Crew member lost overboard
Bulk carrier Kent
Near Verchères, Quebec
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 16 July 2002, in fair weather and good visibility, the loaded bulk carrier Kent was downbound off Verchères, Quebec, under the conduct of a pilot. In the late afternoon, the bosun and another crew member were securing the port lifeboat ready for sea. The bosun was sitting on a davit cradle securing the trigger line when the lifeboat suddenly released and struck him on its descent. He then lost his grip and fell backwards into the water.
The alarm was raised and several life rings were thrown to the bosun's aid. Auxiliary search and rescue craft were quickly on the scene, but the bosun could not be found. His body was recovered five days later. The cause of death was drowning.
Factual information
Particulars of the vessel
| Name | "Kent" | |
|---|---|---|
| Official number | HK-0844 | |
| Port of registry | Hong Kong | |
| Flag | Hong Kong | |
| Type | Bulk Carrier | |
| Gross tonnage | 17 825 | |
| LengthFootnote 1 | 185 m | |
| DraughtFootnote 2 | Forward: 9 m | Aft: 9.1 m |
| Built | 1984, Naikai SB, Setoda, Japan | |
| Propulsion | Hitachi B&W 7L55GA, 9290 BHP, driving a single fixed propeller | |
| Cargo | Wheat | |
| Crew | 20 | |
| Owner | Kent Pacific Shipping, Hong Kong | |
| Operating Managers | Indochina Ship Management (HK) Ltd., Hong Kong | |
Description of the vessel
The Kent is a handy-sized bulk carrier with the wheelhouse, accommodation, and engine room located aft. The vessel has five hatches and four cranes. One 30-person lifeboat on a set of roller track gravity davits is located at each side of the accommodation.
The vessel was delivered in January 1985 and originally sailed as the LT Odyssey. In 1998, the vessel changed ownership and was registered with the Cayman Islands, as the Millennium Osprey. In spring 2002, the vessel again changed ownership, sailing as the Kent under Hong Kong registry. The vessel remained in class with Det Norske Veritas (DNV) throughout.
History of the voyage
On 30 June 2002, the Kent was in Snell lock upbound for Marinette (Wisconsin) to discharge a partial load of pig iron, when the forward cradle of the port lifeboat davit struck the lock wall and became distorted. At Marinette, the vessel was inspected by a DNV class surveyor who issued a condition of class (COC), which stated that repairs to re-align the davit were to be carried out and the system was to be operationally tested for DNV prior to the vessel transiting international waters. After discharging cargo at Marinette, the Kent continued to Thunder Bay, Ontario. On 11 July 2002, the Kent departed Thunder Bay loaded with 17 170 metric tons of wheat.
The voyage downbound through the Great Lakes and St. Lawrence Seaway was uneventful. However, the master was informed by the ship manager that stopping at a berth to repair the port lifeboat davit was to be avoided in order not to delay the voyage. On 12 July, he was instructed by the operating managers to attempt a re-alignment of the davit while under way, using on-board resources at his disposal. It was suggested they use 5/10 ton chain blocks anchored to welded pad eyes on deck to pull the davit into line. Additional instructions followed later requiring the use of cold repair methods only, but hot work had already been initiated.
On 16 July, at around 0220,Footnote 3 the Kent commenced passage through Beauharnois, Ste. Catherine and St. Lambert locks to berth at Montréal at 0925.
That day, the port davit was surveyed by a Transport Canada (TC) inspector and a DNV surveyor who rejected the repairs as they had not been carried out in accordance with class requirements for restoration of the davit to its original state. The classification surveyor viewed the davit repairs by the crew to be temporary, considering that the efficient operation of the davit system during successive lifeboat launching/retrieval drills, or in the event of an emergency could not be relied upon. Consequently, a COC was issued by DNV in the form of a short-term flag state exemption, which stipulated that an additional 20-person liferaft be carried on the port side, until the port davit was properly repaired or renewed, but prior to 15 September 2002.
The starboard lifeboat was lowered and raised to the satisfaction of the TC inspector and the DNV surveyor and properly secured ready for sea. Although the defective davit was not approved for safe use, the master wanted to assure himself that this equipment could be operable in the event of an emergency. Accordingly, he ordered the port lifeboat lowered and then raised to his own satisfaction. The port lifeboat had not been secured for sea. A 20-person liferaft was installed next to the port lifeboat davits in accordance with DNV requirements. At 1720, the pilot was already on board and the vessel prepared to leave Montréal.
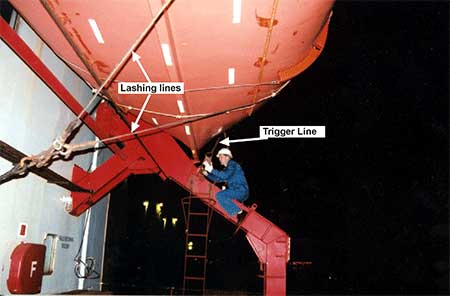
The Kent was under way when the bosun was instructed to secure the port lifeboat properly for sea by connecting the fore and aft trigger lines, and he called on a seaman to help him with the work. When the seaman arrived at the port lifeboat station, the bosun was already at work. He was sitting astride the forward davit cradle, close to the underside of the lifeboat, trying to secure the forward trigger line to the trigger mechanism on the cradle (see Photo 1). The seaman climbed the aft cradle ladder and attempted to do the same with the aft trigger line. When the seaman realized there was not enough slack in the line to permit the connection, he descended the ladder with the intention of lengthening the turnbuckle at the other end. Shortly after reaching the deck he heard a noise, and turned to see the roller gravity davits with the suspended lifeboat, sliding down the cradle.
The noise also alerted the ship's electrician who was nearby. Both the electrician and the seaman rushed to the lifeboat davit winch and applied the brake. The lifeboat stopped descending but not before hitting the bosun, sending him backwards. He clung to the trigger line momentarily, but lost his grip and fell overboard into the water 15 m below. The time was approximately 1825.
"Man overboard" was quickly communicated to the bridge where an officer of the watch, a helmsman and a pilot were navigating the vessel. The pilot immediately put the engine to dead slow ahead, but the confined area of the channel prevented a turning or full astern manoeuvre. The pilot also released the port smoke buoy, but this fell into the partially deployed port lifeboat. At approximately this time, the master arrived on the bridge and released the starboard smoke buoy. Another life ring was also thrown into the water, and persons on deck could see the bosun apparently swimming some 15 to 20 m from one of the buoys; however, they lost sight of him within minutes.
Soon after the pilot had broadcast a PAN PAN PAN message, a yacht came out of Verchères marina and began searching the area. The crew was mustered to the boat stations and the port lifeboat was prepared, but not lowered to the water as the vessel had too much way on to launch the boat safely. As the Kent proceeded down river, reducing speed, the Canadian Coast Guard vessel CG 1204 passed upbound, having joined the search. A military helicopter was also on the scene within approximately one hour of the bosun falling overboard.
At 1915, the Kent came to a safe anchorage off Contrecoeur. It was still daylight and searches continued until darkness at 2130, but without success. Five days later, the bosun's body was recovered approximately 10 miles downstream of the site of the incident.
Victim
According to the ship management company records, the victim had been sailing on various ocean-going vessels since 1990. He had been a deckhand from 1990 to 1994, and, since 1996, he had acted as bosun on four assignments, giving him more than three years of related experience. He held a certificate of competency as a deck rating, issued on 21 November 2001 by the Republic of the Philippines. His last medical exam, given at Manila on 01 April 2002, certified that he was in good health and fit to work.
An autopsy revealed that the cause of death was drowning.
Environmental conditions
The wind was calm, with clear visibility. The St. Lawrence River current was two knots setting at 045° T. The water temperature was approximately 21°C, and the air temperature was 22°C.
Vessel History and Certification
Because of the change of ownership and flag in early 2002, the Kent was issued short-term safety equipment and safety construction certificates by DNV at Tema, Ghana, on 02 May 2002. The certificates were valid until 01 October 2002. The certificate of registry was issued by Hong Kong Marine Department (HKMD) on 18 April 2002.
The vessel's Minimum Safe Manning (MSM) certificate, issued at Hong Kong on 12 April 2002, specified six deck ratings (four seamen grade I, one seaman grade II, and one seaman grade III) and three engine-room ratings. On July 12, the vessel's operating managers applied to the HKMD for a re-examination of the MSM, with the view to having the deck crew reduced from six seamen to four. The proposal was based upon a comparison of mooring arrangements and crew levels on similar ocean-going ships under management. HKMD determined a minimum deck crew of five for the Kent, and a new MSM certificate was issued on 30 July 2002, specifying the requirement for four seamen grade I and one seaman grade II or III.
The vessel held an interim International Safety Management Code (ISM) certificate, which was issued by DNV on 06 May 2002, and was valid to 05 November 2002. The managing company's Document of Compliance was issued by DNV on 04 September 2001.
Emergency drills
Emergency fire drills and abandon ship drills were recorded in the ship's records. An overboard drill was logged on 30 May 2002. The lifeboats had been lowered and raised approximately four or five times since the crew had joined the vessel on 28 April 2002.
Crew information
On 28 April 2002, a new crew of 20 boarded the vessel while at anchor off Tema, Ghana. The master and chief engineer were Russian nationals, and the remainder were from the Philippines. English was the common language used between the senior officers and crew.
The deck department comprised the master, three officers and four seamen grade I (bosun and three deckhands/helmsmen). Another crew member had a lower grade seaman's qualification (II or III), but he was assigned engine-room duties. Throughout the time the vessel was in the Great Lakes and St. Lawrence Seaway, it was operating with four deck ratings and four engine-room ratings.
The bosun was on day work, and when required for special operations such as lock passage, he worked the hours necessary to accomplish the particular task. He participated in the lock operations during the vessel's downbound voyage from Thunder Bay. The ship's records indicate that on July 15, the bosun was given the afternoon off prior to entering the eastern section of the Seaway, where he was required to assist in lock operations between Lake Ontario and Montréal. Consequently, during the 24-hour period prior to the accident, he was "off duty" for approximately four hours.
Port gravity davits
Each set of lifeboat gravity davits, model ST-39, complied with classification rules in force at the time of their manufacture. They were built by Sekigahara Seisakusho Ltd. of Gifu, Japan, and had been installed during vessel construction in 1984.
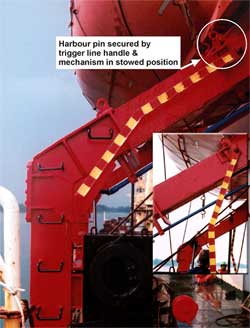
With a lifeboat on its roller gravity davits in the stowed position, the trigger line release handles are in line with the davit cradles (see Photo 2). In this "locked" position, the harbour pins are secured across the roller track to prevent the descent of the gravity davits holding the lifeboat. In the released position, the trigger line release handles are pulled down to the vertical, simultaneously releasing the trigger line and allowing the harbour pin to be swept aside as the gravity davits, with the suspended lifeboat, descend the davit cradle roller tracks (see inset in Photo 2).
The starboard lifeboat/gravity davits had been tested, safety-approved, and made ready in port for the intended voyage, with the lifeboat stowed under the gravity davits in the "locked" position. However, the port side davit system was in the released condition, with the lifeboat held in place with only lashing lines and the winch brake, when the vessel set sail from Montréal.
During the course of the accident investigation, an inspection of the port side gravity davit revealed the following:
- When the weighted inboard end of the brake lever mechanism was lifted into the "brake off" position, it remained stuck in the off position after the lever was released, instead of falling into place to reset the brake.
- With the safety pin on the brake lever mechanism in place to avoid accidental release, a gap of 12 mm existed between the safety pin and the lever. This gap allowed the lever to be lifted sufficiently to disengage the brake and release the lifeboat.
- Parted ends of a broken lashing line showed signs of advanced corrosion and wear. Close examination by the TSB Engineering Branch established that the number of wires within the port lashing line had been reduced to 37 per cent of the original wire count (from 144 to 54).Footnote 4
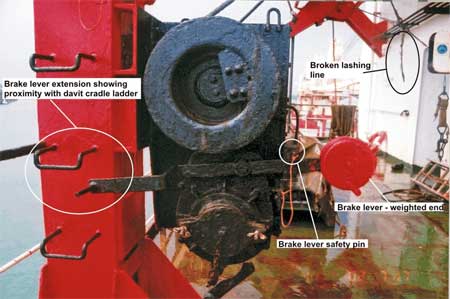
- The outboard end of the brake lever (opposite the weighted end) was extended such that the handle was near the vessel's side to control, within view, the lowering of the lifeboat down the ship's side to the waterline. The handle was in very close proximity to (6 cm below and 5 cm out from) the second rung of the aft cradle ladder (see Photo 3). It was further noted that if this handle was pushed down, it would have the same effect as lifting the brake lever at the inboard (weighted) end, that is, to disengage the brake.
Although a manufacturer's instruction manual for the davit and its equipment was found on board, the lowering and hoisting instructions were of a general nature. They did not include specific safe-working practices or details on the harbour pin and trigger line arrangements.
Analysis
The event
The roller gravity davits suspending the port lifeboat were not in the locked position with the triggers set in place to hold the weight of the moveable boat/davit assembly. Consequently, the load was being taken by the winch/braking system and the lashing lines.
As the bosun tried to secure the forward trigger line while sitting astride the davit cradle, the other seaman was trying to do likewise on the aft davit cradle. Realizing his line was too short to arm the trigger mechanism, the seaman descended the cradle by way of the welded rungs of the cradle ladder. When he descended the ladder, the lifeboat on its roller davits began to move down the cradle track. In the few seconds it took to realize what was happening, the lifeboat had already descended approximately half of its travel, knocking the bosun overboard. The winch brake did not automatically reset, and manual application of the brake to stop the lifeboat was too late. Although the seaman could not say with certainty whether or not he stepped on the brake lever extension during his descent of the ladder, the sequence of events and the fact that the brake lever extension was so close to the welded rungs of the ladder, point toward this possibility. The excessive play in the safety pin arrangement allowed the brake to disengage, and the lashing line that held the boat in place had ruptured as soon as the weight of the boat and roller davits came to bear upon it.
Safe operating procedures
The captain and crew had joined the vessel some two months earlier. Although the gravity davit system was similar to most other types, release mechanisms and davit configurations can differ. The on-board instruction manual for davit use was lacking in detail and poorly translated from the original Japanese.
The lack of clear and accurate descriptions of the equipment and operating instructions was a contributing factor revealed in a recent U.K. Safety Study of lifeboat and launching system accidents.Footnote 5 During the International Maritime Organization (IMO) Sub-Committee meeting on flag state implementation in April 2002, numerous casualty reports were reviewed by the correspondence group on casualty analysis. One of the findings was that without proper guidance or encouragement in the use of easily understood and relevant manuals, crews are at greater risk of making errors of judgment and understanding. A recent IMO MSC circular reiterates this point, citing lack of familiarity with the equipment and design faults as factors contributing to accidents.Footnote 6 National statistics from the U.K. show that 12 lives have been lost in lifeboat accidents since 1989.Footnote 7 According to TSB data on lifeboat operations in Canadian waters, 14 fatalities occurred over a similar period.
On board the Kent, not only had the bosun placed himself in a dangerous position, he was undertaking a two-person task alone. Ideally, one person must hold the securing eye of the trigger line steady, while another arms the trigger line by swinging the trigger release arm up and parallel with the cradle arm, pinning it in place. Preferably, the person holding the securing eye should be in a safe position, clear of the davit cradle track, such as from a vertical ladder located at the side of the davit cradle, directly in the way of the trigger securing position.
Equipment malfunction
The winch brake, although operable, was in poor condition. In particular, the auto-stop safety feature of the brake lever counter-weight did not work. Once the brake lever was lifted into the "brake-off" position, it stayed there, requiring additional physical force to re-engage the brake completely by depressing the lever (instead of the counterweight dropping into place by itself).
The safety pin, which would normally prevent the brake lever from being released accidentally, was positioned in such a way that it did not provide a positive lock. The 12-mm gap allowed the lever to be moved enough to release the brake with the safety pin still in place.
The steel wire cable lashing line was corroded well beyond its serviceable life. Although plastic protected wire cable can hide the condition of a steel wire, in this case, even a cursory inspection would have revealed the deteriorated condition of the cable. The failed cable, together with a similar piece of lashing from the starboard lifeboat davits, was examined by the TSB Engineering BranchFootnote 8 (see photos 4 and 5). It was concluded that only 37 per cent of the steel wires within the port cable were carrying the load and 55 per cent were effective in the starboard cable. Severe corrosion caused the starboard cable to fail under testing at a load of 1638 kg, and the port side would have likely failed at a load of approximately 1119 kg.


A copy of the TSB Engineering Report, LP 089/2002, Failed Cable Examination - Lifeboat Lashing Lines - M.V. Kent, is available upon request.
Most accidents are the result of several factors that combine to produce the event. The physical defences that were meant to protect the crew - davit winch brake, safety pin and lashing line - were disabled or seriously at fault. Consequently, the bosun was working in an unsafe environment.
International Safety Management Code and a safety culture
An interim International Safety Management Code (ISM) certificate had been issued only two months prior to the incident, providing a six-month period to allow full compliance with the code. Although the vessel possessed valid ISM certificates, there were several examples where the code or the intent of the code was not adhered to at the time of the accident. These include:
- Non-Adherence to Minimum Safe Manning Criteria. At the best of times, transiting the St. Lawrence Seaway, with its numerous lockage manoeuvres, is a demanding endeavour for the deck crew. Consequently, a vessel should always have its full complement during Seaway transit. Vessels can receive exemptions from the flag state to operate under the required minimum for short periods of time. This is an accepted practice and reflects operational realities. The Kent, although not operating under an exemption at the time of the accident, had five deck ratings and was, therefore, one person short of the required number at that time. Furthermore, the fifth deck-rated crew member had been assigned to engine-room duties, which left all deck duties for normal operations to be accomplished by the four remaining deck ratings. Although this practice does not contravene flag state rules, when combined with the already reduced crewing level, it effectively resulted in the vessel operating with two fewer deck ratings than the minimum specified in the MSM certificate in force at the time of the accident (or one fewer than the new MSM approved by the flag state on 30 July 2002). Any reductions below the minimum complement in one crew sector will adversely affect the rest periods of the remaining complement in that sector, leaving them susceptible to fatigue during intensive operations such as the successive locking and unlocking during a Seaway transit.
- Fatigue Awareness and Countermeasures. Although the company's safety and training manual gives great detail as to the effects of fatigue, no guidance is offered on how to realistically avoid fatigue given the intense operational pressures of Seaway transit and regular port-of-call duties - particularly in light of the fewer-than-minimum number of deck crew assigned. In the 24 hours preceding the accident, the bosun had approximately four hours off duty, and his judgment, reaction time and alertness would have been adversely affected by fatigue.
- Repairs by Unqualified Personnel. The operation managers instructed the master to undertake repairs on the port davit using on-board resources while under way, in an attempt to avoid delaying the voyage by stopping for in-port repairs. When repairs to a specialized piece of equipment on a vessel are required, the manufacturer (or its representative) ought to be consulted as to the appropriate repairs/replacements required to restore the unit to its original state. Only special shore-based repair facilities have the equipment and skilled tradesmen to perform such work. In this case, without the precise alignment of the port davit cradle roller track and built-in sheave assembly, the efficient operation of the running rigging and roller gravity davits could not be guaranteed.
- Use of Non-Approved Equipment. The port davit and lifeboat were temporarily excluded from use as lifesaving equipment by DNV, until the davit could be repaired satisfactorily. Nevertheless, the master insisted, at Montréal, that the defective port davit be tested by the crew for possible use in an emergency.
Taken individually, each of the above examples did not directly contribute to the accident. Taken collectively, however, they can be considered to have appreciably increased the risk on board the Kent.
Findings
Findings as to causes and contributing factors
- The gap between the safety pin and its brake release lever, and the less-than-adequate maintenance on the brake-lever mechanism, contributed to the unexpected release of the lifeboat down the davit cradle.
- The wire rope used as the lashing line was in a severe state of corrosion and well beyond a serviceable state.
- The davit cradle ladder rungs were located in very close proximity to the faulty winch brake lever, and as the seaman descended the aft davit cradle, he probably stepped on the winch brake lever extension, instead of the ladder rung, and released the lifeboat.
- The ladder rungs only provided vertical access at the extreme outboard end of the davit cradle, compelling personnel to place themselves in a dangerous position on the inclined portion of the davit roller track when securing the lifeboat.
- With the davit winch brake disengaged, the corroded lashing line failed to hold the weight of the port gravity davits and the suspended lifeboat, allowing the assembly to slide down the davit cradle, knocking the bosun overboard.
Findings as to risk
- The vessel Kent was operating with fewer than the minimum number of deck ratings required by the Minimum Safe Manning (MSM) certificate. Additionally, the practice of assigning ratings to duties other than those described in the MSM certificate undermines the criteria under which the MSM was issued.
- In the 24 hours preceding the accident, the bosun only had four hours off duty, and his judgment, reaction time and alertness would have been adversely affected by fatigue.
- The operating managers elected to have the crew attempt repairs on the port davit while under way to avoid delaying the voyage, rather than ensuring classification approval by having a specialized shore-based facility precisely re-align the port davit and restore it to its original state.
Other findings
- The master insisted on using equipment that was neither safe nor class approved.
Safety action
Action taken
The operating managers sent a fleet-training superintendent on board to analyze the accident and carry out corrective training. Subsequent to this visit, certain design features of the lifeboat davits were modified, including the following:
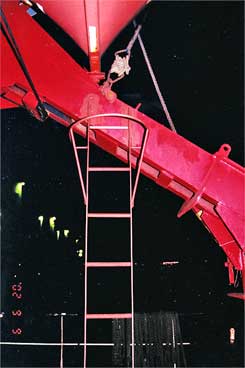
- Permanent vertical ladders were installed under and beside the securing point of the trigger lines, thus giving direct but protected access to the trigger-line securing arrangement (see Photo 6). The existing cradle arm ladders were removed.
- Clearance between the winch brake release lever and its safety pin was removed, so that the lever cannot be moved when the pin is in place.
- Working procedures were established that require the lowering, recovery and securing of the lifeboat to be done with at least two persons and an officer present.
- A report of the incident was promulgated fleet-wide to provide information and stimulate feedback.
The operating managers are in the process of amending the personnel recruitment section of the International Safety Management (ISM) manuals, so that particular attention is paid to crewing levels in relation to the MSM requirements of the flag state. The TSB is unaware of the actual state of these procedural modifications at this time.
Safety concern
Minimum safe manning
The issuance of a new MSM certificate by the flag state affirmed that the Kent had a full complement of qualified crew on board. The certificate included a minimum requirement of five deck ratings (previously assessed at six). However, one of the deck crew who had dual certified ratings was assigned to the engine room, leaving the remaining deck crew of four effectively understaffed. While the practice of re-deploying dual certified crew from one department to another does not contravene flag state rules, if such a practice has the effect of reducing one department below its specified number, it can have a serious impact on the safe operation of a vessel. This contradicts the fundamental premise under which an MSM certificate is issued.
Flag states are responsible for evaluating and approving proposals submitted by vessel operators for establishing the minimum number of crew required for a particular vessel. International Maritime Organization (IMO) Resolution A890 (21), Principles of Safe Manning, is used to establish this number. However, there are no standard methods or formulae provided for actually quantifying the crew required. Nevertheless, a flag state must make a critical and objective assessment of crewing proposals for each particular ship with a given operational envelope.
IMO Resolution A890 (21), Principles of Safe Manning, addresses statutory provisions, performance factors and on-board functions that should be taken into account during the assessment process. However, these principles and guidelines provide only a qualitative reference. In other industries, systems engineering methods have been used to quantify personnel needs. However, this methodology is not part of the IMO Resolution.
Port states regard compliance with the MSM certificate as evidence that vessels are safely staffed and that the use and deployment of the personnel listed will be as described therein.
The St. Lawrence Seaway Management Corporation, in its Seaway Notice No. 3-2004, mentions that vessels accepted with minimum crew must participate in the tie-up service with well-rested crew members. However, this is contingent upon the minimum crew being departmentally assigned in accordance with the MSM certificate.
The TSB is concerned that the IMO's Principles of Safe Manning do not provide sufficient rigour to the process of providing guidelines for the determination of proper ship crew size and the description of crew members' duties.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .
Appendices
Appendix A - Approximate location of occurrence
Appendix B - Glossary
- BHP
- brake horsepower
- C
- Celsius
- cm
- centimetre
- m
- metre
- COC
- condition of class
- DNV
- Det Norske Veritas
- HK
- Hong Kong
- HKMD
- Hong Kong Marine Department
- IMO
- International Maritime Organization
- ISM
- International Safety Management Code
- MAIB
- Marine Accident Investigation Branch
- mm
- millimetre
- MSC
- Maritime Safety Committee
- MSM
- Minimum Safe Manning
- T
- True
- TC
- Transport Canada
- TSB
- Transportation Safety Board of Canada
- U.K.
- United Kingdom
- °
- degree