Striking
Passenger vessel Nordik Express
Entrée Island, Harrington Harbour, Quebec
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
At 2303 eastern daylight time on 16 August 2007, in darkness and good weather, the passenger vessel Nordik Express struck Entrée Island while approaching the entrance to Harrington Harbour. The vessel sustained severe damage, water ingress, and quickly developed a starboard list. After the vessel was brought alongside the dock, the 156 passengers disembarked. There was no pollution and no one was injured.
Factual information
Particulars of the vessel
| Name of vessel | Nordik Express |
|---|---|
| Official number | 364084 |
| Port of registry | Québec, Quebec |
| Flag | Canada |
| Type | Passenger vessel |
| Gross tonnage | 1748 |
| Registered lengthFootnote 1 | 64.91 m |
| DraughtFootnote 2 | Forward: 4.1 m Aft: 4.2 m |
| Built | 1974, Seattle, Washington, United States |
| Propulsion | Two General Motors diesel engines, totalling 5369 kW, driving two controllable-pitch propellers |
| Cargo | 146.6 tonnes (containers and vehicles) |
| Crew | Rated: 24 On board: 25 |
| Passengers | Rated: 268 On board: 156 |
| Registered owner | Transport Desgagnés, Inc. |
| Manager | Relais Nordik, Inc. |
Description of the vessel
The Nordik Express is registered as a passenger vessel with a capacity of 268 passengers, including 72 passenger berths. The vessel also carries general cargo and has a container capacity of 60 TEU.Footnote 3 It was constructed in 1974 as an offshore supply vessel and was modified by a new owner in 1987 to carry passengers and containerized general cargo along the lower north shore of the Gulf of St. Lawrence. Further modifications in 2001 gave the vessel its present configuration (see Photo 1 and Appendix A).

The Nordik Express is built of steel and has a lower deck, a main deck, an upper deck, a bridge deck, and an observatory deck (Decks A through E, respectively). Passenger cabins are located on the lower, main, and bridge decks.
The bridge was equipped with several consoles. One was located approximately on the centreline and forward against the front bridge windows, and contained the autopilot and helm. A console in each wing contained engine, rudder, and bow thruster controls. Two radars and the electronic chart system (ECS) were located between the port and centreline consoles. A third radar was to starboard of the centreline console (see Photo 2).

Neither the radars nor the ECS could be monitored without leaving the helm.
The vessel was not equipped with a voyage data recorder (VDR), nor was one required by regulation.
History of the voyage
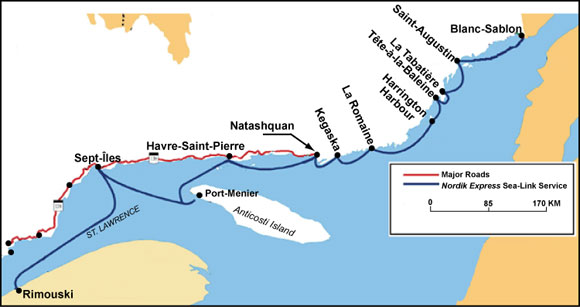
On 14 August 2007 at about 1200,Footnote 4 the Nordik Express left Rimouski, Quebec, on a weekly scheduled run to Anticosti Island and ports of call on the lower north shore of the Gulf of St. Lawrence (see Appendix B). Forty-one passengers were on board, the majority in berthed cabins. The vessel was also loaded with 111.8 tonnes of cargo, consisting of containers and vehicles.
On August 15 and 16, the vessel made six scheduled port calls where various quantities of cargo were loaded or unloaded and passengers embarked and disembarked (see Appendix C for further details). At 1805 on August 16, the Nordik Express left La Romaine, Quebec, bound for Harrington Harbour, Quebec, with 156 passengers and 146.6 tonnes of cargo.Footnote 5
Before retiring to his cabin at about 2000, the master asked the third officer, who was the officer of the watch (OOW), to call him 30 minutes before arrival at Harrington Harbour. The bridge watch thereafter consisted of the OOW, who was following the vessel's position with both the radar and ECS as well as visual cues, and the helmsman, who was acting as lookout while the vessel was on autopilot.
The seas were calm, winds were from the southeast at between 10 and 15 knots, and visibility was very good.
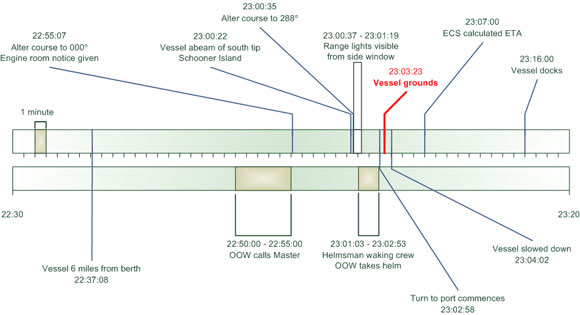
At 2255, with the vessel making way south of Cape Island on a heading of approximately 049° gyro (G)Footnote 6 and at a speed of 12.3 knots, the OOW initiated the planned course change to 000°. Also at this time or shortly before, the OOW phoned the master and informed him that the vessel was 30 minutes from arrival at the dock. The OOW then called the engine room to place them on standby, at which point an extra generator was put on line and a second steering pump and bow thruster were started in preparation for manoeuvres into berth.
The vessel proceeded on a northerly courseFootnote 7 for approximately five minutes before the autopilot was disengaged, the helmsman took the helm, and at 2300:35 near waypoint 11, a course change to 288° was initiated on the order of the OOW.Footnote 8 Almost immediately thereafter, the bridge team realized that the docking crew needed to be on deck/available prior to arrival, but had not yet been called. The OOW therefore hurriedly sent the helmsman below to call them and took the helm.Footnote 9
This left the OOW alone on the bridge and steering the vessel as it completed the turn. The OOW, who found the helm movements difficult to manage, oversteered the intended course to 280.4°, after which it took him approximately one minute to bring the vessel back to a course of 288° by making multiple small helm adjustments. During this time, the flashing light marking the cliffs of Entrée Island would have been visible from the conning position.
At about 2303, or approximately two minutes after leaving, the helmsman returned to the bridge. The vessel, back on its heading of 288°, was still full ahead and making way at 11.7 knots;Footnote 10 its actual track, however, was offset to the northeast, parallel to the intended track (see Figure 1).
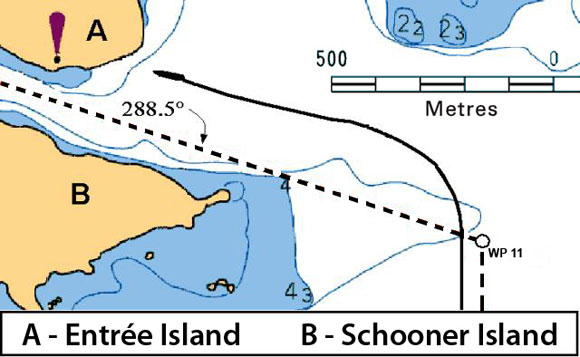
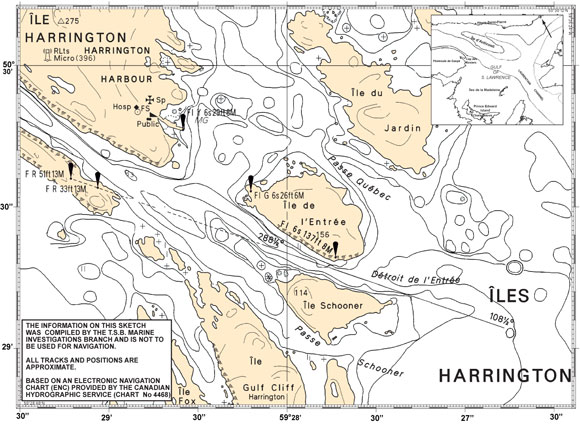
The OOW ordered the helmsman to quickly take the helm, approached the electronic chart, and gave the order to steer 270°. At about the same time, the helmsman saw a rock cliff directly in front of the vessel and applied 20° of port rudder. As the vessel began to turn, it struck Entrée Island at position 50°29.3′ N, 059°27.6′ W at about 2303:30.
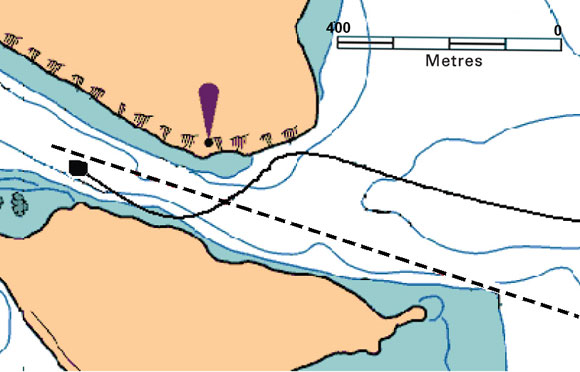
After striking Entrée Island, the vessel crossed the narrow passage, almost grounding on Schooner Island. The helmsman then saw the harbour's leading lights ahead and began to steer the vessel into the middle of the passage (see Figure 2).
The master, who was in the washroom, felt the impact of the striking and rushed to the bridge, followed shortly thereafter by the second officer (2/O), who had been asleep in his cabin.
The master reduced speed to slow ahead while the 2/O took the con. When the vessel was off the berth, the master took the con and manoeuvred it alongside, where it docked at 2316. Shortly after, all 156 passengers disembarked with no injuries.
Within minutes of the striking and as a result of damage below the waterline, the vessel developed a list of approximately 20° to starboard; however, by the time it reached its berth, this was reportedly less than 10°. For a graphic depiction of the occurrence timeline, refer to Appendix E.
Events following the striking
The impact and the listing to starboard roused most passengers and crew; some of the crew began instructing berthed passengers on the lower decks to go to the main salon. Some passenger cabins were checked at this time.
People had difficulty moving in the crowded corridors and climbing the stairs with the vessel in its listed condition, and there was a strong smell of smoke or burning. This smell was most likely the result of slippage and overheating in the clutch of the starboard reduction gear after the propeller struck the bedrock.

Passenger-care crew members, having neither received any information from the bridge nor having sought clarification, were unable to answer passenger questions regarding the situation. Engine room crew attempted to call the bridge, but received no response.
Within minutes, passengers were assembling on the observatory deck (Deck E). Some berthed passengers wore lifejackets; others, still uninformed as to the nature of the emergency, arrived without their lifejackets–some in pyjamas and bare feet. Distribution of lifejackets was done by crew and passengers from the deck storage box just outside the main salon. Lacking clear directions from crew members, only some passengers donned their lifejackets. Some young children were given adult-sized lifejackets. Although some passengers were initially anxious, once the lights of Harrington Harbour came into view, the situation became calmer.
After the vessel docked, it was discovered that two passengers–one of whom had reduced mobility–had remained in their cabin on Deck D. Passengers then disembarked and the crew searched the vessel for any remaining passengers.
During the night, in consultation with office staff, the crew carried out an assessment of the damage, with ballasting operations conducted to bring the vessel upright. Considering the extent of the damage, however, which exceeded the scenarios found in the vessel's stability book, a precise assessment could not readily be made. At approximately 0215 on 17 August 2007, crew and passengers were permitted to re-board.
The same day, the managing company dispatched two employees to help with the emergency; a naval architect was also hired to determine the vessel's safety and to plan unloading operations. These damage stability calculations were sent to the vessel by 1454 that afternoon, informing the crew of the actual stability of the vessel in its damaged condition.
Damage to the vessel
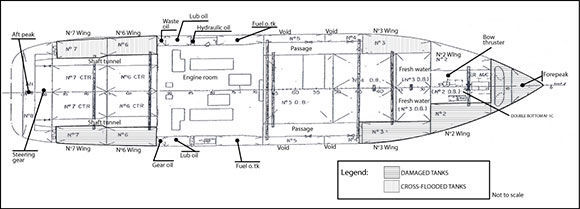
The vessel sustained heavy damage on the starboard side near the bow, quarter, and starboard propeller. The forepeak tank, double-bottom tank No. 1C, as well as starboard tank Nos. 2, 3, 6, and 7, were breached and took on water (see Appendix F). This flooded the Nos. 3, 6, and 7 tanks on the port side by means of the cross-flooding pipes.
Vessel certification
The Nordik Express is a non-Convention passenger shipFootnote 11 and is subject to regular inspection by Transport Canada (TC). It was last issued an annual inspection certificate on 31 March 2007. Relais Nordik, Inc. had no formal safety management system (SMS) in place, nor was one required by regulation.
Crew certification, experience, and familiarization
The master held a certificate of competency valid for the type of vessel and the class of voyage being undertaken.Footnote 12 He had 34 years of seagoing experience, approximately the last 16 of which were as master on various vessels. He joined the Nordik Express in the spring of 2007, spending the first three weeks "doubled up"Footnote 13 with a master experienced in navigating the lower north shore of the Gulf of St. Lawrence. Since that time, the master followed a schedule of "six weeks on/three weeks off" as primary master.
The OOW's certificate of competencyFootnote 14 was also appropriate for the type of vessel and class of voyage being undertaken. He completed his marine training in 1982 and had served as both OOW and master for various companies, including as master on a passenger vessel similar in size to the Nordik Express. The master had known the OOW from previous work experience in the Caribbean. The OOW had worked on the lower north shore of the Gulf of St. Lawrence several years previously, serving a total of five months aboard other vessels in that area.
Before joining the Nordik Express on 07 August 2007, the OOW was informed that he would undergo a 21-day training/work period with the goal of eventually serving as first officer (1/O) on the "six weeks on/three weeks off" regime. The schedule was as follows:
- Week 1: double-up with an experienced OOW (third officer or 3/0) to become familiar with the pilotage aspects of port approaches and vessel routine
- Weeks 2 to 3: serve on vessel as 3/O
The occurrence took place on day three of week 2.
During the first week of his familiarization period, rather than following the watch schedule of the 3/O, the OOW was called to the bridge for each port arrival and departure (15 or 20 minutes before the master) so that he could be briefed, observe and participate, as practical, in the routine for each port approach/departure. As such, he had observed one entry into Harrington Harbour, from the west, before the occurrence. During this time, his hands-on experience with the helm controls was limited.
The helmsman, who had been on the Nordik Express as seaman and helmsman since 1991, had a Bridge Watch Rating certificate of competency. He was also on the primary crew adhering to the regime of "six weeks on/three weeks off."
Bridge procedures for arrivals/departures
The practice for arrivals was for the officer and helmsman on duty to serve as the bridge team, with the master joining them during the approach to assist in the navigation and to accomplish the manoeuvre to berth. A collection of informal "pilotage" notesFootnote 15 was in use on board the vessel and contained specific details for approaches to each port.
For Harrington Harbour, the instructions consisted of a list of typed notes giving courses to steer, course alteration points, and parallel index line settings. These notes, including various handwritten modifications, bore no indication of having been endorsed by senior officers, nor did they include information about the speeds to maintain or the persons to notify (and when) with respect to an imminent port arrival. Onboard practice, however, indicated that it was not uncommon to reduce speed during the approach, and that the timing of the notification of the master was at the master's discretion. The timing of other notifications (such as engine room and docking crew) was learned during familiarization.
Deck watch requirements
The Marine Personnel Regulations specify the number of bridge team members required for a deck watch. At the time of the occurrence, the Nordik Express required an appropriately certified OOW, as well as an appropriately certified additional person and a second additional person.Footnote 16
Under conditions where automatic steering is not prohibited, the regulations do not require the second additional person, provided that specified equipment and facilitiesFootnote 17 have been fitted on or adjacent to the bridge that allow the remaining two crew members to fulfill the three key roles of OOW, helmsman, and lookout. The Nordik Express did not meet all the conditions to be eligible for this.
Electronic Chart System
The bridge of the Nordik Express was fitted, on a voluntary basis, with an ECS. ECS is a navigation information system that electronically displays real-time vessel position and relevant nautical chart dataFootnote 18 as it interfaces with other navigational equipment.Footnote 19 ECS can also provide alerts and prompts for track monitoring, planned course alterations, and other navigation and safety features. These can include cross-track error (XTE) alarms, which are activated when a vessel leaves the course line's set parameters. When vector charts are used, a navigation-danger alarm may be set up that establishes a cone or radius of navigation danger centred on the ship's position. This area is then constantly checked for any dangers that have been pre-determined by the user.
During a voyage, an ECS also maintains a recorded log of data that interfaces with the system and some, but not all, actions. These may be actions undertaken automatically by the ECS or manually by an operator. The ECS log file from the Nordik Express indicated that the last chart loaded before the occurrence was raster chart CHS 446802-Harrington Harbour (Canadian Hydrographic Service).
Furthermore, it indicated that
- the XTE alarm, the only alarm available with a raster chart loaded, had not been set for this, and other, routes;
- the alarm sound was turned off;
- the anti-grounding feature was turned off (it would not have functioned in this case because the chart in use was a raster chart); and
- no alarms were registered before the grounding.
When a raster chart is in use, the look-ahead feature alarm does not function.
Passenger safety and emergency preparedness
Passenger safety briefings
Company practice was to provide one safety briefing. Passengers who embarked at Rimouski were mustered and given a safety briefing on the various lifesaving appliances, including liferafts and lifejackets, as well as their stowage and location. These passengers were told that, in the event of an emergency, they were to assemble in the uppermost central salon. They also received a demonstration of the general alarm.
In this occurrence, 41 passengers embarked at Rimouski and received the briefing; 219 other passengers, who embarked at later ports, did not receive the briefing.Footnote 20
Accounting for passengers
Upon leaving each port, ticket stubs were counted to determine the number of passengers on board. This number was then reported to the officer on duty and entered into the deck logbook.
Each ticket stub shows a passenger's name and the price paid, making it possible to determine if the ticketholder is an adult or a child (including infants). However, there was no separate record kept as to how many adults, children, or infants were on board at any given time.
Ship staff maintained a list of passengers who had made special requests, mostly related to meal requirements, though it also included some information on physical disabilities. There was no dedicated list on board containing information regarding passengers who would require special assistance in the event of an emergency.
Emergency procedures
A muster duty list was posted on board describing the general alarm signal and advising the crew of general emergency duties to be carried out when it sounded. With a crew complement of 25 (as on the night of the occurrence), the passenger-care crew consisted of 10 crew members: one in charge of assembling passengers, two to distribute lifejackets, and seven others assisting.
Also posted on board was an abandon ship list-again describing the signal for the abandon ship order and then assigning duties to each position. These duties were related to boarding the liferafts and boats and evacuating the vessel.
The company had also prepared an evacuation plan providing general information about the characteristics and use of the emergency evacuation equipment and showing the ability to evacuate the vessel within 30 minutes of the abandon ship signal as prescribed by TC regulations.Footnote 21 The plan was based on four emergency scenarios, three of which involved a fire on board and the fourth, a collision between two vessels.
The pre-evacuation phase for each scenario began with the sounding of the general alarm, and then continued to describe the various tasks to be performed by each component of the crew-bridge crew, engine room crew, firefighting crew, crew for the preparation of evacuation equipment and crew for the mustering of passengers (passenger-care crew). Among the tasks to be performed by the bridge crew were to
- establish and stay in radio contact with other crew leaders;
- establish communications with the Canadian Coast Guard; and
- stay in contact with the passenger-care crew and, as needed, reassure passengers using the intercom.
Among the tasks to be performed by the passenger-care crew were
- wake sleeping passengers;
- if needed, send someone to find missing passengers;
- communicate with the master; and
- prepare passengers to abandon ship.
Boat and fire drills that included a passenger muster were conducted each week after the vessel departed Rimouski. These commenced with the sounding of an alarm.
Passenger safety management
Training in passenger safety management has been available for over a decade. Its goal is to provide personnel with "standards for familiarization, basic safety training, and competencies to cope with such hazards and emergencies to the extent appropriate to their functions on board the vessel."Footnote 22
Subjects addressed by this training include
- principles of crowd management, crisis management, and human behaviour in emergencies;
- familiarization with lifesaving appliances and control plans;
- mustering procedures; and
- communication during emergencies.
Although not required at the time of the occurrence, none of the officers or crew of the Nordik Express had completed this training. However, TC, recognizing the importance of this training, has amended regulations such that officers and crew of non-Convention passenger vessels, such as the Nordik Express, who are responsible for passengers (either under normal conditions or in an emergency), successfully complete training in passenger safety management.Footnote 23
Safety information
Stability Book
The most recent inclining experiment for the vessel was carried out on 19 April 2001, following modification to the passenger spaces, with a new intact and damage stability book approved on 22 March 2004. A copy of this book was on board at the time of the occurrence.
The first few pages of the stability book, which is in French, include 10 "Notes to the Master."Footnote 24 These address subjects including
- stowage and securing of cargo;
- load lines;
- measures to minimize free surfaces;
- guidance regarding tank crossflooding;
- watertight doors; and
- stability in icing and snow conditions.
Crossover valve instructions
The Nordik Express is fitted with eight tank pairs, each connected by 10-inch cross-flooding pipes; these have no crossover valves, thereby automatically equalizing the level of water in the tanks in the event of damage to one side and rapidly minimizing any list. On the other hand, the connection between the No. 2 wing tanks is fitted with a crossover isolation valve. Under normal circumstances, this valve must be closed so that the tanks can serve as ballast tanks to compensate for the variable loading of cargo, ensuring that the vessel is always upright. In addition, guidance notes in the stability book describe certain damage situations where it would be recommended to keep this valve closed.
A plaque in the passageway between the master's cabin and the chief engineer's cabin states the following: [Translation]"No. 2 port and starboard wing tanks crossover isolation valve must be left open while at sea."
Watertight doors
The Nordik Express is fitted with three watertight doors, two aft of the engine room giving access to the shaft tunnels and one in way of frame 42 on the main deck. Canadian regulations state that these doors are to be kept closed during navigation except when "necessarily opened for the working of the ship."Footnote 25 The stability book's "Notes to the Master" also states that they must be closed at all times, except for "short durations" to permit passage through the door.
The practice on the Nordik Express was to operate with the watertight doors open, and they remained open following the striking.
Fatigue management
Watch system
During the first and last day and a half of each voyage, the vessel normally calls at three ports. For the middle four days, calls become more frequent. This is an extended period of intense workload for the crew, requiring passengers and cargo to be managed so as to facilitate fast turnarounds in port. Crew rotation takes place on a basis of six weeks on/three weeks off.
Excluding the master, there were three officers available to stand a deck watch on the Nordik Express. They operated with a three-watch systemFootnote 26 for the first and last portion of the trip, and a two-watch systemFootnote 27 for the middle section.Footnote 28 This allowed the 1/O to attend cargo operations on an as-needed basis instead of standing watch. The two-watch system was in use at the time of the occurrence. This watch system formed part of the collective agreement with the officers.
The master was not part of the watch rotation; instead, he joined the bridge team at each arrival and departure, in addition to attending to the other duties of his position.
Hours of rest and fatigue
The OOW's sleep history for the full 72-hour period before the occurrence was not available. However, it is known that he was awake at every port during his first week on the vessel in order to be shown docking procedures and obtained 3.5 hours of sleep in each of the two six-hour rest periods in the 24 hours before the accident. The OOW experienced feelings of extreme fatigue during the initial familiarization week. He took sleeping pillsFootnote 29 to try to ensure that he fell asleep quickly.
A review of both the master's 36-hour sleep history before the occurrence and the ship's schedule indicates that, for the first and last day and a half of each voyage, the schedule allowed him to obtain a total of about eight hours of sleep per day-most of it at night, but with supplemental daytime naps when possible. The schedule for the intervening four days of the voyage reduced the opportunity for total hours and duration of rest periods.
Restorative sleep
It has been shown that, in order for sleep to be fully restorative, it should optimally be obtained in periods of at least seven to eight continuous hours.Footnote 30 The total sleep time may be broken into shorter periods and be restorative–for instance, four hours during a first rest period and four hours during a second rest period. Schedules where rest is broken, such as six on/six off or four on/eight off schedules, can be adequate provided that crew members do obtain sufficient uninterrupted restorative sleep during the allotted rest periods.
However, split rest periods provide several challenges to obtaining restorative sleep. Should one of the periods occur during the crew members' normal "daytime" period, it would be less restorative.Footnote 31 Moreover, breaking a rest period into a number of sections can result in increased sleepiness and decreased performance.Footnote 32 A more general challenge to obtaining sleep across short rest periods is the risk that meals, personal chores, and unscheduled interruptions may prevent the crew member from obtaining the required amount of sleep in the time available. In addition, when schedules are changed, for instance from four/eight hours to six/six hours, there is an accommodation period in which an individual is likely to be fatigued until he or she adjusts to the new schedule.
Fatigue management
The effects of fatigue include increased risk taking, the inability to solve problems in parallel, and persisting with tasks beyond a reasonable end point, all of which may pose serious risks to safety if experienced by personnel in responsible positions. Fatigue management responsibilities require both the company and employees to manage the schedule, health, and environment of crew members to minimize the risk of fatigue. The company is responsible for ensuring that crew schedules, at minimum, meet regulations for rest,Footnote 33 that the schedule allows for sufficient restorative sleep to be obtained, and that the crew quarters and other aspects of their environment facilitate healthy rest. Crew members are responsible for following the rest schedule and reporting when they are unfit to work due to fatigue and whether there are aspects of the company's fatigue management plan that are deficient. A vessel's master is responsible for monitoring and enforcing the company's fatigue management policies and procedures and for working with crew and the company to rectify problems so as to minimize the risk of fatigue.
The vessel's managing company did not have a fatigue management plan, nor was one required by regulation.
Lorazepam
The investigation revealed that the OOW took Lorazepam, which had been prescribed for someone else, to try to fall asleep quickly and obtain sufficient sleep before his next watch. This drug is used to treat anxiety disorders and insomnia due to anxiety or transient situational stress. Its main side effect is drowsiness. Lorazepam affects the central nervous system and patients are cautioned that the medication may impair mental or physical abilities required for the performance of potentially hazardous tasks requiring mental alertness, such as operating a motor vehicle or machinery. The half-life of Lorazepam is 12 to 18 hours.Footnote 34
The taking of the medication was not disclosed to the master as required by the company policy relating to alcohol and drugs.
Analysis
Events leading to the striking
Notification of master
The master instructed the OOW to notify him 30 minutes before arrival at Harrington Harbour. At the sailing speed of approximately 12 knots, this would have meant calling when the vessel was approximately six nautical miles (nm) from the dock–or about 3.7 nm southwest of Cape Airey, Cape Island (see Appendix G). On the night of the occurrence, the Nordik Express reached this point at 2237. The OOW, however, called the master at approximately 2255, when the vessel made a course change at waypoint 10 to 000°.
It could not be determined why the OOW did not call the master earlier, but at 2255, the Nordik Express was only about five minutes from initiating the critical turn at waypoint 11. The master, however, having been informed that arrival was 30 minutes away, was not yet on the bridge when that turn was started nor when the vessel struck Entrée Island approximately 3 to 4 minutes later.
Turn at waypoint 11
According to the pilotage notes, the course change at waypoint 11 was to be initiated when the southern tip of Schooner Island bore 270°. The vessel reached this point at 2300:24. As the vessel continued toward waypoint 11, the autopilot was disengaged and the OOW ordered the helmsman to apply 10° port rudder, resulting in the vessel turning at 2300:37-approximately 80 m (13 seconds) past the point specified in the notes.
After the bridge team realized that the docking crew had not been alerted of the vessel's imminent arrival, the OOW sent the helmsman below and took the helm. With the vessel still turning, the OOW, alone on the bridge, overshot the required course to 280.4°. Focusing on the helm control, it then took him approximately a minute to bring the vessel back to 288°, the course specified in the pilotage notes.
This late start to the turn, combined with minor disruptions to the rate of turn when handing over the helm, resulted in the vessel passing beyond the visible range of the harbour's leading lights.Footnote 35 Although the OOW would normally be able to verify the vessel's course and position by radar or ECS, he was alone on the bridge and unable to see either of these from his position at the helm, nor did he benefit from the visual cue offered by the navigation light on Entrée Island. The Nordik Express thus progressed along its track, offset northeast and parallel to its intended route, but with its position unchecked.Footnote 36
It was not until the helmsman returned that the OOW approached the ECS/radar and ordered a course change to 270°. Shortly thereafter, the helmsman saw the cliff face of Entrée Island, but the 20° of port helm he immediately applied was insufficient to avert the striking.
Procedures for arrivals/departures
Navigation in restricted waters involves narrow margins where even minor deviations from the intended track can have significant consequences. In this occurrence, an initial deviation of approximately 80 m (13 seconds) combined with minor disruptions to the rate of turn were sufficient to create an XTE distance of 100 m–putting the vessel on a course directly toward an island.
A vessel's procedures for navigating in restricted waters, therefore, must be precise and, moreover, they must be followed.
In this occurrence, the verbal order given to the OOW to call the master 30 minutes before arrival at Harrington Harbour was not accompanied by a visual reminder such as a mark on the chart or the ECS. In addition, there were no written standing orders for port arrivals, and although there were informal pilotage notes and a planned route on the ECS, key points were not identified. These included
- abort points;
- where to notify engine room staff;
- where to call the docking crew; and
- no-go areas.
Furthermore, there was no indication that either the pilotage notes, or the subsequent modifications to them, had been endorsed by senior officers.
The absence of sufficiently detailed procedures left the OOW without an important resource to assist him in accomplishing the numerous precise tasks involved in the approach, thereby contributing to this occurrence.
Deck watch
A deck watch composition is based on the various tasks that need to be performed. These can be described in three main categories: navigation, maintaining a lookout, and steering. Under conditions where hand steering is required, a deck watch would need to consist of three persons. However, TC recognises that, under some circumstances where automatic steering is not prohibited and where the appropriate equipment and facilities are fitted, two persons can safely fulfill the tasks of conning the vessel. In addition to the minimum deck watch, industry best practices dictate that the master be present on the bridge during manoeuvring.
Established practice on the Nordik Express was for the deck watch to consist of two bridge team members when using autopilot, with the master joining them for arrivals and departures. This arrangement, however, was insufficient given the lack of the appropriate vessel equipment and facilities.Footnote 37 The standard for safe deck watch composition meant that a second additional person was required.
Consequently, when the helmsman was sent to summon the docking crew, the OOW was left alone at a critical point in the voyage to perform all the necessary tasks.
Passenger safety and emergency preparedness
Notification of emergency
During an emergency, the safety of those on board a vessel is dependent upon prompt and appropriate action by those crew members assigned to perform passenger safety-related duties. These duties are carried out under the guidance of the bridge team, which is responsible for overall management of emergency response and ensuring that passengers are prepared for a possible evacuation. It is therefore the responsibility of the master or bridge team to first assess the situation and to determine the appropriate level of response. Only then can crew be directed what to do, and passengers be informed as appropriate-preferably in accordance with pre-established procedures.
In this occurrence, however, bridge crew focused all their attention after the striking on conning the vessel to the dock. They did not transmit an urgency or distress call, nor was an alarm sounded or any other communication made from the bridge to the passengers or crew members. Moreover, calls to the bridge from the engine room crew were unanswered.
Crew members' response, therefore, was improvised and a number of shortcomings were observed:
- The crew did not ensure that passengers arrived at the muster station in an appropriate state of dress for a possible evacuation.
- There was no systematic search of passenger cabins.
- There was no count taken of passengers at the muster station.
- The crew did not seek guidance/instruction from the bridge.
- Passengers were not provided information about the situation.
- The distribution of lifejackets was disorganized.
Given that previous training and drills, as well as written emergency plans, always commenced with the sounding of an alarm, the lack of an alarm likely caused confusion as to how to react, thereby playing a key role in the aforementioned shortcomings. In addition, the lack of an alarm precluded the heightened mental and physical preparedness that could save crucial time in the event that the unpredictable situation took a turn for the worse.
Passengers, meanwhile, having received little information regarding the emergency and what was expected of them, displayed signs of confusion and anxiety. Literature concerning human behaviour in emergencies indicates that anxiety and stress in a crowd increase when people are not provided with information. Combined with physical indications of danger-such as loud noise, the sensation of impact, the smell of smoke, and the list of a vessel-the risk of counterproductive behaviour or panic is increased.
Contingency planning
In an emergency situation, decisions are made and actions are taken in an environment involving stress and heavy task load and where experience is limited.Footnote 38 While it is understood that emergencies never evolve according to a plan, procedures can nonetheless provide a framework to guide the actions and decision making of the crew. However, to be useful, such procedures must be comprehensive and well practised.
In this occurrence, the vessel had no contingency plans in place specifically for a vessel striking or grounding. Furthermore, the posted duty lists that did relate to emergencies (for example, the muster list and the abandon-ship list) were insufficient in that they did not address the preparatory stages of an evacuation relating to, for example, searching and accounting for passengers. Although the vessel evacuation plan contained some general guidance regarding the preparation of passengers, certain key tasks were not clearly identified as belonging to the pre-evacuation phase (such as conducting a passenger count). Furthermore, it did not specify who was responsible for carrying out each task, nor did it provide any detail of how to carry out the tasks-for example, how to clear the cabins or determine if passengers were missing.
Previous TSB reportsFootnote 39 have identified shortcomings in contingency planning, particularly with respect to the preparation phases of passenger vessel abandonment. Given the risks associated with improperly coordinated preparations for evacuating large numbers of passengers, the Board recommended that
The Department of Transport establish criteria, including the requirement for realistic exercises, against which operators of passenger vessels can evaluate the preparedness of their crews to effectively manage passengers during an emergency.
Transportation Safety Recommendation M08-02 (issued March 2008)
As part of its response, TC referred to proposed amendments to the Fire and Boat Drill RegulationsFootnote 40 that would expand the list of duties for practice muster and drills to include aspects of searching and accounting for passengers. In addition, masters would be required to ensure that drills, insofar as is feasible, are carried out as if they were an actual emergency.
Recognizing the positive intent of these proposed amendments, the Board has assessed the TC response to the recommendation to be Satisfactory Intent.
Passenger safety management training
In addition to comprehensive procedures, crews of passenger vessels must be competent with respect to the performance of their duties as well as the principles of crowd management, crisis management, and human behaviour in emergencies.
Passenger safety management training addresses this and a range of other topics related to the care of passengers during emergency situations. Some of these would have specifically addressed observed/noted shortcomings of the passenger-care crew in this occurrence, such as
- establishing and maintaining effective communications;
- safe embarkation/disembarkation of disabled persons and persons needing assistance;
- organizing a search of accommodation spaces;
- accounting for passengers; and
- ensuring that passengers are suitably clothed and have donned their lifejackets correctly.
Although TC currently recognizes the need for such training for crews of Convention vessels, similar requirements for crews of non-Convention vesselsFootnote 41 will not come into force until November 2011. Until crews have completed this training, however, passengers will continue to be at risk.
Accounting for passengers
A full accounting of passengers and crew at an early stage in an emergency provides responders with critical information as to whether a detailed search is necessary. If so, it can provide insight as to where to begin that search, thus optimizing the use of resources.
In this occurrence, a basic passenger count was not performed until some time after the vessel had docked. It was not until two passengers-one of whom had reduced mobility-emerged from their cabin that the crew would have been aware that not all passengers had been mustered from their cabins. Passenger information that could have been useful to responders, therefore, such as the number of adults, children, and infants, as well as the identification of passengers requiring assistance, was not readily available.
The Board believes that the approach to accounting for passengers must be tailored for each individual vessel in order to address the potential risks of a particular voyage and the most appropriate means of addressing them. It therefore recommended that
The Department of Transport, in conjunction with the Canadian Ferry Operators Association and the Canadian Coast Guard, develop, through a risk-based approach, a framework that ferry operators can use to develop effective passenger accounting for each vessel and route.
Transportation Safety Recommendation M08-01 (issued March 2008)
In response, TC referred to discussions held with the Canadian Ferry Operators Association (CFOA) in relation to the Board recommendation as well as an initiative of the Canadian Coast Guard to develop a system to track and account for all casualties involved in a major marine incident. Furthermore, TC referred to the proposed amendments to the Boat and Fire Drill Regulations, which would make mandatory the various provisions regarding passenger information that were formerly recommended for voluntary early implementation.Footnote 42 These provisions refer to the type of passenger information to be recorded, the updating of that information, and its availability.
Considering that the full implementation of these proposed regulations would significantly reduce the risks to fare-paying passengers, the TC response to the Board recommendation has been assessed as Satisfactory Intent. However, as long as these important measures remain voluntary, passenger-carrying vessels may operate without this information, thereby placing passengers at undue risk.
Passenger safety briefings
It is vital that all passengers be provided with key safety information–through in-person briefings or some other method of transmitting critical safety information–so that they are aware of what can occur and what actions to take in the event of an emergency. The value of this is reflected in both Canadian and international regulations.Footnote 43
It was the practice on the Nordik Express that only those passengers embarking at Rimouski were given safety briefings; those who embarked at the next 20 stops were not. This deprived them of key safety information and thus placed them at increased risk.
Vessel stability information
Vessel stability information–including the "Notes to the Master," as well as posted instructions regarding the use of the crossover valve for ballast wing tanks No. 2–was available in French only. Such an arrangement may leave some masters/officers unable to understand important information.
In addition, in most operational conditions, the crossover valve for wing tanks No. 2 must be closed in order to use these tanks for ballast and to comply with the conditions in the stability book. The posted instructions, however, stated that the valve must be kept open while at sea. This contradicted onboard practice and presented crew members with conflicting information.
Watertight doors
The subdivision of passenger vessel hulls into watertight compartments is a fundamental principle of design intended to improve survivability should a vessel sustain damage below the waterline. Although it is generally accepted that the operations of the ship may require doorways to be fitted in some of these bulkheads, these doors must be of special watertight construction and must be closed to realize the benefits of the watertight subdivisions.
The Nordik Express, however, routinely operated with all watertight doors open, contrary to both the stability book guidance and Canadian regulations, and in this occurrence, they remained open after the striking.
Following the TSB investigation into the sinking of the passenger ferry Queen of the North,Footnote 44 the Board expressed concern that "some Canadian operators continue to operate their vessels with watertight doors open, thereby placing vessels, passengers, crews, and the environment at undue risk." In response, TC noted that the Hull Construction Regulations already state that all watertight doors are to be kept closed at all times while a ship is in operation.Footnote 45 Moreover, TC noted that it has previously issued ship safety bulletins regarding watertight doorsFootnote 46 and that it plans to monitor and participate in ongoing International Maritime Organization (IMO) development of related guidelines.
It is recognized that practices and procedures related to watertight doors are situational and ship-specific, and therefore not easily regulated. However, operating with watertight doors open at all times exposes the vessel, its crew, and passengers to undue risk. It is therefore incumbent on crews and operators to carefully consider their practices and procedures in this regard to ensure that this risk is minimised.
Configuration of ECS
Modern electronic navigating equipment, including ECS units, offers bridge teams many options that can be used to plan, execute, and monitor a voyage. These include, for example, the ability to set alarms and warnings for hazardous situations. This equipment, however, must be properly configured before users can take full advantage of these features.
On the Nordik Express, no cross-track boundaries had been defined in the ECS's electronic voyage plans. Even if they had been set, however, the crew would have received no auditory warning that the vessel was outside the limits because the alarm's sound feature was turned off.
The TSB found previouslyFootnote 47 that navigation equipment not set up to take full advantage of available safety features deprived the crew of warnings and was a contributing factor in the occurrence.
It is recognized that the ECS on the Nordik Express was but one of many pieces of equipment that could have provided the bridge team with information. Furthermore, the cross-track alarm may not have served a useful purpose in this occurrence due to the very restricted waters encountered after the turn at waypoint 11. However, the configuration of the system overall was not managed to benefit fully from the alarm options available and therefore deprived the crew of a potentially useful tool to assist in safe navigation, thereby increasing risk.
Fatigue management
A fatigue management plan is a comprehensive way to ensure that crews obtain sufficient rest to be able to perform their duties. This includes not only work scheduling, but also both the management of generic factors–such as nutrition, medical health, noise around sleeping areas, prescription drugs and caffeine–and specific challenges related to each vessel and voyage.
In this occurrence, there were a number of conditions that fatigue management plans are intended to mitigate.
The 2/O and 3/O (the OOW at the time of the occurrence), for example, worked a four on/eight off schedule followed by a six/six schedule, whereas the 1/O and master followed a more irregular schedule that was determined by the vessel's arrivals and departures. Although both these schedules can allow sufficient opportunities for restorative sleep, this requires proper management: individuals require an acclimatization period to adjust to any new schedule and splitting rest periods into multiple periods throughout a day can reduce the quantity and quality of sleep.
The deck watch system aboard the Nordik Express, however, changed frequently, from a four/eight schedule for the first few days, to a six/six schedule and then back again. This constant changeover pattern would have made proper acclimatization more difficult. In the case of six/six schedules, studies have demonstrated that it is even harder to ensure enough restorative rest because there are fewer opportunities to compensate.Footnote 48 Some operators, aware of the difficulties associated with this schedule, have modified the watch system on their vessels.Footnote 49
Moreover, rest periods would likely have been interrupted every time the vessel made port; for some sections of the voyage, stops would have been frequent. Changes in engine sounds, movements around the crew quarters, and changes to the movement of the vessel would likely have had an effect on the possibility of quality sleep, in addition to those duties required for loading and unloading. More specifically, both the master and the 1/O were required to be present at every stop and, during his familiarization week, the 3/O's rest was broken at every port.
The more generic challenges to obtaining sufficient sleep include the time required to hand over watches, time required for meals and personal hygiene, and time required for ad hoc duties in addition to the normal watch schedule. Additional factors such as stress, poor health, and a noisy environment also have an impact. Although all of these can be dealt with under a proper fatigue management plan, no evidence of one was found on the Nordik Express.
The investigation identified indications of fatigue in crew members as well as behaviours likely to lead to fatigue. Moreover, the vessel's schedule was adapted to meet the company's business–frequent, rapid port turnarounds-but the effect on crew performance was not mitigated by a fatigue management plan. This increased the probability of fatigue and thus fatigue-induced errors by the bridge crew–thereby increasing the risk to vessel, crew, passengers, and the environment.
Use of sleep medication
Use of certain prescribed and over-the-counter medication can impair performance, especially with regard to judgement, reaction time, and vigilance.
The TSB has investigated occurrences where the use of medication by individuals occupying safety-sensitive positions has affected their performance. In its investigation into the striking of the bulk carrier Windoc,Footnote 50 the TSB determined that the operator of a lift bridge had been taking Darvon-N, a narcotic analgesic that acts on the central nervous system. In 2004, the high-speed passenger vessel Famille Dufour IIFootnote 51 struck a wharf, injuring nine passengers and one crew member. In its investigation, the Board determined that the master was taking prescription medication at a dosage at which TC would have likely assessed him as unfit for duty aboard a ship in a safety-sensitive position.
When a doctor prescribes a medication, it is normally accompanied by an assessment of its suitability for the person's circumstances and particular occupation, and also by guidance for its appropriate use and side effects. In this case, the OOW took medication that was not prescribed to him. As a result, no assessment of potential performance degradation was made.
The need for greater awareness of the use of medications has been recognized by the transportation industry. For example, the validity of air crew certificates is tied directly to medical condition, with crews aware of which medications preclude flying. TC has also posted guidance for operators on its websiteFootnote 52 regarding the assessment of medication use by ship's crews.
In this occurrence, the OOW was taking a medication that can impair the mental or physical abilities required for the performance of tasks requiring mental alertness. Although there is no information to indicate that his use of Lorazepam contributed to this occurrence, performance degradation as a consequence of using certain prescription medications remains a risk to vessels, crews, and passengers.
Safety management systems
A safety management system (SMS) is a tool used by both shore- and ship-based personnel to provide for safe practices in ship operation, a safe working environment, and for establishing safeguards against all identified risks, including preparation for emergencies. This is done by formally documenting policies and procedures, detailing operations, and establishing clear responsibilities for all safety-related operations. Furthermore, SMS incorporates procedures for monitoring the system itself and for taking corrective action where deficiencies are noted.
Previous TSB reports have highlighted the benefits of a properly implemented SMS.Footnote 53 TC has similarly recognized these benefits, with its Safety Management Regulations mandating SMS on Convention vessels.
In this occurrence, the following shortcomings with regard to managing safety were identified:
- Important safety information in the vessel's stability book was not available in the working language of all masters.
- The "pilotage" notes in use for port arrivals/departures were incomplete and informal.
- The composition of the deck watch was insufficient.
- The ECS was not configured to take full advantage of available safety features.
- Vessel contingency plans did not deal with all reasonably foreseeable emergencies in a comprehensive manner.
- The vessel routinely operated with watertight doors open.
- Passenger safety procedures were incomplete.
- There were no procedures to manage/monitor fatigue.
Although the vessel's operating company was not required to have an SMS for the Nordik Express, an effective SMS nonetheless helps to ensure that individuals at all levels of an organization have the knowledge and the tools to effectively manage risk, as well as the necessary information to make sound decisions in any operating condition. Effectively implemented, such a system on the Nordik Express would have provided a framework for identifying and addressing these safety issues.
Voyage data recorders
A voyage data recorder (VDR) was not carried, nor was it required by regulation. Although useful information was obtained from the ECS, it did not match the extent of information available from a VDR; for example, bridge audio. This meant the timeline (such as when the master was called) had to be approximated from less precise sources. With a VDR, the investigation would have been able to better establish the exact sequence of events leading to the accident.
This safety issue has been raised in reports worldwide, including the TSB investigation concerning the sinking of the Queen of the North.Footnote 54 In that report, the Board recommended that
The Department of Transport extend the requirement for the carriage of voyage data recorders/simplified voyage data recorders to large passenger vessels over 500 gross tonnage and all other commercial vessels on an equivalent basis to those trading internationally.
Transportation Safety Recommendation M08-03 (issued March 2008)
In response to Recommendation M08-03, TC wrote to the Canadian ferry operators in March 2008 to encourage them to voluntarily adopt this measure. Further to this, TC commissioned a study to conduct a benefit/cost analysis of potential regulatory requirements for VDRs and simplified voyage data recorders (S-VDRs) for non-Convention vessels.
This study, published in December 2008, recommended, among others, that the potential for the benefits to outweigh the costs is greatest for passenger vessels because of the number of passengers carried and the potential to save lives.Footnote 55 TC is currently in the process of preparing draft regulations that would require the carriage of VDRs on certain domestic vessels.
The TC response to the Board recommendation has been assessed as Satisfactory Intent. However, the current lack of a requirement for VDRs or S-VDRs on non-Convention vessels deprives the domestic maritime industry of a proven and valuable tool that can improve safety.
Findings
Findings as to causes and contributing factors
- The combination of the helmsman's departure from the bridge and the timing of the call to the master, giving inaccurate notification, led to the officer of the watch (OOW) being alone on the bridge during the critical turn at waypoint 11.
- The lack of a second additional person on the bridge meant that the OOW was left alone at a critical point in the voyage to perform all the necessary tasks.
- The late start to the turn, combined with minor disruptions to the rate of turn when handing over the helm, resulted in the vessel overshooting the turn at waypoint 11.
- Unable to see the harbour's leading lights once the vessel had overshot the turn, the OOW could not benefit from these navigational cues.
- The OOW did not benefit from the cue provided by the navigation light on Entrée Island and, focused on reaching the intended heading of 288°, he did not leave the helm to verify the vessel's position via either the radar or the electronic chart system (ECS). Therefore, the vessel continued unchecked along an offset track and struck the island.
- The OOW had insufficiently detailed procedures for arrivals/departures, leaving him without an important means of accomplishing the numerous precise tasks involved in the approach.
Findings as to risk
- The failure to notify those on board of an emergency situation delayed emergency response and increased the risk of counterproductive behaviour.
- Until such time as passenger safety measures regarding contingency planning, crew training, and accounting for passengers become standard practice, passengers on non-Convention vessels will continue to be at risk in the event of an emergency.
- Passengers who are not given safety briefings are deprived of key information, putting them at increased risk in the event of an emergency.
- The configuration of the ECS was not managed to benefit fully from the alarm options available and therefore deprived the crew of a potentially useful tool to assist in safe navigation, thereby increasing risk.
- In the absence of a fatigue management plan, the probability of fatigue-induced errors increases, thereby increasing the risk to vessels, crew, passengers, and the environment.
- Performance degradation as a consequence of using certain prescription medications remains a risk to vessels, crews, and passengers.
- The absence of an effective safety management system increases the risk that unsafe conditions and practices will remain unidentified and unaddressed.
- The lack of a requirement for voyage data recorders (VDRs) or simplified voyage data recorders (S-VDRs) on non-Convention vessels deprives the domestic maritime industry of a proven and valuable tool that can improve safety.
- Operating with watertight doors open at all times compromises the integrity of watertight subdivisions, thereby exposing the vessel, its crew and passengers to undue risk in the event of water ingress from below the waterline.
Other findings
- Important stability information was available only in French on the Nordik Express. Such an arrangement may leave some masters/officers unable to understand important information.
- Although the practice of closing the crossover valve for wing tanks No. 2 was necessary in order to render the vessel upright under variable conditions of loading, posted instructions were contradictory and presented crew members with conflicting information.
- Passengers were permitted to re-embark the Nordik Express following a risk assessment by the operator, but prior to a detailed analysis of the stability of the vessel.
Safety action
Action taken
Transportation Safety Board of Canada
On 05 February 2008, the TSB issued Marine Safety Advisory (MSA) 02/08, Adequacy of Operating Procedures and Practices on the Vessel Nordik Express. The advisory, addressed to the operating company, listed the safety shortcomings found on board the vessel, including the lack of passenger safety briefings at all ports, passenger information and tallies, arrival and departure procedures, watertight door operation, emergency response and evacuation procedures, and the use of a six hours on/six off watchkeeping schedule.
On 11 June 2008, the TSB issued MSA 07/08, Use of Medications by Crew in Safety-Sensitive Positions. The advisory, addressed to Transport Canada (TC), reiterated the risks posed to passengers and crew when crew in safety-sensitive positions use certain prescription or over-the-counter medications. TC was invited to raise awareness of this issue within the marine community.
Transport Canada
On 22 March 2010, TC published Ship Safety Bulletin 02/2010, which outlines the possible side effects from over-the-counter or prescription medications that are of particular concern with respect to the performance of crew members in safety-critical positions. Furthermore, it reminds seafarers of their obligation to consult with their health care professional and to avoid working while under the influence of medication having potential effects on their performance.
With respect to safety management systems (SMS) for non-Convention vessels, TC has indicated that it is currently carrying out a two-year pilot project, based in the Pacific region, which is testing SMS domestic implementation with a view to developing a SMS regulation and implementation strategy for vessels that are not required to comply with the International Safety Management (ISM) Code. Furthermore, TC indicates that it encourages all marine operators to consider voluntary compliance with the ISM Code and to proactively promote safety and environmental stewardship within their organizations.
Relais Nordik, Inc.
Relais Nordik, Inc. took the following action in response to MSA 02/08:
- Safety information is now announced in both English and French on the vessel's public address system at each port where new passengers embark. Written safety information brochures are also made available to all passengers.
- New passenger tallies and control measures have been put into effect since the 2008 season. A new list is made at each port and includes each passenger's name, age, and gender. This list is kept on board and a copy is faxed to the company headquarters.
- New procedures were instigated for arrivals and navigation in restricted waters. Pre-defined locations are now marked on navigation charts for all ports with respect to calling the master, as well as "abort points" and no-go areas. These procedures also specify minimum bridge manning levels in normal operating conditions and in restricted waters; they also indicate when the engine room needs to be on "standby."
- The vessel's voyage plans were updated to provide guidance to bridge watchkeepers. Plans now include best practices as modelled on internationally accepted reference works such as the International Chamber of Shipping's Bridge Procedure Guide and the Nautical Institute's book Bridge Team Management.
- Watertight doors are now kept closed at all times except when passage is required. An electric-assisted door operator allows a given door to be opened/closed in approximately 10 seconds.
In addition, the company took the following action:
- improvements to the lighting of certain navigation equipment to permit better visibility of the equipment in conditions of darkness;
- the installation of a washroom on the bridge;
- the installation of a telephone system permitting bridge crew to contact the crew members necessary for the operations of the ship without having to leave the bridge;
- the addition of two electronic chart system (ECS) repeaters; one close to the starboard wing console and the other in the master's cabin;
- the development of an operational guide on the inherent risks to navigation on the middle and lower north shore of the Gulf of St. Lawrence with respect to day-to-day operations and the training of new officers; and
- a requirement that all routes be entered in the ECS and that the cross-track error alarms be functional.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .
Appendices
Appendix A — Vessel layout
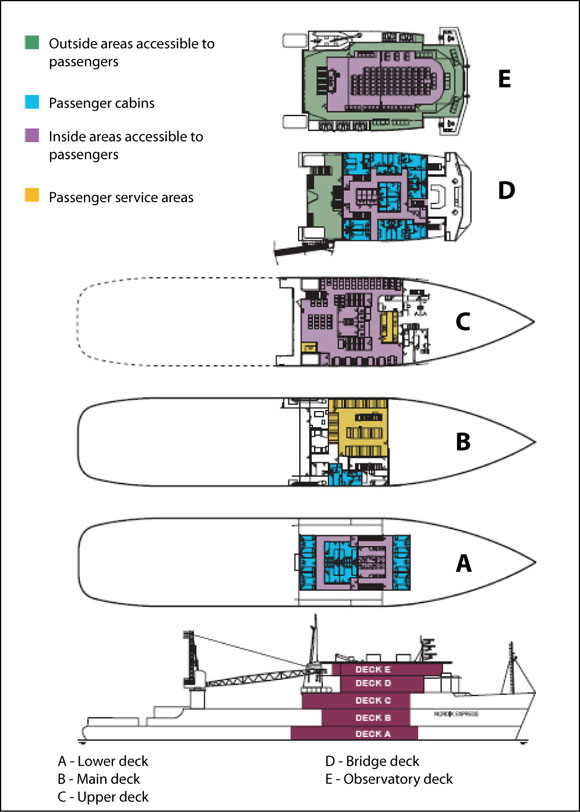
Source: Groupe Desgagnés
Appendix B — Typical Port Schedule
| Port | Day | Arrival | Departure |
|---|---|---|---|
| Rimouski | Tue. | — | 1230 |
| Sept-Îles | Wed. | 2359 | 0600 |
| Port-Menier | 1345 | 1545 | |
| Havre-Saint-Pierre | 2115 | 2215 | |
| Natashquan | Thu. | 0430 | 0800 |
| Kegaska | 1045 | 1230 | |
| La Romaine | 1500 | 1800 | |
| Harrington Harbour | Fri. | 2345 | 0145 |
| Tête-à-la-Baleine | 0345 | 0500 | |
| La Tabatière | 0700 | 0900 | |
| Saint-Augustin | 1145 | 1330 | |
| Blanc-Sablon | 1830 | 2330 | |
| Saint-Augustin | Sat. | 0430 | 0600 |
| La Tabatière | 0845 | 1100 | |
| Tête-à-la-Baleine | 1300 | 1515 | |
| Harrington Harbour | 1715 | 1930 | |
| La Romaine | Sun. | 0115 | 0245 |
| Kegaska | 0515 | 0615 | |
| Natashquan | 0900 | 1100 | |
| Havre-Saint-Pierre | 1715 | 1915 | |
| Port-Menier | Mon. | 0045 | 0300 |
| Rimouski | 1945 | — |
Appendix C — Ports visited and cargo/passengers
| Arrival Date and Time | Port | Cargo (metric tonnes) |
Passengers | ||
|---|---|---|---|---|---|
| Loaded | Unloaded | Embarking | Disembarking | ||
| 15 August 2007 at 0020 | Sept-Îles | 107.25 | 1.07 | 3 | 0 |
| 15 August 2007 at 1320 | Port-Menier | 5.91 | 64.69 | 14 | 5 |
| 15 August 2007 at 2120 | Havre-Saint-Pierre | 1.56 | 5.59 | 15 | 17 |
| 16 August 2007 at 0420 | Natashquan | 35.69 | 9.76 | 168 | 0 |
| 16 August 2007 at 1115 | Kegaska | 0.31 | 6.05 | 3 | 2 |
| 16 August 2007 at 1500 | La Romaine | 0.21 | 29 | 16 | 80 |
Appendix D — Area of the occurrence
Appendix E — Occurrence timeline
Appendix F — Tank plan of vessel
Appendix G — Occurrence voyage

Appendix H — Glossary
- ECS
- electronic chart system
- GPS
- global positioning system
- kW
- kilowatt
- IMO
- International Maritime Organization
- ISM
- International Safety Management
- ISM Code
- International Management Code for the Safe Operation of Ships and for Pollution Prevention (International Safety Management Code)
- m
- metre
- MSA
- Marine Safety Advisory
- OOW
- officer of the watch
- SMS
- safety management system
- SOLAS Convention
- International Convention for the Safety of Life at Sea
- S-VDR
- implified voyage data recorder
- TC
- Transport Canada
- TEU
- 20-foot equivalent unit
- TSB
- Transportation Safety Board of Canada
- VDR
- voyage data recorder
- XTE
- cross-track error
- 1/O
- first officer
- 2/O
- second officer
- 3/O
- third officer
- °
- degree
- °G
- degree gyro
- °T
- degree true