Controlled flight into terrain
Air Nootka Ltd.
de Havilland DHC-2 (floatplane) C-GPVB
Hesquiat Lake, British Columbia 3 nm W
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
At 1015 Pacific Daylight Time, the de Havilland DHC-2 (Beaver) floatplane (registration C-GPVB, serial number 871), operated by Air Nootka Ltd., departed Hesquiat Lake, British Columbia, with the pilot and 5 passengers for Air Nootka Ltd.'s water aerodrome base near Gold River, British Columbia. Visibility at Hesquiat Lake was about 2 ½ nautical miles in rain, and the cloud ceiling was about 400 feet above lake and sea level. Approximately 3 nautical miles west of the lake, while over Hesquiat Peninsula, the aircraft struck a tree top at about 800 feet above sea level and crashed. Shortly after the aircraft came to rest, a post-crash fire developed. All 6 persons on board survived the impact, but the pilot and 1 passenger died shortly after. A brief 406 megahertz emergency locator transmitter signal was transmitted, and a search and rescue helicopter recovered the survivors at about 1600.
Factual information
History of the flight
The pilot arrived at Air Nootka Ltd.'s (Air Nootka) main base at about 0730,Footnote 1 half an hour before any other employee. Air Nootka's main base is located at the Gold River Water Aerodrome (CAU6), about 6 nautical miles (nm) south-southwest of Gold River, British Columbia. The pilot departed the base in C-GPVB at 0850 with passengers bound for Louie Lagoon, British Columbia, about 32 nm west of CAU6. This was the first Air Nootka flight of the day. After dropping off the passengers at Louie Lagoon, C-GPVB departed for Hesquiat Lake, British Columbia, 26 nm southeast of Louie Lagoon, to pick up 5 hikers waiting at a dock at the south end of the lake (Figure 1). Spot and Latitude waypoints in Figure 1 are derived from the pilot's own SPOT© Satellite MessengerFootnote 2 tracker and the aircraft's LatitudeFootnote 3 tracking system.
While flying over Nootka Sound, British Columbia, at just under 300 feet above sea level (asl), en route from Louie Lagoon to Hesquiat Lake, the pilot radioed Air Nootka's base to report that the weather was good enough for 2 company aircraft to depart the company's base for Hesquiat Lake to pick up 9 additional hikers at the Hesquiat Lake dock.
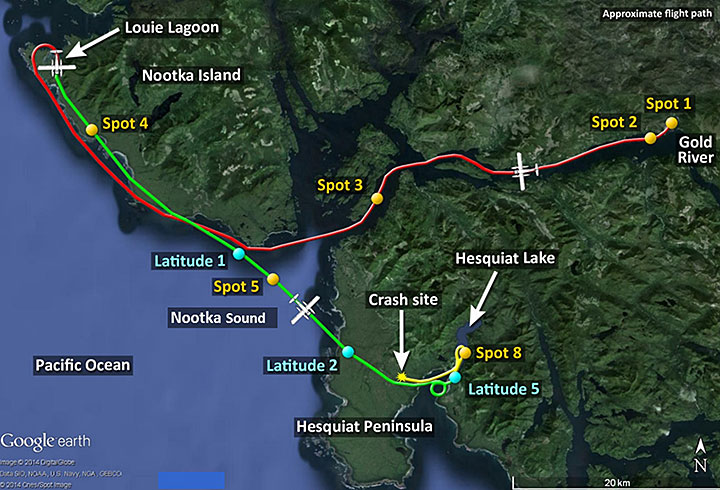
About 6 minutes later, C-GPVB crossed over the west shore of Hesquiat Peninsula while flying at about 400 feet asl. It continued east across the peninsula, arriving at the dock on Hesquiat Lake at about 1004. The weather there included rain, wind from the southeast, visibility about 2 ½ nm, and a ceiling of about 400 feet asl.
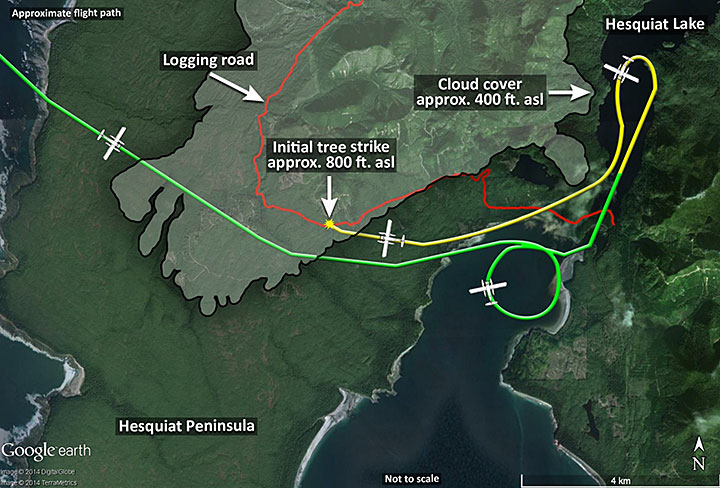
The pilots of the other 2 Air Nootka aircraft inbound to Hesquiat Lake elected to stay over the shoreline of Hesquiat Peninsula for its entire periphery rather than cross the peninsula. The inbound pilots reported their locations and the weather along their route several times to C-GPVB's pilot as they approached. At about 1023, the pilot of C-GPVB radioed the 2 inbound aircraft that he was off the lake and was going to take a look at crossing the peninsula westbound. C-GPVB flew westbound for about 2 minutes, climbing into cloud while staying just above tree-top level, until it struck a tree at about 800 feet asl. The pilots of the 2 inbound aircraft heard a brief “Mayday” on the radio, but were unable to contact C-GPVB afterward. C-GPVB came to rest in forest about 600 feet west of the initial tree strike. All 6 occupants survived the crash, but a short time later a post-crash fire ignited. Four passengers were able to exit the aircraft, but the pilot and 1 passenger remained in the aircraft, which was subsequently consumed by the fire. The 406 megahertz (MHz) emergency locator transmitter (ELT) transmitted a signal for a short period before it was destroyed by the fire.
Accident site
The accident occurred about 3 nm west of Hesquiat Lake in mountainous terrain in the northern portion of Hesquiat Peninsula. The terrain from the southern tip of Hesquiat Peninsula to about 1 mile south of the accident site (about the southern 2/3 of the peninsula) is relatively level ground less than 200 feet asl. The tree that was hit was about 140 feet tall, significantly taller than the trees surrounding it. The aircraft struck the tree about 20 feet below its top and came to rest nose-down in forest about 600 feet further west. The tree is about 400 feet north (uphill) of a logging road running across the hillside in the same direction the aircraft was flying. It is not known if the pilot was using the road as a navigation aid.
The floats detached at final impact, but otherwise the aircraft remained largely intact until consumed in the post-crash fire (Photo 1).

Aircraft
General
The aircraft was manufactured in 1956 and was operated by Air Nootka since April 2006. Records indicate that the aircraft was certified, equipped and maintained in accordance with existing regulations and approved procedures.
The aircraft was equipped with a Garmin GPSMAP 296 global positioning system (GPS), and the pilot carried his own SPOT© Satellite Messenger tracker. The aircraft was not equipped for instrument flight rules (IFR) flight, nor was it required to be by regulation. It is not known if the pilot was using the GPS as a navigation aid on the accident flight leg.
Flight tracking
The aircraft was equipped with a Latitude flight tracking system. This system was normally only activated when Air Nootka was flying clients whose safety policy required a tracking system. It had been turned on partway through the leg of the flight from Louie Lagoon to Hesquiat Lake to ensure it would be working for an upcoming flight. However, it had been turned off when the aircraft landed at Hesquiat Lake and was not turned on again prior to the accident. Tracking system users choose the frequency of position reports transmitted by the equipment installed on the aircraft, in this case, every 6 minutes, and pay based on the number of position reports transmitted. Due primarily to the system's purchase and operating costs, the other 2 company aircraft were not equipped with Latitude flight tracking systems.
Pilot
Records show that the pilot was certified and qualified for the flight in accordance with existing regulations. The pilot held an airline transport pilot licence and current medical. The pilot's flight and duty times were not exceeded, and there were no indications of any health issues on the morning of the accident. The pilot had held a Group 1 instrument rating from January 1991 to February 1992, but did not have a valid instrument rating at the time of the accident, nor was one required for the type of flight, day visual flight rules (VFR), being conducted. The pilot had accumulated approximately 17 000 hours total flying time.
The pilot had purchased Air Nootka in February 1994 and sold the company in May 2006. The pilot returned to fly temporarily for the company during the summer of 2007 and again for the summer of 2013. The pilot was very familiar with the aircraft as well as the local routes, terrain and weather.
Weather
The nearest official weather was recorded at the Estevan Lighthouse, British Columbia, about 6 nm south-southwest of the accident site, and 8 nm southwest of Hesquiat Lake. At 0940 the lighthouse keeper observed:
- overcast with 300 to 400-foot ceiling;
- moderate rain and fog;
- visibility 3 statute miles (sm);
- wind out of the east at 15 knots, gusting to 26 knots;
- sea state 4 feet with moderate low swell;
- barometer 1013.6 hPa and rising (29.94 inches of mercury).
The lighthouse weather at 1240 was nearly identical.
Air Nootka pilots occasionally call Estevan Lighthouse for weather conditions in that area, but C-GPVB's pilot did not speak to the lighthouse keeper on the day of the accident.
It was reported that the weather at Hesquiat Lake when C-GPVB arrived included low cloud ceiling and reduced visibility in drizzle. When the other 2 Air Nootka aircraft arrived at Hesquiat Lake, about 20 minutes after C-GPVB departed, the ceiling was about 400 feet and visibility was about 2 ½ nm in rain with a gusty southeast wind. Weather conditions on the opposite (west) side of Hesquiat Peninsula were marginally better, with ceilings varying from 400 to 600 feet asl and visibility varying from 2 ½ to 4 nm in rain.
The operator
Air Nootka operates a single-engine, day VFR, floatplane transportation service under Subpart 703 (Air taxi – Aeroplane) of the Canadian Aviation Regulations (CARs). Air Nootka does not have a safety management system (SMS), nor is it required by regulation for CAR Subpart 703 operators. Company management is performed by 2 owner/executives and 1 office manager. Aircraft maintenance is contracted.
Air Nootka operates year-round utilizing up to 3 float-equipped aircraft and 5 pilots during the busier summer season. During slower parts of the year, fewer aircraft and pilots are used. Most of the company's operations take place in remote areas of the northwestern portion of Vancouver Island, British Columbia. Most of the airspace in this area is Class G uncontrolled airspace.
As an air taxi operator, Air Nootka is required under Commercial Air Service Standard 723.16 to use a Type D operational control system where authority over the formulation, execution and amendment of an operational flight plan in respect of a flight is delegated, by the company operations manager, to the pilot-in-command (PIC). As such, flights are self-dispatched and released by the PIC. There were no indications of operational pressure to complete flights in weather conditions below the operator's approved minimums. On the day of the accident, there were 4 trips scheduled to pick up hikers at Hesquiat Lake; 3 were in progress at the time of the accident, and the pick-up scheduled for 1800 was cancelled due to weather. The only other trip scheduled that day was successfully completed to Kendrick Arm.
Air Nootka's Company Operations Manual (COM) states that the PIC shall familiarize him/herself with reported and forecast meteorological conditions for the routes and have “alternate flight plans to be followed in the event of the original flight plan becoming impracticable due to unforeseen circumstances.” Section 3.3.1 of the COM requires that a company operational flight plan (OFP) be completed, signed, and a copy left at the point of departure. Pilots are required to access weather information (COM s. 3.2.2) during preparation for a flight, but there is no requirement to attach weather information to the OFP. In accordance with Commercial Air Service Standards (CASS) 723.18(5), Air Nootka's COM s. 3.3.2 allows, for flights terminating at the aerodrome of departure, the use of an informal flight plan in lieu of the OFP. Under this system, only a written record in the form of a dispatch booking sheet, departure/return, and fuel radio log record is required.
The Air Nootka COM also states that, for VFR flights conducted below 1000 feet above ground level (agl) in uncontrolled airspace, the flight visibility must not be less than 2 nm and the aircraft must be operated clear of cloud and with visual reference to the surface. The COM states that IFR, night VFR, and VFR over-the-top are all prohibited. The applicable CARs for this type of operation further state that, other than for take-off or landing, the aircraft must be operated at least 300 feet agl.
The collision avoidance procedures section of Air Nootka's COM states that “The PIC shall not operate the aircraft in such proximity to another aircraft so as to create a risk of collision.”Footnote 4
The pilot was in communication with the other 2 company aircraft en route to the location from which he was departing and was aware that they would be flying along the shoreline around the peninsula.
Other than pilot self-reporting and customer feedback, company management did not have any methods of monitoring flights such that weather, terrain and related pilot decisions could be assessed, either in real-time or as a recording.
Flight recorders
The aircraft was not equipped with a flight data recorder (FDR), a cockpit voice recorder (CVR), or any other lightweight flight data monitoring (FDM) system, nor was any recording system required by regulation. If flight data recordings are not available to an investigation, this may preclude the identification and communication of safety deficiencies to advance transportation safety.
Given the combined accident statistics for CAR Subparts 702, 703 and 704 operations (Table 1), the TSB has previously stated that there is a compelling case for industry and the regulator to proactively identify hazards and manage the risks inherent in these operations.
| Commercial Air Services category | Accidents | Fatal injuries |
|---|---|---|
| 702-Aerial Work | 245 | 51 |
| 703-Air Taxi Operations | 485 | 176 |
| 704-Commuter Operations | 47 | 29 |
| Total | 777 | 256 |
To manage risk effectively, operators need to know why incidents happen and what the contributing safety deficiencies may be. Moreover, routine monitoring of normal operations can help operators improve the efficiency of their operations and identify safety deficiencies before they result in an accident. In the event that an accident does occur, recordings from lightweight flight recording systems can provide useful information to investigators. Based on this, the TSB recommended that:
The Department of Transport work with industry to remove obstacles to and develop recommended practices for the implementation of flight data monitoring (FDM) and the installation of lightweight flight recording systems by commercial operators not currently required to carry these systems.
TSB Recommendation A13-01
In October 2013, Transport Canada (TC) indicated that the department would convene a focus group with industry by March 2014. In February 2014, TC indicated that the department supports the TSB's recommendation and has decided to proceed with the development of an Advisory Circular in 2015/16 to describe recommended practices regarding FDM Programs. In addition, the department will consider adding FDM principles in future regulatory initiatives/amendments, which will be consulted through focus groups at that time.
The Transportation Safety Board assessed TC's response to Recommendation A13-01 as follows:Footnote 5
The Board notes Transport Canada's commitment to proceed with the development of an Advisory Circular and to consider adding FDM principles in future regulatory initiatives/amendments. However, TC is silent on the issues of removing obstacles around the installation of lightweight flight data recording systems. Further, TC has not indicated how it will work with industry on these issues.
Given the paucity of information received from TC, the Board [was] Unable to Assess TC's response.
Survival aspects
All 8 seats were equipped with lap belts but only the 2 front seats were equipped with shoulder harnesses.Footnote 6 All passengers were wearing lap belts. The passenger seated in the front right seat was also wearing the available shoulder harness and was one of the 4 able to exit the aircraft. It could not be determined if the pilot was wearing either his lap belt or shoulder harness.
The TSB has previously recommended (TSB recommendations A94-08 and A92-01) that small commercial aircraft be fitted with seatbelts and shoulder harnesses in all seating positions. Following these recommendations, changes to regulations were made to require shoulder harnesses in all commercial cockpits and on all seats in aircraft manufactured after 1986Footnote 7 with 9 or fewer passengers. This regulatory change did not address the vast majority of the commercial floatplane fleet, which was manufactured prior to 1986.
The TSB considers that, given the additional hazards associated with accidents on water, shoulder harnesses for all seaplane passengers will reduce the risk of incapacitating injury, thereby improving the likelihood of exiting the aircraft.
As a result of TSB investigation A12O0071, the Board recommended that:
The Department of Transport require that all seaplanes in commercial service certificated for 9 or fewer passengers be fitted with seatbelts that include shoulder harnesses on all passenger seats.
TSB Recommendation A13-03
Although safety equipment such as push-out windows and improved door handles are available, this aircraft was not equipped with them nor was it required to be by regulation.
All of the aircraft's occupants were injured during the accident and, due to the rapid progression of the post-crash fire, some of the survivors were unable to exit the aircraft before receiving serious burns. None of the occupants exited the aircraft via the doors after the crash. The front right seat passenger exited through the broken windshield and 1 centre-row passenger and the 2 rear-seat passengers exited via a broken window in the left rear cabin door. The centre row of passenger seats detached from the floor during the crash. The pilot and 1 of the 2 centre-row passengers remained in the aircraft.
Timely egress from a sinking or burning aircraft is essential. The structural deformation that occurs during a crash often results in exits being jammed shut, making it difficult or impossible for survivors to exit the aircraft.
Post-impact fire
The post-impact fire started at the nose of the aircraft about 10 seconds after the aircraft came to rest. The aircraft was equipped with 3 main fuel tanks located in the fuselage under the cabin floor and was also equipped with wing tip tanks. There was no fuel being carried in the wing tip tanks. Because the aircraft came to rest nose-down, any leaked fuel would have run forward. The fire's ignition source was not identified. Possible sources include fuel contact with hot engine components or electrical arcing.
Previous TSB investigations have determined that arcing from damaged electrical systems is often an ignition source. Most of the aircraft's electrical system, including the battery, was located forward of the pilot.
Post-impact fires have been documented as a risk to aviation safety in previous TSB investigations. As well, after TSB Safety Issues Investigation SII A05-01 was completed in 2006, the TSB concluded that the defences against post-impact fires in impact-survivable accidents are and will remain inadequate unless countermeasures are introduced to reduce the risk.
Therefore, on 29 August 2006, the Board recommended that:Footnote 8
To reduce the number of post-impact fires in impact-survivable accidents involving existing production aircraft weighing less than 5700 kg, Transport Canada, the Federal Aviation Administration, and other foreign regulators conduct risk assessments to determine the feasibility of retrofitting aircraft with the following:
- selected technology to eliminate hot items as a potential ignition source;
- technology designed to inert the battery and electrical systems at impact to eliminate high-temperature electrical arcing as a potential ignition source;
- protective or sacrificial insulating materials in locations that are vulnerable to friction heating and sparking during accidents to eliminate friction sparking as a potential ignition source; and
- selected fuel system crashworthiness components that retain fuel.
TC responded to these recommendations in November 2006 and January 2007, but because these responses contained no action or proposed action that will reduce or eliminate the risks associated with this deficiency, TC's overall response to Recommendation A06-10 was assessed as Unsatisfactory. The Board has determined that the residual risk associated with the deficiency identified in Recommendation A06-10 remains significant and, consequently, the TSB will renew efforts to encourage adoption of the recommendation.
C-GPVB had not been retrofitted with any of the technology referred to in TSB Recommendation A06-10, nor was it required to be by regulation.
Visual flight rules flight–into–instrument meteorological conditions accidents
Accident data have consistently shown that continued VFR flight into adverse weather represents a significant threat to aviation safety. VFR flight-into-instrument meteorological conditions (VFR-into-IMC) accidents are 3 to 5 times more likely to be fatal when compared to all other accidents combined. National Transportation Safety Board (NTSB) data on general aviation accident over 20 years showed that about two-thirds of all IMC accidents have resulted in at least 1 fatality, a rate 3 times higher than the fatality rate of all general aviation (GA) accidents.Footnote 9 An Australian Transport Safety Bureau (ATSB) report cited a study on accident data showing that 75.6% of VFR–into-IMC accidents resulted in fatalities.Footnote 10 TSB data has also shown consistently that VFR-into-IMC accidents are disproportionally lethal: data between 1976 and 1985 showed that 50.2% of VFR-into-IMC accidents resulted in fatalities, compared to 12.7% fatal for all of the Canadian accidents.Footnote 11 TSB data between 1995 and 2004 showed similar results, 55% and 10% respectively.
Controlled flight into terrain (CFIT) accidents involve collisions with land or water while the aircraft is under crew control. CFIT accidents account for 5% of accidents, but nearly 25% of all fatalities. Between 2004 and 2013, there were 105 accidents of this type in Canada, resulting in 109 fatalities.
Pilot decision making
Pilot decision making (PDM) is critical to flight safety. The assessment of the available options involves a subjective risk assessment based on experience and knowledge. Pilots usually decide on the option they perceive as most likely to result in the best outcome given their goals.
Pilots' decisions can be influenced by a wide range of factors such as perception of the situation, experience, training, abilities, expectations, goals and objectives, organizational and social pressure, time-criticality and contextual elements. A VFR pilot's decisions are largely influenced by the assessment of existing weather information, the availability of additional navigational aids, and previous experience with a route.
Successful experience under similar circumstances can make pilots very reluctant to select a different course of action. VFR pilots can be overly optimistic on the probability of having to fly from VFR into IMC, and on their own abilities to fly out of IMC if encountered (ability bias). Decision framing can play a role. If pilots frame their decisions in terms of potential losses (that is, delay, disappointing customers, loss of revenue, etc.), they are more likely to prolong flight into deteriorating weather.
Once a decision is made to depart or continue along a route, pilots have a tendency to continue with the selected course of action unless there are compelling reasons not to do so. Additionally, pilots often seek out elements that reinforce, not contradict, the decision made (that is, confirmation bias).Footnote 12
TC's TP 13897, Pilot Decision Making, suggests that some pilots carry out operations below VFR minima because they believe that they can safely operate below the regulated minima and that there is commercial pressure to continue doing so. TP 13897 explains that VFR minima were established because they are considered by the regulator to be the minimum safe limits and that risk increases significantly when pilots decide to accept poorer conditions rather than turn back.
Type D operations, where much of the decision making associated with a flight is delegated solely to the pilot, are not necessarily riskier than other types of flight operations. However, similar to other recent accidents (TSB Investigation Reports A08P0353, A10Q0132, A12C0005, and A12P0034), this accident demonstrates that when pilot decisions and operating practices are not in accordance with procedures laid out in company operations manuals, the risk of accident increases. Pilot and flight monitoring are methods of identifying, and addressing, unsafe conditions, unsafe practices and poor decision making before they lead to a serious incident or accident.
Analysis
Based on information gathered from the survivors, the tracking systems and the maintenance records, it was determined that the aircraft was airworthy at the time of the accident, and that aircraft performance prior to the collision with the tree was not a contributing factor. The analysis will focus on the decisions made by the pilot as well as post-crash safety issues.
This illustrates a common pattern of visual flight rules flight-into-instrument meteorological conditions (VFR-into-IMC) accidents which the TSB has investigated in the past. It is clear that more needs to be done to reduce the risks associated with these types of accidents.
Pilot decision making
By climbing into cloud, and with visibility below 2 nautical miles (nm), the pilot entered IMC, although he was not qualified nor was the aircraft equipped or approved for an instrument flight rules (IFR) flight.
For day VFR operations under Subpart 703 utilizing Type D dispatch, there is no regulatory requirement for second pilot input, dispatcher co-authority, documentation of weather information collected, or remote equipment to be installed at frequent destinations to help the pilots decide whether or not to conduct flights.Footnote 13
Because the accident pilot arrived for work at Air Nootka's main base before anyone else, it is not known what weather information the pilot gathered prior to the flight. It is known that the pilot did not speak to the Estevan Lighthouse keeper. The other 2 company pilots, 1 of whom did speak to the lighthouse keeper, waited to hear what conditions the accident pilot encountered before they decided to undertake their flights. This information provided them with pertinent operational information. Both pilots chose a different route to Hesquiat Lake, British Columbia, and return to Gold River, British Columbia, than the first pilot. The accident pilot, a long-time pilot in the area, was familiar with the various routes to and from Hesquiat Lake. By the time the accident pilot arrived at Hesquiat Lake, the pilot was aware of the ceiling and visibility along at least 2 of those routes as he had just flown one and had been advised by company pilots regarding another.
It is not known why the pilot chose to fly across Hesquiat Peninsula. Flying across the peninsula saved about 13 nm over the route around the peninsula. The pilot had successfully flown across the peninsula on the inbound trip. Takeoff from Hesquiat Lake could have been delayed until the other 2 aircraft arrived, though that would have meant a delay of about 20 minutes. With the passengers already on board, the pilot may have felt pressure to depart as soon as possible. Another factor for the pilot's choice of westbound versus southbound route may have been reluctance to fly in low visibility and low ceiling conditions directly toward the 2 northbound company aircraft that were flying along the shoreline, inbound to Hesquiat Lake. The weather on the chosen route did not meet the minimum weather requirements established in the Company Operations Manual (COM) and Canadian Aviation Regulations (CARs). The pilot flew just above the tree tops into IMC and rising terrain, and the aircraft struck a tree that was significantly taller than the others.
Departing westbound from Hesquiat Lake across the peninsula would entail climbing into cloud in order to remain above the terrain. However, because the pilot had successfully flown this route in the opposite direction minutes before, he may have expected he could retrace that route either by using the GPS track from his inbound flight, or by following the logging road across the peninsula to lower ground and slightly higher ceilings on the west side.
Finally, the pilot had flown in this area of British Columbia's west coast, an area well known for mountainous terrain, rain, fog, wind, low ceilings, etc., for much of his career and had almost certainly flown in challenging weather conditions on many occasions. Though no longer current, the pilot had once held an instrument flight rating.
Air Nootka did not have effective methods to monitor its pilots' in-flight decision making and associated practices. As a result, Air Nootka had no way to detect and correct unsafe behaviour or poor decision making such as occurred on this flight. This highlights an ongoing safety issue. If companies operating under self-dispatch do not monitor their operations, they may not be able to identify unsafe practices that increase the risk to flight crew and passengers.
As a result of these factors, the pilot likely believed he could complete a flight from VFR into IMC while low over tree-covered high ground, but collided with terrain while in controlled flight.
Survivability
In this occurrence, the pilot and 1 passenger did not exit the aircraft before it was consumed in the post-impact fire. Post-crash fires are a well-documented cause of injury and death in aircraft accidents. Had there not been a post-crash fire in this accident, the 2 occupants who were unable to exit the aircraft may have survived.
C-GPVB had not been retrofitted with any of the technology referred to in TSB Recommendation A06-10. It is not known if electrical arcing or hot components were the ignition source for the post-crash fire in this accident, but they are possible sources. If aircraft are not fitted with technology to reduce fuel leakage or to eliminate ignition sources, the risk of post-impact fire is increased.
Transport Canada (TC) does not require this aircraft, nor many similar older aircraft, to be equipped with shoulder harnesses for all of the passenger seat locations. The fatally injured passenger was sitting in a seat that separated from the floor and was not equipped with a shoulder harness. While it is not known to have been a factor in this accident, it is known that shoulder harnesses decrease the likelihood of head and upper body injuries. If aircraft are not equipped with shoulder harnesses for all seating positions then there is an increased risk of injuries.
None of the occupants exited the aircraft via the doors following the crash. Though safety equipment such as push-out windows and improved door handles are available, this aircraft was not equipped with them, nor was it required to be. The incorporation of these modifications may have provided alternatives for passengers to exit the burning aircraft. If aircraft are not equipped with some alternate means of escape such as push-out windows, then there is a risk that post-crash structural deformation will jam doors shut and restrict exit for the occupants.
Findings
Findings as to causes and contributing factors
- The pilot flew just above the tree tops into instrument meteorological conditions and rising terrain, and the aircraft struck a tree that was significantly taller than the others.
- The pilot and 1 passenger did not exit the aircraft before it was consumed in the post-impact fire.
- Air Nootka did not have effective methods to monitor its pilots' in-flight decision making and associated practices. As a result, Air Nootka had no way to detect and correct unsafe behaviour or poor decision making such as occurred on this flight.
Findings as to risk
- If aircraft are not fitted with technology to reduce fuel leakage or to eliminate ignition sources, the risk of post-impact fire is increased.
- If aircraft are not equipped with shoulder harnesses for all seating positions then there is an increased risk of injuries.
- If aircraft are not equipped with some alternate means of escape such as push-out windows, then there is a risk that post-crash structural deformation will jam doors shut and restrict exit for the occupants.
- If companies operating under self-dispatch do not monitor their operations, they risk not being able to identify unsafe practices that are a hazard to flight crew and passengers.
- If flight data recordings are not available to an investigation, this may preclude the identification and communication of safety deficiencies to advance transportation safety.
This report concludes the Transportation Safety Board's investigation into this occurrence. the Board authorized the release of this report on . It was officially released on .