Collision with wires
Canadian Helicopters Limited
Airbus Helicopters AS 350 BA (Helicopter), C-GBPS
Rigolet, Newfoundland and Labrador, 5 nm WSW
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 30 July 2015, the Canadian Helicopters Limited Airbus Helicopters AS 350 BA helicopter (registration C-GBPS, serial number 1277) had been flown to a remote microwave tower site approximately 5 nautical miles west-southwest of Rigolet, Newfoundland and Labrador, with a pilot and 2 passengers on board. At about 1609 Atlantic Daylight Time, the helicopter lifted off from the helipad at the tower site and struck a tower guy wire with the main rotor. The helicopter struck the ground and settled on its upper right side. One passenger sustained fatal injuries, the pilot sustained serious injuries, and the other passenger sustained minor injuries. The helicopter was destroyed. The 406-megahertz emergency locator transmitter did not activate. There was no post-crash fire. The accident occurred during daylight hours.
Factual information
History of the flight
On 30 July 2015, Canadian Helicopters Limited (CHL) operated a charter flight for Bell AliantFootnote 1 using an Airbus Helicopters model AS 350 BA helicopter (AS 350 BA). The objective of the flight was to travel to the Moliak microwave tower site located about 5 nautical miles (nm) west-southwest of Rigolet, Newfoundland and Labrador, to conduct planned site maintenance.
The passengers were a Bell Aliant employee and a contractor. The pilot had flown with these passengers often and they had been working together at other tower sites on the previous 3 days.
The flight departed from CHL's base at the Happy Valley–Goose Bay Airport at 1333Footnote 2 and arrived at the Moliak site about an hour later. The helicopter was landed facing north on the site's raised helipad. The passengers then carried out the site maintenance for about 1.5 hours while the pilot rested in the site radio building. Once the work was completed, the passengers advised the pilot, who began preparing for the return flight. The pilot noted that the wind was light and from the north.
The pilot helped the passengers load their tools and equipment onto the helicopter. Some cargo was placed on the cabin floor behind the left front seat; the left side of the rear split-bench seat had been folded up for this purpose. The pilot was seated in the right front seat, the employee in the left-front seat, and the contractor in the forward-facing passenger seat located behind the pilot, on the outer right side of the helicopter. The pilot began the helicopter start-up procedure, completed the pre-takeoff checks, and confirmed that all doors were latched and that all occupants had their seatbelts fastened.
The pilot visually scanned the area to the left of the helicopter, was interrupted briefly by a non-operational communication made by a passenger, and then continued to scan to the right of the helicopter to ensure that the area was clear for takeoff. The pilot did not note the outer guy wires and did not include them in his departure plan. At about 1609, the pilot lifted off and began intentionally moving forward.
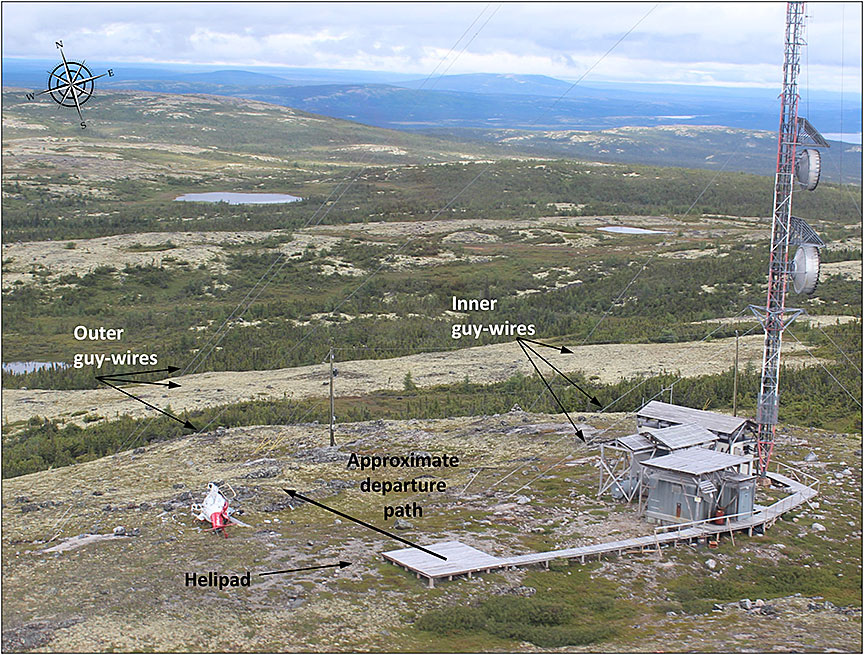
The helicopter was just clear of the helipad and about 2 metres above downward-sloping terrain, when the contractor touched the pilot's left shoulder. The pilot's attention was drawn left and he then saw the tower guy wires in front and to the left of the helicopter. As the pilot moved the cyclic control aft and to the right to avoid the wires, the helicopter's main rotor struck a guy wire. The helicopter rolled rapidly to the right, struck the ground and settled on its upper right side directly below the outer guy wires (Photo 1).
The forward cabin roof, windscreen and right-hand cabin door were destroyed. The pilot and employee exited through the front of the helicopter after releasing their seatbelts. The contractor's seatbelt was found fastened, and the contractor was fatally injured.
The pilot selected the helicopter master electrical switch off, then depressed the emergency button on the satellite flight following cockpit interface panel.
The employee proceeded to the nearby site radio building and used the telephone to call for help. The employee then assisted the injured pilot to the building, administered first aid, and waited until help arrived by helicopter about 1.5 hours later.
The pilot and employee were flown to the Rigolet Community Clinic where they received medical care.
Injuries to persons
| Crew | Passengers | Others | Total | |
|---|---|---|---|---|
| Fatal | – | 1 | – | 1 |
| Serious | 1 | – | – | 1 |
| Minor/None | – | 1 | – | 1 |
| Total | 1 | 2 | – | 3 |
Damage to aircraft
The helicopter was destroyed.
Other damage
Approximately 240 litres of Jet A-1 fuel was spilled and absorbed into the ground around the helicopter.Footnote 3
The main guy wire, the lowest of the 3 outer guy wires located west of the microwave tower, was damaged by one of the main rotor blades.
Personnel information
The pilot held a commercial helicopter license restricted to visual flight rules (VFR) and was certified and qualified for the flight in accordance with existing regulations. The investigation concluded the pilot's performance was not degraded by physiological factors.
| Pilot license | Commercial Pilot License – Helicopter |
|---|---|
| Medical expiry date | 01 January 2016 |
| Total flying hours | 2617.7 |
| Flight hours on type | 1473.5 |
| Flight hours in the last 30 days | 21.3 |
| Flight hours in the last 90 days | 71 |
| Flight hours on type in the last 90 days | 71 |
| Hours on duty prior to occurrence | 3 |
| Hours off duty prior to work period | 18 |
The pilot had worked at CHL since 2005 and often flew to microwave tower sites, including the Moliak site. The pilot was familiar with its layout. The last time the pilot had flown to the Moliak site was 18 December 2014.
Aircraft information
The AS 350 BA is a single-engine, single-pilot, turbine-powered helicopter that has a single main rotor with 3 blades made of composite material. The helicopter has 6 seats and a maximum gross take-off weight of 4630 pounds. The helicopter is equipped with 3 cargo compartments: left and right side compartments and a smaller rear compartment behind the left compartment.Footnote 4 The occurrence helicopter also had an external cargo basket mounted on the left skid.
The pilot compartment had 2 seats, each equipped with a 4-point restraint system using an adjustable lap belt and dual shoulder belts which extended from seat-mounted inertia reels and individually attach to the single lap belt attachment point.
The rear seat was a forward-facing split-bench utility seat configuration with seating for 4 passengers. Either or both seat halves of the split-bench rear seat can be unfastened from floor mounts and folded up to provide additional floor space for cargo, if needed. When the split-bench is folded up, a cargo net can be fastened to the floor to retain any cargo carried in the cabin.
Each rear seat position was equipped with a 3-point restraint system using an adjustable lap belt with an attached single-strap shoulder belt which extended from a rear-mounted inertia reel. For the outer-right seat, the shoulder belt extends over the seated occupant's left shoulder to the lap belt attach point.
Records indicate that the helicopter was certified, equipped, and maintained in accordance with existing regulations and approved procedures, and that there were no known deficiencies before the occurrence flight.
The helicopter's weight and center of gravity were within the prescribed limits.
Emergency locator transmitter
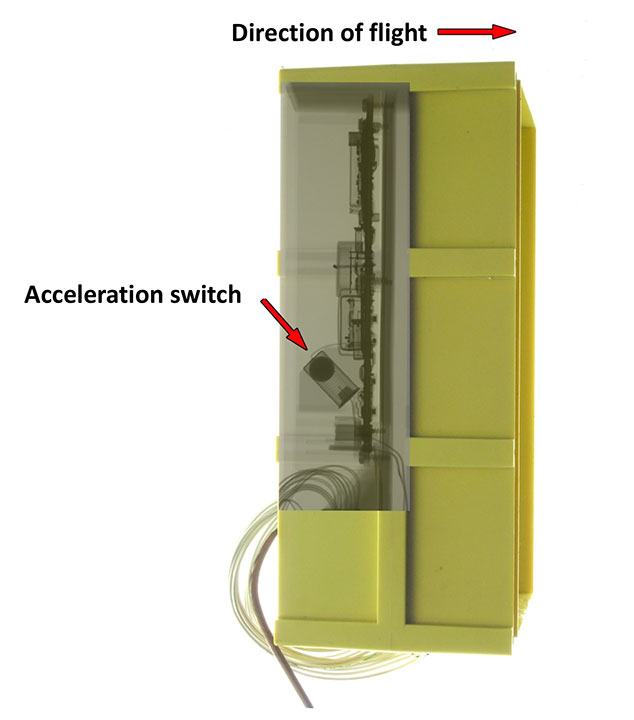
The helicopter was equipped with a Kannad 406-megahertz (MHz) automatic fixed helicopter (AF-H) emergency locator transmitter (ELT) that can be activated either automatically or manually. Automatic activation occurs when impact forces activate its internal acceleration switch. Manual activation occurs either by selecting the remote switch on the cockpit instrument panel or the switch on the ELT itself to the ON position. When activated, the ELT transmits a distress signal to the COSPAS-SARSAT search and rescue satellite system.
When installed in a helicopter, the ELT's acceleration switch axis of detection is angled 45° down in relation to the longitudinal axis of the helicopter in the direction of forward flight (Figure 1).
Satellite tracking system
The occurrence helicopter was equipped with a SkyTrac ISAT-100 system (SkyTrac system). The SkyTrac system provides real-time flight following as well as text messaging, voice, and data communication using satellite and global positioning system (GPS). The SkyTrac system records the time and GPS position for engine start-up, takeoff, landing, and engine shutdown. To record a takeoff, the SkyTrac system requires the collective lever to be raised, and the helicopter to indicate a speed of 5 knots for a minimum of 4 seconds.
SkyTrac programs the system configurations based on an operator's subscription request. In the configuration used by CHL, the SkyTrac system was programmed to transmit the GPS position of the helicopter every 2 minutes after takeoff, and send an overdue notification if 15 position reports had been missed. Operators can subscribe to have the SkyTrac system configured so that it transmits the GPS position reports more frequently.
Meteorological information
At the time of the accident, the weather at the tower site was noted as having good visibility with a few clouds and light northerly winds. The weather was suitable for VFR flight and was not considered a factor in the occurrence.
Aids to navigation
Not applicable.
Communications
Not applicable.
Moliak microwave communications tower site
The Moliak microwave communications tower site is operated by Bell Aliant and is constructed at the top of a hill at an elevation of 365 metres. The tower height is 67.1 metres above ground and is supported on 3 sides (120° azimuth spacing) by steel cable guy wires, arranged in inner and outer groups of wires. The inner group of 3 wires are anchored about 25 metres from the tower, and the outer group of 3 wires are anchored about 55 metres from the tower (Figure 2).
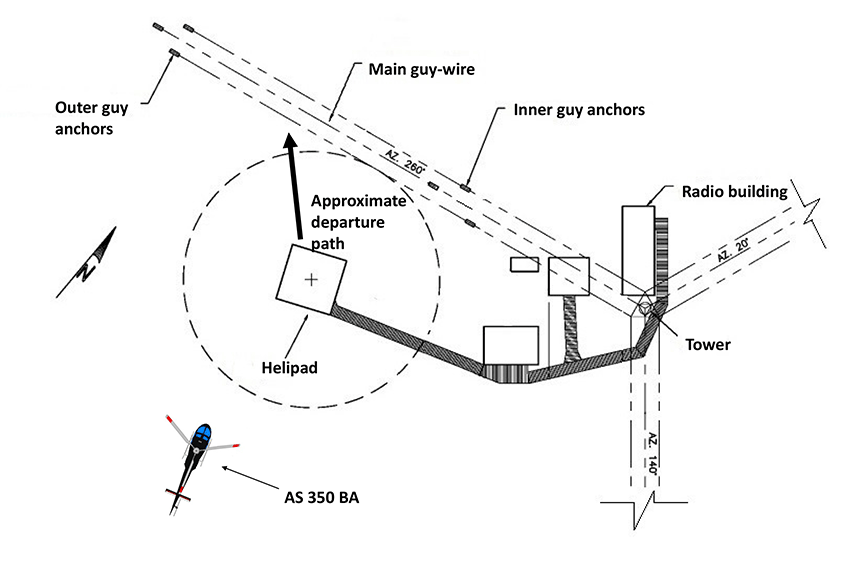
The 3 small buildings at the site contain communications and power generation equipment and are connected by raised walkways covered with wooden decking. One such walkway extends about 35 metres west of the tower to the helipad, which is a raised square wooden deck about 0.5 metre above ground level and about 6 metres square. The centre of the helipad is about 14 metres away from the closest guy wire.
It is normal practice in a helicopter, as it is in any aircraft, to land and take off into the wind. To stay well clear of any obstructions, all company pilots flying to the Moliak microwave tower site approach and depart from the south or southwest. The pilot did not follow this normal departure practice on the occurrence flight.
Moliak is the only Bell Aliant site with the helipad located within the circumference of the outer guy wire anchor points.
The investigation determined that all of the guy wires were visible from an AS 350 helicopter when parked facing north on the helipad, but did not have high-visibility markings.
Flight recorders
The aircraft was not equipped with a flight data recorder or a cockpit voice recorder, nor was either required by regulation. Numerous Transportation Safety Board of Canada (TSB) aviation investigation reports have referred to investigators being unable to determine the reasons an accident occurred due to the absence of on-board recording devices.Footnote 5
If cockpit or data recordings are not available to an investigation, then the identification and communication of safety deficiencies to advance transportation safety may be precluded.
Wreckage and impact information
The helicopter's main rotor hub assembly and blades were destroyed from high-energy impact damage. The forward cabin roof, windscreen and nose section were destroyed from main rotor blade impact. The right cabin door was destroyed, the tail boom was fractured, and the upper aft cabin structure, engine and its cowling received substantial damage from ground contact (Photo 2).

All the cargo compartment doors were closed and the external cargo basket door remained latched. Loose cargo items that had been placed on the floor behind the left rear seat of the helicopter were found on the ground to the right of wreckage and included personal items, tool boxes, and loose tools.
Emergency locator transmitter
Subsequent to the accident, a successful manual activation check was carried out with the ELT installed in the occurrence helicopter. The ELT was removed and sent to the TSB Laboratory, where it passed the signal transmission and activation testing requirements for the unit.
The helicopter struck the ground on its right side. The ELT did not automatically activate due to insufficient impact forces along the acceleration switch axis of detection.
The CHL Flight Operations Manual (FOM) states, “After a crash or forced landing the ELT function switch should be placed to the ‘ON' position as soon as possible after the crash.”
The remote switch on the cockpit instrument panel was noted to be in the ARMED position, and the switch on the ELT was noted to be in the ARM position. A manual activation of the ELT was not carried out after the collision.
Satellite tracking system
On the occurrence flight, the SkyTrac system recorded only the engine start-up time and GPS position. The SkyTrac system did not send an overdue notification following the collision, because the requirements to record a takeoff were not met.
When the helicopter's master electrical switch is on, an emergency notification can be sent by depressing the emergency button on the satellite flight following cockpit interface panel.
After the accident, the pilot selected the helicopter master electrical switch off, then depressed the emergency button on the satellite flight following cockpit interface panel.
In this occurrence, an emergency notification was not sent by the SkyTrac system because it was not powered by the helicopter electrical system when the emergency button on the satellite flight following cockpit interface panel was depressed.
The CHL FOM does not require the SkyTrac system emergency notification feature to be activated after a crash or forced landing.
Medical and pathological information
A post-mortem medical examination was conducted on the contractor.Footnote 6 The examination concluded that the contractor sustained fatal injuries when his upper body was crushed under the helicopter.
The employee's minor injuries included cuts and bruises, mostly to the hands and head.
The pilot sustained minor injuries including cuts and bruises to the head, and more serious injuries including a broken foot due to a puncture wound, and a crush injury to the hand.
Fire
There was no post-crash fire.
Survival aspects
Flight helmet
The pilot was not wearing a flight helmet. The effects of non–fatal head injuries can range from momentary confusion and inability to concentrate, to full loss of consciousness.Footnote 7
Although the Canadian Aviation Regulations (CARs) do not require helicopter pilots to wear a helmet, the TSB has documented a number of cases where wearing a helmet would likely have reduced or prevented injuries. On 30 October 2009, the TSB issued Aviation Safety Advisory A09A0016-D2-A1, Low Usage of Head Protection by Helicopter Pilots, emphasizing that, without ongoing and clear communication promoting the benefits of using head protection, helicopter pilots will continue to operate without a helmet, increasing the risk of head injury and consequent inability to provide necessary assistance to crew or passengers.
CHL strongly encourages their pilots to wear flight helmets, but does not require that they are worn unless the client mandates it. CHL reimburses 50 percent of the helmet purchase cost to their pilots.
Passenger restraints during accidents
In 2014, the greatest numbers of Canadian-registered helicopter accidents were associated with landing (35%), takeoff (26%), and en-route (21%) phases of flight, followed by manoeuvering (18%) and standing/taxiing (12%) phases.Footnote 8
Accidents that occur with low forward speed, such as during hover, takeoff or landing, can result in the helicopter rolling over and substantial side impact forces being generated in the accident sequence. Additionally, because helicopters are top-heavy by design this contributes to their tendency to roll over following an impact or hard landing.
An inertia reel's locking mechanism is designed to activate in a forward impact, when a sudden acceleration force is applied to shoulder belts. This prevents forward movement of the occupant in the event of a sudden, forward impact. Side impact forces may not activate the inertia reel locking mechanism.
Both the pilot and the employee used the full 4-point restraint system and remained restrained in their seats throughout the accident sequence. First responders found the contractor's 3-point restraint system fastened and his upper body outside of the right cabin door. Following the accident, it was found that the contractor's shoulder belt was misrouted under his left arm.
3-point restraints
In vehicle impact studies, a far-side impact is one where the occupant is seated on the side away from the struck side. Far-side impact studies consider that the single-strap shoulder belt of a 3-point restraint is anchored opposite and passes over the shoulder on the occupant's side that is away from the struck side.
A side impact force coming from the side opposite the shoulder that the belt passes over can cause the upper body to slip out of the shoulder belt. As a result, the occupant can experience excessive head velocities and excessive lap belt loads, Footnote 9, Footnote 10
Safety briefing
CARs 703.39(1) states:
The pilot-in-command shall ensure that passengers are given a safety briefing in accordance with the Commercial Air Service Standards [CASS].
The CASS requires a safety briefing to be carried out prior to takeoff. It also states that, if no additional passengers embark on subsequent flights on the same day, it may be omitted for these subsequent flights.Footnote 11
CHL requires that all passengers receive the standard safety briefing as an oral briefing from a crew member, or by audio or audio-visual means. The CHL FOM describes the items that must be covered with the passengers prior to embarking, prior to takeoff, after takeoff (if not covered in the pre-takeoff briefing), in flight (because of turbulence), and prior to disembarking of passengers.
The standard safety briefing must be performed before every flight. However, the pre-takeoff and post-takeoff briefings may be omitted for subsequent takeoffs on the same day when no additional passengers have boarded the flight, and only when a crew member has verified that all carry-on baggage is properly stowed, safety belts or harnesses are properly fastened, and seat backs and chair tables are properly secured.
The standard safety briefing included items such as the use, location, operation and deployment, as applicable, of emergency equipment such as life rafts, life preservers, ELT, survival equipment and first-aid kit. It also includes the location of emergency exits, exit location signs, and how the exit operates.
The passengers were experienced in helicopter operations and had received the CHL standard safety briefing many times. When the passengers and the pilot flew together, their practice was to occasionally review the information in the standard safety briefing.
The standard safety briefing was not conducted on the day of the occurrence.
Cargo restraint
CARs 602.86(1) prohibits the operation of an aircraft unless carry-on baggage, equipment and cargo are:
(a) stowed in a bin, compartment, rack or other location that is certified in accordance with the aircraft type certificate in respect of the stowage of carry-on baggage, equipment or cargo; or
(b) restrained so as to prevent them from shifting during movement of the aircraft on the surface and during take-off, landing and in-flight turbulence.
During the post-accident examination, it was noted that the cargo net was stowed under the right side of the rear split bench.
Tests and research
TSB laboratory reports
The TSB completed the following laboratory report in support of this investigation:
- LP185/2015 – ELT Examination
Organizational and management information
Canadian Helicopters Limited
General
CHL is the largest helicopter operator in Canada. The company operates 184 helicopters from 26 bases across Canada, including 4 from the Happy Valley–Goose Bay base.
For over 30 years CHL had been contracted to provide helicopter transportation services to the Bell Aliant microwave tower sites in Labrador. This occurrence was the first wire strike for CHL at a microwave tower site.
CHL has a safety management system (SMS). The SMS is not required by regulation and its effectiveness has not been verified by Transport Canada. All employees are given initial training on SMS and recurrent training every 36 months.
Flight operations risk assessment
The company Health, Safety and Environment (HSE) manual describes risk assessment procedures and covers work site risk assessment as a company practice. CHL had completed general risk assessments for various flight operation types, including external load operations and VFR operations.Footnote 12 No specific risk assessments had been completed for flight operations into any of the microwave tower sites.
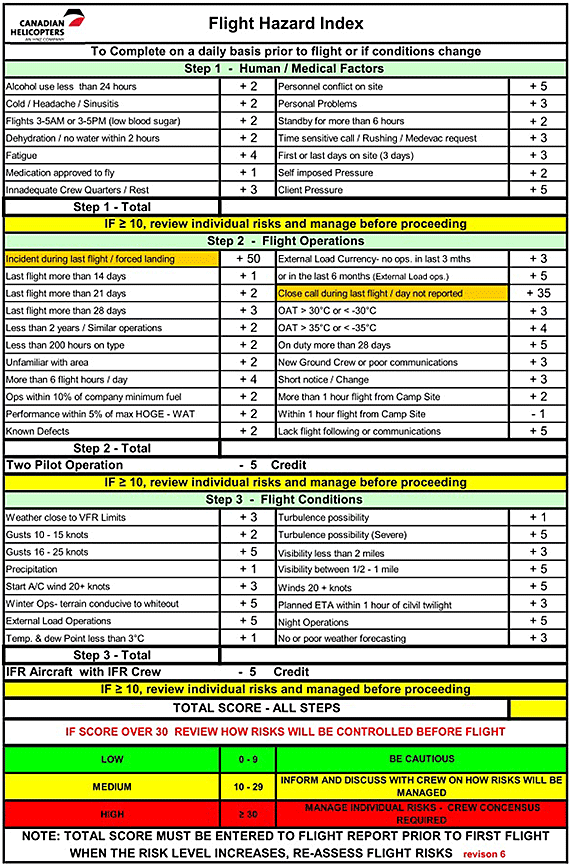
Flight Hazard Index
CHL uses a Flight Hazard Index card,Footnote 13 which considers a series of human factors and flight operation conditions, to assess the level of risk associated with a particular flight (see Appendix A). Completion of the Flight Hazard Index card is mandatory for multi-crew operations and is recommended as a situational awareness enhancement tool for VFR single-pilot operations. CHL's typical practice is to use the Flight Hazard Index card on all flights.
Prior to departure, a risk score is assigned to each factor and condition, and total risk score is calculated for the particular flight. Risk scores above predetermined values require mitigation before proceeding with the flight. The total risk score is recorded following completion of the flight.
The use of the Flight Hazard Index card is covered during pilot indoctrination and annual recurrent training.Footnote 14
The pilot calculated the risk score prior to the occurrence flight and assessed the total risk score to be low. Since the occurrence flight was not completed, the risk score was not recorded. The investigation assessed the level of risk using the Flight Hazard Index card; the total risk score was low.
The company Flight Hazard Index card does not include a flight operations condition for landing site hazards.
Bell Aliant Labrador sites
Bell Aliant operates 27 microwave tower sites in Labrador, all of which are accessed by helicopter.
The helipad locations were collaboratively selected with CHL and Bell Aliant management personnel over 20 years ago, and at that time no formal risk assessments were conducted. Landing site diagrams were not available to the crew at the time of the occurrence.
None of the tower guy wires were equipped with high visibility markings.
Additional information
Visual scan
Human vision is both peripheral and foveal. The foveal vision is in the centre, is relatively small, and provides for perception of details. Central fixation is critical to perceive objects such as static wires. To be effective, a full visual scan requires several displacements in sequence across the visual field, fixating a number of times, to perceive the presence of hazards. However, over time the visual scan can become routine and automatic, leading to a lower level of attention and consequently degraded situational awareness. The interruption of a visual scan can also negatively affect situational awareness.Footnote 15 On the occurrence flight, the pilot did not restart the visual scan from the beginning after the interruption.
Situational awareness
Situational awareness is defined as “the perception of elements in the environment within a volume of time and space, the comprehension of their meaning, and the projection of their status in the near future.”Footnote 16 Following this definition, maintaining situational awareness is a result of 3 individual processes on the part of the pilot. First, the pilot must perceive information from the environment. Second, the relevance of this information on the ability to achieve operational goals must be established. Finally, the pilot must use this information to project future states and events. In this way, three levels of situation awareness are maintained which allows the pilot to “plan ahead and prepare for contingencies”Footnote 17 which leads to more effective decision making. All 3 levels involve information-processing stages where shortcomings may occur and which may result in incomplete or inadequate situational assessments.
Single-pilot resource management
According to the Federal Aviation Administration (FAA), “many CRM [crew resource management] principles have been successfully applied to single-pilot aircraft and led to the development of single-pilot resource management (SRM).”Footnote 18 SRM consists of managing all the resources available to a pilot to ensure a successful flight by enabling the pilot to accurately assess hazards, manage resulting potential risks, and make good decisions. A passenger in a cockpit seat, even with no flying experience, may be one of the most underused resources. When appropriate, the pilot can ask passengers to assist with certain tasks, such as watching for potential hazards.
Another resource is verbal communication as it reinforces an activity. A verbal operational briefing, which can happen whether or not passengers are aboard, can help the pilot with the decision-making process and situational awareness. Briefing passengers is of great value in giving them a better understanding of a situation and gives them an opportunity to contribute to the safety of a flight.
CHL did not have a formal single-pilot resource management training program, nor is such training required by regulation. CHL did not have a policy or procedure regarding verbalizing operational briefings or engaging the passengers to assist with certain tasks.
Sterile cockpit
A sterile cockpit policy is intended to avoid non-operational communications in order to minimize disruption to pilots' operational attentiveness and reduce non-essential engagement of limited attentional resources.Footnote 19
Non-operational communications can include both conversations and activities. Pilots do not necessarily recognize at the time the impact of such communications on their performance. Even though the CARs do not require the implementation of a sterile cockpit, various air operators have included this concept in their daily operations, standard operating procedures or company operations manuals.
The CHL FOM requires a sterile cockpit to be maintained for all takeoff, landing and low level operations. It stipulates that only conversation essential to the safety of the flight may be conducted. The importance of the sterile cockpit is reiterated in the standard safety briefing which includes instructions to eliminate all non-essential conversation during start-up, takeoff, landing, shut-down, and low-level flight operations.
While the CHL FOM specifically states that non-essential conversations are to be avoided during critical phases of flight, it does not specifically state that non-essential activities are to be avoided.
Useful or effective investigation techniques
Not applicable.
Analysis
There was no indication of mechanical or system failure during the occurrence flight, and fatigue, incapacitation or physiological factors did not affect the pilot's performance. The analysis will therefore focus on the operational factors that resulted in the inadvertent flight of the helicopter into the guy wires.
Collision with wires
The pilot flew to microwave tower sites regularly and was accustomed to the presence of guy wires at these sites. The pilot had previously flown to the Moliak site and was aware of the proximity of the guy wires to the helipad. On the occurrence flight, the pilot did not note the outer guy wires and did not include them in the departure plan. The pilot performed a visual scan before departure; however, the visual scan was not effective in perceiving the outer guy wires. The pilot's scan had been interrupted, which may have compromised the scan.
To be situationally aware, a pilot has to be aware of what is happening around them in order to understand how information, events, and the pilot's own actions will impact their goals and objectives in the future—in this case, to achieve a successful takeoff. Both the routine scan and the interruption while performing the visual scan would reduce the level of the pilot's attention, thereby contributing to degraded situational awareness. The pilot's lower level of attention while conducting a routine flight led to an ineffective visual scan resulting in degraded situational awareness.
Company pilots depart the Moliak site to the south or southwest to remain clear of obstructions. However, on the occurrence flight, the pilot did not follow this practice and was not aware of the obstructions until being alerted by the contractor. It is also possible the pilot reverted to the normal practice of taking off directly into the wind. The helicopter struck the guy wires before evasive action could be taken, which caused the helicopter to roll rapidly and impact the ground.
Emergency locator transmitter
The emergency locator transmitter did not automatically activate, and no manual activation was initiated. Therefore, no distress signal was transmitted to the COSPAS-SARSAT search and rescue satellite system.
Although rescue operations were successfully initiated by means of a telephone call in this occurrence, if the emergency locator transmitter signal is not transmitted in a timely manner, then rescue operations could be delayed, increasing the risk that survivability could be compromised.
Flight helmet
The pilot was not wearing a flight helmet and sustained minor head injuries.
Despite the recognized benefits of head protection, there are no regulations for helicopter pilots to wear helmets. If helicopter pilots do not wear flight helmets, then they are at a greater risk of incurring head injuries in a crash and may be unable to evacuate or help evacuate the aircraft, thereby placing the safety of passengers and crew at risk.
Passenger restraint
Helicopter accidents often occur with low forward speed, which can result in substantial side impact forces being generated in the accident sequence. In a side impact where the occupant's upper body is unrestrained, they can experience excessive head velocities and excessive lap belt loads. The unsupported upper body can contact other occupants or the surrounding aircraft interior, or can be forced out of the aircraft.
The contractor may have deliberately or unwittingly misrouted the shoulder belt portion of the restraint under his arm. The helicopter's low forward speed and rapid roll and impact to the right would result in a side impact force coming from the side opposite of the shoulder that the belt passed over. Therefore it is possible that, during the accident sequence, the contractor's upper body slipped out of the shoulder belt which resulted in the shoulder belt becoming misrouted under his left arm. The investigation could not determine which condition resulted in the misrouting of the shoulder belt.
Because the right-hand cabin door was no longer in position, there was no restriction to the sideways movement of the contractor's upper body. The contractor's shoulder belt was found to be misrouted under his left arm, which allowed his upper body to move outside of the cabin in the accident sequence and contributed to his fatal injuries.
If a helicopter is equipped with 3-point restraint systems, then an occupant's upper body may slip out of the shoulder belt during an accident that involves side impact forces, increasing the risk of injury or death.
Safety briefing
The pilot did not provide the standard safety briefing to the passengers before takeoff, possibly because they frequently flew with the operator, had received the briefing on numerous occasions and had flown with this pilot in the 3 days before the accident.
The standard safety briefing provides passengers with information relating to the use and location of safety equipment, and what to do in the event of an emergency. If passengers are not given a full safety briefing, then there is an increased risk that they may not use the available safety equipment or be able to perform necessary emergency functions in a timely manner to avoid injury or death.
Cargo restraints
Post-accident examination revealed that the cargo net was not used, and loose cargo was found outside of the wreckage.
If carry-on baggage, equipment or cargo is not restrained, then occupants are at a greater risk of injury or death if these items become projectiles in a crash.
Single-pilot resource management
By using single-pilot resource management (SRM) principles, pilots will be better prepared to accurately assess hazards and manage the resulting potential risks. Even in a single-pilot environment, verbalizing briefings can assist the pilot in the decision-making process and make passengers aware of the pilot's intentions. Passengers with no flying experience can even assist a pilot by watching for potential hazards.
CHL did not provide any formal SRM training, nor did it have a policy or procedure regarding verbalizing operational briefings, or engaging the passengers to assist with certain tasks.
If pilots are not trained in or do not use SRM principles, such as verbalizing operational briefings, then hazards may go unnoticed and safety of flight could be jeopardized.
Sterile cockpit
During the pre-takeoff visual scan, the pilot was interrupted by a non-operational communication. This type of activity can be a distraction and can affect a pilot's operational attentiveness during a critical phase of flight.
If company procedures do not specify activities to be avoided when maintaining a sterile cockpit, then there is a risk that occupants may inadvertently distract the pilot during critical phases of flight.
If occupants engage in non-essential communication while a sterile cockpit is required, then there is an increased risk of pilot distraction that may cause unintentional errors.
Findings
Findings as to causes and contributing factors
- The pilot did not note the outer guy wires and did not include them in the departure plan.
- The pilot performed a visual scan before departure; however, the visual scan was not effective in perceiving the outer guy wires.
- The pilot's scan had been interrupted, which may have compromised the scan.
- The helicopter struck the guy wires before evasive action could be taken, which caused the helicopter to roll rapidly and impact the ground.
- The contractor's shoulder belt was found to be misrouted under his left arm, which allowed his upper body to move outside of the cabin in the accident sequence and contributed to his fatal injuries.
Findings as to risk
- If the emergency locator transmitter signal is not transmitted in a timely manner, then rescue operations could be delayed, increasing the risk that survivability could be compromised.
- If cockpit or data recordings are not available to an investigation, then the identification and communication of safety deficiencies to advance transportation safety may be precluded.
- If helicopter pilots do not wear flight helmets, then they are at a greater risk of incurring head injuries in a crash and may be unable to evacuate or help evacuate the aircraft, thereby placing the safety of passengers and crew at risk.
- If a helicopter is equipped with 3-point restraint systems, then an occupant's upper body may slip out of the shoulder belt during an accident that involves side impact forces, increasing the risk of injury or death.
- If passengers are not given a full safety briefing, then there is an increased risk that they may not use the available safety equipment or be able to perform necessary emergency functions in a timely manner to avoid injury or death.
- If carry-on baggage, equipment or cargo is not restrained, then occupants are at a greater risk of injury or death if these items become projectiles in a crash.
- If pilots are not trained in or do not use single-pilot resource management principles, such as verbalizing operational briefings, then hazards may go unnoticed and safety of flight could be jeopardized.
- If company procedures do not specify activities to be avoided when maintaining a sterile cockpit, then there is a risk that occupants may inadvertently distract the pilot during critical phases of flight.
- If occupants engage in non-essential communication while a sterile cockpit is required, then there is an increased risk of pilot distraction that may cause unintentional errors.
Other findings
- The emergency locator transmitter did not automatically activate due to insufficient impact forces along its acceleration switch's axis of detection.
- The emergency locator transmitter was not manually activated after the collision.
- The SkyTrac system did not send an overdue notification following the collision, because the requirements to record a takeoff were not met.
- An emergency notification was not sent by the SkyTrac system because it was not powered by the helicopter electrical system when the emergency button on the satellite flight following cockpit interface panel was depressed.
- The company Flight Hazard Index card does not include a flight operations condition for landing site hazards.
Safety action
Safety action taken
Canadian Helicopters Limited
- Canadian Helicopters Limited (CHL) has adopted the policy of conducting an overhead inspection flight prior to landing at any Bell Aliant site. Bell Aliant employees are involved in the decision-making process and in the briefing for the approach and departure, and are asked to be vigilant during those phases of flight.
- Wire strike avoidance training has been developed at CHL and will be presented by training pilots during annual recurrent training.
- CHL has adopted new local operating procedures with detailed overview “plates” that have been designed for each site. They show obstacle avoidance routing for microwave tower sites, tower height, magnetic north, helipads and identify guy wires.
Bell Aliant
- Following this occurrence, the helipad at Moliak was moved outside of the circumference of the outer guy wire anchor points.
- Bell Aliant collaborated with CHL to conduct reviews of all Labrador tower sites to identify hazards. The resulting mitigation includes activities such as removing old wind turbines and high brush, and installing high-visibility guy wire marking at all sites.
- A process has been undertaken to contract an independent organization to conduct risk assessments at all Bell Canada sites accessed by aircraft (sites that would not have an airport used for landing), and to audit all aviation service providers used by Bell Canada.
This report concludes the Transportation Safety Board's investigation into this occurrence. the Board authorized the release of this report on . It was officially released on .
Appendices
Appendix A – CHL Flight Hazard Index card