Loss of directional control and collision with terrain
6442927 CANADA INC. (operating as Héli-Nord)
Bell Helicopter 206B, C-GYBK
Sept-Îles, Quebec, 20 nm N
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 02 September 2015, the Bell 206B helicopter (registration C-GYBK, serial number 1884) operated by Héli-Nord was flying from the airport of Sept-Îles, Quebec, with 1 pilot and 4 passengers on board. The purpose of the flight was to inspect a salmon pass approximately 20 nautical miles north of Sept-Îles. During the final approach, a few feet from the ground, the helicopter began an uncommanded rotation to the right and, after turning a few times, crashed heavily into a rock on its front right side. The accident occurred at about 0940, Eastern Daylight Time. The male passenger occupying the front left seat and the female passenger occupying the rear central seat sustained fatal injuries. The pilot and the other 2 passengers, who occupied the left and right rear seats, sustained serious injuries. The 406-MHz emergency locator transmitter activated on impact. A fire started in the engine tailpipe but was immediately extinguished by persons on site.
Factual information
History of the flight
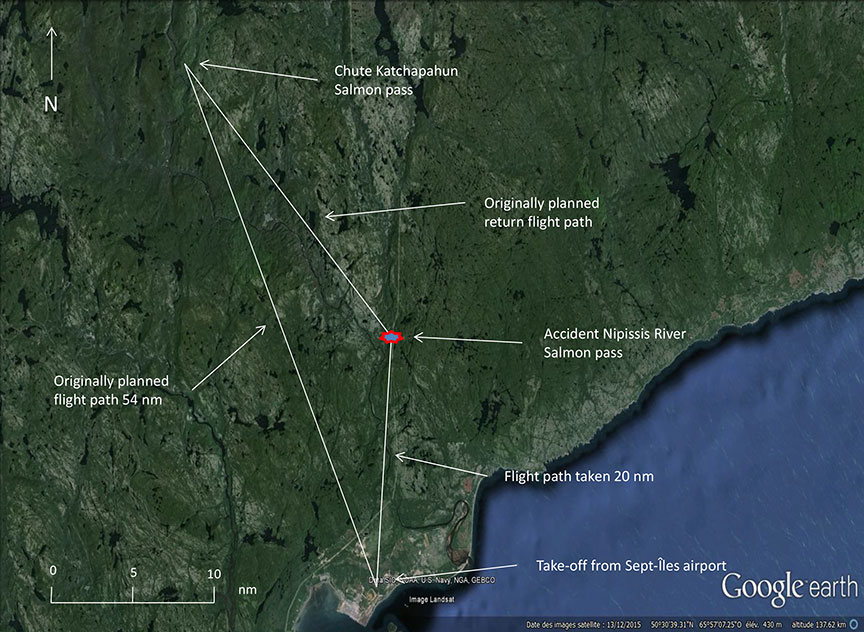
On the morning of the flight, the pilot had agreed to meet the chief pilot at the Héli-Nord facilities at the Sept-Îles, Quebec, airport (CYZV). The flight was scheduled for around 0830,Footnote 1 and the pilot arrived at around 0745. The contract specified that 6 passengers were to travel to 2 salmon passes on the Moisie and Nipissis rivers, which required the use of 2 helicopters. Each helicopter was to carry 3 passengers. The 2 aircraft were to go first to a salmon pass at Chute Katchapahun, Quebec, 54 nautical miles (nm) north of Sept-Îles, and on the return journey land at a second salmon pass on the Nipissis River, 20 nm north of Sept-Îles (Figure 1).
The pilot and chief pilot discussed the flights and the 2 places to which they were to fly. Since this was the first time that the pilot had flown C-GYBK, the chief pilot explained the equipment differences to him, although they presented no particular operational difficulty.
With the agreement of the group, a passenger, who had to return to her work at the Nipissis River camp, was added, and boarded C-GYBK. The flight itinerary was altered, and it was agreed to go first to the Nipissis River camp to drop her off.
It was agreed that the chief pilot would take off first and that C-GYBK would take off 10 minutes later. The chief pilot was to position himself at the landing site in order to guide C-GYBK in its approach and landing. The weather conditions were favourable for a visual flight rules flight. The METARFootnote 2 for CYZV, located 20 nm south of the occurrence site, issued at 1000, some 20 minutes after the accident, indicated visibility of 30 miles, scattered clouds at 11 000 feet above ground level, and a southerly wind of 7 knots.
A weight and balance sheet was completed by the pilot a few minutes before the flight, using the passengers' actual weights. This put the helicopter at 3171.8 pounds, 28.2 pounds below the maximum allowable internal load of 3200 pounds. Based on normal fuel consumption of 25 US gallons per hour, which represents 175 pounds per hour,Footnote 3 it was calculated that fuel used during the flight reduced the weight of the aircraft at the time of the occurrence by 87 pounds to 3084 pounds, 116 pounds below the maximum allowable internal load.
The aircraft flown by the chief pilot was loaded to capacity, and the chief pilot had decided to land closer to the camp in order to clear the landing site for C-GYBK. The approach and touchdown of the first aircraft were normal. The wind was low and created no difficulty for control during touchdown. Immediately after touchdown, the 3 passengers disembarked, and the chief pilot took up a position to guide C-GYBK.
The takeoff and the flight of C-GYBK to the site were without incident, and all aircraft parameters were normal. During the final turn leading to the landing site, the pilot saw the chief pilot, who was standing on a rock. The pilot could see the other aircraft parked. The pilot positioned the aircraft to face the place indicated, and during the final approach, noted that engine torque was at 110%Footnote 4 and that the nose of the aircraft was turning to the right. The pilot then lowered the collective to reduce the torque while applying full left anti-torque pedal to counteract the yaw. However, the nose of the aircraft continued turning to the right and the helicopter kept losing altitude. The pilot again increased the torque by raising the collective to reduce the rate of descent. He pushed the cyclic to initiate a recovery and gain speed, but the yaw increased very quickly. Realizing that he had lost control of the aircraft, the pilot cut engine power to reduce the rate of yaw and prepare for the impact. The aircraft was in a nose-down attitude to the right before it crashed violently into the rock. According to available information, an alarmFootnote 5 sounded in the aircraft shortly before the accident. However, it was not possible to determine which alarm sounded.
Persons on site were able to render assistance to the injured, and informed emergency services using a satellite phone. First, a helicopter with a physician on board arrived at the site and gave first aid to the injured. A second helicopter with 2 paramedics on board arrived a little later, took charge of the injured, and transported them to the Sept-Îles hospital centre.
Damage to aircraft
The helicopter collided with the rock nose down and rotating to the right. The engine did not stop immediately, and a minor fire broke out in the tailpipe but was immediately extinguished by persons on site. On impact, the tailboom detached and came to rest behind the aircraft (Figure 2). Severe damage to the skin on the rear of the right-hand side and the rear stabilizer was noted. Damage to the skids confirmed impact on the right side, with the nose of the aircraft pointing toward the ground. All damage resulted from the impact with the rock. The floor of the aircraft was severed at the rear of the cabin, causing the fuel tank to split.

Since the aircraft made a few turns to the right before crashing, the TSB laboratory conducted a more thorough examination of the tail rotor system in November 2015, in the presence of representatives of Bell Helicopter and Rolls-Royce. No pre-existing damage was found. The investigators were able to determine that the anti-torque pedal control tubes that govern the movement of the tail rotor blades severed sequentially upon impact. One of the control tube breaks was at the full left pedal position, confirming that the left anti-torque pedal was fully applied at the time of impact with the ground.
Aircraft
The helicopter was operated under Subpart 702 (Aerial work operations) of the Canadian Aviation Regulations (CARs) at the time of the occurrence. A review of the helicopter's maintenance records indicated that the helicopter was maintained in accordance with the existing regulations at the time of the occurrence. There were no reported or outstanding defects.
The helicopter was not equipped with a flight data recorder or a cockpit voice recorder, nor was it required to be by regulation. It was fitted with a global positioning system (GPS) (a Garmin GPSMAP 296 device), which was found and sent to the TSB laboratory to attempt recovery of volatile memory. No data of use to the investigation was recorded.
Survivability
The helicopter was fitted with shoulder harnesses in the front and lap belts in the rear. At the time of the visit to the accident site, the pilot's harness had been unbuckled, and the harness of the front passenger had been cut by the rescuers. The investigators noted that the lap belt of the female rear passenger was still fastened fully extended. It was not possible to determine why it was in this position. Nevertheless, the autopsy report states that this passenger died as the result of severe abdominal injuries. It is possible that these fatal injuries were caused by an incorrectly fitted lap belt at the time of impact. The TSB laboratory report also confirms there were no anomalies in the lap belts. The left front passenger died as the result of multiple injuries to the head and trunk. The pilot's injuries were less serious, probably because he was wearing a helmet, which protected him during the impact.
Landing site
The site chosen for the landing presented challenges for an inexperienced pilot. The location was a large rock, with terrain ascending from the river, and there were mountains on either side of the river. In addition, this was the first time that the pilot had been there. The approach was over the Nipissis River, flanked by tall trees on either side, and a mountain covered with mature trees, a camp, the camp employees and the 3 passengers of the helicopter that had touched down a few minutes before were in front of the aircraft. The chief pilot had taken a position on the rock in front of the aircraft, as agreed. Figure 3 shows a photograph taken a few seconds before the accident, during the final approach.

Flight crew
Records show that the pilot held the necessary licences and qualifications for the flight, in accordance with existing regulations. The pilot held a valid commercial pilot licence – helicopter, endorsed for the BH06 helicopter.Footnote 6 At the time of the occurrence, the pilot held a Category 1 civil aviation medical certificate with no restrictions, valid until 01 April 2016.
In June 2011, the pilot completed a 3-year theoretical and practical aeronautical training course at the Centre québécois de formation aéronautique (CQFA) in St-Honoré, Quebec. During the second year of training, the pilot obtained a private pilot licence – aeroplane, on a single-engine aeroplane, accumulating 78 flight hours. During his third year, he chose helicopter flight. He received theoretical and practical training on the Bell 206B, recording 135 flight hours on type.
The pilot started work with Héli-Nord in May 2015. He received ground training, which included a component on awareness of vortex ring state and loss of tail rotor effectiveness (LTE).Footnote 7 LTE is discussed later in this report. The pilot had received 4.1 hours of flight training. He also successfully completed a company-administered pilot proficiency check for the Bell 206B on 05 July 2015. At the time of the accident, the pilot had accumulated 263 hours of flight time, broken down as follows:
- 78 hours on Sundowner, single-engine aeroplane at the C.Q.F.A.
- 135 hours on Bell 206B at the C.Q.F.A.
- 35 hours on Astar 350
- 15 hours on Bell 206B at Héli-Nord
The pilot had a second job, unrelated to the aeronautical field. On the day before the accident, he left work at 2200, and had not worked the previous day.
Bell 206B characteristics
The first version of the Bell 206B entered the industry as the Bell 206B Jet Ranger II. The aircraft was equipped with an Allison 250-C20 engine that produced 400 SHP,Footnote 8 and a 62-inch tail rotor, like that of C-GYBK.
In 1977, the Bell 206B Jet Ranger III model came onto the market. It had a more powerful Allison 250-C20B engine that produced 420 SHP, but the size of the tail rotor was still 62 inches. Later, the manufacturer produced the Bell 206B3 Jet Ranger III, fitted with an Allison 250‑C20J engine, which had a 65-inch tail rotor for greater effectiveness.
A modification can be made to install a longer, and thus more effective, tail rotor. This requires the installation of a more powerful engine. However, C-GYBK was fitted with a 62-inch tail rotor, whereas several helicopters of the same model have a 65-inch tail rotor, similar to those of the C.Q.F.A. It should be noted that the pilot was trained on aircraft that had 65-inch tail rotors, which are less sensitive to loss of rotor effectiveness.
Loss of directional control
During this occurrence, the aircraft experienced a loss of directional control near the ground, without any mechanical failure. Two conditions can cause a loss of directional control:
- The loss of tail rotor effectiveness (LTE)
- An increase of engine torque beyond limits.
Loss of tail rotor effectiveness
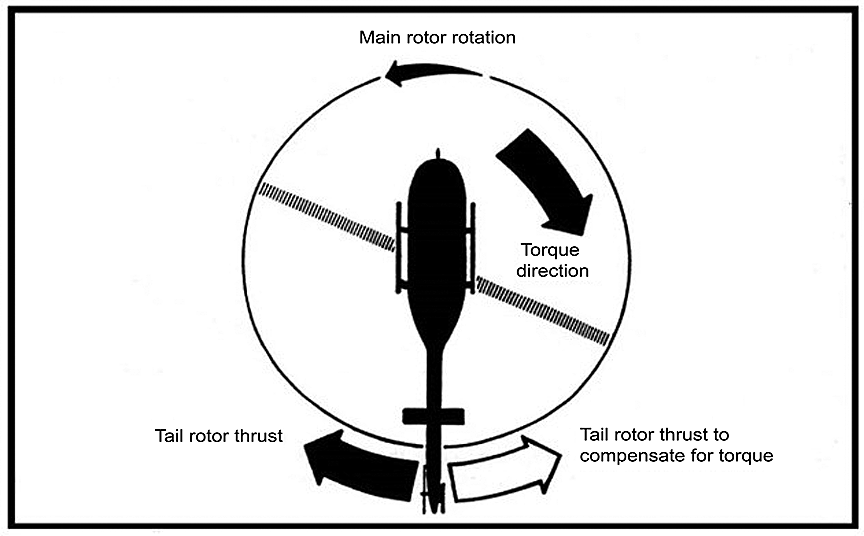
Seen from above, the blades of the main rotor turn counterclockwise (Figure 4). As a result of this rotation, the helicopter experiences a torque reaction in the opposite direction, which results in the helicopter yawing to the right. To neutralize this movement, the helicopter is equipped with a tail rotor. The main rotor produces torque, and the pilot must neutralize the induced yaw by using the anti-torque pedal to increase or reduce tail rotor thrust as needed.
LTE is an uncommanded yaw that does not subside by itself; if not corrected, it can result in loss of control of the helicopter.Footnote 10 LTE is unrelated to equipment failure or defective maintenance, and any single-rotor helicopter flying at low speeds can experience this phenomenon. It is the result of the tail rotor not providing sufficient thrust to maintain directional control. In general, tail rotor thrust that is insufficient for a given power setting can lead to an LTE.
In addition, 4 relative wind azimuth regions can produce an environment that is conducive to an LTE:
- main rotor disc vortex wind (winds from 285° to 315° relative to the helicopter);
- weathercock stability (winds from 120° to 240°);
- tail rotor vortex ring (winds from 210° to 330°); or
- loss of translational lift (winds from all directions).
In this occurrence, although the winds were light, they were blowing from the right with a slight tailwind component. The aircraft was therefore susceptible to the relative wind, which was within the critical wind azimuth region of weathercock stability where yaw could be induced.
Increase of engine torque beyond limits
Available information indicates that the pilot noted that engine torque was at 110%; however, the exact moment at which this was done or for how long is not known. It is also not known whether the torque could have exceeded 110% without the pilot noticing it. When the collective is raised beyond the limit of 110%, the pitch of the main rotor blades increases and the engine must produce sufficient power to compensate for the very large and rapid increase of main rotor drag. As a result, there is a decrease of main rotor rpm, which affects the tail rotor proportionally. According to the aircraft manufacturer, the tail rotor can compensate for the loss of directional control up to the limit of 110% of engine torque for a maximum of 5 seconds. Beyond this limit, the tail rotor's ability to supply the required thrust is exceeded with a resulting loss of directional control similar to an LTE.
Insufficient tail rotor thrust, which can be identified by a yaw to the right, can be countered in 2 ways:
- Apply full left anti-torque pedal and move the cyclic control stick forward; and
- If altitude is sufficient, reduce power.
Safety information
Bell Helicopter issued Information Letter 206-84-41 in 1984, identifying low-altitude flight characteristics that can lead to an uncommanded yaw.
United States Federal Aviation Administration (FAA) Advisory Circular 90-95 discusses the phenomenon of unanticipated yaw and recommends recovery techniques. The circular describes conditions in which LTE may occur, notably during "[a]ny maneuver which requires the pilot to operate in a high-power, low-airspeed environment with a left crosswind or tailwind," especially in right turns.
In an issue of Aviation Safety Vortex,Footnote 11 Transport Canada (TC) discussed the unanticipated right yaw phenomenon and the recommended recovery technique. TC's Study and Reference Guide: Private and Commercial Pilot Licence (Helicopter) identifies LTE as a ground school topic to be discussed as part of aircraft performance.
Training on loss of tail rotor effectiveness
Given the high risk of accidents and of loss of control of an aircraft in flight, training on the LTE phenomenon is given exclusively at the theoretical level. The investigation showed that when an aircraft experiences a partial loss of tail rotor effectiveness during a flight, the pilot may be able to instinctively correct the effect. The important point is not to get to the point of no return, that is, the point at which correction is no longer possible.
The theoretical training that the pilot had received at Héli-Nord addressed LTEs, and the chief pilot had also covered the subject in flight training, explaining the phenomenon, yet without being able to practise it. The only flight training concerning the tail rotor consists in simulating loss of connection between the transmission and the tail rotor; the instructor induces movement to one side or the other using the anti-torque pedal and the student must correct the situation by using the opposite pedal and touching down. This practice requires an ability to control the aircraft on the part of the pilot, but is easier to control than an LTE. It should be noted that practice is conducted in ideal conditions in order to minimize the hazards associated with this manoeuvre.
TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP 212/2015 – Récupération de la mémoire volatile – GPS [Volatile memory recovery – GPS]
- LP 221/2015 – Examen de l'épave [Examination of wreckage]
Analysis
Examination of the wreckage and the data collected during the investigation indicate that there were no pre-existing mechanical issues that could have resulted in the loss of control and collision with the rock. The pilot was qualified and held the appropriate licences for this flight, and nothing indicates that physiological factors, including fatigue, were involved in this accident. The analysis will focus on the pilot's experience and training, and on the loss of directional control during the approach for the landing.
The accident occurred following a loss of directional control during final approach. Lack of flight data recordings, in particular on the rate of descent and the engine torque actually selected during the approach, 2 scenarios that could lead to a loss of directional control were examined.
According to the manufacturer, several in-flight tests have shown that the LTE phenomenon can occur if the wind conditions are favourable and are within one of the 4 relative wind azimuth regions and if engine torque is kept within the prescribed limits, that is 100% or up to 110% for a maximum of 5 seconds. Beyond this limit, the tail rotor's ability to supply the required thrust is exceeded and with a resulting loss of directional control similar to an LTE.
The LTE phenomenon has been well known in the industry for several years, and is taught theoretically during pilot training. Investigating bodies, regulatory bodies and manufacturers have informed pilots about this phenomenon repeatedly. Nevertheless, accidents caused by LTEs still occur today and unfortunately, as in this occurrence, cause serious and fatal injuries.
A successful response to LTE calls for specific skills and good coordination of flight controls so that the appropriate manoeuvre to avoid getting into an LTE situation can be executed in a timely manner, or the recovery manoeuvre can be executed should an LTE occur. Although the pilot had received theoretical training on LTE, he was not able to maintain control of the aircraft when he found himself in this situation. Although the helicopter involved was the same model as that used in his training at the Centre québécois de formation aéronautique (CQFA), there was nonetheless a significant difference in terms of tail rotor performance and available engine power. The pilot was therefore ill-prepared for this eventuality during a critical phase of flight:
- He had little experience.
- He had not flown the Bell 206B regularly since his training had ended in 2011.
- This was the first time he had landed at this site.
The investigation found that the aircraft was being operated nearly at its maximum allowable weight. The photo taken a few seconds before the accident shows that the wind was light and was blowing from the right with a tailwind component.
It is possible that the pilot's attention was focused mainly on the unknown landing site environment and the guidance provided by the chief pilot on the ground, with the result that he noticed belatedly that the engine torque was at 110%. However, due to the lack of flight data recordings, it could not be determined whether the 5-second limit or the 110% limit were exceeded.
An increase in power beyond this limit, the low approach speed and the fact that the aircraft was close to its maximum allowable weight are elements that may have led to the loss of directional control similar to an LTE. As a result, the helicopter was placed in a flight regime that was conducive either to an LTE or to the exceedance of the tail rotor's ability to supply the required power, which led to a loss of directional control at an altitude that precluded recovery: therefore, the aircraft collided with the terrain.
Given the environment, this site presented challenges for a pilot with little experience: the rock was sloping, which required vigilance on landing, and the mountains on either side of the river afforded little space to carry out the procedure to recover tail rotor effectiveness, that is, applying full left pedal, moving the cyclic control stick forward and, if altitude is sufficient, reducing power.
The pilot needed to adjust his rate of descent and the engine power to allow him to touch down in the correct place. To do so, he needed to descend until he attained ground effect close to the rock, and arrest his descent just before touching down. Ground effect would have enabled him to better control the aircraft.
The pilot had been trained at the C.Q.F.A. on a Bell 206B Jet Ranger III helicopter fitted with a longer tail rotor (65 inches) and a more powerful engine, which was therefore more effective and less susceptible to LTE. The pilot's lack of experience on a Bell 206B helicopter with a 62-inch tail rotor prevented him from recognizing the LTE and counteracting it in a timely manner.
The fact that the pilot was wearing a helmet significantly reduced the severity of his head injuries. However, the investigation found that the female rear passenger's lap belt was still fastened and fully extended. The autopsy report states that the female passenger died as a result of severe abdominal injuries, possibly caused at the time of impact by an incorrectly adjusted lap belt. If occupants do not wear safety belts correctly during a flight, there is an increased risk of serious injuries or death in the event of an accident.
Findings
Findings as to causes and contributing factors
- The helicopter was operating in a flight regime that was conducive to either a loss of tail rotor effectiveness or to the exceedance of the tail rotor's ability to supply the required power, which led to a loss of directional control at an altitude that precluded any recovery. Therefore, the aircraft collided with the terrain.
- No in-flight training on loss of tail rotor effectiveness is provided on account of the risks this would entail. Consequently, the pilot was not familiar with the very precise skills required to control the aircraft when such a loss of effectiveness occurred close to the ground.
- The pilot's lack of experience on a Bell 206B helicopter with a 62-inch tail rotor prevented him from recognizing the loss of tail rotor effectiveness and counteracting it in a timely manner.
- The female passenger sustained fatal abdominal injuries, possibly due to the fact that her lap belt was not fitted correctly.
Findings as to risk
- If occupants do not wear safety belts correctly during a flight, there is an increased risk of serious injuries or death in the event of an accident.
Other findings
- The fact that the pilot was wearing a helmet significantly reduced the severity of his head injuries.
This report concludes the Transportation Safety Board's investigation into this occurrence. the Board authorized the release of this report on . It was officially released on .