Runway excursion
Air Labrador Limited
de Havilland DHC-6-300, C-GKSN
La Tabatière, Quebec
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 28 September 2014, a de Havilland DHC-6-300 Twin Otter aircraft (registration C-GKSN, serial number 493) operated by Air Labrador Limited, was on a charter flight from Lourdes-de-Blanc-Sablon, Quebec, to La Tabatière, Quebec, with 2 crew members and 17 passengers on board. The aircraft touched down about 750 feet beyond the threshold of Runway 23. During the rollout, the captain determined that the aircraft would not stop before reaching the end of the runway, and initiated a high-speed left turn onto the taxiway. The aircraft skidded to the right, and the right propeller struck a runway identification sign before the aircraft came to a stop. The aircraft sustained substantial damage. There were no injuries, and no fire occurred. The 406-megahertz emergency locator transmitter did not activate. The accident occurred at 1512 Atlantic Standard Time, in daylight.
1.0 Factual information
1.1 History of the flight
At about 1330 Footnote 1 on 28 September 2014, the crew arrived at the Lourdes-de-Blanc-Sablon airport (CYBX) in preparation for a charter flight to La Tabatière (CTU5), Quebec. The first officer (FO) completed the pre-flight walkaround, and 17 passengers boarded the aircraft.
The aircraft, a de Havilland DHC-6-300 Twin Otter aircraft (registration C-GKSN, serial number 493) operated by Air Labrador Limited, departed at 1437 under visual flight rules (VFR). The captain conducted the takeoff and, shortly after the aircraft became airborne, handed over the control to the FO. For the remainder of the flight, the FO was the pilot flying (PF), and the captain was the pilot not flying (PNF).
At about 1510, the FO conducted an approach briefing.
Ninety seconds later, the FO called for the initial landing checks to be completed and, 10 seconds after that, for the final landing checks to be completed. The flaps were at 20°, and the aircraft was configured for landing.
At 1512:17, at an altitude of approximately 200 feet above ground level (agl), the captain asked the FO a non-operational question. About 10 seconds later, the radar altimeter annunciated 10 feet.
At 1512:32, after floating for 6.3 seconds, the aircraft touched down about 750 feet from the threshold of Runway 23, which is 1649 feet long (Figure 1).

On touchdown, the captain took control of the aircraft, immediately selected reverse thrust, and applied the brakes. The captain determined that the aircraft could not be stopped before the end of the runway and initiated an aggressive left turn onto the taxiway.
During the turn, a tire hit a runway edge light, and the right propeller struck a runway identification sign before the aircraft came to a stop (Figure 1). Debris from the sign penetrated the fuselage just aft of the right cockpit door. As the aircraft was skidding, it came within 3 feet of sliding off the taxiway surface and going down a significant drop.
The crew shut down the aircraft and exited at the same time as the passengers. The 406-megahertz emergency locator transmitter did not activate.
1.2 Injuries to persons
| Injury | Crew | Passengers | Others | Total |
|---|---|---|---|---|
| Fatal | – | – | – | – |
| Serious | – | – | – | – |
| Minor | – | – | – | – |
| None | 2 | 17 | – | 19 |
| Total | 2 | 17 | – | 19 |
1.3 Damage to aircraft
The nose wheel was destroyed, and the right main wheel sustained substantial damage when the nose and right tires separated from their wheel beads.
The right propeller, right engine, and right nacelle structure sustained substantial damage when the propeller struck the runway identification sign.
Debris thrown against the right side of the aircraft punctured the fuselage skin immediately behind the right flight compartment door and caused structural deformation that prevented the door from opening (Photo 1). The aircraft was substantially damaged.

1.4 Other damage
A runway edge light was broken, and the runway identification sign was destroyed.
1.5 Personnel information
Records indicated that the flight crew was certified and qualified for the flight in accordance with existing regulations. There was no indication that fatigue affected the crew's performance.
| Captain | First officer | |
|---|---|---|
| Pilot licence | Commercial pilot licence–aeroplane (CPL-A) | Commercial pilot licence–aeroplane (CPL-A) |
| Medical certificate expiry date | 01 January 2015 | 01 July 2015 |
| Total flying hours | 23 000 | 435 |
| Hours on type | 20 000 | 235 |
| Hours in the last 30 days | 55.9 | 88.5 |
| Hours in the last 90 days | 194.3 | 235 |
| Hours off duty prior to the work period | 12 | 12 |
The captain had been employed at Air Labrador Limited (Air Labrador) for 17 years, and had flown the occurrence Twin Otter aircraft into CTU5 on numerous occasions.
In the months preceding the occurrence, the captain had been experiencing stress due to a family matter which had intensified 2 days prior to the occurrence. Other company personnel, including the director of flight operations and the chief executive officer, were aware of the captain's ongoing situation. Other company personnel indicated that over the past few months, they had noted that the captain seemed distracted while flying.
The FO had been hired at Air Labrador in July 2013, and had been flying with the company since July 2014. The FO had flown into CTU5 about 12 times with the occurrence captain. Due to the captain's record of being distracted, company personnel had considered the pairing of the FO with the captain before the aircraft was dispatched, ensuring that the crew members complemented each other.
1.6 Aircraft information
The de Havilland Canada DHC-6 Twin Otter Footnote 2 is a high-wing unpressurized aircraft with a fixed tricycle landing gear. It is powered by 2 turboprop engines driving 3-blade reversible pitch full-feathering propellers. The aircraft is certified for single-pilot operation, and can carry up to 20 passengers, depending on the seating configuration.
The occurrence aircraft was manufactured in 1976, and at the time of the occurrence, had accumulated a total of 33 032.4 hours since new. Records indicated that the aircraft was certified, equipped, and maintained in accordance with existing regulations and approved procedures, and that there were no known deficiencies before the occurrence flight.
1.6.1 Normal landing procedure
The DHC-6-300 Pilot Operating Handbook describes a normal landing as one in which flaps are set to either 20° or 37.5°, and the DHC-6-300 Aircraft Flight Manual (AFM) recommends that 20° flap be used for all normal operations where landing distance permits. Footnote 3
Landing distances for a specific VREF Footnote 4 are calculated based on the following criteria:
- Distance is calculated from 50 feet over the threshold to stop.
- Engine power is set to maintain a 3° approach to 50 feet, then engine power is set to idle.
- Wheel brakes only are used.
- Runway is a dry, hard level surface.
- Flaps are set to 37.5°.
To determine the landing distance with 20° flaps, the appropriate landing distance with 37.5° flaps stated in the AFM must be multiplied by 1.3.
The investigation calculated the landing distance, in accordance with the AFM criteria, to be 1395 feet Footnote 5 with 37.5° flaps and 1814 feet with 20° flaps. Footnote 6
According to the AFM, the decision to go around should be made before flaps have been extended beyond 10°. If flaps are set to 10° and the propeller levers are at the full increase position, then aircraft performance and handling during the go-around manoeuvre will be very similar to that during a normal takeoff.
Air Labrador's practice is to land with flaps set to 20°. Any landing that requires a 37.5° flap is considered outside the norm. When there is a requirement for landing with flaps set to 37.5°, Air Labrador uses pilots who have received short-takeoff-and-landing training. Footnote 7
1.6.2 Unpaved runway surface
The DHC-6-300 AFM landing performance information is valid only for a dry hard surface. The AFM landing distances are derived from landing distance demonstrations that employ more aggressive landing techniques than that used during normal operations. The surface characteristics of a runway can have an adverse effect on the braking performance of the aircraft, and may therefore increase the stopping distance during landing. The likelihood of a runway overrun may increase when landing on an unpaved runway under limiting conditions.
Air Labrador has a Transport Canada (TC) operations specification, Footnote 8 dated 08 November 2010, which allows the company to operate propeller-driven aeroplanes from or to unprepared surfaces not specifically addressed in the AFM. This specification requires that the air operator comply with section 724.44 of the Commercial Air Service Standards (CASS), which was amended on 30 June 2006. In accordance with section 724.44 of the CASS, when determining the landing distance required for gravel runways by the DHC-6-300 aircraft, a factor of 10% must be added to the performance data for a dry hard surface. No credit for reverse thrust may be used in this calculation.
When considering this 10% factor for the occurrence aircraft, the calculated landing distance increases to 1534 feet with 37.5° flaps and to 1994 feet with 20° flaps.
Air Labrador Twin Otter crews repeatedly fly into the same destinations on scheduled routes, during which the landing performance chart is not always consulted. Consequently, landing distance calculations are not completed for every landing because runway length is not perceived as a threat. At the time of the occurrence, the landing distance performance chart contained a note advising pilots to add 10% for gravel runways.
Air Labrador had been conducting scheduled flights into CTU5 in the 8 years following the 2006 amendment to CASS section 724.44. During that period, Air Labrador's policy was to land using 20° flaps. The conditions on the day of the occurrence, with a 20° flaps setting, would have required a landing distance of 1994 feet; CTU5's Runway 23 is 1649 feet long.
1.7 Meteorological information
The nearest airport that records weather is Lourdes de Blanc-Sablon, which is 77 nautical miles (nm) to the east. At 1500, the reported weather was as follows: wind 300° true at 4 knots, visibility 8 statute miles, few clouds at 800 feet agl, ceiling of broken clouds at 2000 feet agl, overcast at 5000 feet agl, temperature 11 °C, dew point 9 °C, and altimeter 29.55 inches of mercury.
The crew reported the weather at CTU5 was good visibility, no precipitation, and calm winds. Weather was not considered a factor in this occurrence.
1.8 Aids to navigation
CTU5 is not serviced by any ground-based navigational aids.
1.9 Communications
CTU5 is not serviced by any ground-based communications.
1.10 Aerodrome information
CTU5 airport is for VFR use only. It has 1 gravel runway (05/23) which is 1649 feet long by 82 feet wide (Appendix A). The runway has 100-foot extensions at both ends. Beyond these extensions there are substantial drops of about 90 feet in elevation (Photo 2).

Runway 23 has medium intensity threshold, runway end and runway edge lighting. A precision approach path indicator (PAPI), suitable for the DHC-6 aircraft, is located on the approach to both runways. The airport lighting and the PAPI are controlled by aircraft radio. The aerodrome is licensed by TC and maintained by Transport Québec.
The PAPI and runway lights were not used during the occurrence flight. Footnote 9
1.11 Flight recorders
1.11.1 Occurrence aircraft
The aircraft was equipped with a cockpit voice recorder (CVR), as required by Canadian Aviation Regulations (CARs) section 605.33. Footnote 10 The CVR was forwarded to the TSB laboratory with the occurrence data intact. The aircraft was not equipped with a flight data recorder (FDR), nor was it required by regulation.
1.11.2 Benefits of recorded flight data
Numerous TSB aviation investigation reports have attributed the inability of investigators to determine the reasons why an accident occurred to a lack of on-board recording devices. The benefits of recorded flight data in aircraft accident investigations are well known and documented.
Lightweight flight recorder technology is now available. These systems can record aircraft performance data and cockpit audio and image data, and are increasingly being adopted by operators around the world.
In TSB Aviation Investigation Report A11W0048, the Board recommended that:
The Department of Transport work with industry to remove obstacles to and develop recommended practices for the implementation of flight data monitoring and the installation of lightweight flight recording systems by commercial operators not currently required to carry these systems.
Transportation Safety Recommendation A13-01
Transport Canada supports this recommendation and has decided to proceed with the development of an advisory circular in 2015–2016 to describe recommended practices regarding flight data monitoring (FDM) programs. In addition, TC will be consulting, through focus groups, to identify obstacles within TC's mandate and make recommendations for mitigation of those obstacles with respect to the installation of lightweight flight recording systems for commercial operators not required to carry these systems.
The Board is encouraged by the intent of TC to work towards meeting the issues identified in the recommendation; however, the work is ongoing. Therefore, the TSB has assessed TC's response to the recommendation as Satisfactory Intent.
If flight data recordings are not available to an investigation, the identification and communication of safety deficiencies to advance transportation safety may be precluded.
1.12 Wreckage and impact information
Not applicable.
1.13 Medical and pathological information
Not applicable.
1.14 Fire
Not applicable.
1.15 Survival aspects
Not applicable.
1.16 Tests and research
1.16.1 TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP 198-2014 – CVR download and transcription
- LP 224-2014 – NVM Recovery GPS and TAWS
1.17 Organizational and management information
1.17.1 General
Labrador Airways Ltd. was established in 1948, with its head office located in Happy Valley-Goose Bay, Newfoundland and Labrador. It was sold in 2010 and renamed Air Labrador Ltd., with its base of operations remaining the same. The company conducts CARs Subpart 703 air taxi operations and Subpart 704 commuter operations. Its fleet of aircraft includes 6 Twin Otters, 1 Cessna Caravan, 2 Beechcraft 1900Ds, and 2 King Air 100s.
The majority of the company's captains are senior captains as there is very little attrition at the captain level. Applicants for FO positions are mostly hired directly from flight schools and are initially hired as flight followers. FOs move to flying positions when vacancies occur, which can take from several months to a year, according to FO attrition rates.
1.17.2 Air Labrador flight safety
Air Labrador does not have a safety management system (SMS), nor is it required by regulation to have one.
In 2007, Labrador Airways Ltd. was conducting CARs Subpart 705 operations and was therefore required by TC to implement progressively an SMS, including an SMS manual. Accordingly, the company had begun the implementation of an SMS and had completed the 3rd of 4 phases, which included the development of an SMS manual. In the spring of 2009, the company ceased CARs Subpart 705 operations, and the SMS certification process was halted.
The incident reporting component is the only part of the SMS manual that is used on a regular basis. Operational incident reports are reviewed by the general manager, the chief pilot, and the safety officer, using a traditional approach to safety management. This approach relies primarily on regulatory compliance, as well as on the response to undesirable events, which includes identifying their underlying causes and prescribing specific measures to prevent their reoccurrence. No proactive hazard identification or risk assessments are carried out.
Although the company refers new hires to the SMS manual for guidance, there is no requirement for senior pilots to become familiar with the content of the manual.
1.17.3 Air Labrador's response to incidents and accidents
On 27 March 2013, an Air Labrador DHC-6-300 Twin Otter aircraft was involved in a landing accident at St. Anthony Airport, Newfoundland and Labrador. Footnote 11 During the approach, the captain and the FO, who was the PF, discussed approach and landing considerations because a strong crosswind was present at the airport. Just prior to landing, the FO experienced difficulty maintaining control of the aircraft. The captain asked whether the FO wanted to transfer control, and the FO agreed to do so. The transfer of control was completed less than 2 seconds before touchdown. Once control of the aircraft had been passed to the captain, there was insufficient time to position the aircraft for a successful landing because of the strong crosswind.
Air Labrador's response to the St. Anthony accident was to address the immediate safety concerns that it identified as causing the occurrence, and included the following:
- The captain was temporarily downgraded to FO pending his completion of supplementary training.
- The company's Twin Otter standard operating procedures (SOPs) were amended to state that the captain will conduct all landings with crosswinds in excess of 10 knots. However, the amendment states, if the captain feels that the FO is capable of performing the landing, then it will be at the captain's discretion to allow the FO to conduct the landing.
- An amendment was also made to the company's Twin Otter SOPs to restrict all landings to crosswinds of within 30 knots at 90°.
In response to the occurrence at the CTU5 airport, Air Labrador carried out a review of the accident and demoted the captain to FO for 500 flight hours. A directive was issued restricting FOs with fewer than 1000 hours on type to conducting landings only on runways of 2000 feet or longer. If the FO has more than 1000 hours on type, then the landing is at the captain's discretion.
1.17.4 Transport Canada oversight of Air Labrador
Transport Canada develops and administers policies and regulations for the civil aviation system, and carries out surveillance procedures, which include program validation inspections Footnote 12 (PVIs), to measure operational effectiveness and compliance with the CARs.
PVIs are conducted on a routine schedule, and use risk indicators to adjust the frequency of inspection, as necessary. Based on need and available resources, TC conducts additional inspections and interventions, including occasional aircraft inspections of the operator's aircraft at the base.
Transport Canada conducted airworthiness PVIs of Air Labrador in March 2011 and October 2012. It conducted flight operations PVIs in March 2012 and again in September 2014, a few days before the occurrence. The PVIs were conducted in accordance with TC Civil Aviation Staff Instruction SUR-001, Footnote 13 along with supplementary guidance material.
All of the findings of non-compliance resulting from the PVIs were addressed with corrective action plans (CAPs), which were subsequently accepted by TC. The department completed a follow-up inspection in December 2015 to ensure that the CAP proposed for the September 2014 PVI has addressed all findings. Follow-up has been completed on the earlier PVIs, and those files are considered closed.
Transport Canada carried out an evaluation of Air Labrador following the occurrence, and has made no changes to the PVI inspection schedule of the company.
1.18 Additional information
1.18.1 Approach-and-landing accidents are a 2014 Watchlist issue
The Watchlist is a list of issues posing the greatest risk to Canada's transportation system; the TSB publishes it to focus the attention of industry and regulators on the problems that need addressing today. As this occurrence demonstrates, landing accidents continue to occur at Canadian airports. The TSB has called on TC and operators to do more to reduce the number of unstable approaches that are continued to a landing. Footnote 14 TC must complete its risk-based analysis and move forward with regulatory changes. Airports must develop tailored solutions to lengthen runway end safety areas or install other engineered systems and structures to safely stop planes that overrun runways.
In 1998, the Flight Safety Foundation concluded “that failure to recognize the need for and to execute a missed approach when appropriate is a primary cause of approach-and-landing accidents.” Footnote 15 According to the Go-around Safety Forum (26 June 2013), “The lack of a go-around decision is the leading risk factor in approach and landing accidents and is the primary cause of runway excursions during landing. Yet, less than 5% of unstabilised approaches lead to a go-around.” Footnote 16
A missed approach or go-around is a normal phase of flight. Footnote 17 The procedures associated with performing a go-around are included in a pilot's initial training and recurrent training. During training, pilots are prepared for the go-around, as it is carried out under a controlled environment. The height at which a decision to go around occurs affects the challenges associated with the go-around. If a go-around becomes necessary, then immediate and positive action must be taken by the PF. This decision becomes more critical the closer the aircraft is to the ground, as the aircraft is in a lower state of energy.
Air Labrador's approach briefing procedure does not include a requirement for the crew to discuss a touchdown point on the runway or the necessity of conducting a go-around if this touchdown point is not achieved. The company expects that the pilots will use their knowledge and experience to assess the situation and react accordingly, including by determining when a go-around should be carried out. The SOPs do not include information related to potential threats associated with unstable approaches, nor does the company actively encourage pilots to be go-around-minded.
Performing a go-around is not a frequent occurrence. According to the Go-around Safety Forum, a short-haul commercial pilot may make a go-around once or twice a year on average. This infrequency might partially explain pilots' reluctance to perform a go-around. Footnote 18
1.18.2 Situational awareness
Individual situational awareness (SA) describes how a crew member interprets, projects, and takes action on the moment-to-moment changes in the aircraft state. Flight crew actions need to be based on the same understanding of the current state of the aircraft, the intended flight plan, and the threats to these activities in order for crew members to perform in a coordinated, efficient, and safe manner. The accuracy of a pilot's SA during flight contributes to effective decision making by enabling informed, accurate predictions of the results of the pilot's actions and any potential consequences.
In multi-crew teams, shared SA describes the state wherein crew members have a common mental model and shared understanding of the flight situation, such as during takeoffs and landings with one pilot flying and the other pilot monitoring. Shared situational awareness is developed and maintained by a crew through a number of discrete and continuous behaviours. Discrete behaviours include flight planning, in-flight briefings, and identification of key points in the flight, such as attaining minimum altitudes. These activities are planned checkpoints to describe current state and future plans and to provide an opportunity for checking that all crew members have the same understanding.
Continuous behaviours include threat and error management, callouts of changes in aircraft state and instrument setting/mode, and communication of changes to plans. These behaviours ensure that information and state changes are communicated between crew members to update the shared situational awareness on an ongoing basis. Such continuous behaviours are influenced by the training and operational approach taken by operators.
Unlike shared SA, team SA represents the degree to which every team (or crew) member possesses the SA required for his or her responsibilities. Footnote 19 It comprises each team member's individual SA as well as the degree of shared understanding among them. An important element of team SA is effective inter-crew coordination, or transfer of information from one crew member to another. This transfer should not be limited to data alone; rather, it should also include sharing of crew members' comprehension of the situation and its projection into the future. Footnote 20
A pilot's ability to attend to critical stimuli within his or her environment will be impaired if the pilot is distracted or inattentive, and will result in impaired situational awareness. Footnote 21
1.18.3 Briefings
The Air Labrador's Twin Otter SOPs require that the crew carry out a briefing for every approach to ensure that the PNF is aware of the PF's intentions and to identify any tasks that the PNF will need to perform.
A VFR approach briefing typically includes runway orientation and airport name, circuit altitude, aircraft weight, flap position, approach and VREF speeds, and obstacle clearance altitude.
1.18.4 Checklist
Air Labrador's SOPs Footnote 22 require that any in-flight operational communication between flight crew members be acknowledged by the recipient. The word “Check” is used to acknowledge situational information.
The pre-landing and landing checklists are required to be performed in a challenge-and-response format; however, not every item is verbally expressed due to its impact on the desired sterile flight deck environment. Footnote 23 Air Labrador's Twin Otter SOPs identified the landing checklist as challenge-and-response in section 2.20.1: Normal Procedures; however, in section 5.7.1: Normal Landing, the checklist is identified as read-and-do.
The challenge-and-response procedures require the PF to call for the appropriate checklist, for the PNF to read the challenge, and for the PF to respond appropriately. The read-and-do checklist does not require the PF to verbally respond.
During the occurrence approach and landing, the PNF did not respond to the PF's call for the initial and final landing checks.
In high-risk situations, such as carrying out a landing, following the appropriate checklist or procedure provides pilots with the safest and most efficient course of action in most cases. However, if checklist and procedural discipline is not taught, practised, reinforced, and monitored, there is a danger that pilots will deviate from prescribed procedures or respond inappropriately to unusual situations.
The investigation confirmed that the senior captains were less likely to observe checklist protocol than the pilots who were recently advanced to the position of captain.
1.18.5 Sterile flight deck
Sterile flight deck rules, which require pilots to refrain from non-essential activities and non-operational conversation, are intended to minimize distraction during critical phases of flight and ensure that critical tasks are not interrupted. Air Labrador's SOPs require a sterile flight deck for all flight operations below 3000 feet, except cruise flight. The only exception is in an emergency or when communicating information essential to the safety of passengers or aircraft.
Research on the speech of pilots during simulated flight Footnote 24 shows that prosodic features of speech, such as word frequency per unit of time, increase as a function of increased mental workload.
During the final approach, the captain asked the FO a non-operational question. The FO replied with an abrupt, one-word response.
1.18.6 Complacency
When pilots routinely fly the same routes to the same destinations, their performance can become automatic. They may pay less attention to detail and become complacent. Complacency results from a state of overconfidence, repetition of action, contentment with the status quo, familiarity, and boredom. It is associated with experience and confidence, both found in high-time pilots.
Pilot complacency can also impair the ability to maintain SA, and has been implicated as a contributing factor in aviation accidents and incidents. When pilots receive information about the environment that they expect to receive, they tend to react quickly and without errors. However, when they receive information that is contrary to their expectations (and their SA), their performance tends to be slow or inappropriate. Footnote 25
While employed at Air Labrador, the captain had regularly flown into La Tabatière without incident.
1.18.7 Crew resource management
The objective of crew resource management (CRM) is to reduce human error by providing flight crews with a variety of strategies to help improve their effectiveness. A widely accepted definition of CRM is the effective use of all human, hardware, and information resources available to the flight crew to ensure safe and efficient flight operations. Research has shown that pilots with recent CRM training are better able to handle novel situations than those without recent CRM training. Footnote 26
In 1995, the TSB issued Recommendation A95-11, which called for TC to establish guidelines for CRM and decision-making training for all operators and aircrew involved in commercial aviation. TC's response targeted only CARs Subpart 705 operators, and did not include CARs subparts 703 and 704 operators. Consequently, the TSB assessment of TC's response was Satisfactory in Part. Footnote 27
On 09 October 2009, the TSB recommended that:
The Department of Transport require commercial air operators to provide contemporary crew resource management (CRM) training for Canadian Aviation Regulations (CARs) subpart 703 air taxi and CARs subpart 704 commuter pilots.
Transportation Safety Recommendation A09-02
In its responses to Recommendation A09-02, TC has accepted the recommendation in principle and indicated that it is working toward a regulation that would make CRM a requirement for CARs Subpart 703 air taxi and CARs Subpart 704 commuter operations.
Transport Canada has recently developed CRM training standards for CARs subparts 703 and 704 commercial air operators. These are currently in notice of proposed amendment (NPA format) and TC plans to publish the NPA in 2016.
Following the disposition of comments received, TC intends to move ahead with implementation and a resulting mandatory requirement for operator CRM training, applicable to flight crew, cabin crew, dispatchers, and maintenance personnel associated with aircraft operations.
The Board is encouraged that action on this recommendation is nearing completion. The proposed course of action should substantially reduce or eliminate the safety deficiency identified in TSB Recommendation A09-02. Until the standards are amended and fully implemented, this safety deficiency will continue to exist. The response is considered Satisfactory Intent.
Air Labrador does not provide CRM training, nor is it required to do so by regulation. The captain had never taken a CRM course, and the FO had received 8 hours of CRM training while attending flight school.
Even though CARs Subpart 703 and 704 operators are not currently required to provide CRM training, there is nothing preventing them from proactively and voluntarily providing their crews with modern CRM training.
1.18.8 Organizational safety culture
Safety culture can be described as “the way we do things around here” Footnote 28 or “what people at all levels in an organisation do and say when their commitment to safety is not being scrutinised.” Footnote 29 According to the International Civil Aviation Organization (ICAO), “Organizational safety culture sets the boundaries for accepted operational performance in the workplace by establishing the norms and limits” and “provides a cornerstone for managerial and employee decision-making.” Footnote 30 Culture is deeply ingrained, and its impact on safety may not be readily apparent to those working within those cultures.
One of the largest influences on safety culture is management commitment and style. ICAO has described the role of management in creating a “good” organizational safety culture as follows:
Those in the best position to effect accident prevention by eliminating unacceptable risks are those who can introduce changes in the organization, its structure, corporate culture, policies and procedures, etc. No one is in a better position to produce these changes than management. Footnote 31
Organizations differ considerably in the level of risk they tolerate within their operations. Organizations which take proactive steps to identify and mitigate risks are considered to have good safety cultures, while organizations with poor safety cultures—knowingly or unknowingly—operate with higher levels of risk. An organization that operates with significant risk faces a greater potential for an accident.
The traditional approach to safety management is based on compliance with regulations and a reactive response to incidents and accidents. According to the ICAO Safety Management Manual (SMM), follow-up actions may generate safety recommendations aimed at the specific, immediate safety concern identified as causing the occurrence. Little emphasis is placed on other hazardous conditions that, although present, are not causal in the occurrence, even though they hold damaging potential for aviation operations under different circumstances. Footnote 32
While this perspective is quite effective in identifying what happened, it is considerably less effective in disclosing why it happened, which is essential to correcting the underlying safety deficiency. Footnote 33 Further, the manual states:
Although compliance with safety regulations is fundamental to the development of sound safety practices, contemporary thinking is that much more is required. Organizations that simply comply with the minimum standards set by the regulations are not well situated to identify emerging safety problems. Footnote 34
[…]
As global aviation activity and complexity continue to grow, deeply changed operational contexts with their new challenges make traditional methods of managing safety to an acceptable level less effective and efficient. Different, evolved methods of understanding and managing safety are necessary. Footnote 35
1.18.9 Safety management systems
Transport Canada describes an SMS as:
[a] businesslike approach to safety. It is a systematic, explicit and comprehensive process for managing safety risks. As with all management systems, a safety management system provides for goal setting, planning, and measuring performance. A safety management system is woven into the fabric of an organization. It becomes part of the culture, the way people do their jobs. Footnote 36
As summarized in TSB Aviation Investigation Report A07A0134:
Modern safety management principles promote a proactive search for hazards, identification of risks, and the best defences to reduce risk to an acceptable level. These principles must be embedded within an organization's management system so that safety policies, planning, procedures, and performance measurement are integrated into day-to-day operations.
In its Watchlist, the TSB urges TC to implement regulations requiring all operators in the air industry to have formal safety management processes, and to oversee these processes. It also calls on companies that do have a safety management system to demonstrate that it is working—that hazards are being identified and effective risk mitigation measures are being implemented. Finally, when companies are unable to effectively manage safety, TC must not only intervene, but do so in a manner that succeeds in changing unsafe operating practices. Footnote 37
1.19 Useful or effective investigation techniques
Not applicable.
2.0 Analysis
There was no indication of a component or system failure during the occurrence flight and fatigue was not considered a factor. The analysis will focus on why the serviceable aircraft landed about halfway down the runway, and on the safety culture and practices of the company.
2.1 Approach and landing
The aircraft was configured for landing according to Air Labrador's SOPs. There was no tailwind, and there was no indication that the crew experienced a problem with the aircraft. The aircraft was not equipped with an FDR; therefore, it was not possible to determine the aircraft's height or speed as it crossed the threshold. The aircraft floated for 6.3 seconds over the runway and touched down about 750 feet from the threshold, which reduced the length of runway available for stopping.
The Air Labrador SOPs for approach briefing do not include a requirement to discuss threats that would dictate that the crew perform go-around, such as the aircraft passing a predetermined landing point when airborne. The company has neither SOPs nor a policy stating when to conduct go-arounds, and relies solely on pilot experience to determine when a go-around should be performed. Since neither crew member perceived runway length as a threat, there was no discussion concerning the point at which a safe landing would no longer be possible.
Neither crew member initiated a go-around while the aircraft floated over the runway for more than 6 seconds. If pilots are not prepared to conduct a go-around on every approach, there is a risk that they will not be ready to react to a situation that requires a go-around.
Air Labrador's policy is to land using 20° flaps, and it considers any runway requiring landing with 37.5° flaps to be outside the norm, even though the Twin Otter AFM states that such a landing is normal. With flaps set at 20°, the occurrence aircraft would have required a runway distance greater than that available at CTU5.
The calculation for runway length implemented in 2006, which uses 37.5° flaps and includes a 10% factor for gravel runways, would have given them the required runway distance for landing on the day of the occurrence. The crew used 20° flaps for landing, which did not permit them to meet the calculated landing distance requirement of the AFM and the 10% factor required by regulation for landings on unprepared surfaces.
If performance charts are not consulted, there is a risk that the required landing distance will be greater than the actual length of the runway.
2.2 Sterile flight deck
To ensure that pilots are not distracted during critical phases of flight, Air Labrador requires that a sterile flight deck be maintained. During the final approach, the first officer (FO) was interrupted by a non-operational question from the captain. The FO's abrupt, one-word response is typical of what would be expected of prosodic speech resulting from the FO's increased mental workload associated with landing an aircraft.
If flight crews do not adhere to sterile flight deck procedures, they may be distracted during critical phases of flight, which could jeopardize the safety of flight.
2.3 Crew resource management
Crew resource management training is specifically designed to address much of the behaviour identified in this report regarding the interaction between flight crew members. Research has shown that CRM-trained crews operate more effectively as teams and cope more effectively with non-routine situations than crews without CRM training. Additionally, when there is no effective reinforcement of CRM concepts by way of recurrent training, improvement in attitudes observed after initial indoctrination tends to disappear.
Although some commuter and air taxi operators have voluntarily provided CRM training to their pilots, others do not. Additionally, companies voluntarily providing refresher training do not necessarily do so on a recurring basis.
Despite TSB recommendations calling for CRM training to be required for all air operators in Canada since 1995, CARs subparts 703 and 704 operators are still not required to provide CRM training. If CRM training is not a regulatory requirement, then it is less likely to be introduced by operators, and as a result, their crew coordination may be less effective.
The captain had not received CRM training. In 2012, the first officer received 8 hours of CRM training that included role playing and case histories while completing flight training in a professional pilot diploma program. Neither pilot had received further CRM training with Air Labrador, nor is it required by regulation.
The stress arising from the captain's personal situation may have led to inattention and loss of situational awareness during the landing phase on the occurrence flight. The company was aware of his personal situation, and considered it when pairing an FO with him. The captain's preoccupation with personal matters may also have contributed to the non-adherence to SOPs and violation of the sterile flight deck directive. The captain did not recognize that the aircraft was floating until it was approximately 750 feet down the runway.
Crew resource management training could have helped the crew members to recognize and mitigate deficiencies by instilling in them the necessity to monitor each other's performance and point out any deviation as soon as possible. A long landing would be considered a deviation, particularly on a short and challenging runway.
The captain took control almost halfway down the runway, with insufficient runway remaining. The captain was familiar with the airport, and therefore turned left into the taxiway to avoid the steep drop and power lines off the end of the runway. The aggressive turn in combination with striking the runway identification sign resulted in significant damage to the aircraft.
If CRM training is not provided, pilots may be unprepared to respond to situations that may jeopardize the safety of flight.
2.4 Complacency and checklist use
For high-time pilots who fly the same routes every day, complacency can creep into daily activities. The routine of repetitive actions can lead to disengagement from and non-vigilance to the task at hand.
The captain had flown into this airport many times. On the day of the occurrence, it was a non-eventful flight until the landing phase. Routine, familiarity, repetitive actions, and confidence, along with the expectation that the landing would be typical, likely caused the captain to be less attentive. The captain had flown into CTU5 with the FO as PF without incident on several occasions. Given his expectations regarding the capabilities of the FO, the captain may have been less vigilant in terms of monitoring the unfolding situation.
The previous experiences of the captain could have influenced his level of alertness and, consequently, his reaction time in the role of pilot monitoring. If pilots do not focus on the task at hand, there is a risk that they will not react to conditions that could affect the safety of flight.
The fact that the PNF did not read aloud the checklist indicated a lack of shared situational awareness and complacency due to a perceived lack of hazards on what is, to an experienced captain, a routine approach. A read-and-do checklist was used by the crew, whereas a challenge-and-response checklist could have served as a defence to help prevent the crew's loss of shared situational awareness and also to guard against complacency.
2.5 Air Labrador safety management
In 2007, Air Labrador was conducting CARs Subpart 705 aircraft operations and beginning implementation of an SMS, as required by Transport Canada (TC). In the spring of 2009, the company had completed the 3rd of 4 phases, including the development of an SMS manual, when the company ceased CARs Subpart 705 operations, and the SMS certification process was halted.
Air Labrador's review of 2 occurrences (TSB Aviation Investigation Report A13A0033 and the current occurrence) resulted in corrective actions that reflect a traditional approach to safety management. Organizations respond to operational pressures because these priorities are clearly measurable and provide immediate feedback. Under these pressures, safety concerns may become less prominent, and organizations may unwittingly introduce risk into their operations.
In November 2010, an operations specification permitting operations to and from unprepared surfaces was issued to Air Labrador. TC had implemented an amendment to CASS 724.44 in 2006, requiring a factor of 10% to be added to the landing distance calculations for dry hard runway surfaces when operating DHC-6-300 aircraft on gravel runways. It is unknown whether Air Labrador conducted a review of its destinations and completed a risk analysis with this new information; however, the company continued flights into CTU5 using 20° flaps.
The traditional approach to safety management in which organizations comply with regulations and react to incidents and accidents is not well suited to identify emerging safety problems. In today's aviation environment, modern safety management practices must be embedded within an organization's management system so that the management of safety is integrated into day-to-day operations. Even though there are no regulatory requirements for CARs subparts 703 and 704 operators to have an SMS, nothing prevents these operators from implementing one.
If organizations do not use modern safety management practices, there is an increased risk that hazards will not be identified and mitigated.
3.0 Findings
3.1 Findings as to causes and contributing factors
- The aircraft floated for 6.3 seconds over the runway and touched down about 750 feet from the threshold, which reduced the length of runway available for stopping.
- The captain took control almost halfway down the runway with insufficient runway remaining in which to stop, requiring an aggressive left turn onto the taxiway that resulted in significant damage to the aircraft.
3.2 Findings as to risk
- If pilots are not prepared to conduct a go-around on every approach, there is a risk that they will not be ready to react to a situation that requires a go-around.
- If performance charts are not consulted, there is a risk that the required landing distance will be greater than the actual length of the runway.
- If flight crews do not adhere to sterile flight deck procedures, they may be distracted during critical phases of flight, which could jeopardize the safety of flight.
- If crew resource management training is not a regulatory requirement, it is less likely to be introduced by operators, and as a result their crew coordination may be less effective.
- If crew resource management training is not provided, pilots may be unprepared to respond to situations that may jeopardize the safety of flight.
- If pilots do not focus on the task at hand, there is a risk that they will not react to conditions that could affect the safety of flight.
- If organizations do not use modern safety management practices, there is an increased risk that hazards will not be identified and mitigated.
- If flight data recordings are not available to an investigation, the identification and communication of safety deficiencies to advance transportation safety may be precluded.
3.3 Other findings
- The crew used 20° flaps for landing, which did not permit them to meet the calculated landing distance requirement of the Aircraft Flight Manual and the 10% factor required by regulation for landings on unprepared surfaces.
4.0 Safety action
4.1 Safety action taken
4.1.1 Air Labrador Limited
A directive was issued to all crews restricting first officers (FO) with less than 1000 hours on type to conduct landings only on runways 2000 feet or greater. If the FO has more than 1000 hours on type, the final decision as to whether the landing can be conducted safely by the FO rests with the captain, taking into consideration the conditions at the time.
Since the occurrence, Air Labrador has provided a laminated landing-distance performance chart in each aircraft that advises pilots to add 10% for gravel runways to landing calculations.
On 16 January 2015, the company issued an amendment to its SOPs and normal checklist to reflect that the landing checklist may be executed in a read-and-do or challenge–and-response format.
On 27 February 2015, the company issued a directive to its crews stating that a flap setting of 37.5° must be used for all landing on airstrips shorter than 2000 feet.
This report concludes the Transportation Safety Board's investigation into this occurrence. the Board authorized the release of this report on . It was officially released on .
Appendices
Appendix A – La Tabatière aerodrome information
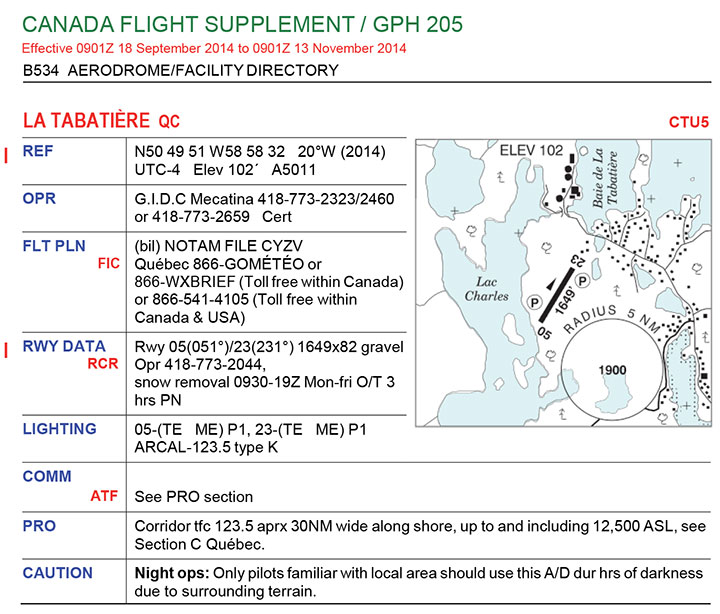
Source: NAV CANADA, Canada Flight Supplement, CTU5