Collision with terrain
Manan Air Services (dba Atlantic Charters)
Piper PA-31 Navajo, C-GKWE
Grand Manan, New Brunswick
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The Atlantic Charters Piper PA-31 (registration C GKWE, serial number 31-7812037) aircraft had carried out a MEDEVAC flight from Grand Manan, New Brunswick, to Saint John, New Brunswick. At 0436 Atlantic Daylight Time, the aircraft departed Saint John for the return flight to Grand Manan with 2 pilots and 2 passengers. Following an attempt to land on Runway 24 at Grand Manan Airport, the captain carried out a go-around. During the second approach, with the landing gear extended, the aircraft contacted a road perpendicular to the runway, approximately 1500 feet before the threshold. The aircraft continued straight through 100 feet of brush before briefly becoming airborne. At about 0512, the aircraft struck the ground left of the runway centreline, approximately 1000 feet before the threshold. The captain and 1 passenger sustained fatal injuries. The other pilot and the second passenger sustained serious injuries. The aircraft was destroyed; an emergency locator transmitter signal was received. The accident occurred during the hours of darkness.
1.0 Factual information
1.1 History of the flight
At 0221,Footnote 1 Atlantic Charters received a telephone call from the Ambulance New Brunswick (ANB) Medical Communication Management Centre (MCMC) advising of a possible patient transfer (MEDEVAC flight) from Grand Manan, New Brunswick, to Saint John, New Brunswick. The MCMC also requested a weather check. During a follow-up telephone call, Atlantic Charters indicated that the departure would not be a problem, but that since fog was starting to come in, the return flight might be delayed.
About 30 minutes later, the MCMC contacted Atlantic Charters and confirmed the flight. Atlantic Charters indicated that it would advise the pilots, as well as meet the patient, paramedic, and nurse at the airport. The captain contacted the first officer (FO) then filed a flight plan.
The FO prepared the aircraft for the flight and helped load the patient. The FO then installed a forward-facing passenger seat on the left rear side of the cabin adjacent to the entrance door, entered the cockpit through the cabin, and sat in the right seat.
An ANB paramedic occupied the rear-facing seat that was installed behind the captain's seat on the left side of the cabin, and a nurse from the Grand Manan Hospital occupied the forward-facing passenger seat. The captain closed the cabin entrance door from the outside, entered the cockpit via the cockpit door, and sat in the left seat.
After the engines were started, the captain noted that there was only 1 headset. Because the engines were already running, the captain decided to continue with only the single headset on board and used this headset during the flights.
At about 0400, the aircraft departed Grand Manan Airport under an instrument flight rules (IFR) flight plan to Saint John. The flight was uneventful, and the aircraft landed in Saint John at 0417, where it was met by an ambulance to transfer the patient to the hospital.
At 0436, the aircraft departed Saint John under an IFR flight plan to Grand Manan with the 2 pilots, the paramedic, and the nurse on board. All occupants sat in the same seats as before.
The captain contacted Atlantic Charters' duty personFootnote 2 on the radio and advised that they were inbound. At 0457, approximately 20 nautical miles (nm) from Grand Manan, the captain closed the IFR flight plan with the Moncton Area Control Centre (ACC).
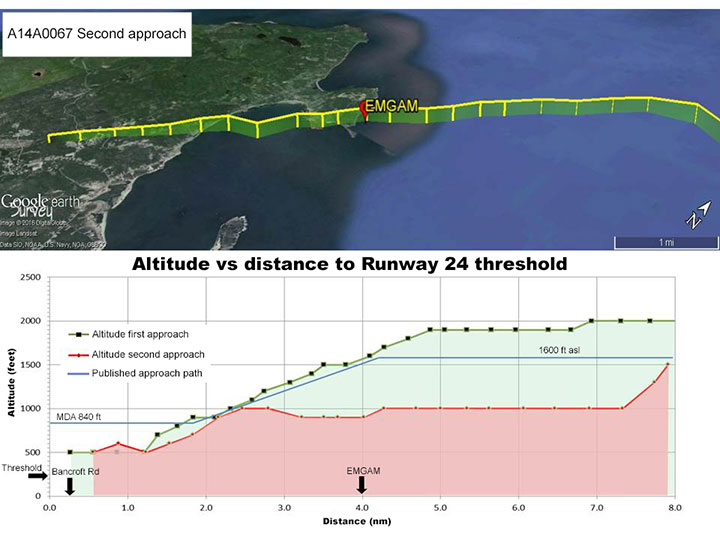
The aircraft began to descend from 1900 feet above sea level (asl) at 4.87 nm from the threshold of Runway 24.Footnote 3 The captain made an advisory radio call on the aerodrome traffic frequency (ATF) at EMGAM,Footnote 4 which is 4 nm from the threshold of Runway 24 (Appendix A). At EMGAM, the aircraft was at an altitude of 1600 feet asl, with a ground speed of 90 knots. The aircraft then levelled off at 500 feet asl, 1.2 nm from the threshold. The aircraft remained at 500 feet asl, which is approximately 250 feet above ground level (agl), until it was at least 0.26 nmFootnote 5 from the threshold, with a ground speed of 90 knots. Soon after this point, the captain initiated a descent in an attempt to land. However, the captain elected to carry out a go-around, and 36 seconds later, the aircraft was 0.23 nm past the end of Runway 24 at 300 feet asl (50 feet agl).
At about 0508, the aircraft intercepted the final approach approximately 7 nm from the threshold at an altitude of 1000 feet asl for a second attempt to land on Runway 24. Two minutes later, the aircraft passed over EMGAM at 900 nm feet asl, with a ground speed of 100 knots. The aircraft remained at this altitude until it was 2.46 nm from the threshold, when it started to descend. Approximately 1 minute later, the aircraft was at 500 feet asl and 1.23 nm from the threshold, with a ground speed of 90 knots. The aircraft remained at approximately this altitude for 24 seconds. At abou 0512, which is the time of the last recorded radar position, the aircraft was 0.56 nm from the threshold, with a ground speed of 90 knots.
The approach to Runway 24 was over a dimly lit, sparsely populated area, and was carried out with the aircraft's landing light and strobes off, and with the runway lights illuminated.Footnote 6
The aircraft contacted the north side of Bancroft Road on all 3 wheels, about 15 feet above and approximately 0.25 nm before the threshold of Runway 24 (Photo 1).
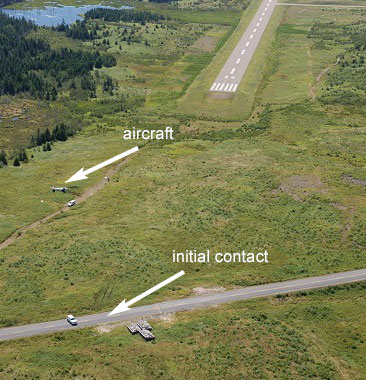
The aircraft continued across the approximately 25-foot-wide road and straight through 100 feet of brush and uneven terrain. All 3 tires made distinctive marks on the road and as the aircraft continued through the brush. The left outboard landing gear door separated, a portion of the nose landing gear strut fractured, and the left main wheel contacted a tree stump before the terrain dropped off. The aircraft became airborne and began to bank to the left, then the lower portion of the nose landing gear strut and wheel assembly separated from the aircraft.
The aircraft continued an increasingly steep left bank. When the bank angle was almost 90°, the left wingtip contacted the ground, causing the aircraft to rotate downward in a cartwheel motion. The aircraft's nose and both propellers struck the ground. The aircraft bounced and pitched nose up before coming to rest approximately 1000 feet before the threshold.Footnote 7
The captain and paramedic were fatally injured. The captain was found in the left seat in the cockpit with the shoulder harness and seatbelt fastened. The paramedic was found on the left wing adjacent to the fuselage below the cockpit door. The FO and nurse were severely injured; both had been wearing their seatbelts and both evacuated the aircraft without assistance. During the evacuation, the FO had to manoeuvre around loose cargo while moving through the cabin. After exiting the aircraft, the FO made a 911 telephone call at 0514.
About 15 minutes after the impact, first responders were on Bancroft Road, in a location that aligned with the runway, which was about 500 feet from the aircraft. Members of the Royal Canadian Mounted Police (RCMP) also arrived shortly after the accident. They secured the site and remained in control until the arrival of TSB investigators.
1.2 Injuries to persons
| Crew | Passengers | Others | Total | |
|---|---|---|---|---|
| Fatal | 1 | 1 | – | 2 |
| Serious | 1 | 1 | – | 2 |
| Minor/None | – | – | – | – |
| Total | 2 | 2 | – | 4 |
1.3 Damage to aircraft
The aircraft was destroyed.
1.4 Other damage
Not applicable.
1.5 Personnel information
The captain was certified and qualified for the flight in accordance with existing regulations.
During the week preceding the occurrence, the captain carried out a multi-leg charter operation. The flights ranged from 15 minutes to 1.5 hours each day. On 15 August, the day before the occurrence, the captain had flown approximately 3.5 hours and had returned to Grand Manan at 1600. There was no indication throughout the week that the captain was fatigued. The captain had about 5 hours' rest before preparing for the MEDEVAC flight to Saint John. Fatigue was not considered a factor in this occurrence.
The FO was certified and qualified for the flight in accordance with existing regulations. The FO had completed a multi-engine IFR rating in April 2014 and started working at Atlantic Charters the same month. The FO completed the company's indoctrination, survival equipment, and MEDEVAC training. The FO was hired to assist in the daily activities at the hangar, such as cleaning and moving aircraft, and to act as FO on MEDEVAC and charter flights. The day before the occurrence, the FO worked at the hangar for 3 hours in the morning, cleaning aircraft and doing paperwork.
| Captain | First officer | |
|---|---|---|
| Pilot licence | Airline transport pilot licence (ATPL) | Commercial pilot licence (CPL) |
| Medical expiry date | 01 January 2015 | 01 June 2015 |
| Total flying hours | 17 400 | 304 |
| Hours on type | Unknown | 67.5 |
| Hours in the last 90 days (all types) | 79.5 | 72.8 |
| Hours on type in the last 30 days | 1.2 | 27.7 |
| Hours in the last 3 days (all types) | 4.5 | 3.9 |
| Hours on duty prior to occurrence | 2 | 2 |
| Hours off duty prior to work period | 10.5 | 15 |
The investigation could not determine the captain's total hours on a PA-31 aircraft because numerous records had been destroyed in an earlier house fire. The captain had been flying PA-31 aircraft for over 20 years.
1.6 Aircraft information
1.6.1 General
The Piper PA-31 is a twin-engine aircraft with retractable landing gear and constant-speed propellers. The aircraft is certified to be flown with a single pilot and, depending on its configuration, can have cabin seating for a maximum of 6 passengers.
1.6.2 Occurrence aircraft
The occurrence aircraft was manufactured in 1978, and had been owned and operated by Atlantic Charters since it was imported in April 2011. The aircraft was certified for day or night flights under visual flight rules (VFR) or instrument flight rules (IFR). The aircraft was equipped with wing nacelle fuel tanks and a global positioning system (GPS). Aircraft documentation indicated the GPS was certified for IFR enroute, terminal and approach modes.
On the occurrence flight, the aircraft was configured to carry 2 pilots, 2 passengers, and 1 patient on an air ambulance system, which was installed in a longitudinal orientation on the right side of the cabin.
Records indicate that the aircraft was maintained in accordance with the Atlantic Charters approved maintenance schedule. There were no deferred or outstanding defects recorded in the aircraft journey log.Footnote 8 There was no report of any technical difficulties before the occurrence flight, nor was there any indication of a component or system failure during the flight. At the time of the accident, the aircraft had accumulated a total of 5762.5 hours.
1.6.3 Weight and balance
1.6.3.1 General
Aircraft are designed to operate within their specified weight and balance (centre of gravity) limitations, and these limitations are critical for the safe operation of an aircraft.
Canadian Aviation Regulations (CARs) 703.37 requires that the load restrictions, the weight and the centre of gravity of the aircraft conform to the limitations specified in the aircraft flight manual (AFM).Footnote 9 Additionally, the aircraft operator must specify in its company operations manual (COM) its weight and balance system, as well as instructions to employees regarding the preparation and accuracy of weight and balance forms.
CARs 605.92(1)(c) requires aircraft owners to retain an empty weight and balance report that meets regulatory standards. Standards require that:
The empty weight of an aircraft stated in a weight and balance report shall include all items required by the basis of the aircraft type certification, and all additional items of installed equipment. Any item not forming part of the type design shall be entered in an equipment list with its associated weight and moment. This list constitutes a part of the weight and balance report.Footnote 10
According to this standard, when modifications or major repairs are made to an aircraft that involve a change to the empty weight or centre of gravity, a description of the change, the effective date of the change, and the weight and moment arm of each item installed or removed shall be transcribed in the empty weight and balance report for that aircraft.
When aircraft operate in 2 or more different configurations, a separate weight and balance report addendum for each configuration may be used providing that the current applicable addendum is identified in the aircraft journey log.
1.6.3.2 Occurrence aircraft
When the occurrence aircraft was imported into Canada in April 2011, the aircraft records indicated a basic empty weight of 4598.55 pounds with a moment arm of 128.16 inches.
In June 2011, Atlantic Charters had the aircraft reweighed; the aircraft records showed a basic empty weight of 4244.0 pounds with a moment arm of 127.3 inches. The aircraft records did not include a current equipment list nor did they identify any modifications or major repairs that would account for the 354-pound reduction in weight. Atlantic Charters did not provide supporting documentation which accounted for the difference in weight.
The empty weight and balance report was amended twice after the aircraft was imported; the final weight was identified as 4241.8 pounds.Footnote 11 However, Atlantic Charters continued to use the June 2011 basic empty weight for its weight and balance calculation form.
The investigation could not confirm the aircraft's basic empty weight, nor could it identify what equipment was included in the recorded weight of the aircraft. Therefore, the investigation could not determine the aircraft's exact weight and centre of gravity location for the occurrence flight.
1.6.3.3 Atlantic Charters weight and balance
Atlantic Charters repeatedly reconfigured the aircraft from the passenger seating configuration to the MEDEVAC configuration. Each configuration change required an addendum to the weight and balance, and the configuration change was to be recorded in the aircraft journey log and technical records. However, there were no records of configuration changes, or the applicable weight and balance information, in the aircraft journey log or technical records.
The Atlantic Charters' COM describes the company's procedures pertaining to weight and balance control. The manual includes the following information:
- 2.5.4 The weight & balance calculation may take two forms: one that is precomputed for different fuel and passenger/freight loads, and the other that is individually prepared for a specific flight reflecting non-standard loading. Blank forms and those pre-computed are kept in […] each aeroplane.
[…] a copy [of the weight and balance calculation form] will be left at the point of departure with instructions that it be retained for 24 hours, or an electronic copy may be emailed to [the company]. The original of the form will be returned and retained in the company files for a six month period following the flight.Footnote 12
[…]- 2.5.9 Sample Weight and Balance form may be found in Chapter 8 of [the COM].
Post-accident examination revealed that there were no blank forms on board the aircraft.
Atlantic Charters used the pre-computed weight and balance calculation form for the MEDEVAC flights. However, the investigation noted a number of discrepancies in the recorded information on the pre-computed form provided for the occurrence flight. Atlantic Charters did not provide supporting documentation which accounted for the differences in weights.
Occasionally, Atlantic Charters would use the wing nacelle fuel tanks; however, the pre-computed form did not have a provision to enter fuel weights for the nacelle fuel tanks.
1.6.4 Airworthiness / type design
1.6.4.1 General
In respect of an aircraft or other aeronautical product, the CARs define airworthy as being “in a fit and safe state for flight and in conformity with its type design.Footnote 13”
Regulations prohibit an aircraft from being flown unless it is maintained in accordance with any airworthiness limitations applicable to the aircraft type design.Footnote 14
1.6.4.2 Supplemental type certificate
A supplemental type certificate (STC) is a document issued by Transport Canada (TC) to record the approval of a change to the original type design of an aeronautical product identified in the document.Footnote 15 This document also describes how the change affects the original type design. The STC may include supporting technical data, such as supplements to the approved aircraft flight manual (AFM) and aircraft maintenance manual (AMM). The AFM supplements contain information that supersedes or supplements the basic AFM regarding procedures, performance, and limitations, such as permissible operating weights and critical airspeeds.
1.6.4.2.1 Boundary Layer Research, Inc.
When the aircraft was imported into Canada, it was equipped with a Boundary Layer Research, Inc. (BLR) STC.Footnote 16 This STC included the installation of 4 engine nacelle strakes, 86 vortex generators (VG) affixed to the wings and vertical tail, the remarking of the airspeed indicators (ASI), and the insertion of the approved supplement into the AFM.
In October 2011, the aircraft was paint-stripped and repainted. There is no record of the VGs having been removed as part of the painting process.
During the post-occurrence examination of the aircraft, it was noted that there were no VGs installed, only 2 of the engine nacelle strakes were installed, both ASIs were marked in accordance with the STC markings, and the AFM included the STC supplement as well as amendments to speeds and performance charts to reflect the STC.
1.6.4.2.2 Aeromed Systems, Inc.
The aircraft was equipped with an Aeromed Systems, Inc. air ambulance system (serial number 3800-078), which consisted of an ambulance unit with overhead panel (referred to as a medical unit), a stretcher, and an adapter unit. A total of 93 such air ambulance systems were built.
The Aeromed Systems, Inc. air ambulance system (Federal Aviation Administration [FAA] STC SA1423GL)Footnote 17 is approved for installation on various aircraft, including the PA-31. The STC documentation included an AFM supplement, an electromagnetic interference (EMI) test plan, and a maintenance program.Footnote 18 According to the AFM supplement, the medical unit, stretcher, adapter, and overhead panel had a combined weight of 218 pounds.
Atlantic Charters did not provide a record of the installation of the Aeromed Systems, Inc. air ambulance system, nor did it provide a copy of the AFM supplement, the EMI test plan or the maintenance program.Footnote 19 TC does not have a record of Atlantic Charters incorporating this STC on the occurrence aircraft. None of the aircraft's technical records contained any information related to the installation of the air ambulance system.
The air ambulance system requires the adapter unit to be installed on the right side of the fuselage, using the aircraft's existing seat track. An electrical interface consisting of a 40-amp circuit breaker/switch is installed in the circuit breaker panel, and an electrical plug is mounted in the right side cabin floor adjacent to the adapter.
The adapter unit consists of a left-side and right-side rail, each with 4 plates attached. Each right-side plate had 2 slotted holes and each left-side plate had a single slotted hole. Cross tubes are attached between the left- and right-side plates and are held in place by 2 bolt assemblies per plate, installed through the slotted holes. The slotted holes in the plates allow for adjustment of the side rails. Two locking pins, 1 in each seat track, are installed to locate the adapter unit on the seat tracks and to restrict the adapter unit from moving forward.
During initial installation, the width of the adapter unit is adjusted to fit the seat tracks. Both sides of the cross tubes are then secured to the plates by tightening the bolt assemblies. A quick-release pin is to be installed between a bracket on the left side of the cross tube and the plate both on the forward and aft locations.
By removing the 2 quick-release pins and loosening the 8 bolts that secure the left side of the cross tubes to the plates, the left-side rail can then be moved to allow the complete adapter unit to be detached from the aircraft. When reinstalling the adapter unit, the right-side rail is placed on the seat track, and then the left-side rail is adjusted until the 2 quick-release pins can be installed. The 8 bolts are then tightened to secure the rail in place.
Post-occurrence examination of the adapter unit revealed the following:
- Only 1 locking pin had been installed, in the left seat track.
- The locking pin had been pulled free, and the adapter unit had moved forward about 2 inches.
- The adapter unit was twisted and was no longer fully retained by the 2 seat tracks.
- Of the 16 bolts which secured the cross tubes to the plates, 4 were found loose in their slotted holes.Footnote 20
- The quick-release pins were not installed.
1.6.5 Elementary maintenance work
CARs 605.85 discusses the certification of maintenance conducted on an aircraft as follows:
[…] no person shall conduct a take-off in an aircraft, or permit a take-off to be conducted in an aircraft that is in the legal custody and control of the person, where that aircraft has undergone maintenance, unless the maintenance has been certified by the signing of a maintenance release pursuant to section 571.10.
[…]
No maintenance release is required in respect of tasks identified as elementary work in the Aircraft Equipment and Maintenance Standards.
CARs 605.96 requires all tasks designated as elementary work to be recorded in the aircraft's journey log.Footnote 21 Atlantic Charters had used the occurrence aircraft for both charter and MEDEVAC flights, and considered the installation of the air ambulance system to be elementary work although it was not listed as such in the maintenance control manual (MCM). In addition, the aircraft's journey log had no entries for the completion of elementary work tasks.
For CARs subpart 703 operators, the designated elementary work tasks must be listed in the operator's MCM, along with a reference to the training to be undertaken by persons authorized to perform these tasks. Atlantic Charters' MCM listed 8 elementary work tasks that could be performed on its aircraft by persons trained for elementary maintenance by the approved maintenance organization (AMO). The task list included the removal and installation of passenger seats and passenger seatbelts; however, it did not include the removal and replacement of equipment designed for rapid removal and replacement. The MCM stated that the elementary work training record sheet would be maintained for not less than 2 years. However, Atlantic Charters could not provide any elementary work training record sheets.
The occurrence aircraft was reconfigured from the charter to the MEDEVAC configuration the day before the occurrence flight. The pilot who installed the air ambulance system did not have approved training, nor was the pilot approved to carry out elementary work in accordance with the company's MCM.
1.7 Meteorological information
Saint John (CYSJ) is the nearest aviation weather station to Grand Manan (CCN2), at 53 nm away. According to the aerodrome routine meteorological report (METAR), the weather at 0500 at CYSJ was as follows: wind 140° true (T) at 6 knots, visibility 15 statute miles (sm), overcast ceiling 500 feet agl, temperature 14°C, dewpoint 13°C, altimeter 29.90 inches of mercury (in. Hg), remark: stratocumulus 8 oktas.Footnote 22
According to the aerodrome forecast (TAF) for CYSJ issued at 0238 on 16 August 2014, the weather between 0300 to 0900 called for wind 160°T at 5 knots, visibility 2 sm in mist, scattered clouds at 200 feet agl, broken clouds at 400 feet agl, overcast at 12 000 feet agl. There was a temporary condition of visibility 6 sm in mist, scattered clouds at 400 feet agl, broken clouds at 12 000 feet agl, and a 30% probability of ½ sm visibility in fog, vertical visibility 200 feet agl.
At the TSB's request, Environment Canada carried out a post-occurrence assessment of the meteorological conditions present before and around the time of the crash at Grand Manan Airport. The assessment concluded that, “At the time of the crash, the aircraft at Grand Manan airport would have most likely been flying into dense fog with extremely limited visibilities in both the vertical and horizontal direction.”Footnote 23
Persons near the airport around the time of the accident indicated there were localized areas of fog.
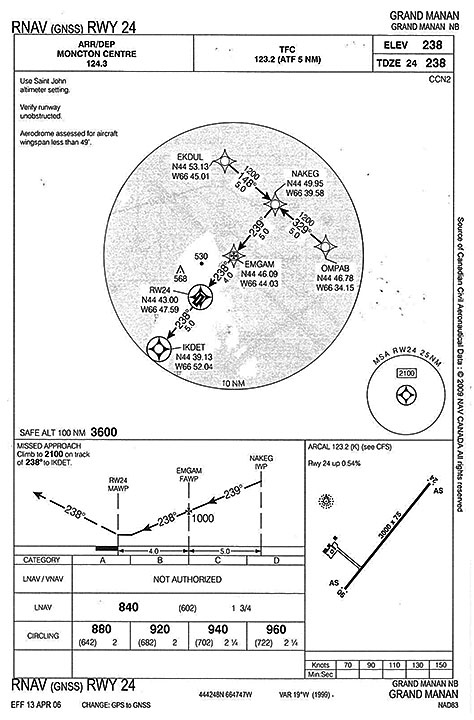
1.8 Aids to navigation
The airport is equipped with a non-directional beacon (NDB). IFR approaches to Runway 06 include an NDB non-precision approach as well as an area navigation (RNAV) non-precision approach. The only IFR approach for Runway 24 is an RNAV non-precision approach (Appendix A). An RNAV approach uses global navigation satellite system (GNSS) guidance, and is commonly referred to as a GPS approach.
According to the Canada Air Pilot (CAP),Footnote 24 the RNAV Runway 24 approach depicts a constant descent angle of 3 degrees, the optimum descent path for a non-precision final approach segment. When flying at a ground speed of 90 knots, a rate of descent of 480 feet per minute (fpm) is needed to achieve this descent path. This descent can continue until reaching the minimum descent altitude (MDA), which is 840 feet asl (609 feet agl) for Runway 24. Pilots of aircraft on instrument approaches are prohibited from continuing the descent below the MDA unless the required visual reference is established and maintained in order to complete a safe landing.Footnote 25
1.9 Communications
The Grand Manan Airport uses an ATF to ensure that all radio-equipped aircraft operating on the ground or within the area are listening on a common frequency and following common reporting procedures.
Radio communications with Moncton ACC while en route were carried out by the captain.
1.10 Aerodrome information
Grand Manan Airport has an asphalt runway (Runway 06/24), which is 3009 feet long by 75 feet wide. Runway 24, which is oriented 236° magnetic (M), has a 0.54% upslope. The aerodrome elevation is 244 feet asl; the elevation of the threshold of Runway 24 is 228 feet asl.
The airport has a type K aircraft radio control of aerodrome lighting (ARCAL) system, which activates the entire aerodrome lighting system.Footnote 26 Runway 24 has runway identification lights as well as medium-intensity threshold and runway end lights. The airport is owned, operated and maintained by the Village of Grand Manan.
1.11 Flight recorders
1.11.1 General
The aircraft was not equipped with a flight data recorder (FDR) or a cockpit voice recorder (CVR), nor was either required by regulation.
1.11.2 Benefits of recorded flight data
Numerous TSB aviation investigation reports have referred to investigators being unable to determine the reasons an accident occurred due to the absence of on-board recording devices.Footnote 27 The benefits of recorded flight data in aircraft accident investigations are well known and documented.Footnote 28
Commercially operated aircraft weighing less than 5700 kg are not usually fitted at manufacture with the system infrastructure required to support an FDR, expensive modifications would be required to install conventional FDRs in this category of aircraft.
Several affordable, stand-alone, lightweight flight recording systems are currently being manufactured that can record combined cockpit image, cockpit audio, aircraft parametric data and/or data-link messages, and that require minimal modification to the aircraft to install.
If cockpit data recordings are not available to an investigation, then the identification and communication of safety deficiencies to advance transportation safety may be precluded.
In 2013, following its investigation into the March 2011 loss of control / in-flight break-up occurrence, northeast of Mayo, Yukon (TSB Aviation Investigation Report A11W0048), the TSB found that if cockpit or data recordings are not available to an investigation, the identification and communication of safety deficiencies to advance transportation safety may be precluded. It further concluded that in the event that an accident does occur, recordings from lightweight flight recording systems will provide useful information to enhance the identification of safety deficiencies in the investigation. Therefore, the Board recommended that
[t]he Department of Transport work with industry to remove obstacles to and develop recommended practices for the implementation of flight data monitoring and the installation of lightweight flight recording systems by commercial operators not currently required to carry these systems.
Transportation Safety Recommendation A13-01
The TSB assessed TC's latest response to Recommendation A13-01 as follows:
In its response, Transport Canada has indicated proposed action in the form of an advisory circular to describe recommended practices regarding flight data monitoring programs. In addition, it will conduct focus group consultation to identify obstacles within Transport Canada's mandate and make recommendations for mitigation of those obstacles with respect to the installation of lightweight flight recording systems for commercial operators not required to carry these systems. The Board is encouraged by the intent of Transport Canada to work toward meeting the issues identified in the recommendation; however, the work is ongoing.
Therefore, the response was assessed as Satisfactory Intent.Footnote 29
1.12 Wreckage and impact information
1.12.1 General
The aircraft nose structure forward of the cockpit instrument panel was crushed and displaced to the right. The instrument panel and cockpit floor were buckled so that the cockpit volume was reduced. The fuselage structure was buckled between the cockpit and cabin sections and deformed such that the cockpit door could not be closed and latched. The cockpit door support rod had separated at the fuselage, allowing the door to travel beyond its normal range.
The non-structural interior partitions between the aft baggage area and cabin, and between the cabin and cockpit were fractured and separated from their attachment points. Both the captain's and the rear forward-facing passenger's seats had separated from their seat mounting points.

The flaps were in the full down position and the landing gear was fully extended. The left main landing gear lower leg piston fractured and separated inboard. The nose gear lower leg piston fractured and separated aft. The right main landing gear upper torque link attachment point fractured.
The left wing separated at the wing root, remaining connected to the fuselage by control cables, wires and tubing. About 6 feet of the outer portion of the left wing separated from the main wing but remained connected by control cables, wires and tubing. There was no indication of pre-impact structural failure or failure of the flight control system. Both engine mount trusses had separated from the wings. Fuel was observed in the fuel supply lines, between the emergency fuel pump and the engine-driven pump, for both engines.
TSB investigators supervised the removal of the wreckage from the accident site. The wreckage was transported to the TSB's Dartmouth, Nova Scotia, regional wreckage examination facility where further examination was carried out. Several components were removed and sent to the TSB Laboratory in Ottawa, Ontario, for detailed examination. The investigation determined that both propellers were in fine pitch and the engines were producing power at the time of impact. There was no pre-existing condition found that would have prevented the engines or propellers from operating normally.
1.13 Medical and pathological information
1.13.1 Captain
In April 2012, the captain was diagnosed with vestibular neuritis. Vestibular neuritis symptoms include dizziness or vertigo, disequilibrium or imbalance, and nausea. Even though the vestibular neuritis symptoms had been present for about 6 months, the captain continued to fly during that period and continued to fly immediately after being diagnosed. Neither the diagnosis nor the preceding symptoms were recorded on the captain's subsequent Medical Examination Report (MER), nor were they reported directly to TC.
The captain's last TC Category 1 medical examination was completed in early June 2014. In July 2014, the captain had experienced an episode of weakness, confusion and blurred vision due to an allergic reaction to a prescription medication. Although the captain had a medical examination, TC had no record of the examination.
In both the April 2012 and the July 2014 medical examinations, conducted at the emergency department of a local hospital, no record was made by the hospital staff indicating the patient was a pilot.
Notwithstanding, the investigation determined that there was nothing to indicate that the captain's performance was degraded by physiological factors or incapacitation.
1.13.2 Transport Canada medical requirements for pilots
The primary activity of TC's Civil Aviation Medicine Branch (CAM) is the performance of medical assessments required for the certification of licensed aviation personnel. CARs Standard 424.17(3)(a) states that:
The purpose of the medical examination is to determine whether an applicant meets the standards that apply in respect of the issuance of the Medical Certificate that is needed to issue a particular permit, licence or rating […].Footnote 30
With aviation medical examinations, TC is chiefly concerned with managing the risk to aviation over the short term, that is, the validity period of the medical certificate. As such, TC reviews the risk of incapacitation for the period of the licence.
It is the responsibility of the civil aviation medical examiner (CAME) to interview and perform a complete examination on all applicants. CARs Standard 424 requires the CAME to examine the applicant in accordance with medical practices recognized by the medical profession, and with the personnel licensing standards. The CAME is usually the only person who physically examines the applicant and makes a recommendation for medical certification. TC considers the CAME to be the most important link in the medical certification process.
The CAM Handbook for Civil Aviation Medical Examiners (TP 13312) stipulates that, during the medical examination, there is a shared responsibility, with the onus on the applicant to report any symptoms and a requirement for the CAME to conduct a careful and thorough examination.
Pilots are required to report on their TC medical report form all visits to medical professionals. CARs Standard 424 requires applicants to sign the Aviation MER, which states that the information provided is complete and correct, and that they are aware that it is an offence to knowingly make a false declaration.
1.13.3 Reporting requirements
CARs 404.06 prohibits a pilot from exercising the privileges of their licence if they suffer from an illness, injury or disability that could impair their ability to exercise those privileges safely. The Transport Canada Aeronautical Information Manual (TC AIM) addresses the issue of medical reporting. The TC AIM reminds pilots that before they have a medical examination by any physician, they must identify themselves as a holder of a pilot's licence, and it states that the attending physician must notify TC of any finding that may constitute a hazard to aviation safety.
Subsection 6.5(1) of the Aeronautics Act requires physicians to report to TC any holder of a Canadian aviation document who they believe (on reasonable grounds) may, for medical reasons, constitute a hazard to aviation safety. Section 26 of the Canadian Medical Association's CMA Driver's Guide, 8th Edition, which addresses aviation, states that, “Physicians are required by law to report to regional aviation medical officers of Transport Canada any pilots, air traffic controllers or flight engineers with a medical condition that could affect flight safety.”Footnote 31
Section 26 of the CMA Driver's Guide also alerts physicians to aspects of medical fitness that are of unique importance to aircrews and provides a list of common reportable conditions. If the physician is certain that a condition poses a risk to aviation, the condition must be reported. If uncertain, the attending physician can contact a regional aviation medical officer (RAMO) for guidance.
The CMA Driver's Guide requires any medical condition that affects balance organs or vision to be reported to TC, as it may induce or exaggerate dangerous spatial disorientation. Therefore, vestibular neuritis and episodes of weakness, confusion and blurred vision are medical symptoms that must be reported to TC.
In this occurrence, even though the captain's general practitioner, who was also the CAME, was aware of the April 2012 and the June 2014 medical examinations, neither medical condition was reported to the RAMO.
TSB investigations have previously identified the issue of information not being reported to TC.Footnote 32
1.14 Fire
Not applicable.
1.15 Survival aspects
1.15.1 Seatbelts
During an impact, an unrestrained passenger can be thrown about the cabin, possibly contacting aircraft structures and/or other occupants, thereby increasing the risk of injury or death to themselves and to others.
The occurrence aircraft's passenger seats were equipped with seatbelts, and a seatbelt extension was readily available. Post-accident examination revealed that the paramedic's seatbelt was fastened and adjusted to a length that would have been too short for the paramedic's waist. There was no indication that the state of the seatbelt had been altered during post-accident emergency response activities.
1.15.2 Cargo restraints
CARs 602.86(1) prohibits the operation of an aircraft unless carry-on baggage, equipment and cargo are
- (a) stowed in a bin, compartment, rack or other location that is certified in accordance with the aircraft type certificate in respect of the stowage of carry-on baggage, equipment or cargo; or
- (b) restrained so as to prevent them from shifting during movement of the aircraft on the surface and during take-off, landing and in-flight turbulence.
The PA-31 interior includes a baggage compartment aft of the main cabin door which will accommodate up to 200 pounds of cargo. Regarding the stowage of baggage, the AFM states, “Baggage tie down straps should be used in all baggage areas for safe and secure stowage of baggage.”Footnote 33
Post-accident examination revealed that tie-down straps were not used, and medical equipment bags were found forward of the aft baggage compartment area.
The Aeromed Systems, Inc. ambulance unit was equipped with seatbelt-style cargo restraints to secure medical equipment. In the occurrence aircraft, a single fitting with an attached buckle had been installed on the left outboard seat track, between the rear-facing seat and the cabin door. ANB's practice was to place the defibrillator on the floor and secure it in place by fastening the restraint to the buckle.
Post-accident examination found that the defibrillator was loose in the cabin, and the restraint and buckle were not fastened.
1.15.3 Safety briefing
CARs 703.39(1) states, “The pilot-in-command shall ensure that passengers are given a safety briefing in accordance with the Commercial Air Service Standards [CASS].”
The CASS require a safety briefing to be carried out prior to takeoff, and if no additional passengers embark on subsequent flights on the same day, it may be omitted.
According to ANB's contract with Atlantic Charters, the operator was to provide the flight paramedics with annual flight safety training. Atlantic Charters and ANB had subsequently agreed to provide Aircraft Orientation and Safety Training to the flight paramedics every 6 months. This training was in lieu of providing a safety briefing prior to takeoff at the start of each flight, and included topics such as the use of seatbelts, the securing of various types of medical devices/gear, and the location and operation of safety devices. The occurrence paramedic had completed the most recent training in April 2014.
According to TC's Guide to Air Ambulance Operations:
[…] medical attendants are not normally crew members under the Canadian Aviation Regulations. They may be designated as crew members provided they receive approved flight attendant training. In this case, medical attendants may be assigned duties such as passenger briefing, evacuation, and look-out for helicopter landings, otherwise these functions remain the responsibility of the flight crew.Footnote 34
The paramedics were not designated as part of the flight crew, they did not receive any approved flight attendant training, nor were they required to.
1.16 Tests and research
1.16.1 TSB laboratory reports
The following TSB laboratory reports were completed in support of this investigation:
- LP 181-2014 – Instrument and lamp examination
- LP 182-2014 – Cell phone NVM [non volatile memory] examination
- LP 187-2014 – Cell phone examination
- LP 219-2014 – GPS [global positioning system] Analysis
- LP 226-2014 – Examination of exhaust pipes
- LP 049-2015 – Radar Data Analysis
1.17 Organizational and management information
1.17.1 General
Atlantic Charters is a privately owned company that has been operating from Grand Manan since 1982. The owner and founder of the company, who was also the occurrence captain, held the positions of accountable executive, operations manager, chief pilot and maintenance coordinator. This individual was responsible for the company business decisions including contract negotiations. The owner had over 30 years of flying experience from the Grand Manan Airport and was very familiar with the surrounding environment as well as the challenges associated with flying in the local weather conditions.
Atlantic Charters conducts CARs subpart 703 air taxi operations, providing domestic and international air charters. The company had been providing patient transfer charter services for over 30 years, with the majority of this work being carried out as single-pilot operations. At the time of the accident, the company employed 5 pilots, including the owner and a member of the owner's family. The company operated a Piper Cheyenne III, 3 Piper Navajos, a Piper Seneca, and a Cessna Skyhawk. With the exception of the owner and the owner's family member, the company typically hired pilots with limited flying experience who normally stayed with the company for about 2 years before moving on.
With the exception of maintenance tasks designated as elementary work, all maintenance was carried out by an AMO. Atlantic Charters did not have any maintenance staff or approved maintenance capabilities.
1.17.2 Atlantic Charters flight safety
Atlantic Charters did not have a safety management system (SMS), nor was it required by regulation to have one.
There was no documented flight safety program at Atlantic Charters. According to the COM, the operations manager was responsible for safe flight operations, and the chief pilot was responsible for the professional standards of the flight crew under his authority.
1.17.3 Atlantic Charters operations manual
1.17.3.1 Navigation tools
According to regulations, if conducting an IFR flight, “all of the necessary current aeronautical charts and publications covering the route of the proposed flight and any probable diversionary route”Footnote 35 must be carried on board.
For flights between Grand Manan and Saint John, the required current charts and publications would include the CAP 7, the Enroute Low Altitude Chart, and the Canada Flight Supplement (CFS).
Post-accident examination found only an outdated CFS (expired 24 July 2014) on board the aircraft.
Regulations state that if an aircraft is operated on an IFR flight and using database-dependent navigation equipment such as a GPS, the current database covering the route must be carried on board.Footnote 36
Post-accident examination revealed that the GPS database had expired on 01 May 2014.
For a CARs subpart 703 company to conduct a GPS approach on revenue flights, it must obtain TC Operations Specification (OPS Spec) 100. To be granted OPS Spec 100, a company must have ground and flight training on GPS approaches and standard operating procedures (SOP) that address the use of GPS during approach operations when flying with 2 crew members, and must demonstrate competency in using the equipment.
Atlantic Charters did not have OPS Spec 100. However, its typical practice was to use the GPS when conducting approaches on Runway 24.
1.17.4 Standard operating procedures
SOPs represent an important information resource available to pilots to assist with problem solving and decision making. SOPs are designed to help pilots operate within organizational risk-management boundaries and maintain situational awareness through the use of predetermined procedures and standardized phraseology.
Atlantic Charters had developed SOPs in 2012 to meet the requirements of ANB's latest contract. The SOPs mention aspects of communications between pilots, such as standard altitude calls, standard take-off briefing, and the fact that all checklists are to be completed verbally (challenge and response).
A challenge-and-response checklist requires that the pilot not flying read the item and the pilot flying respond with the appropriate wording (e.g., set, on, complete, etc.). To carry out the challenge-and-response checklist procedures, it would be necessary for the captain and FO to communicate effectively with each other.
When flying with this captain, the FO was expected to learn and gain experience by observing what the captain did. The FO would follow the actions of the captain by reviewing the checklist. During the occurrence flight, since no headset was available to the FO, the checklists were not completed in a challenge-and-response manner.
During the approach, the FO was monitoring the ASI and GPS, as well as looking outside to locate the runway.
1.18 Additional information
1.18.1 Air ambulance services in Canada
TC considers all non-government air ambulance services as commercial air services, subject to Part VII of the CARs. Therefore, there is no requirement for a company to have an amendment to its operations specification in order to operate an air ambulance service.
According to TC's publication Guide to Air Ambulance Operations, as certain situations may place a great deal of stress on pilots, companies “contracting for air ambulance services may wish to specify requirements over and above the minimum required by regulation such as two pilots on all flights, [and] additional training and experience…”Footnote 37
The Guide to Air Ambulance Operations also states:
A successful company safety management program can have a positive effect on many aspects of air ambulance operations and one of the most important is pilot judgment. Training in Pilot Decision Making (PDM) and Cockpit Resource Management (CRM) are developments in the aviation industry and are particularly applicable to the often life and death nature of the air ambulance mission.Footnote 38
1.18.1.1 Ambulance New Brunswick
Since 2007, ANB has been operating as the province's ambulance service, providing land and air ambulance services throughout the province. ANB responds to nearly 100 000 calls each year.
ANB's Air Ambulance Service (referred to as AirCare) consists of a dedicated fixed-wing aircraft and crew, which are provided under contract. During the 2013–2014 fiscal year, AirCare completed about 500 patient transfers, of which 46% were classified as emergent or urgent, and 54% were classified as non-urgent.
ANB's MCMC is the centralized ambulance dispatch centre. The MCMC is staffed by emergency medical dispatchers, who respond to emergency medical calls, coordinate inter-facility transfers, and dispatch emergency medical services land and air crews. When ANB receives a request for a patient transfer, the attending physician will consult with the provincially appointed medical control physician. They will determine if the patient requires care that is outside the primary care paramedic scope; this type of patient is referred to as a high acuity patient. For high acuity patients, the preferred method of transfer is through AirCare.
ANB also contracts air services, on an as-needed basis, from Atlantic Charters for non-urgent patient transfers from Grand Manan. Atlantic Charters may transport high acuity patients when the sending physician, medical control physician, and receiving physician (as required) agree that the Grand Manan medical facility can provide an appropriate escort, such as a registered nurse, and that it would be more expeditious than waiting for AirCare. Atlantic Charters carried out about 100 patient transfers per year.Footnote 39
1.18.1.2 Ambulance New Brunswick contract requirements
AirCare has been provided by the same operator since before ANB was established. The current contract requires the pilot-in-command to have a minimum of 2000 hours total time, with 500 hours as pilot-in-command of a multi-engine aircraft, and 100 hours on the specific type used for the service. The FO is required to have a minimum of 500 hours total time and a minimum of 100 hours on a multi-engine aircraft. In an effort to make all flights as safe as possible, the operator's flight crew training program must emphasize a challenge-and-response checklist, and include cockpitFootnote 40 resource management.
ANB's contract with Atlantic Charters requires 2 pilots who are certified and qualified to operate the type of aircraft used. The 2-pilot requirement is a change that came about during the last contract negotiation (2012) with Atlantic Charters. ANB had conducted informal research and determined that 2 pilots should offer a higher level of safety; more specifically, if 1 pilot became incapacitated and could no longer perform their duties, someone else could fly the aircraft. Up until the latest contract, Atlantic Charters had been providing the ANB patient transfer service using a single pilot.
ANB has indicated that the wording of the 2 contracts, with the exception of some minor changes, had been in place prior to ANB's existence. ANB has also indicated that it has limited aviation knowledge and experience, and was unfamiliar with what was meant by terms such as challenge-and-response and CRM.
1.18.2 Crew resource management
Atlantic Charters does not have a formal crew resource management (CRM) training program, nor is such training required by regulation or as part of ANB's contract requirements. However, Atlantic Charters indicated that informal CRM training was carried out.
When operating in a 2-crew environment, pilots must successfully interact with each other, their aircraft, and their environment to effectively manage threats, errors, or undesired aircraft states that may be encountered. CRM training focuses on critical cognitive and interpersonal skills with the objective of reducing human error in aviation. Research has shown that flight crews with recent CRM training are better able to deal with novel situations than flight crews without recent CRM training.Footnote 41
From a CRM standpoint, effective communication plays a critical role in the alignment of the crew's understanding of the situation. However, communication skills require practice and reinforcement to be effective, particularly during periods of high workload, such as during an instrument approach or an abnormal situation.
Modern CRM programs highlight barriers to effective communication and provide multiple communication strategies that allow individuals to select the most appropriate strategy, depending on the severity of the situation, the time available, and the other person(s) involved in the communication process.
Situational awareness is defined as “the continuous extraction of environmental information, the integration of this information with previous knowledge to form a coherent mental picture, and the use of that picture in directing further perception and anticipating future events.”Footnote 42
Flight crew actions need to be based on a common understanding of the current state of the aircraft, the intended flight plan, and the threats to these activities in order to perform in a coordinated, efficient, and safe manner. This common understanding between the crew members is referred to as team or shared situational awareness.Footnote 43, Footnote 44 When this understanding is consistent, crews are better able to effectively anticipate and coordinate their actions toward achieving their common goal.
Shared situational awareness is developed and maintained by a crew through a number of discrete and continuous behaviours. Discrete behaviours include flight planning, in-flight briefings, and identification of key points in the flight, such as attaining minimum altitudes. These activities are planned checkpoints to describe current state and future plans, and to provide an opportunity for checking that all crew members have a common understanding.
Continuous behaviours include threat and error management, callouts of changes of aircraft state and instrument setting/mode, and communication of changes to plans. These behaviours ensure that information and state changes are communicated between crew members to update the shared situational awareness on an ongoing basis. Such continuous behaviours are influenced by the training and operational approach taken by operators.
Following its investigation into a collision with terrain which occurred in Sandy Bay, Saskatchewan, in January 2007 (TSB Aviation Investigation Report A07C0001), the TSB concluded that some operators are unlikely to provide CRM training in the absence of a regulatory requirement to do so. Therefore, some commercial pilots may be unprepared to avoid, trap, or mitigate crew errors encountered during flight. In light of the risks associated with the absence of recent CRM training for air taxi and commuter crew members, the Board recommended that
[t]he Department of Transport require commercial air operators to provide contemporary crew resource management (CRM) training for Canadian Aviation Regulations (CARs) subpart 703 air taxi and CARs subpart 704 commuter pilots.
Transportation Safety Recommendation A09-02
The TSB report on its investigation into the August 2011 controlled flight into terrain accident which occurred in Resolute Bay, Nunavut (TSB Aviation Investigation Report A11H0002) identified ineffective crew interactions as a significant contributing factor to the accident. This investigation also found that if operators do not take steps to ensure that flight crews routinely apply effective CRM practices during flight operations, risk to aviation safety will persist. Therefore, the Board expressed concern that, without a comprehensive and integrated approach to CRM by TC and aviation operators, flight crews may not routinely practice effective CRM.
TSB Recommendation A09-02 was first issued in 2009. TC’s project plan has been under development since December 2012. Work continues on the development of standards for CRM. A Notice of Proposed Amendment on CRM standards has been developed and is expected to be published in 2016.
The Board is encouraged that action on this recommendation is nearing completion. The proposed course of action should substantially reduce or eliminate the safety deficiency identified in Board Recommendation A09-02. Until the standards are amended and fully implemented, this safety deficiency will continue to exist. The TC response was last assessed as Satisfactory Intent.
1.18.3 Controlled flight into terrain
Controlled-flight-into-terrain (CFIT) accidents occur when an airworthy aircraft under the control of the pilot is inadvertently flown into the ground, water, or an obstacle. In these cases, pilots are unaware of the danger until it is too late. This type of accident often happens when visibility is low, at night, or in poor weather conditions. Such conditions reduce a pilot's situational awareness of surroundings and make it difficult to tell whether the aircraft is too close to the ground. Between 2003 and 2013, there were 117 CFIT accidents in Canada, which resulted in 121 fatalities. Collisions with land and water account for 3% of all accidents, but nearly 18% of all fatalities.
In a study of airline accidents, the Flight Safety Foundation (FSF) noted that CFIT was the leading category of approach-and-landing accidents.Footnote 45 Its findings included the following:
- “omission of action/inappropriate action” by a flight crewmember was identified as the most common primary causal factor. This usually referred to the crew continuing descent below the decision height (DH) or minimum descent altitude (MDA) without adequate visual reference;
- the second most common primary causal factor was “lack of positional awareness in the air,” generally resulting in controlled flight into terrain (CFIT);
- [a majority of] CFIT occurrences were during poor-visibility conditions;
- disorientation or visual illusions […] were involved in 21.1 percent of all occurrences, […][with a] lack of vigilance, assigning a lower priority to monitoring primary instruments, and a lack of training for and awareness of such illusions [identified as] associated factors.Footnote 46
The FSF has determined that the majority of CFIT accidents occurred when aircraft were on final approach to the runway.Footnote 47 Some common causes of CFIT accidents are
- loss of situational awareness,Footnote 48
- unstable approaches, and
- poor communications.
Atlantic Charters' COM required pilots to undergo initial CFIT training, then biennial recurrent training. This training included factors that may lead to CFIT accidents and incidents, CFIT prevention strategies, methods of improving situational awareness, and escape manoeuvre techniques and profiles. The captain had received recurrent CFIT training in June 2013 and the FO had completed it in April 2014.
1.18.4 Visual illusions
The FSF Approach and Landing Accident Reduction (ALAR) Task Force's Briefing Note 5.3 states:
Visual illusions result from the absence of visual references or the alteration of visual references, which modify the pilot's perception of his or her position (in terms of height, distance and/or intercept angle) relative to the runway threshold.Footnote 49
The briefing note also states:
Visual illusions are most critical when transitioning from instrument meteorological conditions (IMC) and instrument references to visual meteorological condition (VMC) and visual references.Footnote 50
Flying in light rain, fog, mist, or darkness creates an illusion of being too high. If this illusion is not recognized, a pilot may push the nose forward, descending below the ideal approach path. Entering a fog layer also creates the illusion of pitching up. The pilot who does not recognize this illusion will steepen the approach, often quite abruptly.Footnote 51
The Airbus Operational Briefing Notes state that:
The following crew actions and the consequences are often cited in the analysis of approach-and-landing incidents or accidents resulting from visual illusions:
[…]
- Natural tendency to descend below the glide slope or the initial glide path (i.e., “ducking under”);
- Inability to arrest the rate of descent after descending below the intended glide path (i.e., late recognition of the flattening of runway and runway environment) […]Footnote 52
The TC Human Factors for Aviation Basic Handbook (TP 12863E) states that landing illusions can affect even the most experienced pilots.
1.18.5 Flying through clouds
The PA-31 Pilot Operating Handbook contains the following warning:
Turn off anti-collision lights […] during flight through cloud, fog or haze.Footnote 53
The Flight Safety International Navajo Pilot Training Manual, Models 310, 325, 350 and T1020, issues a warning which states:
Strobe lights should not be operating when flying through overcast and clouds since the reflected beam may produce spatial disorientation.Footnote 54
Landing lights and strobe lights are typically not used when flying through cloud, fog or haze because their illumination can cause reflection or glare that can adversely affect the pilot, making it more difficult for the pilot to identify outside lights.
1.18.6 Descent rates
1.18.6.1 First approach
The aircraft began its approach from 1900 feet asl, 4.87 nm from the threshold. The aircraft continued on a constant descent until it was at 500 feet asl, at 1.2 nm from the threshold. The aircraft's ground speed was 90 knots. At this ground speed, the descent rate would have been approximately 470 fpm. This rate of descent is consistent with what the CAP identifies for a constant descent angle for a GPS approach.
When the aircraft was 0.26 nm from the threshold, it was at 500 feet asl and at 90 knots. To touch down at the threshold from this point would require a descent rate of about 1590 fpm. This descent rate does not take into account the need for the aircraft to flare prior to touching down on the threshold.
1.18.6.2 Second approach
On the second approach, at 0.56 nm from the threshold, the aircraft was level at 500 feet asl at 90 knots.
To touch down at the threshold from this point would require a descent rate of about 730 fpm. To touch down on Bancroft Road from this point would require a descent rate of about 1215 fpm. These descent rates do not take into account the need for the aircraft to flare before touching down.
1.18.7 Transport Canada oversight
1.18.7.1 General
TC expects companies to proactively manage the safety of their operations—where risks are managed to acceptable levels—and to have programs in place to ensure their continued compliance with all regulatory requirements. TC's surveillance program is designed to assess whether an aviation company has implemented appropriate and effective systems; specific systems-based surveillance inspections are conducted at intervals based on risk indicators. The program is targeted at key systems determined by certificate type and whether or not the company is required to have an SMS. The surveillance program is based on a systemic approach to managing risk and includes the following steps: documentation review; on-site interviews and on-site sampling conducted by inspectors; and production of a report with findings of systemic deficiencies. This allows inspectors to understand how a company plans to meet a specific regulatory requirement. The sampling portion is where inspectors select specific areas, or outputs, to test compliance with that system and to the applicable regulations.
Program validation inspections (PVI) are conducted on a routine schedule, and use risk indicators to adjust the frequency of inspection, as necessary. During a PVI, the TC team will conduct interviews, gather evidence to support observations, and analyze those observations. It will then determine if the operator is in compliance with regulations and whether its SMS is effective (if the organization is required to have an SMS). The TC PVI team will also prepare any findings of non-compliance and document the results of the on-site review.
A process inspection (PI) is another surveillance tool employed by TC to determine whether an operator's processes meet regulatory requirements and are functioning as intended. A PI may also generate findings. The PI report shall indicate whether the process meets applicable regulatory requirements and is being followed as published in approved company manuals, or whether the process is not documented, not implemented, or not effective.
In principle, any process required by regulation may be the focus of a PI or a PVI. Targeted PIs across a range of areas have the potential to identify a lack of compliance with regulations requiring those processes.
1.18.7.2 Oversight at Atlantic Charters
TC verified that Atlantic Charters was in compliance with applicable regulations and standards by carrying out PVIs and PIs.
Prior to the accident, Atlantic Charters had been on a 3-year surveillance cycle.
The TSB reviewed the surveillance activities carried out by TC and the company's responses for the 3 years preceding the occurrence. During this period, TC carried out 2 PVIs and 1 PI, none of which examined aircraft weight and balance or continuing airworthiness.
In June 2011, TC carried out a PVI of Atlantic Charters on the operational control described in the approved COM. The inspection identified 1 finding: the COM outlined a procedure which had been cancelled by Advisory Circular 700-018, which had come into effect 13 days before the inspection.Footnote 55 Atlantic Charters submitted a corrective action plan which was accepted by TC in August 2011.
In February 2012, TC carried out a PVI of Atlantic Charters focused on quality assurance for air operations maintenance. The inspection identified 2 findings, which included items such as audit reports not available, technical records not available at the time of the inspection, and missing personnel and training records. Atlantic Charters submitted a corrective action plan which was accepted by TC in November 2012. Atlantic Charters’ corrective action plan indicated that the records had been lost in a house fire.
In June 2012, TC carried out a PI of Atlantic Charters in order to verify compliance with regulatory requirements. The inspection involved an off-site file review, and familiarization with the company's training program and aircraft equipment requirements. The PI identified 1 finding: the COM had 7 sections which no longer met the Commercial Air Services Standards. Atlantic Charters submitted a corrective action plan which was accepted by TC in August 2012.
1.18.8 Office of the Auditor General report
In the spring of 2012, the Office of the Auditor General (OAG)Footnote 56 published the report of an audit it conducted to determine whether TC has adequately managed the risks associated with overseeing its civil aviation safety program.
The OAG report issued recommendations with respect to the number of surveillance activities conducted, the manner in which surveillance was conducted and documented, and management oversight of surveillance activities. The report did not comment on the focus of surveillance activities except to note that in moving to SMS, the role of inspectors was changing from being auditors of regulatory compliance to taking on the role of system evaluators while conducting traditional audits as necessary.
1.18.9 Organizational safety culture
According to the International Civil Aviation Organization (ICAO), “Organizational culture sets the boundaries for accepted executive and operational performance by establishing the norms and limits […]” and “[…] provides a cornerstone for managerial and employee decision making.”Footnote 57 Culture is deeply ingrained, and its impact on safety may not be readily apparent to those working within those cultures.
One of the largest influences on safety culture is management commitment and style. ICAO has described the role of management in creating a positive organizational safety culture as follows:
Those in the best position to effect accident prevention by eliminating unacceptable risks are those who can introduce changes in the organization, its structure, corporate culture, policies and procedures, etc. No one is in a better position to produce these changes than management.Footnote 58
Organizations must strike a balance between safety and production by managing risks present in their operation. The challenge for an organization is to operate efficiently while minimizing safety risks. The reality within many organizations is that production and operational concerns may at times seem more pressing since they are more measurable and provide immediate feedback in terms of results. Therefore, in the minds of decision-makers, operational concerns may be more salient than concerns dealing with safety. In this context, organizations may unwittingly introduce risk into their operations.
Organizations differ considerably in the level of risk they tolerate within their operations. Organizations that take proactive steps to identify and mitigate risks are considered to have positive safety cultures, while other organizations with poor safety cultures knowingly or unknowingly operate with higher levels of risk. An organization that operates with significant risk faces a greater potential for an accident.
The traditional approach to safety management is based on compliance with regulations and a reactive response to incidents and accidents. Although compliance with safety regulations is fundamental to the development of sound safety practices, organizations that simply comply with the standards set by the regulations are not well situated to identify emerging safety problems. According to the ICAO Safety Management Manual:
As global aviation activity and complexity continue to grow, […] traditional methods of managing safety to an acceptable level [become] less effective and efficient. Different, evolved methods of understanding and managing safety are necessary.Footnote 59
As summarized in TSB Aviation Investigation Report A07A0134,
Modern safety management principles promote a proactive search for hazards, identification of risks, and the best defences to reduce risk to an acceptable level. These principles must be embedded within an organization's management system so that safety policies, planning, procedures, and performance measurement are integrated into day-to-day operations.
1.18.10 TSB Watchlist
The Watchlist is a list of issues posing the greatest risk to Canada's transportation system; the TSB publishes it to focus the attention of industry and regulators on the problems that need addressing today.
1.18.10.1 Approach-and-landing accidents are a TSB 2014 Watchlist issue
As this occurrence demonstrates, landing accidents continue to occur at Canadian airports representing a significant risk to the safety of air transportation.
1.18.10.2 Safety management and oversight are a TSB 2014 Watchlist issue
Transportation companies have a responsibility to manage safety risks in their operations.
The TSB urges TC to implement regulations requiring all operators to have formal safety management processes, and for TC to oversee these processes.
When companies are unable to effectively manage safety, TC must not only intervene, but do so in a manner that succeeds in changing unsafe operating practices.
1.19 Useful or effective investigation techniques
Not applicable.
2.0 Analysis
There was no indication of an aircraft component or system failure during the occurrence flight and fatigue was not considered a factor. The analysis will focus on possible scenarios as to why the serviceable aircraft was inadvertently flown into the ground, the culture and practices of the company, and Transport Canada (TC) oversight.
2.1 Weather
During the initial telephone conversations with Ambulance New Brunswick (ANB), Atlantic Charters indicated a concern with the weather for the return flight to Grand Manan, New Brunswick. A post-occurrence assessment by Environment Canada found that, at the time of the accident, the weather was most likely dense fog with extremely limited visibility.
The first approach followed a constant descent angle consistent with the area navigation (RNAV) approach for the runway. Had the aircraft continued on this profile, it would have been in a position to land on Runway 24. However, the aircraft levelled off at 500 feet above sea level (asl), and remained at that altitude for at least 40 seconds, likely because the captain did not see the required visual references. At 0.26 nautical mile (nm) from the runway, for the aircraft to touch down at the threshold, it would have required a descent angle much steeper than the approach profile normally flown for a visual approach. This is likely why a go-around was carried out.
Following the go-around, the captain flew about 7 nm downwind from the threshold before intercepting the final approach at 1000 feet asl. About 3 minutes later, the aircraft started to descend, then levelled off at 500 feet asl for 24 seconds, which is inconsistent with what would be done during a visual approach. The second approach was flown with the landing lights and the aircraft strobes off, which is in accordance with the published warnings when flying through fog or cloud. Shortly after the accident, the first responders could not see the aircraft due to the limited visibility. Therefore, it is likely that the weather at the time of both approaches was such that the captain could not see the necessary visual references to ensure a safe landing.
2.2 Controlled flight into terrain
This occurrence involved several of the most common factors associated with controlled flight into terrain (CFIT) accidents. In particular, it involved a non-precision instrument approach conducted at night over a dimly lit, sparsely populated area, and with limited visibility in fog.
Under the conditions present at the time of the accident, the road would likely have been indistinguishable from the surrounding terrain.
The following scenarios were considered:
2.2.1 Scenario 1
On the second approach, the descent was initiated at 0.56 nm from the threshold, even though during the first approach it was not possible to see the runway until the aircraft was less than 0.26 nm from the threshold. Therefore, it is possible that the captain initiated the second descent to get under the weather in an attempt to see the runway lights early enough to ensure a safe landing.
The contact across the road is consistent with the captain not seeing the required visual references to ensure a safe landing.
2.2.2 Scenario 2
One of the most common causes of CFIT accidents is a loss of situational awareness. Visual illusions contribute to the loss of situational awareness, and these illusions are caused by the absence of visual references, which cause the pilot to lose depth perception. At the time of the accident, the weather and terrain conditions were conducive to a visual illusion, which would create the illusion that the aircraft was too high.
If the captain believed that the aircraft was too high, then it is possible that a steep rate of descent was initiated. The rate of descent from the last radar point was calculated to have been about 1215 fpm, which is steeper than the typical descent path.
The contact across the road is consistent with the late recognition of the flattening of the runway and the captain not seeing the required visual references to ensure a safe landing. This is typical of an approach-and-landing accident resulting from visual illusions.
Therefore, it is possible that the captain succumbed to a visual illusion during the descent to Runway 24.
It could not be determined which of these scenarios was more likely to have been the cause of the accident; however, not seeing the required visual references to ensure a safe landing is the significant factor in both scenarios. The first officer (FO) was focused on locating the runway and was unaware of the captain's actions during the descent.
2.3 Crew resource management
Because most of Atlantic Charters' flying operations were carried out with a single pilot, the company did not provide any formal crew resource management (CRM) training, nor was such training required by regulation. Research has shown that CRM-trained crews operate more effectively as teams and cope more effectively with non-routine situations than crews without CRM training.
A key element of successful CRM is effective communication. Since only the captain was wearing a headset, communication between the 2 pilots would have been limited to hand-gesturing and/or yelling above the ambient noise, neither of which are effective ways to communicate. The captain chose to continue with the flight even after realizing that there was only 1 headset available for the 2 pilots. The captain typically operated as a single pilot; therefore, it is likely that the captain did not consider the need to communicate effectively with the FO to be significant enough to obtain a second headset. Because the captain and FO could not communicate effectively with each other, the FO would not have been aware of the captain's intentions nor of the captain's radio communications. Because of this ineffective communication, shared situational awareness between the 2 pilots was reduced. If crew members are unable to communicate effectively, then they are less likely to anticipate and coordinate their actions, which could jeopardize the safety of flight.
CRM requires practice and reinforcement to be effective. If CRM training is not provided, used and continuously fostered, then there is a risk that pilots will be unprepared to avoid or mitigate crew errors encountered during flight.
2.4 Weight and balance
The investigation could not determine if the aircraft was within its weight and balance limitations because the aircraft's actual basic empty weight could not be confirmed, and there were a number of undocumented discrepancies in the recorded weights. If an actual weight and balance cannot be determined, then the aircraft may be operating outside of its approved limits, which could affect the aircraft's performance characteristics.
The company's pre-computed weight and balance form did not include a line item to indicate nacelle fuel. If pre-computed weight and balance forms do not include standard items, then it increases the likelihood of omissions in weight and balance calculations, which increases the risk of inadvertently overloading or incorrectly loading the aircraft.
2.5 Elementary work
A company pilot had installed the air ambulance system the day before the occurrence. Because the company's maintenance control manual (MCM) did not include this as elementary work, no company employee would have been approved to carry out this task. If organizations carry out a maintenance task that they consider to be elementary work and the task is not approved as elementary work, then there is a risk that the aircraft will not conform to its type design, which could jeopardize the safety of flight.
The individual who installed the air ambulance system had not received any approved training to do so. The design of the air ambulance system is such that it requires all adapter plate bolts to be installed correctly to ensure that the system meets airworthiness standards. Post-occurrence examination revealed that 4 of the 16 bolts which secure the cross tubes to the plates had not been tightened, and that the adapter unit had moved forward and partially separated from the seat tracks. If individuals are performing maintenance tasks for which they have not received approved training, then there is a risk that the task will not be performed in accordance with the manufacturer's instructions. If components are not installed in accordance with the manufacturer's instructions, then occupants are at a greater risk of injury or death during an incident or accident if these components are not properly secured.
According to regulations, when elementary work is performed, the task must be recorded in the aircraft's journey log. Even though the occurrence aircraft had been operated in both passenger and MEDEVAC configurations and Atlantic Charters' pilots had performed elementary work on the aircraft, there were no entries in the aircraft journey log. If organizations do not record when maintenance is carried out, then the proper completion of tasks cannot be confirmed, and there is a risk that the aircraft will not conform to its type design, which jeopardizes the safety of flight.
2.6 Airworthiness
An aircraft is considered airworthy when it is maintained in accordance with the limitations applicable to its type design.
A supplemental type certificate (STC) is an approved change to the aircraft's type design and, therefore, all STC information that supersedes or supplements the basic aircraft flight manual (AFM) and aircraft maintenance manual (AMM) must be complied with to ensure that the aircraft is airworthy. Atlantic Charters had installed the air ambulance system in the occurrence aircraft. There was no record of TC having approved this STC for installation in the occurrence aircraft; there was no record of the installation in any of the occurrence aircraft's technical documents; and Atlantic Charters could not provide any of the required STC supporting documentation. If an aircraft is modified without regulatory approval and without supporting documentation, then the aircraft is not in compliance with all applicable standards of airworthiness, which could jeopardize the safety of flight.
Prior to importation into Canada, the occurrence aircraft had been modified to increase its gross take-off weight in accordance with an STC. Post-occurrence examination revealed that the aircraft had been modified such that it was no longer in compliance with the STC changes, and that these changes were not recorded in the aircraft's technical records. If an operator undertakes unapproved changes to an STC, then there is a risk that the aircraft will not be airworthy, which could jeopardize the safety of flight.
2.7 Company safety culture
According to the International Civil Aviation Organization (ICAO), management is in the best position to create a positive organizational safety culture. To accomplish this, management needs to develop and foster an environment where the organization does more than simply comply with the regulations. Management can make the necessary changes to company structure, culture, policies and procedures to ensure that the company pro-actively influences accident prevention by eliminating unacceptable risks.
Since the owner of Atlantic Charters was also the accountable executive and held all of the management positions, the owner would have been responsible for fostering the manner in which safety was managed and for establishing the company's safety culture.
An organization's culture sets the boundaries for what is considered acceptable performance. These norms and limits are what managers and employees use when making decisions.
Atlantic Charters did not provide supporting documentation which explained the discrepancies in the weight and balance information. Maintenance tasks were being carried out without the approved training, and much of this work was not being recorded in the aircraft's journey log. By not complying with the requirements of the STCs, the company was not ensuring that the aircraft met airworthiness standards. Because these practices had been ongoing, they would have been considered normal company practice and, therefore, a reflection of what management considered acceptable performance, i.e., the company's safety culture.
Organizations respond to operational pressures because these priorities are clearly measurable and provide immediate feedback. Under these pressures, concerns dealing with safety may become less prominent, and organizations may unwittingly introduce risk into their operations.
The traditional approach to safety management has been shown to be ineffective in identifying potential hazards and associated risks. Organizations that comply with the minimum standards and manage safety using the traditional approach are not well situated to identify emerging safety problems. In today's aviation environment, modern safety management practices must be embedded within an organization's management system, so that the management of safety is integrated into day-to-day operations. If organizations do not use modern safety management practices, then there is an increased risk that hazards will not be identified and risks mitigated.
2.8 Transport Canada oversight
In the 3 years preceding this occurrence, TC's surveillance activities had not identified the discrepancies in the company's operating practices related to weight and balance and continuing airworthiness. Consequently, these practices persisted.
While a move toward safety management systems (SMS) has great potential to enhance safety by encouraging operators to put in place a systemic approach to proactively manage safety, the regulator must also have assurances of compliance with existing regulations. The current approach to regulatory oversight, which focuses on an operator's processes, is at risk of failing to identify and address unsafe practices and conditions. If TC does not adopt a balanced approach that combines thorough inspections for compliance with audits of safety management processes, unsafe operating practices may not be identified, thereby increasing the risk of accidents.
2.9 Ambulance New Brunswick
ANB's AirCare contract clearly outlined the requirements for crew experience and crew coordination; however, the most recent Atlantic Charters contract provided no such requirements. The wording in both the Atlantic Charters and the AirCare contracts had been in place before ANB's existence. For many years, Atlantic Charters had been providing MEDEVAC services with a single-pilot operation. However, under Atlantic Charters' latest contract, ANB had an expectation that the operation would be safer because there would be an additional pilot in the cockpit. Because of ANB's limited aviation knowledge and experience, it relied on its service providers to ensure regulatory compliance. ANB was unfamiliar with what was meant by standard industry terms such as challenge-and-response and CRM and, therefore, was unaware of the importance of these practices for the management of safety during flight. If organizations contract aviation companies to provide a service with which the organizations are not familiar, then there is an increased risk that safety deficiencies will go unnoticed, which could jeopardize the safety of the organizations' employees.
ANB required Atlantic Charters to provide semi-annual flight safety training to paramedics in lieu of providing a safety briefing prior to takeoff at the start of each flight. However, this practice does not meet the regulatory requirements of the pilot-in-command ensuring that passengers are given a safety briefing prior to takeoff on the first flight of the day. If passengers are not provided with a regular safety briefing, then there is an increased risk that they will not use the available safety equipment or be able to perform necessary emergency functions in a timely manner to avoid injury or death.
2.10 Survival aspects
2.10.1 Seatbelts
The paramedic's seatbelt was found fastened and adjusted in such a manner that it would not have fit around the paramedic's waist, and there was no indication that its state was altered after the aircraft came to rest. The investigation determined that, at the time of the accident, the paramedic was not wearing the seatbelt.
If passengers are not properly restrained, then there is an increased risk of injuries and death to those passengers and the other occupants in the event of an accident.
2.10.2 Cargo restraints
Post-accident examination revealed that tie-down straps were not used, and medical equipment was found loose within the cabin.
If carry-on baggage, equipment or cargo is not restrained, then occupants are at a greater risk of injury or death if these items become projectiles in a crash.
If carry-on baggage, equipment or cargo is not restrained, then there is an increased risk that the occupants' access to normal and emergency exits, and to safety equipment, will be completely or partially blocked.
2.11 Area navigation approach
The captain had cancelled the instrument flight rules (IFR) flight plan when approximately 20 nm from Grand Manan. The weather conditions at the time of the accident were such that visual reference to the runway would have been unlikely. The radar data indicate that the aircraft was aligned with the runway. Runway 24 was equipped with an RNAV instrument approach and the captain had reported passing the EMGAM final approach fix. Therefore, for the captain to navigate in such a way that the aircraft was aligned with the runway, it is likely that the GPS was being used to carry out an RNAV approach. When operating under CARs subpart 703, as during the occurrence flight, the company was not authorized to conduct GPS approaches.
In both approaches, the aircraft descended about 350 feet below the minimum descent altitude (MDA) and levelled off at 250 feet above ground level (agl). The MDA ensures adequate terrain clearance for an aircraft inside the final approach fix until the crew can visually acquire the runway environment. If pilots continue an approach below published MDAs without seeing the required visual references, then there is a risk of collision with terrain and/or obstacles.
No approach charts were found on board the aircraft, and the GPS database was out of date. Having a current database is important because it ensures that all data are up to date, including obstacles and waypoints. If current charts and databases are not used, then navigational accuracy and obstacle avoidance cannot be assured.
TC requires that CARs subpart 703 companies on revenue flights have the Operations Specification (OPS Spec) 100 in order to conduct GPS approaches. Having the OPS Spec ensures that there is adequate ground and flight training provided and demonstration of competency when using a GPS. If GPS approaches are conducted without the approved OPS Spec, then there is a risk that the pilot's training and knowledge will be inadequate to safely conduct the approach.
2.12 Medical reporting
The captain's medical status was being followed by a general practitioner who was also the civil aviation medical examiner (CAME). The captain had 2 medical events which should have been reported to TC. However, no such reports were made by the captain, the attending physician, or the captain's general practitioner. If medical symptoms/conditions are not reported to TC, then it negates some of the safety benefit of examinations and increases the risk that pilots will continue to fly with a medical condition that poses a risk to safety.
3.0 Findings
3.1 Findings as to causes and contributing factors
- The captain commenced the flight with only a single headset on board, thereby preventing a shared situational awareness among the crew.
- It is likely that the weather at the time of both approaches was such that the captain could not see the required visual references to ensure a safe landing.
- The first officer was focused on locating the runway and was unaware of the captain's actions during the descent.
- For undetermined reasons, the captain initiated a steep descent 0.56 nautical mile from the threshold, which went uncorrected until a point from which it was too late to recover.
- The aircraft contacted a road 0.25 nautical mile short of the runway and struck terrain.
- The paramedic was not wearing a seatbelt and was not restrained during the impact sequence.
3.2 Findings as to risk
- If cockpit data recordings are not available to an investigation, then the identification and communication of safety deficiencies to advance transportation safety may be precluded.
- If crew members are unable to communicate effectively, then they are less likely to anticipate and coordinate their actions, which could jeopardize the safety of flight.
- If crew resource management training is not provided, used and continuously fostered, then there is a risk that pilots will be unprepared to avoid or mitigate crew errors encountered during flight.
- If an actual weight and balance cannot be determined, then the aircraft may be operating outside of its approved limits, which could affect the aircraft's performance characteristics.
- If pre-computed weight and balance forms do not include standard items, then it increases the likelihood of omissions in weight and balance calculations, which increases the risk of inadvertently overloading or incorrectly loading the aircraft.
- If organizations carry out a maintenance task that they consider to be elementary work and the task is not approved as an elementary work task, then there is a risk that the aircraft will not conform to its type design, which could jeopardize the safety of flight.
- If individuals are performing maintenance tasks for which they have not received approved training, then there is a risk that the task will not be performed in accordance with the manufacturer's instructions.
- If components are not installed in accordance with the manufacturer's instructions, then occupants are at a greater risk of injury or death during an incident or accident if these components are not properly secured.
- If organizations do not record when maintenance is carried out, then the proper completion of tasks cannot be confirmed, and there is a risk that the aircraft will not conform to its type design, which could jeopardize the safety of flight.
- If an aircraft is modified without regulatory approval and without supporting documentation, then the aircraft is not in compliance with all applicable standards of airworthiness, which could jeopardize the safety of flight.
- If an operator undertakes unapproved changes to a supplemental type certificate, then there is a risk that the aircraft will not be airworthy, which could jeopardize the safety of flight.
- If organizations do not use modern safety management practices, then there is an increased risk that hazards will not be identified and risks mitigated.
- If Transport Canada does not adopt a balanced approach that combines thorough inspections for compliance with audits of safety management processes, unsafe operating practices may not be identified, thereby increasing the risk of accidents.
- If organizations contract aviation companies to provide a service with which the organizations are not familiar, then there is an increased risk that safety deficiencies will go unnoticed, which could jeopardize the safety of the organizations' employees.
- If passengers are not provided with a regular safety briefing, then there is an increased risk that they will not use the available safety equipment or be able to perform necessary emergency functions in a timely manner to avoid injury or death.
- If passengers are not properly restrained, then there is an increased risk of injuries and death to those passengers and the other occupants in the event of an accident.
- If carry-on baggage, equipment or cargo is not restrained, then occupants are at a greater risk of injury or death if these items become projectiles in a crash.
- If carry-on baggage, equipment or cargo is not restrained, then there is an increased risk that the occupants' access to normal and emergency exits, and to safety equipment, will be completely or partially blocked.
- If pilots continue an approach below published minimum descent altitudes without seeing the required visual references, then there is a risk of collision with terrain and/or obstacles.
- If current charts and databases are not used, then navigational accuracy and obstacle avoidance cannot be assured.
- If GPS (global positioning system) approaches are conducted without the approved Operations Specification, then there is a risk that the pilot's training and knowledge will be inadequate to safely conduct the approach.
- If medical symptoms/conditions are not reported to Transport Canada, then it negates some of the safety benefit of examinations and increases the risk that pilots will continue to fly with a medical condition that poses a risk to safety.
3.3 Other findings
- The pilot who installed the air ambulance system did not have approved training, nor was the pilot approved to carry out elementary work.
- Atlantic Charters was not approved to install the air ambulance system as an elementary work task.
- Atlantic Charters' pre-computed weight and balance form did not include a line item to indicate nacelle fuel.
- The semi-annual safety training offered to paramedics in lieu of safety briefings prior to flights did not meet regulatory requirements.
This report concludes the Transportation Safety Board's investigation into this occurrence. the Board authorized the release of this report on . It was officially released on .
Appendix A – Grand Manan area navigation (RNAV) global navigation
satellite system (GNSS) approach to Runway (RWY) 24
Not for navigation