on 121.5 MHz.
[…]
5.1.4 From 1 January 2005, [all] emergency locator transmitters shall operate on 406 MHz and 121.5 MHz simultaneously.
5.1.5 All emergency locator transmitters installed on or after 1 January 2002 shall operate simultaneously on 406 MHz and 121.5 MHz.Footnote 30
Consequently, as of 01 January 2005, unless a country has filed a difference, ICAO signatory countries must have regulations requiring ELTs that operate on 406 MHz and 121.5 MHz simultaneously.
In Canada and the United States, there is no regulatory requirement for aircraft to carry an ELT capable of transmitting on 406 MHz. The United States filed a difference to the ICAO standard;Footnote 31 however, Canada is not complying with the standard and has not filed a difference with ICAO. According to TC, a difference was not filed due to turnover among subject-matter expert staff, and the requirement was not acted upon as a result.
In 2008, TC proposed regulatory changes in the Canada Gazette, Part I, which “will require that aircraft operated in Canadian airspace be equipped with ELTs able to broadcast simultaneously on the frequencies of 406 MHz and 121.5 MHz or with an alternate means of emergency location that meets the performance criteria of a 406 MHz ELT.”Footnote 32 The Canada Gazette listed the following benefits of the proposed regulatory change:
- Rapid confirmation of a distress situation
- Measured relief response
- Improved crash location accuracy on initial transmission
- Reduced search time
- 40-fold reduction in false alerts
- Reduced exposure of SAR personnel to risks associated with low flying.Footnote 33
In the rationale section of the Canada Gazette, Part I, it was stated that “the potential benefits of these proposed amendments greatly surpass their cost”, and that “these proposed amendments will bring Canada into compliance with ICAO's ELT recommendations.”Footnote 34 However, this proposed rule change was met with considerable resistance, particularly among those in the recreational flying community. TC elected not to proceed with publishing this proposed regulatory change in the Canada Gazette, Part II.
On 01 February 2009, Cospas-Sarsat stopped monitoring 121.5 MHz ELT signals. If an aircraft equipped with a 121.5 MHz-only ELT is involved in an accident, that signal will therefore not be detected by SAR satellites. The only way the signal will be heard is if an aircraft monitoring 121.5 MHz happens to fly overhead and picks up the signal, or if a ground-based radio is being used to monitor the 121.5 MHz frequency. By comparison, 406- MHz beacons transmit information about a flight, such as the aircraft's registration number, which can be used to obtain emergency contact information and description of the aircraft, among other important information, from a beacon registration database. Some modern ELTs are also equipped with a GPS that sends position information along with a distress call.
On 11 June 2015, a Notice of Proposed Amendment(NPA) on 406 MHz ELTs was published on the TC CARAC activity website.Footnote 35 In it, TC proposed changes to CARs 605.38, 605.39, and 605.40 mandating the installation of 406 MHz-capable ELTs. According to the NPA, TC is proposing that dual 121.5 MHz/406 MHz ELTs be mandated. According to TC, this requirement can be met by a dual-frequency ELT unit, or by a dedicated 406 MHz ELT and a 121.5 MHz ELT. TC has indicated that virtually all new 406 MHz ELTs are dual-frequency units (i.e., 406 MHz and 121.5 MHz). CARs Part VII operators and Subpart 604 operators would have a one-year implementation period following the coming-into-force date. Private aircraft engaged in non-commercial, recreational operations would have a five-year implementation period.
Under the current regulations, approximately 27 000 Canadian-registered aircraft require an ELT. In March 2016, only 10 086 Canadian-registered aircraft in TC's Civil Aircraft Register database were equipped with at least one active 406 MHz ELT registered through the Canadian Beacon Registry. Of those aircraft, 5256 were private, 4604 were commercial, and the remaining 226 were state-owned. Therefore, more than half of all Canadian-registered aircraft that require an ELT are being operated with an ELT whose signal is not detectable by the Cospas-Sarsat system.
1.15.3.5 Emergency locator transmitter design standards and specifications
1.15.3.5.1 Emergency locator transmitter crashworthiness
According to CARs Part V—Airworthiness Manual, Chapter 551—Aircraft Equipment and Installation, approved ELTs must meet the performance and environmental standards of
1) CAN-TSO-C91 or CAN-TSO-C91a; or
2) CAN-TSO-C126.Footnote 36
According to CAN-TSO-C91a, 121.5 MHz and 243.0 MHz ELTs must meet the performance standards set out in Radio Technical Commission for Aeronautics (RTCA) document RTCA/DO-183: Minimum Operational Performance Standards for Emergency Locator Transmitters—Automatic Fixed–ELT (AF), Automatic Portable–ELT (AP), Automatic Deployable–ELT (AD), Survival–ELT (S) Operating on 121.5 and 243.0 Mega hertz. Likewise, CAN-TSO-C126 states that new 406 MHz ELTs must meet the requirements in RTCA/DO-204A: Minimum Operational Performance Standards for 406 MHz Emergency Locator Transmitters (ELT). According to this document, ELT system design “should provide a reasonable degree of crash survivability”Footnote 37 and be expected to survive a post-crash fire.
The RTCA/DO standards set out a number of specifications for the main unit of an ELT; however, they provide very little direction with regard to the crashworthiness requirements of the antenna and wiring components of the system. The AWM provides some additional direction on this issue, stating that “ELTs must be located and mounted so as to minimise the probability of damage to the transmitter and antenna by fire or crushing as a result of crash impact.”Footnote 38
In the United States, the FAA also requires that 121.5 MHz and 406 MHz ELTs meet the performance standards set out by the RTCA/DO-183 and -204A. In Europe, the European Organization for Civil Aviation Equipment (EUROCAE) acts in a similar capacity to the RTCA by setting out minimum performance specifications for ELTs in ED-62: Minimum Operational Performance Specification for Aircraft Emergency Locator Transmitters 406 MHz and 121.5 MHz (Optional 243 MHz). According to ED-62, “There is no significant difference between this document and DO-204A.”Footnote 39 At the request of the FAA, the RTCA established Special Committee 229 (SC-229) to update DO-204A (creating DO-204B), while EUROCAE created Working Group 98 (WG-98). Both groups were tasked with updating ED-62A (to create ED-62B) and developing a new specification establishing in-flight triggering criteria of ELTs. The RTCA and EUROCAE currently work in coordination in joint meetings, with the participation of the Cospas-Sarsat Secretariat and Cospas-Sarsat participant governments.
With a view to reducing the number of instances in which a potentially life-saving signal does not reach the Cospas-Sarsat satellite system, the investigation examined some possible ways of improving the crashworthiness of aircraft ELT systems. Some of those options are discussed in Appendix C.
1.15.3.5.2 Emergency locator transmitter signal-transmission requirements
According to ICAO Standard 5.3.1.2, “the period between transmissions shall be 50 seconds plus or minus 5 per cent.”Footnote 40 The Specification for COSPAS-SARSAT 406 MHz Distress Beacons (C/S T.001) specifies that beacons should be designed to prevent inadvertent activation. Section 4.5.6 states that, as a means of prevention, a beacon shall not transmit a 406 MHz distress signal until at least one repetition period has elapsed. Therefore, the absolute soonest that a distress signal can be transmitted to the Cospas-Sarsat system following activation is 47.5 seconds. This parameter is referred to as the first-burst delay period. According to Cospas-Sarsat, the first-burst delay was initially designed to allow an internal component, referred to as an oscillator, to stabilize. This delay also evolved into an opportunity for beacon owners to deactivate an inadvertently activated beacon before its first transmission. Modern oscillators do not require as long to reach stability, and modern beacons are often equipped to report their location in the first alert message using an on-board navigation receiver. The Cospas-Sarsat system allows for location calculations from a single burst.
The risk associated with the first-burst delay was previously identified in TSB Aviation Investigation Report A11W0070, which involved an ELT antenna that became submerged before a distress signal could be transmitted to SAR satellites. Likewise, in a 2011 presentation by the Cospas-Sarsat Secretariat, the 50-second first-burst delay was identified as one of the limitations of the current system. Of note, no maximum allowable time is specified for the first-burst delay; this maximum is up to the beacon manufacturer. According to Cospas-Sarsat, there are some beacons in production that have a first-burst delay of 100 seconds. Work is currently being done by Cospas-Sarsat and ICAO to develop requirements for a second-generation ELT system that will offer a number of refinements over the current specifications. Found in C/S G.008: Operational Requirements for COSPAS-SARSAT Second Generation 406 MHz Beacons, these refinements include a first-burst transmission within 3 seconds of activation rather than after 50 seconds. Enhanced accuracy specifications and an in-flight activation capability, much like that in some of the systems currently in use, are also included. At the same time, second-generation ELTs will be required to have the capability to cancel a distress message that has been either transmitted inadvertently or sent intentionally in the belief that an accident was imminent. This feature should result in many fewer false alerts needing to be investigated by SAR personnel. Second-generation ELTs are anticipated to be in service by the end of 2018, with prototypes in operation by 2016 or 2017.
1.16 Tests and research
Several flight instruments were collected and sent to the TSB laboratory for further examination. The instruments sent for examination included
- 2 airspeed indicators
- 1 altimeter
- 1 radio altimeter
- 1 vertical speed indicator.
All of these instruments, with the exception of the radio altimeter, had been damaged by fire. The radio altimeter had visible impact damage. The remaining instruments may also have had some impact damage, but their exposure to the fire had made that impossible to determine.
The radio altimeter recovered from the crash site was from the right side of the cockpit, where the first officer had been seated. The only information yielded by the radio altimeter was that its low-height bug was found at a setting of 150 feet, which was consistent with information obtained from the CVR. Although there was no set procedure in the S-76A SOPs, this low-height bug setting was a common practice among many company S-76A pilots. The altimeter was badly heat-damaged; however, it was possible to determine that it was set to 30.00 in. Hg. Examination of the airspeed indicators and vertical speed indicator provided no reliable information as to their indications at the time of impact.
1.16.1 TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP105/2013—Instrument and Non Volatile Memory Examination
- LP125/2013—Helmet Examination
1.17 Organizational and management information
1.17.1 General
Ornge is a not-for-profit company responsible for the provision of air medical transport to the population of Ontario. To carry out its mandate, Ornge created 2 for-profit corporate entities to oversee the fixed-wing and rotor-wing aspects of the company's EMS mandate. Ornge's fixed-wing operation is Ornge Global Air Inc., and its rotor-wing operation is 7506406 Canada Inc. Although each operation is incorporated, both are operated under the larger Ornge umbrella. These companies do not have formal “doing business as” names; however, they are commonly referred to internally as “Ornge fixed-wing (FW)” and “Ornge rotor-wing (RW)”. To reduce the potential for confusion, this report uses “Ornge FW” or “Ornge RW” when referring to each of these aviation entities, and uses “Ornge” when referring to the senior management team that is responsible for both sides of the company's aviation operations.
At the time of the accident, Ornge FW consisted of 10 Pilatus PC-12s, and Ornge RW consisted of 11 S-76A helicopters and 10 AW139 helicopters. The company had owned 2 additional AW139s that were sold in late April 2013. On the day of the occurrence, only 3 of Ornge RW’s 11 S-76A helicopters were in service. Two other S-76As were undergoing unplanned maintenance. The remaining 6 helicopters were either in heavy maintenance or long-term storage, or were being used for spare parts.
Together, Ornge's fixed-wing and rotor-wing operations have more than 600 employees operating out of 7 dedicated RW bases, 3 dedicated FW bases, and the head office in Mississauga, Ontario. At the time of the accident, the S-76A was operated out of bases located in Kenora, Moosonee, and Thunder Bay, while the AW139 was operated out of Ottawa, Toronto, London, and Sudbury. The company's FW bases are located in Timmins, Sioux Lookout, and Thunder Bay.
1.17.2 History of 7506406 Canada Inc. (Ornge Rotor-Wing)
In 1997, the Ontario Ministry of Health and Long-Term Care (MOH) established an air ambulance program with a single helicopter at the Toronto Buttonville Airport. In 2002, the program grew to include bases in Sioux Lookout, Thunder Bay, Sudbury, and Timmins. In April 2005, Ontario Air Ambulance was incorporated as an independent, not-for-profit organization coordinating all air ambulance services in the province. In July of that same year, the provincial government announced the appointment of the Ontario Air Ambulance Corporation to coordinate all aspects of Ontario's air ambulance program. In July 2006, the organization changed its name to Ornge.
In 2009, Ornge Global Air Inc., which is wholly owned by Ornge, was incorporated and granted a CARs Subpart 703 air operating certificate to operate PC-12-47E aircraft for EMS flights. In 2011, Ornge RW, which is owned by Ornge Global Air Inc., was incorporated and began preparations to assume the Ontario helicopter air ambulance operation, which had previously been contracted out to another Canadian helicopter operator. On 06 January 2012, Ornge RW was granted CARs Subpart 702 and 704 operating certificates for the AW139 helicopters and CARs Subpart 702 and 703 operating certificates for its S-76A helicopter fleet. In addition, it was granted Operations Specification (Ops Spec) 600 to conduct air ambulance operations on both the S-76A and the AW139.
The company's original plan was to employ AW139s at all of the company's RW bases, with the exception of CYMO. For CYMO, the company was considering contracting out the helicopter requirements to a third party. The AW139 implementation, which began in early 2012, was planned to occur base by base. However, implementation was delayed due to logistical issues with the AW139's full ice-protection system, tail-rotor blade airworthiness inspections, and serviceability rates. To ensure an acceptable level of service was maintained, the company then elected to delay the deployment of the AW139s in Kenora and Thunder Bay, and to continue using the S-76As that had been acquired by Ornge Global Air Inc. from the previous operator in 2009. Also in early 2012, Ornge RW abandoned its efforts to find another solution for CYMO, opting to maintain the status quo using the S-76A that was originally stationed there.
Since the decision to delay the AW139 implementation was intended to be a temporary measure until the AW139s' serviceability rates improved sufficiently for them to be used in Kenora and Thunder Bay, the company did not complete any type of risk assessment to determine which bases would benefit most from use of the AW139 versus the S-76. According to the company, transition to the AW139 had already begun at the southern bases, and moving the AW139s to the northern bases would have entailed a considerable amount of additional training. The northern crews would have to be trained on the AW139, while the southern crews, who had already been converted over to the AW139, would have to be requalified for the S-76A.
In the months leading up to September 2010 when the transition from the previous operator to Ornge RW began, the previous operator had recommended, based on installed safety features, the order in which S-76A aircraft should be removed from service upon delivery of the AW139s. However, when the AW139 implementation was delayed, some S-76A helicopters, including the occurrence aircraft, were left in service at their regular operating bases rather than being retired in the recommended order. Ornge did not conduct any type of risk assessment to determine whether or not risk levels could be reduced, either by reintegrating some of the retired S-76A airframes back into service, or by using those retired aircraft as a means to upgrade the in-service airframes that lacked the more modern components.
In 2012, Ornge underwent significant organizational change. In January 2012, the previous board of directors resigned, a new volunteer board was appointed, and an interim chief executive officer (CEO) was appointed. From January to July 2012, a transition team was put in place to establish a new direction for the organization. In December 2012, a permanent President/CEO was appointed, and he assumed duties on 21 January 2013.
1.17.3 Organizational structure at Ornge Global Air Inc.
1.17.3.1 General
At the time of the occurrence, the majority of the senior management team of Ornge FW and Ornge RW came from a predominately fixed-wing background. The only members of the management team with rotor-wing experience were occupying the OM and CP positions at Ornge RW. There was a widespread perception among Ornge RW employees that the senior management at Ornge did not have a full appreciation of the challenges associated with running a HEMS operation, due to their lack of rotor-wing experience.
At the time of the accident, Ornge RW's organizational structure was as shown in Figure 7.
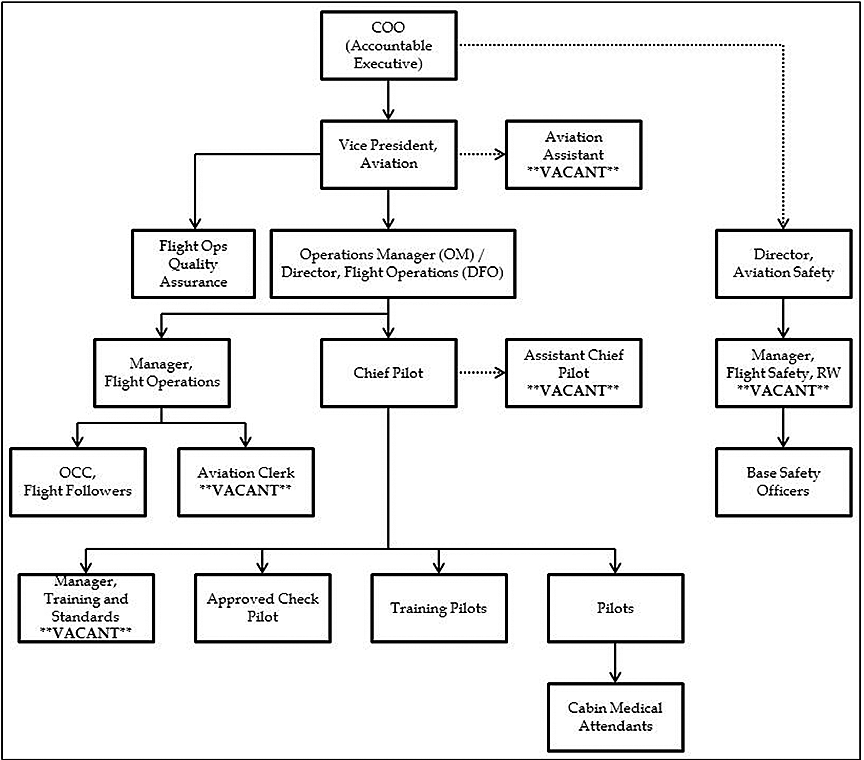
Ornge RW's OM and CP are based at Ornge's head office in Mississauga. These 2 positions are largely responsible for all aspects of Ornge RW operations. Shortly after Ornge RW was granted its operating certificates, there were a number of personnel changes within the OM and CP offices. On 29 February 2012, Ornge RW's OM of that time resigned from the company. The CP of that time assumed the position of interim OM in addition to his CP duties. Then on 31 March 2012, the Chief Operating Officer (COO)/Accountable Executive (AE) resigned, and the company's person responsible for maintenance (PRM) was appointed AE of both Ornge FW and Ornge RW, in addition to his PRM responsibilities. Then on 02 April 2012, the individual who was the OM at the time of the occurrence joined the management team as the Assistant CP. The following month (May 2012), the individual holding both the CP and interim OM positions went on extended leave.
To fill these voids, the company proposed to TC that the newly appointed Assistant CP assume both the interim OM and interim CP positions. On 17 April 2012, less than 1 month after this individual had been appointed Assistant CP, TC approved the company's request to make this person the interim OM, and he was also appointed interim CP by the company. The previous interim OM/CP returned for a couple of weeks in June and then resigned from the company.
On 29 June 2012, the interim OM was appointed full-time to that substantive position and continued to hold the interim CP position. TC had no objections to this dual-hatted appointment, and the OM occupied these 2 positions until 25 April 2013, when the Assistant CP was appointed to the CP position. This individual was the CP at the time of the accident; however, this individual subsequently left the company and later returned as a line pilot.
In December 2012, a new COO/AE was hired. During the period of April 2012 to December 2012, in the absence of a COO/AE, the Vice President (VP) of Aviation, acting as the AE, reported directly to the Acting CEO. Then in January 2013, a CEO/President was hired. Figure 8 depicts the staff changes within some of the key management positions at Ornge RW. Each colour represents a different individual. Interim positions are represented by vertical stripes.
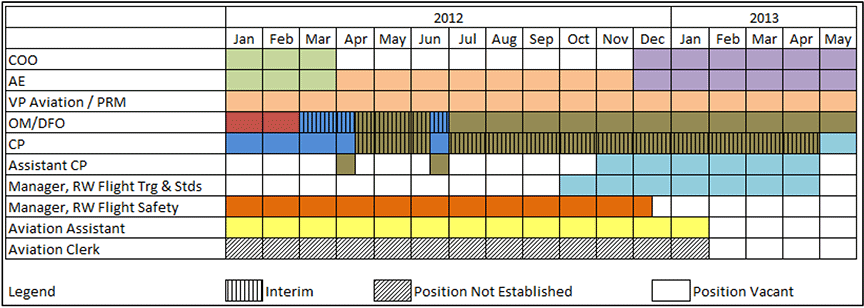
In the fixed-wing and rotor-wing operations, CPs report to their respective OMs, who in turn reports to the VP of Aviation. At the time of the accident, Ornge RW's OM and CP were responsible for more than 80 pilots spread out across the company's 7 rotor-wing bases. In contrast, Ornge FW had an OM, a CP, and a dedicated Training/Check Pilot located at the company's head office. These 3 individuals were responsible for overseeing 45 pilots operating out of 3 bases. The Ornge FW staff provided all ground school, and all simulator and flight training for company pilots, while Ornge RW staff did not provide ground school or simulator training.
1.17.3.2 Vice President of Aviation
According to Ornge RW's COM, the VP of Aviation is also the PRM for Ornge Global Technical Services, which is Ornge's approved maintenance organization. This VP, who reports directly to the COO, is responsible for ensuring compliance with all applicable laws, rules, regulations, policies, and procedures, as well as for developing and maintaining “an organizational framework and structure to provide an effective, safe, secure and sustainable operation.”Footnote 41
At the time of the accident, the VP of Aviation/PRM, who had previously worked for TC, had an extensive background in fixed-wing maintenance, as well as some experience in rotor-wing maintenance.
1.17.3.3 Operations manager
According to CASS 723.07(2)(a) and CASS 724.07(2), the OM is responsible for, among other things, crew scheduling and rostering, training programs, and flight safety, as well as for maintaining qualifications of flight crew. As previously identified in the report, the OM at Ornge RW also fulfills the role of DFO. Section 1.3.3 of the COM states that one of the main responsibilities of the OM is to ensure
[c]ontrol of operations and the operational standards for all helicopters operated through overall direction and supervision of Company Flight Operations and the development of policy governing these functions. He shall ensure that all operations under all licences and certificates held by the Company will be conducted in accordance with the general and specific policies and instructions contained in this Manual, current regulations and standards.Footnote 42
Before joining Ornge RW's management team in 2012, the OM had served for approximately 10 years as a line EMS captain flying the S-76A in Ontario. In addition, the OM was a training captain and an ACP on both the S-76A and AW139 for over 4 years. He had no previous management experience prior to joining Ornge RW's management team.
In the months leading up to the accident, the OM had reached task saturation due to the extreme workload associated with the combined OM and interim CP positions. As a result, he was unable to carry out some of his duties, such as verifying that pilots had the necessary training and qualifications to carry out their roles. The OM and Assistant CP made several requests to Ornge senior management for additional resources to help ensure regulatory compliance of the more than 80 helicopter pilots employed by the company. On multiple occasions, the OM was advised that steps were being taken to acquire additional resources; however, no additional resources were assigned to assist the OM and Assistant CP, so the workload of the double-hatted OM/interim CP continued to increase over the span of more than 1 year.
1.17.3.4 Chief pilot
According to CASS 723.07(2)(b) and CASS 724.07(3), the CP was responsible for, among other things, developing SOPs, implementing all required approved training programs, and issuing directives and notices to S-76A and AW139 flight crews as required. As outlined in Ornge RW's COM, the CP is also responsible for the professional standards and qualifications of the flight crews. The CP supervises the company's training pilots, who are responsible for conducting training in accordance with the TC-approved Training Manual.
The individual who was CP at the time of the accident had been hired by Ornge RW on 15 November 2010, before the company obtained an air operator's certificate. Prior to joining Ornge RW, the CP had flown the Bell 412 in the offshore environment and had owned a helicopter tour operation in the Caribbean. He had no previous EMS experience when he was hired by Ornge RW. Originally, he was hired to fill the CP RW position. Another individual was hired to fill the OM position of the newly formed company. However, during an initial meeting with TC's POI, the POI advised the 2 new hires that they did not meet the qualification requirements in CASS 723 and CASS 724, since they did not possess Canadian ATPL-H licences.
As an interim measure, the CP was appointed to the position of Associate Director of Aviation Business, effective until he completed the steps required to become CP. Although his official title did not reflect it, his role in the certification of Ornge RW was consistent with that of a CP. On 09 October 2012, the Associate Director of Aviation Business became the Manager of Training and Standards; then, at the end of October 2012, he became the Assistant CP. Then in December 2012, having completed his Canadian ATPL-H, he was nominated by Ornge RW to be the company's CP, and a letter of recommendation was signed by the POI. On 20 March 2013, he completed the required TC interview, and on 25 April 2013, he was officially accepted by TC in the capacity of CP.
As highlighted above, one of the CP's primary responsibilities is developing company SOPs. During the course of the investigation, it was determined that the CP lacked familiarity with Ornge RW's S-76A SOPs, experiencing difficulty identifying many of the limitations and procedures detailed in them.
In addition to this lack of familiarity, some of the CP's duties were not being carried out because of the excessive workload associated with that position. In the months leading up to the accident, the OM and CP continued to fall behind on their responsibilities, which made it difficult for them to ensure that the company was compliant with the CARs. For example, the CP experienced considerable difficulty accurately tracking and monitoring the training and qualifications of the company's pilots.
1.17.3.5 Pilot managers
Before the summer and fall of 2012, Ornge RW had pilot managers located at each of its bases. The pilot managers reported directly to the CP, who was also the OM for several months. In addition to their flying duties, each pilot manager was responsible for “the aircraft, personnel and equipment assigned to his Base [sic]”Footnote 43 and “for the safety of the flight operations at his base”.Footnote 44 In essence, the pilot managers were responsible for the day-to-day operation of the base. One of the key aspects of the job was the scheduling of flight crews. Because the pilot managers worked at the base, they knew the base pilots very well and had a very good idea of each pilot's strengths and weaknesses. They used this knowledge when preparing the schedule, to assign crew pairings that offered the greatest safety margin. For example, if a pilot was relatively new to the base, the pilot manager would make sure that pilot was scheduled with a more experienced pilot to help offset that lack of local experience.
On transition from the previous operator, Ornge RW management determined that the base pilot managers were not always effective in providing appropriate oversight. The qualifications of some of the pilot managers prompted a review of these positions. There was a sense among senior management at Ornge that the Ornge RW pilot managers, who had all come over from the previous air ambulance operator, were resistant to Ornge's new direction and brought little value to the operation. A decision was made to eliminate these positions. All but one of the 7 pilot managers were awarded line pilot positions within the company. The remaining pilot manager's employment was terminated.
In mid-June 2012, Ornge Global Air Inc. assumed responsibility for Ornge RW pilot scheduling and implemented a centralized scheduling system like the one already being used for Ornge's FW operation. As this transition occurred, and given the pilot manager positions were being eliminated, many of the pilot manager duties shifted to the CP position, which was being filled by the OM. In addition to receiving those additional responsibilities, the OM became responsible for pilot scheduling under the centralized scheduling model. Given his other responsibilities, the OM delegated pilot scheduling responsibility to the central scheduling department at Ornge Global Air Inc. Ultimately, due to the excessive workload of the OM/CP and the Assistant CP, neither was actively involved in pilot scheduling.
This decision to eliminate the pilot manager positions was not made following any type of formal task analysis to ensure that the responsibilities associated with that position could be properly redistributed to other personnel within the company. Many Ornge RW employees indicated that this change in scheduling methods reduced safety margins, as base-level scheduling had taken into account the experience levels of the pilots to ensure optimum crew pairings. Aside from a rudimentary “green” or “non-green” status, central scheduling did not consider individual differences in experience when populating the schedule. Instead, it simply used the available pool of captains and first officers to fill vacancies as they arose.
1.17.3.6 Line pilots
At the time of the accident, Ornge RW had a budgeted roster for 46 captains and 39 first officers. Between 01 January 2012 and 31 May 2013, 16 pilots had resigned from Ornge RW and 1 pilot had been terminated. Of the 16 pilots who had resigned, 13 were captains, which represented approximately one third of the company's captain roster. During that same period, the company hired 26 pilots (including the occurrence pilots).
Due to the remoteness of Moosonee, Ornge RW has traditionally had difficulty finding pilots who are willing to relocate there. As a means of attracting pilots to work at CYMO, the company allows pilots based there to work on a 2-week-on, 2-week-off rotation. During their off-hours, pilots and medics stay in a dedicated crew house. Each crew member has an individual room in the house. Despite the shift rotation and the provided accommodations, the company has continued to struggle to find pilots willing to work out of CYMO. The company was also experiencing difficulties staffing some of its other northern bases, creating a situation described internally by Ornge as “exceptional levels of downstaffing.”Footnote 45 Follow-up correspondence from the MOH conveyed a notable concern about these staffing shortages, as well as interest in the projected timelines for filling the vacancies. During these exchanges with the MOH in April 2013, Ornge indicated that it had 4 new hires who would be based at Thunder Bay, Kenora, and Moosonee. The captain involved in the occurrence was one of the 4 pilots referred to in this correspondence.
To overcome the high turnover rate among captains at Ornge RW since January 2012, the company hired contract part-time captains, like the captain involved in the occurrence, to fill in during periods when there were personnel shortages. Some company pilots were also given the opportunity to work overtime at one of the bases experiencing personnel shortages, if they were interested in working additional shifts.
1.17.3.7 Vacant management positions at Ornge Rotor-Wing
At the time of the accident, a number of key positions were vacant at Ornge RW. These vacancies will be discussed below.
1.17.3.7.1 Manager, Rotor-wing Flight Safety
The Manager of RW Flight Safety position became vacant on 17 January 2013. This is 1 of 5 positions within the company's aviation safety department reporting directly to the Director of Aviation Safety. According to the COM, one of the responsibilities of this manager is “monitoring and detecting items of significant flight operations concern, and to provide an oversight level of flight safety as it relates to flight operations.”Footnote 46
1.17.3.7.2 Manager, Rotor-wing Flight Training and Standards
The position of Manager of RW Flight Training and Standards was vacant at the time of the occurrence. One of the responsibilities of this position is to “ensure attendance at all training is tracked and verified and all records are completed fully and properly entered in the training records.”Footnote 47 These duties include ensuring that all regulatory and company training requirements are met before a pilot is released for operational duty.
This position was filled from October 2012 to April 2013 by the Assistant CP, who then assumed CP duties on 25 April 2013. However, this individual was also required to continue carrying out the duties of Manager of RW Flight Training and Standards.
In late 2012, an Aviation Assistant was assigned to assist with the duties of Manager of RW Flight Training and Standards by ensuring that training files were kept up to date. The Aviation Assistant position became vacant following the January 2013 program validation inspection (PVI),Footnote 48 and was not filled. Therefore, the Assistant CP assumed these duties.
1.17.3.7.3 Aviation Clerk
The position of Aviation Clerk was created following the January 2013 PVI to reduce the workload on the OM and CP. The major responsibilities associated with this position were to ensure that all training was tracked and verified, and to ensure that all records were completed fully and properly entered in the training records. However, at the time of the accident, that position had not been filled, so these duties remained with the CP.
1.17.4 Scheduling at Ornge Rotor-Wing
According to Ornge's Performance Agreement with the MOH, “for Dedicated Aircraft emergent and urgent Calls, if the Dedicated Aircraft is fuelled, the pilot-in-command will request Air Traffic Control clearance within 15 minutes of the pilot-in-command's acceptance of the Call.” If the aircraft requires fuel, the maximum permissible time increases to 25 minutes.Footnote 49
However, Ornge RW has a legacy off-site night-shift standby posture outlined in its COM. According to Ornge RW's COM, during off-site staffing hours, crews are required to be able to respond within 1 hour of the PIC's acceptance of the call. Although there is no reference to night-shift standby in the Performance Agreement with the MOH, Ornge RW's Moosonee base operates on an off-site standby posture from 1900 to 0700. During that time, pilots remain at the local crew house in the town of Moosonee and, if required, are expected to report within one hour. In light of Ornge RW's off-site night-shift standby posture and the fact that Ornge RW pilots are permitted to conduct day scene callsFootnote 50, the company places a higher priority on ensuring that day shifts are staffed. Given that the company does not conduct night scene calls, it was felt by Ornge management that FW resources could be used to provide supplemental coverage when night RW shifts are unstaffed.
During the year preceding the accident, Ornge RW experienced a large number of unstaffed shifts due to personnel shortages as a result of short-term illnesses and pilot resignations. In the 3 months preceding the accident, Ornge RW experienced the down times at CYMO as a result of pilot shortages (Table 4).
| Month (2013) | Days | Nights | Total | |||
|---|---|---|---|---|---|---|
| Hours | % | Hours | % | Hours | % | |
| May | 4.0 | 1 | 171.5 | 46 | 175.5 | 23.6 |
| April | 7.2 | 2 | 252.0 | 70 | 259.2 | 36.0 |
| March | 41.8 | 11 | 132.0 | 35 | 173.8 | 23.4 |
| Total | 53.0 | 5 | 555.5 | 50 | 608.5 | 27.6 |
In an effort to address pilot shortages at CYMO and other bases, Ornge RW would sometimes use augmentee pilots from other bases to fill gaps in the schedule. A review of Ornge RW's schedule over the year preceding the accident revealed that, in some cases, augmentee pilots from other bases went directly onto night shift without first having flown at that base during the day. The investigation determined that concerns had been raised by company employees about new hires being scheduled to start immediately on night shift. Concerns were also raised about augmentee pilots from another base being paired and creating a green-on-green situation. In correspondence with the Manager of RW Flight Safety of that time, and copied to the OM/interim CP, the base safety officer at CYMO reported that safety was being jeopardized for the sake of filling empty slots, citing an instance in which 2 new hires were scheduled to start immediately on night shifts. In that correspondence, the pilot raising the concern wrote that “the holes in the Swiss cheese are starting to line up.”Footnote 51
In a response to the base safety officer, copied to the OM/interim CP, the Manager of RW Flight Safety indicated that he did not like the idea of having a pilot's first departure be one from Moose Factory as a southwest-bound black-hole scenario, due to the challenges associated with such a departure. The OM/interim CP advised the concerned individuals in response that the new pilots had completed all of the required training, and the schedule was not changed.
Although Ornge RW did not have a fully functioning SMS at the time of the accident, and one was not required by regulation, the company provided its employees with SMS training. In an Ornge SMS training presentation titled Safety Management System Fundamentals 2013, it is stated that the employee's role is to “report openly all hazards and incidents”Footnote 52 to help avoid future incidents and for trending purposes. The presentation also outlines the company's requirement to report “every accident, occurrences or hazards arising in the course of or in connection with your work”Footnote 53 via aviation safety reports (ASR). However, despite this requirement, these pairing concerns were not entered into the company's ASR system and were not brought to the attention of the Director of Aviation Safety.
Less than 1 week after the accident, an ASR was filed by a company pilot regarding the scheduling of 3 new pilots immediately on night shifts for their first block of shifts. One of the 3 pilots was scheduled to be the PIC. In the report, the originator indicated that it was unacceptable and unsafe. In its root cause analysis, the company identified that the schedule system needs improvement and that there were no documented policies requiring a new pilot to be scheduled for day shifts only until approved for night operations. The schedule was rescinded, and a revised schedule was published with the newly hired pilots starting on day shifts.
1.17.5 Company operations manual
1.17.5.1 General
The COM, dated 25 April 2013, was approved by TC on 02 May 2013. According to the preamble in the COM:
The standards, practices, procedures, and specifications laid down reflect Company operating policies and are in accordance with the regulations of Transport Canada. Adherence with the provisions contained is mandatory.Footnote 54
The following section outlines several of the policies and procedures in the COM that are relevant to the investigation.
1.17.5.2 Crew qualifications, experience, and recency
Section 2.2 of the COM states that a captain must possess a valid PPC to “Captain standards on type” in order to act as a PIC, and that a first officer must possess a valid PPC to second-in-command (SIC) or PIC standards on type.Footnote 55 However, the COM provides no details about what constitutes PIC or SIC standards.
In addition to requiring a valid PPC on type, Ornge RW's COM states that prior to acting as PIC with passengers on board, a pilot shall have completed all company training in accordance with the company's TC-approved Training Manual. In some instances, companies may implement requirements that go beyond the regulatory requirements as a means of enhancing flight safety. However, by including more stringent requirements in a TC-approved Training Manual or COM, the operator then becomes bound by regulation to meet those requirements.Footnote 56 Under the CARs, if a company then fails to meet those requirements, then it is no longer in compliance with regulation and could be subject to enforcement action.
Ornge RW had included several requirements in its TC-approved COM and Training Manual that exceeded the requirements outlined in the CARs. Some of those additional requirements will be discussed in the next several sections of this report. It was discovered during TC oversight activitiesFootnote 57 and during the TSB investigation that Ornge RW had both knowingly and inadvertently deviated from some of these requirements. For example, there were repeated instances identified by TC in which Ornge RW pilots were not completing practical CFIT-avoidance training in accordance with the TC-approved Training Manual. In addition to these training deficiencies, the company was not following the procedures it had established in its COM related to the use of direct-entry captains and the tracking of first officer progression, both of which are discussed in greater detail later in this report.
Ornge RW's COM echoes the regulatory requirements listed in CARs 703.88 and 704.108 for takeoffs and landings, stating that prior to acting as PIC or SIC, a pilot shall have completed at least 3 takeoffs and landings (day or night) on type within the previous 90 days. It also lists the requirements found in CAR 401.05(2), which state that in order to carry passengers, a pilot must have completed the following in the previous 6 months:
(A) five night or day take-offs and five night or day landings, if the flight is conducted wholly by day, or
(B) five night take-offs and five night landings, if the flight is conducted wholly or partly by nightFootnote 58.
1.17.5.3 Operational progression
Section 2.3 of Ornge RW's COM outlines first officer operational progression in order to become a captain. The process, intended to provide “a safe progression into full flight operations”,Footnote 59 involves a gradual reduction in restrictions as a first officer.
Ornge RW's operational progression process has undergone some revision since the inception of the company. The original COM was approved on 06 January 2012. That COM outlinedFootnote 60 the following steps for the operational progression of first officers:
- A first officer who has less than 50 hours of experience at the company is restricted to non-flying duties (i.e., left seat).
- Once having gained more than 50 hours of operational experience with the company, a first officer may be permitted to conduct flying-pilot duties with a training pilot or ACP, at the discretion of the training pilot or ACP.
- A pilot with less than 1000 hours in total of helicopter flight experience will undergo 1 hour of flight training in PF duties once reaching 100 hours of operational flight experience. Upon successful completion of this training, the first officer will be permitted to conduct flying-pilot duties at the discretion of the PIC.
- A pilot with more than 1000 hours in total of helicopter flight hours requires at least 75 hours of operational experience to meet the requirements for the additional training and subsequent approval to conduct flying-pilot duties with any PIC.
On 24 September 2012, Ornge issued Flight Operations Directive (FOD) 031: Minimum Requirements to Occupy Right Seat. According to the company, the intent of this FOD was to clarify the requirements in the COM, to ensure retention and improvement of flying competency, and to allow newly qualified first officers to fly from the left seat immediately upon starting their first shift. The new process outlined in FOD 031 was as follows:
- After accumulating 25 hours of operational experience, First Officers will be permitted to fly from the right seat with a Flight Standards Training or Check Pilot at their discretion.
- After accumulating 50 hours of operational experience, First Officers will receive a minimum of 1 hour of operational type training from the right seat. This training is to review the Takeoff and Landing profiles as detailed in the SOPs. First Officers who undergo this recurrent training must satisfy the training pilot that they have full understanding of aircraft procedures and systems as it relates to normal and abnormal situations.
- After having received the above noted training, First Officers are authorized to fly the aircraft from the either seat [sic] and assume all the duties of the PF at the discretion of the Captain.Footnote 61
On 25 April 2013, TC approved a new COM to reflect the appointment of the new OM. The operational progression process in the original COM had not been amended to incorporate the changes associated with FOD 031. Instead, this section contained the same operational progression process from the original, 06 January 2012 version. According to Ornge RW, the company had a process in place to ensure that FODs are addressed in one of the company's publications prior to being rescinded. However, there was no process in place to ensure that FODs were incorporated into the next revision/amendment of the COM. According to the company, the responsibility for incorporating FODs rested with the OM. The company indicated that a quality assurance audit had not identified this situation as a systemic issue, despite the fact that it could result in information being published in a COM that had been superseded by a previously issued FOD. As a result, the 25 April 2013 COM contained an operational progression process that was 19 months out of date at the time of publication.
At the time of the accident, Ornge did not have a formal mechanism in place, such as a training record, to track the operational progression of its first officers. Instead, the onus was placed on first officers to track and facilitate their own progression, and to request a right-seat checkout once they had gained the required operational experience. At that point, a first officer's experience was then verified by the OM and the CP. Since operational progression was not tracked in a systematic fashion, there was no way for captains to easily verify the operational experience of a first officer, short of contacting the OM or CP to verify whether the first officer had met all of the requirements for conducting flying-pilot duties from the right seat.
According to Ornge RW, the first officer involved in the occurrence had completed the 1 hour of operational training from the right seat. However, there was no record of it in the first officer's training files, and the company was unable to produce any documentation confirming that the training had been completed. Investigators determined that this was not an isolated incident. In some cases, Ornge RW was able to provide email correspondence from training pilots confirming that training had been completed. In several cases, however, this information either did not make its way into a first officer's training file or the information was nonexistent.
1.17.5.4 Direct-entry captains
In addition to the operational progression process for first officers, section 2.4 of Ornge RW's COM contains a procedure to be followed for direct-entry captains. Although not formally defined in the COM, a direct-entry captain is one who is hired directly into a captain position, rather than a first officer who has been promoted from within the company. Although not required to do so by regulation, Ornge had implemented this procedure as a risk mitigation measure, to ensure that newly hired captains were given the opportunity to learn the operation before they were employed for operational flights as PICs. According to senior management at Ornge, this procedure was introduced by a previous OM specifically to reduce the risks associated with hiring contract pilots to temporarily fill captain positions. The direct-entry captain requirements, as outlined in the COM, are as follows:
- Qualified direct entry captains will fly as a second-in-command for a minimum of 50 hours on line operations.
- This will include 5 hours of night operations including at least 3 black hole approaches.
- After 50 hours they will be given a line assessment by an ACP prior to being cleared to fly as a captain. Once cleared, the ACP will place a letter on his training file approving him to conduct line operations as a captain.Footnote 62
The investigation determined that the company was not following the direct-entry captain procedure. The procedure was not followed in the case of the captain involved in this occurrence because he had been assessed as a non-direct-entry captain based on his experience and qualifications. Investigators ascertained that at least 9 pilots had been hired by Ornge RW directly into captain positions without having first completed the direct-entry captain requirements outlined in the COM.
Ornge RW management had exercised judgement and discretion in the application of section 2.4. The decision was based on the fact that these pilots each had previous EMS experience, held a valid PPC on type, and met the company's minimum experience requirements to be employed as an EMS captain. In the case of the captain involved in this occurrence, the OM had sought advice regarding his suitability for employment as an S-76A captain from a former CP/ACP of the operator that had previously provided helicopter air ambulance services in Ontario. The OM had received a strong endorsement of the captain from the individual in question, and therefore had no reservations about employing him immediately as an S-76A captain. According to Ornge, no external forces, such as pilot shortages or pressure from the MOH, had influenced the decision to treat these new-hire captains as non-direct-entry captains rather than following the direct-entry captain procedure in the COM.
The company indicated that careful consideration had been given to each of the 9 pilots who did not follow the direct-entry captain procedure. However, it was unable to provide any type of documentation associated with the decision to bypass the direct-entry captain requirements. In the case of the occurrence captain, Ornge RW was unaware of his extremely limited night and instrument flight experience over the previous 24 months, and that he had not completed any unaidedFootnote 63 night flying in that period, when the company decided to employ him as an EMS captain at CYMO. Likewise, with respect to the other 8 pilots who did not follow the direct-entry captain requirements, there was no indication that the company took into consideration such things as time away from the role or whether or not the pilots had sufficient recent unaided night and instrument flight hours to be able to respond to any mission that could be expected of an EMS captain at the company.
1.17.5.5 Flight duty time
To help reduce the risk of pilot fatigue, limitations on flight duty time have been put into the CARs, and are often included in a COM. According to the CARs, the standard flight duty time limitation is “14 consecutive hours in any 24 consecutive hours.”Footnote 64 However, there are provisions that permit non-scheduled air taxi or aerial work operations to extend the maximum flight duty time to 15 consecutive hours if the minimum rest period is increased by 1 hour or if the maximum flight time does not exceed 8 hours in any 24-hour period. Ornge RW has Operations Specification (Ops Spec) 093, which authorizes the increase in flight duty time to 15 consecutive hours as long as the conditions listed above are met.
Section 2.9.1 of the COM states that flight duty time includes the total time from when a flight crew member first reports for duty or begins holding standby and finishes when the engines are shut off or the rotors stopped on the final flight.Footnote 65 However, that section also states that performance of work-related duties prior to reporting time is considered as flight duty time as well.Footnote 66 The intent of this requirement is to ensure that flight crew members get adequate rest, by way of restricting the amount of work that is permitted over the course of a day. According to regulation, a rest period is one in which a flight crew member is free from all duties, and the minimum rest period permitted shall ensure that a flight crew member has the opportunity to obtain not less than 8 consecutive hours of sleep.Footnote 67 According to one of the presentations provided to the captain during his company indoctrination training, “It is the responsibility of the flight crew members to use rest periods provided to obtain the required rest and shall ensure [sic] that they are adequately rested before reporting for flight duty.”Footnote 68
During the course of the investigation, a number of pilots and medics described activities such as work-related email correspondence as an activity that would start a flight crew member's duty period, affecting flight duty time limitations.
1.17.5.6 Ornge's operational control system
Ornge RW employs a Type C operational control system, in which the pilot self-dispatches and has sole authority to make decisions regarding the initiation, continuation, delay, diversion, or re-routing of the flight when conditions are such that operational decisions are necessary. Flight following for a Type C operational control system involves “monitoring of a flight's progress, the provision of such operational information as may be required by that flight, and the notification of appropriate air operator and search-and-rescue authorities if the flight is overdue or missing.”Footnote 69
1.17.5.7 Flight preparation
Section 4.2 of Ornge's COM states that the captain is responsible for ensuring that licences and ratings of the assigned flight crew are valid. However, there is no system in place at Ornge RW to assist captains so that they can verify that a first officer has completed all of the required training and meets the regulatory currency requirements.
1.17.6 Pilot recency tracking/monitoring at Ornge
Section 3.7.8 of Ornge's Flight Following Manual requires that pilot takeoffs and landings be recorded to track currency requirements. Flight followers are required to check the “Alerts and Exceedances” section of the AvAIO software option upon commencing each flight-following shift. If an alert or exceedance cannot be immediately resolved, the flight follower must communicate the problem to the crew planner/scheduler and/or to the CP.
According to Ornge, the Flight Following Manual was written before the establishment of central scheduling, when flight followers were responsible for checking the Alerts and Exceedances page in AvAIO. When Ornge switched over to central scheduling, that department assumed the duties of checking the alerts screen to ensure that all documents (such as medical certificates, instrument ratings, and PPCs) were current. However, central scheduling did not adopt the procedure to verify pilot currencies prior to scheduling pilots for flight duty, despite the company's issue in October 2012 of FOD 019: Minimum Rest Period, which stated that day and night takeoff and landing data must be tracked to ensure regulatory compliance. The central scheduling department was not using that function of their scheduling software, and there was no other layer of supervision at the bases to monitor pilot currencies.
The AvAIO was originally designed as a CARs Subpart 705 fixed-wing software solution. Ornge had decided to migrate it over to the rotor-wing side of the operation. Following the roll-out, a number of flaws were discovered in relation to the way in which information was recorded.
Consequently, Ornge was not ensuring that its pilots had met all of the required currencies (i.e., takeoffs, landings, and night requirements) prior to scheduling them for operational duty. Instead, the onus to do so was placed on the pilots. Although the company's scheduling software had the capability to warn of expired currencies or upcoming expiry dates of training and/or currencies, that function had not been activated at the time of the accident.
A review of AvAIO information was carried out, which determined that some of its data were not accurate. Specifically, AvAIO was not being updated to reflect the takeoffs and landings completed during simulator training and, in other instances, takeoffs and landings were understated as a result of software limitations. In particular, the system was unable to track more than 1 takeoff and 1 landing per flight, since that is the norm for an airline operation. Information in the system at the time of the accident showed that 14 of 28 company S-76A pilots had not completed at least 3 night takeoffs and night landings in the previous 90 days. It also showed that 13 out of the 28 pilots had not completed at least 5 night takeoffs and night landings in the previous 180 days. However, further review revealed that all but 2 of the 28 S-76A pilots had met the 180-day currency requirements for night takeoffs and night landings. These 2 pilots did not operate at night.
On the AW139 side of Ornge RW's operation, a similar situation was discovered, albeit on a smaller scale. In the case of AW139 aircrew, 2 of the more than 50 pilots had not completed at least 3 night takeoffs and night landings in the previous 90 days, despite a stipulation by the company's AvAIO report that this was a minimum requirement. The report indicated that all of the active pilots on Ornge RW's AW139 roster had met their 180-day currency requirements for day and night takeoffs and landings.
During the investigation, the company provided feedback related to some of the deficiencies that were noted. According to Ornge RW, pilot records were disorganized and not user-friendly, and the company did not have a way of tracking pilot qualifications, making it possible that unqualified pilots would be scheduled for duty. Likewise, the company was not tracking pilot currencies to ensure regulatory compliance.
The investigation determined that none of the issues outlined in this section had been identified previously during internal company audits or through the company's ASR system.
1.17.7 Safety management system at Ornge Global Air Inc. and Ornge Rotor-Wing
1.17.7.1 General
Although not required by regulation to do so, Ornge voluntarily began implementing an SMS into its fixed-wing and maintenance operations in November 2009, and SMS implementation began in Ornge RW in December 2011. Because of the two-year head start, SMS implementation was much further ahead in Ornge's fixed-wing operation than in its rotor-wing operation. According to company documentation, SMS implementation was 88% complete on the fixed-wing side of the operation versus 27% complete on the rotor-wing side at the time of the accident. Ornge RW's COM stated that the company was an SMS transitioning enterprise.Footnote 70 However, at the time of the accident, neither Ornge FW nor Ornge RW had fully implemented a TC-recognized SMS or had been granted transitioning SMS company status by TC.
1.17.7.2 Reporting procedures
The Ornge Aviation Corporate Safety Manual,Footnote 71 which covers the company's FW, RW, and maintenance organizations, states that “an employee will not be subject to disciplinary action or reprisal for reporting hazards or occurrence [sic]”Footnote 72 unless it involves substance or alcohol abuse, criminal acts, deliberate misconduct, or failure to report an event within a reasonable time frame, or unless it is determined that an employee deliberately misrepresented the facts in a report.
Themanual also advises that de-identified, completed investigation reports may be circulated for the purpose of improving safety. This practice is consistent with guidance provided in TC's Safety Management Systems for Small Aviation Operations—A Practical Guide to Implementation (TP 14135), which encourages feedback to company employees in a “rapid, accessible and informative”Footnote 73 manner, so that employees are aware of any safety issue that may arise and will be better equipped to deal with that issue should it arise again. The practice also sends a message to employees that the company is actively seeking to address such issues. In Ornge's operations, completed safety investigation reports were not distributed to line personnel. However, the company's safety department published short safety summaries as a means of communicating with company employees.
TC advocates that safety information be shared within companies to encourage development of an appropriate safety culture and to share both lessons learned and corrective measures. However, the Department also indicates that companies may choose not to share an entire report due to sensitivity and privacy issues. At Ornge RW, one of the summaries used to transmit information is called the 360 Feedback report, and it is distributed quarterly to line personnel. Ornge also produces Looking Back reports, which are editorials written by company pilots and engineers for “the purpose of sharing lessons that have been learned through their own experiences.”Footnote 74 Looking Back reports are published when they are deemed appropriate from a learning standpoint.
1.17.7.3 Risk assessments
Ornge employs risk management principles to address corporate risk concerns, which range from issues related to corporate culture to operational issues such as night flying. However, the company does not have an established risk management process for flight crew or the OCC to determine whether the risks associated with a proposed trip are acceptable, and such a process is not required by regulation. Instead, OCC's decision to use an air ambulance asset is based on the following criteria:
- the distance between facilities is greater than 240 kilometres;
- specialized transport team is required;
- the mission is time-sensitive because the patient requires prompt attention;
- geographic considerations;
- scene call; and
- special circumstance.
In accordance with Ornge's COM, patient condition is never used as a factor in the decision to decline or accept an assignment. All medevac requests are assessed based on the criteria listed above. Pilots are advised by the OCC of a potential flight and asked whether the weather is suitable for the flight. If the pilots determine that the weather is acceptable, they normally accept the flight. The decision not to provide patient condition information to pilots is a fairly common practice among EMS providers. Its intent is to prevent a pilot from accepting an unacceptable level of risk because of the patient's condition. A night VFR flight in a remote location with marginal weather, for example, presents a higher level of risk than a similar mission during daylight hours in clear skies. If the crew of that night mission lacks experience or proficiency, the risk associated with that flight will be considerably higher than it would be if it were a daylight flight. In some situations, the best course of action may be to delay a launch until daybreak to reduce risk to an acceptable level. According to Ornge's OCC, the occurrence flight was deemed a regular or routine night mission for CYMO flight crews. However, the OCC did not take into account—and did not have any type of risk management tool to take into account—the weather at the time, aircraft configuration, or crew composition.
At Ornge RW, night scene calls are not permitted due to the increased risk associated with that type of mission. According to Ornge, the decision to prohibit night scene calls was not based on a formal risk assessment.
In some countries, risk management tools are provided to pilots as a way of ensuring that the risks associated with a particular flight are included in a pilot's decision-making process. For example, the National Emergency Services Pilots Association in the United States makes a risk assessment matrix available on line, which allows pilots to assign numerical values to various risk factors, such as geography, adverse weather, crew fatigue, experience levels, equipment, etc. Likewise, the Helicopter Association International offers its members access to a free online Flight Risk Assessment tool that users are able to customize to meet their unique operational and environmental needs. In organizations that employ a risk management matrix of some type, different risk levels usually require different levels of authorization. For example, if the risk is scored as low, the pilot may be able to self-authorize. However, if the risk score is too elevated, it may be necessary to have the flight approved by an on-duty manager, the CP, or perhaps the OM. This type of process is designed to ensure that risk levels are accepted at the appropriate level within an organization and to help pilots consider the overall risks associated with a particular mission prior to launching.
When Ornge RW began operations, it inherited a long history of experience that had been gained by many of the managers and senior employees who moved over from the previous operator. One piece of history that was not forgotten in the transition to Ornge RW was a 2008 accident involving the previous operator. As Ornge RW prepared to take over, there were some internal discussions about whether or not to adopt NVGs for its night operation. The senior management of Ornge at the time decided not to adopt NVGs, since Ornge RW would not conduct night scene calls. One of the major reasons cited against NVG implementation was the cost of retrofitting the AW139 aircraft, which had not been purchased with the NVG-compatible cockpits, together with the costs associated with modifying the aging S-76A fleet. No formal risk assessment was conducted at the time this decision was taken.
In February 2013, Ornge initiated a risk assessment of black-hole approaches. During that process, it was identified that night enhancement technology and additional lighting options required further review. However, NVGs were still considered at that time to be cost-prohibitive and, as such, were not considered in depth.
1.17.7.4 External audit of 7506406 Canada Inc. (Ornge Rotor-Wing): December 2012
It is common practice in industry for companies to hire private contractors for auditing purposes as a way of obtaining an unbiased report on the status of a company. In preparation for TC's January 2013 PVI, Ornge RW hired a third-party provider to conduct an on-site audit to determine whether the company's rotor-wing operation was in compliance with CARs Subparts 704 and 706, CASS 724 and 726, and the Standards and Requirements for Government of Ontario Approved Air Operators. The audit was conducted from 05 to 07 December 2012, through interviews with key personnel, review of approved documents, sampling of relevant records, and random inspections throughout Ornge RW's system. The audit report stated that Ornge was capable of providing RW air services to a “highly professional standard”.
A major component of the audit report is a section titled “Risk Management”, which is broken down into functional and mission areas. The audit found that Ornge RW's management systems conformed to the policies and procedures contained in its COM and Maintenance Control Manual. The report did not identify that senior management at Ornge RW had limited rotor-wing experience, that key management positions were not filled, and that other management positions were being filled in an acting capacity.
In the aircraft type and pilot experience categories of its audit, the third-party provider assigned Ornge RW the lowest possible hazard scores, indicating that those areas had low risk levels. According to the audit report, weather extremes represented a high risk to the company.
The report identified 4 issues that needed to be addressed by Ornge RW; however, none of them were considered major non-compliance issues. The audit findings were related to amendment procedures in the COM and company SOPs, the list of effective pages in the COM, and the procedure in the COM for refueling with patients on board. Hence, the December 2012 audit conducted by the third-party provider led Ornge to believe that its RW operation was ready for TC's January 2013 PVI.
1.17.8 Flight operations directives
1.17.8.1 General
Ornge RW uses FODs to introduce changes in policies or procedures, and as a way of amending the COM in a timely manner rather than waiting until the next time the COM is updated. FODs are distributed to employees electronically via Ornge's electronic bulletin system called QPulse, and are effective immediately upon issue. According to Ornge RW's COM, future amendments to the COM “will encompass these directives and they will be rescinded, removed from the manual and tracked in the listing of Effective Flight Operations Directives.”Footnote 75 However, as previously identified in this report, this process was not always being carried out.
According to the COM, section 3.11, “any information which impacts regulatory approvals will be communicated to the TC POI prior to issue. Some examples are fuel policy or landing limits. If there is a question whether approval is required then the TC POI will be consulted.”Footnote 76 This passage is consistent with CARs 703.104(4) and 704.120(4), which require TC to approve any changes to a COM that are related to a regulatory requirement. However, the investigation showed that the FOD approval process was not fully understood nor consistently followed, and that there were different interpretations of the process by Ornge personnel prior to the accident.
During the early stages of the investigation, the company indicated that under the currently approved Ornge RW COM, FODs were not required to be approved by TC. However, in February 2013, an FOD had been forwarded, via email, to the POI for approval because it affected “operational policies/procedures”. During a subsequent exchange with investigators, the company indicated that the process had changed following the accident, and that a new procedure had been requested by and agreed to with TC, whereby TC would approve all newly issued FODs prior to distribution to company flight crews. In the latter months of the investigation, the company indicated that the process had always been that all FODs were to be approved by TC prior to dissemination to flight crews. Nevertheless, the investigation disclosed that on more than one occasion, FODs that affected the contents of the TC-approved COM or the Training Manual had been published prior to approval by TC. In some cases, TC was advised of the FOD after it had been distributed within the company. These inconsistencies in the approval process occurred both prior to and following the accident.
1.17.8.2 Flight Operations Directive 039: Black Hole Operations
On 24 January 2013, Ornge RW issued FOD 039: Black Hole Operations. In this directive, the company stated that steps were being taken “to ensure that all future night training emphasizes the principles of risk management where little or no cultural or ambient light exists” and “to minimize the risk of controlled flight into terrain (CFIT) by maximizing height over distance.”Footnote 77 It outlined several initiatives that the company had undertaken, some of which were:
- Development of improved Black Hole proficiency guidelines.
[…]- Development of flight following software to track night and black hole events to ensure proficiency and currency.
[…]- An enhanced CFIT training program, specifically focusing on our operating environment, is being developed. Included will be revised SOP profiles/call outs, EGPWS and escape maneuvers techniques applicable to the S76[A] and A[W]139.
- Reassessment of the current simulator training program to include CFIT, black hole and low visibility procedures.Footnote 78
The FOD also advised flight crews that if they had not received annual recurrent black-hole operations training in the past year, they had the OM's approval to decline calls at night to any of the designated black-hole locations, which were listed in the directive. Like the other certified aerodromes with lit runways employed by Ornge RW, CYMO was not included in the company's list of designated black-hole locations.
1.17.8.3 Flight Operations Directive 034: Green on Green
On 15 October 2012, Ornge RW issued FOD 034 (Revision 0): Green on Green as a direct result of concerns raised by senior company pilots to the OM. Ornge RW did not complete a formal risk assessment to assess the level of risk associated with the identified concerns or to determine the residual risk that would remain as a result of FOD 034. The identified hazard was also not captured by the company's SMS.
According to FOD 034 Revision 0, the new policy prohibited green-on-green pairing of pilots. Specifically, the policy was introduced to prevent new first officers from flying with new captains or with transient captains who were unfamiliar with the operation. The FOD stated the following:
- No green pilots will be scheduled to fly together on any operational shifts.
- Unless the scheduled First Officer has at least 6 months of operational experience at that base, Green Captains who are scheduled to fly at a different base will have a preceding day scheduled to receive a proper orientation.
- New First Officers will be given an orientation of their base prior to any shift assignments.
- Flight Standards reserves the right to extend the “Green” time requirement of any pilot.Footnote 79
The FOD included the following definitions:
- Green First Officer: A First Officer who has less than 6 months current operational experience.
- Green Captain: A Captain who has less than 3 months current operational P.I.C. command experience. This definition also applies to any Captain qualified First Officer.
- Green Pilot: Any pilot who has no operational experience at the specific base, or who has not operated from that base within the last 3 months.
- Orientation: Training provided by a Flight Standards Training Pilot or another designated Senior Captain involving daily duties, paperwork, base procedures and aircraft familiarization.Footnote 80
Based on the definitions in FOD 034 Revision 0, the occurrence captain would have been considered a green pilot when he arrived for his first shift at CYMO in April, since it had been more than 3 months since he had last flown out of CYMO. The first officer had approximately 8 months of operational experience at the CYMO base, so he was no longer a green first officer in accordance with FOD 034 Revision 0.
On 28 February 2013, Ornge issued Revision 1 of FOD 034. In this revision, some of the green criteria were removed. In particular, FOD 034 Revision 1 stated:
- No Green Pilots will be scheduled to fly together on any operational shifts.
- Green Captain/Green Captain, or Green Captain/Green First Officer shall not be paired together.
- An orientation shall be provided to a Green Pilot.
- The company reserves the right to extend the “Green” time requirement of any pilot.Footnote 81
The revised FOD included the following definitions:
- Green Captain: Any Captain with less than 50 hours operational line experience on type, or a newly upgraded Captain, or a Captain-qualified First Officer with less than 50 hours' operational line experience on type as Captain and who has not been cleared of his “green” status by the company.
- Green Pilot: A pilot without any previous operational experience at a specific base.
- Green First Officer: A First Officer with less than 50 hours' operational line experience.
- Orientation: Familiarization briefing provided by a company designate; involving specific base operations.Footnote 82
Revision 1 of FOD 034 introduced 3 significant changes to Revision 0. Most noticeably, the revised directive removed the requirement for a company pilot to have operated from a specific base during the previous 3 months. With the introduction of Revision 1 of FOD 034, a pilot would not be considered green as long as that pilot had previous operational experience at that specific base, no matter how long ago it was. During the investigation, however, Ornge RW indicated that the requirement for “previous operational experience at a specific base” was met by completion of the aerodrome and area of operation qualification training ground briefing. According to the company, no flying is required.
The investigation revealed that pilots had raised concerns with the OM and the Director of Aviation Safety about this change to the definition of a green pilot, citing that it was “too vague” and that it had the potential to create a situation that “is uncomfortable and unsafe.”Footnote 83 One pilot suggested that a time frame for previous operational experience be included, as per the FOD 034 Revision 0. The OM responded to this concern by stating that a planned “aggressive black hole training program”, coupled with FOD 039 (Black Hole Operations), would hopefully leave them in “very good shape.”Footnote 84 As with the concerns that had been raised about new hires going immediately onto night shift, this issue was not submitted via Ornge's ASR system, so the Safety department did not log it as a hazard requiring additional follow-up. According to the Safety department, if the OM's response did not satisfy the reporter, then an ASR should have been generated as per company policy.
The second significant change to FOD 034 involved the definition of a green first officer. In the new version of the FOD, this definition changed from a requirement of 6 months of operational line experience to one of 50 hours. An analysis of first officer flying hours in 2013 showed that it took on average approximately 5 months for first officers to acquire 50 hours of operational line experience.Footnote 85
The third significant change to FOD 034 involved the orientation provided to green pilots. In Revision 0, the intent was to ensure that this orientation was conducted by a senior pilot. In Revision 1, it is implied that any captain could conduct the orientation, which, according to the company, could be done as a ground-based exercise.
At the beginning of May 2013, the occurrence pilots were scheduled to hold night standby together at another base, even though neither had any previous operational experience at that base. This situation created a green-on-green pilot pairing; however, the occurrence pilots advised the company that they were not comfortable being paired at night at a new base, and the schedule was subsequently changed.
Based on FOD 034 Revision 0 and Revision 1, the occurrence pilots would not have represented a green-on-green pilot pairing at CYMO, since only the captain would have been considered green under Revision 0, and neither pilot was considered green under Revision 1.
Although FOD 034 established the criteria for green pilots, there was no easy way for pilots at a particular base to know whether another pilot met the criteria for a green pilot. As with currency tracking, short of contacting the CP or OM, captains had to rely on their first officers to advise them of whether they were or were no longer green pilots.
1.18 Additional information
1.18.1 Standard operating procedures
1.18.1.1 General
Under current regulations, CARs Subpart 702, 703, 704, and 705 operators must “establish and maintain standard operating procedures”Footnote 86 for aircraft that are required to be operated by 2 or more pilots. CARs Subpart 705 operators are required to submit their SOPs to TC for review. There is no such requirement for CARs Subpart 702, 703, or 704 operators, although in the past, SOPs were traditionally submitted to TC for review. In several cases, TSB investigation reports have highlighted deficiencies related to inadequate company SOPs.Footnote 87
Ornge RW has separate SOPs for the AW139 and the S-76A. On 06 February 2012, Ornge RW's POI advised the company that its S-76A SOPs had been reviewed and met the requirements of CAR 703.107(1).
Ornge RW's S-76A SOPs are divided into several sections, coinciding with different aspects of the company's operation. While night sequences are discussed to a certain extent in various sections, the SOPs do not include a dedicated night-flying section that addresses some of the hazards specific to night operations at Ornge RW, nor do they outline precautions to take when flying at night to ensure adequate safety margins are maintained. For example, the SOPs do not specifically outline crew duties during a critical phase of flight, such as during departure.
1.18.1.2 Takeoff procedures (general)
Ornge RW's S-76A SOPs describe several different types of takeoffs. The general takeoff section states that takeoff power is determined by adding 10 to 15% to the hover torque. There is no mention in the CARs or company SOPs of a maximum angle of bank or turnout altitude for day or night operations. However, the SOPs for each of the different types of takeoffs instruct the pilots to “Carry out the post take-off checks through 300 ft. AGL before proceeding on course”.Footnote 88
The Ornge RW AW139 SOPs contain the following guidance to pilots:
When departing VFR at night it is important to reach a safe altitude above obstacles as soon as possible. A high speed, dragged-out, climb may bring the aircraft dangerously close to obstructions. NVFR climb to MOCA [minimum obstruction clearance altitude] will be made steeply at an airspeed no greater than 100 KIAS, and when possible, at a rate of climb of at least 1000 fpm until obstacle clearance is assured.
This information is not included in the S-76A SOPs.
1.18.1.3 Black-hole departures
The black-hole effect typically occurs over water or over dark, featureless terrain where the only visual stimuli are lights located on and/or near the airport or landing zone.Footnote 89 The absence of visual references in a pilot's near vision affects depth perception and can lead to a sensation of being too high on approach. In many cases, pilots will react to these false sensations by correcting altitude to below the correct flight path. Likewise, departing from a lit area into an area of darkness presents its own unique challenges, as a pilot must carefully transition from a visual manoeuvre to a predominantly instrument manoeuvre. If pilots allow their guard to drop during a black-hole approach or departure, they may quickly find themselves in a situation where safety margins are reduced to unacceptable levels.
Section 4.22 of Ornge RW's SOPs outlines the company's black-hole departure procedure. This section warns that, “with little or no forward visual reference, the risk of hitting terrain is much greater than the risk of having an engine failure on departure. As such, this procedure minimizes the risk of controlled flight into terrain (CFIT) by maximizing height over distance.”Footnote 90 About the procedure, the SOPs state that “this departure requires the PF to fly away based solely on instruments.”Footnote 91 This is done by initiating a vertical climb while maintaining position over the departure point, and then transitioning to forward flight as the helicopter reaches 30 to 50 feet agl. At the point of transition, “the pilot must transition from outside references to instrument flight.”Footnote 92 This section advises that the minimum IFR airspeed must be achieved and maintained as soon as possible after takeoff to ensure obstacle clearance through to 500 feet agl. According to the SOPs, “this procedure will normally be used at night in an area with little or no background lighting, or any time the ability to see obstructions in the takeoff path is limited such as departing from a snow or dust-covered area.”Footnote 93
Like the other take-off procedures outlined in the SOPs, the black-hole departure procedure advises pilots to carry out the post-takeoff checks through 300 feet agl. However, this section of the SOPs also directs pilots to climb to at least 500 feet agl before proceeding on course. Therefore, unless departing from one of the company-designated black holes, S-76A flight crew were permitted, whether day or night, to proceed on course after reaching 300 feet agl. Since CYMO had not been designated as a black hole, it was acceptable, according to company SOPs, for pilots to turn at 300 feet agl, day or night, when taking off from CYMO.
1.18.1.4 Cross-checking procedures
A widely accepted crew resource management (CRM) strategy in multi-crew cockpits is to cross-check instrument settings, frequency selections, and flight director/autopilot selections. This cross-checking is done as a threat-and-error management (TEM) strategy to prevent mistakes from having an adverse consequence on the flight. For example, it is common practice in multi-crew operations for pilots to read back altimeter settings to verify that both pilots have the proper altimeter setting. There have been many instances in which aircraft have crashed due to incorrect altimeter settings. By diligently cross-checking, pilots can detect an error such as an incorrect altimeter setting early enough to rectify the problem before it leads to an undesired aircraft state. In the Ornge RW S-76A SOPs, there are 2 references to cross-checking of altimeters. The Enroute section of the SOPs specifies that each crew member is to read back altimeter settings and state “set right” and “set left”, respectively. Section 8.1 states that pilots are supposed to cross-check altimeters as they cross the final approach fix inbound on final approach. The SOPs do not include any guidance with regard to radio altimeters and a requirement to cross-check the low-height bug settings.
1.18.1.5 Pilot monitoring duties
Another widely accepted CRM practice relates to pilot monitoring (PM) duties, which involve closely watching the other pilot for any signs of performance degradation or deviation from the agreed-upon flight profile. PM duties and strategies are not spelled out in Ornge RW's S-76A SOPs; however, section 8.1 of the IFR Procedures section states that significant deviations will be called by the pilot who is not flying (i.e., PM).
It is common to refer to pilots as either the PF or the PNF. These terms have been used for many years in the multi-crew environment. In recent years, there has been a shift in thinking within the CRM community and a move to place more emphasis on the role of the pilot who is not physically at the controls. Under the legacy definition, this pilot was the one “not flying.” However, despite the fact that this individual may not be physically manipulating the flight controls, he plays a critical role in monitoring the flight progress. Consequently, the term “PNF” has been replaced by many operators with the term “PM”, to place more emphasis on the active role played by this pilot in a multi-crew environment.
From a CRM best practices standpoint, the PM must be alert to any deviations from the planned flight path, and be ready to intervene in a timely manner. In some scenarios, when there is insufficient time for dialogue, the PM may actually be required to intervene and assume control in order to return the aircraft to a safe flight regime. As with any other skill, it is vital that procedures be established and pilots be trained in a realistic manner for its application. For example, many operators have SOPs that spell out specific PM duties for such things as takeoffs and landings, altimeter changes, flight director changes, etc. As a general rule, PMs must remain diligent in monitoring all flight path changes, pilot actions, system mode changes, and aircraft responses, particularly while operating in a critical phase of flight, when workload increases the risk of errors going unnoticed.Footnote 94
1.18.1.6 Radio altimeters
Radio altimeters are an important tool for enhancing situational awareness and reducing the risk of CFIT.Footnote 95 In Ornge RW's S-76A SOPs, the only reference to radio altimeters is found under IFR Procedures, in section 8.2. That section says that pilots are to set any minimum altitude restriction given, or 1000 feet if no minimum is given. It goes on to say that pilots are free to set lower altitudes on departure, but must brief the PNF on the reason. The investigation showed that there was no consistent methodology or practice among pilots with regard to radio altimeter settings.
Pilots who chose to set one radio altimeter low-height bug to 500 feet and the other to 150 feet did so as a means of establishing a two-tiered alerting system. The intent was for the PNF to receive the initial warning as the aircraft goes below 500 feet agl and to then verbalize the condition with the intent that corrective action would be taken prior to descent below 150 feet agl.
1.18.1.7 Informal night-flying procedures: Common practice at Ornge
In addition to the differences noted above, there were a number of informal variations of Ornge RW's black-hole departure and approach procedures. These procedures varied among flight crew and the different bases. Many of the variations were related to the past experience of pilots, some of which had carried over from the previous EMS provider. Experienced captains at Ornge RW recognized the inherent risks of night flying, and some had implemented their own procedures to ensure safety margins were maintained during night flights. As a result, there was no commonly used standard procedure for black-hole approaches and departures. For example, many pilots at Ornge RW had adopted the widely accepted practice of restricting all turns at night to a maximum of rate 1. This restriction was to ensure that smooth, controlled turns, which reduce the risk of disorientation, were conducted at night. During interviews, several pilots indicated that they believed this restriction was included in the company SOPs. Others indicated that it was a carryover from the previous operator that was contracted for EMS services. According to company SOPs, there is no recommended or maximum bank limit for night operations.
Beyond the common practice of limiting turns to a maximum of rate 1, several of the company's experienced pilots believed that there was a requirement in the SOPs to climb to 500 feet agl at night before proceeding on course. This informal procedure had originated during the days of the previous operator, and it continued to be employed by a large number of experienced pilots.
Another widely accepted practice among experienced S-76A pilots at Ornge RW was to closely monitor the PF during night takeoffs and night landings. Many pilots indicated that they would not conduct any in-flight checks during the departure phase. Instead, they would closely monitor the flight instruments in case the PF experienced difficulties, and conduct non-essential post-takeoff checks once no longer in a critical phase of flight at low altitude. Experienced S-76A captains at Ornge RW were fully cognizant of the risks associated with night departures, and they would closely monitor less experienced pilots who were being given an opportunity to carry out PF duties at night, particularly during the takeoff and landing phases when the margin for error is extremely small.
1.18.2 Training
1.18.2.1 General
According to CAR 703.88, no air operator shall permit a person to act, and no person shall act, as a flight crew member in an aircraft unless that person has fulfilled the requirements of the air operator's TC-approved ground and flight training program, even if those requirements go above and beyond the regulatory requirements. This stipulation is echoed in Ornge RW's Training Manual, which states that contracted training must be conducted in accordance with the company's TC-approved training program. According to Ornge RW, the company monitors its contracted training through a combination of base visits, training observations, and feedback from flight crews.
This section will highlight some of the key elements in Ornge RW's training program that are relevant to this occurrence.
1.18.2.2 Ornge Rotor-Wing's simulator training
Before June 2012, Ornge RW was using an S-76 training provider that offered initial and recurrent training in an S-76A model simulator. However, since Ornge RW planned to move away from the S-76A for its air ambulance service, it did not secure additional S-76A training slots with the previous provider. Following the decision to keep flying the S-76A, Ornge attempted to return to its original S-76 training provider; however, all of the S-76A slots had already been booked. Ornge RW therefore needed another solution. After briefly using a simulator in Vancouver, Ornge RW selected the CAE training facility in Whippany, New Jersey, for initial and recurrent S-76 training. Training of Ornge RW pilots at the CAE Whippany facility, using CAE instructors, began in January 2013. In Whippany, the training facility has a fully coupled S-76C+ simulator that can be converted to an S‑76B configuration. Although the first recurrent course in January 2013 was conducted using the C+ model configuration, the standard practice was to convert it to an S-76B configuration for Ornge RW initial and recurrent training. The S-76C+ and S-76B configurations are considerably different from the older S-76A models flown by Ornge RW, but given the difficulty in locating another S-76A simulator, the company elected to use the CAE facility in Whippany. Ornge RW's initial and recurrent AW139 training is also conducted at the CAE training facility in Whippany; however, the AW139 training is carried out by Rotorsim personnel on an AW139 full-flight simulator. Rotorsim is a 50-50 joint venture between AgustaWestland and CAE.
Before the accident, Ornge RW conducted black-hole training in the simulator, not on aircraft. Although not required by regulation, Ornge RW's TC-approved Training Manual includes a requirement for black-hole training, emphasizing the importance of maximizing height over distance during black-hole takeoffs and landings. Through interviews, a review of training records, and TC surveillance reports, investigators determined that the black-hole portion of Ornge's initial and recurrent S-76 simulator training at the CAE Whippany facility was not consistently taught in accordance with Ornge's black-hole departure SOPs (section 1.18.1.3) or the TC-approved Training Manual, nor was it being carried out in an operationally realistic manner. As previously stated in the report, the occurrence captain and his training partner did not complete the black-hole training scenario used by CAE because it was not considered operationally realistic. As a result, neither pilot took credit for having completed black-hole training. This was clearly documented on the captain's record of line indoctrination and training in aerodrome and area of operation qualification training. In addition, the other pilot advised Ornge RW management that because it was not completed during the recurrent course, that he required black-hole training before being dispatched to one of the black-hole locations.
Ornge RW received several complaints from company pilots, both verbal and written, about the quality of the S-76 training at the CAE Whippany training facility. Common issues identified were that the contractor's instructors were not familiar with Ornge's SOPs, and at times the crews either received no black-hole training or conducted the exercise on their own initiative. A number of pilots also cited concerns over the fact that IFR training was being conducted in United States airspace, using United States flight publications. Some of these issues were raised with CAE management before the accident. In addition, Ornge RW also discussed the quality of the graphics/visuals, instructor continuity, the need for better modelling of the company's landing sites equipped with reflective cones and for improved SOP training, as well as a review of the training program to mandate at least one full night sortie.
At the time of the accident, the company's S-76 initial and recurrent training courses did not include a dedicated night session. Instead, night VFR sequences were typically embedded within one or both of the two-day recurrent VFR simulator sessions. According to the company's Training Manual and simulator training forms, 64 sequences in total were conducted over the course of 3 VFR and 3 IFR sessions. Of the 64 sequences, only 1 item specifically referred to night-related sequences, and was listed as “Loss of visual reference—Black Hole”. Likewise, recurrent S-76 training consisted of 56 sequences evaluated during 2 VFR and 1 IFR sessions. Of the 56 items listed, only 2 items specifically referred to night-related sequences: “Towering and Black Hole Takeoffs” and “Loss of Visual Reference—Black Hole”. The Ornge RW training forms do not include any items related to black-hole approaches/landings. According to the company's S-76 simulator training provider, black-hole landings could not be supported on the CAE simulator due to visual system limitations. However “black hole landing and takeoff” had been added to the list of optional tasks completed on CAE's flight training record form. Black‑hole landings were required as per the TC-approved Training Manual.
In addition, according to CAE, practical CFIT-avoidance training is documented on the CAE flight training records as “Situational Awareness” and “Positional Awareness” listed under the category of “Crew Resource Management”. The CAE training records use the annotation “D” to indicate that a particular sequence was either demonstrated or discussed, but not evaluated. As a result, there is no way to differentiate, from looking at the CAE training record, whether a manoeuvre or procedure was demonstrated or discussed during the training. According to CAE's flight training record for the captain, the captain received a “D” on each of the 3 simulator sessions completed during his course for all 11 of the items listed under the “Crew Resource Management” section of the flight training record, including “Situational Awareness” and “Positional Awareness”. The captain's CAE flight training record also indicated “D” for “black hole takeoff and landing” on the first 2 simulator sessions.
Other than the training records, no additional direction was provided to the simulator instructors to guide them through the S-76 initial or recurrent training with regard to the specific sequences that must be completed. In comparison, for its AW139 initial and recurrent training, Ornge RW developed a training binder outlining the instructor's duties and the company's requirements.
In early May 2012, Ornge RW provided the POI with a summary of observations collected by the company regarding the AW139 simulator training in Whippany. The report to the POI noted that there was “an overall deficiency in crew SOP adherence”,Footnote 96 and that Rotorsim training personnel were not following Ornge RW's TC-approved training program.
In an effort to gain a better understanding of the effectiveness of Ornge RW's training program, investigators reviewed the PPCs conducted on Ornge RW AW139 and S-76A pilots between 06 January 2012 and 31 May 2013. In total, there were 108 passed PPCs and 9 failed PPCs, which represents a failure rate of approximately 8%. The failures among the Ornge RW trainees were attributed to undetected altitude deviations (2 failures); excessive airspeed decay in instrument meteorological conditions (IMC) (3 failures); unacceptable skill and knowledge during emergency procedures (2 failures); and unacceptable depth of knowledge of aircraft limitations, SOPs, and IFR takeoff minima (2 failures). In each case, the POI reviewed the circumstances of the failure with the approved check pilot (ACP) in question, and all failures were confirmed as valid.
In follow-up, post-occurrence discussions (May 2014), TC indicated to TSB investigators that Ornge RW's failure rate was largely related to instrument flying and to procedures related to instrument flying. A formal response from TC stated that “the failure rate demonstrates that there are ongoing challenges within the training program […]”.Footnote 97
1.18.2.3 Pilot proficiency checks
The required sequences that must be completed during a PPC are listed in the PPC schedules found in the CASS. Aside from stating that PICs and SICs should be evaluated from their respective seat positions in the cockpit, the helicopter PPC schedules for CARs Subpart 702, 703, and 704 pilots are identical for PICs and SICs. However, depending on the operations specifications (ops spec) in place at a company, captains may be required to complete additional sequences in order to meet the PIC requirements associated with a particular ops spec. The crew status box on the PPC form, which is a Canadian aviation document, indicates how the candidate was tested during the PPC. In the absence of additional requirements associated with an ops spec, captains and first officers are held to the same standard in helicopters, which is either pass or fail.
The consequence of this lack of differentiation is that there is no such thing as a “first officer PPC” or a “captain PPC”. Any pilot who passes a PPC on a helicopter has met the minimum requirement to act as PIC on that aircraft type. Short of failing a pilot, there is no mechanism in place for an ACP to restrict a pilot from carrying out PIC duties in helicopters. The same is true for the aeroplane PPC schedules for CARs Subpart 702 and 703 pilots. The PPC schedules for aeroplane pilots operating under CARs Subparts 704 and 705 include additional requirements that must be completed by PICs, and there is a different PPC schedule for CARs Subpart 705 cruise relief pilots.
Beyond the fact that there is only one PPC standard for helicopter pilots, the current PPC schedules do not take into account mission complexity and operational requirements. Therefore, an operator wanting to verify a pilot's ability to conduct a specific sequence, such as night black-hole approaches, cannot test the pilot's ability under the current PPC schedules. An operator wanting to ensure a pilot's proficiency in a particular aspect of operations that is not testable under the current PPC schedules must find another way of verifying that the pilot has achieved an acceptable level of proficiency.
1.18.2.4 Pilot line indoctrination training
Ornge RW's TC-approved Training Manual includes a section on pilot line indoctrination training. According to the manual, line indoctrination training is required only for AW139 flight crews and is not applicable to S-76 flight crews. As per CASS 724.115, all new CARs Subpart 704 pilots must undergo line indoctrination training, which consists of at least 6 hours in 4 mandatory sectors.Footnote 98 According to TC:
The purpose of line indoctrination is to refine, in a line context, the initial training a pilot candidate has received on that aircraft type. This training should ensure that the candidate will be fully prepared to conduct operations in his/her designated position on all company routes for which he/she may be assigned.Footnote 99
Since Ornge RW's AW139 fleet is certified under CARs Subpart 704, those pilots must meet the requirements in CASS 724.115. According to Ornge RW, the company elected to operate the AW139 under CARs Subpart 704 to increase safety. Since the company had originally intended to stop using the S-76A when the AW139 was introduced into service, there was never any plan to operate the S-76A aircraft under CARs Subpart 704, and the decision was never revisited.
Unlike the line indoctrination requirements for CARs Subpart 704 and 705 pilots, the regulations do not specify a minimum number of flight hours or sectors that a CARs Subpart 703 pilot must complete before assuming operational duties. Furthermore, there is no requirement for holders of multiple air operating certificates to establish a common standard across their fleets. As a result, Ornge RW's S‑76A pilots, who operate under CARs Subpart 703, are not required to complete formal line indoctrination, despite the fact that the company's AW139 and S-76A fleets are operated with the same crew composition and have virtually identical mission profiles.
1.18.2.5 Aeromedical resource management training
As per Ornge RW's Training Manual, all new employees must complete AMRM training, which is designed to provide employees with “skill-based strategies that can be used in effectively managing resources, error prevention and error management”Footnote 100 and which focuses on crew member behaviour and how that behaviour impacts the safety system. According to the manual, AMRM includes CRM and pilot decision making, and covers the following topics:
- Threat and error management;
- Resources available and their limitations;
- Crew Resource Management (CRM skills);
- Communication;
- Situation Awareness;
- Decision Making;
- Workload Management;
- Crew Performance;
- Identifying Observable Behaviours;
- Developing Preventable Strategies; and
- Human Factors (Fatigue, Stress, Personalities, Group Dynamics).Footnote 101
Although Ornge RW was not required by regulation to conduct CRM training, CRM is a critical element of effective multi-crew operations. The AMRM initial training material was therefore reviewed and compared with modern CRM training philosophies. Based on a review of current CRM standards, it was found that the core content of Ornge RW's AMRM course outline met the requirements outlined in the current CRM standard, which is applicable only to CARs Subpart 705 operators.Footnote 102
Modern CRM training is intended to provide flight crew with practical skills to reduce the probability of errors occurring (error avoidance), to detect and correct errors before they have an operational impact (error trapping), or to contain and reduce the severity of errors that become consequential (error mitigation).
Two different AMRM courses were being delivered at Ornge. One was conducted by an independent contractor, and the other was conducted internally by the DFO at Ornge FW. According to Ornge RW, the company had the flexibility to use either course, since both met the training objectives outlined in the Training Manual. The training package provided by the contractor was largely awareness-based, with a heavy focus on legacy CRM topics and exercises, including well-known non-aviation synergy/survival exercises and personality assessments. The course provided by the DFO at Ornge FW also had a large awareness component. However, it contained more modern CRM training material and provided more practical CRM strategies than the course provided by the contractor. In general, neither of the 1-day AMRM courses reviewed in the investigation provided many practical strategies that could be transferred into day-to-day flight operations.
Beyond the initial AMRM training received by all new pilots and medics, all flight crew must receive annual recurrent CRM training, to include the following items as listed in the company's TC-approved Training Manual:
- Situational Awareness;
- Understanding Human Error;
- Threat and Error Management;
- Culture;
- Crew Co-operation;
- SOPs and Checklist Philosophy;
- Stress and Fatigue Management;
- Automation;
- Communication and Assertiveness;
- Decision Making; and
- Risk Management.Footnote 103
As was done with the initial AMRM training package, Ornge RW's recurrent CRM training package was reviewed and compared with modern CRM training philosophies. It was similar to the 2 initial AMRM training packages in that it did not provide many practical CRM tools or strategies that were designed to help flight crews effectively manage the threats and errors that may be encountered during operational flights. Primarily awareness-based, it focused more instead on how to deal with physiological problems in flight.
The TSB has previously identified a safety concern related to current CRM training standards. During TSB Aviation Investigation A11H0002, it was found that the flight crew had not received initial and recurrent CRM training that provided them with sufficient practical strategies to assist with decision making and problem solving, communication, and workload management. As outlined in the TSB report on that investigation, initial CRM training must teach effective CRM skills, and then those skills must be reinforced during recurrent training. Otherwise, flight crews may not adequately manage risk while on the flight deck. The Board has therefore expressed concern that, without a comprehensive and integrated approach to CRM by TC and aviation operators, flight crews may not routinely practice effective CRM.
1.18.2.6 Ground training in controlled-flight-into-terrain avoidance
According to CASS 723.98(24) and CASS 724.115(27), CARs Subpart 703 and 704 helicopter operators are required to provide initial and biennial CFIT-avoidance training to all flight crew members who operate helicopters approved for flight under IMC. The initial and biennial CFIT-avoidance training must include the following:
- Factors that may lead to CFIT accidents/incidents
- CFIT prevention strategies
- Methods of improving situational awareness
As well, Ornge RW incorporated some of the additional CFIT-avoidance training requirements, not required by regulation for CARs Subpart 703 and 704 helicopter operators, listed for aeroplanes in CASS 723.98(29) and CASS 724.115(32). For example, the company's TC-approved Training Manual includes the following initial and recurrent CFIT-avoidance training requirements:
- Operational characteristics, capabilities, and limitations of enhanced ground proximity warning system (EGPWS);
- Escape manoeuvre techniques and profiles applicable to the helicopter;
- In the simulator, performance of 1 VMC (visual flight rules meteorological conditions) escape manoeuvre in response to an EGPWS warning; and
- In the simulator, performance of 1 IFR escape manoeuvre in response to an EGPWS warning.
The classroom portion of Ornge RW's initial CFIT-avoidance training consisted of a two-hour presentation. During that presentation, pilots were instructed on some of the factors that can lead to CFIT and some prevention strategies, and they learned a generic CFIT escape manoeuvre. One of the presentation slides cites a United States EMS study from 1992–2004, stating that 84% of CFIT accidents happened at night, and 58% of those were in VMC. The presentation identified the “biggest risk[s] in Ontario Air Ambulance operations”as those involving
- black-hole operations
- flights in marginal VFR
- night VFR operations.
Several individual and team performance factors that can reduce the risk of CFIT were listed; 2 of those factors were experience and currency.
A review of the company's initial CFIT-avoidance training presentation determined that the material provided a general awareness of the threats associated with CFIT. In the introduction to the presentation, the notes state that the training will teach prevention strategies. In reality, the training does not provide much in the way of practical prevention strategies (i.e., SOPs) that transfer to the cockpit. For example, the CFIT-avoidance training package does not address any of the challenges associated with operating at night from an aerodrome, nor does it address specific flight crew responsibilities (such as monitoring flight instruments) and the importance of ensuring that only essential tasks are carried out during critical phases of flight. Although a slide is included that outlines the CFIT escape-manoeuvre procedure, it is a generic procedure that refers to EGPWS warnings and “go-around” button. Only some of the S-76As were equipped with EGPWS, and none had a go-around capability. The generic escape manoeuvre described in the presentation provides no specific guidance on attitudes to select, power settings, or airspeeds. The procedure appears to be written for more advanced aircraft, like the AW139, and it lacks specific direction for flight crew to follow when carrying out the CFIT-avoidance manoeuvre.
Several pilots, including the captain involved in the occurrence, had not completed the required practical portion of CFIT-avoidance training as stipulated by the TC-approved Training Manual.
1.18.3 Captain qualification process in other organizations
Some EMS operators have established a process requiring all pilots, regardless of past experience, to demonstrate that they are ready to assume the role of captain before being employed operationally as a captain. This is done to ensure that pilots have an opportunity to gain, or regain, the skills necessary to safely carry out captain duties in accordance with the CARs and the company's SOPs. One large EMS provider in Western Canada requires all potential captains to undergo formal captain training, receive nominations from training captains, and then undergo a captain review board where they are required to answer a number of aircraft, company, and mission-related questions to demonstrate they have acquired the necessary knowledge and skills to act as PIC of a multi-crew aircraft.
1.18.4 Night flying
1.18.4.1 Night visual flight rules
The principle behind VFR flight is that the pilot takes attitude reference from visual cues outside of the aircraft. Some basic requirements must therefore be met when conducting VFR flight, whether day or night, in Canada. Under CARs 602.114 and 602.115, regardless of whether it is operated in controlled or uncontrolled airspace, the aircraft must be “operated with visual reference to the surface.”Footnote 104 The CARs define surface, in part, as “any ground or water, including the frozen surface thereof”.Footnote 105 Therefore, using TC's interpretation of the night VFR requirements, a flight conducted over an area away from cultural lighting and where there is inadequate ambient light to clearly discern a horizon (i.e., to continue flight solely by reference to the surface), does not meet the requirements for operation under VFR. Instead, the flight would fall into the realm of IFR, which requires pilots to rely on their flight instruments to ensure safe operation of the aircraft.
As in Canada, night VFR is permitted in several countries. However, the night flying regulations in some countries differ significantly from the CARs. In Ireland, for example, night VFR flights are not authorized unless they are conducted within a control zone, at which point they will be operated as special VFR flights.Footnote 106 Night flights conducted outside a control zone must be conducted in accordance with IFR regulations. In the United States, the Federal Aviation Regulations (FARs) specify that no person shall operate a helicopter under VFR at night unless that person has “visual surface light reference, sufficient to safely control the helicopter.”Footnote 107
Currently, there is no requirement for Canadian commercial air operators to demonstrate that they will be able to maintain visual reference to the surface along a proposed night VFR route, either through cultural lighting or alternative means. One exception, however, is a special provision in CAR 702.18(3)(c) that permits single-engine VFR flights at night where the pilot does not hold an instrument rating. According to the CASS, the area overflown must be “illuminated by lights on the surface to ensure visual surface reference and conditions provide for a discernible horizon.”Footnote 108
In addition to the basic regulatory requirement outlined above, pilots involved in night flights with passengers must meet the recency requirements set out in CAR 401.05(2), which specifies that a pilot must have conducted 5 night takeoffs and 5 night landings within the 6 months preceding the flight. These requirements were included in Canadian regulations long before the CARs, which came into effect in 1996, replacing the Air Navigation Orders and the old Air Regulations. TC was unable to provide an explanation as to why 5 night takeoffs and 5 night landings were selected as the requirements in CAR 401.05(2). The investigation established that there is a general sense among TC inspectors that the requirements for night takeoffs and night landings were based on values that were selected arbitrarily many years ago, not according to any type of research.
In Australia and New Zealand, the national Civil Aviation Authorities have established requirements for night takeoffs and night landings that are more restrictive, in terms of recency requirements, than the Canadian requirements. Under the Australian Civil Aviation Regulations, if passengers are carried at night, “there is an additional requirement under the [Australian] CARs to have completed at least three takeoffs and three landings at night within the previous 90 days.”Footnote 109 These requirements are similar to those currently in effect in New Zealand. In the United States, the FARs state that “no person may act as pilot in command of an aircraft carrying passengers during the period beginning 1 hour after sunset and ending 1 hour before sunrise, unless within the preceding 90 days that person has made at least three takeoffs and three landings to a full stop during the period beginning 1 hour after sunset and ending 1 hour before sunrise”.Footnote 110
1.18.4.2 Night rating
In Canada, a helicopter pilot must first obtain a night rating in order to be allowed to conduct a VFR night flight. Part of that process involves completion of 10 hours of night flight time and 10 hours of dual instrument flight time.Footnote 111 The intent of this instrument flight time is to prepare pilots for the possibility of inadvertent entry into IMC. However, there is no requirement for pilots to undergo any type of formal evaluation of instrument flying competency prior to being granted a night endorsement, as long as the minimum required hours are obtained. Once a pilot has successfully obtained a night rating, the only currency requirement to maintain a night rating entails the takeoff and landing requirements for carrying passengers at night, as outlined in CAR 401.05 and mentioned earlier in this report. There is no requirement for a pilot who conducts night VFR flights to acquire additional instrument flight time, despite the well-documented importance of instrument flying skill during night VFR operations.
This discrepancy was previously identified in TSB Safety Study 90-SP002, which found that a large proportion of night flying accidents result from loss of aircraft control and frequently involve pilots with little additional instrument flight experience beyond what they obtained to earn the night endorsement. The important distinction between being current as per regulations and being proficient was captured in this excerpt from the Australian Transport Safety Bureau's report, Visual flight at night accidents: What you can't see can still hurt you:
Although a pilot may be legally entitled to fly on a dark night based on recent flights over an urban area at night, the flight will probably be at a higher risk if the pilot does not have recent experience in a dark night environment. While night flight ratings allow flight to and from airstrips with minimal nearby lighting, many pilots rarely fly in that environment. Instrument flying is a complex skill and, once developed, needs to be maintained by regular practice. If a pilot does not have recent experience in dark night operations, it is preferable not to take off, fly or land in these conditions unless assisted by a suitably competent and qualified pilot.Footnote 112
As stated in TSB Safety Study 90-SP002, “since instrument flying skills are perishable and require regular practice to maintain even a modicum of proficiency, the criteria for obtaining and maintaining a night endorsement apparently do not adequately reflect the skills required to cope with inadvertent entry into adverse weather.”Footnote 113 In recognition that there is currently no way of ensuring a minimum level of instrument flying skill prior to issue of a night endorsement, and no way of ensuring that a minimum level of instrument flying proficiency is maintained, the TSB recommended that:
The Department of Transport revise conditions for the issue and maintenance of a night endorsement by:
- including a practical evaluation of the pilot's skill prior to issue of the endorsement; and
- verifying continued proficiency on a recurrent basis.
Transportation Safety Recommendation A90-72
In its response, TC indicated that industry had rejected the idea of an in-flight evaluation of instrument flying skill. Instead, the Department stated, a ground-only periodic seminar was being considered. Since this response did not address the underlying safety deficiency, it was assessed by the Board as Unsatisfactory. TC later made some changes to the Flight Instructor Guide: Aeroplane (TP 975) with regard to night ratings, highlighting that the instructor needs to make sure that the “student is competent to exercise the privileges of the rating, which is more than simply acquiring necessary dual and solo time.”Footnote 114 However, this additional guidance was not added to TC's Flight Instructor Guide—Helicopter (TP 4818). Following the changes to TP 975, and in the absence of other action on TC's part, the Board assigned TC's response a rating of Satisfactory in Part.Footnote 115
1.18.4.3 Hazards associated with night flying
1.18.4.3.1 General
There are a number of hazards associated with night flying. First and foremost, visual performance is significantly degraded under conditions of night illumination. Even under ideal night VFR conditions with a full moon, a pilot likely has a visual acuity in the order of 20/200.Footnote 116 This degraded visual performance can create compelling sensory illusions that can lead to spatial disorientation, which is defined as “an erroneous sense of one's position and motion relative to the plane of the Earth's surface.”Footnote 117 In other words, spatial disorientation occurs when a person's brain misinterprets cues from the environment, and that person experiences difficulty resolving mentally why, for instance, an aircraft does not appear to be doing what the brain believes that it is doing. There are 3 specialized sensory systemsFootnote 118 that help people determine which way is up and which way they are oriented:
- The visual system (our eyes);
- The vestibular system (the organs in both inner ears that sense balance); and
- The somatosensory system (nerves in the skin, muscles, and joints that work with our hearing).
In April 2013, Ornge's safety department published Safety Bulletin AS-BULL-106: Spatial Disorientation. The bulletin included hyperlinks to a safety report published by SKYbrary and a report published by the Australian Transport Safety Bureau (ATSB), “to raise awareness of spatial disorientation.”Footnote 119 In the ATSB report, it was stated that “the visual system is by far the most important of the 3 sensory systems”,Footnote 120 responsible for approximately 80 to 90% of the raw information that is received by the brain.Footnote 121, Footnote 122 Therefore, in night or poor weather conditions, a pilot may be missing an enormous amount of information that could be used to determine the orientation of an aircraft. Studies conducted by aviation researchers at the University of Illinois in the 1990s estimated that, on average, it took 178 seconds for VFR pilots exposed to simulated IMC conditions to become spatially disoriented.Footnote 123 In situations where there is little to no outside visual reference, spatial disorientation can be overcome by reverting to instrument flight. Training in instrument flight helps pilots learn to manage their attention effectively, prioritizing activities to ensure that they attend to the critical pieces of information. It also helps them learn to ignore false sensory perceptions and to trust their flight instruments.Footnote 124
The hazards associated with night VFR flight are amplified during the takeoff phase, as the pilot transitions from a well-lit airport into what may seem like total darkness.Footnote 125 For example, as explained earlier in this report, there is virtually no cultural lighting to the north of Runway 06 at CYMO. According to a number of pilots who have flown from CYMO to Attawapiskat on a cloudy night, the flight could best be described as a flight conducted in IMC but operated under VFR, since it is impossible to maintain visual reference to the surface.
Further complicating matters is the fact that it takes approximately 30 minutes for the human eye to fully adjust to lower levels of light (a period referred to as night adaptation). A pilot departing within that 30-minute adaptation period may therefore have severely degraded night vision when attempting a night VFR departure.Footnote 126 This degradation in vision can create a very risky situation. According to TC's Aviation Safety magazine, “the mixing of VFR and IFR procedures can be deadly in NVFR [night VFR] operations.”Footnote 127 In these situations, a pilot who does not transition to instruments and maintain a proper instrument cross-check will be at increased risk for visual and/or spatial disorientation.Footnote 128 For this reason, it is essential that pilots of multi-crew aircraft remain extremely alert during this critical phase of flight and be ready to assume control at a moment's notice.
1.18.4.3.2 Night visual-flight-rules flight in areas of poor illumination
During the course of the investigation, more than 20 experienced helicopter pilots were interviewed. Most indicated that they felt strongly that flying night VFR in remote or sparsely settled areas is significantly more difficult than doing so in heavily populated areas, where cultural lighting is abundant. In many instances, pilots reported having conducted night VFR flights in which they were unable to maintain visual reference to the surface or make out a discernible horizon. According to these interviewees, instrument flight skills played a critical role in the successful completion of those flights.
Notably, none of the pilots interviewed indicated having turned down a night VFR flight strictly due to darkness, or having considered such a flight to be in contravention of CAR 602.115, which states that an aircraft must be operated with visual reference to the surface. There appeared to be an overwhelming consensus among helicopter pilots that they would be expected to carry out night VFR flights as long as the reported weather was suitable for night VFR operations, even if there were inadequate cultural or ambient lighting to maintain visual reference to the surface. Most of these pilots pointed out that, during such flights, they would essentially be flying using the instruments, carefully tracking their positions using the GPS to ensure adequate clearance from the surface.
1.18.4.4 Night-vision imaging systems
1.18.4.4.1 General
In recent years, the use of night-vision imaging systems (NVIS), such as night-vision goggles (NVG) and enhanced vision systems, has gained considerable popularity due to the increased operating envelope and safety that these systems can provide to operators involved in night VFR operations. In particular, there has been an enormous increase in the use of NVGs beyond military applications. As far back as 1994, the FAA identified that “when properly used, NVG's can increase safety, enhance situational awareness, and reduce the pilot workload and stress that are typically associated with night operations.”Footnote 129
While several NVIS options are available, this section of the report will focus on NVGs, as these are the leading NVIS in use among members of the civilian helicopter industry. NVGs are “binocular devices that amplify light reflected from the terrain to enhance vision at night.”Footnote 130 They use ambient light to provide pilots with a picture of the outside world that may otherwise not be visible. In recent years, a number of enhancements have been made to NVGs. See Appendix G for a discussion of the recent advances in NVG development.
A large number of helicopter emergency medical services (HEMS) operators, police forces, civilian SAR organizations, and forestry and wildlife agencies, have adopted NVGs for their night operations.Footnote 131 According to the Flight Safety Foundation, NVG use among civilian HEMS providers in the United States has grown from between approximately 2% and 5% in 2006 to more than 90%.Footnote 132 In Canada, a large HEMS provider based in Western Canada has been actively flying with NVGs at night since the mid-2000s. NVGs are employed by the Royal Canadian Mounted Police rotor-wing division, as well as some other provincial and municipal police and government agencies. Recently, a large Canadian offshore helicopter operator also began using NVGs for its night SAR operation. TC expects the use of NVISs to continue to rise, given the increased safety margins that they provide during night VFR operations.Footnote 133 See Appendix H for a detailed discussion of the pros and cons of NVGs.
1.18.5 Instrument flying recency requirements
As stated in TC's Instrument Procedures Manual (TP 2076), instrument flight “is one of the most skilled tasks a pilot can achieve. Such skill however is not a natural attribute and can only be gained by careful training, constant practice and a methodical approach.”Footnote 134 Like any other skill, instrument flying skill erodes over time if it is not exercised, making it unreliable to pilots who do not take the necessary steps to maintain instrument flight proficiency.Footnote 135
According to CAR 401.05(3):
(3) No holder of an instrument rating shall exercise the privileges referred to in section 401.47 unless the holder has
(a) within the 12 months preceding the flight, successfully completed an instrument rating flight test […];
(b) within the six months preceding the flight, acquired six hours of instrument time and completed six instrument approaches to the minima specified in the Canada Air Pilot in an aircraft, in actual or simulated instrument meteorological conditions, or in a Level B, C or D simulator of the same category as the aircraft or in a flight training device under the supervision of a person who holds the qualifications referred to in subsection 425.21(9) of the Personnel Licensing and Training Standards respecting Flight Training;
(c) within the six months preceding the flight, acquired six hours of instrument time and completed six instrument approaches to the minima specified in the Canada Air Pilot in an aircraft, in actual or simulated instrument meteorological conditions, while acting as a flight instructor conducting training in respect of the endorsement of a flight crew licence or permit with an instrument rating; or
(d) successfully completed, for an aircraft, a competency check or pilot proficiency check for which the validity period has not expired and that included the instrument procedures portion of [the schedule to the appropriate standard for aircraft operated under that subpart.]Footnote 136
The investigation determined that there were different interpretations of CAR 401.05(3) among TC inspectors. In particular, some believed that pilots who had met the requirements of CAR 401.05(3)(a) were also required to have acquired a minimum of 6 hours of instrument flight time and have completed 6 instrument approaches in the 6 months preceding the flight, as per CAR 401.05(3)(b). According to TC's formal response, the wording of CAR 401.05(3) is such that as long as pilots renew their instrument ratings and their PPCs annually, then there is no requirement for them to meet the stipulations outlined in CAR 401.05(3)(b).Footnote 137 Therefore, under current regulations, CARs Subpart 703 or 704 pilots can legally conduct a flight under IFR, without restriction, as long as they have completed their PPCs and instrument rating within the previous 12 months. This is also how the regulation is interpreted by Ornge FW and Ornge RW.
During the course of the investigation, a number of people were interviewed, including flight crew, management at Ornge RW, regional TC inspectors, senior regional managers at TC, and TC HQ staff. Most of these individuals expressed concern that the current IFR recency regulations reduce safety margins to an unacceptable level. Most pilots stated that they did not feel that it would be safe to launch on an actual IFR flight, with low ceilings and visibility, if they had logged no instrument flight time during the previous 12 months. Some of the pilots reported that they had found themselves in such a situation, and expressed their lack of comfort and a sense that they were not adequately prepared for a challenging IFR flight. Some also expressed concern that the current regulations made it difficult for a pilot to refuse an IFR flight on the grounds of proficiency, since a refusal could be viewed negatively by the company.
In general, there was overwhelming support for increased IFR recency requirements among those interviewed. Many pilots believe that stricter requirements are necessary to ensure that operators provide pilots with adequate opportunity to maintain their instrument flying proficiency. A large EMS provider based in Western Canada has taken the additional step of requiring its pilots to complete a minimum of 2 instrument approaches per quarter as a way of helping them maintain their instrument flying proficiency. This same operator also supplements annual recurrent simulator training by sending company pilots to the simulator every 6 months for a full day (2 hours as PF and 2 hours as PNF) of refresher VFR and IFR flight training, and provides each pilot with 1 hour of in-aircraft flight training each year.
Aside from initial and annual recurrent simulator training, Ornge RW pilots rarely engaged in instrument flight or conducted instrument approaches. According to the company, approximately 5% of its annual flights are conducted under IFR. There were no reported IFR departures out of CYMO by Ornge RW pilots in the year before the occurrence.
Since Ornge RW pilots renew their PPC and instrument rating every year, the company does not track the instrument flight hours and instrument approaches completed by its pilots. As a result, Ornge RW has no way of monitoring the instrument proficiency of its flight crews in the time between annual PPCs. According to TC, instrument flight hours and approaches were not examined during the January 2013 PVI “because all company pilots complete a PPC including an instrument rating renewal on an annual basis. Therefore, there is no need for the company to record or to track the hours or approaches (i.e., they do not have to comply with 401.05(3)(b) or (c).”Footnote 138 According to TC, companies are expected to record instrument flight hours and instrument approaches if that information is needed to ensure that a crew member is qualified for a flight.
1.18.6 Controlled flight into terrain
CFIT accidents occur when an airworthy aircraft under the control of the pilot is inadvertently flown into the ground, water, or an obstacle. Often, this type of accident happens when visibility is low, at night, or during poor weather. Such conditions reduce a pilot's situational awareness of surroundings and make it difficult to tell whether the aircraft is too close to the ground. The risk is greater when aircraft venture into remote wilderness or into mountainous terrain.
Collisions with land and water account for 5% of accidents, but nearly 25% of all fatalities. Between 2000 and 2009, there were 129 accidents of this type in Canada, resulting in 128 fatalities. In 2010, and again in 2012, collision with land and water was identified as a TSB Watchlist item. Since 2010, Canada has averaged approximately 9 CFIT accidents per year.Footnote 139
The 2010 and 2012 TSB Watchlists identified improved non-precision approach procedures, along with a wider use of technology, such as TAWS, as ways of reducing the risk of CFIT. While CFIT remains an international problem, it was not included in the TSB's 2014 Watchlist due to recent regulatory changes introduced to reduce the threat of its occurrence. The following section of this report discusses some of the benefits of TAWS.
1.18.7 Terrain awareness and warning system
In recent years, there have been significant advances in technology that greatly reduce the risk of CFIT accidents. One of the most significant was the introduction of ground proximity warning systems (GPWS) and TAWS. The terms GPWS and TAWS are often used interchangeably; however, there are some differences between the 2 systems. According to Advisory Circular (AC) 600-003:Regulations for Terrain Awareness Warning Systems, TAWS are “intended to provide the flight crew with both aural and visual alerts to aid in preventing inadvertent controlled flight into terrain, obstacles or water”Footnote 140 by allowing the crew sufficient time to take evasive action. Although GPWS is also designed to prevent CFIT, TAWS provides a much earlier aural and visual warning of an impending collision, and it provides these warnings under some conditions that GPWS cannot. For example, GPWS does not have a look-ahead capability, whereas TAWS has a forward-looking terrain display, based on real-time comparison of an aircraft's location with stored terrain data.
According to ICAO Annex 6, the current standard requires that all commercially operated piston- and privately or commercially operated “turbine-engined aeroplanes of a maximum certificated take-off mass in excess of 5 700 kg or authorized to carry more than 9 passengers shall be equipped with a ground proximity warning system which has a forward-looking terrain avoidance function.”Footnote 141
ICAO recommends that the same requirements be applied to privately operated piston-engined aeroplanes that have a maximum certificated take-off weight in excess of 5700 kg or are authorized to carry more than 9 passengers. It also recommends that smaller, privately operated turbine-engined aeroplanes (that have a maximum certificated take-off weight of 5700 kg or less and are authorized to carry more than 5 but not more than 9 passengers) be equipped with a ground proximity system that has a forward-looking terrain avoidance function.
At time of report writing, there are no ICAO standards requiring helicopters to be equipped with TAWS. However, ICAO Annex 6 includes the following recommendation:
A helicopter when operating in accordance with IFR and which has a maximum certificated take-off mass in excess of 3 175 kg or a maximum passenger seating configuration of more than 9 should be equipped with a ground proximity warning system which has a forward-looking terrain avoidance function.Footnote 142
The TSB has long recognized the need to use technology as a means of helping to reduce the risk of CFIT accidents. In 1995, the TSB recommended that:
The Department of Transport require the installation of GPWS on all turbine-powered, IFR-approved, commuter and airline aircraft capable of carrying 10 or more passengers.
Transportation Safety Recommendation A95-10
TC's initial response to Recommendation A95-10, which came in 04 July 1995, did not substantially address the underlying safety deficiency. The response was therefore assessed as Unsatisfactory.Footnote 143 Then in 2003, TC presented new Notices of Proposed Amendments for TAWS to the CARAC. These proposed regulations were published on 04 July 2012, in the Canada Gazette, Part IIFootnote 144. Under the new regulations, no private or commercial operator shall operate a turbine-powered aeroplane that has a seating configuration, excluding pilot seats, of 6 or more, unless the aeroplane is equipped with an operative TAWS and an enhanced altitude accuracy function.Footnote 145 The stipulations came into effect immediately for any aeroplane manufactured on or after 04 July 2012, while affected aeroplanes manufactured before 04 July 2012 were required to be in compliance by 04 July 2014. The new TAWS regulations superseded the previous requirements for a GPWS in CAR 605.37, and following from them, the TSB assessed TC's 2012 response to be Fully Satisfactory.Footnote 146
The TSB has investigated a number of helicopter occurrences at night or in IMC where TAWS may have proven useful in preventing an accident.Footnote 147 However, there continues to be no requirement for private and commercial turbine-powered helicopters, regardless of seating capacity and operating environment (i.e., night and/or IFR), to be equipped with TAWS. The investigation determined that TC elected not to make TAWS a requirement for helicopters because such a requirement is not part of the ICAO standard. No additional rationale was provided by the Department to explain why TAWS may not be appropriate for helicopters.
Nevertheless, some helicopters have been using that technology since the late 1990s,Footnote 148 and the technology continues to improve. There are several commercially available TAWS that are specifically designed for helicopters. While several aircraft in Ornge RW's S-76A fleet, and all aircraft in its AW139 fleet, are equipped with TAWS, the occurrence helicopter was not, nor was it required to be so under current regulations.
1.18.8 Transport Canada
1.18.8.1 General
TC's Departmental vision is to have a transportation system that is recognized worldwide as safe and secure, efficient, and environmentally responsible.Footnote 149 For civil aviation (TCCA), that means “an integrated and progressive […] system that promotes a proactive safety culture.”Footnote 150 The 3 main tools TC uses to promote a safe and secure transportation system are rule-making, outreach, and oversight.Footnote 151
1.18.8.2 Organizational structure
TC carries out its civil aviation responsibilities through the Civil Aviation Directorate (commonly referred to as TC HQ) in Ottawa and at Civil Aviation branches (i.e., regional TC offices) in 5 regions across the country. The Director General of Civil Aviation (DGCA) is responsible for overseeing the overall and ongoing performance and operation of TC's Civil Aviation program.Footnote 152 The DGCA reports to the Assistant Deputy Minister, Safety and Security, who in turn reports to the Deputy Minister, Transport.
In each of TC's 5 regions, a Regional Director of Civil Aviation (RDCA) is responsible for overseeing TC's Civil Aviation program in that respective region. The RDCAs have a line-reporting relationshipFootnote 153 with a Regional Director General (RDG), who is responsible for all modes within the region. The RDGs report directly to the Deputy Minister, Transport. The RDCA also has a functional relationshipFootnote 154 with the DGCA, which allows the DGCA to provide direction within the scope of the Civil Aviation program.
Reporting directly to the RDCA is the Associate Director of Operations (ADO). The ADO is responsible for ensuring the strategic management of delivery of the Civil Aviation program within a regional area of responsibility. In Ontario, the region is divided into East and West, and there is an ADO assigned to each region. Reporting to the ADOs are technical team leaders (TTL), who are responsible for supervising delivery of assigned Civil Aviation program responsibilities. Working under the TTLs are the regional inspectors, responsible for the day-to-day interaction with operators.
1.18.8.3 Evolution of oversight
The expected results of TC's aviation safety program are that the aviation community have a strong safety culture and that aviation hazards and risks be systematically managed by the aviation community.Footnote 155
Traditional oversight was largely composed of audits and inspections aimed at ensuring regulatory compliance. This approach, however, is only a first step, as ensuring compliance with regulations alone does not assure the regulator that identified problems will not reoccur. TC has therefore moved toward a systems approach to oversight whereby, in addition to verifying a company's regulatory compliance, its internal processes are examined to verify that the organization has an effective system to manage the risks associated with its operations.
Initially, the move toward a systems approach to oversight was intended to coincide with a requirement that safety management systems, or SMS, would be implemented throughout the aviation industry. ICAO describes an SMS as
[…] a system to assure the safe operation of aircraft through effective management of safety risk. This system is designed to continuously improve safety by identifying hazards, collecting and analysing data and continuously assessing safety risks. The SMS seeks to proactively contain or mitigate risks before they result in aviation accidents and incidents.Footnote 156
In 1999, TC outlined the expected benefits of this approach as well as its anticipated change to a more cooperative oversight model, whereby the Department would take on a greater role in education and facilitation of safety management practices. Flight 2005: A Civil Aviation Safety Framework for Canada (TP 13521) stated:
The aim here is to improve safety through proactive management rather than reactive compliance with regulatory requirements. As aviation organizations generally possess an in-depth knowledge of the risks inherent to their operations, they are well placed to manage them and achieve positive shifts in their safety culture. Transport Canada's role is to provide these organizations with information on the safety management concept and to facilitate its implementation.Footnote 157
In 2006, TC published Flight 2010: A Strategic Plan for Civil Aviation (TP 14469). This document included objectives for implementing SMS and assisting the aviation community's transition to SMS. It demonstrated that TC remained confident that the move to SMS would facilitate the transition to a systems approach to oversight:
In the period immediately following 2010, the aviation industry will have implemented robust safety management systems in which the public and regulator have confidence. As companies evolve from compliance to safety risk-management thinking, regulators will transform from regulatory compliance auditors into system evaluators, as the underlying philosophy shifts the onus for proving or disproving adequate safety performance from the regulator to the organization.Footnote 158
The introduction of SMS and a systems approach to oversight was expected to foster a more cooperative approach to improving safety than would be possible under a traditional model of regulatory oversight. Among the objectives Flight 2010 outlined for facilitating this change was to “[c]reate a proactive culture within the industry, where the focus is on addressing issues and concerns, and not on imposing punitive measures.”Footnote 159
However, TC recognized its role in ensuring compliance with regulations and has stated that
SMS regulations are in addition to the pre-existing regulations and Transport Canada verifies that companies comply with all regulations. For those sectors that do not have SMS regulations, Transport Canada continues to verify that companies comply with existing regulations.Footnote 160
In order to develop a regulatory environment that is conducive to the successful implementation of SMS, TC has embodied its philosophy of greater cooperation in policies and procedures that favour use of an operator's safety management processes to address issues over use of punitive sanctions. For example, Civil Aviation Directive 107-004, Aviation Enforcement – Safety Management Systems states:
Transport Canada agrees to promote voluntary compliance with regulatory requirements, without necessarily resorting to punitive action, by providing certificate holders governed by an SMS, the opportunity to determine, by themselves, proposed corrective measures to prevent recurrence of a contravention, as well as the best course of action to help foster future compliance.Footnote 161
Since not all operators are required to have an SMS, this directive and the associated procedures supporting its implementation (e.g., Staff Instruction [SI] SUR-006Footnote 162) cannot yet be applied to all oversight activities.
1.18.8.3.1 International approach to safety management
ICAO is a special agency of the United Nations charged with creating and overseeing standards and recommended practices for civil aviation around the world. The ICAO Safety Management Manual provides states with guidance on the development and implementation of a state safety program (SSP). It provides guidance material for the establishment of SMS requirements by states and for SMS development and implementation by affected product and service providers.
The manual describes the rationale behind a systems approach to managing safety. It defines safety as “the state in which the possibility of harm to persons or of property damage is reduced to, and maintained at or below, an acceptable level through a continuing process of hazard identification and safety risk management.”Footnote 163 The manual also provides this description of the importance of SMS and a systems approach:
[…] traditional data collection and analysis efforts, which had been limited to the use of data collected through investigation of accidents and serious incidents, were supplemented with a new proactive approach to safety. This new approach is based on routine collection and analysis of data using proactive as well as reactive methodologies to monitor known safety risks and detect emerging safety issues. These enhancements formulated the rationale for moving toward a safety management approach.Footnote 164
Recognizing the benefits of a proactive approach to safety management, ICAO has incorporated the following standard requiring SMS:Footnote 165
3.1.3 As part of its SSP [state safety program], each State shall require that the following service providers under its authority implement an SMS:
[…]
b) operators of aeroplanes or helicopters authorized to conduct international commercial air transport, in accordance with Annex 6, Part I or Part III, Section II, respectively
Other countries have also begun to implement requirements for operators to implement SMS. By way of example, the situation in the United States and Australia will be discussed briefly.
FAA Order 8000.369A established a national policy with respect to SMS. It requires FAA organizations to develop implementation or continuous improvement plans for SMS and to establish guidance for their own SMS activities and their respective industry segments on implementing SMS. The order describes how SMS supplements traditional oversight and outlines the expected benefits of SMS:
With SMS, the FAA is better able to allocate resources and conduct safety oversight using safety management principles. The FAA establishes safety requirements for, and promotes SMS implementation in, product/service provider organizations, as appropriate. The FAA verifies compliance with regulations using a variety of means such as audits, evaluations, and inspections and confirms implementation and effectiveness of the aviation product/service provider's safety systems. In this way, FAA personnel are used more efficiently, and there is a higher level of confidence that an aviation product/service provider will meet safety standards, whether the FAA is present or not.Footnote 166
The FAA is also implementing requirements for SMS. For example, the FAA passed a rule requiring each air carrier operating under 14 Code of Federal Regulations (CFR) part 121 (scheduled air carriers) to develop and implement an SMS. The rule, which came into effect on 09 March 2015, specifies:
Air carriers authorized to conduct operations under part 121 must develop and implement an SMS within 3 years of the effective date of the final rule. To demonstrate that the air carrier's SMS will be fully implemented by the end of this three-year period, the air carrier will be required to submit an implementation plan within 6 months of the effective date of the final rule.Footnote 167
As described in the next section of this report, Canada has had requirements for this sector (CARs Subpart 705) since 2005.
As of March 2015, the FAA is considering requiring SMS for part 135 (unscheduled carriers) commercial operators.Footnote 168
The Civil Aviation Safety Authority in Australia has also recognized the additional benefits for safety afforded by the implementation of SMS:
To improve on existing levels of aviation safety in the light of the continuing growth of the industry, additional measures are needed. One such measure is to encourage operators to develop and implement their own SMS that fits the size and complexity of their operation.Footnote 169
Australia has implemented requirements for high-capacity regular public transport operators to complete a phased implementation of SMS by July 2010Footnote 170 and for low-capacity regular public transport operators to do so by February 2011.Footnote 171
1.18.8.3.2 Implementation of safety management systems in Canada
In 2005, the first SMS regulations came into effect, targeting Canadian airline operators (CARs Subpart 705) and the companies that perform maintenance on their aircraft. They were followed in 2008 and 2009 by SMS regulations for airports and air traffic service providers.
In 2009, TCCA introduced an enforcement policy to enable a non-punitive approach to a non-compliance with the CARs for operators transitioning to SMS.Footnote 172 Operators were required to have an effective internal reporting process and a reactive event-analysis process.
Also in 2009, TC delayed implementation of SMS regulations for the remaining aviation sectors “to allow more time for industry to prepare and for TC to refine oversight tools and provide updated training to front-line employees.”Footnote 173 As a result, SMS regulations have yet to be implemented in the following areas: commuter services, air taxi, aerial work, other approved maintenance operations, aircraft manufacturing, aircraft certification, and flight training.Footnote 174 These segments together comprise approximately 800 air operators representing more than 90% of Canadian certificate holders, although many companies within this group have voluntarily chosen to implement SMS.
Although TC had stated previously that SMS would be implemented in all regulated civil aviation sectors by 2015,Footnote 175 Footnote 176 the implementation schedule on TC's website at time of writing states:
Before putting in place SMS requirements for [sectors other than 705], Transport Canada is conducting an assessment to identify areas requiring attention and to verify that its inspectors and the industry are ready for this extension.Footnote 177
1.18.8.4 Air operator certificate
An operator must submit an application to TC for the issuance of an air operator certificate (AOC). According to CARs 703.07 and 704.07, the Minister shall
[…] issue or amend an air operator certificate where the applicant demonstrates to the Minister the ability to
- maintain an adequate organizational structure;
- maintain an operational control system;
- meet training program requirements;
- comply with maintenance requirements;
- meet the Commercial Air Service Standards for the operation; and
- conduct the operation safely.Footnote 178
To demonstrate those abilities, the operator is required to provide TC with documents that lay out the company's plan for maintaining an adequate organizational structure and an operational control system. These documents include a training manual outlining the company's approved training program, and a company operations manual (COM).
In addition, initial certification requires an applicant to have managerial personnel, approved by the Minister, in a number of positions, including an Operations Manager and Chief Pilot.
An AOC also contains a number of general conditions, outlined in CARs 703.09 and 704.09. For example, an air operator must conduct flight operations in accordance with its TC-approved COM and must conduct training in accordance with its TC-approved ground- and flight-training program.
1.18.8.5 Transport Canada's approach to surveillance
Regulatory oversight requires the regulator to determine what surveillance activities will be carried out, to conduct surveillance activities, and to follow up to verify that identified deficiencies have been addressed. The sections that follow describe TC's approach to the planning, conduct, and follow-up of oversight, including the guidance material to be used by inspectors in each phase—and how that approach evolved during the period surrounding the occurrence.
1.18.8.5.1 Planning
TC's surveillance activities fall under 2 broad categories: planned and unplanned. The former are conducted at a predetermined interval; the latter are conducted in response to unforeseen events or issues—such as accidents, incidents, or indications of increased risk.
In May 2012, TC adopted a risk-based approach to determining surveillance intervals for all companies, whether or not the companies have an SMS.Footnote 179 Previously, TC's surveillance policy had established a baseline surveillance interval for all TCCA enterprises, irrespective of the risk inherent to those operations.
Under the revised system, planned surveillance intervals may be as frequent as each year for high-risk or high-impact companies, or as infrequent as once every 5 years for those determined by TC to pose a lower risk or impact. These intervals are subject to an annual review and are determined using the following 2 criteria:
- A risk-indication level: This is a number from 1 to 5. The elements considered in determining this rating are the National Aviation Safety Information Management System (NASIMS) risk-indicator number, the results of the most recent surveillance activity, the availability of safety information, and whether the company has an SMS.
- An impact-value determination: This is a rating from A to E that takes into account the number of certificates held, number of employees, bases, aircraft types, type of operations, and whether the operator conducts international operations.
At the time of the occurrence, Ornge RW was on a one-year PVI schedule. Only operators with a risk-indicator level of “very high” and an impact-value score of “high” or “extreme” are subject to such a frequent surveillance interval.
An important tool in the surveillance-planning process, NASIMS includes a risk-indicator module consisting of 77 questions pertaining to 10 key hazard areas. According to SUR-005 Issue 01,Footnote 180 “question responses must be updated as new safety intelligence is received. This provides a near real-time risk picture […].” The responses are analyzed to calculate an operator's risk-indicator number.
1.18.8.5.2 Conduct
The move toward a systems approach to oversight has resulted in a change in the methods that TC uses to conduct surveillance. Traditional audits and inspections have been replaced by assessments,Footnote 181 PVIs, and PIs as the primary surveillance tools. These tools allow TC to evolve beyond compliance auditing and include a review of the effectiveness of a certificate holder's management systems.
The procedures outlining the use of these surveillance tools are found in SUR-001. There have been multiple versions of this document. At the time of the occurrence, SUR-001 Issue 04 was in effect. Issue 05 was published approximately 1 month after the occurrence.
1.18.8.5.2.1 Program validation inspections
A PVI is used to determine whether “all the requirements of a particular component of the SMS model or other parts of the regulations are documented, implemented, in use and effective.”Footnote 182
For each PVI, a convening authority is appointed and is responsible for
- determining the objective and scope of the PVI;
- appointing a PVI manager;
- overseeing selection of the PVI team;
- attending entry/exit meetings as required;
- reviewing and approving the PVI report and ensuring that the certificate holder receives it within the required time frame;
- ensuring appropriate, timely action is taken when an immediate threat to safety is identified;
- ensuring appropriate follow-up action is completed after the PVI; and
- sending a letter to the certificate holder upon completion of the PVI.
Six weeks prior to conducting a PVI, the team gives the operator notice.Footnote 183 Once a PVI team is selected, copies of documentation are requested for review, and the PVI manager develops a plan for the approval of the convening authority. This PVI plan includes details of the interviews and documents to be reviewed. Guidelines are provided to help determine the appropriate sample size.
The PVI manager then verifies that requested documents have been provided. A document review is conducted by the PVI team 2 weeks before the on-site portion of the PVI. Other relevant information is also reviewed at this time, including the results of previous surveillance activities, safety data, compliance history, and administrative actions with respect to the operating certificate.
During the on-site portion of the PVI, the team conducts interviews and sampling, gathers evidence to support observations, analyzes those observations, determines whether the operator is in compliance with regulations, and, if the organization is required to have an SMS, whether that SMS is effective.
SUR-001 Issue 04 set out a scoring system, for internal use, to assist in describing the extent to which an organization is in compliance with a list of expectations. A scale of 1 to 5 was used, wherein a score of 1 meant that a given element was missing, undocumented, or completely ineffective; a score of 3 meant that the element met regulatory requirements; and a score of 5 meant that the element met all regulatory requirements and represented industry best practice.
The PVI team also prepares any findings of non-conformance where applicable, and documents the results of the PVI using worksheets provided for that purpose.
Findings are recorded on a form that provides areas for an inspector to identify the applicable regulatory requirement and sufficient examples to illustrate the non-conformance.
Under SUR-001 Issue 04, assessment and PVI findings of non-conformance with a regulatory requirement or a best practice were classified using 1 of 4 designations: minor, moderate, major, or critical (Appendix D).
The on-site portion of the PVI concludes with an exit meeting, and a report is presented to the certificate holder within 30 days.
1.18.8.5.2.2 Process inspection
Similar to a PVI, a process inspection (PI) is used to determine whether an operator's processes meet regulatory requirements and are functioning as intended. It is also conducted in a similar manner to a PVI. However, the scope of a PI is limited to a single process and is intended to help TC determine the level of risk associated with an operator and whether additional surveillance is required.
A PI may also generate findings, and may lead to the initiation of additional surveillance. However, unlike a PVI, findings identified during a PI are not assigned ratings. When a PI reveals safety-related issues, “a PVI may be conducted on an urgent basis to collect sufficient material to support the issuance of a formal report and an NoS [Notice of Suspension], as necessary.”Footnote 184
The report produced at the end of a PI must indicate whether the process being inspected meets applicable regulatory requirements and is being followed as published in approved company manuals, or whether the process is not documented, not implemented, or not effective.
1.18.8.5.3 Follow-up
As stated above, upon conclusion of a PVI or PI, the convening authority is responsible for selecting appropriate follow-up action. Tools intended to guide an operator into compliance will be discussed in the sections that follow. Those tools include
- Corrective action plan (CAP): a plan submitted in response to findings that outlines how the certificate holder proposes to address identified deficiencies and manage the associated risks.
- Enhanced monitoring (EM): increased surveillance while a certificate holder develops and implements measures to address identified systemic deficiencies or regulatory non-compliance.
- Certificate action: notice given to an operator, either immediate or with a timeline attached, that action will be taken against the AOC. This is done via an NoS or a Notice of Cancellation (NoC).
- Enforcement action: the application of administrative or monetary penalties.
The guidance given to inspectors on selecting and applying the appropriate follow-up actions from these 4 options evolved over time. The following 7 TC publications contained much of the guidance available, and are relevant to the analysis in this report:
- SUR-001 Issue 04, Surveillance Procedures (17 November 2010)
- SUR-002 Issue 02, Enhanced Monitoring (22 September 2010)
- SUR-014 Issue 01, Suspension or Cancellation of Canadian Aviation Documents for Safety Reasons (19 July 2011)
- Internal Process Bulletin (IPB) 2012-02, Changes to Clarify Transport Canada's Surveillance of Certificated Enterprises (07 May 2012)
- SUR-001 Issue 05, Surveillance Procedures (28 June 2013)
- Internal Process Bulletin (IPB) 2013-02, Clarification in Respect to Certificate Action in Accordance with Section 7.(1), 7.1(1)(b), and 7.1(1)(c) of the Aeronautics Act (06 August 2013)
- SUR-002 Issue 03, Enhanced Monitoring (02 December 2013).
Only the first 4 of these documents were in effect during the period leading to the occurrence and for the surveillance resulting from the occurrence. A summary of relevant guidance, and of how it changed over time, is provided below.
1.18.8.5.3.1 Guidance in effect in the period up to and immediately after the occurrence
SUR-001 Issue 04, Surveillance Procedures (17 November 2010)
This document specified that a CAP was required for all findings. Post-surveillance actions in addition to a CAP were linked to the severity of findings. For example, for a critical finding, SUR-001 Issue 04 states that an immediate NoS is appropriate in relation to paragraph 7.1(a) of the Aeronautics Act. A major finding, by comparison, “will typically require a more rigorous and lengthy CAP than a minor or moderate finding. An NoS with a 30 day notice period and Enhanced Monitoring should be considered.”Footnote 185
SUR-001 Issue 04 also described how the CAP process would verify that an operator had corrected the identified deficiencies. At a minimum, a CAP would include a review of the non-conformance, a root-cause analysis identifying what caused the non-conformance, proposed corrective actions, an implementation timeline, and confirmation of managerial approval for the corrective action.
This document also specified time frames for the CAP process as follows:
- TC had to present a report of its surveillance to the certificate holder within 30 calendar days of the last day of the on-site portion of its surveillance.
- Upon receipt of the surveillance report from TC, an operator had to provide a CAP within 30 days.
- The primary inspector had 10 days to review the CAP.
- If a CAP was accepted, a plan for either administrative or on-site follow-up was to be produced by TC and the certificate holder notified.
- For a CAP deemed unacceptable, an operator could be given 5 days to amend it, with TC having an additional 5 days for its review. The SUR also specified that, where a CAP required major changes, an NoS could be issued.
- In most cases, follow-up to close a CAP was expected within 90 days of TC's acceptance of the CAP. The 90-day period did not begin until a CAP was accepted.
SUR-002 Issue 02, Enhanced Monitoring Program (22 September 2010)
This document defines EM as
a process to closely monitor a certificate holder, after an assessment or PVI has been conducted, to ensure that the certificate holder's regulatory performance does not deteriorate further while the certificate holder develops and implements measures to deal with its systemic deficiencies or regulatory non-compliance before the second or subsequent PVI is conducted.Footnote 186
SUR-002 Issue 02 also sets out 2 expectations for the use of EM: first, that the company will improve its systems, ensuring compliance with regulations; and second, that a comprehensive look by TC at the certificate holder's systems will confirm a company's ability or inability to maintain compliance with regulations.
Of note, SUR-002 Issue 02 links the initiation of EM to an NoS as follows:
(b) a score of 2 where there are major findings may result in the issuance of a Notice of Suspension (in effect in 30 days) and may place the certificate holder under EM; and
(c) a score of 1 will result in the issuance of a Notice of Suspension (in effect immediately) and may place the certificate holder under EM.Footnote 187
That information is consistent with the post-surveillance decision-making guidance provided in SUR-001 Issue 04, which describes possible actions to be taken based on the severity of the findings. However, SUR-002 Issue 02 also states that the convening authority has discretion as to when EM will be used, and that it will be applied to certificate holders with a history of non-compliance or a failure to produce an effective CAP.Footnote 188
SUR-002 Issue 02 sets out the process for initiating and terminating EM, and outlines the relevant roles and responsibilities for each stage of this process. In particular, when an enterprise is placed under EM, an EM plan will be prepared by the selected team leader for approval by the EM manager. Among other specifications, the plan will identify what surveillance tools will be used during the EM period and how often. The surveillance may include CADORSFootnote 189 report reviews, ramp checks, training monitors, on-site interviews with staff, discreet surveillance, review of company documents, etc. The SUR establishes a maximum period of 90 days for a first period of EM and the requirement for a PVI to be conducted to terminate the EM.
SUR-014 Issue 01, Suspension or Cancellation of Canadian Aviation Documents for Safety Reasons (19 July 2011)
This document provides guidance on how to take certificate action under 2 sections of the Aeronautics Act: section 7 (immediate threat to safety) and section 7.1 (other grounds).
Under section 7 of the Aeronautics Act, the Minister of Transport has the authority to suspend a Canadian aviation document “when there are grounds to believe that an immediate threat to aviation safety exists or will occur as a result of an action carried out in accordance with the privileges granted by a CAD.”Footnote 190
What constitutes an immediate threat to aviation safety is not defined in the Aeronautics Act. However, according to SUR-014, the phrase is defined as “a threat to the safety of an aircraft that currently exists or is about to exist, and creates a reasonable expectation that unless immediate action is taken to neutralize the threat, death, injury or significant damage to property is imminently likely.”Footnote 191
SUR-014 also specifies that certificate action can be taken, in accordance with subsection 7.1(1) of the Aeronautics Act, for the following reasons:
- Incompetence: The SUR states that certificate action based on incompetence is applicable only to individuals, and not to organizations.
- Certification: The SUR indicates that certificate action under this section of the Act is appropriate when an operator no longer meets the qualifications required for the certificate to be issued. However, it specifies that certificate action is not appropriate under this section where an operator does not meet the general conditions associated with the operating certificate (e.g., for non-compliance with its COM or training manual). Rather, in these circumstances, enforcement action may be taken under the associated section of the CARs.
- Public interest: This category is used when the aviation record of the document holder includes non-compliances that are “serious and repeated enough to conclude that there is a risk of further offenses.”Footnote 192 In pursuing certificate action under this section of the Act, the SUR states that it would be appropriate to consider records, including accident records, compliance records (aviation enforcement division records), and audit, program validation or assessment records as they relate to system compliance. The SUR adds that non-compliance issues that were identified during oversight and have been resolved through corrective action are not suitable for pursuing such certificate action.
Internal Process Bulletin (IPB) 2012-02, Changes to Clarify Transport Canada's Surveillance of Certificated Enterprises (07 May 2012)
This document modifies some of the procedures found in SUR-001 Issue 04. It provides additional guidance with respect to the systems approach to surveillance, the planning and conducting of sampling, the development and documentation of findings, and the post-surveillance analysis and decision-making process.
In its post-surveillance and decision-making sections, IPB 2012-02 states that, when non-compliances have been identified, the convening authority shall consider the number of findings, their severity, the systemic nature of the findings, and the organization's compliance and enforcement history in deciding on the most appropriate actions to address the unsafe conditions. According to IPB 2012-02, the convening authority's options include:
- Requesting a CAP;
- Issuing a detection notice;
- Requesting a CAP and issuing a detection notice; or
- Issuing a notice of suspension or cancellation.Footnote 193
Enhanced monitoring (EM) is not one of the options.
In regard to taking certificate action, IPB 2012-02 reiterates that it must be done in accordance with SUR-014.
1.18.8.5.3.2 Guidance issued after the occurrence
SUR-001 Issue 05, Surveillance Procedures (28 June 2013)
This document is an extensive restructuring of SUR-001 Issue 04, and provides guidance related to post-surveillance decision making. It specifies that the surveillance team will recommend follow-up action for every non-conformance, which will be reviewed by a surveillance review committee, consisting of, at minimum, the convening authority and the surveillance manager.
A CAP is required for each finding that results from the surveillance activity. Where findings are not severe in nature and the organization has demonstrated an ability to comply with regulatory requirements, the surveillance team may recommend that the CAP process be used on its own. In other circumstances, the surveillance team can recommend adding any combination of the following actions:
- Enforcement action
- Enhanced monitoring
- Certificate action
The criteria to be considered in developing these recommendations are
- the number of findings;
- the classifications of the findings;
- the organization's compliance history;
- the organization's safety record; and
- the organization's ability to produce a CAP.Footnote 194
Of note, the guidance provided in SUR-001 Issue 05 differs from that in the previously issued IPB 2012-02 in that EM is specifically listed in the SUR as a post-surveillance option. In addition, SUR-001 Issue 05 specifically instructs inspectors to consider an operator's ability to produce an acceptable CAP when selecting post-surveillance options.
Internal Process Bulletin (IPB) 2013-02, Clarification in Respect to Certificate Action in Accordance with Section 7.(1), 7.1(1)(b), and 7.1(1)(c) of the Aeronautics Act (06 August 2013)
This document was issued to address a “misconception” that inspectors lacked “the appropriate tools to take certificate action when warranted.”Footnote 195 IPB 2013-02 states that this misconception was rooted in 3 factors:
[1] a lack of information around the evidence required to support “public interest” requirements,
[2] a misunderstanding of the requirements attached to “establish and maintain” […] and
[3] a lack of knowledge as to when section 7.(1) of the [Aeronautics] Act may be used.Footnote 196
According to IPB 2013-02, after all evidence has been gathered to support findings, the possible courses of action that can be taken are
- Requesting a CAP, including a root-cause analysis;
- Assessing punitive enforcement action; or
- Taking certificate action (notice of suspension or notice of cancellation of a Canadian aviation document).
To help determine which option is most appropriate, IPB 2013-02 states that
where a non-compliance does not indicate a safety issue, a CAP or punitive enforcement measure are the appropriate measures. If the corrective measure is not effective and the problem reoccurs, firmer action can be taken. Where a safety issue is evident, certificate action should be considered and can be taken in conjunction with other enforcement measures as required.Footnote 197
On the subject of certificate action, IPB 2013-02 advises, “The success of the certificate action taken relates directly to the quality of the match between the regulation that is in non-compliance and the provision of the Act that is used to pursue certificate action.”Footnote 198 The bulletin goes on to provide a test for use in determining the most appropriate section of the Act to apply if pursuing certificate action as a consequence of non-compliance with provisions related to certification requirements or with rules of conduct (offence-creating provisionsFootnote 199). In particular, it suggests that the surveillance team ask the following question: “If the CAD holder was applying for the document given its current state of compliance, would the CAD be issued?”Footnote 200 If the answer to that question is no, certificate action is supported under paragraph 7.1(1)(b) of the Act. If the answer is yes, then a public-interest case under paragraph 7.1(1)(c) would be the most appropriate recourse.
SUR-002 Issue 03, Enhanced Monitoring (02 December 2013)
This document contains extensive revisions of Issue 02, although the purpose of and process for EM that it outlines remain essentially the same. A critical difference between the 2 documents is that, in Issue 03, the link between the initiation of EM and the use of an NoS has been removed.
SUR-002 Issue 03 states that EM may be initiated following a surveillance activity with major findings demonstrating systemic failures that have led to non-compliance with regulatory requirements, or in response to an accident or persistent record of non-compliance. Issue 03 also institutes a requirement that EM be approved by, at minimum, a regional ADO or HQ chief, who will then assume the role of convening authority.
1.18.8.6 Training on surveillance procedures
Investigators conducted a review of the mandatory training being provided to new TCCA Inspectors at the time of the occurrence.
The majority of TC's Surveillance Procedures Training Program was focused on conducting SMS assessments, which are applicable only to SMS enterprises. In total, approximately 20 hours of classroom time was dedicated to SMS assessments. Approximately ½ hour of classroom time was dedicated to PVI training, despite the fact that more than 90% of Canadian commercial air carriers are not required by regulation to have an SMS, and are therefore not subject to assessments. According to the training program, the major differences between an SMS assessment and a PVI are their scope, degree of formality, and timelines.
Of note, the training made no reference to an organization's resources or ability to effectively develop CAPs that would address the underlying cause of any identified findings.
1.18.8.7 Previous TSB communications on regulatory oversight
1.18.8.7.1 Previous TSB recommendation
Following a 1999 accident involving a de Havilland DHC-6-300 Twin Otter that crashed while conducting a below-minimums instrument approach procedure,Footnote 201 the TSB issued Recommendation A01-01. Recommendation A01-01 recognized that effective oversight of smaller or remote operations is a challenging task. The TSB nonetheless believes strongly that the level of acceptable risk should not be greater for passengers and crews who fly on those aircraft simply because oversight is more difficult. During its investigation of the 1999 occurrence, the TSB determined that more needed to be done by TC to reduce the level of risk in these operations. In particular, the TSB pointed out that TC's sole reliance on traditional methods of inspection, audits, general oversight, and regulatory penalties appeared to have had limited success in fostering the appropriate safety cultures in some companies and individuals; consequently, unsafe conditions continued to exist, and unsafe acts were still being committed. The Board therefore recommended that
The Department of Transport undertake a review of its safety oversight methodology, resources, and practices, particularly as they relate to smaller operators and those operators who fly in or into remote areas, to ensure that air operators and crews consistently operate within the safety regulations.Footnote 202
Transportation Safety Recommendation A01-01
In its 2001 response, TC advised that it is “continually reviewing its safety oversight program methodology, resources and practices […]”Footnote 203 It cited the promulgation of the CARs in 1996, the Safety of Air Taxi Operations Task Force report published in 1998, and the planning document Flight 2005, and stated that a “comprehensive external review of the Civil Aviation safety oversight program”Footnote 204 had been completed in July 2001.
Due to the general nature of TC's response, combined with its stated commitment for ongoing improvement, the TSB assessed the response as Satisfactory Intent. In 2005, TC provided an updated response to Recommendation A01-01; it echoed its earlier statements about continually reviewing its safety oversight program, and advised that the Department had moved forward to include the following:
- Safety Management Systems in the aviation program and regulations instilling a safety culture in the aviation industry;
- instilled a risk management philosophy for decision making;
- produced the Flight 2010 – A Strategic Plan for Civil Aviation document;
- adopted the TC Civil Aviation Business Model; and
- reviewing internal organizations optimizing its resources for safety.Footnote 205
Based on these stated improvements, the TSB believed that the measures listed would substantially reduce the safety deficiency that existed. In June 2006, therefore, the Board assessed TC's response as Fully Satisfactory, and no further follow-up action was deemed necessary.
1.18.8.7.2 Recent investigations
The TSB has conducted a number of investigations examining the effectiveness of regulatory oversight.
1.18.8.7.2.1 TSB Aviation Investigation Report A07C0001
This report included the following 2 findings as to risk:
- Transport Canada (TC) Prairie and Northern Region (PNR) management practices regarding the June 2006 replacement of the regional combined audit program, in order to manage safety management system (SMS) workload, did not conform to TC's risk management decision-making policies. Reallocation of resources without assessment of risk could result in undetected regulatory non-compliance.
- Although TC safety oversight processes identified the existence of supervisory deficiencies within TWA, the extent of the deficiencies was not fully appreciated by the PNR managers because of the limitations of the oversight system in place at that time.Footnote 206
In its description of safety actions taken, the report stated:
TC forecasts that draft regulations will be published in Part I of the Canada Gazette in December 2009 requiring CAR 703 and 704 operators to implement safety management systems (SMS) in accordance with a phased schedule. Adoption of an effective SMS by these operators should significantly mitigate the types of management and operational issues identified in this report.Footnote 207
1.18.8.7.2.2 TSB Aviation Investigation Report A10Q0098
This report included 1 finding as to causes and contributing factors related to regulatory oversight: “The significant measures taken by TC did not have the expected results to ensure compliance with the regulations, and consequently unsafe practices persisted.”Footnote 208
The following safety action was reported by TC:
Transport Canada has made significant changes to its surveillance program. These changes include updates to the methods used for surveillance planning and the introduction of tools that provide an improved capacity for the monitoring and analysis of risk indicators within the aviation system.Footnote 209
1.18.8.7.2.3 TSB Investigation Report A10Q0117
This report included 1 finding as to causes and contributing factors related to regulatory oversight: “The action taken by TC did not have the desired outcomes to ensure regulatory compliance; consequently, unsafe practices persisted.” In addition, the report included another finding that: “The carrier's operations manual had been approved by Transport Canada for the carriage of external loads, despite the fact that the carrier did not have the required supplemental type certificate (STC).”Footnote 210
1.18.8.7.2.4 TSB Aviation Investigation Report A12W0031
This report included 1 finding as to risk related to regulatory oversight: “If adequate surveillance is not maintained by Transport Canada, there is an increased risk that operator safety deficiencies will not be identified.”Footnote 211
1.18.8.7.2.5 TSB Aviation Investigation Report A12C0154
This report included 1 finding as to risk related to regulatory oversight: “If Transport Canada does not provide the same degree of oversight for repetitive charter operations as it does for a scheduled operator, the risks in the operator's activities may not be fully evaluated.”Footnote 212
1.18.8.7.2.6 TSB Aviation Investigation Report A13W0120
This report included 2 findings as to causes and contributing factors related to safety management and regulatory oversight:
The operator's safety management system was ineffective at identifying and correcting unsafe operating practices.
Transport Canada's surveillance activities did not identify the operator's unsafe operating practices related to weight and balance and net take-off flight path calculations. Consequently, these unsafe practices persisted.Footnote 213
The report also included the following finding as to risk related to regulatory oversight:
If Transport Canada does not adopt a balanced approach that combines inspections for compliance with audits of safety management processes, unsafe operating practices may not be identified, thereby increasing the risk of accidents.Footnote 214
1.18.8.7.2.7 TSB Aviation Investigation Report A13H0002
This investigation report included the following 3 findings as to risk:
If identified regulatory surveillance intervals are not respected, then there is an increased likelihood that systemic deficiencies that could increase risk will go unidentified and unaddressed.
If findings are overly general, it increases the scope of possible corrective actions and makes it more difficult for the regulator to assess whether the underlying deficiency is addressed through the corrective action plan increasing the risk that safety deficiencies will remain unaddressed.
If Transport Canada does not take action to require operators to respect corrective action plan implementation timeframes, there is a risk that safety deficiencies will not be corrected in a timely manner.Footnote 215
1.18.8.8 TSB Watchlist
In 2012, SMS was added to the TSB's Watchlist, which identifies the issues posing the greatest risk to Canada's transportation system.
In 2012, the Watchlist highlighted that TC “does not always provide effective oversight of aviation companies transitioning to safety management systems, while some companies are not even required to have one.”Footnote 216 It went on to state that “Transport Canada must effectively monitor the integration of SMS practices into day-to-day operations. Moreover, SMS practices need to be adopted by all companies.”Footnote 217
In 2014, a newer edition of the Watchlist further identified that some transportation companies are not effectively managing their safety risks, and that TC oversight and intervention has not always proven effective at changing companies' unsafe operating practices.Footnote 218, Footnote 219 To resolve these issues, the Watchlist states:
- Transport Canada must implement regulations requiring all operators in the air and marine industries to have formal safety management processes. And Transport Canada must oversee these processes.
- In all transportation modes, those companies that do have SMS must, in turn, demonstrate that it is working—that hazards are being identified and effective risk mitigation measures are being implemented.
- Finally, when companies are unable to effectively manage safety, Transport Canada must not only intervene, but do so in a manner that succeeds in changing unsafe operating practices.Footnote 220
1.18.9 Transport Canada's oversight of Ornge Rotor-Wing
1.18.9.1 General
Ornge RW was granted its operating certificate in January 2012. The following sections provide a chronology of some of the significant surveillance activities that TC has since carried out in respect to the company.
1.18.9.2 Training issue (May 2012)
In early May 2012, before any formal surveillance, TC's POI assigned to Ornge RW learned that there were gaps in the company's simulator training program. In particular, practical CFIT-avoidance training was not being completed as required by the company's TC-approved Training Manual.
In response to this observation, Ornge RW informed TC that it had addressed the issue with its training provider, and that the training would now be completed. Since the company had indicated that the issue was resolved, TC took no further action.
1.18.9.3 Process inspection (27 November to 02 December 2012)
In mid-January 2012, the POI of Ornge RW advised senior regional TC management that, because the company was a “very large and complicated operator”,Footnote 221 TC should plan to review the operation within the next 12 months, and suggested that a post-certification PI be planned for the fall of 2012. That routine surveillance opportunity came in late November 2012. The PI consisted of monitoring of Ornge RW's AW139 recurrent flight crew training by the POI. The pilots undergoing the training were the company's OM and Assistant CP.
The POI determined that the majority of the training was conducted as approved, in accordance with CARs Subpart 704. However, the POI observed the 2 pilots carrying out black-hole approaches without the use of SOPs. Furthermore, the pilots received no reinforcement or training from the instructor on the use of company SOPs during the recurrent training. On returning from the recurrent training, the POI emailed the OM and Assistant CP, and outlined his concerns about the lack of SOP usage during a TC-monitored simulator ride.
The AW139 Recurrent Training Process Inspection Report indicated that there were non-conformance issues related to company SOPs and to training in the use of SOPs. On 03 January 2013, TC issued Finding FO-05-01: Operational Control Flight Operations. In that finding, the Department advised Ornge RW that it had a non-conformance with CAR 704.12(1), which states, “An air operator shall ensure that all operations personnel are properly instructed about their duties and about the relationship of their duties to the operation as a whole.”Footnote 222
In its response to TC, Ornge RW indicated that changes had been made to the company's SOPs, and that flight crews had been advised to decline black-hole approaches if they had not received black-hole training in the previous 12 months. Ornge RW also reported that meetings had been held with the training provider to ensure that all required training was being completed, that the training syllabus had been updated to include variance training, and that the requirement to include CFIT-avoidance training during aircraft flight training was being met.
The company's CAP identified the losses and subsequent lack of key operational personnel during the company's start-up and transitional periods as the root cause of the deficiencies that had been identified in the areas of SOPs and training.
On 20 February 2013, TC sent a letter informing Ornge RW that its CAP associated with Finding FO-05-01had been reviewed and accepted. In that letter, TC advised that it would “continue to monitor the progress of your CAP by completing a follow-up process which may include an administrative process and/or an on-site inspection to ensure your proposed plan has in fact addressed all of the findings.”Footnote 223 That follow-up had not happened at the time of the accident.
1.18.9.4 Program validation inspection (09 to 24 January 2013)
1.18.9.4.1 General
As part of its planned surveillance, TC scheduled a PVI of Ornge RW from 09 to 18 January 2013. The purpose of the PVI was to verify that the organization had an effective operational control system and a quality assurance program. The PVI was conducted in accordance with SUR-001 Issue 04 and SUR-001-P Issue 03. Due to issues discovered during the PVI, the process was extended until 24 January 2013. The PVI consisted of an off-site review of the company's operational control system and quality assurance program as described in the COM. It also comprised an on-site portion involving interviews with key personnel, sampling of records, and observance of work.
1.18.9.4.2 On-site portion of the program validation inspection
On 09 January 2013, in a briefing note, the PVI team advised the regional ADO and RDCA that there were “strong indications that some portions of the flight crew training program have not been completed.”Footnote 224 During a meeting later that afternoon, the PVI team advised Ornge RW's senior management that the management had until 0900 on 10 January 2013 to “demonstrate that the crews were qualified.”Footnote 225 Later that evening, the OM/interim CP and the Assistant CP conducted a review to determine the certification of the company's flight crews. As a result of their research, they discovered that all 14 crew members starting day shift on 10 January 2013 were missing the required “Emergency Procedures Practical Training”, and that 2 of those flight crew members also required “Ground Service and Handling Training.” This information was communicated to the PVI team on the morning of 10 January 2013.
According to notes produced by TC following the afternoon meeting on 09 January, Ornge RW “voluntarily made the decision to shut down the rotary operation at shift change”Footnote 226 to ensure that the training was completed prior to commencing the next shift. The investigation learned that the PVI team intended to issue an immediate-threat-to-safety NoS, due to the nature of its findings, if the company did not voluntarily shut down operations. In TC notes, the lack of CFIT-avoidance training in accordance with Ornge RW's TC-approved Training Manual was also discussed. According to those notes, “the rotary wing crews have not been trained in accordance with their training manual (requirement for IFR and night VFR operation).”Footnote 227 This observation was essentially the same as the earlier observation made by the POI in May 2012, which the company indicated had since been rectified with its AW139 training provider.
In addition to identifying the deficiency in CFIT-avoidance training, the PVI team discovered that many of the company's pilots were missing
- the practical portion of emergency procedures training;
- critical surface contamination and airborne icing recurrent training;
- servicing and ground-handling training; and
- aircraft-type technical ground-training records.
In a letter to TC dated 10 January 2013, Ornge RW advised that the 16 pilots scheduled for day shift on 10 January 2013 “were notified both by phone and email that prior to conducting any flight operations, these deficiencies were to be rectified by provision of missing paperwork or by completion of identified training gaps.”Footnote 228 The letter also stated that “[f]lying activities at all rotor bases were temporarily suspended until compliance was confirmed.”Footnote 229 On the subject of the missing practical CFIT-avoidance training, the letter indicated that a CAP had been developed “pending TC approval” and “[t]o comply with our Training Manual, a short term corrective action plan is forthcoming to address the absent flight training portion of CFIT.”Footnote 230
On 11 January 2013, the PVI team requested training records to see how Ornge RW was documenting the operational progression of its recently hired first officers. The company advised TC that there were no such training records. Later that day, the PVI team reviewed 7 pilot training files that Ornge RW had verified as being complete and acceptable. According to correspondence between the PVI team and the OM, “[a] quick sampling of the (7) files shows that 100% of the files still have significant concerns […]”Footnote 231 Notably, several of the concerns cited by TC at this time were the same as those raised on 09 January 2013, before the company temporarily shut down its operation.
The PVI team leader advised Ornge RW that, contrary to its 10 January 2013 letter to TC (which stated that a CAP had been developed “pending TC approval”), a CAP had not been received to address the absence of practical CFIT-avoidance training, and requested that Ornge RW respond regarding the status of this matter. Shortly thereafter, the PVI team leader advised the ADO and the RDCA that there were “some very significant issues within the process, procedures and management structure at 7506406 Canada Inc.”Footnote 232 The PVI team also indicated to the regional TC management that Ornge RW would be advised that it was not permitted to operate without completion of the entire flight crew training program. In Ornge RW's response to TC, later that day, the company indicated: “we will certainly advise Transport Canada as soon as possible of a corrective action plan, including CFIT, to ensure all possible risks are appropriately mitigated in the future.”Footnote 233 However, as described above, the pilots who were missing the practical portion of the required CFIT-avoidance training did not complete the training before returning to operational status.
Given the PVI team's additional identification of missing training or documentation, Ornge RW voluntarily suspended operations again on 14 January 2013. In its response to the PVI team, the company again reported that the pilots in question had been notified by phone and email that the identified deficiencies must be rectified, either by provision of missing paperwork or by completion of the missing training.Footnote 234 The letter also repeated that a short-term CAP was forthcoming to address the absence of CFIT-avoidance training.Footnote 235
Subsequent to this second operational shutdown, the PVI team discovered several other training deficiencies. Those items were captured in email correspondence sent on 17 January 2013 by the PVI team to Ornge RW management. That correspondence stated that, “as discussed at the meeting, held this afternoon, the following items must be addressed and an immediate action plan developed to ensure regulatory compliance.”Footnote 236 The items identified were as follows:
- Variant and differences training on the S-76A type had not been completed as required by regulation.
- Ornge RW did not have a process in place to ensure that flight crews had completed the entire ground and flight training program.
- The AvAIO tracking software needed to be reviewed to determine compliance with all required flight crew training items, ensuring that the software reflects the exact status of each flight crew member.
- Ornge RW needed to establish a weight-and-balance control system that ensures weight-and-balance calculations are completed and documented on all flights.
- Flight and duty times needed to be tracked daily for all flight crews, and the flight crews needed to understand and use the tracking system and process.
Later in the evening of 17 January 2013, in correspondence with senior regional management at TC, the PVI team wrote that Ornge RW's “operational control system has not identified and reacted to several program/system issues”Footnote 237 and cited problems related to the issues listed above.
In response to TC's 17 January 2013 request, Ornge RW provided TC with an immediate CAP that addressed the 5 items identified above. The CAP included a number of different actions to address deficiencies identified during the PVI; however, it did not mention practical CFIT-avoidance training. Senior personnel at the company advised the Department that it would take time to rectify the CFIT-avoidance training issue, since it involved third-party training providers. Given that the senior leadership at Ornge RW had been fully cooperative with the PVI team and indicated a strong desire to rectify this training deficiency, TC agreed to give the company some time to sort out the issue with its training providers and did not restrict the company in any way at that point in time. On 24 January 2013, Ornge RW submitted a CAP to TC that addressed practical CFIT-avoidance training as well as some other missing ground and flight training items. That CAP is discussed later in this report.
1.18.9.4.3 Transport Canada's decision-making process following the program validation inspection
On 22 February 2013, members of the PVI team met with senior TC regional management to discuss the way ahead with regard to Ornge RW. The outcome of that meeting was captured in a decision record, which was signed hours after the accident on 31 May 2013. Although the company had not addressed the issue of missing CFIT-avoidance training, the 31 May 2013 decision record indicated that Ornge RW supplied documents and records “to show that all required non-conformances had been addressed and that no crew would operate an aircraft without appropriate training.”Footnote 238
According to the decision record, the PVI team and senior TC regional management considered the 2 following options: 1) issuing an NoS, or 2) allowing the operator to develop a CAP within the regular time frame of 30 days. The latter option was selected and the following rationale provided in the decision record:
This decision was (and is) aligned with the current policy and operational philosophy in place at Transport Canada (see addendum) - If an operator unequivocally agrees with the findings and is willing to take a proactive approach by developing a comprehensive short-term and long-term corrective action plan, they can be given the option to do so.Footnote 239
The decision record of 31 May 2013 indicated that additional monitoring and oversight would be discussed in “the near future”,Footnote 240 and cited another decision record, dated 18 March 2013, that had been produced shortly after the PVI report was sent to Ornge RW. In that 18 March decision record, TC stated, “The operator responded to these issues [identified non-conformances] proactively and corrected any immediate deficiencies.”Footnote 241 However, as stated above, Ornge RW's CFIT-avoidance training deficiency had not yet been addressed, as the company was still working with the training provider to obtain an agreement that the practical CFIT-avoidance training would be conducted.
The investigation also examined whether Ornge RW's provincial role influenced TC's decisions in the aftermath of the January 2013 PVI. Following a number of interviews and a review of all documentation related to the post-PVI decision-making process, there was no indication that, subsequent to the January 2013 PVI, regional TC personnel had been influenced by Ornge RW's provincial emergency medical services role.
1.18.9.4.4 Program validation inspection report and Ornge Rotor-Wing's corrective action plan
According to SUR-001 Issue 04, a PVI report “shall be presented to the certificate holder within 30 calendar days calculated from the last day of the on-site portion of the PVI”.Footnote 242 In this instance, TC produced its report on Ornge RW's January 2013 PVI on 01 March 2013. The report indicated that the PVI team had discovered “several examples of non-conformance to the Company Operations Manual, and in some cases the Canadian Aviation Regulations”Footnote 243 as well as examples of non-compliance of the Maintenance Control Manual with the CASS. Further, the report stated:
There were strong indicators that areas of the operational control system were not effective. The dates of some crew training records were not recorded and a range of crew training program requirements had not been met. On-site interviews revealed confusion both at the management level, and with the flight crews, over the application and management of the “flight time and flight duty time” program.Footnote 244
Although the report did not include a PVI score, the company received a score of 2 out of 5 as a result of the January 2013 PVI findings, according to TC. There were 9 findings in total: 3 critical, 2 major, and 4 moderate, classified in accordance with SUR-001 Issue 04. Each finding is explained later in this section.
On 10 April 2013, Ornge RW submitted CAPs for each of the 9 findings identified in the PVI report. The OM and the Assistant CP were primarily responsible for drafting the CAPs, with input from the PRM. This was the first time that the OM and the Assistant CP had been involved in preparing CAPs for TC. On 18 April 2013, TC advised the company that 8 of the 9 submitted CAPs had been rejected. The remaining CAP, associated with a finding related to the company's Maintenance Control Manual, was accepted on 25 April 2013.
On 26 April 2013, regional TC personnel met with senior management from Ornge RW to discuss the CAPs that had been rejected. During that meeting, TC advised the company that it “had not done a sufficient in depth analysis to get to root cause [sic] of the majority of the findings.”Footnote 245 TC then advised Ornge RW senior management that the company had been granted an additional 2 weeks to complete further analysis and re-submit the 8 outstanding CAPs to TC.
On 13 May 2013, Ornge RW re-submitted the 8 outstanding CAPs for TC's approval. These revised CAPs were accepted by TC in a letter dated 30 May 2013.
The paragraphs below describe each of the January 2013 PVI findings and, where applicable, include relevant information pertaining to Ornge RW's associated CAPs.
1.18.9.4.4.1 Critical Finding no. 1: FO-08-01—Crew Training Records
A number of required items were missing from crew training records. For example, a large number of pilots and medics did not have records of the following training:
- Servicing and ground handling
- Emergency procedures
- Surface contamination
- Aircraft icing
- Aeromedical resource management (AMRM)
- Line indoctrination flight training
- CFIT avoidance
- Persons assigned on-board duties (PAOBD)
According to TC, the expectation was that “[t]he Chief Pilot has established and maintained a ground and flight training program, as well as records for each person who is required to receive training.”Footnote 246
In its initial CAP, Ornge RW confirmed that its training records were not complete and accurate, citing “inadequate oversight, no documented internal processes […], and lack of qualified personnel”Footnote 247 as a root cause. That CAP also indicated that the OM/interim CP was task-saturated due to vacant positions, that he did not appropriately delegate the authority for management of the training records, and that no one was managing the flight crew training records.
In its revised CAP, the company reported that
- training files had been reformatted to make it easier to audit them for compliance, and that migration of training record information into AvAIO for automatic and real-time tracking of certification had begun (targeted completion date: 30 May 2013).
- a Manager of Flight Training and Standards, reporting to the OM/interim CP, would be hired to ensure that all flight crew members had correct/complete training (targeted completion date: 30 June 2013).
- a Flight Operations Quality Assurance Inspector had been appointed, and was responsible for auditing training files to ensure accuracy and compliance (targeted completion date: 30 June 2013).
1.18.9.4.4.2 Critical Finding no. 2: FO-07-01—Crew Training Program
The PVI found that several flight crew members had not fulfilled the requirements of Ornge RW's ground and flight training programs. In particular, multiple crew members had not received some or all of the following required training:
- Aircraft servicing ground handling
- Emergency procedures
- Aircraft surface contamination
- AMRM
- Line indoctrination
- CFIT avoidance.
In response to this finding, Ornge RW conducted an internal review and concluded that all 77 of the company's pilots had 1 or more required training items that either had not been completed or were not documented. In its CAP, Ornge RW stated that this finding revealed a “systemic failure”Footnote 248 within the company. During its internal review, the company determined that the training provider was not providing the flight portion of the company's CFIT-avoidance training, despite the fact that previous TC surveillance activities had identified its absence in May 2012 and again in December 2012.
Ornge RW cited similar root causes to the previous critical finding (FO-08-01), identifying that both the OM and the person responsible for tracking flight crew training (i.e., the Assistant CP) were task-saturated. This task-saturation had led, according to the CAP, to “failures in record keeping procedures coupled with insufficient oversight, tracking and auditing [which together had] resulted in the Company permitting crew's [sic] to act as flight crew members, without fulfilling the requirements of the company training program.”Footnote 249 It had also led to “missed operational triggers and training dates.”Footnote 250 Additionally, moving training binders to head office made it difficult for pilot trainers to ensure that base pilots were compliant with company policy and regulatory requirements.
As corrective action, Ornge RW's CAP for this finding echoed FO-08-01 regarding the reformatting of training files, migration of data into AvAIO, and appointment of a Flight Operations Quality Assurance Inspector.
1.18.9.4.4.3 Critical Finding no. 3: FO-07-02—Flight Crew Training Program
The PVI found that several pilots had not received differences training prior to flying the S-76A. This training was required by regulation because the flight simulator used to conduct the training was an S-76B, which is significantly different from the S-76A in terms of performance, systems, cockpit layout, and configuration.
In response, the company indicated that it had recently made a transition to a new training provider, and that a formal vendor change review had not been completed in accordance with regulatory, COM, and training manual requirements. As a root cause, the company identified a failure to implement an appropriate change management process to ensure that the new training provider was providing all of the required training. The company again highlighted that the OM was task-saturated, as was the Assistant CP, who was responsible for tracking flight crew training.
Corrective actions for this finding included preparing a training package and written examination to be completed by company pilots; regular meetings with the CP, OM, and training captains to address any training deficiencies; and the appointment of a Flight Operations Quality Assurance Inspector. As with the corrective actions addressing the other critical findings, this position would help address the excessive workload of the OM/interim CP and the Assistant CP. The targeted completion date was 30 August 2013.
1.18.9.4.4.4 Major Finding no. 1: FO-02-01—Air Operator Certificate and Operations Specifications
The PVI found that Ornge RW was not ensuring that the OM, who had also been filling the interim CP role since July 2012, had the necessary human resources to carry out his duties.
Ornge RW agreed, citing “the attrition of senior executives, Operations Managers, and Chief Pilots during the certification and transition phase and the company's inability to source qualified replacements […]”Footnote 251 as factors contributing to the task-saturation of the OM/interim CP. These factors, combined with the removal of the pilot manager positions without a formal delegation of responsibilities or resource analysis, affected the OM/interim CP's ability to effectively manage and administer operational programs.
Ornge RW's CAP highlighted that efforts were under way to hire a Manager of Flight Training and Standards, with a projected candidate to be selected by 30 June 2013. The company also planned to create an Aviation Records Administrative Clerk position and have it filled by 30 May 2013. Finally, the plan stated that an annual audit schedule led by the Flight Operations Quality Assurance (FOQA) Inspector was now in place, with a projected completion date of August 2013.
1.18.9.4.4.5 Major Finding no. 2: FO-10-01—Flight Documentation
The PVI found that some flights were conducted with incomplete or missing weight-and-balance calculations, and that the company did not have a system in place to ensure that these were being completed. According to Ornge RW, the root cause was a lack of management oversight, and inadequate instructions for completion of the weight-and-balance and load sheets. To address this finding, Ornge RW issued new operational flight plans and load sheets to all flight crews, accompanied by instructions for their proper use.
1.18.9.4.4.6 Moderate Finding no. 1: FO-09-01—Operational Control System
The PVI found that Ornge RW had not established a system to monitor the flight time, flight duty time, and rest periods of flight crew members.
The company again cited an inadequate change-management process, as well as repeated changes in key personnel, as causes.
In its CAP, Ornge RW stated that it would
- develop and implement a change-management process (targeted date: 30 May 2013);
- publish a flight operations directive outlining tracking procedures for flight and duty times; and
- have the newly appointed FOQA Inspector conduct a scheduled audit (targeted date: 30 June 2013).
1.18.9.4.4.7 Moderate Finding no. 2: AOC-02-01—Maintenance Control Manual
The PVI found that Ornge RW's Maintenance Control Manual was missing some elements related to record keeping and quality assurance program procedures, required as per regulation. In response to this finding, the manual was to be rewritten to address the identified deficiencies.
1.18.9.4.4.8 Moderate Finding no. 3: CS-01-01—Cabin Safety
The PVI found that Ornge RW was not ensuring that all PAOBDs were properly instructed about their duties. Ornge RW agreed, acknowledging that 79 medics had not received PAOBD training. The CAP proposed the following:
- issuance of a flight operations directive instructing flight crews to immediately treat all persons on board as passengers;
- migration of the training and tracking of qualifications of PAOBDs into AvAIO (targeted date: 30 June 2013); and
- performance of an audit by the FOQA Inspector (targeted date: 30 August 2013).
1.18.9.4.4.9 Moderate Finding no. 4: FO-03-01—Company Manuals
The PVI found that the COM did not include the instructions and information necessary to enable personnel to perform their duties as applicable to the operation. In particular, the COM did not reflect recent changes in the organizational structure; it provided no guidance regarding icing, weight-and-balance requirements, and helicopter performance limitations; and it lacked instruction on form completion.
As a root cause, Ornge RW cited a “lack of sufficient operational management and support personnel”Footnote 252 and mentioned the company's high turnover of key personnel throughout 2012. The CAP stated that, as a corrective measure, the CP position had been filled on 25 April 2013, removing the responsibilities of interim CP from the OM. Ornge RW also indicated that a full re-issue of the COM would be required due to the large number of issues that were found during the January 2013 PVI.
1.18.9.4.5 Process inspection (post-accident: June 2013)
Following the accident, from 12 to 21 June 2013, TC conducted a PI of Ornge RW. The purpose of the PI, which was conducted in accordance with SUR-001 Issue 04 and IPB 2012-02, was to verify that the company's flight crew training, qualifications, and flight duty assignments “met the regulatory requirements and were being followed”Footnote 253 according to the company's documented procedures. The PI consisted of an off-site review of documents and an on-site visit to observe personnel and verify that procedures were being followed.
The PI concluded that the company's flight crew training program did not meet the minimum regulatory requirements, making 9 findings related to non-conformances with the CARs. Those findings are summarized below.
1.18.9.4.5.1 Finding 07-01: Flight Crew Training Program
The PI foundFootnote 254 that several S-76A pilots at Ornge RW had not completed in-flight CFIT-avoidance training. This non-conformance had been documented previously, in May 2012 and again during the 2013 PVI. Although Ornge RW had indicated in its PVI CAP that this training issue had been resolved, an internal audit subsequent to the PI determined that approximately 50% of all S-76A flight crews had not completed the required practical CFIT-avoidance training.
As a root cause, the company cited a lack of management resources, together with insufficient oversight, tracking, and auditing, which had resulted in an ineffective CFIT tracking system and allowed the problem to go uncorrected. The proposed corrective action was identical to Finding 07-02, which is described in the next paragraph.
1.18.9.4.5.2 Finding 07-02: Flight Crew Training Program
Similarly to the previous finding related to practical CFIT-avoidance training for S-76A pilots, the PI found that some AW139 pilots were also missing this training. Here, too, Ornge RW's internal review determined that approximately 50% of all AW139 flight crews had not completed the training.
In its CAP, Ornge RW indicated that it would
- issue a flight operations directive prohibiting pilots without the required training from operating IFR;
- institute a program of on-aircraft CFIT-avoidance training as an interim measure (targeted completion date: 31 October 2013); and
- work with simulation providers to ensure CFIT escape-manoeuvre training was taught in both initial and recurrent flight training programs (beginning in June 2013).
1.18.9.4.5.3 Finding 07-03: Flight Crew Training Program
The PI found that some AW139 flight crews had not received some of the required technical training as per the TC-approved company Training Manual. Ornge RW cited “inadequate oversight, no documented internal processes and controls, and lack of assigned dedicated personnel”Footnote 255 as the root cause. The CAP proposed additional training and an online examination to verify understanding and competence. In addition, the company indicated that it had filled 2 positions with responsibility for monitoring training files, and planned an audit of AvAIO to ensure that all training requirements were tracked in accordance with the company's flight crew training manual.
1.18.9.4.5.4 Finding 05-01: Management Personnel and Operations Coordination
The PI found that reports produced from data in Ornge RW's AvAIO tracking system indicated that a large number of pilots, including the first officer involved in the occurrence, did not meet company and regulatory recency requirements for flights conducted wholly or partly at night when passengers are carried on board.
The company once again cited insufficient oversight, tracking and auditing as factors that had resulted in an ineffective night currency tracking program. On 13 June 2013, Ornge RW suspended IFR operations and instructed all pilots to provide confirmation that they had met night currency requirements as per the COM.
1.18.9.4.5.5 Finding 05-02: Management Personnel and Operations Coordination
The PI found that Ornge RW was unable to produce records documenting the progression of first officers from left-seat to right-seat flying duties, including that of the first officer involved in the occurrence.
The company confirmed that no formal process for documenting operational progression existed. In its CAP, it identified “a lack of sufficient operational management and support personnel lead[ing] to the Company's inability to fully and effectively manage all aspects of a First Officer's progression to right seat flying duties”Footnote 256 as the root cause, again citing insufficient oversight, tracking and auditing, which had resulted in an ineffective tracking program.
1.18.9.4.5.6 Finding 05-04: Management Personnel and Operations Coordination
The PI found that Ornge RW first officers had been assigned to PIC flight crew duties even though some pilots' files lacked the following records, as required by the COM:
- Letters of recommendation from a pilot manager, flight standards pilot, or company line captain;
- Records showing that a detailed review of the COM, SOPs, and ambulance procedures had been completed; and
- Properly completed line-check evaluation forms.
In its CAP, the company indicated that it possessed several of the required records but that these had not yet been added to the applicable files. According to Ornge RW, the company was relying on an inherited tracking program that was assumed to be acceptable. An updated process for documenting upgrade training was to be implemented, and personnel files would be audited by the FOQA Inspector.
1.18.9.4.5.7 Finding 05-05: Management Personnel and Operations Coordination
The PI found that several new pilots had been hired directly into PIC positions without first having completed direct-entry captain procedures as outlined in the COM. There was no documentation justifying the decision to bypass this requirement, which had been implemented to reduce the risks associated with employing contract pilots as captains. Instead, the company indicated, these pilots had been promoted directly into captain positions based on their experience and qualifications. The company indicated that it would amend the COM to include criteria defining a direct-entry captain, along with a process to train and evaluate direct-entry captains.
1.18.9.4.5.8 Finding 07-06A: Flight Crew Training Program
The PI found that Ornge RW pilots trained on the S-76B simulator had not received aircraft differences training prior to being assigned to operational duties on the S-76A. Gaps in aircraft differences training had been previously identified in the 2013 PVI (critical finding FO-07-02). In this instance, the company reviewed pilot files and determined that this was a documentation issue for 2 pilots. Ornge RW again identified insufficient oversight, tracking, and auditing as reasons behind this issue and, as corrective action, appointed a FOQA Inspector and a Flight Operations Compliance and Logistics Specialist.
1.18.9.4.5.9 Finding 07-06B: Flight Crew Training Program
The PI found examples of steep turns that were not being conducted during PPCs of S-76 flight crews. In its CAP, Ornge RW argued that the approved check pilot (ACP), acting as a delegate of the Minister, is responsible for the conduct of the PPC, and that it is therefore TC's responsibility to ensure that ACPs complete all of the necessary sequences required for a PPC. However, the company indicated that it would take steps to ensure that all company ACPs were aware of the steep-turn requirement for future PPCs. The company also said it had instituted a process to ensure that all future PPC forms were checked for accuracy, and to conduct random audits on PPC documentation.
1.18.9.4.6 Transport Canada's internal discussions following the post-occurrence process inspection
On 18 June 2013, the PI team advised senior TC regional management that it had no confidence that Ornge RW had a system in place to ensure that all training requirements were met.Footnote 257 Two days later, the PI team advised the ADO(W) and the RDCA that Ornge RW's operational control over flight crew training was ineffective, citing a number of examples to support this conclusion.Footnote 258
On 25 June 2013, the Director of Policy and Regulatory Services at TC contacted the Director of Standards at TC and the Chief of Enforcement at TC, requesting that they provide support to the region, “with a view of reviewing options for administrative and punitive sanctions.”Footnote 259 According to TC's Aviation Enforcement Policy Manual (TP 13794), administrative action is “[d]eterrent action taken by or on behalf of the Minister, including oral counselling, suspension or cancellation of documents of entitlement, and imposition of a monetary penalty.”Footnote 260
On 26 June 2013, a draft NoS, along with supporting documentation, was submitted by the PI team to the ADO(W) and the RDCA. Based on paragraph 7.1(1)(b) of the Aeronautics Act, it stated that Ornge RW “has ceased to meet the qualifications necessary for the issuance of an air operator certificate and to fulfill the conditions subject to which its air operator certificate was issued.”Footnote 261 Specifically, the draft NoS stated that the company had failed to meet the requirements of CARs 704.07(2)(e) and 703.07(2)(d), which require that an applicant shall have “flight crew members who are qualified for the area of operation and the type of operation”.Footnote 262
The draft NoS was submitted to TC HQ for review and comments. The Enforcement division provided the following feedback to the region:
- Ornge RW's S-76 pilots all received training that met regulatory standards; however, some training elements, which go beyond regulatory requirements, were not completed in accordance with the company's COM.
- Ornge RW's AW139 pilots had all received some training, although some elements of the training program were not completed as required by regulations.
- Some of the outstanding CAP items from the January 2013 PVI had not yet been implemented. However, the due date on these CAPs was 30 June 2013.
- Some of the procedures in the COM were not being adhered to.Footnote 263
The Enforcement division advised that an NoS under the certification section [paragraph 7.1(1)(b)] of the Aeronautics Act was not appropriate, since the company still met the conditions for initial certification found in paragraphs 704.07(2)(e) and 703.07(2)(d) of the CARs.
In considering an alternative course of action, TC HQ staff suggested that there would be a higher likelihood of success if the NoS were pursued on the grounds of public interest [paragraph 7.1(1)(c) of the Aeronautics Act]. The TC regional office was advised that establishing such grounds requires demonstration of “a continuous or repetitive state of non-compliance by the operator; both prior and following the accident. The Minister must also demonstrate that this state of non-compliance still exists today.”Footnote 264 The regional office was advised that if it decided to proceed, then the NoS should be issued after 30 June 2013, since that was the deadline in the company's CAPs. The regional office was then told that Enforcement staff would remain available to help if the region decided to continue with plans to issue an NoS.
TC regional staff considered the advice received and decided not to pursue an NoS on public interest grounds.
1.18.9.4.7 Enforcement action following the process inspection (June 2013)
Following the June 2013 PI, TC initiated enforcement action by issuing 8 detection notices related to the PI findings. The notices are summarized below, along with the outcomes of TC's enforcement process:
- Failure to meet night currencies: No further action; no violation. According to TC, the pilot cited in the detection notice was scheduled but did not fly the aircraft; therefore, no violation had occurred. However, TC did not issue a detection notice regarding the occurrence first officer who, according to the AvAIO records, did not meet night currency requirements.
- Direct-entry captain requirements: No further action; investigation abandoned. According to TC, the investigation was abandoned because it was similar to count 5, listed below.
- Failure to complete steep turns during PPCs: No further action; statute limited. According to TC, this violation was detected almost a year after the date on which it occurred, and it was felt that there was insufficient time remaining within the statutory period to investigate it.
- Aircraft differences training: There was a finding; however, TC elected to abandon the investigation because it was similar to count number 5, listed below, “where a monetary penalty was going to be issued”.Footnote 265
- Incomplete CFIT-avoidance training on S-76A: It was determined that Ornge RW committed offences of non-compliance with CARs 703.88(1) and 704.108(1). A monetary penalty was assessed and paid by Ornge RW.
- Incomplete CFIT-avoidance training on AW139: There was a finding; however, TC elected to take no further action and the investigation was abandoned since it was similar to count 5, listed above, for which a monetary penalty was to be issued.
- Some AW139 flight crew missing recurrent technical training: It was determined that Ornge RW committed an offence under CAR 704.108(1), and a monetary penalty was assessed and paid by Ornge RW.
- Upgrade training requirements: The regulation cited was changed to CAR 704.108(1); however, the result was no further action, and the investigation was abandoned because, according to TC, after interviews there was “no evidence to pursue further”.Footnote 266
1.18.9.5 Program validation inspection (October 2014)
1.18.9.5.1 General
On 14 and 15 October 2014, TC conducted a planned PVI of Ornge RW “to verify that the organization was in compliance and has the systems in place to ensure on-going compliance with regulatory requirements.”Footnote 267 The operator was notified that the scope of the surveillance would include a review of the company quality assurance program and company operational control, with emphasis on the training programs.
The report documenting the results of the PVI indicated that “all areas of enterprise operation were in compliance with the regulatory requirements and the PVI is considered closed.”Footnote 268 No findings were issued.
Of note, the methodology of the 2014 PVI was significantly different from previous surveillance in that it used a much narrower scope. This methodology is described in detail in the following section.
1.18.9.5.2 Routine versus focused sampling
The sampling plan for the October 2014 PVI consisted of the following areas: operational flight plans, interviews with key personnel and available flight crew, internal quality audits, corrective actions, auditor training records, and pilot training.
The scope of this sampling plan differed from that used in both the PVI and PI conducted in 2013. For example, the previous surveillance had identified that company pilots had not completed a number of training-related elements, including CFIT-avoidance training, black‑hole training, and differences training. Those elements are listed in the TC-approved flight crew training manual, but they are not required by regulation, and are therefore not offense-creating.
By contrast, the scope of the pilot training file review during the 2014 PVI was limited to a small number of regulatory requirements that were offence-creating provisions:
- Medical certification validity
- PPC validity
- Completion of minimum required times for flight training
- Completion of line indoctrination (AW139 only)
- Completion of aerodrome and area of operation qualification training
- Completion of emergency procedures training
- Night currency
In total, training files were reviewed for 13 of 87 pilots (both S-76A and AW139).
As all of the required items from this list were found to be properly documented, no additional files were checked. The result was that the PVI did not evaluate compliance with any company requirements that went beyond these regulatory requirements, and issues identified during previous TC surveillance were not re-examined to verify that the problems had not reoccurred.
The decision to limit the scope of the surveillance in this way (i.e., to only offense-creating provisions) was based on an interpretation of focused sampling, a methodology introduced in SUR-001 Issue 05. That document, which was published on 28 June 2013, shortly after the previous surveillance, states that a surveillance manager will develop a sampling plan based on worksheets provided for this purpose. The worksheets provide a high-level, systems-based list of expectations, which describe what an enterprise is expected to do. For example, the Control of Operations worksheet for CARs Subpart 703 and 704 operators reads, “Chief Pilot has established and maintained a ground and flight training program, as well as records for each person who is required to receive training.”Footnote 269 The surveillance manager is required to link each expectation to all applicable regulatory requirements.
The SUR also specifies:
Whenever possible, an offence creating provision (as identified in CAR 103 Schedule II) should be the primary link such that, should the surveillance activity result in a need for enforcement action, it will be readily available. Following the linkage of expectations to designated offence creating provisions, linkages should be made to any other regulatory requirements which apply to the expectations.Footnote 270
Based on this mapping, the surveillance manager is required to identify what is to be sampled to validate each expectation. The SUR outlines 2 sampling methods that can be selected based on research outputs and the history of the company. These are:
- focused sampling, which is carried out in one or several areas of a surveillance activity where an enterprise has historically been weak; and
- routine sampling, which is carried out in areas where the enterprise has not had any weakness.
However, given the PVI team's lack of experience using this approach, the extent and severity of the findings that had been generated previously against Ornge RW, and the fact that this was the first PVI of the company conducted since the accident in May 2013, some PVI team members expressed concerns about the appropriateness of using focused sampling. None of them had received any training on the changes associated with SUR-001 Issue 05. Internal correspondence among the October 2014 PVI team members showed a considerable amount of confusion as to the most appropriate sampling method to employ and the way in which focused sampling was to be carried out.
1.18.10 Helicopter emergency medical services in the United States
In the past 10 years, the NTSB has conducted studies, made numerous observations, and issued recommendations intended to enhance the safety of helicopter emergency services in the United States. On 21 February 2014, several new regulations, intended to enhance the safety of helicopter EMS operations, came into effect in the United States. In particular, the major changes associated with the FAA revisions are summarized as follows:
- Helicopter air ambulance flights with medical personnel on board shall be conducted under Part 135, which is equivalent to CARs Subpart 704in Canada.
- Helicopter air ambulance operations that consist of 10 or more helicopter air ambulances must establish an Operations Control Centre (OCC).
- Helicopters operated for the purpose of air ambulance must be equipped with a helicopter TAWS.
- Helicopter air ambulances must be equipped with a flight data monitoring (FDM) system.
- Helicopter air ambulance operators must establish and document an FAA-approved pre-flight risk analysis process.
Despite these recent changes to the FARs, a number of NTSB Recommendations related to air ambulance safety have not yet been acted on by the FAA. As a result, these recommendations have either been classified as “Open” or “Closed—Unacceptable Action”. (The NTSB's recommendations, along with the FAA's responses to those recommendations, are provided in Appendix I.)
From a regulatory standpoint, TC has a number of policies and procedures in place to harmonize Canada's regulations with those of other regulatory bodies, including the FAA. In February 2011, for example, Canada and the United States launched the Regulatory Cooperation Council (RCC) as a means of facilitating closer cooperation between the 2 countries, and “to develop smarter and more effective approaches to regulation”Footnote 271 by harmonizing regulations where applicable. According to the RCC's August 2014 Joint Forward Plan, the FAA and TC “will continue to collaborate in the area of aviation safety. They will establish procedures to identify safety initiatives of common interest, exchange regulatory priorities, and develop opportunities for joint regulatory work.”Footnote 272 As well, the report advised that TC and the FAA would attempt “to align as much as possible their respective rulemaking programs.”Footnote 273 According to TC, the Department strives to “harmonize regulations where possible with other regulatory bodies.”Footnote 274 However, at time of report writing, none of the recent changes to the FARs have been incorporated into the CARs.
1.18.11 Previous occurrence
On 08 February 2008, an S-76A helicopter under contract to Ornge crashed at Temagami, Ontario,Footnote 275 while conducting a black-hole approach to landing. The helicopter crashed in a forested area at the edge of a frozen lake, coming to rest on its left side. Three of the 4 occupants sustained serious injuries. The fourth occupant sustained minor injuries. The captain had over 2200 flight hours on the S-76A, while the first officer had 147 flight hours on the S-76A. During the last 1.5 minutes of the approach, the PF was explaining to the PNF what he was doing, step by step, and what to watch for during night approaches, including black-hole illusions.
The helicopter was equipped with an EGPWS, a dual Garmin GNS 530 GPS/Navigation/Communication unit, a Latitude Technologies SkyNode satellite tracking system, and a CVR.
The investigation report on that accident underlined the importance of diligently monitoring the helicopter's flight instruments during critical phases of flight. It also stated that the PF's attention had been split between flying the approach and explaining why things were happening and what to watch for during a black-hole approach. This teaching likely distracted the pilots, who did not perceive the excessive rate of descent leading up to the crash.
1.19 Useful or effective investigation techniques
The crash site of the Ornge RW helicopter was located in dense bush and swampy terrain. Access to the site was made possible by assistance from local volunteer firefighters and the OPP, who made a path through the woods using all-terrain vehicles. This local assistance was critical in allowing timely examination of the wreckage and preservation of perishable evidence.
In addition to providing land-based resources to the investigation team, the OPP made one of its Eurocopter EC135 helicopters and a pilot available to the investigation team. After the first night, members of the OPP cleared a landing zone for the helicopter near the crash site. This clearing permitted rapid transit to and from the crash scene. It also enabled the investigation team to easily remove several aircraft components that were sent for further examination at the TSB laboratory in Ottawa.
2.0 Analysis
There was no indication that an aircraft system malfunction contributed to this controlled flight into terrain (CFIT) accident. This analysis focuses on the operational and organizational factors that contributed to the accident, on Transport Canada Civil Aviation's (TCCA) regulatory oversight program, and on the current regulatory environment.
2.1 Inadvertent descent and impact with terrain
Canadian Aviation Regulations (CARs) 602.114 and 602.115 stipulate that all night visual flight rules (VFR) flights, whether conducted in controlled or uncontrolled airspace, be operated with visual reference to the surface. Night flying, even in visual meteorological conditions (VMC), requires crews to maintain an instrument scan and be ready and able to change over to flying by reference to flight instruments when visual cues outside the aircraft are insufficient to maintain control.
Due to lack of cultural lighting in the area, very few visual cues are available off the departure end of Runway 06 at Moosonee Airport (CYMO) at night. Exacerbating this situation on the night of the occurrence was an overcast ceiling, which would have limited the ambient lighting available to provide a visible horizon or other visual cues necessary to maintain orientation. Hence, the crew conducted a flight under night VFR regulations without sufficient ambient or cultural lighting to maintain visual reference to the surface. As a result, the occurrence pilots would have required complete reference to flight instruments to maintain control after passing the end of the lit departure runway.
The initial stages of the departure were conducted as per standard operating procedures (SOPs). While turning left on course at 300 feet above ground level (agl), the pilot flying (PF) inadvertently allowed the bank angle to reach 30°, and the aircraft descended during the turn. These deviations were not acted upon until they were identified by the pilot monitoring (PM). As a result, 23 seconds after commencing the turn, the aircraft struck the trees.
The attention of the PF could have been focused on a number of possible areas at that time. The visual cues that the PF was using to manage the turn during the climb disappeared as the aircraft passed the end of the lit departure runway. If the PF did not recognize the need to switch to instrument flight, his attention would have been devoted to searching the outside visual field for references. Alternatively, if the PF did recognize the lack of adequate external cues, his attention could have been devoted to making the transition to flight by reference to instruments, which could take several seconds if he were unprepared to make this switch. It is also possible that the PF's attention was diverted by completing the after-takeoff checklist. The investigation could not determine which of these scenarios was most likely.
In this occurrence, the PM became focused on completing minor checklist procedures (i.e., post-takeoff check) and turning the landing light off at a time when the priority was to monitor the conduct of the flight. When the PF encountered a lack of visual cues off the departure end of Runway 06, necessitating transition to flight by reference to instruments, an excessive bank angle and rate of descent developed, which were not recognized by the crew at an altitude that permitted recovery.
To appreciate the systemic issues that allowed this situation to develop, a broad range of factors must be understood.
2.2 Impact sequence
Based on the available information, investigators determined that the combination of high forward velocity, shallow angle of descent, and loss of a tail-rotor blade during the impact sequence caused the helicopter to bounce and skip across the ground, and to rotate to the right until it likely began to cartwheel in the original direction of travel. As a result, the damage path gradually narrowed from approximately the diameter of the main rotor to half of its diameter as the blades broke free and the tailboom detached just left of the direction of travel.
The severity of the impact forces caused the deaths of the first officer and one of the flight paramedics, and likely rendered the captain and the other flight paramedic unconscious. The latter 2 individuals likely succumbed rapidly to their injuries before significant inhalation of fire combustion products.
2.3 Operational readiness of the crew
It is the responsibility of a company to ensure that its flight crews are operationally ready to deal with both normal and abnormal situations that can be anticipated in their roles. Although the crew of the occurrence flight were both experienced pilots, both had minimal night flying and instrument flying experience. Therefore, effective training and supervision were critical to adequately prepare the pilots for multi-crew, instrument flight rules (IFR), and night operations.
Between 2011 and 2013, the captain, who was the PM on the occurrence flight, had logged very few night flight and instrument flight hours. He had most likely not conducted any in-aircraft night flight operations between 2011 and the accident date without using night-vision goggles (NVG). However, the night takeoffs and landings he had conducted during his most recent simulator training satisfied both regulatory and company currency requirements for night flight with passengers. Both the captain and the company approved check pilot (ACP) had noted that the captain's IFR and multi-crew procedures were weak during the captain's S-76 recurrent training, and had agreed that a period of working as a first officer would be appropriate. To this end, the ACP filled in the “First Officer” dot in the Crew Status section of the Flight Test Report Pilot Proficiency Check (PPC) (form 26-0249/0279). The ACP's concerns, and the fact that “First Officer” had been indicated on the flight test report, were communicated to the Operations Manager (OM)/interim Chief Pilot (CP) and to the Assistant CP. However, no action was taken by the company, and the captain went directly into a role for which he was unprepared.
Additionally, the captain had received little preparation from the company to assume operational duties. Given that line indoctrination training for CARs Subpart 703 operations is not required and that the company decided to bypass its direct-entry captain procedure, the captain received no additional in-flight training or supervision between undergoing his PPC and undertaking flight duties as a captain. Further, at no time did the company address the fact that the captain had not received black-hole training, although that fact had been identified during his area-of-operations briefing and communicated to the company. As set out in the Company Operations Manual (COM), had the company elected to follow its direct-entry captain process, the captain would have flown a minimum of 50 hours as second in command, including 5 hours of night operations and 3 black-hole approaches, prior to being assessed by an ACP to determine whether he was ready to assume pilot-in-command (PIC) duties. In fact, the occurrence flight was the captain's first unaided night flight since completing recurrent training in the simulator, which likely accounts for the difficulties that the captain experienced locating lighting controls in the cockpit.
The first officer, who was the PF on the occurrence flight, had experienced difficulty adapting to multi-crew IFR operations during initial S-76 training, likely due to his limited IFR experience. However, after some additional training, he had successfully completed the PPC, with 3 major deviations observed by the ACP. One of those documented weaknesses was specifically related to problems controlling airspeed and rate of climb during an IFR departure. The occurrence flight, although a night VFR flight, required complete reference to instruments and would have placed similar demands on the first officer. Yet, beyond the first officer's initial conversion course, the company implemented no additional measures to ensure that he received the training necessary to overcome these documented weaknesses. Instead, for the first 6 months of his employment at Ornge RW, and again in April and part of May 2013, the first officer was allowed to switch his night shifts for day shifts, until overtime became an issue. At that point, he began to hold night shifts on a more regular basis, while continuing to switch some night shifts for day shifts. During one of those night shifts, the first officer experienced difficulties acting as the PF during a night VFR departure (heading 1.5.3.6) that required the captain to intervene to ensure adequate safety margins were maintained. However, the problems encountered by the first officer were not documented, and no remedial action was taken to ensure that he possessed a suitable level of proficiency for night VFR operations out of CYMO.
At the time of the accident, the first officer had logged 33 hours of instrument flying experience, but had gained no actual IFR experience during his employment with Ornge RW. In addition, the first officer did not have continuity in terms of regularly scheduled night flights to build proficiency in night operations, for which he had limited experience and had previously encountered difficulties. Although the first officer met the minimum regulatory night currency requirements to carry passengers, his most recent night flight had been carried out 85 days before the accident flight. Furthermore, Ornge RW was unable to produce documentation following the accident to demonstrate that the first officer had completed the company-required training to conduct PF duties from the right seat.
At the time of the occurrence flight, both crew members possessed minimal IFR and night proficiency. As a result, the crew were not operationally ready to safely conduct a night VFR departure that brought the flight into an area of total darkness.
At the time of the accident, the captain was employed as the CP of the Ontario Ministry of Natural Resources (MNR). Despite having been explicitly instructed at least twice by MNR management not to do both jobs at the same time and to comply with rest and duty time regulations, the captain engaged in MNR-related teleconferences while in Moosonee and was involved in extensive email correspondence during and outside of his scheduled shift times at CYMO. Likewise, Ornge RW company indoctrination training emphasized the importance of ensuring that flight crew obtain the required rest before reporting for flight duty.
Nevertheless, the captain performed extensive MNR duties during the morning and early afternoon on the day of the occurrence, to the extent that senior personnel at the MNR were unaware that he was in Moosonee at the time. The captain's MNR-related activities while stationed in Moosonee constituted work-related tasks that would normally initiate a flight crew member's flight duty time. As stated previously, it is highly likely that the captain napped during the afternoon before the commencement of the occurrence night shift. Although there is no indication that the captain's performance was degraded as a result of fatigue during the short occurrence flight, if pilots engage in other work-related activities before the commencement of scheduled flight duty time, there is a risk that regulatory flight duty time limitations will be exceeded, which may degrade performance due to fatigue.
2.4 Training
Training is critical to ensure that company pilots are operationally prepared for the normal and abnormal situations they may face. To be effective, training must be designed to meet the operational needs of the company, be effectively delivered, and be followed up with recurrent training to encourage ongoing skills retention and development. In the case of Ornge RW, weaknesses in all of these areas reduced the effectiveness of the company's training, and contributed to the crew's unpreparedness during the occurrence flight to handle the conditions they encountered on departure from CYMO.
Although Ornge RW had developed a TC-approved training manual that met (and in some aspects exceeded) regulatory requirements, the training as designed included weaknesses that reduced its capacity to meet the operational needs of Ornge RW crews. For example:
- The company's CFIT-avoidance training program was not specific to each aircraft type. Rather, it provided generic guidance that was, at times, not applicable to the S-76A fleet.
- Very little dedicated night VFR training was included in the S-76 simulator training, and little guidance was provided to instructors on how the required night VFR sequences that were included should be presented. As a result, there was little realistic training in night VFR operations.
- Crew resource management (CRM) training provided by the company was mostly awareness-based and provided few practical strategies that could be employed by pilots. Moreover, 2 different courses were being taught to company pilots.
Weaknesses in the training syllabus were exacerbated by ineffective or inconsistent delivery of many aspects of the training. A number of instances were identified in which pilots (including the pilots involved in the accident) were provided with little time and no company publications to prepare for initial or recurrent simulator training. Once on site, pilots still lacked access to company publications and, in many cases, the training—including black-hole training—was not conducted in accordance with Ornge RW's SOPs and the Training Manual.
As pointed out by company pilots and TC on multiple occasions, some of the training required by the company training manual was not included in the simulator training provided by the contractors. Among the training components that were consistently not delivered were practical CFIT-avoidance training and black-hole training, which were largely included at the discretion of the instructor or conducted on the initiative of the pilots undergoing the training. In the case of the crew of the occurrence flight, the captain had received no black-hole training during his recurrent S-76 course because he had declined the training on the basis that it was not realistic. There is no record on Ornge RW training record forms indicating that he received practical CFIT-avoidance training.
Following completion of company training, there was little or no follow-up to ensure ongoing skills development and retention. The pilots involved in the occurrence flight had received no additional flight training or checking following completion of their simulator training, as line indoctrination training was not required, and area familiarization training consisted of a verbal briefing delivered by another company line captain. Under current regulations, there is no requirement for multi-crew CARs Subpart 703 pilots to undergo any type of line indoctrination. As a result, there is a risk that pilots will not be fully prepared to safely conduct operations in their designated positions on all company routes.
Furthermore, the company had no process in place to follow up on problems identified during company training, nor was such a process required by regulation. Therefore, the deficiencies identified with regard to both pilots involved in the accident went unaddressed. Despite having been flagged by the company ACP as requiring additional experience as a first officer before assuming PIC responsibilities, the captain was assigned PIC shifts immediately. The fact that the captain had not received the required black-hole training was never addressed by the company, despite having been identified during his area operations briefing. Insufficient and inadequate training contributed to the difficulties that the crew encountered during the departure from Runway 06 at CYMO.
Some pilots at Ornge RW had acquired copies of company exams and were distributing those exams to newly hired pilots. If companies do not take adequate steps to protect the integrity of mandatory exams administered to their pilots, there is a risk that the tests will not be effective in validating that pilots possess the prerequisite knowledge needed to safely carry out their duties as flight crew.
2.5 Standard operating procedures
Effective SOPs are a framework for consistent and safe operations. They establish expectations and norms with respect to specific operations, and set parameters that enable detection of deviations from standard flight profiles. As detailed in this report, Ornge RW's SOPs were inadequate in a number of areas and lacked guidance intended to enhance safety. This is not the first time that inadequate SOPs have been identified in a TSB aviation investigation report.
The Ornge RW S-76A SOPs in effect at the time of the occurrence were a carryover from the previous provider of helicopter emergency medical services (HEMS). The SOPs did not contain a dedicated night-flight section. Consequently, the crew carried out a briefing for and followed the profile of a standard VFR departure, which allowed an on-course turn at 300 feet agl and did not specify any differences in the procedure when carried out at night.
Although the SOPs had a specific procedure for black-hole departures, CYMO was not a company-designated black-hole location, so use of that procedure was not required and may not have been considered by the crew. The section on black-hole departures directed pilots to climb to at least 500 feet agl before turning, and most of the more experienced company pilots had adopted this procedure for all night departures. The practice of delaying the turn until 500 feet agl provides an additional margin to stabilize the departure, ensure obstacle clearance, and reduce the risk of CFIT.
In this occurrence, the first bank-angle call was at 30°, and the PF acknowledged that this angle was excessive. To reduce the risk of spatial disorientation, many of the company's experienced pilots would not permit turns in excess of rate 1 at night.Footnote 276 However, no section in the Ornge RW S-76A SOPs specifies normal or maximum bank angles while in a turn. As a result, flight crews have no predetermined limits to help them recognize deviations from set flight parameters.
On the occurrence flight, the PF was the only one to indicate the radio altimeter setting during the pre-flight sequence. Procedures with respect to use of the radio altimeter are included only in the IFR sections of the Ornge RW S-76A SOPs. The investigation determined that there were a number of informal procedures employed by pilots at Ornge RW with respect to the use of the radio altimeter low-height bug setting. Informal procedures can lead to confusion and lack of coordination if pilots who are paired use different procedures for the radio altimeter, reducing its effectiveness as a mitigation for CFIT.
In multi-crew operations, SOPs assist in communication, coordination of flight crew duties, and threat-and-error management. The practice of cross-checking instrument settings ensures that crews are relying on the same information, and that the information is accurate. Readbacks of checklist items, instructions, and clearances are used to detect and trap errors in the performance of both the PF's and PM's duties. The Ornge RW SOPs contained very little direction to pilots with respect to cross-checking procedures, and did not include any readback requirements other than in the Enroute section. The investigation found few indications that cross-checks and readbacks were performed on the occurrence flight.
Embedding practical CRM strategies in SOPs improves crew coordination, crew communication, and the ability of crews to manage errors effectively. Effective CRM dictates that the roles of the PF and PM must be clearly defined, especially during critical phases of flight, when margins of error are reduced. In this occurrence, the PM's attention was focused on completing the post-takeoff checks and attempting to locate the landing light switch during a critical phase of flight. As a result, the increasing bank angle and rate of descent were not detected in time to recover. The Ornge RW S-76A SOPs contained very little guidance on the specific crew roles and responsibilities of the PM and PF.
The best practices identified in this section were not used by all Ornge RW pilots, and had not been formally identified as such or incorporated into the S-76A SOPs. Similarly, the deficiencies in the company's SOPs were not identified or addressed with updates, in part because none of these best practices or deficiencies were reported through the company's safety reporting system. Given that the aircraft type involved in the occurrence was being phased out, it is likely that SOPs for the S-76A were also not a high priority. Additionally, the CP at the time of the occurrence, whose role involved responsibility for the development and maintenance of SOPs, lacked familiarity with those of the S-76A, and was inexperienced in the emergency medical services (EMS) role. The high workloads of the OM and the CP, together with the resource issues that existed during the period leading up to the accident, are analyzed under heading 2.7.2.
Ornge RW did not have dedicated night-flight SOPs to address the hazards specific to night operations, except for designated black-hole locations, which did not apply to Moosonee. As a result, the inadequacy of the company's night-flight SOPs contributed to the accident.
Robust SOPs, founded on effective CRM principles, industry best practices, and operational experience, enhance operational safety. In CARs Subpart 705 operations, SOPs must be reviewed by TC, which gives the regulator insight into how a company is operating and how it compares to others in the sector. The review process also allows for input from the regulator when SOPs are inadequate or do not represent best practices. There may be benefit for TC to review SOPs of multi-crew CARs Subpart 702, 703, and 704 operators during routine surveillance activities, particularly for new operators.
As identified in previous TSB aviation investigation reports, there is currently no regulatory process for multi-crew CARs Subpart 702, 703, and 704 operators to have company SOPs reviewed by TC. As a result, there is a risk that non-optimal procedures will be adopted.
2.6 Pilot proficiency checks
Under current regulations, all helicopter CARs Subpart 702, 703, and 704 captains and first officers are subject to the same PPC standard, as per the applicable subpart of the operation. All helicopter pilots, regardless of whether the intent is for them to act as captain or as first officer, must pass the appropriate PPC for that subpart at the captain level.
The consequence of this lack of differentiation is that there is no such thing as a “first officer PPC” or a “captain PPC”. Any pilot who passes a PPC on a helicopter has met the minimum requirement to act as PIC on that aircraft type. There is no mechanism in place, short of failing a pilot, for an ACP to restrict a pilot from carrying out PIC duties in helicopters.
A pilot may receive as many as 4 assessments of 2 (i.e., major deviations that are recognized and corrected in a timely manner) on the PPC and still pass, and be permitted to act as captain on that aircraft type. This standard may not allow for the determination of whether a pilot is adequately prepared to act as PIC on a multi-crew aircraft, given the complexity of some multi-crew helicopter operations. If a pilot experiences a single major deviation during a PPC and corrects it in a timely manner, the deviation may be a simple slip that anyone could make. However, multiple such deviations in a brief flight may indicate a lack of proficiency for a candidate for PIC.
The risks associated with allowing an individual who experiences multiple major deviations to act as PIC could have significant consequences for the saftey of flight. Therefore, it would be appropriate to hold first officers and captains of multi-crew helicopters to different standards, commensurate with their responsibilities. Although the occurrence captain had passed his PPC in March 2013, both the ACP and the TC principal operations inspector (POI) had expressed serious concerns about immediate employment of the captain as a PIC. However, the ACP had little recourse to restrict the captain's designation, since the captain had not failed the PPC. Therefore, the ACP advised the company OM and CP that the occurrence captain should be employed only as a first officer until he was able to gain some additional experience. Despite this, the occurrence captain was not restricted from PIC duties in any way.
Under current regulations, CARs Subpart 702, 703, and 704 helicopter first officers and captains are held to the same PPC standard. As a result, there is an increased risk that a pilot assigned to captain duties will lack the required proficiency and CRM skills to safely carry out those responsibilities.
2.7 Company organizational and management factors
To ensure that pilots are well prepared to conduct flight operations, a company must have safety processes in place, such as effective training, SOPs, supervision of pilots, and crew pairing. At the time of the accident, there were a number of safety deficiencies in these areas at Ornge RW. Some of these deficiencies were known to management but had not yet been fully addressed. Training and SOPs have been discussed under headings 2.4 and 2.5 respectively.
2.7.1 Crew scheduling and pairing
Air taxi helicopter operations encounter a wide range of operational, technical, environmental, and geographical conditions. There is a heavy reliance on crew expertise to manage the variable and unpredictable nature of such operations, which is why crew scheduling and optimal pairing is essential.
Between summer and fall of 2012, Ornge RW eliminated the pilot manager positions at its rotor-wing bases. There were indications that this was done to change the management structure from that of the previous operator and to further the transition of the company to Ornge RW. A key function of the pilot managers had been the scheduling and pairing of pilots. With knowledge of their local operating areas and crews, the pilot managers would consider pilots' skills and experience, balancing their individual strengths and weaknesses when generating crew pairings. While the pilot manager positions were not required by regulation, their removal increased the potential for sub-optimally paired crews being scheduled for flight.
In July 2012, following the elimination of the pilot manager positions, Ornge RW implemented a centralized scheduling system that was already in use by Ornge FW. Pilot availability and the “green on green” policy outlined in Flight Operations Directive (FOD) 034 were the only criteria applied by central scheduling to schedule and pair pilots. The 2 pilots of the occurrence flight had similar weaknesses in terms of IFR and night flight experience, creating a poor multi-crew pairing. Due to differences in the nature of the operations and in the types of expertise required, a centralized scheduling system that uses only pilot availability as a criterion is likely not sensitive enough to take into account the experience, strengths, and weaknesses of helicopter pilots as necessary for aerial work and air taxi operations. If the experience and proficiency of pilots are not factored into crew scheduling, there is a risk of sub-optimal crew pairings, resulting in a reduction of safety margins.
Although the central scheduling department was responsible for tracking and checking pilot qualifications and currencies, it was not doing so at the time of the accident. Before the transition to a centralized scheduling system, flight followers were responsible for checking pilot qualifications and currencies as per the Flight Following Manual. The responsibility for checking and tracking qualifications and currencies was transferred to central scheduling, but the relevant processes were not adopted. Ornge RW was not using the company's currency tracking program (i.e., AvAIO) as intended to ensure that pilots were qualified in accordance with both company and regulatory night-flight currency requirements. As a result, the central scheduling department did not identify that, according to inaccurate data in AvAIO, the first officer was not qualified for the flight.
2.7.2 Erosion of company policies and procedures
The occurrence pilots were not operationally prepared for the conditions they encountered on departure from CYMO. Although Ornge RW had established a series of policies and procedures defining the operational readiness of its pilots that exceeded minimum regulatory requirements, these were bypassed and eroded as challenges arose.
The following examples demonstrate that, when faced with pilot shortages or staffing pressures, Ornge RW altered or did not utilize defences that had been put in place to ensure the operational readiness of its pilots:
- The direct-entry captain procedure (COM, section 2.4) was not applied to 9 individuals (including the occurrence captain) who were newly hired into captain roles, because the company assessed the experience and qualifications of these individuals as appropriate. The rationale behind these decisions was not systematic or documented in accordance with basic risk-assessment principles.
- No action was taken in response to the ACP's concerns regarding the captain's readiness to assume PIC duties, and the company immediately employed the captain in a PIC capacity.
- First officer progression and authorization to fly from the right seat was neither tracked nor monitored, and no documentation was available for the right-seat qualification of the first officer who was involved in the occurrence.
- The first officer was permitted to trade night shifts for day shifts for an extended period. This imbalance reduced the number of opportunities for the first officer to gain IFR and night flight experience.
- The company was not accurately tracking and monitoring the qualifications, currency, and experience of its pilots to ensure optimal crew pairing.
- The company was not providing black-hole training to all pilots, and no action was taken when the captain's lack of black-hole training was identified.
- Practical CFIT-avoidance training was not consistently delivered during simulator training, and thus the captain never received the training.
- In February 2013, Ornge RW revised FOD 034 (Green on Green) to eliminate the requirement for a pilot to have operated from a specific base during the previous 3 months to be considered non-green; instead, any previous operational experience at that specific base was considered satisfactory.
Although Ornge RW had established policies and procedures defining the operational readiness of its pilots, these were bypassed and eroded by the company, which resulted in the crew not being operationally prepared for the conditions encountered on the night of the occurrence.
Underlying the erosion of company policies and procedures intended to ensure operational readiness was an under-resourced Flight Operations department at Ornge RW. This department experienced significant turnover in its first year following certification in 2012. Although the staffing of key positions stabilized in the fall of 2012, the individuals who filled the combined OM/interim CP role and the role of Assistant CP were new to management and EMS operations, respectively.
In addition to being inexperienced in their new roles, the OM/interim CP and the Assistant CP had little operational support within Ornge RW. Specifically:
- Following a program validation inspection (PVI) by TC in January 2013, an aviation clerk position was created to handle the checking and tracking of records, but this position was still vacant at the time of the accident.
- The positions of Manager of RW Flight Safety and Manager of RW Flight Training and Standards were both vacant at the time of the accident. The Assistant CP had assumed some of the training and standards duties.
- There was an assistant to the Manager of RW Flight Training and Standards position, but it was vacant at the time.
- In mid-2012, the pilot manager positions at helicopter bases were cut, and most of those positions' responsibilities were transferred to the CP position.
The workload in the Flight Operations department was too high for only 2 individuals, adversely affecting the organization's ability to manage and administer operational programs. This finding was issued by TC during its January 2013 PVI and was known to the company, but was not rectified before the accident, in part because the OM/interim CP and the Assistant CP remained overworked and had too few resources. The high workload was further exacerbated by the fact that they then were required to play an integral role in developing the corrective action plans (CAPs) resulting from the January 2013 PVI. Consequently, a number of safety-related and regulatory tasks were not resourced adequately, and were either incomplete or not being done at all, including the following:
- Problems with external training, which was not being provided in accordance with the TC-approved training manual (e.g., practical CFIT-avoidance and black-hole training), were not rectified in a timely manner.
- Pilot trainees were not effectively supported in their training (e.g., with provision of SOPs and training materials in advance of courses, and allottment of sufficient time for pre-training preparation and study).
- Training records were not being tracked and verified.
- Checking and tracking of pilot qualifications and currencies (including “green” status and second-in-command progression) was not being conducted.
- SOPs were not being updated and approved as required.
- Key positions in the Flight Operations department remained unfilled.
- Publications were not being updated to include the most current operational procedures.
As a result, the company was dispatching unprepared and unqualified pilots for flight. Ornge RW was operating with insufficient and inexperienced personnel in key positions, which allowed unsafe conditions to persist.
2.7.3 Safety management
The goal of safety management is to identify hazards and mitigate risks. A benefit of formal safety management processes is that safety information is documented and can be acted upon by the organization. Ornge RW had a number of safety management processes in place under the parent company's safety management system (SMS), but these processes were not yet adequately resourced or being used effectively by line pilots and managers. Operational safety issues were predominantly managed informally rather than through the company's safety reporting system. The following examples were relevant to the unsafe conditions present on the day of the accident:
- Although experienced S-76A pilots at Ornge RW were employing strategies to manage night hazards, these best practices had not been included in company SOPs.
- Pilots had raised concerns that new hires were being scheduled to start immediately on night shift, and that augmentee pilots from other bases were being paired, creating “green on green” situations. This issue was also the subject of an aviation safety report in the week following the occurrence, when 3 newly hired pilots, including 1 captain, were scheduled to start immediately on night shifts for their first block of shifts.
- Pilots had also raised concerns with respect to Revision 1 of FOD 034 (Green on Green), in which the requirement for company pilots to have operated from a specific base during the previous 3 months was removed.
These safety concerns were not entered in the company's safety reporting system; therefore, no risk assessments were conducted, and no mitigations were implemented. As a result, no changes to the company's procedures or scheduling practices were made, and the informally identified risks were allowed to persist.
Ornge RW contracted an external auditor in December 2012 to prepare for TC's January 2013 PVI. The audit found no instances of non-compliance with regulations, despite the deficiencies existing at the time that were later identified by the investigation into this occurrence. Ornge RW itself was unaware of non-conformances in its training program and in its process of tracking and checking pilot qualifications and currencies. The fact that Ornge RW was not aware of these significant regulatory non-compliances and unsafe conditions constitutes a breakdown in the management of safety. At the time, the Flight Operations department was not resourced to be able to meet regulatory requirements, and there was no flight operations quality assurance function.
Informal approaches to managing safety concerns in flight operations are not always effective in reducing risk. Safety issues at Ornge RW were managed informally rather than through the safety reporting system. If safety issues are not reported formally through a company's safety reporting system, there is a risk that hazards will not be managed effectively.
2.8 Survival aspects
The TSB has previously identified a large number of instances in which use of head protection likely would have reduced or prevented injuries sustained by a pilot. Although helmets were used by a large proportion of Ornge RW pilots, they were not worn by all pilots, including the captain involved in the occurrence. It was not possible to determine the extent to which use of a helmet would have mitigated the injuries sustained by the captain. If head protection is not worn by helicopter flight crew, they are at greater risk of injury and death due to head injuries following a crash.
2.9 Emergency locator transmitters
2.9.1 General
In November 1999, new International Civil Aviation Organization (ICAO) standards were adopted stipulating that, effective 01 January 2005, all ICAO countries require emergency locator transmitters (ELT) to operate on both 406 MHz and 121.5 MHz simultaneously. As a member country of ICAO, Canada is required to abide by its standards, unless TC files a difference with ICAO that enables foreign operators to make informed decisions about operating in Canadian airspace. In 2008, TC initiated a rule-making process, citing the 2005 changes to the ICAO standard and the numerous benefits of 406 MHz ELTs; however, TC elected to withdraw the proposed changes to the ELT regulations. Then in June 2015, a Notice of Proposed Amendment (NPA) was published on the TC Canadian Aviation Regulation Advisory Council (CARAC) activity website. That NPA proposes mandating the installation of dual 121.5/406 MHz–capable ELTs. However, at the time of report writing, the ELT regulations have not been amended to require a 406 MHz ELT in Canada. Therefore, Canada is not abiding by the International Civil Aviation Organization standards, which require ELTs to operate on 406 MHz and 121.5 MHz simultaneously, and TC has not filed a difference with ICAO as per the Convention on International Civil Aviation. If aircraft are not equipped with a 406 MHz-capable ELT, flight crews and passengers are at increased risk for injury or death following an accident because search-and-rescue (SAR) assistance may be delayed.
2.9.2 Emergency locator transmitter design standards
A number of 406 MHz ELT system design standards are spelled out in CAN-TSO-C126. However, these standards are lacking in their identification of crashworthiness requirements for the wiring and antenna components of the ELT installation.
The ELT on board the occurrence flight was most likely serviceable at the time of the occurrence; however, no signal was received due to a damaged antenna. As a result, the SAR crew did not have a precise location for the crash site or a signal that could be homed in using onboard equipment. It was therefore necessary to commence a search in the vicinity of CYMO before the wreckage was located. There have been many other occurrences in which no ELT signal was received by SAR satellites due to issues related to the crashworthiness of the ELT antenna, and these issues are widely documented. Studies conducted by Defence Research and Development Canada (DRDC), the Canadian Mission Control Centre (CMCC), the United States National Aeronautics and Space Administration (NASA), and the Australian Transport Safety Bureau (ATSB) have all identified a need for improved ELT system design standards that will enhance crash-impact survivability. The DRDC study determined that impact-related damage accounted for 92% of all ELT failures in the occurrences it examined.
If these issues can be overcome through better use of technology, the result would likely be a much lower ELT failure rate. In recent years, ELT systems have emerged that feature an integral global positioning system (GPS) receiver and internal antenna. These newer ELT systems provide an additional level of redundancy that could greatly increase the likelihood of ELT signal detection when the external antenna system is compromised during a crash sequence. However, this is just one example of efforts to improve the success of ELTs following an accident, and it is evident that more must be done to address the issue of ELT system crashworthiness. Despite extensive documentation of problems related to the crashworthiness of ELTs, no significant changes have been made to the ICAO standards in this regard. The current ELT system design standards do not include a requirement for a crashworthy antenna system. As a result, there is a risk that potentially life-saving SAR services may be delayed if an ELT antenna is damaged during an occurrence.
According to Cospas-Sarsat specifications for ELTs at time of writing, 406 MHz ELTs are required to have a minimum first-burst delay of approximately 50 seconds from the time of activation to the time of the first and subsequent transmissions. Further, there is no maximum allowable interval before the first transmission, with some ELTs in production having a first-burst delay of 100 seconds. If an ELT system is somehow rendered inoperative during the first-burst delay, a distress signal will not reach the Cospas-Sarsat system. While efforts are currently under way to develop a new 406 MHz specification for ELT systems with a significantly reduced first-burst delay threshold, those systems are still a long way from being available. The current 406 MHz ELT specifications call for a first-burst delay of 50 seconds or more from the time of activation. As a result, flight crew and passengers may be at increased risk of injury or death following an occurrence if an ELT is rendered inoperable during the first-burst delay period.
There is a documented history of the Kannad 406 MHz AF-H ELT, which was used in the occurrence helicopter, coming free from the hook-and-loop fastener that is intended to secure it to its mounting tray. The TSB, the United States National Transportation Safety Board (NTSB), the United States Federal Aviation Administration (FAA), the European Aviation Safety Agency (EASA), and the manufacturer have previously issued safety communications, including recommendations, on this subject. In late 2012, the FAA issued Technical Standard Order (TSO) C126b to indicate that hook-and-loop fasteners were no longer an acceptable means of complying with the crash safety requirements of Radio Technical Commission for Aeronautics (RTCA) RTCA/DO-204A. However, this change did not apply to previously installed ELTs.
Although TC has indicated its intent to adopt TSO-C126b, and recently published a Preliminary Issue and Consultation Assessment (PICA) related to this topic, there is no indication of when the current ELT design standards will be amended. Further, TC has indicated that, even if the ELT design standards are amended, it has no intention of requiring previously installed ELTs that met TSO-C126a specifications to be updated to the newer TSO-C126b standard. Consequently, hook-and-loop fasteners for ELT installations continue to be permitted in Canada, and a large number of them will remain in service for the foreseeable future. Despite a well-documented history of problems with hook-and-loop fasteners, TC has not yet adopted TSO-C126b. As a result, there is an ongoing risk that signals originating from ELTs secured by hook-and-loop fasteners will not be received due to the failure of these fasteners during an impact sequence.
2.10 Night regulations
2.10.1 Definition of night visual flight rules in Canada
Flights under VFR regulations must adhere to 2 principles—navigation with visual reference to the surface and the “see-and-avoid” concept of traffic separation—regardless of whether the flight is conducted in daylight or darkness. CARs 602.114 and 602.115 stipulate that all night VFR flights, whether conducted in controlled or uncontrolled airspace, be “operated with visual reference to the surface.”Footnote 277
Night VFR regulations vary around the world. In some countries, night VFR is prohibited and pilots who fly at night outside of control zones are required to conduct such flights under IFR. In other nations, night VFR is heavily restricted in terms of where the flight can be conducted. In the United States, night VFR regulations for helicopters require that there be sufficient light to safely control the aircraft. In Canada, there is no such requirement in general night VFR regulations.
What “visual reference to the surface” means is open to interpretation, as the concept is not defined in the regulations. TC has indicated that one of the expectations for night VFR is that there be a discernible horizon. However, in remote areas or areas with little or no cultural lighting, night VFR flights are frequently conducted in conditions where no discernible horizon is present, and where visual reference to the surface is not possible. This issue is considered throughout the aviation industry as presenting a risk to night operations, such that it was addressed in a Safety Bulletin issued by Ornge RW during the month preceding the accident. The bulletin highlighted scenarios in which pilots who enter areas with little or no outside visual reference are subject to the rapid onset of spatial disorientation.
Industry operators and crews have generally come to interpret “night VFR” as meaning that a flight is operated adhering to VFR weather requirements and, in the absence of visual cues, is conducted using instrument-flying skills and procedures. It was apparent during this investigation that most pilots at Ornge RW did not believe that operating flights in this manner represented a contravention to regulations. TC itself approves night VFR routes in areas with little or no cultural lighting, and there is no requirement for operators to demonstrate that visual reference can be maintained along such routes.
Ornge RW operates using a Type C operational control system, under which its pilots have the ultimate authority to accept a flight or not. Under current regulations, air ambulance operators are not required to conduct any type of formal risk assessment to determine whether the risks associated with a flight are warranted in light of the circumstances. On the night of the occurrence, the captain had turned down the flight to Attawapiskat twice due to poor weather. When the reported weather had improved to a 9000-foot overcast ceiling with 9 statute miles (sm) of visibility, the captain accepted the flight. However, with a mid-level overcast ceiling and very limited to no cultural lighting, it is unlikely that the crew would have been able to discern a horizon or maintain visual reference to the surface after departing CYMO and en route.
CAR 602.115 does not define “visual reference to the surface”, which has been widely interpreted by the industry as meaning VMC. As a result, night flights may be conducted with inadequate visual references, thereby increasing the risk of CFIT and loss-of-control accidents.
2.10.2 Night-vision imaging systems
Canada has vast areas with little or no cultural lighting to help a pilot maintain visual reference to the surface during unaided night VFR operations. In these regions, maintaining visual reference to the surface requires clear skies and significant celestial lighting, or the use of some type of night-vision imaging system (NVIS).
In 2006, the NTSB published its Special Investigation Report on Emergency Medical Services Operations. This document highlighted the potential benefits of night-vision goggles (NVG), but the NTSB did not issue a recommendation at that time to require their use. In 2009, the NTSB recommended that the FAA require HEMS operators to install NVIS equipment and that pilots be trained in their use during night operations. To date, the FAA has not made NVIS a regulatory requirement for HEMS operations. However, more than 90% of HEMS operators in the United States have adopted NVGs to take advantage of the enhanced situational awareness and increased level of safety afforded by their use.
Other countries have introduced regulations requiring NVIS for night HEMS operations, and have introduced specific regulations related to the approval of NVIS for night VFR operations.
In Canada, there is currently no requirement for NVIS use in HEMS or any other operation. Nevertheless, in recent years, there has been a significant increase in the number of operators that have adopted some type of NVIS. With the emergence of newer-generation NVGs, many of the limitations that existed in earlier versions are no longer factors deterring operators from adopting them. Consequently, NVG use among the civil rotor-wing community has steadily increased.
The decision by Ornge RW not to equip the AW139 fleet with NVG-compatible lighting or to convert the S-76 fleet to NVG use was partly due to its policy of not conducting scene calls at night. However, the company routinely conducts night VFR flights over large areas with little or no cultural lighting. In weather that is technically suitable for VFR but provides little ambient lighting, it is not always possible to conduct these flights with visual reference to the surface. Even if such flights are commenced with reference to the surface, there is a risk—especially in remote areas with limited weather forecasting—that conditions along the route will change and the required visual reference to the surface will be lost.
If, during night VFR operations, pilots continue flight in conditions where no cultural or ambient lighting exists without an alternate means of maintaining visual reference to the surface, there is an increased risk of CFIT and loss-of-control accidents.
2.11 Instrument currency requirements
Instrument proficiency is a required defence for commercial night VFR operations, even when flights are performed with visual reference to the surface. Crews must maintain a proper instrument scan at all times, and be ready to transition to flying solely by reference to flight instruments if they encounter areas where the visual cues outside the aircraft are insufficient to maintain control. Pilots are required to be current in accordance with CAR 401.05(3), which permits them, as a minimum, to exercise the privileges of an instrument rating if they have successfully completed an IFR PPC within the previous 12 months on the type being flown, with no other requirements.
Some instrument-rated pilots are able to maintain a higher level of currency through operational flights or training flights. However, Ornge RW operates almost exclusively in VFR conditions, and its pilots rarely carry out any instrument flying between annual recurrent simulator training sessions. The investigation determined that there is widespread sentiment among line pilots and regional inspectors, as well as some senior TC personnel, that the current instrument currency requirements do not provide an adequate level of safety due to the amount of time that could lapse since a pilot's last instrument flight. Despite these concerns, pilots would likely be reluctant to refuse an instrument flight, due to the anticipated perception of the refusal, if they were still current as per the regulations. Hence, the current regulations create a situation that would make it very difficult for pilots who are not comfortable with their instrument flight proficiency to refuse a flight for fear of potential repercussions from an employer that expects a pilot to be able to operate within the regulations.
Some operators in Canada have recognized the risks associated with the current regulations and taken it upon themselves to implement additional quarterly and semi-annual instrument-flight recency requirements. The recency requirements for instrument flight are more stringent in the Federal Aviation Regulations (FARs) and Joint Aviation Requirements (JAR-OPS), which require pilots to complete instrument-related currency training every 6 months to maintain their instrument ratings.
In this occurrence, both pilots had met the minimum instrument currency requirements as per the regulations, but were unprepared for the conditions they encountered during the flight. The PF had experienced difficulties in instrument procedures during his initial simulator training 9 months before the occurrence, and had required extra training hours. Following the training, he passed an IFR PPC with 3 major deviations. There is no evidence that the PF had carried out any IFR flight between his initial training and the occurrence flight. Indeed, the PF had no actual IFR time logged in helicopters at the time of the occurrence, and had only flown on instruments in a simulator. The captain had conducted no IFR flights, other than training, between 2011 and his date of hire by Ornge RW. Other than the IFR portion of his recurrent S-76 course in March, he had not conducted any IFR flights or received any IFR training while at Ornge RW before the accident.
The instrument currency requirements in the CARs allow pilots who have not flown using instrument procedures for up to 12 months to be considered current. As a result, pilots can conduct flights in IFR or dark night conditions with minimum IFR proficiency, increasing the risk of CFIT and loss-of-control accidents.
2.12 Terrain awareness and warning system
CFIT is a global safety issue. One of the most significant advances to counter CFIT has been the introduction of ground proximity warning systems (GPWS) and the more modern terrain awareness and warning systems (TAWS). In 1995, the TSB issued Recommendation A95-10 calling for GPWS in turbine-powered, IFR-approved, commuter and airline aircraft capable of carrying 10 or more passengers. After significant delays, TC issued new regulations stating that no private and commercial operator shall operate a turbine-powered aeroplane that has a seating configuration, excluding pilot seats, of 6 or more, unless the aeroplane is equipped with an operative TAWS and an enhanced altitude accuracy function. While an improvement, the new regulations did not apply to private and commercial helicopters, which routinely operate at lower altitudes than fixed-wing aircraft.
In this occurrence, the aircraft was not equipped with TAWS, nor was it required to be by regulation. Consequently, the flight crew did not receive a warning that the aircraft was inadvertently descending. Under current regulations, there is no requirement for TAWS to be installed on private or commercial helicopters, regardless of seating capacity. If helicopters are not equipped with TAWS, flight crews and passengers are at an increased risk for CFIT, particularly during night flights or instrument flights.
2.13 Regulatory oversight: Transport Canada
2.13.1 General
All transportation companies have a responsibility to manage the safety risks within their operations. However, given that companies will inevitably have varying degrees of ability or commitment to effectively manage safety, the regulator must be able to provide oversight in a manner that encourages the proactive identification and mitigation of risks, while intervening when necessary to ensure, at a minimum, regulatory compliance.
This investigation revealed problems with respect to the timely rectification of regulatory non-conformances at Ornge RW, as well as with the manner in which those non-conformances were addressed by TC and by Ornge RW itself. All of this took place in a period during which TC was transitioning to a more systems-level approach to surveillance, with one result being that the training and guidance provided to inspectors resulted in uncertainty and in surveillance that was either inconsistent, ineffective, or both.
2.13.2 Timely rectification of non-conformances
Developing the safety culture necessary to support a systems approach requires that enforcement action be reserved for situations in which an operator is unwilling to fix a problem that has been identified, or in which there are indications of willful wrongdoing or non-conformance. While there are obvious merits in allowing an operator to take an active role in addressing findings discovered during surveillance activities, it is important that TC ensures that non-conformances are rectified in a timely manner.
Between May 2012 and the date of the accident, multiple instances were identified, by the company and by TC, in which portions of the flight crew training program had not been completed, including CFIT-avoidance training as well as IFR and VFR components of the simulator training program. When the training issues were identified during TC's January 2013 PVI, the inspection team considered issuing a Notice of Suspension (NoS) to Ornge RW if the company proved unwilling to take action to address the issues. However, the operator voluntarily suspended flight operations on 2 separate days while pilot training records were verified and deficiencies addressed.
Upon completion of the PVI, the operator had taken sufficient action to satisfy the immediate concerns, including verifying training records and advising pilots that they were not to accept a flight unless all aspects of their training program had been completed. The exception to this was CFIT-avoidance training, since the company had indicated that it would take more time to complete, and that it would prepare a short-term CAP on the issue. This approach was acceptable to TC; however, the CAP was never submitted or actioned. The result was that the CFIT-avoidance training issue persisted until after the accident. Although there were clear indications during the January 2013 PVI that Ornge RW lacked the necessary resources to ensure the timely return of the company to a state of compliance, these were not considered during the post-surveillance decision-making process. Instead, TC permitted Ornge RW to address the non-conformances by relying solely on the CAP process, even though there were tools, such as enhanced monitoring and NoS, that were available to assist in the timely return to compliance. The reasons underlying the decision to use only the CAP process will be further analyzed under heading 2.13.3.
The CAP process can be lengthy. In the case of Ornge RW, the time required to prepare the CAPs and rewrite the ones that TC had rejected meant that 127 days had elapsed from the day on which the training issues had been identified to the day of the accident. At the time of the accident, since the long-term CAP implementation dates had not yet passed, TC had not yet completed its follow-up to ensure that the identified corrective actions had been implemented. Although long-term corrective action is to be completed within 90 days when using the process, CAP preparation is not included in this timeline, and the 90-day period only begins once a CAP has been accepted.
As seen in this occurrence, systemic training deficiencies were repeatedly identified, first by the company in May 2012, then during TC surveillance activities in December 2012 and January 2013. Each time, TC received assurances that the issues would be addressed. However, at the time of the post-occurrence process inspection (PI), 4 months had passed since the PVI; more than 6 months had elapsed since incomplete training had been identified during a PI conducted in November 2012; and more than a year had elapsed since this issue was first raised by company personnel. Despite the ongoing CAP process, the post-occurrence PI identified deficiencies related to
- practical CFIT-avoidance training;
- lack of sufficient operational management and support personnel to ensure COM requirements were being followed; and
- documentation of the progression of first officers and direct-entry captains.
Therefore, this accident highlights the fact that TC's approach to surveillance activities did not lead to the timely rectification of non-conformances that were identified, allowing unsafe practices to continue.
2.13.3 Selection of surveillance option
As described in the 2014 TSB Watchlist issue, Safety management and oversight, the wide range of differences in capability and willingness on the part of operators to manage safety means that a key element of advancing safety is a balanced approach to regulatory oversight. It must include proactive auditing of an operator's safety systems, in addition to traditional inspections to ensure compliance with regulations, backed up by timely interventions to eliminate unsafe operating practices.
In 2005, TC adopted a systems approach to regulatory oversight, and transitioned from determining regulatory compliance only by direct inspection to a model that included a review of the effectiveness of a certificate holder's safety management processes. TC's original intent was to have a 2-layered system that would permit it to examine an operator's safety management processes while maintaining the ability to conduct regulatory audits and inspections as required. Such focus on compliance is necessary when an operator is unable or unwilling to follow the CAP process in a timely manner, or in situations of intentional non-compliance.
Under a balanced approach to regulatory oversight, the regulator could maintain increased direct-inspection oversight activities in the case of an operator that did not have an SMS, or that was in the early stages of developing one. This approach would provide sufficient assurance that the company was operating in compliance with regulations. As the company's management system matured, direct-inspection activities could be reduced.
As demonstrated under heading 2.7.2, TC had ample indications at the conclusion of the January 2013 PVI that Ornge RW lacked the capability to return to regulatory compliance in a timely manner. However, the decision by TC to use only the CAP process was driven by the operator's willingness to participate and not by its actual ability to rectify non-conformances.
TC had 3 other oversight tools, each with the potential to motivate change or provide greater monitoring:
- An NoS, which would have provided a limited time frame for the operator to address issues of non-compliance, was considered in post-surveillance decision making but was not thought to be appropriate. Several factors influenced this decision, including the facts that this was Ornge RW's first PVI, that the company had taken immediate actions to address identified non-compliances, that it accepted all of the PVI findings, and that it demonstrated a willingness to complete the short- and long-term corrective actions.
- Detection notices, which would have initiated enforcement action for areas of non-compliance, were never considered during post-surveillance decision making—likely for the same reasons that an NoS was not considered appropriate. The initiation of enforcement action was seen as contrary to the spirit of cooperation necessary for a systems approach to surveillance to be successful. In fact, it was not until similar issues were found during the post-accident PI in June 2013 that inspectors issued 8 detection notices to TC Enforcement to initiate enforcement action.
- Enhanced monitoring (EM), which would have resulted in an increased level of surveillance of the operator while issues of regulatory non-compliance were addressed, was not considered during post-surveillance decision making. At the time, EM was not considered to be an available option, because TC regional personnel believed that it could be used only after an NoS had been issued, as per SUR-001 Issue 04 and SUR-002 Issue 02.
Therefore, the selection of the CAP process as the sole means of returning Ornge RW to a state of compliance resulted from the belief that other options were either unavailable or inappropriate for use with a willing operator. This belief contributed to non-conformances being allowed to persist.
2.13.4 Training and procedures supporting the transition to a systems approach to surveillance
Under a traditional approach to surveillance, TC inspectors were limited to verifying an operator's compliance with regulations. However, to provide an improved level of safety beyond regulatory compliance, TC has moved toward a systems-level approach. This type of approach involves verifying not only that operators are in compliance, but that they also have processes in place to develop corrective actions that address the underlying causes of non-conformances and to manage those actions effectively. In the long term, this approach will have a greater impact on safety than a program that relies solely on traditional inspections and local fixes.
Such broad change is not without its challenges, and has required a significant degree of learning and adaptation within all areas of the regulator. In particular, TC inspectors require clear training and procedures to understand how to provide oversight effectively under the new system. The investigation found that, despite extensive documentation and revisions to TC guidance materials, areas of uncertainty remain. These uncertainties resulted in the inconsistent application of surveillance procedures in the areas of post-surveillance decision making, the initiation of certificate action, and the scoping and sampling strategies used by inspectors.
2.13.4.1 Post-surveillance analysis and decision making
As noted under heading 2.13.3, the selection of the CAP process as the sole means of returning Ornge RW to a state of compliance resulted from the belief that other options were either unavailable or inappropriate for use with a willing operator. The training and guidance provided to inspectors contributed to this understanding. For example:
- Internal Process Bulletin (IPB) 2012-02, which was in effect at the time of the January 2013 PVI, said managers were to analyze findings according to 5 criteria: the number, nature, and systemic nature of the findings, and the compliance and enforcement history of the organization. The convening authority was then to decide on a course of action from 4 options: requesting a CAP, issuing a detection notice, using both of these processes in tandem, or issuing a notice of suspension/notice of cancellation. However, the bulletin gave no additional criteria to assist with this analysis or decision making, leaving considerable scope for subjectivity. Nor was there any process to document this. It should also be noted that EM was not one of the listed options.
- The decision record documenting the selection of the CAP process—which was signed several hours after the accident—indicated only that the convening authority had chosen this option as it was consistent with the cooperative approach emphasized in the policies and procedures. A full assessment of all 4 options was never completed, nor was it common practice to do so.
- Weaknesses in inspector training may also have contributed to the perception that the CAP process was the only option available. Training provided on SUR-001 Issue 04 was taught using one major SMS-related case study for most of the course. Both the procedure and training were highly focused on teaching inspectors to conduct SMS assessments. Guidance on assuring compliance from an organization that did not have a TC-assessed SMS, and that was more willing than capable to apply the CAP process, was not covered in detail during the training.
2.13.4.2 Initiation of certificate action
Following the post-occurrence PI, TC regional personnel encountered difficulties developing a case for certificate action, which reinforced the belief that they lacked the appropriate tools to do so when warranted. Here, too, training and guidance were contributory.
In recent years, for instance, the guidance provided to TC inspectors has evolved considerably with respect to how to suspend or cancel an operating certificate under the Aeronautics Act. Initially, SUR-001 Issue 04 indicated that an immediate NoS was appropriate in response to a critical finding that represented an immediate threat to safety. Yet this document provided no criteria as to what information was required to demonstrate that an immediate threat to safety existed. Subsequently, TC published SUR-014 Issue 01 in July 2011, which provided more information regarding what justification was required for an NoS.
As a result, following the post-occurrence PI, TC regional inspectors believed certificate action was justified in response to safety concerns and their loss of confidence in the company. SUR-014 described 2 sections of the Aeronautics Act (regarding certification and public interest) as being appropriate for certificate action against an organization. A case to issue an NoS was initially developed under the certification section. However, TC HQ advised the PI team that a case could not be made under this section, but that they may have a case under the public-interest clause. Efforts to take certificate action under this clause were abandoned as the required aviation record had not been established.
In August 2013, TC published IPB 2013-02, clarifying what it referred to as a “misconception,” and again giving inspectors further guidance as to which section of the Act was appropriate for various circumstances. Yet this guidance was not available to TC inspectors at the time they were preparing the case for an NoS for Ornge RW.
2.13.4.3 Scoping and sampling
A PVI was conducted in October 2014 using a focused sampling procedure described in the recently issued SUR-001 Issue 05.This document did not specify whether focused sampling was to be used in isolation or in addition to routine sampling. Issue 05 differed significantly from Issue 04, and inspectors had not yet received training specific to this new version. This led to a great deal of uncertainty among inspectors as to how focused sampling should be applied and whether it was appropriate for use in isolation.
The PVI's scope and depth were limited to offence-creating provisions, due to the perception among some of the regional inspectorate that examining non-offence-creating provisions was a waste of time because they could not lead to enforcement action. This perception had resulted, in part, from the experience of abandoning the NoS following the June 2013 post-occurrence PI, when the information required to pursue an NoS was not readily available.
SUR-001 Issue 05 does state that offense-creating provisions should be the primary link to the expectations that define the intent of regulatory requirements, as this would ensure the required information would be available should enforcement action be required. However, Issue 05 does not limit surveillance activities to offense-creating provisions.
The use of focused sampling, targeting only offence-creating provisions for the review of the pilot training files, meant that only a small portion of regulatory requirements were verified by the PVI team. For example, the inspection simply verified that the required number of training hours had been completed, and not that all of the training specified in the company training manual had been delivered to all pilots. Therefore, there was no validation that the training program was being applied as intended.
During the lead-up to the October 2014 PVI, it was evident that the lack of training on the updated SUR for some inspectors was leading to confusion and uncertainty as to how the new procedures were to be applied. Following the PVI, TC communicated to the operator that all areas of enterprise operation were in compliance with regulatory requirements. However, this was a focused sampling limited to offence-creating provisions and, as conducted, could not assure that the non-conformances leading to the previous findings related to non-offence-creating provisions had not recurred.
The issues described above demonstrate that, prior to the occurrence, there was limited consideration of the options available to bring Ornge RW into compliance. Following the occurrence, inspectors had difficulty initiating an NoS when they had lost confidence in the operator, and the scope of a subsequent PVI, conducted over a year after the occurrence, was limited such that it could not provide assurance that the systemic issues identified previously had been rectified.
Although TC has made significant efforts toward transitioning to a systems approach to oversight, the training and guidance that was provided to TC inspectors resulted in uncertainty, which led to inconsistent and ineffective surveillance of Ornge RW.
2.13.5 Application of systems-level oversight to non-safety management system companies
TC's policies, procedures, and training with respect to a systems approach to oversight were premised on the understanding that SMS would be progressively implemented for all air operators, and that all would have formal systems in place to manage safety. One key aspect of an SMS is the capability of an operator to identify and rectify underlying unsafe conditions, including non-compliance with regulations. This capability was a foundation for the use of a non-punitive approach to regulatory compliance. In practice, it meant that inspectors were encouraged to use the CAP process until corrective actions were either not effective or the problem recurred.
While TC was building its experience and capability to provide surveillance in this manner, it supported the industry in SMS implementation through a phased-in approach:
- TC worked cooperatively with operators through a phased implementation, managed by an exemption, to develop and implement the required 6 SMS components into their air operations.
- TC conducted a full SMS assessment at the end of the phased implementation, whereby the capability of the air operator to manage safety was assured through an SMS assessment.
Because a systems approach to oversight was introduced with the understanding that all operators would eventually be required to have an SMS, it was originally intended that an operator's capability to identify and rectify underlying unsafe conditions would be assured before the systems-level surveillance tools were used. However, in 2009,Footnote 278 TC paused its introduction of SMS regulations for CARs Subpart 702, 703, and 704 operators, to allow more time for industry to prepare, and for TC to refine oversight tools and provide updated training to inspectors.
Despite the pause, TC continued to evolve its systems approach to surveillance for all air operators, including those that were not subject to SMS requirements. The systems approach can be effective for all systems and processes, but the operators' capability to identify and rectify underlying unsafe conditions themselves must first be assured.
Ornge RW identified problems with its training program in May 2012, and TC identified similar problems in November 2012 and January 2013. Through its lack of success with the CAP process on repeated occasions, the company demonstrated that it was not adequately resourced and capable of rectifying the underlying unsafe conditions in a timely manner. Ornge RW's ability to follow the CAP process had not been developed nor assessed before TC decided to rely solely on it; the decision was based primarily on the company's willingness to rectify non-conformances.
TC's approach to systems-level oversight is predicated on all operators, even those without an assessed SMS, possessing the capability to address non-conformances. If operators do not have the capability to address non-conformances, this increases the risk that unsafe conditions will persist.
3.0 Findings
3.1 Findings as to causes and contributing factors
- The crew conducted a flight under night visual flight rules regulations without sufficient ambient or cultural lighting needed to maintain visual reference to the surface.
- When the pilot flying encountered a lack of visual cues off the departure end of Runway 06, necessitating transition to flight by reference to instruments, an excessive bank angle and rate of descent developed, which were not recognized by the crew at an altitude that permitted recovery.
- The severity of the impact forces caused the deaths of the first officer and one of the flight paramedics, and likely rendered the captain and the other flight paramedic unconscious. The latter 2 individuals likely succumbed rapidly to their injuries before significant inhalation of fire combustion products.
- The crew were not operationally ready to safely conduct a night visual flight rules departure that brought the flight into an area of total darkness.
- Insufficient and inadequate training contributed to the difficulties that the crew encountered during the departure from Runway 06 at Moosonee Airport (CYMO).
- Ornge Rotor-Wing did not have dedicated night-flight standard operating procedures (SOPs) to address the hazards specific to night operations, except for designated black-hole locations, which did not apply to Moosonee. As a result, the inadequacy of the company's night-flight SOPs contributed to the accident.
- Ornge Rotor-Wing was not using the company's currency tracking program (i.e., AvAIO) as intended to ensure that pilots were qualified in accordance with both company and regulatory night-flight currency requirements. As a result, the central scheduling department did not identify that, according to inaccurate data in AvAIO, the first officer was not qualified for the flight.
- Although Ornge Rotor-Wing had established policies and procedures defining the operational readiness of its pilots, these were bypassed and eroded by the company, which resulted in the crew not being operationally prepared for the conditions encountered on the night of the occurrence.
- Ornge Rotor-Wing was operating with insufficient and inexperienced personnel in key positions, which allowed unsafe conditions to persist.
- Transport Canada's approach to surveillance activities did not lead to the timely rectification of non-conformances that were identified, allowing unsafe practices to continue.
- The selection of the corrective action plan process as the sole means of returning Ornge Rotor-Wing to a state of compliance resulted from the belief that other options were either unavailable or inappropriate for use with a willing operator. This belief contributed to non-conformances being allowed to persist.
- The training and guidance that was provided to Transport Canada inspectors resulted in uncertainty, which led to inconsistent and ineffective surveillance of Ornge Rotor-Wing.
3.2 Findings as to risk
- If pilots engage in other work-related activities before the commencement of scheduled flight duty time, there is a risk that regulatory flight duty time limitations will be exceeded, which may degrade performance due to fatigue.
- Under current regulations, there is no requirement for multi-crew Canadian Aviation Regulations Subpart 703 pilots to undergo any type of line indoctrination. As a result, there is a risk that pilots will not be fully prepared to safely conduct operations in their designated positions on all company routes.
- If companies do not take adequate steps to protect the integrity of mandatory exams administered to their pilots, there is a risk that the tests will not be effective in validating that pilots possess the prerequisite knowledge needed to safely carry out their duties as flight crew.
- There is currently no regulatory process for multi-crew Canadian Aviation Regulations Subpart 702, 703, and 704 operators to have company standard operating procedures reviewed by Transport Canada. As a result, there is a risk that non-optimal procedures will be adopted.
- Under current regulations, Canadian Aviation Regulations Subpart 702, 703, and 704 helicopter first officers and captains are held to the same pilot proficiency check standard. As a result, there is an increased risk that a pilot assigned to captain duties will lack the required proficiency and crew resource management skills to safely carry out those responsibilities.
- If the experience and proficiency of pilots are not factored into crew scheduling, there is a risk of sub-optimal crew pairings, resulting in a reduction of safety margins.
- If safety issues are not reported formally through a company's safety reporting system, there is a risk that hazards will not be managed effectively.
- If head protection is not worn by helicopter flight crew, they are at greater risk of injury and death due to head injuries following a crash.
- If aircraft are not equipped with a 406 MHz-capable emergency locator transmitter, flight crews and passengers are at increased risk for injury or death following an accident because search-and-rescue assistance may be delayed.
- The current emergency locator transmitter (ELT) system design standards do not include a requirement for a crashworthy antenna system. As a result, there is a risk that potentially life-saving search-and-rescue services may be delayed if an ELT antenna is damaged during an occurrence.
- The current 406 MHz emergency locator transmitter (ELT) specifications call for a first-burst delay of 50 seconds or more from the time of activation. As a result, flight crew and passengers may be at increased risk of injury or death following an occurrence if an ELT is rendered inoperable during the first-burst delay period.
- Hook-and-loop fasteners for emergency locator transmitter (ELT) installations continue to be permitted in Canada, and a large number of them will remain in service for the foreseeable future. Despite a well-documented history of problems with hook-and-loop fasteners, Transport Canada has not yet adopted Technical Standard Order C126b. As a result, there is an ongoing risk that signals originating from ELTs secured by hook-and-loop fasteners will not be received due to the failure of these fasteners during an impact sequence.
- Canadian Aviation Regulation 602.115 does not define “visual reference to the surface”, which has been widely interpreted by the industry as meaning visual meteorological conditions. As a result, night flights may be conducted with inadequate visual references increasing the risk of controlled-flight-into-terrain and loss-of-control accidents.
- If, during night visual flight rules operations, pilots continue flight in conditions where no cultural or ambient lighting exists without an alternate means of maintaining visual reference to the surface, there is an increased risk of controlled-flight-into-terrain and loss-of-control accidents.
- The instrument currency requirements in the Canadian Aviation Regulations allow pilots who have not flown using instrument procedures for up to 12 months to be considered current. As a result, pilots can conduct flights in instrument flight rules (IFR) or dark night conditions with minimum IFR proficiency, increasing the risk of controlled-flight-into-terrain and loss-of-control accidents.
- If helicopters are not equipped with terrain awareness and warning systems, flight crews and passengers are at an increased risk for controlled flight into terrain, particularly during night flights or instrument flights.
- Transport Canada's approach to systems-level oversight is predicated on all operators, even those without an assessed safety management system, possessing the capability to address non-conformances. If operators do not have the capability to address non-conformances, this increases the risk that unsafe conditions will persist.
3.3 Other findings
- There was no indication that, subsequent to the January 2013 program validation inspection, regional Transport Canada personnel had been influenced by Ornge Rotor-Wing's provincial emergency medical services role.
- There were no signs of pre-existing or impact-related damage to explain why the helmets were not found on the victims, and it was not possible to determine whether they had been properly secured before the occurrence.
- It was not possible to determine whether all of the occupants were wearing their seat belts and shoulder harnesses at the time of impact.
- The landing-gear warning horn sounded just prior to impact, and was most likely activated as a result of erroneous pitot-static readings caused by impact with the trees.
4.0 Safety action
4.1 Safety action taken
4.1.1 Transport Canada
Since the occurrence, Transport Canada (TC) has undertaken a number of different actions. Although TC has indicated that none of these actions were taken as a direct result of this occurrence, it is important to understand the evolution of TC oversight since the accident. Several of those actions were described earlier in this report. Other actions taken included the following:
- 2014: Launched Staff Instruction (SI) SUR-001 Issue 05 e-learning for all inspectors.
- 2014: Lauched a two-day classroom course on the surveillance procedures described in SUR-001 Issue 05. The training included exercises/case studies and examples of correctly completed forms for new inspectors.
- 2014: Established a Multi-modal Technical Training (MITT) office to create a more efficient, innovative and streamlined technical training program for the department's technical and inspectorate community in all modes and to develop a core curriculum that delivers greater consistency through an integrated approach.
- 2015: Issued Internal Process Bulletin (IPB) 2015-03 on certificate action policy to ensure more timely and effective risk-based decision making in response to surveillance findings.
- 2015: Developed a sampling plan builder tool to improve the ability of inspectors to conduct sampling and detect regulatory non-compliance.
- 2015: Published guidance material on root cause analysis and effective corrective action plans (CAP).
- 2015: Convened a surveillance learning working group.
- 2015: Issued Advisory Circular (AC) SUR-004 Issue 01, Civil Aviation Surveillance Program. According to the document, the purpose of the AC is to describe TC's surveillance program based on SUR-001.
- 2015: Established National Oversight Office (NOO) to assist with managing the way safety oversight is delivered and monitored. The NOO facilitates discussion with management on a monthly basis to review national and regional oversight risks related to industry performance and compliance as well as oversight delivery performance. This provides a platform for decision making on issues related to complex oversight matters as well as continuous monitoring of enterprise performance and compliance.
- 2015: Established an Oversight Advisory Board (OAB). The mandate of the OAB is to provide support and recommendations to operational branches for addressing concerns and processing complex oversight decisions quickly and effectively, and consistently allowing operational branches to take timely action against certificate holders that are not operating within regulatory requirements.
- 2015: Made substantial changes to the oversight planning process, which highlight the progress that has been made with respect to planning and reporting as well as improvements to program delivery.
- 2015: Recently reconstituted the National Civil Aviation Learning Committee to provide direction pertaining to learning activities with a view to making adjustments to training material, where and when required.
- 2015: Issued AC SUR-002 to provide more information to certificate holders and inspectors regarding root cause analysis and corrective action for Transport Canada Civil Aviation findings.
4.1.2 7506406 Canada Inc. (Ornge Rotor-Wing)
Following the accident, Ornge RW took the following safety actions:
- Suspended black-hole operations until an acceptable risk mitigation plan could be put in place.
- Revised company standard operating procedures (SOPs) to include
- New approach, go-around, and departure procedures;
- Revised crew briefings;
- Standard flight deviation guidance to enable flight crews to effectively identify an unstabilized situation;
- Additional guidance regarding the use of radio altimeters;
- Restrictions requiring at least 1 crew member to have flown to the planned black-hole site within the previous 6 months.
- New black-hole procedures.
- Set out restictions requiring flight crew not to attempt or continue a black-hole approach unless certain conditions exist.
- Set out the following restrictions for all night takeoff and departure procedures:
- Calling for the after-takeoff checklist only after passing 500 feet above ground level (agl);
- No turns below 1000 feet agl unless otherwise instructed by air traffic services or in adherence to a published procedure.
- Prohibited normal or emergency checklist usage during turns unless operationally required.
- Prohibited turns exceeding standard rate 1 for night and instrument flight rules (IFR) operations.
- Amended the Company Operations Manual (COM) to include provisions under Flight Crew Member Incapacitation Alert Conditions and actions to be taken in the event of flight crew member incapacitation.
- Amended emergency locator transmitter (ELT) maintenance procedures to include a verification of proper retention strap tension and overall condition of the hook-and-loop fastener.
- Enhanced crew pairing procedures, and made flight crew assignments the sole responsibility of the chief pilot (CP) or the CP's delegate.
- Created a formal First Officer Progression Monitoring program to ensure that all necessary steps in a first officer's progression are completed and documented in the pilot's training file.
- Revised procedures for captain assessment with regard to upgrades to captain status.
- Efforts were accelerated, and ground-based lighting has been installed at 91 helipad locations. The remaining 2 pads are day only and are awaiting re-location of the pads.
- Formed a working group to study available technological opportunities for night visual flight rules (VFR) operations. As a result of this working group, Ornge RW conducted a trial of white phosphur night-vision goggles (NVG) at its Sudbury, Ontario, base. The company's flight training pilots and most of the base pilots in Sudbury participated in the NVG trial. On 01 April 2016, Ornge RW announced that the NVG trial had been successful and that it would be implementing NVGs across its entire AW139 fleet, beginning with the northern bases. Ornge RW plans to have NVGs implemented at additional northern bases by the end of calendar year 2016, with the project completed in 2017.
- Removed one of the S-76As from service due to its differences from the remainder of the fleet.
- Hired a Standards and Training Pilot to ensure consistent simulator and line training. The person hired into that position was subsequently promoted to the position of Manager, Standards and Training. Efforts are currently underway at Ornge RW to fill the Standards and Training Pilot vacancy resulting from this person's promotion.
- Introduced line checks (in aircraft) in the base operating area.
- Amended the recurrent flight training program to include on-aircraft training in avoidance of controlled flight into terrain, black-hole flight training, and night VFR flight training.
- Following simulator training and a pilot proficiency check, mandated additional on‑aircraft training followed by a further operational evaluation for its CARs Subpart 703 pilots.
- Ensures that all new hire pilots are paired with a company training captain for initial assignment to emergency medical services (EMS) shifts.
- Now uses an online testing website to administer all exams, in order to protect the integrity of company exams. The site allows individual exams to be randomly generated from category-specific question banks. Additionally, exams are reviewed on an annual basis and updated as required.
- Added a proficiency flying program, allowing pilots to do non-EMS flying to maintain proficiency on night, black-hole, IFR, manoeuvres, and hover exits.
- Developed company night visual approach charts (NVA) to provide flight crew with a safe and efficient means to transition between an enroute phase of a night VFR flight, to a final approach at a company-approved helipad. These charts were patterned in a similar fashion to a NAV CANADA Instrument Approach Chart, with which all flight crew are familiar. The waypoints and minimum altitudes were developed using Air Navigation software for instrument approach design. The obstacle database this software references is updated on a 56-day cycle. The approach procedure in these charts is flight tested under day VFR conditions to ensure accuracy and obstacle clearance before being approved for night VFR operations.
- Introduced a mandatory helmet policy for pilots.
- Introduced aviation safety quick turns (QT), which immediately identify events or safety concerns to frontline staff within 48 hours of a report.
- Introduced electronic flight bags (EFB) in a trial program to add capability for aircraft library.
- Working on the initial stages of a flight data recording (FDR) and associated flight operations quality assurance (FOQA) program.
- Working on developing a flight risk assessment tool (FRAT) for EFBs to be used as a pre-flight and pre-shifts tool to measure and mitigate operational risk.
- Established a new-hire mentoring program to help new employees acclimate more quickly into the organization. During initial simulator training, an experienced company pilot works in conjunction with the simulator instructor to provide guidance on company standard operating procedures and to provide advice and support as the candidates progress throughout their training.
- Underwent an extensive operational risk assessment process for night VFR operations that looked at all elements associated with night flying. This assessment looked at various elements such as the company's standard operating procedures, training and currency, organizational support networks, aircraft performance, human factors and many other items, and developed and implemented mitigation strategies.
- In the early summer 2014, Ornge RW converted its Kenora, Ontario, and Thunder Bay, Ontario, bases to the AW139.
- Made the decision to replace the company's S-76A helicopters currently operating in Moosonee, Ontario, with AW139 aircraft. According to Ornge RW, the S-76A helicopters will be withdrawn from service in June 2016. Ornge is adding 1 additional AW139 airframe to its fleet to accomplish this change. Ornge RW's goal is to have this additional AW139 in service by October 2016.
4.2 Safety action required
In this occurrence, the aircraft's 406-megahertz (MHz) ELT was compromised, rendering it unable to transmit a distress signal to the Cospas-Sarsat satellite system. This led to a further examination of the ELT's serviceability, ELT design standards, and the ELT regulatory requirements for Canadian-registered aircraft.
4.2.1 406-megahertz emergency locator transmitters
According to the International Civil Aviation Organization (ICAO) ELT Standards, there is no longer a requirement for ELTs to transmit on 121.5 MHz. Since 01 February 2009, Cospas-Sarsat no longer monitors 121.5 MHz. Cospas-Sarsat is capable of detecting and locating only 406 MHz signals, and is Canada's primary means for search and rescue (SAR) alerting, detection and response. Despite this, currently only 121.5 MHz ELTs are required by regulation in Canada. Canada is not abiding by the ICAO ELT Standards, which came into effect in 2005 and require aircraft to be equipped with a 406 MHz ELT. As a result, Canadian-registered aircraft are permitted to operate in Canada with ELTs whose distress signals cannot be detected by the international Cospas-Sarsat system.
According to TC, approximately 27 000 Canadian-registered aircraft require an ELT. However, in March 2016, there were only 10 086 Canadian-registered aircraft in TC's Aircraft Registry database equipped with at least one active 406 MHz ELT registered through the Canadian Beacon Registry. Of those aircraft, 5256 were private, 4604 were commercial, and the remaining 226 were state-owned. Therefore, more than half of all Canadian-registered aircraft that require an ELT are being operated with an ELT whose signal is not detectable by the Cospas-Sarsat system.
Previously, TC advocated for and promoted the benefits of 406 MHz ELTs, and initiated the formal rule-change process to make them a regulatory requirement. However, in the face of opposition from segments of the aviation community, TC discontinued those efforts. In June 2015, 10 years after the ICAO 406 MHz ELT requirement came into effect, TC published a Notice of Proposed Amendment (NPA) on the Canadian Aviation Regulation Advisory Council (CARAC) Activity website proposing mandatory installation of dual 121.5/406MHz-capable ELTs. According to TC, the intent of the proposed regulation can be met with a stand-alone 406 MHz ELT in addition to an existing 121.5/243.0 MHz ELT; however, TC has indicated that virtually all 406 MHz ELTs are now dual frequency.
If the regulations are not amended to reflect the ICAO standards, it is highly likely that non-406 MHz ELTs will continue to be used on Canadian-registered aircraft and foreign aircraft flying in Canada. As a result, flight crews and passengers will continue to be exposed to potentially life-threatening delays in SAR services following an occurrence.
Therefore, the Board recommends that
The Department of Transport require all Canadian-registered aircraft and foreign aircraft operating in Canada that require installation of an emergency locator transmitter (ELT) to be equipped with a 406 MHz ELT in accordance with International Civil Aviation Organization standards.
Transportation Safety Recommendation A16-01
4.2.2 Emergency locator transmitter system crashworthiness
In this occurrence, as in numerous others investigated by the TSB,Footnote 279 the ELT system was rendered inoperative nearly immediately or within seconds following impact by damage sustained during the crash sequence. As a result, the ELT was unable to transmit a distress signal to the Cospas-Sarsat SAR satellite system. In many instances, ELT signals have not reached the Cospas-Sarsat system due to a broken antenna or a break in the wire connecting the ELT unit to the antenna. In this occurrence, it was determined that although the ELT unit was operable, a broken ELT antenna prevented the signal from being transmitted. The crashworthiness design specifications are robust for the actual ELT unit; however, the specifications are significantly less stringent for the other key components (i.e., the wiring and antenna) of the ELT system.
One of the inherent limitations of a 121.5 MHz ELT is its requirement for a whip-style antenna, which extends outward from the aircraft fuselage, significantly increasing the likelihood that it will be damaged or broken by impact with terrain, trees, or other parts from the aircraft during a crash sequence. Modern 406 MHz ELTs permit the use of low-profile (i.e., flush-mounted) antenna installations, which are significantly less susceptible to such damage. TC has recently issued an NPA that would mandate 406 MHz ELTs; however, the NPA also states that the regulation will mandate the carriage of dual 121.5-/406 MHz ELTs. According to TC, retaining the 121.5 MHz requirement for new 406 MHz ELT installations, in accordance with Technical Standard Order (TSO) C126b, is to allow for homing. If these dual-frequency units are designed to use a single antenna, that antenna would need to be whip-style to accommodate the 121.5 MHz frequency. Some 406 MHz ELT units now come equipped with a backup, internal global positioning system (GPS) receiver and antenna that meet the specifications of Radio Technical Commission for Aeronautics (RTCA) RTCA DO-204A and European Organisation for Civil Aviation Equipment (EUROCAE) document ED62A. However, the internal antenna has not been tested and approved by Cospas-Sarsat, whose standard does not include details on the design's radiation and power output. Finally, depending on the location of the ELT unit, the signal from an ELT using an internal antenna may be emitted at a reduced effectiveness due to shielding from aircraft components or terrain. TC has indicated that it will not stipulate a dual-antenna requirement for new dual 121.5/406 MHz ELTs. As a result, if the design standards allow for a single antenna, versus separate 121.5 MHz and 406 MHz antennas, to be used on dual-frequency units, the risks associated with the use of a whip-style antenna will persist.
ICAO establishes International Standards and Recommended Practices for member states. However, it has not established any ELT system design standards; these are currently determined by national regulatory bodies such as TC, the Federal Aviation Administration (FAA), and the European Aviation Safety Agency (EASA). In Canada, Canadian Aviation Regulations (CARs) Part V—Airworthiness Manual (Chapter 551: Aircraft Equipment and Installation) states that ELTs must meet the performance standards for 121.5 MHz and 406 MHz ELTs set out by the RTCA. In the United States, although there is no regulatory requirement for 406 MHz ELTs, the FAA only accepts requests for new ELT technical standard order authorizations for 406 MHz ELTs. As in Canada, the FAA relies on the performance specifications set out by the RTCA. In Europe, EASA has taken a similar approach, requiring that ELTs meet the design specifications set out by EUROCAE. A considerable body of research now indicates that current ELT design standards do not ensure a reasonable degree of crash survivability.
As a result, it is highly likely that aircraft equipped with ELT systems that meet the current design standards will continue to be involved in occurrences in which potentially life-saving SAR services will be delayed as a result of damage to the ELT system, decreasing the survivability of an accident.
Therefore, the Board recommends that
The International Civil Aviation Organization establish rigorous emergency locator transmitter (ELT) system crash survivability standards that reduce the likelihood that an ELT system will be rendered inoperative as a result of impact forces sustained during an aviation occurrence.
Transportation Safety Recommendation A16-02
The Radio Technical Commission for Aeronautics establish rigorous emergency locator transmitter (ELT) system crash survivability specifications that reduce the likelihood that an ELT system will be rendered inoperative as a result of impact forces sustained during an aviation occurrence.
Transportation Safety Recommendation A16-03
The European Organisation for Civil Aviation Equipment establish rigorous emergency locator transmitter (ELT) system crash survivability specifications that reduce the likelihood that an ELT system will be rendered inoperative as a result of impact forces sustained during an aviation occurrence.
Transportation Safety Recommendation A16-04
The Department of Transport establish rigorous emergency locator transmitter (ELT) system crash survivability requirements that reduce the likelihood that an ELT system will be rendered inoperative as a result of impact forces sustained during an aviation occurrence.
Transportation Safety Recommendation A16-05
4.2.3 Emergency locator transmitter first-burst delay
In this occurrence, the aircraft's ELT system was unable to transmit a signal that could be detected by the Cospas-Sarsat satellite system. The ELT system in this instance was compromised within the prescribed 50-second (± 2.5 seconds) period from activation to first transmission of a distress signal. This 50-second delay, referred to as the first-burst delay, is a Cospas-Sarsat design requirement. The first-burst delay was initially intended to allow time for one of the earlier-generation components, called an oscillator, to stabilize; but it also evolved into an opportunity to deactivate an inadvertently activated beacon before its first transmission. Modern ELT systems no longer require a period this long before being capable of transmitting a distress signal.
The TSB has investigated a large number of occurrencesFootnote 280 in which an ELT system was rendered inoperative within the first-burst delay, preventing a distress signal from reaching the Cospas-Sarsat system responsible for SAR alerting, detection, and response in Canada.
Although initially there were component-related reasons for the introduction of the 50-second first-burst delay, it is no longer necessary. However, the first-burst specification has not been updated to reflect this reality. As a result, ELT distress signals will not be received if an ELT system is compromised during the 50-second first-burst delay period.
If an ELT system is compromised (i.e., damaged or submerged) before its first-burst delay period has elapsed, it is highly likely that critical life-saving SAR services will be delayed, potentially leading to further injury or death following an aviation accident.
Therefore, the Board recommends that
Cospas-Sarsat amend the 406-megahertz emergency locator transmitter first-burst delay specifications to the lowest possible timeframe to increase the likelihood that a distress signal will be transmitted and received by search-and-rescue agencies following an occurrence.
Transportation Safety Recommendation A16-06
4.2.4 Hook-and-loop fasteners
In this occurrence, the aircraft's ELT unit was secured to its mounting tray by a strap with a hook-and-loop fastener. During the crash sequence, the ELT became dislodged from this strap, and was found hanging by the wire that connects the unit to the antenna. There have been a number of cases in which hook-and-loop fasteners have failed to retain an ELT unit in its mounting tray. In several instances, the units were compromised as a result of breaking free from the fastener, which prevented a distress signal from being transmitted to the Cospas-Sarsat search-and-rescue satellite system. The vulnerability of this type of fastener was previously identified during TSB Aviation Investigation A11W0151, and resulted in the issuance of a TSB Safety Advisory to TC and the manufacturer of the ELT. Despite the known vulnerability of hook-and-loop fasteners, they continue to be an approved means of attaching an ELT unit to an airframe.
There are a large number of ELT systems in use in Canada, and in other parts of the world, that rely on hook-and-loop fasteners to secure an aircraft's ELT to the airframe. According to the ELT manufacturer, there are approximately 2000 registered Kannad ELTs in Canada that rely on hook–and-loop fasteners. In the United States, there are more than 7000. According to the company, only 2 of those registered in Canada are fitted with a new type of non-hook-and-loop fastener in accordance with TSO-C126b.
The problems associated with hook-and-loop fasteners are well documented, and some national regulatory bodies have already taken action to address these problems. In the United States, the FAA adopted TSO-C126b, which prohibits the use of hook-and-loop fasteners for new ELT installations. However, this revised TSO is not retroactive, so these fasteners will continue to be used in the United States in existing installations for the foreseeable future. Likewise, the EASA has recently issued an NPA stating its intent to adopt ETSO-C126b, which mimics the requirements specified in TSO-C126b.
Although the TSB has identified the risk of using hook-and-loop fasteners for securing an ELT to an airframe, they are still permitted for use in Canada. In June 2015, TC issued a Preliminary Issue and Consultation Assessment (PICA) Form indicating the Department's intent to review its maintenance/installation and airworthiness standards for ELTs. According to TC, it intends to adopt TSO-C126b; like the FAA and EASA, however, it has indicated that the requirement will not be retroactive. There is no timeline for these potential changes to the maintenance/installation and airworthiness standards, nor is it certain whether the changes will be adopted in the CARs or the airworthiness standards. As a result, the risks associated with hook-and-loop fasteners will persist.
While hook-and-loop fasteners continue to be permitted for ELT installations, there is a significant risk that signals originating from these ELTs will not be transmitted due to damage associated with an ELT coming free from its mounting tray during a crash sequence. This lack of transmission could result in delays in life-saving SAR services.
Therefore, the Board recommends that
The Department of Transport prohibit the use of hook-and-loop fasteners as a means of securing an emergency locator transmitter to an airframe.
Transportation Safety Recommendation A16-07
4.2.5 Night visual flight rules regulations
In this occurrence, the pilots took off on a night VFR flight in conditions that did not permit them to safely maintain visual reference to the surface. Although the CARs indicate that night VFR requires a pilot to maintain visual reference to the surface, they do not adequately define the visual references required for compliance. For example, the regulations do not define the cultural/ambient light requirements, nor do they provide for an alternate means of compliance when this cannot be achieved. During the investigation, it was determined that many pilots who conduct night VFR operations believe that it is acceptable to do so at night, regardless of lighting conditions, as long as the reported weather conditions (i.e., ceiling and visibility) meet the minimums specified by regulation. These differences in the ways in which the regulations are being interpreted significantly increase the risk to those who travel on VFR aircraft at night. Further, there is no regulatory requirement, as there is in some countries, for commercial operators to demonstrate to TC that their night VFR routes can be reasonably carried out by relying on cultural or ambient lighting, or by alternative means such as NVGs, before they receive TC approval of their night VFR routes.
Night VFR flights are routinely conducted across Canada. In heavily populated areas, it may be easy for pilots to maintain visual reference to the surface using cultural lighting. However, flights are often conducted in remote locations of Canada, where there may be little to no cultural lighting available to help pilots maintain visual reference to the surface without some type of alternative means, such as NVGs. The risks associated with conducting night VFR operations in conditions where pilots are unable to maintain visual reference to the surface are well documented in TSB investigation reports.Footnote 281 In a TC study, the regulator identified a number of instances in which flights were conducted under the auspices of night VFR, but with inadequate cues to maintain reference to the surface.Footnote 282 Strong evidence therefore exists to suggest that the current night VFR regulations should be re-examined and amended to clearly establish the conditions required to meet the intent of the regulation. For example, in the United States, the Federal Aviation Regulations (FARs) state that no person shall operate a helicopter under VFR at night unless that person has “visual surface light reference, sufficient to safely control the helicopter.”Footnote 283
Without clearly defined night VFR requirements that establish unaided visual reference/lighting considerations or alternative means of maintaining visual reference to the surface (i.e., night-vision imaging systems), it is highly likely that accidents such as this one will continue to occur.
Therefore, the Board recommends that
The Department of Transport amend the regulations to clearly define the visual references (including lighting considerations and/or alternate means) required to reduce the risks associated with night visual flight rules flight.
Transportation Safety Recommendation A16-08
4.2.6 Instrument flight currency requirements
As seen in this occurrence, 2 pilots lacking instrument flying proficiency departed for a night VFR flight in conditions that required the use of instrument flying skills because the cultural and/or ambient lighting needed to maintain visual reference to the surface was lacking. Although both pilots had met the instrument flight currency requirements in the CARs, once the aircraft passed the end of the runway lights necessitating transition to flight by reference to instruments, an excessive bank angle and rate of descent developed, which were not recognized by the crew at an altitude that permitted recovery.
Under the current regulations, instrument-rated pilots may go up to 12 months following their instrument ride before they are required to conduct any actual or simulated instrument flying. After 12 months, the regulations require pilots to have completed 6 hours of instrument flying, including 6 instrument approaches during the previous 6 months to maintain their instrument qualification. Many of these instrument-rated pilots do not routinely conduct instrument flight training or operations to maintain a reasonable degree of instrument flying proficiency. As a result, pilots who have had little to no instrument flying experience for 12 months may legally be called upon to carry out, and may accept, a challenging instrument flight without recent practice in the skills essential to the safe conduct of an instrument flight.
As identified in TC's Instrument Procedures manual, instrument flight is a skill that requires “careful training, constant practice and a methodical approach.”Footnote 284 As for any other skill, repetition is essential to prevent erosion of a pilot's instrument flying skill. As explained above, the instrument currency requirements allow for an extended period (i.e., up to 12 months) to lapse before a pilot is required to complete any type of instrument flight. In contrast, there are a number of semi-annual currency requirements in the CARs, such as takeoffs and landings, which a pilot must complete in order to remain current for operational duty. A similar semi-annual requirement also exists for instrument flight; however, it only applies after the first 12 months following the issuing or renewal of an instrument rating. TC does not impose the 6/6/6 instrument currency requirement during the first 12 months. In the United States, FARs paragraph 61.57(c) specifies semi-annual instrument currency requirements that must be met before a pilot can act as pilot-in-command under instrument flight rules or in weather conditions less than the minimums prescribed for visual flight rules only.
The instrument recency requirements in the CARs do not provide adequate assurance that an instrument-rated pilot will possess an acceptable level of proficiency to ensure the safe conduct of a flight in challenging instrument meteorological conditions. As a result, pilots may conduct flights in challenging instrument meteorological or dark night conditions without the level of instrument flying proficiency required to maintain safe flight operations.
Therefore, the Board recommends that
The Department of Transport establish instrument currency requirements that ensure instrument flying proficiency is maintained by instrument-rated pilots, who may operate in conditions requiring instrument proficiency.
Transportation Safety Recommendation A16-09
4.2.7 Terrain awareness and warning systems for helicopters
This occurrence was a controlled flight into terrain (CFIT) accident, in which a serviceable aircraft was unintentionally flown into the ground. While attempting to conduct a night visual departure in extremely dark conditions, an inadvertent descent developed, and the aircraft struck the terrain. When the flight crew recognized that an inadvertent descent had developed, they were at an altitude from which they were unable to recover. Although some aircraft of the operator's S-76A fleet were equipped with a terrain awareness and warning system (TAWS), the occurrence aircraft was not, and was not required by regulation to be equipped with one. As a result, the flight crew did not receive a timely warning of the inadvertent descent or the impending impact.
A large number of commercial helicopters routinely conduct flight operations at night or in instrument meteorological conditions (IMC), or both. Without the benefit of TAWS, such aircraft are at significantly greater risk for CFIT. The TSB has investigated a number of helicopter occurrences that took place at night or in IMC where TAWS may have proven useful in preventing an accident.Footnote 285
In Canada, commercially operated aeroplanes and some privately operated aeroplanes are required by regulation to be equipped with TAWS. However, there is no regulatory requirement for commercial helicopters to be equipped with TAWS, despite the fact that they often operate along similar routes as commercial fixed-wing aircraft, and sometimes carry larger numbers of passengers. As a result, the regulations do not currently provide for an equivalent level of safety between commercial fixed-wing versus commercial rotary-wing operations.
Until there is a requirement for Canadian-registered commercial helicopters to be equipped with TAWS, the crew members and passengers who travel on those aircraft at night or in IMC will continue to be at increased risk for injury or death due to CFIT.
Therefore, the Board recommends that
The Department of Transport require terrain awareness and warning systems for commercial helicopters that operate at night or in instrument meteorological conditions.
Transportation Safety Recommendation A16-10
4.2.8 Pilot proficiency check standards
In this occurrence, the captain's pilot proficiency check (PPC) was conducted, based on the approved check pilot's (ACP) belief that, rather than assuming pilot-in-command (PIC) duties immediately, he would be employed as a first officer until he gained some recent operational experience in the air ambulance role. Although the ACP selected “first officer” on the captain's PPC form, the company assigned the occurrence captain to carry out PIC duties in a very demanding role and from a very challenging remote location. In this instance, the only recourse for the ACP would have been to assess the occurrence captain's PPC as a fail. There is currently no way for an ACP to restrict a pilot to second-in-command (SIC) duties based on the ACP's assessment that the pilot is not ready to act in a PIC capacity, potentially as captain of a multi-engine, multi-crew aircraft responsible for the safe completion of demanding night or IFR flights, or both.
The current PPC standards, and associated PPC schedules, for CARs Subpart 702, 703, 704, and 705 operators make little distinction between the respective PPCs conducted on captains versus first officers. The aeroplane PPC schedules for Subparts 702, 703, 704, and 705 identify that it may not be possible to conduct some taxi checks from the SIC position. Those for Subparts 704 and 705 also identify differing engine-out landing requirements for the PIC versus for the SIC. For helicopter pilots, the PPC schedules for Subparts 702, 703, and 704 note only that pilots occupying the SIC position may not be able to complete all of the taxi checks identified in the PPC schedule. With the exception of these small variances, both aeroplane and helicopter pilots are required to meet the same performance standards, as per their respective subpart, regardless of whether they will be assigned to captain or first officer duties following the PPC. There is no requirement for captains to demonstrate a higher degree of proficiency, commensurate with their increased responsibilities.
In addition, the PPC standards do not take into account the unique challenges associated with the potential for acting as captain of a multi-engine, multi-crew aircraft in demanding IFR or night flight conditions, or both. Therefore, despite the considerable difference in responsibilities between a captain and first officer, both pilots are tested to the same standard, which allows up to 4 major deviations from the qualification standards. A major deviation may be assessed when “aircraft handling is performed with limited proficiency”Footnote 286 or when “technical skills and knowledge reveal limited technical proficiency and/or depth of knowledge”.Footnote 287 Once a pilot passes a PPC on a particular aircraft type, that PPC is transportable if the pilot moves to a different company that operates that same aircraft type.
Currently, the risk associated with employing a pilot as a captain is managed through internal company policies and insurance or contractor requirements. However, in many cases, companies rely on the regulations to determine the minimum requirements for employment in a PIC position. As seen in this occurrence, Ornge RW was aware that the captain had encountered problems during the PPC and that “first officer” had been selected on the PPC form. However, since there is only one PPC standard for Subpart 703 helicopter pilots, and based on the company's assessment of his experience, Ornge RW elected to employ the occurrence captain as a PIC without any additional training or supervision. As a result, on the night of the occurrence, the captain was not adequately prepared to carry out his duties.
In other jurisdictions, this issue has been recognized. For example, in the United States, Title 14 of the Code of Federal Regulations, Section 61.58, specifies that a pilot must complete a PIC proficiency check in order “to serve as pilot in command of an aircraft that is type certificated for more than one required pilot flight crewmember or is turbojet-powered”.Footnote 288 A pilot who will be acting as SIC (i.e., first officer) is not required to complete the same PIC proficiency check. Instead, there are less stringent requirements outlined in the FARs that must be met for a pilot to be permitted to act as SIC aboard an aircraft type certificated for more than one required pilot flight crew member. There is no such distinction in Canada for crew members who will be filling an SIC position.
The current PPC standards do not ensure that captains possess an adequate level of proficiency to safely carry out the operational duties of a PIC. As a result, there is a risk that Subpart 702, 703, 704, and 705 pilots will continue to be assigned to PIC duties without having first demonstrated an adequate degree of proficiency in a captain capacity.
Therefore, the Board recommends that
The Department of Transport establish pilot proficiency check standards that distinguish between, and assess the competencies required to perform, the differing operational duties and responsibilities of pilot-in-command versus second-in-command.
Transportation Safety Recommendation A16-11
4.2.9 Oversight of commercial aviation in Canada
Transportation companies have a responsibility to manage safety risks in their operations. Compliance with regulations can only provide a baseline level of safety for all operators in a given sector. Since regulatory requirements cannot address all risks associated with a specific operation, companies need to be able to identify and address the hazards specific to their operation.
In the traditional oversight model, companies are not required to have formalized systems in place to continuously manage safety at a systems level. Oversight is accomplished using an inspect-and-fix approach. In this approach, the regulator's role is focused on finding instances of regulatory non-compliance, which the operator must correct. The impact on safety of this approach is limited for 2 main reasons.
First, it is not possible for the regulator to examine continuously all aspects of an operation. Challenges in detecting non-conformances have been identified in a number of previous TSB investigations (e.g. A12W0031, A12C0154, and A13W0120). For example, in A13W0120, although TC had assessed the operator involved as high risk, and was conducting frequent surveillance activities, the focus had not shifted to verifying regulatory compliance, and remained at a systems level. As a result, TC's surveillance did not identify the unsafe operating practices that contributed to the severity of the occurrence.
Secondly, if the systemic causes of non-conformance are not identified and addressed, it is likely that unsafe conditions will persist. The TSB has also previously identified this pattern in a number of investigations (e.g. A10Q0098, A10Q0117, and A13H0002). For example, in A13H0002, the report identified weaknesses in the oversight of an operator with a transitioning safety management system (SMS). In this case, the operator experienced difficulty producing acceptable CAPs and meeting its proposed implementation time frames. This resulted in repeated delays in addressing deficiencies. During this period, TC postponed any additional surveillance activities pending CAP implementation. The suspension of surveillance activities while waiting for the CAP process to run its course effectively reduced the frequency of oversight for an operator that was considered high risk and left the operator with less than the planned level of oversight for an extended period.
When implemented properly, SMS provide a framework for companies to effectively manage risk and make operations safer. Regulatory requirements for companies to implement SMS are the first step in ensuring that all operators are capable of meeting their safety responsibility. It is for this reason that the TSB has echoed calls from ICAO and the worldwide civil aviation industry emphasizing the advantages of SMS.
Still, even with SMS requirements, companies will vary in degrees of ability or commitment to effectively manage risk. Less frequent surveillance, focused on an operator's safety management processes, will be sufficient for some companies. However, the regulator must be able to vary the type, frequency, and focus of its surveillance activities to provide effective oversight to companies that are unwilling or unable to meet regulatory requirements or effectively manage risk. Further, the regulator must be able to take appropriate enforcement action in these cases.
Operators with a mature, effective SMS, along with a corresponding safety culture and abilities, may be the subject of less-frequent, systems-level oversight. In contrast, companies that have not demonstrated the capability to effectively manage risks at a systems level should be subject to more frequent surveillance, with a greater emphasis on ensuring compliance with regulations. As an operator's systems mature and become more effective, the frequency of oversight may be reduced and the balance of oversight can shift from the compliance-based model to more systems-level surveillance activities.
In the investigation of the Ornge RW accident at Moosonee, Ontario, the TSB found that TC's approach to surveillance activities did not lead to the timely rectification of non-conformances. It also found that TC inspectors believed that tools other than a corrective action plan to guide the operator back into compliance were either unavailable or inappropriate for use with a willing operator. As a result, the operator's willingness to address surveillance findings superseded concerns about the operator's capability to address the deficiencies in post-surveillance decision making. In addition, the investigation found that the training and guidance that was provided to TC inspectors contributed to uncertainty, which led to inconsistent and ineffective surveillance of Ornge. Ultimately, although TC was conducting frequent and detailed surveillance, the approach to returning the operator to a state of compliance was not well matched to the capabilities of the operator.
The investigation also noted that although TC was relying heavily on the CAP process, the operator was not required to have an SMS and, as a result, had not demonstrated to TC that it had the processes in place to effectively manage safety.
The TSB has previously identified these issues; safety management and oversight is a multi-modal item on the TSB Watchlist, which identifies those issues posing the greatest risk to Canada's transportation system. The Watchlist proposes the following solutions in this area:
- TC must implement regulations requiring all air operators to have formal safety management processes, and TC must oversee these processes.
- Companies that do have SMS must, in turn, demonstrate that it is working—that hazards are being identified and effective risk mitigation measures are being implemented.
- Finally, when companies are unable to effectively manage safety, TC must not only intervene, but do so in a manner that succeeds in changing unsafe operating practices.
The investigation into this accident and other recent occurrences emphasize the need for operators to be able to effectively manage safety. More than 10 years after introducing the first SMS regulations for airline operators and the companies that perform maintenance on their aircraft, SMS implementation has stalled. While many companies, such as Ornge RW, have recognized the benefits of SMS and voluntarily begun implementing it within their organizations, approximately 90% of all Canadian aviation certificate holders are still not required by regulation to have an SMS. As a result, TC does not have assurance that these operators are able to effectively manage safety.
Therefore, the Board recommends that
The Department of Transport require all commercial aviation operators in Canada to implement a formal safety management system.
Transportation Safety Recommendation A16-12
and that
The Department of Transport conduct regular SMS assessments to evaluate the capability of operators to effectively manage safety.
Transportation Safety Recommendation A16-13
This, and other investigations have also highlighted the need for TC to adapt its approach to regulatory oversight to the competence of the operator. The documentation provided to TC inspectors evolved considerably in the time period covered by this investigation, and TC continues to provide new training to its inspectors as outlined in the Safety action taken section of this report.
However, recent investigations have highlighted the fact that, when faced with an operator that is unable or unwilling to address identified safety deficiencies, TC has difficulty adapting its approach to ensure that deficiencies are effectively identified and that they are addressed in a timely manner.
TC's risk-based approach to surveillance planning resulted in the operators, which were all viewed as higher risk, being scheduled for more frequent surveillance. However, in A13W0120, unsafe conditions remained unidentified when the surveillance remained focused on processes. In other occurrences, unsafe conditions were allowed to persist for an extended period while TC relied heavily on a CAP process, in which the operators were ill-equipped to participate.
Therefore, to ensure that companies use their SMS effectively, and to ensure that companies continue operating in compliance with regulations, the Board also recommends that
The Department of Transport enhance its oversight policies, procedures and training to ensure the frequency and focus of surveillance, as well as post-surveillance oversight activities, including enforcement, are commensurate with the capability of the operator to effectively manage risk.
Transportation Safety Recommendation A16-14
This report concludes the Transportation Safety Board's investigation into this occurrence. the Board authorized the release of this report on . It was officially released on .
Correction
The report has been amended to reflect new information provided to the Transportation Safety Board after the report's initial release.
The Board has amended Sections 1.17.1 and 1.17.2 of the report as follows:
Section 1.17.1
Removed the last 2 sentences of the second paragraph that read
According to Ornge, the previous operator had determined which of the S-76A airframes were removed from service upon delivery of the AW139s. Ornge was not involved in the decision to remove certain airframes from service, but assumed that the removals were based on remaining component life.
Section 1.17.2
Added the following 2 new sentences at the beginning of the fifth paragraph:
In the months leading up to September 2010, when the transition from the previous operator to Ornge RW began, the previous operator had recommended, based on installed safety features, the order in which S-76A aircraft should be removed from service upon delivery of the AW139s. However, when the AW139 implementation was delayed, some S-76A helicopters, including the occurrence aircraft, were left in service at their regular operating bases rather than being retired in the recommended order.
Section 1.18.2.2
Removed the fourth, fifth, sixth and seventh sentences of the third paragraph that read
In other instances, pilots experienced technical problems with the simulator that sometimes required the simulator to be restarted, or to be repaired by a technician. In at least one case, technical difficulties required a crew pairing to be scheduled for multiple double sessions in an attempt to meet the scheduled PPC time. Ultimately, that crew refused to participate in a second double session because it would not have provided them adequate time to sleep and prepare for their PPC, which was scheduled for the next day. This resulted in their PPCs being delayed.
These changes were made in the interest of accuracy and completeness, and do not affect the Analysis, Findings, or Safety action sections of the report.
This correction was approved by the Board on and the corrected version of the report was released on .
Appendices
Appendix A – Ornge Rotor-Wing S-76 aircraft differences
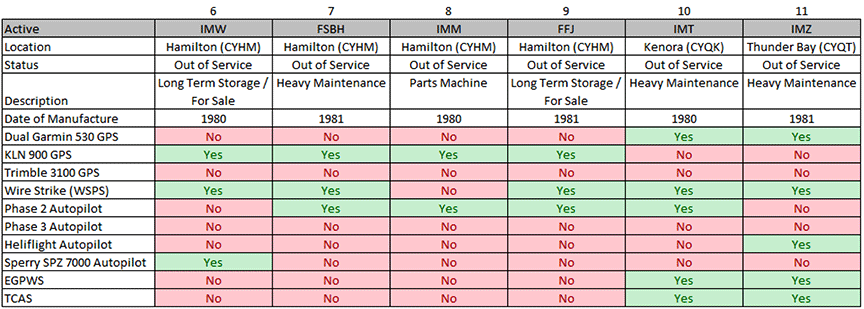
Appendix B – Safety communications related to hook-and-loop fasteners on emergency locator transmitter installations
On 19 April 2012, the TSB issued Safety Advisory 825-A11W0151-D1-A1: Loose Attachment of Kannad 406 AF-Compact (ER) ELT. The advisory stated that Transport Canada (TC) may wish to inform owners, operators, and maintainers of aircraft with emergency locator transmitters (ELT) featuring fabric hook-and-loop retention systems of the necessity to ensure adequate retention of the ELT in the event of an accident. The TSB issued a similar Safety Advisory(825-A11W0151-D1-A2) on 19 April 2012 to ELT manufacturers using hook-and-loop retention systems, advising that they may wish to develop and publish methods for determining degree of strap tightness and to inform maintenance personnel of the necessity of proper installation.
In addition to the safety advisories produced by the TSB, the United States National Transportation Safety Board (NTSB) had issued Safety Recommendations A-10-169 and A-10-170 in January 2011, which recommended that the Federal Aviation Administration (FAA):
Require a detailed inspection, during annual inspections, of all emergency locator transmitters installed in general aviation aircraft to ensure that the emergency locator transmitters are mounted and retained in accordance with the manufacturer's specifications. (A-10-169)
Determine if the emergency locator transmitter (ELT) mounting requirements and retention tests specified by Technical Standard Order (TSO) C91a and TSO C126 are adequate to assess retention capabilities in ELT designs. Based on the results of this determination, revise, as necessary, TSO requirements to ensure proper retention of ELTs during airplane accidents. (A-10-170)Footnote 289
On 23 May 2012, the FAA issued Special Airworthiness Information Bulletin (SAIB) HQ-12-32. The purpose of the SAIB was to inform ELT manufacturers, installers, and aircraft maintenance personnel of concern regarding the capability of hook-and-loop style fasteners to restrain an ELT during an accident impact. The bulletin cited several examples of these types of fasteners failing, in many cases causing wires to be severed and rendering the ELT ineffective. The SAIB recommended to ELT manufacturers previously using hook-and-loop fasteners for ELT retention that the following information be included in manufacturers' instructions for continued airworthiness:
- Instructions for properly securing the ELT during installation and reinstallation as well as a method to determine the appropriate tension of the hook and loop style fasteners.
- Instructions for inspecting hook and loop style fasteners for wear, contamination, environmental degradation, or other effects to ensure they will continue to meet the requirements in the applicable TSO. Incorporating this inspection with the inspection required by 14 Code of Federal Regulations (CFR) Part 91.207 is appropriate.
- Replacement interval for the hook and loop style fasteners.Footnote 290
In response to SAIB HQ-12-32, Kannad Aviation issued Service Bulletin (SB) S1800000-25-00, which provided detailed guidance on how to properly secure an ELT using the hook-and-loop style of fasteners. However, SBs are not mandatory. Compliance is strictly voluntary, and it is therefore up to each company whether or not it chooses to comply. The SB placed particular emphasis on ensuring proper tightening, cautioning that incorrect tightening could prevent the transmission of a distress message by the ELT. The SB also recommended that visual inspections of the hook-and-loop style of fasteners be performed at each installation or reinstallation of the ELT and during periodic inspections required by national authorities.
On 11 February 2013, Kannad Aviation issued Safety Letter (SL) S1840501-25-05 (Revision 01), titled Kannad 406 AF-Compact, Kannad 406 AF-Compact (ER) Integra ELTs Family: Guidelines for Periodic Inspection. On 19 February 2013, Kannad Aviation issued SL18XX502-25-12 (Revision 02), titled Kannad 406 ELTs: Guidelines for Periodic Inspection. These documents describe usual operations for periodic checks required by major aviation authorities.
On 13 February 2013, the European Aviation Safety Agency (EASA) issued Safety Information Bulletin (SIB) 2013-04, which echoed FAA SAIB HQ-12-32. EASA's SIB indicated that EASA planned to update European Technical Standard Order (ETSO) C126a to reflect the changes made to TSO-C126b. At the time of report writing, ETSO C126a was still in effect.
As a result of TSB Aviation Investigation Report A11W0151, TC published an article in Aviation Safety Letter Issue 2/2013 specifically addressing the issue of retaining straps made from hook-and-loop fabric and the need to ensure that they are adequately tightened.
Appendix C – Potential options for improving crashworthiness of emergency locator transmitters
One of the options examined as a means of improving emergency locator transmitter (ELT) crashworthiness involved determining whether or not it would be possible to design a low-profile ELT antenna, similar to ones used for satellite telephone and global positioning system (GPS) installations. However, because certain ELTs transmit on 121.5 MHz, 243.0 MHz, and 406 MHz, some design limitations exist, related to radiation patterns and signal strength. The 121.5 MHz and 243.0 MHz frequencies require a vertical polarization, which would make a flush-mounted, low-profile antenna impossible. As with a satellite phone and GPS, a low-profile antenna would be possible if only 406 MHz were used for the ELT. Another possibility might be to use a dual antenna installation, whereby there would be a conventional blade or whip antenna for the 121.5 MHz and 243.0 MHz signals and a low-profile antenna for the 406 MHz signal.
The manufacturer of the occurrence ELT has taken steps to address the issue of redundancy in ELT design by developing a new family of ELTs, approved by Industry Canada, that are equipped with an internal integral antenna. If the unit detects a low standing-wave ratio due to a lost connection with the external antenna, the ELT automatically switches to the internal 406 MHz antenna. The design is intended to prevent distress signals failing to reach the Cospas-Sarsat system in the event of a broken antenna. This ELT is also fitted with an internal GPS receiver and antenna, to provide positional information and a 121.5 MHz emitter for radio guidance in the final phase of rescue operations. The internal antenna has been designed to meet the specifications of Radio Technical Commission for Aeronautics (RTCA) RTCA/DO-204A and European Organisation for Civil Aviation Equipment (EUROCAE) document ED62A. However, the internal antenna has not been tested and approved by Cospas-Sarsat, whose standard does not include details on the design's radiation and power output. Finally, depending on the location of the ELT unit, the signal from an ELT using an internal antenna may be emitted at a reduced effectiveness due to shielding from aircraft components or terrain.
Appendix D – SUR-001 Issue 04 assessment and process validation inspection finding classifications
According to SUR-001 Issue 04, process validation inspection findings are classified using the following criteria:
(a) Minor — A finding is considered minor where a surveillance activity has identified that a component and/or element has been maintained and demonstrated effective, but where the component or element requires administrative enhancement to existing areas (for example, formatting issues).
(b) Moderate — A finding is considered moderate where a surveillance activity has identified that a component and/or element has not been fully maintained and non-conformance findings indicate that the component is not fully effective, but where the certificate holder has clearly demonstrated the ability to carry out the activity required by the component/element and a simple modification to their process is likely to correct the issue.
(c) Major — A finding is considered major where a surveillance activity has identified examples that the component and/or element has not been established, maintained and adhered to or is not effective, and a systemic failure is evident. A major finding will typically require a more rigorous and lengthy corrective action plan (CAP) than a minor or moderate finding. A notice of suspension (NoS) with a 30 day notice period and Enhanced Monitoring should be considered.
[…]
(d) Critical — Where a finding resulting from a surveillance activity identifies that a component has not been implemented or is wholly ineffective (i.e. scored as a level (1) a Notice of Suspension (NoS) with immediate effectivity is appropriate in accordance with Section 7.1 (a) of the Aeronautics Act. A lack of a maintained and effective SMS in accordance with the applicable CAR reference would be cited as grounds for suspension. For an assessment, the NoS is issued as a failure to meet Section 107.02 of the CARs and the appropriate paragraphs of Section 107.03 of the CARs and the parts and subparts relevant to the Certificate holder being reviewed. For a PVI [program validation inspection], the NoS is issued as a failure to meet the parts and subparts relevant to the Certificate holder being reviewed.Footnote 291
Appendix E – SUR-001 Issue 04 scoring levels
According to SUR-001 Issue 04, scores are assigned based on the following criteria:
- A score of 1; the element is not documented and/or implemented, or it is completely ineffective;
- A score of 2; the element is partially implemented but may not be fully effective […];
- A score of 3; the element meets the regulatory requirements;
- A score of 4; the element exceeds the regulatory requirements […]; and
- A score of 5; the element meets all the criteria for an award level of 3 plus all of the additional requirements listed under the criteria for that element […].Footnote 292
According to SUR-001 Issue 04, “where any component is assessed at an award level of 1 a Notice of Suspension (NoS) shall be issued.”Footnote 293 The document states that the associated NoS may have an immediate effective date. If a component is assessed “at an award level of 2 and interpretation of the findings indicate major issues … the convening authority will decide the appropriate course of action, which may include the issuance of an NOS and Enhanced Monitoring.”Footnote 294
Appendix F – Corrective action plan timelines for January 2013 program validation inspection
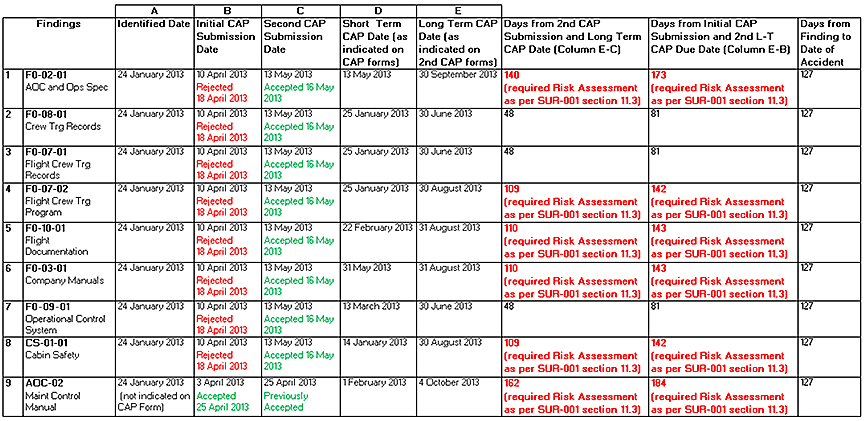
Appendix G – Recent advances in night-vision goggles
According to Transport Canada, current generation (GEN III) night-vision goggles (NVG) have several distinct advantages over the previous GEN II and GEN I NVGs; they automatically adjust to ambient conditions, from overcast starlight to dusk and dawn, and have significantly better low-light performance. To put this advancement in perspective, GEN III NVGs are capable of operating in light conditions 100 times lower than with GEN II NVGs and 1000 times lower than with GEN I NVGsFootnote 295 (see figure below).



In addition to the general advancements associated with GEN III NVGs, some companies are now producing NVG heads-up displays, which project critical flight and navigation information on the image displayed in the NVGs, greatly reducing pilots' heads-down time in the cockpit (see figure below). Increased heads-up time enables pilots to maintain a better visual scan of their surroundings, which results in a greater level of situational awareness and an increased level of safety.Footnote 296

Appendix H – Pros and cons of night-vision goggles
Although there are some challenges associated with night-vision goggles (NVG) operations, it is widely accepted that NVGs significantly reduce the risks associated with night visual flight rules (VFR) operations—particularly the risk of controlled flight into terrain (CFIT). The most notable benefit of NVGs is that they can drastically improve visual acuity at night, bringing it almost to daytime levels; 20/30 acuity or better is easily achievable with properly focused NVGs. According to Transport Canada (TC), this increased visual acuity at night assists with spatial awareness and helps improve situational awareness.Footnote 297
In a large survey conducted by the National EMS Pilots Association (NEMSPA),Footnote 298 participants were asked a series of questions related to their experience with NVGs and asked for their thoughts on the technology as a means of enhancing flight safety. NEMSPA determined that 85% of the pilots surveyed felt strongly that NVGs improved the safety of night helicopter emergency medical services (HEMS) operations.Footnote 299 The comments received by participants included the following:
“NVG's are the most significant improvement in night EMS [emergency medical services] history.”
“The ability of the NVG's to enhance the night is remarkable […]”
“I feel night vision goggles have improved the safety in our program more than any other thing I have seen in 17 years of EMS flying.”
“Landing in unimproved areas at night is dangerous. Landing in unimproved areas at night without NVGs is idiotic!”
“The use of NVG's has been the single most significant safety improvement in helicopter night flying operations I have seen during 41 years (18 000 hours) as a helicopter pilot.”
“Do not ever want to fly at night without them.”
Similar sentiments have been expressed publicly by members of TC's Flight Standards division. In an article for Canadian Skies, the Project Officer for Night Vision Imaging Systems Regulation Development within the Flight Standards division was quoted as saying, regarding NVGs, “My personal goal is that in a few years it would actually do away with unaided night VFR in areas with very little cultural lighting.”Footnote 300
Although a number of pilots at Ornge RW had no operational experience with NVGs at the time of the accident, the investigation showed that the vast majority of company pilots were strongly in favour of NVGs, particularly for the northern bases, because of the lack of cultural lighting in these areas to help pilots maintain visual reference to the surface during night VFR flights.
In its survey report, NEMSPA noted that the strongest resistance to use of NVGs for EMS had come from pilots and Federal Aviation Administration (FAA) inspectors with little to no experience flying with NVGs. On the other hand, some parties with vast NVG experience have gone so far as to assert that NVGs are more valuable in the fight against CFIT than helicopter terrain awareness and warning systems (HTAWS). The reason is that HTAWS warn the pilots of hazards that they cannot see, while NVGs allow pilots to see, identify, and avoid hazards in much the same way that pilots would do during the daytime when they are able to see outside.Footnote 301
Despite the widely recognized benefits of NVGs, they have some limitations that must be considered by companies contemplating adoption of NVGs into their night VFR operations. One of the more significant of these is that NVGs have a very restrictive field of view (approximately 40 degrees). This restriction makes it necessary for pilots to move their heads a great deal more than they would normally be required to do, since they lack the benefit of the peripheral vision afforded them during the daytime. NVGs can also partially obstruct a pilot's vision, making it harder to see some of the instruments in the cockpit, and NVG operations can be more fatiguing, especially if the goggles are not properly focused. Other issues related to NVG limitations may make it harder to detect certain land features due to terrain masking, and both depth perception and judgement of closing rates can be more difficult without proper training.
In addition to the limitations noted above, it is important to consider that under the current regulations, the night currency requirements can be met while operating using NVGs. As a result, it is possible that unaided night-flying proficiency will be degraded if pilots rely solely on NVGs to meet night currency requirements. Despite these limitations, there is overwhelming agreement among rotor-wing pilots that NVGs provide an increased margin of safety when conducting night VFR operations.
Appendix I – Helicopter emergency medical services in the United States
In 2006, the United States National Transportation Safety Board (NTSB) published its Special Investigation Report on Emergency Medical Services Operations. The report stated that the NTSB had studied 55 accidents between January 2002 and January 2005 and found that, in 13 of them, use of night-vision imaging systems (NVIS) might have prevented the accident by helping the pilots clearly see oncoming obstacles and take evasive action in a timely manner.Footnote 302 The NTSB did not issue a recommendation at that time because “NVIS was not feasible in some situations, such as populated areas with ambient light and numerous streetlights. Additionally, the costs, availability, and FAA [Federal Aviation Administration] certification policies and manpower were not mature enough to warrant a reasonable recommendation.”Footnote 303 In closing, the NTSB indicated that it would closely monitor the FAA's involvement in promoting use of night-vision goggles (NVG).Footnote 304
While the NTSB did not issue a formal NVIS recommendation in 2006, it did issue several safety recommendations to the FAA. These recommendations, along with the FAA's responses, are outlined below.
Recommendation A-06-12: Require all emergency medical services operators to comply with 14 Code of Federal Regulations Part 135 operationsFootnote 305 specifications during the conduct of all flights with medical personnel on board.Footnote 306
In response to Recommendation A-06-12, the FAA proposed a revision to 14 Code of Federal Regulations (CFR) Part 135 to define helicopter air ambulance operations as those conducted by a Part 135 certificate holder. This revision came into effect on 21 February 2014. As a result, the FAA's response was classified by the NTSB as Closed—Acceptable Action.
Recommendation A-06-13: Require all EMS [emergency medical services] operators to develop and implement flight risk evaluation programs that include training all employees involved in the operation, procedures that support the systematic evaluation of flight risks, and consultation with others trained in EMS flight operations if the risks reach a predefined level.Footnote 307
In response to Recommendation A-06-13, the FAA proposed a revision to 14 CFR Part 135 to require an FAA-approved procedure for conducting pre-flight risk analyses when helicopter air ambulance operations are being conducted. This regulation came into effect on 21 February 2014. As a result, the FAA's response was classified by the NTSB as Closed—Acceptable Action.
Recommendation A-06-14: Require EMS operators to use formalized dispatch and flight-following procedures that include up-to-date weather information and assistance in flight risk assessment decisions.Footnote 308
In response to Recommendation A-06-14, the FAA proposed revisions to 14 CFR Part 135 to mandate creation of an Operations Control Center (OCC) and use of operations control specialists for helicopter air ambulance operations with 10 or more helicopter air ambulances. These regulations came into effect on 21 February 2014. As a result, the FAA's response was classified by the NTSB as Closed—Acceptable Alternate Action.
Recommendation A-06-15: Require EMS operators to install TAWS [terrain awareness and warning systems] on their aircraft and to provide adequate training to ensure that flight crews are capable of using the systems to safely conduct EMS operations.Footnote 309
In response to Recommendation A-06-15, the FAA has proposed a revision to 14 CFR Part 135 mandating the use of helicopter TAWS in helicopter air ambulance operations. This regulation came into effect on 21 February 2014. As a result, the FAA's response was classified by the NTSB as Closed—Acceptable Action.
In October 2008, the NTSB added helicopter emergency medical services (HEMS) to its Most Wanted List,Footnote 310 identifying it as one of the areas where critical changes were needed to reduce transportation accidents and save lives. Then in February 2009, the NTSB held public hearings on HEMS. As a result of these hearings, the NTSB issued 19 safety recommendationsFootnote 311 related to pilot training, aircraft equipment, airspace infrastructure, Centers for Medicare and Medicaid Services reimbursement, and HEMS utilization criteria. Some of the recommendations aimed at the FAA, particularly relevant to this occurrence, are listed below.
Recommendation A-09-87: Develop criteria for scenario-based HEMS pilot training that includes inadvertent flight into IMC [instrument meteorological conditions] and hazards unique to HEMS operations, and determine how frequently this training is required to ensure proficiency.Footnote 312
In response to Recommendation A-09-87, the FAA has proposed a number of revisions to 14 CFR Part 91, some of which overlap previous NTSB recommendations. However, since those proposed changes did not include developing criteria for scenario-based HEMS pilot training that includes inadvertent flight into IMC and hazards unique to HEMS, nor was a training frequency identified, the FAA's response was classifed by the NTSB as Closed—Unacceptable Action.
Recommendation A-09-88: Once the actions recommended in Safety Recommendation A-09-87 are completed, require HEMS pilots to undergo periodic FAA-approved scenario-based simulator training, including training that makes use of simulators or flight training devices.Footnote 313
Since the FAA did not take the action recommended in NTSB Safety Recommendation A-09-87, the FAA's response was classified by the NTSB as Closed—Unacceptable Action.
Recommendation A-09-89: Require helicopter emergency medical services operators to implement a SMS [safety management system] program that includes sound risk management practices.Footnote 314
The FAA did not adopt this recommendation, and therefore, the FAA's response was classifed by the NTSB as Closed—Unacceptable Action.
Recommendation A-09-90: Require HEMS operators to install flight data recording (FDR) devices and establish a structured flight data monitoring (FDM) program that reviews all available data sources to identify deviations from established norms and procedures and other potential safety issues.Footnote 315
In its response, the FAA indicated that it was seeking comments on the potential use of lightweight aircraft recording systems (LARS) in the HEMS industry. The FAA also indicated that it was considering making it a requirement to install LARS on all HEMS aircraft regardless of passenger seating capacity or number of pilots, unless a certificate holder can demonstrate that a cockpit voice recorder (CVR) or flight data recorder (FDR) could be used to comply with the requirements. Since this change has not yet come into effect, the FAA's response was classified by the NTSB as Open—Acceptable Response.
Recommendation A-09-95: Require HEMS operators to install NVIS and require pilots to be trained in their use during night operations.Footnote 316
Since the FAA has not introduced any proposed regulations, nor have any regulations been approved, to address Recommendation A-09-95, the FAA's response was classified by the NTSB as Closed—Unacceptable Action.
Recommendation A-09-96: Require helicopters that are used in EMS transportation to be equipped with autopilots and that the pilots be trained to use the autopilot if a second pilot is not available.Footnote 317
The FAA has not introduced any proposed regulations, nor have any regulations been approved, to address Recommendation A-09-96. Therefore, the FAA's response was classified by the NTSB as Closed—Unacceptable Action.
In October 2010, the FAA issued a fact sheet titled FAA Initiatives to Improve Helicopter Air Ambulance Safety, in which it addressed some of the issues identified in the NTSB recommendations mentioned above. In particular, the fact sheet highlighted the need for better training for night operations and response to inadvertent flight into deteriorating weather. It also promoted the use of new technologies such as NVGs, TAWS, and radio altimeters. Despite these developments, all but one of the responses to the 2009 NTSB recommendations mentioned above are currently assessed by the NTSB as Unacceptable Action. As a result, the associated safety deficiencies remain a threat, according to the NTSB. Notably, the NTSB also issued the 2009 recommendations discussed above to 40 public HEMS operators. The vast majority of responses to each recommendation from those 40 operators have been assessed as either Acceptable Response, Acceptable Action, or Exceeds Recommended Action.
As alluded to earlier, there have been some recent regulatory changes in the United States that are pertinent to this investigation. On 21 February 2014, the FAA published new regulations for helicopter air ambulance, commercial helicopter, and Part 91 helicopter operations.Footnote 318 The changes, which became effective 22 April 2014, address the causes behind 62 helicopter air ambulance accidents that occurred in the United States from 1991 to 2010 and that resulted in the deaths of 125 people. According to the Federal Register, there were 4 common factors in these accidents:
- Inadvertent flight into IMC
- Loss of control
- Controlled flight into terrain
- Night conditions.
In a similar study, TC reviewed medevac accidents that occurred between 1977 and 1997. During that period, there were a total of 54 accidents and 6 incidents related to medevac operations. The study determined that “the greatest potential for reduction of MEDEVAC fatalities lies in the reduction of controlled flight into terrain (CFIT), particularly during hours of darkness.”Footnote 319 It also concluded that “most of the mishaps occurred in uncontrolled airspace, often with no radar coverage, and at night, usually in dark night conditions.”Footnote 320
The major changes associated with the FAA revisions are summarized as follows:
- Helicopter air ambulance flights with medical personnel on board shall be conducted under Part 135, which is equivalent to CARs Subpart 704in Canada.
- Helicopter air ambulance operations that consist of 10 or more helicopter air ambulances must establish an OCC.
- Helicopters operated for the purpose of air ambulance must be equipped with a helicopter TAWS system.
- Helicopter air ambulances must be equipped with an FDM (flight data monitoring) system.
- Helicopter air ambulance operators must establish and document an FAA-approved pre-flight risk analysis process.
Despite the fact that the FAA has declared its support for NVGs in HEMS, and despite the overwhelming support for NVGs within the United States HEMS industry, the FAA did not put forward new regulations requiring night HEMS to be conducted using NVIS. In its Notice of Proposed Rulemaking, the FAA indicated that it had considered allowing NVGs as an alternate method of compliance for the helicopter TAWS (HTAWS) requirement, but ultimately decided that NVGs may not be appropriate for all operations and that further research would be required to determine whether NVGs were a suitable replacement for HTAWS. According to the Federal Register, which documents submitted opinions from industry stakeholders, several operators were of the opinion that NVGs should be mandated in lieu of HTAWS, while other operators believed that both NVGs and HTAWS should be required given that the systems complement each other.
Appendix J – Glossary
- AC
- advisory circular
- ACP
- approved check pilot
- ADO
- Associate Director, Operations
- AE
- Accountable Executive
- AF
- automatic fixed
- AFCS
- automatic flight control system
- agl
- above ground level
- AMRM
- aeromedical resource management
- AOC
- air operator certificate
- AP
- automatic portable
- asl
- above sea level
- ASR
- aviation safety report
- ATPL
- Airline Transport Pilot Licence
- ATSB
- Australian Transport Safety Bureau
- AvAIO
- Aviation All In One (software)
- AWM
- Airworthiness Manual
- AWOS
- automated weather observation system
- CAAP
- Civil Aviation Advisory Publication
- CAD
- Canadian aviation document
- CADORS
- Civil Aviation Daily Occurrence Reporting System (Transport Canada)
- CAP
- corrective action plan
- CARs
- Canadian Aviation Regulations
- CARAC
- Canadian Aviation Regulation Advisory Council
- CASS
- Commercial Air Service Standards
- CFIT
- controlled flight into terrain
- CFR
- Code of Federal Regulations
- CMCC
- Canadian Mission Control Centre
- COM
- Company Operations Manual
- COO
- Chief Operating Officer
- CP
- Chief Pilot
- CRM
- crew resource management
- CTAISB
- Canadian Transportation Accident Investigation and Safety Board
- CVR
- cockpit voice recorder
- CYMO
- Moosonee Airport
- DFO
- Director of Flight Operations
- DGCA
- Director General of Civil Aviation
- DRDC
- Defence Research and Development Canada
- EASA
- European Aviation Safety Agency
- EGPWS
- enhanced ground proximity warning system
- ELT
- emergency locator transmitter
- EM
- enhanced monitoring
- EMS
- emergency medical services
- EUROCAE
- European Organisation for Civil Aviation Equipment
- FAA
- Federal Aviation Administration
- FARs
- Federal Aviation Regulations
- FDM
- flight data monitoring
- FDR
- flight data recorder / flight data recording (device)
- FOD
- Flight Operations Directive
- FOQA
- flight operations quality assurance
- FW
- fixed-wing
- GEN
- generation
- GPS
- global positioning system
- GPWS
- ground proximity warning system
- HEMS
- helicopter emergency medical services
- HQ
- headquarters
- HTAWS
- helicopter terrain awareness and warning system
- ICAO
- International Civil Aviation Organization
- IFR
- instrument flight rules
- IMC
- instrument meteorological conditions
- in. Hg
- inches of mercury
- IPB
- Internal Process Bulletin
- JAR-OPS
- Joint Aviation Requirements (Commercial Air Transport Operation)
- LARS
- lightweight aircraft recording system
- M
- magnetic (degrees)
- MHz
- megahertz
- MNR
- (Ontario) Ministry of Natural Resources
- MOH
- (Ontario) Ministry of Health and Long-Term Care
- MPFR
- multi-purpose flight recorder
- NASA
- National Aeronautics and Space Administration (United States)
- NASIMS
- National Aviation Safety Information Management System
- NEMSPA
- National EMS Pilots Association
- NoC
- Notice of Cancellation
- NoS
- Notice of Suspension
- NTSB
- National Transportation Safety Board (United States)
- NVG
- night-vision goggles
- NVIS
- night-vision imaging system
- OCC
- Operations Control Centre
- OM
- Operations Manager
- OPP
- Ontario Provincial Police
- PAOBD
- persons assigned on-board duties
- PF
- pilot flying
- PI
- process inspection
- PIC
- pilot-in-command
- PICA
- Preliminary Issue and Consultation Assessment
- PM
- pilot monitoring
- PNF
- pilot not flying
- POI
- principal operations inspector
- PPC
- pilot proficiency check
- PRM
- person responsible for maintenance
- PVI
- program validation inspection
- RCC
- Regulatory Cooperation Council
- RDCA
- Regional Director of Civil Aviation
- RDG
- Regional Director General
- RTCA
- Radio Technical Commission for Aeronautics
- RW
- rotor-wing
- SAIB
- Special Airworthiness Information Bulletin
- SAR TECH
- search-and-rescue technician
- SAR
- search and rescue
- SB
- Service Bulletin
- SI
- Staff Instruction
- SIC
- second-in-command
- sm
- statute mile
- SMS
- safety management system
- SOPs
- standard operating procedures
- TAWS
- terrain awareness and warning system
- TC
- Transport Canada
- TCCA
- Transport Canada Civil Aviation
- TSB
- Transportation Safety Board
- TSO
- technical standard order
- TTL
- technical team leader
- VFR
- visual flight rules
- VMC
- visual meteorological conditions
- VP
- Vice President
- W
- west