Hard landing and runway excursion
Maritime Air Charter Limited
Beechcraft King Air A100, C-FDOR
Margaree, Nova Scotia
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 16 August 2015, a Maritime Air Charter Limited Beechcraft King Air A100 (registration C-FDOR, serial number B-103) was on a charter flight from Halifax Stanfield International Airport, Nova Scotia, to Margaree Aerodrome, Nova Scotia, with 2 pilots and 2 passengers on board. At approximately 1616 Atlantic Daylight Time, while conducting a visual approach to Runway 01, the aircraft touched down hard about 263 feet beyond the threshold. Almost immediately, the right main landing gear collapsed, then the right propeller and wing contacted the runway. The aircraft slid along the runway for about 1350 feet, then veered right and departed off the side of the runway. It came to rest about 1850 feet beyond the threshold and 22 feet from the runway edge. There were no injuries and there was no post-impact fire. The aircraft was substantially damaged. The occurrence took place during daylight hours. The 406-megahertz emergency locator transmitter did not activate.
This report is also available in English.
1.0 Factual information
1.1 History of the flight
On 16 August 2015, Maritime Air Charter Limited (MAC) was to carry out a charter flight from Halifax Stanfield International Airport (CYHZ), Nova Scotia, to Margaree Aerodrome (CCZ4),Footnote 1 Nova Scotia, with 2 passengers on board.
MAC's operations manager determined that the flight would be carried out with the company's Beechcraft King Air A100 (A100). This decision was primarily based on personnel availability, as well as the knowledge that the company had landed at CCZ4 in the A100 on 2 previous occasionsFootnote 2 and that, with the expected landing weight, the calculated landing distance would be 1700 feet, 800 feet shorter than the runway.
The operations manager assigned a part-time employed pilot to be the captain and a full‑time employed pilot to be the first officer (FO). Although these pilots had flown together before, neither had previously flown into CCZ4.
In preparation for the flight, the operations manager and the captain discussed hazards that the crew should be aware of, primarily the possibility that people or animals could be on the runway, and that, if required, a diversion to Port Hawkesbury Airport (CYPD) was an option.Footnote 3 The operations manager expected the captain to make the decision as to whether a safe landing could be carried out.
Neither the captain nor the FO indicated that he had any concerns about undertaking the flight. The crew discussed landing on Runway 01 and noted that it was shorter than the runways that they had typically flown into. The crew agreed that the final approach would be carried out at 120 knots and that they wanted to touch down as close as possible to the threshold. Due to high terrain near CCZ4, the crew planned to stay high and descend at a steeper rate during final approach.
Prior to departure, even though this was the first flight of the day for the aircraft, the crew did not perform the required Engine Run-up checklist.
At 1529,Footnote 4 the aircraft departed Halifax Stanfield International Airport under visual flight rules (VFR). The captain was the pilot flying (PF) and occupied the left seat, and the FO was the pilot not flying (PNF).
At 1551, a descent from the enroute altitude of 9500 feet above sea level (ASL) was initiated.
The crew re-confirmed that, based on the wind reported by the automated weather observation system at Port Hawkesbury Airport, they would land on Runway 01.
At 1600, the PNF made an advisory transmission on the aerodrome traffic frequency (ATF)Footnote 5 informing any traffic in the area that the aircraft would be joining a left base legFootnote 6 for Runway 01.
At 1604, the crew performed the Descent Checks checklist in accordance with the company standard operating procedures (SOP), with the exception of the approach briefing, which was abbreviated and described the approach as being visual for Runway 01.
At 1607, the PNF reported on the ATF that the aircraft was at 2700 feet ASL and about 20 nautical miles (nm) from CCZ4. No other aircraft reported being in the area.
When the aircraft was at 2500 feet ASL, the PNF made an advisory transmission on the ATF indicating that the aircraft was joining the circuit on a left base for Runway 01.
At 1613, about 5 nm from the runway, the power was reduced to 600 foot-pounds of torque, and approach flaps were selected to initiate a steep rate of descent.Footnote 7
The crew observed a tower along the flight path, and the PNF focused his attention on ensuring that clearance was maintained.
At about 1614, the PF reduced the power to idle to further increase the rate of descent. The engine auto-ignition system igniters activated, indicating that engine power was below 400 foot-pounds of torque. The igniters remained on until the aircraft touched down.
The landing gear was selected down and, once the PNF had confirmed that the aircraft was clear of the tower, full flaps were selected.Footnote 8 The crew did not complete the Landing Checks checklist as required by the SOPs. About 20 seconds later, the aircraft was descending through 1900 feet ASL (about 1700 feet above runway elevation) and 2.1 nm from the runway threshold.
At about 1615:34, the PNF indicated that the airspeed was below the planned speed. The PF indicated that he was making the appropriate correction and began to increase the airspeed by pitching the aircraft down; there was no change in engine power. This correction was followed by automated calls of "SINK RATE," "PULL UP, PULL UP," and "FIVE HUNDRED" (indicating 500 feet above ground elevation) in very quick succession from the terrain awareness and warning system (TAWS). The PF acknowledged the TAWS calls and began to reduce the rate of descent by pitching the aircraft up; there was no change in engine power.
At 1615:56, when the aircraft was about 120 feet above the runway elevation, the PNF began to move the propellers toward fullFootnote 9 while asking the PF if the propellers should be advanced. Almost immediately, the PF acknowledged the PNF's statement by replying "check." There was no change in engine power, and the aircraft's rate of descent increased.
At 1616:06, the propellers reached the full position; 4 seconds later, the PF requested that the propellers be selected to full. Almost immediately following this, the aircraft touched down hard in a flat attitude about 263 feet beyond the runway threshold. The right main landing gear (MLG) collapsed, and 82 feet further down the runway, the right propeller contacted the runway. The aircraft settled onto its right wing and engine nacelle, and subsequently veered to the right and departed the runway. The aircraft came to rest about 1850 feet from the threshold and 22 feet from the runway edge, on a heading of approximately 090° (Figure 1).
There were no injuries and there was no post-impact fire. The crew and passengers evacuated the aircraft through the cabin door.

1.2 Injuries to persons
| Crew | Passengers | Others | Total | |
|---|---|---|---|---|
| Fatal | – | – | – | – |
| Serious | – | – | – | – |
| Minor/none | 2 | 2 | – | 4 |
| Total | 2 | 2 | – | 4 |
1.3 Damage to aircraft
The aircraft was substantially damaged.
1.4 Other damage
The runway had multiple scrapes caused by the aircraft sliding along it and the right propeller contacting the runway surface.
1.5 Personnel information
Records indicated that the crew was certified and qualified for the flight in accordance with existing regulations.
| Captain | First officer | |
| Licence | Airline pilot | Commercial pilot |
| Medical expiry date | 01 September 2015 | 01 November 2015 |
| Total flying hours | 1723.9 | 532 |
| Flying hours on Beechcraft King Air A100 | 298.3 | 70.1 |
| Flying hours on Beechcraft King Air B200 | 177.3 | 107.5 |
| Flying hours in last 90 days | 33.9 | 56.5 |
| Flying hours on A100 in last 90 days | 19.2 | 39.5 |
| Days off duty prior to work | 15 | 1 |
The captain had been employed part time at MAC for about 10 years. The captain's last A100 recurrent pilot proficiency check had been in May 2015, and his last flight on the A100 had been 16 days prior to the occurrence flight. All of the captain's flying hours on the A100 had been accumulated during his employment at MAC.
The FO had been employed at MAC for about 2 years. The FO had completed a pilot competency check for the A100 in May 2015, and his last flight in the A100 had been 10 days prior to the occurrence flight. The FO's pilot competency check did not qualify him to be a captain on the A100.
1.6 Aircraft information
| Manufacturer | Beechcraft* |
|---|---|
| Type, model, and registration | Aeroplane, King Air A100, C-FDOR |
| Year of manufacture | 1972 |
| Serial number | B-103 |
| Certificate of airworthiness issue date | 27 March 1972 |
| Total airframe time | 14 345 hours |
| Engine type (number of engines) | Turboprop, Pratt & Whitney Canada, PT6A-28 (2) |
| Maximum allowable take-off weight | 11 500 pounds |
| Recommended fuel types | Jet-A1, Jet-A, Jet-B |
| Fuel type used | Jet-A1 |
* The Beechcraft Corporation is owned and operated by parent company Textron Aviation Inc.
1.6.1 General
The A100 is a pressurized twin-engine turboprop aircraft. The occurrence aircraft was configured to carry 2 crew members and up to 8 passengers.
Records indicate that the aircraft was certified, equipped, and maintained in accordance with existing regulations and approved procedures. There was no indication of a component or system failure prior to the occurrence landing. The aircraft's weight and centre of gravity were within prescribed limits.
The investigation determined that the landing distance calculated by MAC was in accordance with the A100 Airplane Flight Manual (AFM) for landing with full flaps and without propeller reversing, under the conditions of that day and at the reported landing weight.
1.6.2 Landing gear system
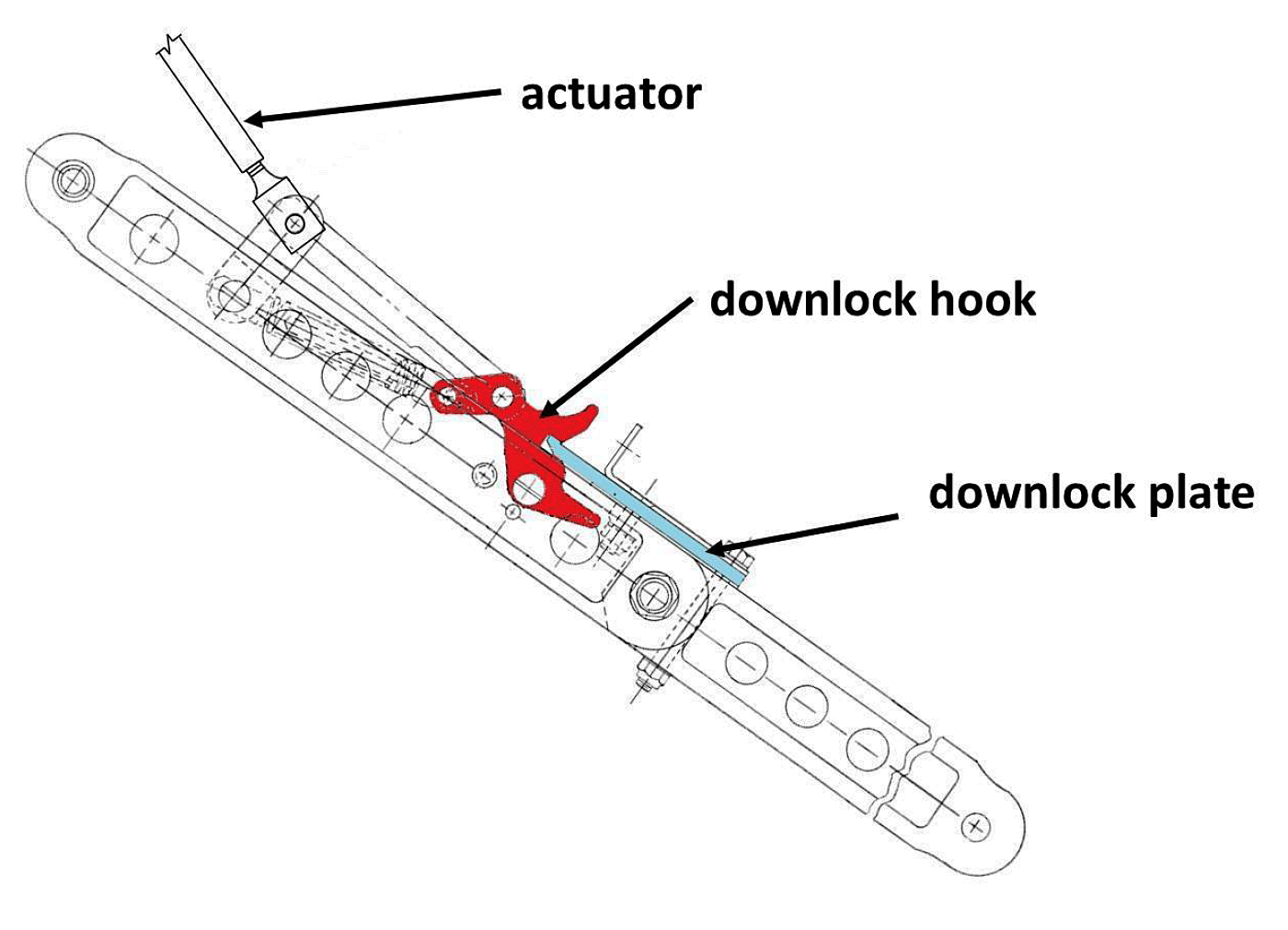
The A100 is equipped with a retractable tricycle landing gear system. The landing gear is retracted and extended by hydraulic actuators, which receive fluid under pressure from an electrically driven pump.Footnote 10 Extending the actuators lowers the landing gear. The MLG drag brace assembly includes a downlock hook on the upper drag brace and a plate on the lower drag brace. When the actuator is extended, the 2-piece drag brace assembly unfolds, causing the hook to rotate and engage the end of the plate. When the landing gear is fully extended and in the down and locked position, the drag brace pivot points are aligned, and the hook and plate are fully engaged. This configuration maintains the drag brace assembly in a positive down and locked position and allows the drag brace to act as a rigid component of the landing gear assembly (Figure 2).
1.6.3 Emergency locator transmitter
The aircraft was equipped with an Ameri‑King Corporation 406-megahertz automatic fixed emergency locator transmitter (ELT) that can be activated either manually or automatically. Manual activation occurs by selecting the switch on the ELT to the "ON" position. Automatic activation occurs when the switch on the ELT is in the "ARM" position, and forward impact forces activate its internal acceleration switch.
The ELT was found mounted in the correct orientation and the activation switch was in the "ARM" position. The TSB Laboratory tested the ELT and no discrepancies were noted. There were insufficient forward impact forces to automatically activate the ELT.
1.6.4 Passenger seat shoulder harness
The passenger seats installed in the occurrence aircraft were not equipped with shoulder harnesses, nor were shoulder harnesses required by regulation.
According to Canadian Aviation Regulations (CARs) subsection 605.24(3),Footnote 11 any small aircraft manufactured after 12 December 1986 with an initial type design that provides for not more than 9 passenger seats must have passenger seats equipped with a safety belt that includes a shoulder harness. There are no regulatory requirements mandating the installation of the shoulder harness in small aircraft built prior to this date, including the occurrence aircraft.
In 1970, Beechcraft issued Service Instruction 0937, "Notice of Availability of Shoulder Restraint Belts for Passengers," to notify owners of various Beechcraft aircraft models, including the A100, of the availability of chair assemblies or harness kits that would provide shoulder restraints for passengers. The installation of these upgrades was strongly recommended as a means of enhancing passenger safety.
The occurrence aircraft's serial number indicates that compliance with this Service Instruction would require the aircraft owner to acquire the complete chair assembly, as the harness kits were not applicable.
MAC had not considered the lack of passenger seat shoulder harnesses to be a safety concern, and was unaware of Service Instruction 0937.
1.6.5 Navigation system
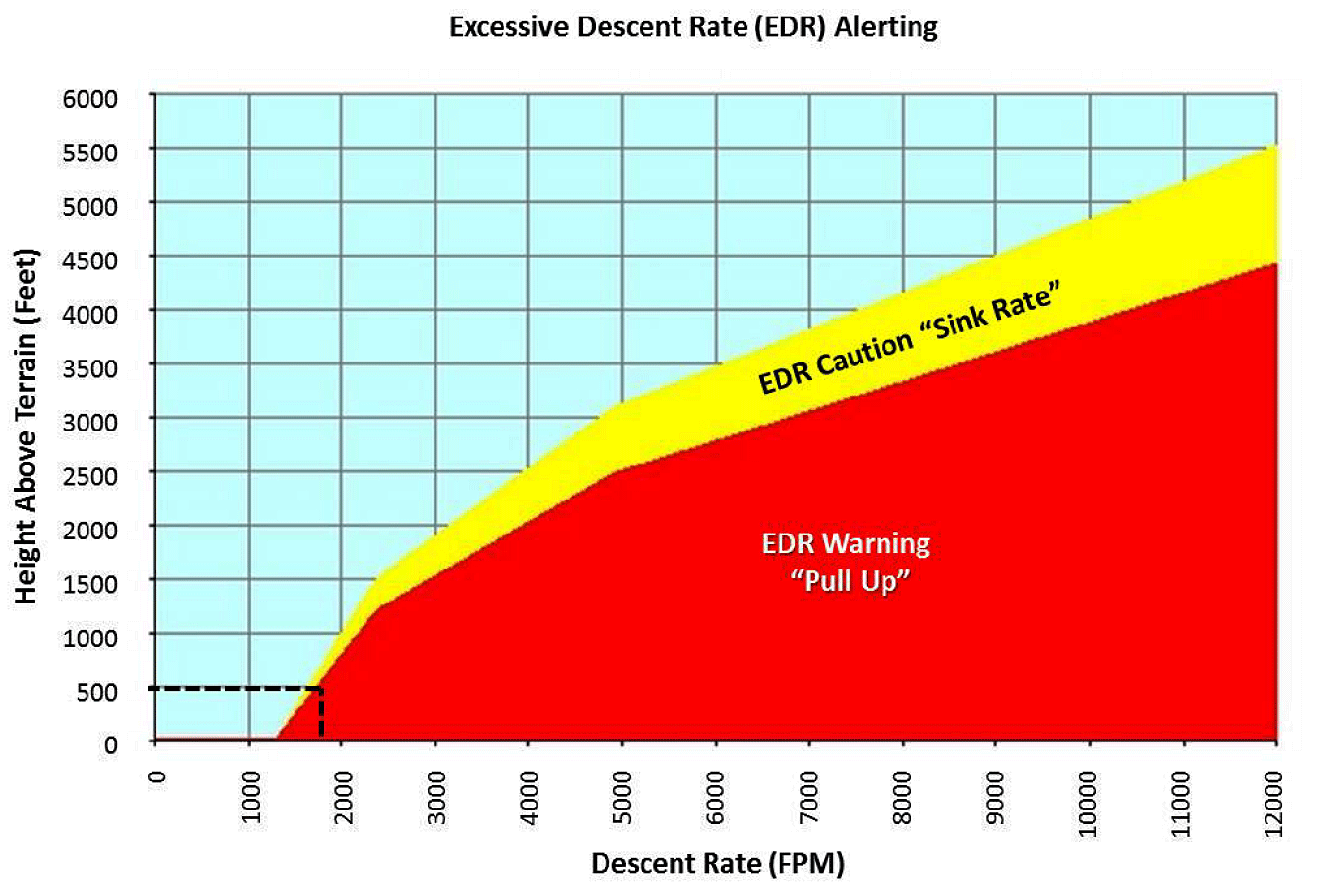
The aircraft was equipped with a Garmin International, Inc. GTN 750 navigation system. The system's TAWS feature includes excessive descent rate alerts to provide notifications when the aircraft is determined to be descending toward terrain at an excessive rate.
Based on the excessive descent rate criteria, for the TAWS to call "SINK RATE" then "PULL UP, PULL UP" in very quick succession when the aircraft is about 500 feet above terrain, the descent rate would have had to be at least 1750 feet per minute (Figure 3).
1.7 Meteorological information
About 20 minutes prior to the landing, the Port Hawkesbury Airport automated weather observation system reported the weather as follows: wind 310° magnetic at 10 knots, visibility greater than 9 statute miles, sky clear, temperature 29°C, dewpoint 19°C, altimeter 29.98 inches of mercury.
1.8 Aids to navigation
CCZ4 is not serviced by any ground-based navigational aids.
1.9 Communications
All communications with the aircraft during the flight were normal.
1.10 Aerodrome information
CCZ4 is an uncontrolled aerodrome operated and maintained by the Municipality of the County of Inverness. It has a single asphalt runway, 01/19, which is 2500 feet long by 75 feet wide. Runway elevation is 181 feet ASL.
The NAV CANADA Canada Flight Supplement includes a caution stating that high terrain of up to 1400 feet ASL is located within 3 nm of the aerodrome.
1.11 Recorders
The aircraft was not equipped with a flight data recorder, nor was one required by regulation.
The aircraft was equipped with a cockpit voice recorder (Honeywell Model AR-30, part number 980-6023-001, serial number 0590), although this was not required by regulation either. The cockpit voice recorder had a recording capacity of 30 minutes, and its recorded data included the data of the occurrence flight. The cockpit voice recorder memory was downloaded successfully and contained good-quality audio of the occurrence flight, which provided useful information to the investigation.
Numerous TSB aviation investigation reports have cited a lack of onboard recording devices as a factor in investigators' inability to determine all of the reasons why an accident occurred.Footnote 12 The benefits of recorded flight data in aircraft accident investigations are well known and documented.Footnote 13 If data recordings are not available to an investigation, then the identification and communication of safety deficiencies to advance transportation safety may be precluded.
1.12 Wreckage and impact information
1.12.1 General
When the aircraft departed the runway, it struck several small trees and came to rest on its right wing and engine nacelle. The left MLG and the nose landing gear remained extended.
The right propeller blades were bent and abraded. The right flaps were crushed, and the right wing sustained damage to the tip, the leading edge, and the upper and lower surfaces. The right engine oil cooler scoop sustained abrasion damage, and the right MLG doors were buckled and abraded. The right side of the fuselage adjacent to the propeller sustained several small dents.
1.12.2 Right main landing gear
The right MLG drag brace downlock plate was found bent. The plate had disengaged from the downlock hook, the drag brace assembly had folded up to the retracted position, and the right MLG actuator was found fully extended.
The right MLG drag brace assembly and the downlock assembly components were examined by the TSB Laboratory. The downlock plate had a bend of approximately 33°, consistent with an overload resulting from a hard landing. When the plate had disengaged from the hook, it had allowed the drag brace to fold up (retract) under the weight of the aircraft.
1.13 Medical information
The investigation determined that there was nothing to indicate that the crew's performance was degraded by fatigue.
1.14 Fire
Not applicable.
1.15 Survival aspects
1.15.1 Passenger seat shoulder harness
The use of a 3-point or 4-point safety restraint (safety belt and shoulder harness) is known to reduce the severity of upper-body and head injuries and to more evenly distribute impact forces.Footnote 14
The risk of serious injury or death is increased for light-aircraft occupants who are not wearing upper-torso restraints or shoulder harnesses. The results of previous safety studiesFootnote 15 have been more recently supported by a Federal Aviation Administration study on fatal and serious-injury accidents in Alaska.Footnote 16
1.16 Tests and research
1.16.1 TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP262/2015 – Main Landing Gear Examination
- LP265/2015 – ELT Examination
- LP266/2015 – G-Switch Examination
1.17 Organizational and management information
1.17.1 Maritime Air Charter Limited
MAC is a privately owned company that has been operating since 1996. The company conducts CARs Subpart 703 air taxi operations, providing domestic and international air charters. At the time of the occurrence, in addition to the occurrence aircraft, the company operated 1 Beechcraft King Air B200 (B200) and 2 Piper Navajo PA-31s.
According to the company operations manual, the operations manager was responsible for safe flight operations, the chief pilot was responsible for the professional standards of the flight crews, and the maintenance coordinator was responsible for the effective control of the air operator's maintenance system. The individuals occupying these positions were all pilots and carried out flying duties in addition to their management responsibilities.
In January 2015, MAC had a new individual approved by Transport Canada (TC) for the position of operations manager. This person was also assigned the responsibilities and duties of chief pilot. At the time of the accident, in addition to the new operations manager / chief pilot and the company president, MAC employed 1 part-time pilot and 3 full-time pilots.
1.17.2 Maritime Air Charter Limited's safety management system
Although not required by regulation to do so, MAC had voluntarily implemented a safety management system (SMS) in 2007. The system was consistent with the SMS components identified in TC's Technical Publication 14135, Safety Management Systems for Small Aviation Operations: A Practical Guide to Implementation.Footnote 17 Because there is no regulatory requirement for CARs Subpart 703 operators to have an SMS, TC did not review or approve MAC's SMS.
MAC's SMS defines the process of identifying safety hazards and minimizing the resulting risks and states, "Following SOPs that are rooted in safe practices and avoiding shortcuts that can detract from safety should be the daily goal of all individuals."Footnote 18
The accountable executive'sFootnote 19 safety policy statement reads, in part, "SMS cannot succeed without the full support of the company's management."Footnote 20
The operations manager was identified as the individual responsible for overseeing all aspects of the SMS and ensuring that all supervisory personnel were fully aware of them. Aspects of the SMS included investigating and analyzing reported hazards to identify their root causes and ensure that corrective actions were carried out.
Section 5.12.1 of the company operations manual indicates that a pilot's initial and annual training would include 12 minutes to cover the SMS. However, none of the company manuals included a description of the SMS training.
Both the captain and FO had received SMS training during their 2015 recurrent training.
MAC's SMS included the following elements:
- safety hazard reports;
- risk management reports with root-cause analysis descriptions;
- short- and long-term corrective action plans that end with an effectiveness review at a prescribed future date;
- a no-blame reporting policy and safety goals;
- a maintenance policy for the SMS;
- an annual trend analysis; and
- a retention schedule for SMS documentation.
MAC used the SMS elements proactively, to implement employees' suggestions for improvements, and reactively, in response to TC findings identified during previous surveillance activities and through safety concerns identified by company personnel.
MAC produced annual SMS trend analyses in 2012 and 2013, and SMS report summaries in 2011, 2012, and 2013. A safety newsletter was also published in 2011, highlighting the more important safety hazards and their corrective actions. These instances were the only occasions on which these reports were produced.
1.17.3 Transport Canada oversight
1.17.3.1 General
TC expects companies to proactively manage the safety of their operations—where risks are managed to acceptable levels—and to have programs in place to ensure their continued compliance with all regulatory requirements. TC's surveillance program is designed to assess whether an aviation company has implemented appropriate and effective systems. Specific systems-based surveillance inspections are conducted at intervals that are based on risk indicators. The program is targeted at key systems determined by certificate type and whether or not a given company is required to have an SMS.
The surveillance program is based on a systemic approach to managing risk and includes the following steps:
- documentation review;
- on-site interviews and on-site sampling conducted by inspectors; and
- production of a report with findings of systemic deficiencies.
This approach allows inspectors to understand how a company plans to meet a specific regulatory requirement. The sampling portion involves selection by inspectors of specific areas, or outputs, to test compliance with that system and with the applicable regulations.
TC normally conducts program validation inspections (PVI) on a routine schedule, based on risk indicators that are used to determine the frequency of inspection. Under TC's current approach to surveillance, planned surveillance intervals may be as frequent as every year for high-risk or high-impact companies, or as infrequent as every 5 years for those that pose a lower risk or impact, as determined by TC. These intervals are subject to annual review, and may be adjusted at any time if TC believes that it is warranted by changes in a company's risk indicators.
During a PVI, the TC team will conduct interviews, gather evidence to support observations, and analyze those observations. It will then determine whether the operator is in compliance with regulations and whether the operator's SMS is effective (if the organization is required to have an SMS). The team will also prepare any findings of non-compliance and document the results of the on-site review.
A process inspection (PI) is another surveillance tool used by TC to determine whether an operator's processes meet regulatory requirements and are functioning as intended. Unlike a PVI, the scope of a PI is limited to a single process and is intended to help TC determine the level of risk associated with an operator and whether additional surveillance is required. Like a PVI, a PI may also generate findings; however, those findings are not assigned ratings. The PI report indicates whether the process meets applicable regulatory requirements and is being followed as published in approved company manuals, or whether the process is not documented, not implemented, or not effective. In some cases, the results of a PI may lead to a PVI being conducted at an earlier interval than originally planned.
In principle, any process required by regulation may be the focus of a PI or a PVI. Targeted PIs across a range of areas have the potential to identify a lack of compliance with regulations requiring those processes. If a PI reveals safety-related deficiencies, then a PVI may be conducted on an urgent basis to collect sufficient material to support the issuance of a formal report and certificate action, if necessary.
TC uses a risk indicator "which provides a numerical representation of conditions or changes within an enterprise that have an impact on TCCA's [Transport Canada Civil Aviation's] surveillance decision making process."Footnote 21 A formal risk assessment (outside of the risk indicator) is not usually carried out for each enterprise when the planned surveillance schedule is determined. TC also uses information from the Civil Aviation Daily Occurrence Reporting System, enforcement records, intelligence information, and TC's historical knowledge of the enterprise—all of which could reduce the interval proposed by the risk indicator tool.
Under section 7 of the Aeronautics Act, the Minister of Transport has the authority to suspend a Canadian aviation document. TC Staff Instruction "Suspension or Cancellation of Canadian Aviation Documents for Safety Reasons" (SI SUR‑014)Footnote 22 provides guidance on how to take certificate action under the Aeronautics Act. SI SUR‑014 specifies that one of the reasons that certificate action may be taken, in accordance with paragraph 7.1(1)(c) of the Aeronautics Act, is for public interest.
This paragraph of the Aeronautics Act is used when the aviation record of the document holder includes instances of non-compliance that are "serious and repeated enough to conclude that there is a risk of further offences."Footnote 23 In regard to pursuing certificate action under this part of the Act, SI SUR-014 states that it would be appropriate to consider records, including accident records, compliance records (aviation enforcement division records), and audit, program validation, or assessment records as they relate to system compliance. SI SUR‑014 adds that non-compliance issues that were identified during oversight and have been resolved through corrective action do not warrant the pursuit of such certificate action.
1.17.3.2 Notice of suspension
In October 2014, the 2 owners of MAC were the company president / chief pilot and the maintenance coordinator / person responsible for maintenance (PRM).
On 03 October 2014, TC issued a notice of suspension (NOS) to MAC under paragraph 7.1(1)(c) of the Aeronautics Act, effective 03 November 2014. The NOS listed 23 regulatory reasons for the grounds for suspension. All but one of these originated from the period between January 2010 and February 2014.
Of the 23 regulatory reasons, 17 were directly related to the operations manager not ensuring that the company was in compliance with the CARs, and the remaining 6 were specifically about the person who held the position of PRM. Some of the reasons pertained to exceedances of flight and duty times and inadequate rest periods for pilots, including for the chief pilot, the operations manager and the PRM.
A total of 6 violations were identified, with the company or individual, or both, receiving a monetary penalty. The violations included the following incidents:
- In June 2012, an aircraft with a known landing-gear defect was used for a commercial passenger-carrying flight, resulting in a landing-gear collapse accident.
- In October 2007, an aircraft flown by MAC's PRM ran out of fuel during a commercial passenger-carrying flight and was forced to land at an alternate airport with no engine power.
The conditions for terminating the suspension stipulated that MAC was to carry out an analysis to determine the root cause(s) of the operations manager's failure to fulfill some of the responsibilities of the position. Among these was the responsibility to ensure that the air operator's operations were being conducted in accordance with current regulations, standards, and air operator policy.
As part of the corrective action plan submitted and accepted by TC, MAC hired a new individual for the operations manager / chief pilot position. After accepting MAC's corrective action plan, TC determined that the conditions for terminating the suspension had been complied with, and on 28 October 2014, the NOS was terminated.
In January 2015, TC approved MAC's new operations manager.
1.17.4 Maritime Air Charter Limited's A100 standard operating procedures
1.17.4.1 General
MAC's A100 SOPs are intended to ensure that flight crews operate within the aircraft's limitations and the manufacturer's approved AFM. The SOP manual states that it supplements the AFM and that the AFM always takes precedence. Although the SOPs cannot cover all circumstances, MAC expects all personnel to exercise sound judgment and consistency in their application.
According to the SOPs, checklists are required to be used during normal operation.
1.17.4.2 Engine Run-up checklist
MAC's Engine Run‑up checklist must be completed prior to the first flight each day.Footnote 24
The investigation determined that it had become common practice for MAC pilots not to perform the Engine Run-up checklist when passengers were on board the aircraft. For training flights and flight tests, the Engine Run-up checklist was followed.
1.17.4.3 Landing checklists
On final approach, the PF is to call for the Landing Checks checklist and the PNF is to confirm that the checklist has been completed.
The Landing Checks checklist includes setting the flaps to approach, selecting and confirming that the landing gear is down, selecting the propeller levers to obtain 2000 revolutions per minute, then selecting the flaps to full.
The After Landing Checks checklist requires the propeller controls to be selected to the full position.
For a visual approach, in addition to carrying out the Landing Checks checklist, the PNF is required to call out "1000 above" and "500 above."Footnote 25
1.17.4.4 Briefings
The SOPs do not identify a requirement for the crew to perform a pre-flight briefing.
An approach briefing is required for every approach to ensure that the PNF is aware of the PF's intentions and to identify any tasks that the PNF will need to perform.
The company's VFR approach briefing consists of air traffic control instructions, the runway in use, altitudes, and missed-approach instructions.
1.17.4.5 Approach and landing guidance
MAC does not have formalized stable approach criteria and does not perform a formal risk assessment when dispatching crews and aircraft. Neither of these elements is required by regulation.
The SOPs do not contain information related to potential threats associated with unstable approaches, nor do they identify a requirement for crews to discuss a touchdown point on the runway. The company expects pilots to use their knowledge, skills, and experience to assess whether an approach is stable and react accordingly, including by conducting a go‑around when circumstances dictate.
The SOPs specify that when pilots are carrying out an approach, the aircraft is to descend at 600 to 800 feet per minute. The engine power set during a standard approach would be higher than what is required to activate the auto-ignition system.
The SOPs include a diagram depicting the company's visual approach/VFR circuit. MAC's diagram shows that when the aircraft is in the downwind leg, the flaps should be set at 30% and the speed at below 153 knots. When the aircraft is abeam the runway threshold, the landing gear should be lowered and the landing checks completed. When the aircraft is turning base leg, the speed should be reduced to 120 knots and a descent begun at a standard 3° approach slope. On final approach, the speed should be 120 knots with full flaps selected, slowing to 100 knots for landing.
The PNF is to make a standard call whenever the speed has deviated from the planned approach speed. This call is to include the deviation.
1.17.5 Propeller full position
According to the A100 AFM, the only time the propellers are to be selected to full just prior to touchdown is when a maximum reverse power landing is being performed. However, before the propellers can be adjusted, the fuel condition levers must be selected to the high idle position, which increases engine power. MAC's SOPs do not include a maximum reverse power landing, nor does the company have an applicable checklist.
According to the B200 AFM, the propellers must be selected to full prior to touchdown. There is no requirement to select the fuel condition levers to the high idle position.
1.18 Additional information
1.18.1 Organizational safety culture
Safety culture can be described as "the way we do things around here."Footnote 26 Culture is deeply ingrained, and its impact on safety may not be readily apparent to those working within a given culture.
According to the International Civil Aviation Organization (ICAO),
Organizational culture sets the boundaries for accepted executive and operational performance by establishing the norms and limits. Thus, organizational culture provides a cornerstone for managerial and employee decision making.Footnote 27
One of the largest influences on safety culture is management commitment and style. ICAO describes the role of management in creating a positive organizational safety culture as follows:
Those in the best position to effect accident prevention by eliminating unacceptable risks are those who can introduce changes in the organization, its structure, corporate culture, policies and procedures, etc. No one is in a better position to produce these changes than management.Footnote 28
Organizations must strike a balance between safety and production by managing risks present in their operation. The challenge for an organization is to operate efficiently while minimizing safety risks. The reality within many organizations is that production and operational concerns may at times seem more pressing, since they are more measurable and provide immediate feedback in terms of results. Therefore, in the minds of decision-makers, operational concerns may be more salient than safety-related concerns.
The traditional approach to safety management is based on compliance with regulations and a reactive response to incidents and accidents. Although compliance with safety regulations is fundamental to the development of sound safety practices, organizations that simply comply with the standards set by regulations are not well situated to identify emerging safety problems.
According to ICAO,
As global aviation activity and complexity continue to grow, […] traditional methods of managing safety to an acceptable level [become] less effective and efficient. Different, evolved methods of understanding and managing safety are necessary.Footnote 29
And, as summarized in TSB Aviation Investigation Report A07A0134,
Modern safety management principles promote a proactive search for hazards, identification of risks, and the best defences to reduce risk to an acceptable level. These principles must be embedded within an organization's management system so that safety policies, planning, procedures, and performance measurement are integrated into day-to-day operations.
Organizations differ considerably with regard to the level of risk they tolerate within their operations. Those organizations that take proactive steps to identify and mitigate risks are considered to have positive safety cultures, while other organizations with poor safety cultures knowingly or unknowingly operate with higher levels of risk. An organization that operates with significant risk faces greater potential for an accident.
1.18.2 Unstable approaches are a 2016 Watchlist issue
The Watchlist identifies the key safety issues that need to be addressed to make Canada's transportation system even safer.
Every year, there are millions of successful landings on Canadian runways. Unstable approaches, however, significantly increase the risk of accidents during the landing phase of flight—accidents that can result in aircraft damage, injuries, and even fatalities. These accidents include hard landings. Unless there is more compliance with airlines' stable‑approach policies, unstable approaches will carry on being continued to landing, increasing the risk of approach-and-landing accidents.
As this occurrence demonstrates, accidents involving unstable approaches continue to occur at Canadian aerodromes.
1.18.3 Landing technique
According to TC's Aeroplane Flight Training Manual,
Achieving the performance figures given in the Aircraft Flight Manual requires careful handling of the aircraft and good judgement. The aim is to approach at the airspeed recommended for the aircraft weight and to touch down at the desired spot at the lowest possible airspeed commensurate with safety. Touching down at the required spot requires precise control of the approach so that the flare is at the right point and at the right speed.
[…]
On a short field approach power is required to more accurately control the rate of descent. When power is used, very little change in the aircraft's pitch attitude is required to make any necessary corrections in the approach slope.Footnote 30
Reducing the rate of descent without applying engine power would require the aircraft to be pitched up, thereby causing the airspeed to decrease.
1.18.4 Stable approach
1.18.4.1 General
Stable approaches significantly increase the chances of a safe landing. Research indicates that 3.5% to 4% of approaches are unstable. Of these, 97% are continued to a landing, with only 3% resulting in a go-around. Without improvements in stable-approach policy compliance, most unstable approaches will continue to a landing, increasing the risk of approach‑and‑landing accidents.Footnote 31
According to TC, an approach is considered stabilized if it meets the air operator's stabilized approach criteria.
1.18.4.2 Civil Aviation Safety Alert
On 06 August 2015, TC issued Civil Aviation Safety Alert (CASA) No. 2015-04, "Stabilized Approach." The purpose of the CASA was "to stress the importance of, and to outline the elements of a stabilized approach."Footnote 32 The document summarizes the stabilized approach concept as "maintaining a stable speed, descent rate, and vertical/lateral flight path in the landing configuration."Footnote 33
CASA No. 2015-04 also states the following:
Rushed and unstabilized approaches remain a significant factor in Controlled Flight Into Terrain (CFIT) and other Approach-and-Landing Accidents (ALA). The safety benefits derived from a stabilized final approach have been recognized by many organizations including ICAO, the FAA [Federal Aviation Administration], EASA [European Aviation Safety Agency] and TCCA [Transport Canada Civil Aviation]. These benefits include:
- Increased flight crew situational awareness;
- More time and attention for monitoring ATC communications, weather conditions and systems operation;
- More time and attention for flight path and energy monitoring;
- Defined flight parameter deviation limits and minimum stabilization heights to support the decision to land or to go-around; and,
- Landing performance consistent with expected performance values.Footnote 34
TC has indicated that all operators should define stabilized approach criteria for all of the approaches they fly, and that an approach is considered stabilized when those criteria are based on the following:
- Range of speeds specific to the aircraft type;
- Power setting(s) specific to the aircraft type;
- Range of attitudes specific to the aircraft type;
- Configuration(s) specific to the aircraft type;
- Crossing altitude deviation tolerances;
- Sink rate; and
- Completion of checklists and flight crew briefings.Footnote 35
TC encourages operators to always follow their stabilized approach procedures, and recommends that those procedures include
- close monitoring of airspeed, sink rate, and energy state during a visual or instrument approach;
- monitoring of the aircraft state and flight path using all available lateral and vertical guidance and visual aids;
- verbal communication about the aircraft state and its progression along the approach; and
- an announcement and prompt correction of any significant deviations from planned flight path, airspeed, or descent rate.
If the approach cannot be continued within the company's stabilized approach parameters, then a go-around is required.
TC states that "[i]t is important to note that the decision to execute a go-around is not an indication of poor flight crew performance but rather prudent decision making."Footnote 36
1.18.5 Flight Safety Foundation
The Flight Safety Foundation (FSF) has stated that "[t]he failure to recognize the need for and to execute a missed approach when appropriate is a primary cause of approach-and-landing accidents."Footnote 37 The FSF has also noted that "[t]he lack of a go-around decision is the leading risk factor in approach and landing accidents and is the primary cause of runway excursions during landing. Yet, less than 5% of unstabilised approaches lead to a go-around."Footnote 38
A go-around, or missed approach, is a normal phase of flight.Footnote 39 The procedures associated with performing a go-around are included in a pilot's initial training and recurrent training. Although a go-around is not a frequent occurrence, if it becomes necessary, then immediate and positive action must be taken by the pilot. This decision and the actions taken become more critical the closer the aircraft is to the ground, because the aircraft is in a lower state of energy.
Aircraft energy is a function of the airspeed and airspeed trend, altitude, vertical speed, drag (flaps and landing gear), and thrust. One of the primary tasks of the flight crew is to control and monitor the aircraft's state of energy to maintain the appropriate energy condition for the flight phase or to recover the aircraft from a low- or high-energy condition.Footnote 40
According to the FSF,
he flight crew's inability to assess or to manage the aircraft's energy condition during approach is cited often as a cause of unstabilized approaches. Either a deficit of energy (low/slow) or an excess of energy (high/fast) may result in an approach-and-landing incident or accident. . . .Footnote 41
These incidents or accidents can include a hard landing.
1.18.6 Pilot decision making
Pilot decision making can be described as making the right choice at the right time, and avoiding circumstances that can lead to difficult choices. Many decisions are made on the ground, and a well-informed pre-flight choice avoids the need for a much more difficult in‑flight decision.
An important component of pilot decision making is good situational awareness, which requires a pilot to align the reality of a situation with his or her expectations. Inadequate or ineffective pilot decision making can result in operating beyond an aircraft's capability or exceeding the pilot's abilities.
1.18.7 Crew resource management
The objective of crew resource management (CRM) is to reduce human error in aviation. In Canada, CRM training is not required by regulation for CARs Subpart 703 and 704 operators.
Every flight presents hazards that must be handled by the crew. These hazards, referred to as threats, increase the risks during a flight and include short runways and unfamiliar aerodromes. Provided the crew members have an opportunity to handle the threat, effective management of a hazard leads to a positive outcome with no adverse consequences—that is, the crew members take action to mitigate the threat. However, mismanagement of the threat can lead to crew error, which the crew must also manage. Mismanagement of crew error may lead to an undesired aircraft state, which can lead to an accident. At any point, effective management of the situation by the crew, such as by performing a go-around, can mitigate the risk and the situation may be inconsequential.
The most common crew behaviours cited for effective error management are vigilance and crew member advocacy and inquiry. The effective management of risks by the flight crew is inextricably linked to effective CRM.
In terms of CRM, effective communication plays a critical role in the alignment of the crew's understanding of the situation. However, communication skills require practice and reinforcement to be effective, particularly during periods of high workload, such as during an abnormal situation.
Situational awareness is defined as "the perception of elements in the environment within a volume of time and space, the comprehension of their meaning, and the projection of their status in the near future."Footnote 42
By this definition, maintaining situational awareness is a result of 3 individual processes on the part of the flight crew. First, the crew must perceive information from the environment. Second, the relevance of this information to the ability to achieve operational goals must be established. Third, the crew must use this information to project future states and events. As a result, maintaining these 3 levels of situational awareness allows crews to "plan ahead and prepare for contingencies,"Footnote 43 which leads to more effective decision making. All 3 levels involve information-processing stages at which shortcomings may occur and that may result in incomplete or inadequate situational assessments.
Flight crew actions need to be based on a common understanding of the current state of the aircraft and the intended flight plan, and on the threats to these activities, in order for the crew to perform in a coordinated, efficient, and safe manner. This common understanding between the crew members is referred to as team or shared situational awareness.Footnote 44, Footnote 45 When this understanding is consistent, crews are better able to effectively anticipate and coordinate their actions toward achieving their common goal.
Shared situational awareness is developed and maintained by a crew through a number of discrete and continuous behaviours. Discrete behaviours include flight planning, in-flight briefings, and identification of key points in the flight, such as attaining minimum altitudes. These activities are planned checkpoints to describe current state and future plans, and to provide an opportunity to ensure that all crew members have a common understanding.
Continuous behaviours include threat-and-error management, callouts of changes in aircraft state and instrument setting/mode, and communication of changes to plans. These behaviours ensure that information and state changes are communicated between crew members to update the shared situational awareness on an ongoing basis. Such continuous behaviours are influenced by the training and operational approach taken by operators.
In 2009, during its investigation into a January 2007 occurrence involving a collision with terrain in Sandy Bay, Saskatchewan (TSB Aviation Investigation Report A07C0001), the TSB found that ineffective CRM had contributed to the accident. Therefore, the Board recommended that
The Department of Transport require commercial air operators to provide contemporary crew resource management (CRM) training for Canadian Aviation Regulations (CARs) subpart 703 air taxi and CARs subpart 704 commuter pilots.
Transportation Safety Recommendation A09-02
The TSB assessed TC's latest response to Recommendation A09-02 as follows:
Transport Canada (TC) continues to make progress toward implementation of this recommendation. Until all regulatory changes proposed by TC are enacted, the deficiency identified in Recommendation A09-02 will continue to exist. However, the proposed regulatory changes, if fully implemented, should reduce the risks associated with the safety deficiency identified in Recommendation A09-02.
The Board considers the response to the recommendation to indicate Satisfactory Intent.
Training records indicated that MAC had provided 4 hours of CRM training during the pilots' annual recurrent training. However, none of the company manuals included a description of the CRM training.
1.18.8 Information processing
Pilots operate in a complex environment where there are multiple sources and types of information to monitor and keep track of. When pilots receive information that is contrary to their expectations, their reactions will be slower and may be inappropriate.Footnote 46 A number of biases are known to have an impact on how information is interpreted and attended to in complex environments.
Expectation bias contends that when individuals expect one situation, they are less likely to notice cues indicating that the situation is not quite what it seems. Expectation bias is worsened when people are required to integrate new information that arrives piecemeal over time in incomplete, sometimes ambiguous, fragments.Footnote 47
Plan continuation bias is a "deep-rooted tendency of individuals to continue their original plan of action even when changing circumstances require a new plan."Footnote 48 Once a plan is made and committed to, it becomes more difficult for stimuli or conditions in the environment to be recognized as indicating change than if a plan had not been made. If a reason to change the plan is to be recognized and acted upon by a pilot in a timely manner, a condition or stimulus needs to be perceived as sufficiently salient to require immediate action
1.19 Useful or effective investigation techniques
Not applicable.
2.0 Analysis
2.1 Introduction
The aircraft was certified, equipped, and maintained in accordance with regulations, and no discrepancies were noted that would have prevented it from operating normally. The flight crew members were certified and qualified in accordance with regulations.
In an effort to establish an understanding of why the accident happened, this analysis will focus on the events, conditions, and underlying factors that caused or contributed to the accident, including the crew selection process, crew resource management (CRM), the go‑around decision, the approach, and organizational safety culture.
2.2 Crew selection and pairing
It is the responsibility of the company to ensure that its flight crews are operationally ready to deal with both normal and abnormal situations that can be anticipated in their roles. Maritime Air Charters Limited (MAC) did not have an established process for determining whether the risks associated with a proposed flight were acceptable.
The captain's last flight in the Beechcraft King Air A100 (A100) was 16 days prior to the occurrence, and the first officer's was 10 days prior to the occurrence. In the last 90 days, the captain had flown a total of 19.2 hours on the A100. Over the same period, the first officer had accumulated more than twice that number of flying hours (39.5) on the A100. Although the first officer's qualifications prevented him from being the captain, they would not have precluded him from being the pilot flying (PF).
Even though both crew members were experienced pilots and had previously flown together, neither had flown to Margaree Aerodrome (CCZ4) before, and neither had landed an A100 on a runway as short as 2500 feet.
MAC's crew pairing was based on personnel availability. The company relied on the pilots' expertise to manage the variable conditions and risks that could be encountered during the flight, including deciding whether to continue with an approach and landing, whether a go‑around is necessary, and whether to execute a go-around if circumstances dictate. This heavy reliance on crew expertise to manage the potentially unpredictable nature of landing on a short, unfamiliar runway with known high terrain is why optimal crew pairing is essential. If the experience and proficiency of pilots are not factored into crew selection, then there is a risk of suboptimal crew pairing, resulting in a reduction of safety margins.
2.3 Crew resource management
Flight crew actions need to be performed in a coordinated, efficient, and safe manner to ensure that the crew achieves their goals, such as landing as close as possible to the threshold on a short runway.
Neither pilot had considered that landing on a short runway, which was shorter than either had landed on before in the A100, at an unfamiliar aerodrome with high terrain nearby, and joining the circuit on a left base were hazards that may create additional risks.
CRM is directly linked to the effective management of risks by the flight crew. To achieve this, the crew must have a shared situational awareness, which is developed through behaviours such as pre-flight planning, in-flight briefings, and identification of key points in the flight.
When crews use planned checkpoints, such as required checklists and standard callouts, and effectively communicate events, such as a change in aircraft state, on an ongoing basis, then they are more likely to have a shared situational awareness. Having this shared awareness allows crews to effectively anticipate and coordinate their actions to ensure that they achieve their goals. The behaviours associated with shared situational awareness must be continuously practiced and fostered, and are influenced by the training and operational approach taken by operators.
Although the crew's training records indicated that MAC had provided 4 hours per year of CRM training, there was no explanation as to what was included in this training.
Standard operating procedures (SOP) are designed to help pilots maintain situational awareness. They represent an important information resource available to pilots to assist with effectively managing risks and decision making.
MAC's SOPs included a requirement for crews to carry out the Engine Run-up checklist and the Landing Checks checklist. Neither of these was performed by the crew. The approach briefing was to include missed-approach instructions; however, these instructions were not included in the approach briefing provided on the occurrence flight. Although the pilot not flying (PNF) noted that the airspeed was below the planned speed, this deviation was not identified. The callouts of "1000 above" and "500 above" were also not made. If pilots do not carry out checklists in accordance with the company's and manufacturer's instructions, then there is a risk that a critical item may be missed, which could jeopardize the safety of the flight.
Moving the propellers to full was not in accordance with the A100 SOPs. Since the crew did not perform the Landing Checks checklist, the requirement to set the propellers to 2000 revolutions per minute was never conveyed. Therefore, it is likely that the PNF moved the propellers to full while the aircraft was still in flight because of his experience with the Beechcraft King Air B200 (B200), whose propellers must be selected to full prior to touchdown.
Although the PF acknowledged the PNF's action, the acknowledgment was likely just a reflexive response, because, shortly thereafter, the PF commanded that the propellers be moved to the full position. That breakdown in communication, and the actions of the PF and PNF, were consistent with an increased workload and reduced situational awareness, and resulted in a departure from approved procedures.
Although both pilots had received some CRM training, their actions during the occurrence flight were indicative of a breakdown in CRM because they did not have a shared situational awareness during the descent and landing. CRM requires practice and reinforcement to be effective. If CRM is not used and continuously fostered, then there is a risk that pilots will be unprepared to avoid or mitigate crew errors encountered during flight.
2.4 Go-around decision
Prior to departure, the crew discussed the approach; however, they did not discuss under what conditions a go-around would be conducted.
Although MAC's approach briefing is to include missed-approach instructions, the company did not have a go-around policy, nor did it have published guidance to which the pilots could refer. The company relied on its pilots to make decisions regarding when to continue with an approach and when to perform a go-around. If organizations do not have a clearly defined go-around policy, then there is a risk that flight crews will continue an unstable approach, increasing the risk of an approach-and-landing accident.
During the pre-flight briefing and the landing briefing, the crew did not discuss what actions would be taken if a safe landing could not be carried out, such as conducting a missed approach. If pilots are not prepared to conduct a go-around on every approach, then there is a risk that they may not respond to situations that require a go-around.
2.5 Approach
One of the primary tasks of the flight crew is to maintain the appropriate energy condition for the flight phase and, if deemed necessary, to recover the aircraft from a low- or high‑energy condition.
Prior to departure, the crew planned to land as close as possible to the threshold on Runway 01. As the aircraft got closer to the aerodrome, the crew's plan was updated to include entering the circuit directly on a left base leg. The crew broadcasted their intention to join the left base leg about 5 nautical miles from the aerodrome. They planned to remain at a higher altitude until closer to the aerodrome, and did so.
Neither pilot had considered that landing on a short runway at an unfamiliar aerodrome with known high terrain nearby and joining the circuit directly on a left base were hazards that may create additional risks, all of which would increase the crew's workload.
The presence of the tower along the flight path resulted in the PNF focusing his attention on monitoring the aircraft's location rather than on monitoring the flight or the actions of the PF. The PF also had to factor in the tower as a potential risk. The crew's increased workload, together with the unexpected distraction of the presence of the tower, led to a reduced situational awareness that caused them to omit the Landing Checks checklist.
To expedite the descent, the PF reduced the engine power to idle. At no time during the final descent was the engine power increased above about 400 foot-pounds of torque. Therefore, any change in the rate of descent would have been carried out by controlling the pitch (that is, reducing the rate of descent without applying engine power would require the aircraft to be pitched up, thereby causing the airspeed to decrease).
Just after the landing gear was selected down and the flaps were set to full down, the PF corrected for a low airspeed condition by pitching the aircraft down. Since no engine power was applied, this action would have caused the rate of descent to increase.
Almost immediately after that correction was made, the aircraft was descending at about 1750 feet per minute, about 500 feet above the ground. The PF corrected for the excessive rate of descent by pitching up, which would have caused the airspeed to decrease.
Touching down at a specific spot requires precise control of the approach so that the flare is at the right point and at the right speed. When engine power is used to accurately control the rate of descent, very little change in the aircraft's pitch attitude is required to make any necessary corrections. Using only pitch to control the rate of descent prevented the PF from precisely controlling the approach, which would have ensured that the flare occurred at the right point and at the right speed.
The flight crew's inability to effectively manage the aircraft's energy condition led to an unstable approach.
Although the PF acknowledged the terrain awareness warning system calls, neither pilot recognized that the steep rate of descent was indicative of an unstable approach.
When the aircraft was about 120 feet above ground level, the PNF advanced the propellers to full. Because there was no change in engine power, the descent rate would have increased. Therefore, advancing the propellers to full would have increased the drag and further increased the rate of descent, exacerbating the already unstable approach.
During the approach, there was nothing sufficiently salient to cause the crew to re-evaluate their original plan of action, which is consistent with plan continuation bias.
The aircraft crossed the runway threshold with insufficient energy to arrest the rate of descent in the landing flare, resulting in a hard landing that caused the right main landing gear to collapse.
If operators do not have a stable approach policy, then there is a risk that an unstable approach will be continued to a landing, increasing the risk of an approach-and-landing accident.
2.6 Company safety culture
Since the owners of the company also held most of the management positions, they would have been the individuals responsible for fostering the manner in which safety was managed and for establishing the company's safety culture. An organization's culture sets the boundaries for what is considered acceptable performance. These norms and limits are what managers and employees use when making decisions.
In the 7 years preceding Transport Canada's issuance of the notice of suspension, MAC's safety management system (SMS) had not detected the discrepancies that were identified in the notice of suspension. MAC's practice of not carrying out the Engine Run-up checklist on the first flight of the day when carrying passengers was also unidentified by the SMS. Consequently, these practices persisted. Because these practices had been ongoing, they would have been considered normal company practice and, therefore, a reflection of what management considered acceptable behaviour (in other words, the company's safety culture).
Organizations respond to operational pressures because these priorities are clearly measurable and provide immediate feedback. Under these pressures, concerns related to safety may become less prominent, and organizations may unwittingly introduce risk into their operations.
Even though MAC had a small number of employees, the company voluntarily implemented an SMS and demonstrated that it was capable of using the elements of that system. However, the SMS elements were primarily used as a reactive method to address potential safety concerns.
The traditional approach to safety management has been shown to be ineffective in identifying potential hazards and associated risks. Organizations that comply with the minimum standards and manage safety using the traditional approach are not well situated to identify emerging safety problems. In today's aviation environment, modern safety management practices must be embedded within an organization's management system, so that the management of safety is integrated into day-to-day operations. If organizations do not use modern safety management practices, then there is an increased risk that hazards will not be identified and risks will not be mitigated.
Even though the majority of the regulatory reasons for suspension identified in the notice of suspension were directly related to the actions of the operations manager and the person responsible for maintenance, others within the management group exceeded flight and duty times; they should all have been aware of the applicable provisions of the Canadian Aviation Regulations.
MAC's SMS training consisted of only 12 minutes of training per year. Given that management commitment has the largest influence on a company's safety culture, a positive safety culture requires management to foster an environment whereby safety is integrated into day-to-day operations.
If an organization's safety culture does not fully promote the goals of an SMS, then it is unlikely that it will be effective in reducing risk.
2.7 Passenger seat shoulder harness
The use of shoulder harnesses is known to reduce the severity of upper-body and head injuries. The risk of serious injury or death is increased for light-aircraft occupants who are not wearing upper-torso restraints or shoulder harnesses. If passenger seats installed in light aircraft are not equipped with shoulder harnesses, then there is an increased risk of passenger injury or death in the event of an accident.
3.0 Findings
3.1 Findings as to causes and contributing factors
- Neither pilot had considered that landing on a short runway at an unfamiliar aerodrome with known high terrain nearby and joining the circuit directly on a left base were hazards that may create additional risks, all of which would increase the crew's workload.
- The presence of the tower resulted in the pilot not flying focusing his attention on monitoring the aircraft's location, rather than on monitoring the flight or the actions of the pilot flying.
- The crew's increased workload, together with the unexpected distraction of the presence of the tower, led to a reduced situational awareness that caused them to omit the Landing Checks checklist.
- At no time during the final descent was the engine power increased above about 400 foot-pounds of torque.
- Using only pitch to control the rate of descent prevented the pilot flying from precisely controlling the approach, which would have ensured that the flare occurred at the right point and at the right speed.
- Neither pilot recognized that the steep rate of descent was indicative of an unstable approach.
- Advancing the propellers to full would have increased the drag and further increased the rate of descent, exacerbating the already unstable approach.
- The aircraft crossed the runway threshold with insufficient energy to arrest the rate of descent in the landing flare, resulting in a hard landing that caused the right main landing gear to collapse.
3.2 Findings as to risk
- If data recordings are not available to an investigation, then the identification and communication of safety deficiencies to advance transportation safety may be precluded.
- If organizations do not use modern safety management practices, then there is an increased risk that hazards will not be identified and risks will not be mitigated.
- If passenger seats installed in light aircraft are not equipped with shoulder harnesses, then there is an increased risk of passenger injury or death in the event of an accident.
- If the experience and proficiency of pilots are not factored into crew selection, then there is a risk of suboptimal crew pairing, resulting in a reduction of safety margins.
- If pilots do not carry out checklists in accordance with the company's and manufacturer's instructions, then there is a risk that a critical item may be missed, which could jeopardize the safety of the flight.
- If crew resource management is not used and continuously fostered, then there is a risk that pilots will be unprepared to avoid or mitigate crew errors encountered during flight.
- If organizations do not have a clearly defined go-around policy, then there is a risk that flight crews will continue an unstable approach, increasing the risk of an approach-and-landing accident.
- If pilots are not prepared to conduct a go-around on every approach, then there is a risk that they may not respond to situations that require a go-around.
- If operators do not have a stable approach policy, then there is a risk that an unstable approach will be continued to a landing, increasing the risk of an approach-and-landing accident.
- If an organization's safety culture does not fully promote the goals of a safety management system, then it is unlikely that it will be effective in reducing risk.
3.3 Other findings
- There were insufficient forward impact forces to automatically activate the emergency locator transmitter.
4.0 Safety action
4.1 Safety action taken
4.1.1 Maritime Air Charter Limited
4.1.1.1 Corrective action regarding captain
On 02 September 2015, a Maritime Air Charter Limited (MAC) training pilot completed 2 hours of in-flight training on the Beechcraft King Air B200 with the captain of the occurrence flight. On the same date, the captain successfully passed a pilot proficiency check with a Transport Canada–approved check pilot. On 29 October 2015, MAC limited the captain to acting as pilot-in-command only under direct supervision of another MAC captain who is certified on type.
4.1.1.2 Aircraft pre-flight run-ups
During a MAC flight operations meeting held on 24 September 2015, all company pilots were informed that they must conduct a pre-flight run-up in accordance with the manufacturer's instructions and the approved aircraft checklist.
4.1.1.3 Pre-flight Risk Assessment checklist
On 19 August 2015, MAC introduced a new Pre-flight Risk Assessment checklist that must be completed prior to departure for all flights conducted by the company's pilots, with the exception of training flights, flight tests, and test flights. The checklist is intended to provide a quantifiable assessment of operational hazards prior to acceptance of a flight by the captain.
4.1.1.4 Accelerate-stop distance
On 18 September 2015, MAC issued a memo restricting the Beechcraft King Air A100 and B200 aircraft from operating into or out of aerodromes where the runway length is less than 3000 feet. An accelerate-stop distance must now be calculated prior to departure from all runways that are less than 4000 feet in length. If the calculated accelerate-stop distance is not adequate for the planned runway, then departure is not authorized.
4.1.1.5 Training program
MAC's training program has been revised to include the following elements:
- There is increased emphasis on stabilized approach criteria and controlled flight into terrain avoidance.
- Reduced-thrust takeoffs are now prohibited.
- All new pilots will receive a minimum of 25 hours of line indoctrination training.
- Flight training will be carried out using dedicated training flights.
This report concludes the Transportation Safety Board's investigation into this occurrence. the Board authorized the release of this report on . It was officially released on .