Loss of control during landing
Privately registered
Daher TBM700 N (TBM 910), C-FFYM
Westlock Aerodrome, Alberta
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 10 October 2021, the privately registered Daher TBM700 N (registration C-FFYM, serial number 1190) was conducting an instrument flight rules flight from Vernon Airport, British Columbia, to Westlock Aerodrome, Alberta, with a stop at Calgary/Springbank Airport, Alberta, to pick up passengers, after which 1 pilot and 3 passengers were on board. At 1102:26 Mountain Daylight Time, while the aircraft was landing on Runway 28 at Westlock Aerodrome, the aircraft bounced and the pilot initiated a go-around. During the application of engine power for the go-around, the aircraft rolled to the left, struck the runway inverted, and came to rest on the runway’s south side.
The 3 passengers exited the aircraft through the main cabin door with the assistance of persons nearby. One passenger received serious injuries, and the other 2 had minor injuries. The pilot, who was seriously injured, was trapped in the cockpit for approximately 2 hours before first responders could safely rescue him from the wreckage. An emergency locator transmitter signal was received by the search and rescue satellite system. The aircraft was significantly damaged and there was no post-impact fire.
1.0 Factual information
1.1 History of the flight
On 10 October 2021, the privately registered Daher TBM700 N (TBM 910) aircraft was conducting an instrument flight rules (IFR) flight from Vernon Airport (CYVK), British Columbia. The planned destination was Edmonton/Villeneuve Airport (CZVL), Alberta, with a brief intermediate stop at Calgary/Springbank Airport (CYBW), Alberta. The pilot and 1 passenger were on board for the first leg of the flight, and 2 additional passengers boarded at CYBW.
During the stopover at CYBW, the aircraft stopped at the end of an uncontrolled taxiway to pick up the 2 passengers. The pilot remained in the cockpit with the engine running and the propeller turning. Given that the aircraft was on an uncontrolled taxiway, there was no ramp safety supervision or marshallers present. There is no regulation precluding loading an aircraft in this manner.
The 2 passengers approached the aircraft and opened the main cabin door. They unloaded a bike before boarding the aircraft, and then they loaded their baggage primarily into the passenger compartment. The baggage was not secured.
The pilot then phoned a family member to report that he and the passengers would be arriving in an hour. One of the 3 passengers was seated in the mid-cabin, rear-facing seat on the right side of the aircraft, and only secured the lap belt. One passenger was seated in the aft cabin forward-facing seat on the left side of the aircraft, beside the main cabin door. This passenger secured both the lap belt and shoulder harness. The third passenger was seated in the aft cabin forward-facing seat on the right side of the aircraft and only secured the lap belt.
The passengers had routinely flown with the pilot on the occurrence aircraft and were familiar with boarding the aircraft, operating and locking the main cabin door, stowing baggage, and fastening safety harnesses.
The aircraft departed CYBW at 1013Footnote 1 on an IFR flight plan and proceeded to CZVL at 16 000 feet above sea level (ASL).
Thirty minutes into this leg of the flight, the pilot requested that the flight-planned destination be amended from CZVL to Westlock Aerodrome (CES4), Alberta, because weather conditions at that location met visual meteorological conditions, which would permit a visual flight rules (VFR) approach. At the time of the occurrence, CES4 did not have any instrument approach procedures.Footnote 2. The Edmonton terminal controller approved the change, and the flight was cleared to proceed visually, direct to CES4.
The aircraft approached CES4 from the south (Figure 1), and at 1059:40, it crossed over the aerodrome mid-field at approximately 1250 feet above ground level (AGL)Footnote 3 and 126 knots indicated airspeed (KIAS), configured with the landing gear extended and the flaps set to the take-off position (10°).Footnote 4 The aircraft then banked right to join the mid-right downwind leg.
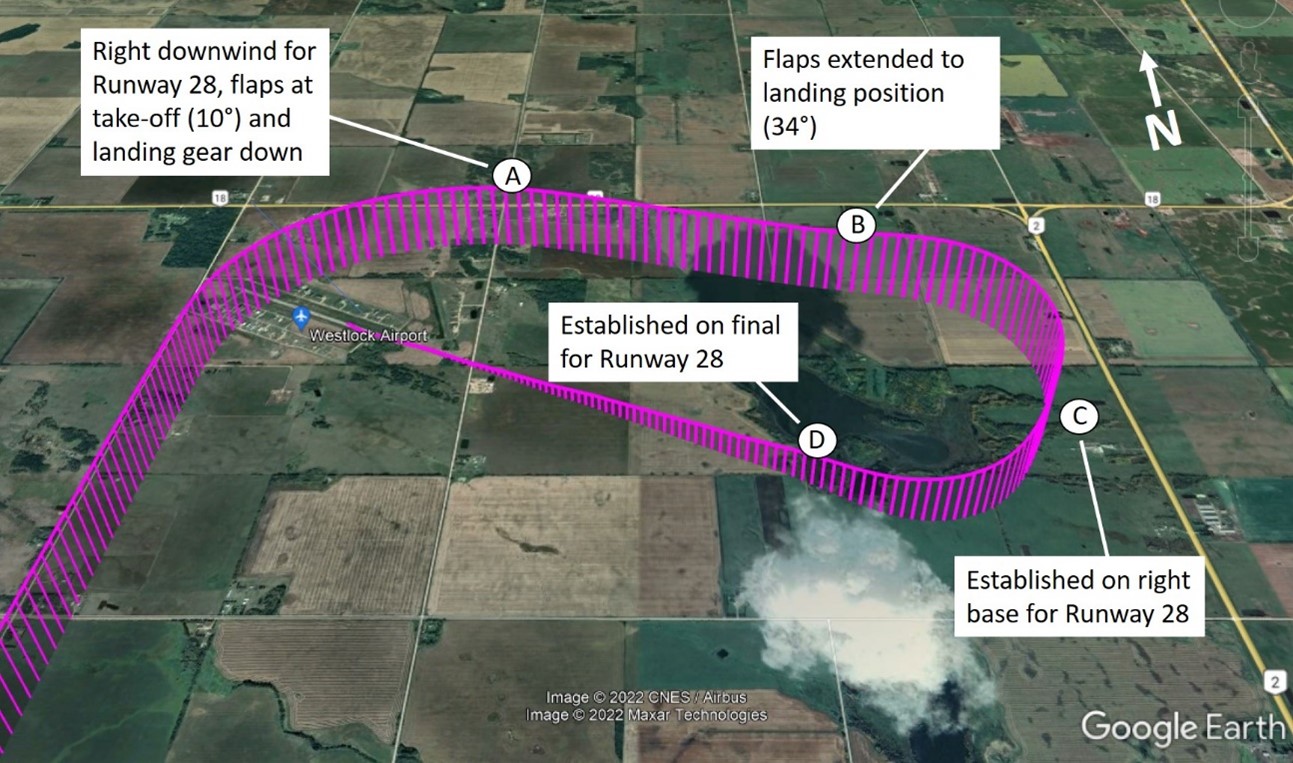
As the aircraft turned right to join the base leg, the flaps were lowered to the landing position (34°,Footnote 5 the full-flap setting), and the aircraft climbed to 1400 feet AGL (Figure 2). On the base leg, the aircraft was travelling at 104 KIAS, with a torque setting of 36%, and a rate of descent of 1200 fpm.
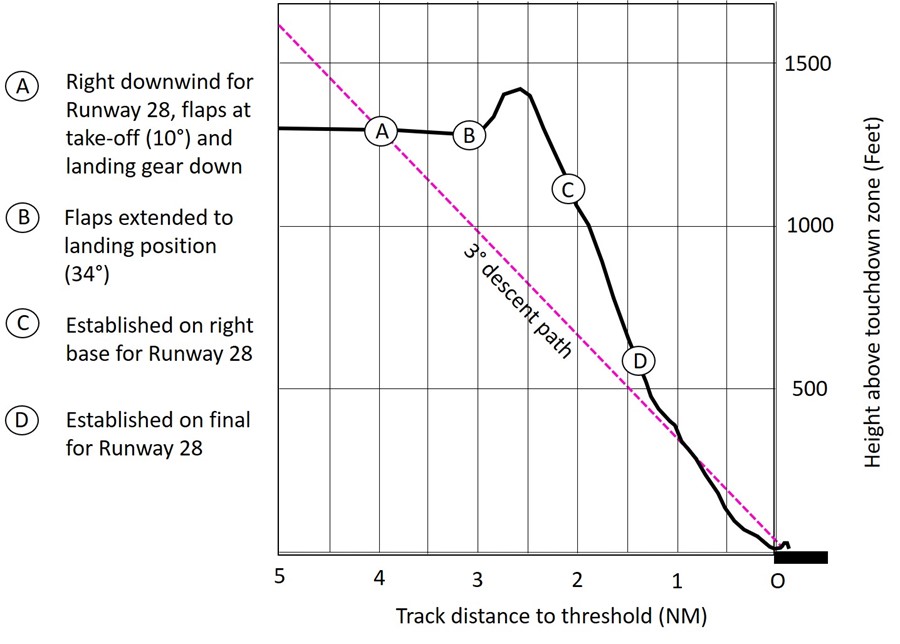
At 1101:20, the pilot rolled out of the right turn and entered the final approach on the extended centreline of Runway 28. The aircraft was 1.4 nautical miles (NM) from the threshold of Runway 28, at a height of 631 feet above the landing elevation. At this point, a descent path of 3.9° would have been required to cross the threshold at 50 feet AGL; this was significantly steeper than an optimal or typical descent path of 3°.Footnote 6 The aircraft’s indicated airspeed was 104 knots, and the pitch attitude was 9° nose down. The descent rate was 1500 fpm, and the engine power was set to 11% torque (Appendix A).
The approach was flown visually, without external vertical guidance from a visual approach slope indicator system because this system was not installed at CES4, and without the aid of vertical guidance on the primary flight display because there is no instrument approach at CES4.
At 1101:23, the pilot made a radio call to report that the aircraft was on final approach to make a full-stop landing. At 1101:27, while the aircraft was approximately 1.25 NM from the runway, the aural warning system altitude alert identified that the aircraft was at 500 feet AGL. At this time, the aircraft was descending at 1000 fpm, with an 8° nose-down attitude. The aircraft’s speed was 103 KIAS with a torque setting of 10%.
Overall, during the first 40 seconds of the approach, the engine torque remained under 14%. At the same time, the pitch increased by 8° (from 9.0° nose down to 1.0° nose down), and the indicated airspeed decreased by 23 knots, down to 81 knots.
When the aircraft was 1 NM on final at 350 feet AGL, it began to sink below the optimal 3° descent path (Figure 2). When it reached 100 feet AGL, at 0.45 NM from the runway, it was descending at 500 fpm, with a level pitch attitude and an airspeed of 80 KIAS. At this time, the engine torque was increased from 14% to 24% over 6 seconds. During this increase in engine power, the aural alerting system announced a single “STALL” warning as the airspeed decreased to 78 KIAS. When it was 600 feet short of the runway threshold, the aircraft was at 18 feet AGL, descending at 350 fpm and decelerating through 70 KIAS. At this time, the pitch started to increase, and the alerting system announced an “AIRSPEED” aural warning because the speed had fallen below 70 KIAS.
When the aircraft descended to 1 foot above the ground and was not yet over the paved surface of Runway 28, the aural warning system annunciated 2 successive “STALL” warnings. The indicated airspeed had dropped to 66 knots as the pitch of the aircraft increased to 11° nose up, with 15% engine torque. The pitch and torque remained at these values until 1102:26, when the aircraft made its initial touchdown just within the paved area of Runway 28, approximately 200 feet short of the threshold.
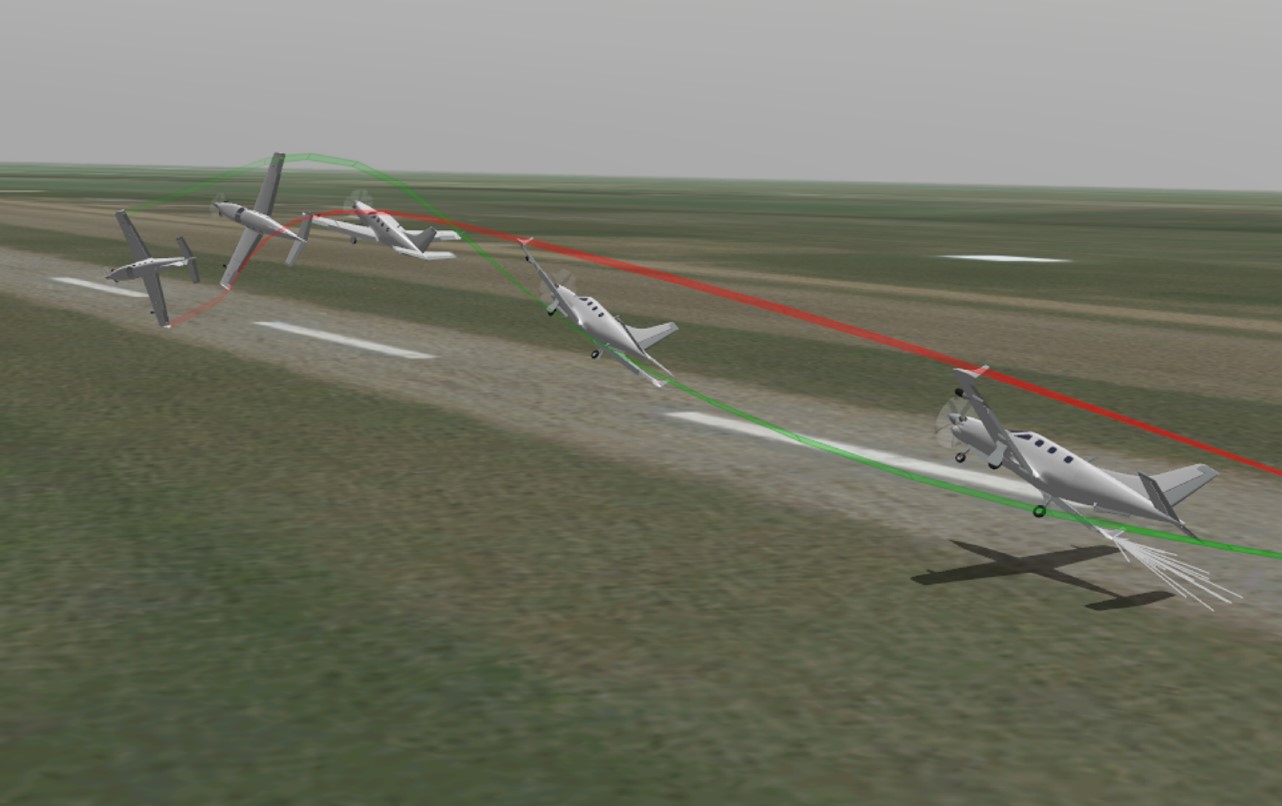
Following the initial touchdown, the aircraft bounced and became airborne again. As the aircraft bounced, the engine power was increased to full power. The aircraft briefly touched down once more, approximately 34 feet left of the runway centreline. At this time, the torque was increasing through 70%, the roll attitude was increasing to the right, and the airspeed was accelerating through 69 knots. The aural alerting system once again annunciated a “STALL” warning.
The aircraft continued to bank right to 43.5°, at which point engine torque was increasing through 83%. During the roll excursion, the right wing tip dragged along the ground (Figure 3 and Appendix B).
After the right wing tip had contacted the runway, the roll reversed and was increasing through 5° left bank as the aircraft approached the centreline and began to pitch up to 24°. The aircraft climbed 28 feet, and the stall warning system activated again with repetitive stall warnings. The aircraft continued to roll left and began to descend, whereupon the left wing contacted the runway surface and fractured. The aircraft continued to roll, and, at 1102:34, it struck the ground inverted, slid off the south side of Runway 28, and came to rest in the grass approximately 50 feet from the runway’s south edge.
The passengers were all wearing lap belts and remained in their seats. Only the passenger seated in the left forward-facing seat at the rear of the cabin wore the available shoulder harness. This passenger and the one in the adjacent rear forward-facing seat received minor injuries; they had no issues unfastening their belts and exiting their seats. During the impact, the unrestrained upper torso of the passenger seated in the right mid-cabin rear-facing seat twisted to her right as the left side of the aircraft collided with the runway. She contacted unsecured baggage stowed beside her seat and was struck by unsecured cabin items accelerating forward. She received serious injuries, was disoriented, and was therefore assisted by another passenger when unfastening her lap belt.
One of the passengers unlocked the main cabin door and attempted to open it. The door was slightly jammed but was eventually opened with a kick from the passenger and with assistance from eyewitnesses who had arrived at the accident site. The passengers were able to egress the aircraft without further issues.
The pilot was wearing a lap belt, but not the available airbag-equipped shoulder harness. During the impact sequence, both cockpit (left and unoccupied right seat) shoulder harness air bags activated. The pilot struck his head on the ceiling and pilot door frame structure and received serious life-changing injuries. He remained trapped in the cockpit for approximately 2 hours until first responders rescued him from the wreckage.
There was no post-impact fire. A signal from the aircraft’s emergency locator transmitter (ELT) was detected by the Canadian Mission Control Centre, and that information was relayed to the Joint Rescue Coordination Centre (JRCC) in Trenton, Ontario.
1.2 Injury to persons
The pilot was seriously injured. The 2 passengers sitting in the rear, forward-facing seats received minor injuries. The passenger in the mid-cabin, rear-facing seat received serious injuries.
| Degree of injury | Crew | Passengers | Persons not on board the aircraft | Total by injury |
|---|---|---|---|---|
| Fatal | 0 | 0 | – | 0 |
| Serious | 1 | 1 | – | 2 |
| Minor | 0 | 2 | – | 2 |
| Total injured | 1 | 3 | – | 4 |
1.3 Damage to aircraft
The aircraft was substantially damaged due to its contact with the runway while inverted and the subsequent impact forces.
1.4 Other damage
Runway lights and runway light reflectors on Runway 28 at CES4 were damaged during the accident sequence. In addition, fuel spilled onto the runway when the left wing fractured during impact.
1.5 Personnel information
The pilot held a private pilot licence for single- and multi-engine land aeroplanes and helicopters, and a Group 3 instrument rating. He completed type training Footnote 7 for the TBM700 N Footnote 8 in June 2019; however, Transport Canada (TC) had no record of the training, nor did the pilot’s licence document record the required type rating. The investigation was given a copy of the training completion letter that was sent to TC and this letter demonstrates that the pilot received TBM700 N type training. A review of the aircraft’s journey log and the pilot’s licensing booklet demonstrated that he satisfied the regulatory recency requirements per section 401.05 of the Canadian Aviation Regulations (CARs). The pilot’s licence was validated with a current Category 3 medical certificate. His last instrument proficiency check was conducted on 06 October 2020 and was valid until 06 October 2022.
The investigation was unable to determine the pilot’s exact amount of flight time. Although the pilot’s log book was not recovered, a review of the occurrence aircraft’s journey log showed that the pilot had 235 flight time hours on that aircraft, of which 15.3 hours were flown in the 90 days preceding the accident. The pilot also previously owned a TBM700 N from 2008 to 2011. The investigation was unable to determine how much flight time was accrued by the pilot on this previous aircraft.
| Pilot licence | Private pilot licence—aeroplane (single- and multi-engine land), private pilot licence—helicopter |
|---|---|
| Type ratings | C25BS, R66 |
| Medical expiry date | 01 October 2023 |
| Total flying hours | Approximately 3000 |
| Flight hours on type | 235* |
| Flight hours in the 7 days before the occurrence | 2 |
| Flight hours in the 30 days before the occurrence | 5.2 |
| Flight hours in the 90 days before the occurrence | 15.3 |
| Flight hours on type in the 90 days before the occurrence | 15.3 |
* This total represents only the hours flown on the occurrence aircraft and does not include any flight time the occurrence pilot may have accumulated on the TBM700 N he owned previously.
1.5.1 TBM700 training
Initial and recurrent training for TBM700 N series aircraft is available from Daher, SIMCOM, and other private training providers. The occurrence pilot completed the SIMCOM initial training program in 2018 and received recurrent training from a private trainer in 2019, 2020, and 2021.
The private training provider administered a recurrent training program that consisted of:
- loss of cabin pressure
- emergency descent mode
- emergency descent without emergency descent mode
- steep turns
- stalls
- system failures
- missed approaches
1.6 Aircraft information
The Daher TBM700 N (TBM 910) is an all-metal, low-wing, pressurized, 6-seat, high-performance turboprop aircraft.
The TBM700 N is produced under the TBM700 type certificate. TBM700 N is the aircraft model designation, which was manufactured under the initial production name TBM 850. The TBM 850 was equipped with a Pratt & Whitney Canada PT6A-66D engine, rated at 850 hp. The TBM 900 is an enhanced version of the TBM 850, with various aerodynamic refinements, including winglets, a redesigned induction system, and a Garmin G1000 avionics suite. The TBM 910 (the production name of the occurrence aircraft) was introduced as a successor to the TBM 900 in 2017; it upgraded the avionics to the Garmin G1000 NXi avionics suite.
The occurrence aircraft was manufactured in 2017. The investigation did not identify any technical malfunctions that would have prevented the aircraft from operating normally during the occurrence flight. As of July 2022, there were 25 TBM700 series aircraft registered in Canada.Footnote 9
| Manufacturer | Daher |
|---|---|
| Type, model, and registration | TBM700 N, C-FFYM |
| Year of manufacture | 2017 |
| Serial number | 1190 |
| Certificate of airworthiness issue date | 17 November 2018 |
| Total airframe time | 449 |
| Engine type (number of engines) | Pratt & Whitney Canada PT6A-66D (1) |
| Propeller type (number of blades) | Hartzell HC-E5N-3C (5) |
| Maximum allowable take-off weight | 3353.86 kg |
| Recommended fuel type(s) | Jet A, Jet A-1, Jet B |
| Fuel type used | Jet A |
1.6.1 Aircraft seating configuration
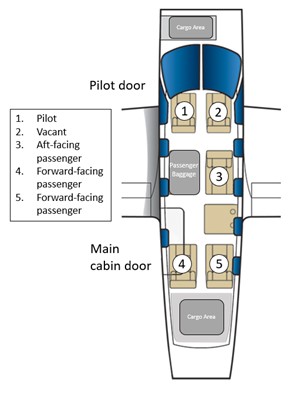
The TBM700 N cockpit is configured with 2 front seats (Figure 4) mounted on rails attached to the floor structure.
The occurrence aircraft passenger cabin was configured with 3 seats.Footnote 10 This seating configuration consisted of 2 individual, forward-facing seats at the rear of the cabin and a mid-cabin rear-facing passenger seat located behind the right cockpit seat. The 4th seat, a rear-facing seat located behind the left cockpit seat, had been removed to accommodate a pet travel kennel and passenger baggage. All cabin seats are mounted on the same rails as the cockpit seats.
1.6.2 Restraint systems
1.6.2.1 Crew safety belts
Each cockpit seat was equipped with a 4-point restraint system (Figure 5) consisting of an adjustable lap belt and a dual-strap inertia reel-type shoulder harness with airbags. The airbags are inflated by 2 inflators located under the backrest fairing, which are activated by an accelerometer fixed under the floor panel in front of the seat. Safety belts are referred to as seat belts by Daher in company publications. The TBM 910 pilot’s operating handbook (POH) states, “[i]f airbags [are] installed, unoccupied seat belts have to be strapped. It is forbidden to fly with these belts unstrapped.”Footnote 11 The concern being that should there be an inadvertent airbag deployment, their inflation could interfere with the pilot’s operation of the aircraft.

The pilot wore the lap belt; however, he was not wearing the airbag-equipped shoulder harness at the time of the accident. The unoccupied right cockpit seat safety belt was not fastened.
1.6.2.2 Passenger safety belts
Each passenger seat was equipped with a 3-point restraint system consisting of an adjustable lap belt and an inertia reel-type shoulder harness diagonally crossing the torso.
The passengers were all wearing the provided lap belts. Only the passenger seated in the forward-facing, rear left cabin seat wore the provided shoulder harness.
1.6.3 Garmin G1000 NXi avionics
The aircraft was equipped with the Garmin G1000 NXi avionics suite. The suite features an integration of all avionics, 3 high-resolution flight displays, a dedicated auto flight mode control panel, a data input keypad, and wireless connectivity options with personal electronic devices.
1.6.3.1 Airspeed indicator
The airspeed indicator on the primary flight display shows airspeed on a moving tape rolling number gauge (Figure 6). A colour-coded (white, green, and red/white barber pole pattern) speed range strip is located on the moving tape. The colours denote the flaps operating range, normal operating range, and maximum operating speed. A red range is also present for low-speed awareness.
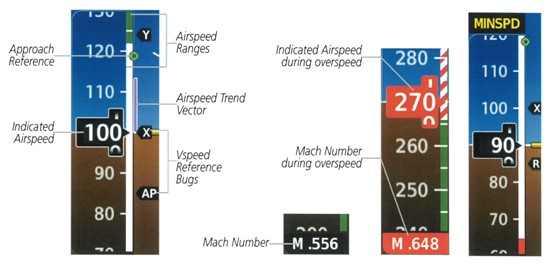
The hollow green circle controlled by the angle of attack (AOA) computer is the approach reference indication. It indicates “an approximate airspeed of 1.3 times the stall speed for the current weight, g loading[Footnote 12] and aircraft configuration.”Footnote 13 The approach reference is most accurate when the aircraft is near approach speed; it will move based on the aircraft’s attitude and flap position. When the aircraft turns, it indicates a speed that provides a safety margin over stall speed, similar to what approach speed provides in level flight.Footnote 14
1.6.3.2 Electronic Stability and Protection
The function of the Electronic Stability and Protection (ESP) system is explained in the Garmin pilot’s guide:
The Garmin Electronic Stability and Protection (ESP™) is designed to provide automatic control inputs to discourage aircraft operation outside a normal flight envelope. Garmin ESP™ works to maintain the desired pitch, roll, and airspeed operating envelope by automatically engaging one or more servos when the aircraft is near a defined pitch, roll and/or airspeed operating limit. While ESP™ utilizes the same sensors, processors, and actuators as the autopilot, it is a separate function. The ESP™ system only operates when autopilot is not engaged and the aircraft is above 200 feet AGL.Footnote 15
1.6.4 Aircraft landing performance
Based on the prevailing weather conditions and the aircraft’s weight at the time of the accident (a density altitude of 2084 feet, a headwind of 10 knots, and an aircraft weight of 6590 pounds), TSB investigators calculated that a full-flap landing at CES4 requires a landing distance of 2175 feet on a paved, level, and dry runway. These data are based on a normal approach speed of 85 KIAS and a 78 KIAS touchdown speed.
1.6.5 TBM 910 go-around procedure
The TBM700 N (TBM 910) POH describes the procedure to follow in the case of a go-around (Appendix C). This procedure also applies in the event that a rejected landing is initiated (see Section 1.18.3 Rejected landing of this report).
In summary, it requires the pilot to select the go-around push button to set the flight director to 10° nose up, apply take-off power, maintain directional control with right rudder, pitch to 10° nose-up attitude, and retract the flaps to 10°. When a positive rate of climb is observed and the speed is 90 KIAS or higher, the landing gear should be selected to the UP position. Once the aircraft accelerates through 115 KIAS, flaps should be retracted to 0°.
1.7 Meteorological information
The graphic area forecast (GFA) Clouds and Weather chart issued for the Prairies region at 0527 indicated that, starting at 0600, CES4 would be under the influence of a cold front moving east-southeast at 10 knots. Frontal passage was forecast to occur in the CES4 area before the arrival of the aircraft. According to the GFA, weather after the frontal passage was forecast to be broken clouds at 4000 feet ASL with tops at 8000 feet ASL and patchy ceilings at 1200 feet AGL.
The GFA Icing, Turbulence and Freezing Level chart issued at 0527 indicated that for the CES4 area at 0600, there would be patchy moderate mechanical turbulence from the surface to 3000 feet ASL. From 5000 feet ASL to 14 000 feet ASL, patchy moderate mixed icing could be present.
The closest aviation weather reporting station was CZVL, 24 NM to the south of CES4.
The aerodrome forecast (TAF) for CZVL issued at 0540 stated that from 0900 weather was forecast to be:
- winds from 320° true at 15 knots, gusting to 25 knots
- visibility greater than 6 statute miles (SM)
- few clouds at 2000 feet AGL, overcast ceiling at 6000 feet AGL
- temporarily between 0900 and 1300, visibility of 5 SM in light rain showers and mist, and a broken ceiling at 2000 feet AGL with an overcast layer at 4000 feet AGL
The automated aerodrome routine meteorological report (METAR) for CZVL issued at 1100 stated:
- winds from 290° true at 14 knots, gusting to 20 knots
- visibility of 9 SM in light rain
- broken ceiling at 5500 feet AGL and overcast clouds at 6500 feet AGL
1.8 Aids to navigation
Not applicable.
1.9 Communications
Not applicable.
1.10 Aerodrome information
CES4 is a registered aerodrome owned by the Town of Westlock and Westlock County. The aerodrome is uncontrolled and has 1 east/west runway (Runway 10/28). The airport elevation is 2250 feet ASL. The asphalt runway is 3000 feet long by 75 feet wide, and the thresholds of runways 10 and 28 are displaced by 200 feet. The runway is equipped with threshold and runway end lights and medium-intensity runway edge lights. At the time of the occurrence, there were no instrument approaches to CES4. In November 2022, NAV CANADA published an area navigation localizer performance with vertical guidance (RNAV LPV) approach for both Runway 10 and Runway 28.
The aerodrome does not have any emergency response or fire-fighting vehicles stationed on site.
At the time of the occurrence, there were no NOTAMs issued for the aerodrome.
1.11 Flight recorders
The aircraft was not equipped with a flight data recorder as defined in section 605.33 of the CARs or a cockpit voice recorder as defined in section 605.34 of the CARs, nor was either required by regulation.
1.11.1 Lightweight data recorder (LDR1000)
The occurrence aircraft was equipped with an LDR1000 lightweight data recorder (LDR), which is a crash-survivable system that records flight data and 2 channels of cockpit audio.
A lightweight flight recording system is one that meets the European Organisation for Civil Aviation Equipment’s (EUROCAE) ED-155 minimum operational performance standard. Unlike a conventional flight data recorderFootnote 16 fitted to most large commercial aircraft, the ED-155 lightweight flight recording system is fitted to smaller aircraft and generally has less stringent crash-survivability requirements.
The occurrence LDR was removed and sent to the TSB Engineering Laboratory in Ottawa, Ontario, for data download and analysis. The audio recorded by the LDR was considered of good quality.
Data from the previous 524 landings, in addition to the occurrence landing, were also downloaded from the LDR for observation and analysis. In the data analyzed, there was no evidence of the pilot routinely controlling the rate of descent during approach with pitch inputs.
1.12 Wreckage and impact information
Following the accident, the wreckage was examined at CES4 with the participation of a safety investigator from the aircraft manufacturer. All airframe fractures, fuel and hydraulic lines, system components, and flight controls were examined to determine continuity and modes of failure. No pre-existing defects were identified.
1.13 Medical and pathological information
1.13.1 Fatigue
According to information gathered during the investigation, there was no indication that the pilot’s performance was affected by fatigue.
1.13.2 Pilot prescription medication
In July 2021, the pilot’s family physician prescribed him a psychostimulant medication, for use on an as-needed basis, that was not approved by TC’s Civil Aviation Medicine Branch. The family physician did not report the use of this medication to the Civil Aviation Medical Examiner (CAME), because he assessed the pilot to not be a risk to aviation safety.
Pilots are required to report on their TC medical report form all visits to medical professionals and current medications (prescription or over-the-counter drugs) they are taking. The pilot did not report the use of this medication to the CAME during his last civil aviation medical examination, 3 weeks before the occurrence.
Following the accident, when the office of the Regional Aviation Medical Officer (RAMO) became aware of the pilot’s use of the prescription medication, the RAMO issued a suspension of the pilot’s medical certificate.
1.13.3 Transport Canada aviation medical certification
The primary activity of TC’s Civil Aviation Medicine Branch is the performance of medical assessments required for the certification of licensed aviation personnel. According to paragraph 424.04(1)(b) of the CARs Standards,
[…] Medical Certificates are issued by the Minister of Transport through the office of the Regional Director, Aviation Licensing following receipt of:
(P) a medical examination report, provided the candidate meets the pertinent medical standards and has been assessed medically fit or fit subject to any restriction or limitation recommended by Civil Aviation Medicine Division Medical Staff […]Footnote 17
1.13.3.1 Civil Aviation medical examination
The purpose of the medical examination is to determine whether an applicant meets the standards that apply to the issuance of the medical certificate that is needed to validate a pilot’s licence. TC is chiefly concerned with managing the risks to aviation, such as the risk of incapacitation, for the validity period of the licence and, if necessary, may request further medical examination.
To obtain or revalidate a medical certificate, an applicant must undergo a medical exam performed by a CAME. CARs Standard 424 requires that the CAME examine the pilot carefully and also stipulates that the examination “shall be sufficiently thorough so as to determine whether the applicant meets the requirements in respect of the category of medical certificate that is applied for or in respect of which a validation is sought.”Footnote 18
TC provides CAMEs with the Handbook for Civil Aviation Medical Examiners,Footnote 19 which contains guidance on how to perform medical examinations and assess medical fitness. During the medical examination, CAMEs are required to complete a Civil Aviation Medical Examination Report, the original of which should be sent to their regional office for the RAMO to review, if required.
For Category 3 medical certificates for private pilots, pilots are required to renew their TC medical certificate, and therefore attend a TC medical examination, every 60 months. If the pilot is over the age of 40, this frequency increases to every 24 months.Footnote 20 The occurrence pilot, who was 60 years of age, had regularly attended a TC medical examination every 24 months.
1.13.3.2 Reporting responsibilities of family physicians
The Aeronautics ActFootnote 21 requires physicians to report to TC any patient whom they believe, on reasonable grounds, to be a holder of a Canadian aviation document and who may, for medical reasons, constitute a risk to aviation safety.
In July 2021, the pilot was prescribed a medication by his family physician that was not approved for use by holders of flight crew licences. No documentation related to the issuing of this medication had been sent to, or requested by, the CAME that had most recently examined the pilot.
The pilot’s family physician was aware that the patient was a licensed pilot and did not report the use of the prescribed medication to the CAME because he assessed the pilot to not be a risk to aviation safety given that he was using the medication on an as-needed basis.
Since 2000, there have been 8 accidents, including this one, in which a finding as to risk was made regarding pilots who had medical conditions that affected safety but were not reported to TC.Footnote 22 These accidents resulted in 10 fatalities and 7 serious injuries.
As part of TSB Air Transportation Safety Investigation Report A21W0089, where it was determined that the pilot’s family physician did not inform TC about prescribed medication, the TSB issued Safety Advisory Letter A21W0089-D2-A1 on 11 January 2023. The letter informed TC that not all physicians were aware of the requirement to report medical issues for their patients that hold a pilot licence. It also encouraged TC to work with the Canadian Medical Association to develop communication strategies to increase the awareness of the reporting requirements for physicians under the Aeronautics Act.
On 19 January 2023, TC responded to the TSB’s Safety Advisory Letter A21W0089-D2-A1. It its response, TC stated that Transport Canada Civil Aviation Medicine had coordinated with the Canadian Medical Association to increase awareness of the reporting requirements for physicians.
1.13.3.3 Disclosure responsibilities of pilot applicants
Since CAMEs are often not the applicant’s family physician, they must rely to a large extent on information disclosed by the applicant. Disclosed information could relate to the pilot’s medical symptoms, medication use, or use of drugs such as cigarettes and alcohol.
TC recognizes that aviation personnel may not volunteer information that could affect their medical certification, typically because they fear losing their medical certificate and, in some cases, their employment. CARs Standard 424 requires an applicant to sign a statement on the medical examination report to confirm that the information provided is complete and correct and that the applicant is aware that it is an offence under the Aeronautics ActFootnote 23 to knowingly make a false declaration. However, the applicant is not required by TC to provide the results of personal medical tests, such as laboratory results, unless these results are required as part of the civil aviation medical certification process.
The pilot did not report the use of the prescribed medication to the CAME.
1.14 Fire
There was no pre- or post-impact fire.
1.15 Survival aspects
During the impact sequence, the pilot and passenger seats remained attached to the aircraft floor beams. The cockpit was partially crushed from the impact; however, the pilot’s occupiable space was retained. The cockpit upper fuselage structure, windscreen, and pilot door remained intact during the impact sequence and subsequent movement off the runway surface. The passenger cabin was not subject to any crushing during the impact, and the occupiable cabin space was retained.
The aircraft was equipped with a 406 MHz ELT,Footnote 24 which activated during the accident.
1.15.1 Seat and safety belt requirements
Subsection 605.25(1) of the CARs requires that
[t]he pilot-in-command of an aircraft shall direct all persons on board the aircraft to fasten safety belts, including any shoulder harness,
(a) during movement of the aircraft on the surface;
(b) during takeoff and landing; and
€) at any time during the flight that the pilot-in-command considers it necessary that safety belts be fastened.Footnote 25
In addition, paragraph 605.26(1)(a) of the CARs requires that “[w]here the pilot-in-command […] directs that safety belts be fastened, every passenger who is not an infant shall ensure that the passenger’s safety belt, including any shoulder harness, or restraint system is properly adjusted and securely fastened.”Footnote 26
Contrary to paragraph 605.27(1)(a) of the CARs, which requires crew members on aircraft to be “seated at their stations with their safety belts, including any shoulder harness fastened during take-off and landing,”Footnote 27 the pilot was wearing the lap portion of the safety belt only; he was not wearing the available airbag-equipped shoulder harness.
1.15.2 Survivability with inflatable restraint systems
The U.S. National Transportation Safety Board (NTSB) published a safety study titled Airbag Performance in General Aviation Restraint Systems.Footnote 28 According to the study, the most common cause of death noted on autopsies for pilots in general aviation (GA) airplane accidents is blunt trauma, accounting for 86% of all GA pilot fatalities.Footnote 29 The study concluded that aviation airbags can mitigate occupant injuries in severe but survivable crashes in which the principal direction of force is longitudinal.
According to the study, occupant injury in GA aircraft can be mitigated by airbags in certain cases. However, the study’s findings were not strong enough to recommend the installation of airbags on all GA aircraft. Only a small number of accidents were analyzed, and of those, beneficial effects were seen in only a small number of cases.
The NTSB also conducted an analysis on the efficacy of lap belt/shoulder harness combinations in GA during the course of the study. This new analysis has provided definitive evidence that the use of both a lap belt and a shoulder harness consistently reduces the risk of fatal or serious injury in pilots when compared to the use of a lap belt alone. The risk of fatal or serious injury with a lap belt alone was nearly 50% higher than with the lap belt/shoulder harness combination.Footnote 30
AMSAFE Aviation Inflatable Restraints published a study titled Evaluations and Survivability of Inflatable Restraint Systems in Small Fixed Wing Aircraft.Footnote 31 The study identified that improved crashworthiness through the use of shoulder harness airbags helps to improve the survivability threshold of dynamic impact accidents. According to the study, impact accidents resulted in aortic and contact type injuries:
[aortic injuries] are caused by the inertial movement of body tissues, when the impact force is well distributed to the body. The other type of injury is referred to as “contact” or force based. These occur usually from excessive occupant flailing, and direct forces cause localized trauma.Footnote 32
The report concludes that survivability issues in small aircraft, as well as opportunities for their improvement, are highlighted in recent accident analyses and other published research related to survivability in GA aircraft, that drastic improvements are possible with existing technology, and that resource priorities should focus on making these aircraft more survivable. The report also states that high-energy impacts in accidents have become more survivable as a result of airbags and their ability to mitigate blunt trauma to the head and chest.
1.15.3 Passenger briefing
The CARs outline the pilot-in-command’s responsibility to ensure that all passengers on board the aircraft are briefed before takeoff with respect to the following:
(a) the location and means of operation of emergency and normal exits;
(b) the location and means of operation of safety belts, shoulder harnesses and restraint devices
(c) the positioning of seats and the securing of seat backs and chair tables;
(d) the stowage of carry-on baggage;
(e) where the aircraft is unpressurized and it is possible that the flight will require the use of oxygen by the passengers, the location and means of operation of oxygen equipment; and
(f) any prohibition against smoking.Footnote 33
TC also provides recommendations and guidance for GA passenger briefings.Footnote 34
In addition, the Daher TBM 910 POH describes the following procedure to be completed during the inside inspection:
Check for pilot and passengers correct locking of belt buckles, as well as automatic locking of shoulder harness by exerting a rapid pull on the latter. If airbags installed, unoccupied seat belts have to be strapped. It is forbidden to fly with these belts unstrapped.Footnote 35
The POH also includes the item “Passenger briefing – As required” in its before taxiing and approach procedures.Footnote 36
There was no indication that the pilot provided passenger briefings during the pre-taxi or approach phases of each leg of the occurrence flight.
1.15.4 Carry-on baggage, equipment and cargo
Subsection 602.86(1) of the CARs states that
[n]o person shall operate an aircraft with carry-on baggage, equipment or cargo on board, unless the carry-on baggage, equipment and cargo are
(a) stowed in a bin, compartment […] or other location that is certified in accordance with the aircraft type certificate […] or
(b) restrained so as to prevent them from shifting during movement of the aircraft on the surface and during take-off, landing and in-flight turbulence.Footnote 37
1.15.5 Ramp and propeller safety
Aircraft propeller-to-person accidents and injuries are not common, but they are often serious and can be fatal. TC’s Small Aircraft Passenger GuidelinesFootnote 38 describe that the most direct route around parked aircraft is not always the safest. The guidelines recommend passengers always follow the directions given by the crew and, if there is one, follow the painted walkway. This way passengers can be seen by any moving aircraft and will stay clear of hazards like propellers or wings.
According to industry best practices, flight crews should never attempt to load or unload an airplane with the engine running.Footnote 39 The aircraft’s engine should always be shut down for loading or discharging passengers or cargo. It is the pilot’s responsibility to ensure passengers understand which areas to avoid and to make sure passengers understand the danger of a moving propeller. Spinning propeller blades are difficult to see in the daytime and nearly invisible at night.Footnote 40
1.16 Tests and research
1.16.1 TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP015/2022 – LDR1000 Data Recovery and Analysis
- LP016/2022 – CVR Download
1.17 Organizational and management information
Not applicable.
1.18 Additional information
1.18.1 Effects of propeller performance on aircraft dynamics
1.18.1.1 Propeller torque
Propeller-driven aircraft are affected by propeller torque, which is a force in the direction opposite to propeller rotation. The propeller torque effect is greatest at high power settings and low airspeeds. The propeller torque produced will cause the left wheel to exert more force on the runway than the right wheel, resulting in some drag. This will induce a yaw to the left while on the ground. The propeller on the TBM700 N rotates clockwise when viewed from the cockpit and, once the aircraft is airborne, propeller torque will cause the aircraft to roll to the left in the absence of the countering aerodynamic control forces produced by the ailerons in response to pilot control inputs. The aircraft is designed such that aileron and rudder controls can counter propeller torque when airspeeds are in the normal and flap-operating speed range. The green speed range strip on the airspeed indicator indicates the normal speed range. The bottom of the white (flap-operating range) speed range strip on the airspeed indicator indicates the power-off stall speed in the landing configuration (gear and flaps down). Aircraft operation below the white speed range may not provide sufficient aileron and rudder control authority to overcome propeller torque forces (including propeller slipstream and P-factor forces).
1.18.1.2 Propeller slipstream
A propeller produces a helically shaped slipstream of accelerated air. The TBM700 N propeller slipstream rotates clockwise, looking forward from the tail of the aircraft, striking the left side of the vertical stabilizer and rudder. This slipstream will cause the aircraft to yaw to the left in the absence of countering aerodynamic control forces produced by the rudder in response to pilot control inputs. This effect is greatest at high power settings and low airspeeds, such as during takeoff or during a go-around, and is countered by the pilot's application of opposite rudder and use of rudder trim.
1.18.1.3 P-factor
P-factor, or asymmetric propeller loading, results when the descending blades have a higher AOA and produce more thrust than do the ascending blades, and causes the aircraft to yaw to the left. This effect is greatest at high power settings and high AOAs, when the aircraft has forward speed. P-factor is countered by the pilot's application of opposite rudder and the use of rudder trim. When the aircraft is rotated for takeoff, the AOA and the P-factor effect both increase.
1.18.1.4 Loss of control on single-engine turboprop aircraft
In February 2014, the French Bureau d’Enquêtes et d’Analyses pour la sécurité de l’aviation civile (BEA) published a case study on loss of control on fast single-engine turboprop aircraft.Footnote 41 The study reviewed 36 accidents involving the TBM700 between 02 August 1991 and 01 March 2010. The accidents generally involved a combination of low speed while in a landing configuration with a rapid increase in thrust. The purpose of the study was to suggest explanatory factors for this. While the study also identified that a few of the accidents recorded involved professional operating organizations, the majority of the accidents reviewed involved private and professional pilots using the aircraft for personal use.
The International Civil Aviation Organization (ICAO) defines a loss of control in flight as “an extreme manifestation of a deviation from intended flight path in flight.”Footnote 42 The BEA’s report expands on this definition and states:
the term “loss of control” covers events during which the attitude and/or the flight path of the aeroplane is no longer controlled by the pilot. This does not necessarily mean that the aeroplane has become uncontrollable.Footnote 43
According to the partial conclusion in the report, “it was not possible to link the accidents reviewed in the study with a lack of effectiveness of the ailerons […] of the TBM 700.”Footnote 44
The BEA study also identified that initial training of private pilots is less in-depth than that of professionals, and recurrent training is less frequent. In addition, the flight conditions of the TBM700 generally comprise long flights carried out with the use of autopilot. It is therefore logical that
when [pilots are] confronted with a sudden and unusual situation, [they] may tend to react by virtue of what [they] learned and practised during initial training on a single-engine piston aircraft. […] [W]hen [the pilot] increases the power in a single-engine turboprop aircraft at low speed, the pilot may be surprised by the delayed onset and intensity of engine torque. Under these conditions, unsuitable inputs to correct the trajectory on final approach or to miss an approach may lead to a loss of control […].Footnote 45
Although fatigue was not a factor in this occurrence, the report also states that in many of the accidents studied, fatigue probably reduced pilot performance levels and
may have led to difficulties in correctly interpreting an unusual situation, in making and executing the appropriate decision, in controlling flight parameters on final approach, and in making the necessary corrections on the controls at the right time.
Although this is true of the end of any flight, it is more evident in the context of using a fast aircraft over long distances to meet personal obligations. This specific context and the possible consequences on the pilot’s performance are not always mentioned explicitly in training […], especially for private pilots.Footnote 46
1.18.2 Stabilized approach
1.18.2.1 General
ResearchFootnote 47 showed that unstable approaches were a causal factor in 66% of 76 approach-and-landing accidents and serious incidents worldwide from 1984 to 1997. As shown in previous investigations by the TSBFootnote 48 and foreign agencies, negative outcomes include tail strikes, runway overruns, and controlled flight into terrain (CFIT). As a result of this knowledge, significant improvements have been made by industry to reduce unstable approach accidents.
The U.S. Federal Aviation Administration (FAA) describes stabilized approaches as:
a key feature to a safe approach and landing. Operators are encouraged by the FAA and the International Civil Aviation Organization (ICAO) to use the stabilized approach concept to help eliminate CFIT. The stabilized approach concept is characterized by maintaining a stable approach speed, descent rate, vertical flightpath, and configuration to the landing touchdown point.Footnote 49
In November 2000, the Aircraft Owners and Pilots Association published an article titled “The Stabilized Approach.”Footnote 50 The article states that the concept of stabilized approaches was first advocated in turbine aircraft in the late 1950s and early 1960s, when pilots were discovering that new jet transport aircraft were harder to slow during approach for landing than the large piston and turboprop aircraft they were used to. At the time, turbine engines also responded to power changes more slowly compared to aircraft with propellers, and turbine aircraft were frequently involved in undershoot accidents, in which they landed short of a runway.
Later accidents with turbine aircraft showed that pilots were having trouble with overshoots, which often resulted in excursions off the end of a runway. These accidents occurred when pilots did not slow their aircraft to approach speed and configure for landing early enough to land on the runways that they were using.
This trend led the airline industry to adopt a procedure called the stabilized approach. As the article explains,
[t]his means that at some predetermined point on the approach, usually 500 or 1000 feet AGL, the aircraft will be at the correct final approach speed, configured (landing gear down, final flaps), on glide path (or a "normal descent angle for a normal landing"), and spooled (all engines are at the final power setting for landing). Thus, everything is complete.Footnote 51
The article continues, stating that time is the major benefit when flying a stabilized approach because time facilitates pilots’ perception of changes, allowing them to make corrections to course, altitude, or aircraft management accordingly:
The key to a stabilized approach is to slow the pace of the critical final segment. If you're doing it right and stabilize early, it seems that there is nothing left to do; time expands as you sit observing the airplane during the final minute to the runway. At this time on the approach you are primarily monitoring, not manipulating, and that is better for situational awareness during the approach.Footnote 52
The accepted methodFootnote 53 of controlling the descent path to achieve a stable approach is by using the elevator to control pitch, which in turn controls airspeed, and power to control the rate of descent.
Similarly, the FAA’s Airplane Flying Handbook further describes how the descent angle is controlled during the final approach:
On final approach, the pilot adjusts the pitch attitude, power, and trim so that the airplane is descending directly toward the aiming point at the appropriate airspeed in the landing configuration. If it appears that the airplane is going to overshoot the desired landing spot, a steeper approach results by reducing power and lowering the pitch attitude to maintain airspeed. […] If the desired landing spot is being undershot and a shallower approach is needed, the pilot increases both power and pitch attitude to reduce the descent angle.Footnote 54
1.18.2.2 Transport Canada stabilized approach criteria (visual flight rules)
TC’s Flight Test Guide—Private Pilot Licence—Aeroplane contains a generic description of a VFR stabilized approach.
On the correct final approach flight path:
- Briefings and checklists complete;
- Aircraft must be in the proper landing configuration appropriate for wind and runway conditions;
- Appropriate power settings applied;
- Maximum sink rate of 1000 feet per minute;
- Speed within +10/-5 knots of the reference speed;
- Only small heading and pitch changes required;
- Stable by 200 feet AGL.
Note: If stability is not established by 200 feet AGL, an overshoot will be executed.Footnote 55
1.18.2.3 Daher TBM700 series stabilized approach criteria
Daher TBM stabilized approach criteria are published in Flight Information Letter (FIL) FIL.2015-T1.Footnote 56 The stabilized approach criteria provide guidelines and parameters necessary to define a stabilized approach during final descent. The FIL recommends that pilots flying approaches under the normal procedures outlined in the POH who cannot continuously meet the stabilized approach criteria should consider executing either a go-around or a missed approach as a prudent action.
The FIL further states that for visual meteorological conditions, the stabilized approach criteria shall be met no later than 500 feet above airport elevation. The following procedure is provided:
Landing Configuration
- Gear down and landing flaps indicated
- Exception: Emergency procedure
Profile
- ON flight path (visual cue and / or instrument back-up)
Speed
- +10 KIAS / -5 KIAS of target speed (Vref increased for wind/gust)
- Elevator trim — neutral elevator control pressure
Minimum power (torque)
- 10% TRQ
Maximum rate of descent
- 1,000 ft. / min.Footnote 57
1.18.3 Rejected landing
A rejected landing, also known as an aborted landing, is “a go-around maneuver initiated after touchdown of the main landing gear.”Footnote 58 The Flight Safety Foundation lists some of the factors that may result in bouncing during landing:
- loss of visual references
- excessive sink rate
- late flare initiation
- incorrect flare technique
- excessive airspeedFootnote 59
The Flight Safety Foundation also acknowledges that bounce-recovery techniques vary with each aircraft type and with the height reached during the bounce, and summarizes 2 recovery techniques. To recover from a light bounce, the pilot will typically maintain or regain a normal landing pitch attitude, continue the landing, use power as required to soften the second touchdown, and be aware of the increased landing distance. In the case of a more severe or hard bounce, the pilot should not attempt to land because the remaining runway may be insufficient for a safe landing. A rejected landing should be initiatedFootnote 60 (see Section 1.6.5 TBM 910 go-around procedure of this report).
2.0 Analysis
An examination of the wreckage showed that there was no indication of airframe or engine failure or system malfunction during the occurrence flight. There was also no indication that the pilot’s performance was degraded due to physiological factors such as fatigue or medications. The analysis will therefore focus on the execution of the approach, touchdown, and go-around. It will also discuss safety belts, unsecured cabin items, and ramp safety, as well as the use of prescription medications not approved by Transport Canada’s Civil Aviation Medicine Branch.
2.1 Unstable approach
On arrival at Westlock Aerodrome (CES4), the pilot flew a visual approach without external and internal aircraft vertical guidance; at the time of the occurrence, CES4 had neither a visual approach slope indicator system nor an instrument approach.
The aircraft joined the circuit at 1250 feet above ground level (AGL), and on the downwind leg of the approach, when landing flaps were selected, the aircraft gained altitude and climbed to 1400 feet AGL.
When the aircraft completed the turn to establish the final approach, it was 1.4 nautical miles (NM) from the threshold at 631 feet AGL. At this point, a descent path of 3.9°, which is significantly steeper than an optimal descent path of 3°, would have been required to cross the threshold at 50 feet AGL. The airspeed was 104 knots indicated airspeed (KIAS), 19 knots faster than the normal approach speed of 85 knots listed in the pilot’s operating handbook. The aircraft was pitched nose down 9° and was descending at 1500 fpm with an engine torque setting near idle (11%).
When the aircraft reached 500 feet AGL, at 1.25 NM from the runway, the aural warning system notified the pilot with a 500-feet altitude call-out. At this time, the airspeed was 103 KIAS, and the aircraft was pitched nose down 6°, descending at 1000 fpm with a torque setting of 10%.
Stable approach guidance from the aircraft manufacturer states that by 500 feet above airport elevation, the aircraft shall be “ON flight path” with an airspeed of no more than 10 KIAS over the target approach speed and no less than 5 KIAS below, with a torque setting of no less than 10% and a vertical speed less than 1000 fpm. At this point in the occurrence flight, the aircraft was 18 KIAS above the normal target speed and approximately 50 feet or 0.5° above the optimal 3° approach slope. It could not be determined whether the pilot was intentionally flying a steeper than optimal approach path or simply unaware, without guidance, that he was above the optimal path.
At 500 feet AGL, the airspeed was above the required range, and the aircraft was in a state of deceleration. Although stable approach policies and guidance normally provide a specific altitude or height at which the aircraft’s stability should be assessed, the intent of the stabilized approach concept is that the parameters are stabilized early and maintained until touchdown.
As the approach continued below 500 feet AGL, the aircraft’s speed continued to decrease steadily, and by 350 feet AGL, when the aircraft was descending through the optimal 3° slope, the airspeed was 92 KIAS. When the aircraft reached 100 feet AGL, 0.45 NM from the threshold, the aircraft was descending at 500 fpm, with a level pitch attitude and an airspeed of 80 KIAS. At this time, the aircraft was 75 feet or approximately 2° below the optimal slope.
Finding as to causes and contributing factors
The aircraft joined the final approach well above the optimal 3° descent path and, during the steep approach that followed, the aircraft’s airspeed continually decreased and resulted in an unstabilized approach.
2.2 Flight path corrections on short final
As the approach continued, the aircraft continued to decelerate, and when the aircraft was approximately 600 feet short of the runway and at an altitude of 18 feet AGL, the airspeed was decreasing through 70 KIAS. The pilot then began correcting for the low altitude by increasing the pitch of the aircraft, which resulted in a further decrease in airspeed.
When the aircraft descended to 1 foot above the ground prior to the paved surface of Runway 28, the aural alerting system annunciated 2 successive “STALL” warnings as the airspeed had decreased to 66 KIAS. The pilot continued to hold the pitch at an 11° nose-up attitude, while engine torque remained constant until the aircraft contacted the runway.
The accepted method of controlling the aircraft while on an approach is by using the elevator to control pitch, which in turn controls airspeed, and power to control the rate of descent. However, during the occurrence approach, the pilot used pitch to control the rate of descent rather than power and, as a result, the aircraft’s airspeed continued to decay.
Finding as to causes and contributing factors
On short final, the pilot reduced the rate of descent by increasing pitch rather than by adding power. As a result, the airspeed continued to decrease and the aircraft entered a stall, resulting in a hard landing and a subsequent bounce.
2.3 Rejected landing
In response to the bounce during the hard landing, the pilot initiated a rejected landing (see Section 1.18.3 Rejected landing). During the rejected landing, the pilot did not maintain a 10° nose-up attitude, as required by the procedure outlined in the TBM 910 pilot’s operating handbook. Instead, the aircraft’s pitch was increased to a 25° nose-up attitude, resulting in the aircraft approaching a stall. In this condition, the effectiveness of the rudder and ailerons were greatly reduced, and they were unable to counter the torque, slipstream and P-factor being produced by the engine and propeller at full power.
Finding to causes and contributing factors
During the attempted rejected landing, the aircraft entered a 25° nose-high attitude and approached a stall condition. This low-speed condition combined with the high power setting resulted in the aircraft entering a rapid roll to the left and striking the runway in an inverted attitude.
2.4 Cabin safety
When the 2 passengers boarded the aircraft at Calgary/Springbank Airport, the pilot did not provide a safety briefing on the safety features of the aircraft nor did he ensure that items in the cabin were secure. Before landing, the pilot did not ensure that the passengers wore their 3-point restraint system correctly; 2 of the 3 passengers did not wear their shoulder harness.
During the impact sequence, loose items in the cabin tumbled about the cabin and accelerated forward as the aircraft rolled inverted, struck the ground, and slid off the runway. The rear-facing forward seated passenger was injured by the loose items, which were not properly secured. The passenger also received injuries when she struck the cabin bulkhead because she was not restrained by her shoulder harness.
Finding to causes and contributing factors
The passengers did not receive a safety briefing before departure or before landing, and multiple items in the cabin were not secured. As a result, 1 passenger sustained serious injuries due to the deceleration forces and the loose items that were thrown around in the cabin during the accident.
2.4.1 Pilot safety belt usage
Although the pilot was wearing his lap belt, he did not wear the airbag-equipped shoulder harness. The shoulder harness straps were not fastened to the lap belt, and this allowed the pilot to be flung about the cockpit during the accident. At some point during the impact sequence, the pilot’s head struck the ceiling and pilot door frame structure and he received serious head injuries.
Finding as to cause and contributing factors
The pilot was not wearing the available shoulder harness, and his torso was unrestrained during the impact. As a result, he sustained serious injuries.
2.5 Prescription medications
The investigation determined that the pilot did not report to his Civil Aviation Medical Examiner the use of a medication that was prescribed by his family physician. This medication was not approved by Transport Canada (TC) for use by pilots. In addition, the pilot’s family physician did not report the pilot’s medication to TC. Both of these contributed to TC’s lack of understanding of the pilot’s health.
Finding as to risk
If pilots do not declare all health issues to TC Civil Aviation Medical Examiners and pilots’ family physicians do not declare issues assessed to be a risk to aviation safety to TC, there is an increased risk that pilots will operate with diagnosed medical conditions or medical side effects that could affect flight safety.
Finding: Other
Following a review of the pilot’s medical history and prescription medication use, the investigation determined that the medication did not contribute to the accident.
2.6 Ramp safety/propeller safety
During the stopover at the Calgary/Springbank Airport to pick up 2 passengers and offload a bike through the main cabin door, the aircraft engine was not shut down and remained running during the passenger embarkation. The pilot remained in the cockpit. While there is no TC regulation precluding the loading of an aircraft in this manner, TC does provide various guidelines for small aircraft passenger safety.
Finding as to risk
If an aircraft propeller is rotating and passengers are not supervised during boarding operations, there is a risk that passengers may inadvertently contact the propeller, potentially causing fatal injuries.
3.0 Findings
3.1 Findings as to causes and contributing factors
These are conditions, acts or safety deficiencies that were found to have caused or contributed to this occurrence.
- The aircraft joined the final approach well above the optimal 3° descent path and, during the steep approach that followed, the aircraft’s airspeed continually decelerated and resulted in an unstabilized approach.
- On short final, the pilot reduced the rate of descent by increasing pitch rather than by adding power. As a result, the airspeed continued to decrease and the aircraft entered a stall, resulting in a hard landing and a subsequent bounce.
- During the attempted rejected landing, the aircraft entered a 25° nose-high attitude and approached a stall condition. This low-speed condition combined with the high power setting resulted in the aircraft entering a rapid roll to the left and striking the runway in an inverted attitude.
- The passengers did not receive a safety briefing before departure or before landing, and multiple items in the cabin were not secured. As a result, 1 passenger sustained serious injuries due to the deceleration forces and the loose items that were thrown around in the cabin during the accident.
- The pilot was not wearing the available shoulder harness, and his torso was unrestrained during the impact. As a result, he sustained serious injuries.
3.2 Findings as to risk
These are conditions, unsafe acts or safety deficiencies that were found not to be a factor in this occurrence but could have adverse consequences in future occurrences.
- If pilots do not declare all health issues to Transport Canada Civil Aviation Medical Examiners and pilots’ family physicians do not declare issues assessed to be a risk to aviation safety to Transport Canada, there is an increased risk that pilots will operate with diagnosed medical conditions or medical side effects that could affect flight safety.
- If an aircraft propeller is rotating and passengers are not supervised during boarding operations, there is a risk that passengers may inadvertently contact the propeller, potentially causing fatal injuries.
3.3 Other findings
These items could enhance safety, resolve an issue of controversy, or provide a data point for future safety studies.
- Following a review of the pilot’s medical history and prescription medication use, the investigation determined that the medication did not contribute to the accident.
4.0 Safety action
4.1 Safety action taken
4.1.1 Transport Canada
After the accident, Transport Canada learned of the pilot’s use of a non-approved prescription medication and suspended the pilot’s medical certificate until further reassessment is completed.
This report concludes the Transportation Safety Board of Canada’s investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .
Appendices
Appendix A – Approach flight data plot

Source: TSB Recorders & Vehicle Performance Division
Appendix B – Landing flight data plot
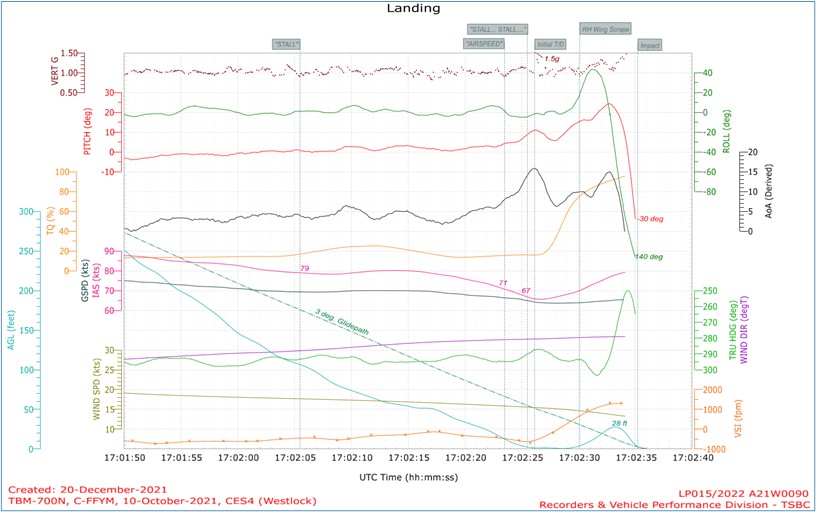
Source: TSB Recorders & Vehicle Performance Division
Appendix C – TBM700 N (TBM 910) go-around procedure
1 - GO AROUND push-button.......................................................................... Press
It provides the moving up of the flight director to + 10°.
Simultaneously:
2 - THROTTLE....................................................................................................... T/O power
NOTE: The airplane will tend to yaw to the left when power is applied. Right rudder pressure will be required to maintain coordinated straight flight until the rudder trim can be adjusted.
3 – Attitude.......................................................................................................... 10° Up
4 - FLAPS lever..................................................................................................... TO
>> Weight below 6579 lbs (2984 kg):
If airspeed has been maintained at 80 KIAS or more and TRQ 100 %, select flaps to TO position as soon as the 10° Up attitude has been attained.
When the vertical speed is positive and when airspeed is at or above 85 KIAS:
5 - LANDING GEAR lever.................................................................................... UP
All warning lights OFF
When airspeed is at or above 110 KIAS :
6 - FLAPS lever..................................................................................................... UP
7 - Climb airspeed............................................................................................... As required
>> Weight above 6579 lbs (2984 kg):
If airspeed has been maintained at 85 KIAS or more and TRQ 100 %, select flaps to TO position as soon as the 10° Up attitude has been attained.
When the vertical speed is positive and when airspeed is at or above 90 KIAS:
8 - LANDING GEAR lever.................................................................................... UP
All warning lights OFF
When airspeed is at or above 115 KIAS:
9 - FLAPS lever..................................................................................................... UP
10 - Climb airspeed............................................................................................. As required
All:
11 – TRQ............................................................................................................... As required
(Source: reproduction of procedure from Daher, TBM 910 Pilot’s Operating Handbook, pp. 4.4.62-4.4.63.)