Loss of control during rejected takeoff
Privately registered, Cessna 140, C-GOFK
Stave Lake abandoned aerodrome
British Columbia
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
History of the flight
On 27 July 2020, a privately registered Cessna 140 aircraft (registration C-GOFK, serial number 11313) was flying from Ross Creek Aerodrome (CRC3), British Columbia (BC), to Pitt Meadows Airport (CYPK), BC, with an intermediate stop at Vernon Airport (CYVK), BC. The pilot-in-command (PIC) was the owner of the aircraft and was accompanied by another pilot. The pilots were taking turns performing the role of pilot flying.
At 1042,Footnote 1 the aircraft departed CRC3 for CYVK, where the pilots had planned to take a lunch break. They landed in CYVK at 1127, had lunch, and fuelled the aircraft to its maximum capacity. The pilots departed CYVK at 1259. Approximately 10 minutes into the flight, the pilots detected an abnormal vibration in the aircraft, noting that the engine appeared to be running rough. They diverted to Kelowna Airport (CYLW), BC, which was approximately 7 nautical miles (NM) to the southeast, where the aircraft landed uneventfully at 1315. After closing the flight plan, the pilots conducted an engine run-up and observed an abnormal drop in engine rpm while operating on the right-hand magneto. They shut down the aircraft and, after consulting with an aircraft maintenance engineer by phone, they restarted it. The pilots repeated the engine run-up procedure 3 times with normal results. They departed CYLW at 1333 for the flight to CYPK.
En route to CYPK, the pilots made an impromptu stop at a gravel airstrip on a golf course located 5.9 NM north of the Chilliwack Airport (CYCW), BC. The aircraft arrived at approximately 1524, and departed again at 1639.
When the pilots were approaching Mission, BC, they decided to make a second impromptu stop at an abandoned aerodrome with a gravel airstrip at the north end of Stave Lake, BC. The aircraft landed on the airstrip at 1704, with the pilot in the left seat performing the landing and the PIC in the right seat.

Following a brief time on the ground, the aircraft was restarted and taxied to the northern end of the runway where the pilots performed another engine run-up with normal results. The aircraft flaps were set to 10° and the take-off roll was commenced at 1717, with the PIC flying from the right seat.
The aircraft did not become airborne. When the aircraft was approximately 200 feet from the end of the runway and at approximately 40 mph, the takeoff was rejected. While braking, the aircraft rapidly nosed over and came to rest inverted on the runway. The pilot in the left seat sustained minor injuries and the PIC, who was the pilot flying, was fatally injured. The aircraft sustained substantial damage (Figure 1). There was no post-impact fire.
Aerodrome information
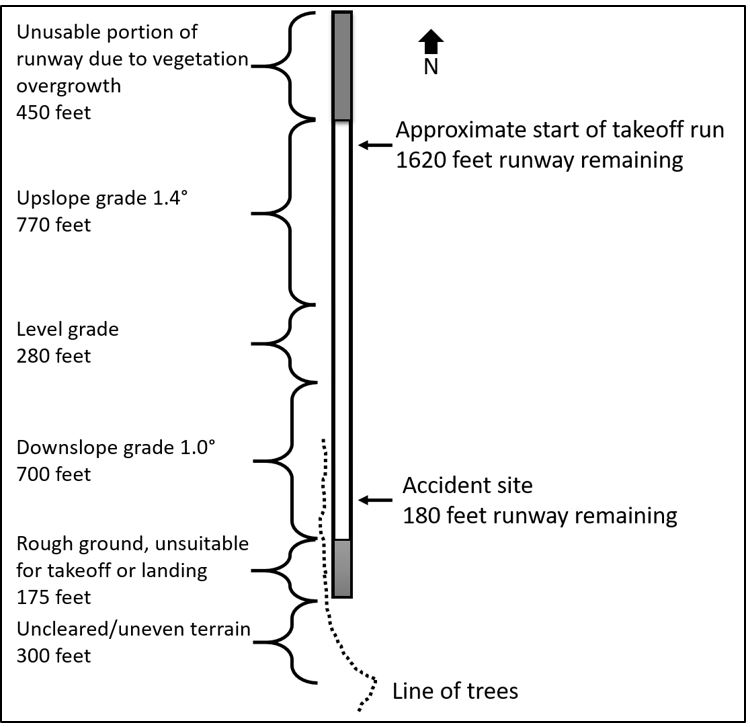
The Stave Lake abandoned aerodrome is located 20 NM north of Mission, at an elevation of 350 feet above sea level (ASL). The gravel airstrip is approximately 2375 feet long and 50 feet wide, with a usable length of approximately 1750 feet oriented in a north-south direction (Figure 2). The first 450 feet of the northern end of the runway cannot be used because of vegetation overgrowth, and the last 175 feet of the southern end of the runway is rough ground. There is a line of trees approximately 80 feet high located 300 feet beyond the southern end of the runway. For aircraft departing southbound, the runway slopes up at 1.4° for 770 feet, remains level for 280 feet, and then slopes down at 1.0° for 700 feet.
On the day of the accident, there were numerous areas of grass covering more than half of the runway’s width, with much of the grass taller than 8 inches. The remaining width, approximately 20 feet of the eastern side of the runway, was rough loose gravel.
Pilot information
The PIC held a private pilot licence with a valid Category 3 medical certificate and had accumulated approximately 1200 total flight hours. The accompanying pilot held both a private pilot and a glider pilot licence with a valid Category 1 medical certificate and had accumulated approximately 400 flight hours.
The PIC had been to the Stave Lake abandoned aerodrome at least 4 times in the 2 months preceding the occurrence, including 3 times with the accompanying pilot. Both of them had conducted a successful takeoff and landing on the airstrip 29 days earlier. The investigation determined that it was routine for the PIC to fly this aircraft from the right seat.
Weather information
There is no aviation weather information specific to the accident location. The nearest aviation weather reporting station to the occurrence site is the Abbotsford Airport (CYXX), BC, which is approximately 27 NM south-southwest of Stave Lake. The aerodrome routine meteorological report (METAR) at the time of the occurrence for CYXX was as follows:
- Winds: 220° true (T), varying from 200°T to 260°T, at 8 knots
- Visibility: 30 statute miles
- Clouds: few at 24 000 feet
- Temperature: 32 °C
- Dew point: 16 °C
- Altimeter setting: 29.82 inches of mercury
A helicopter pilot conducting flight training in the vicinity of the Stave Lake abandoned aerodrome recorded an outside air temperature of 32 °C at 1721 on the day of the occurrence. The helicopter landed at the occurrence site at 1742 and noted the surface winds at the aerodrome were calm. The density altitude at the time of the occurrence was calculated by the investigation to be at least 2700 feet ASL.
Aircraft information
The occurrence aircraft was manufactured by the Cessna Aircraft Company in 1946 and was equipped with a Continental C-85-12F engine. At the time of the occurrence, the aircraft had accumulated approximately 4268 total air time hours. The engine had 40.1 hours time since overhaul.
On 23 June 2020, an engine compression check and oil change were completed, and no anomalies were noted.
The aircraft was equipped with a Narco Avionics emergency locator transmitter (ELT), model ELT 10, which transmits on 121.5 MHz. The ELT switch was in the armed position but the unit did not activate during the occurrence likely due to the impact forces being insufficient to trigger the g-switch.
The pilots were carrying a SPOT personal GPS (global positioning system) tracking device on board. Following the accident, the accompanying pilot transmitted a distress message, which was received at 1755.
Aircraft performance
Cellphone videos taken from on board the aircraft recorded the successful takeoff from the Stave Lake abandoned aerodrome 29 days earlier, as well as the rejected takeoff on the day of the occurrence. The TSB Engineering Laboratory separated the audio files from the video files and compared the propeller speeds for both takeoffs. Audio spectral analysis determined the aircraft’s propeller rpm was similar on both takeoffs, and exceeded the minimum rpm required in the full throttle rpm check detailed in the aircraft’s operation manual.Footnote 2
The TSB determined that the aircraft was being operated within its weight and balance and centre of gravity limits.
The aircraft’s operation manualFootnote 3 provides a single performance chart for take-off data, indicating that the take-off distance required with a temperature of 32 °C, with the flaps up, and on a hard-surface, level runway would be approximately 1050 feet. The manual indicates that the shortest take-off roll can be obtained by keeping the aircraft’s tail wheel low, but off the ground. The video of the occurrence indicates that the tail wheel remained on the ground throughout the take-off attempt. This is consistent with ground scars on the runway observed by investigators.
The investigation determined that during the previous successful takeoff from Stave Lake, which took place when the density altitude was approximately 1550 feet ASL, the occurrence aircraft required approximately 1000 feet to become airborne. During that take-off roll, the aircraft’s position on the runway was further to the left (eastern side of the runway), than during the occurrence take-off roll, thus largely remaining on the gravel surface and avoiding the grassy areas.
In the absence of detailed performance data in an aircraft’s operation manual, pilots may also use a number of rule-of-thumb calculations to assist in deriving take-off performance data. For example, From the Ground UpFootnote 4 indicates that on rough, rocky, or short grass (up to 4 inches) runways, aircraft may require an additional 10% of take-off roll. If the grass is taller than 4 inches, the performance penalty can be as much as 30%. Additionally, for every 1° of upslope in the runway, a pilot should add 10% to the take-off roll, and at 2° of upslope, the pilot can expect significant penalties to take-off rolls. The investigation determined that take-off performance or calculations were not discussed between the 2 pilots before takeoff.
The performance criteria for pilots during recreational pilot permit,Footnote 5 private pilot licence,Footnote 6 and commercial pilot licence flight testsFootnote 7 include assessment of the candidate’s proficiency to specify a GO/NO-GO decision point to the examiner before the attempted takeoff. Guidance material suggests:
At 25% of the ground roll to take-off, the airplane should have achieved 50% of its lift-off speed.
At 50% of the ground roll, it should have achieved 70% of its lift-off speed.
At 80% of the ground roll, it should have achieved 90% of its lift-off speed.
Lift-off speed should be reached within the first 75% of the usable runway. If lift-off has not been achieved in this distance, the take-off should be aborted.Footnote 8
Examination of wreckage
The aircraft systems were examined to the degree possible at the accident site and no indication of a malfunction was found.
The engine was removed for further investigation and an engine run was conducted on an engine test stand. All engine parameters were found within the manufacturer specifications, and the engine produced full power. A review of the aircraft’s maintenance records did not reveal any discrepancies that could have contributed to the accident.
The Cessna 140 aircraft’s baggage compartment is directly behind the pilots’ seats and is covered by a small shelf. It is accessed by folding the back of the pilot’s seat forward. The pilots typically placed individual articles of clothing, logbooks, charts and other aeronautical publications on the shelf. In the baggage area of the occurrence aircraft were the pilots’ personal items, a survival kit in a metal box, and a metal step stool. The investigation determined that the total weight of all articles removed from the aircraft was 97 pounds, with the survival kit weighing 10 pounds. The items that had been placed on the raised shelf and in the baggage compartment were not restrained and all entered the cockpit space during the accident sequence.
Lap belt centre bracket
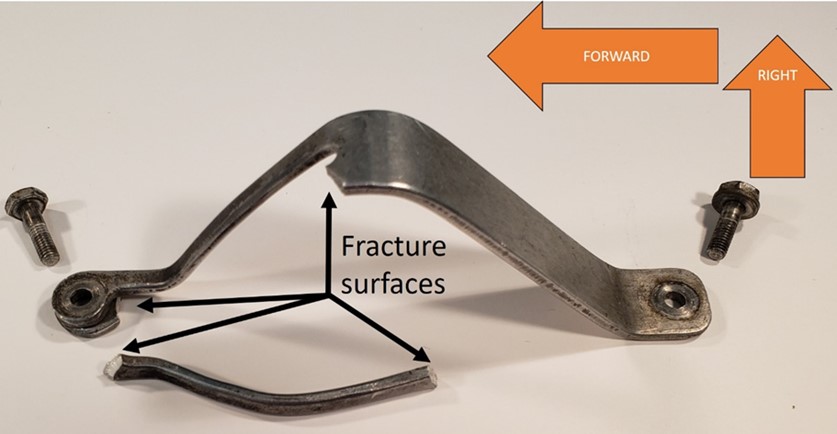
In July 2011, the occurrence aircraft was fitted with a shoulder harness for each cockpit seat in accordance with supplemental type certificate SA1429GL.Footnote 9 The shoulder harnesses attach to the aircraft’s lap belts, which are anchored at 2 locations for each seated position: on the sloped side of the aircraft fuselage, and to a common centre bracket (Figure 3) with individual attachment points for each of the 2 seated positions.

At the time of the occurrence, both occupants were wearing their safety belts.Footnote 10 The lap belt and shoulder harness used by the pilot in the left seat were intact and secure. However, the inboard portion of the lap belt for the pilot in the right seat was found detached from the lap belt’s centre bracket, which was found broken (Figure 4). The broken centre bracket allowed the PIC to become unrestrained during the accident. During the examination of the wreckage, the investigation noted that the lap belt worn by the pilot in the left seat was twisted where it attached to the bracket, indicating that the pilot in the left seat had been using a portion of the lap belt intended for the right seat occupant.
The lap belt centre bracket was removed from the aircraft and sent to the TSB Engineering Laboratory in Ottawa, Ontario. It was determined that the bracket failed due to shearing overstress during the accident. The bracket did not have a part number. However, the TSB’s compositional analysis is consistent with the bracket likely being an original aluminum component manufactured for this type of aircraft.
This lap belt centre bracket was used in both Cessna 120 and 140 aircraft. During the manufacturing life of both aircraft, the Cessna Aircraft Company issued an engineering drawing change notice in which the bracket material was changed from aluminum alloy (Alclad 2024-T3) to steel alloy (SAE 4130), increasing the yield strength of the component by approximately 40%.
Following a 2014 accident of a Cessna 140 aircraft in Parma, New York, United States, the investigation conducted by the National Transportation Safety BoardFootnote 11 found that the aluminum alloy lap belt centre bracket failed due to shearing overstress during the nose-over accident. This resulted in the pilot flying becoming unrestrained during the accident sequence. The pilot’s head contacted the overhead area of the cockpit interior and, as a result, the pilot was fatally injured.
After the 2014 accident, Textron Aviation Inc., which was now the type certificate holder, issued a Single Engine Service Bulletin (SEB-25-03)Footnote 12 on 17 February 2015, affecting Cessna 120 aircraft (serial numbers 8000 through 15075) and Cessna 140 aircraft (serial numbers 8000 through 15075). This required that, at the next 100-hour or 12-month (annual type) inspection, the lap belt centre bracket be inspected to determine if the latest type of lap belt centre bracket (in steel alloy) was installed, and if not, to replace the aluminum centre bracket with the new steel one (part number 0425132). Two months later, on 15 April 2015, the Federal Aviation Administration (FAA) issued a Special Airworthiness Information BulletinFootnote 13 (SAIB CE-15-13) to alert owners, operators, and aircraft maintenance technicians of its airworthiness concern with the aluminum lap belt centre bracket.
A search in the Transport Canada (TC) Canadian Civil Aircraft RegisterFootnote 14 found 175 Cessna 140 and 68 Cessna 120 aircraft registered in Canada at 22 December 2020. Of these, 132 (75%) of the Cessna 140 and 46 (68%) of the Cessna 120 aircraft were manufactured before the change from aluminum to steel alloy became effective.
The owner of the occurrence aircraft had purchased the aircraft in 2016—after SEB-25-03 was issued. However, the investigation was unable to determine if the aircraft owner was aware of the bulletin or of the aluminum bracket installed in the aircraft. Compliance with service bulletins is not required by regulations.Footnote 15
On 09 November 2020, the TSB issued a safety advisory letterFootnote 16 addressed to TC to inform it about the issue and encourage TC to take the necessary steps to reduce the likelihood of the centre bracket failure identified in this occurrence happening again.
As a result, TC engaged in discussions with the FAA, who published an Airworthiness Concern Sheet on 14 December 2020 as a part of their evaluation to determine if additional action was needed. Using the data gathered through the Airworthiness Concern Sheet, TC planned to evaluate the need for mandatory corrective action in consultation with the FAA. TC was also planning to publish a Civil Aviation Safety Alert at the end of January 2021 to bring attention to the concern with aluminum seat belt mounting brackets addressed in SAIB CE-15-13.
Safety messages
In this occurrence, the aircraft was departing from a short runway at an abandoned aerodrome in environmental conditions that would have decreased the performance of the aircraft. This highlights the importance of proactively identifying factors (e.g., runway conditions and density altitude) that can negatively affect aircraft performance, as well as the importance of establishing and committing to appropriate GO/NO-GO points during the takeoff run. Similarly, pilots must exercise additional caution when planning to operate an aircraft from surfaces, or in conditions, not represented in aircraft operation manuals.
Similar to the 2014 accident in the United States, this occurrence shows that without the incorporation of the steel lap belt centre bracket in Cessna 120 and 140 aircraft, failure of the aluminum lap belt centre bracket during accidents may continue, potentially resulting in serious or fatal injuries.
Finally, baggage that is not properly secured may contribute to the severity of injuries sustained by occupants during an accident.
This report concludes the Transportation Safety Board of Canada’s investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .