Accidental death
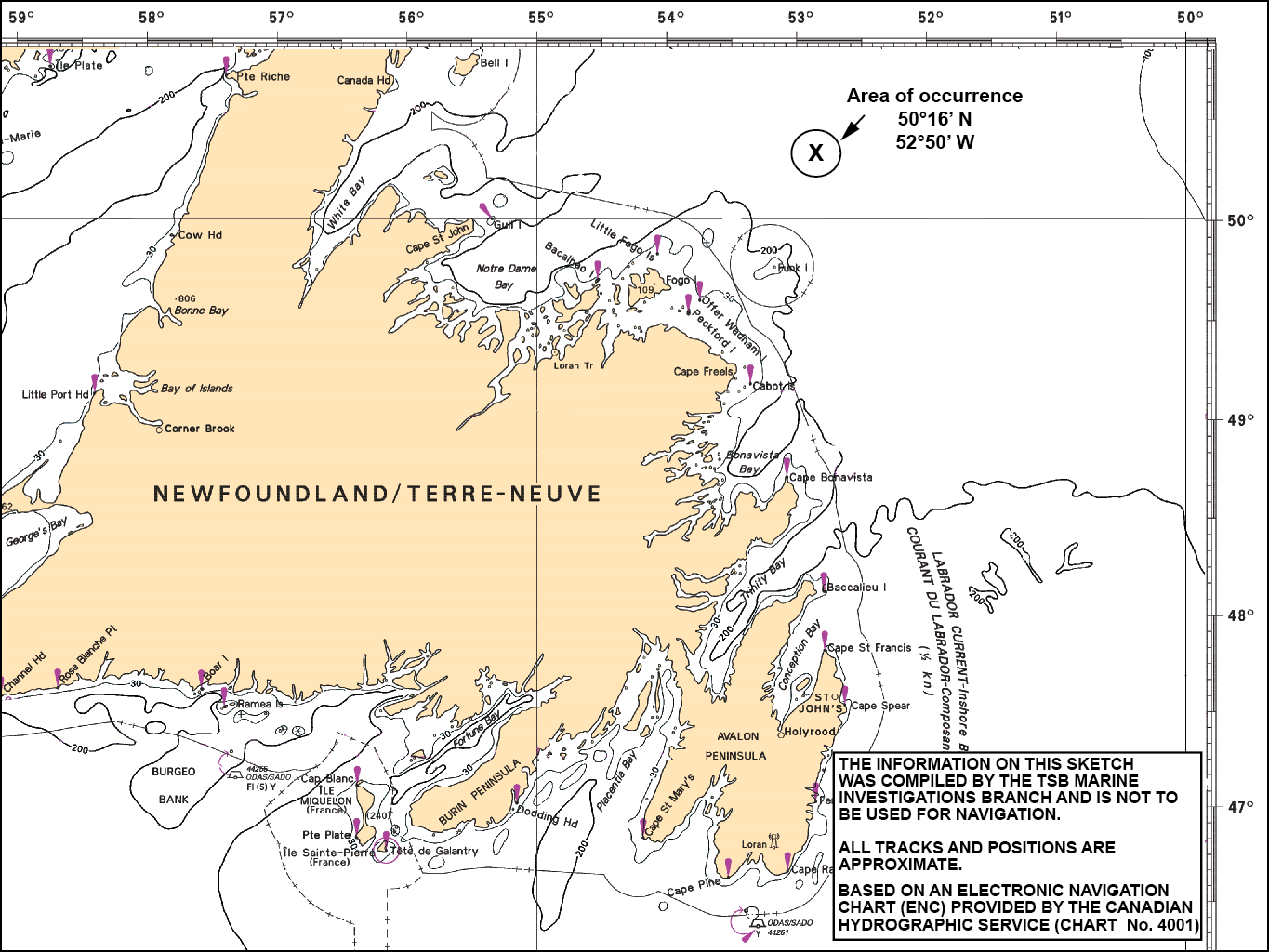
Large fishing vessel Katsheshuk II
65 nautical miles NNE of Cape Freels,
Newfoundland and Labrador
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 10 February 2012, at approximately 2000 Newfoundland Standard Time, a crew member on the large fishing vessel Katsheshuk II lost his life when a hydraulically-operated shutter door closed on him as he was exiting the holding tank in the vessel’s processing factory.
Factual information
Particulars of the vessel
| Name of the vessel | Katsheshuk II |
|---|---|
| Official number | 824944 |
| Port of registry | St. John’s, Newfoundland and Labrador |
| Flag | Canada |
| Type | Large fishing vessel |
| Gross tonnage | 1885 |
| LengthFootnote 1 | 55.12 m |
| Draught | Forward: 6.5 m Aft: 6.5 m |
| Built | Kristiansund, Norway, 1995 |
| Propulsion | Diesel engine, single-screw (2999 kW) |
| Cargo | Approximately 365 tonnes of shrimp. |
| Crew | 25 |
| Registered owner | Katsheshuk Fisheries, Ltd. |
Description of the vessel
The Katsheshuk II was built in Norway in 1995 as a single-screw stern trawler of all-welded steel construction (photo 1). The navigating bridge and crew accommodation are located forward, and the engine room is located aft. The vessel’s shrimp-processing factory is situated one deck above the fish hold (Appendix A). The hull is subdivided by 5 transverse watertight bulkheads. A watertight inner bottom, enclosing double-bottom tanks, extends the length of the fish hold, while the hull in way of the engine room is of part double-bottom construction.

The vessel is engaged in the shrimp fishery off the East Coast of Canada and is equipped for on-board processing and freezer storage of shrimp catches. At the after end of the factory deck, the vessel has 2 holding tanks that hold the shrimp prior to processing. These tanks are filled by dumping the shrimp through hatches on the main deck. For processing, the shrimp are transferred to the factory conveyor belt by way of 2 openings in the aft bulkhead. The size of these openings, and consequently the flow of shrimp, is controlled by 2 hydraulically-operated shutter doors. When activated, these doors, which each open to a maximum of 40 cm by 40 cm, take about 2 seconds to partially or fully close, depending on the operator’s needs.
History of the voyage
On 26 January 2012, at 1600, Footnote 2 the Katsheshuk II sailed from Harbour Grace, Newfoundland and Labrador, with a crew of 25. The vessel was bound for the shrimp fishing grounds on Funk Island Bank, NL (Appendix B). On 09 February, with 365 tonnes of shrimp processed and stowed in the cargo hold, the crew began cleaning the vessel while it was heading toward Harbour Grace. In preparation for arrival in port, the deckhands worked on the trawl deck while the processors cleaned the factory. Cleaning the factory involved scrubbing the conveyor belts, all stainless steel surfaces, and the port and starboard holding tanks.

One of the crew members, who was working as a processor and will be hereafter referred to as “the 5 kg processor”, had been assigned to pack 5 kg boxes at the forward end of the factory for this trip. He had done this task on the previous trip, which had been his first on this vessel. His duties also included cleaning, and on this trip he was assigned to clean the aforementioned holding tanks.
Although he had received an orientation tour of the vessel, including familiarization with the lifesaving appliances and firefighting arrangements, the orientation did not include the factory. A formal briefing of the task at hand had not been provided, other than a description of the actual cleaning to be done, and no instructions regarding the operation of the shutter doors had been given.
There were 2 means of access to the shrimp-holding tanks: via the hatches on the main deck or through the 40 cm by 40 cm spaces made when the hydraulically-operated shutter doors were fully open. The 5 kg processor, dressed in full oilskins, used the shutter door openings to enter and clean the tanks for expediency and because the deck crew were working in the vicinity of the hatches on the main deck. During the cleaning process, he used these openings several times, sometimes to retrieve cleaning supplies and other times to egress for breaks.
At 1700 on 10 February, the 5 kg processer ceased cleaning for meal time. Afterward, a safety committee meeting was held at 1745 with 14 of the crew in attendance, including the factory foreman and the 5 kg processor. The topics of the meeting were working alone and accident reporting. The meeting was chaired by the second mate, and none of the vessel's senior officers or engineers attended.
Following the safety committee meeting, the 5 kg processor resumed cleaning the holding tanks, and, upon completion, he exited the tanks and approached the factory foreman to request they be inspected. Both men entered the starboard holding tank via the shutter door opening; the inspection was carried out and the job approved. The 5 kg processor then started to exit the tank feet first and on his back. When the 5 kg processor was partway through the opening, he had to manoeuvre his body over the conveyor belt located just ahead of the shutter door. Once clear, he stood up and turned to see the factory foreman following him; the foreman had chosen to exit headfirst and face down. The foreman's head had just cleared the opening when the shutter door closed on his neck, killing him.
The 5 kg processor alerted other nearby crew and 1 of the other processors alerted the second mate, who was on watch in the wheelhouse. The second mate, a former paramedic, came down to the factory and reported the death of the foreman.
The master of the Katsheshuk II contacted Maritime Rescue Sub-Centre St. John's to report the accident. The vessel arrived at Bay Roberts, NL at 0921 on 11 February.
Vessel certification
At the time of the occurrence, the Katsheshuk II held the class 1A1 Stern Trawler KMC ICE-1B with Det Norske Veritas. It was also subject to regular inspection under the Transport Canada (TC) Marine Safety Large Fishing Vessel Inspection Regulations. The vessel was certificated and equipped in accordance with Canadian regulations and was last issued a safety inspection certificate (SIC 31) on 20 December 2011.
Personnel certification and experience
The master and the officers of the vessel were in possession of valid certificates for their positions and the trade in which they were engaged. The factory foreman and the 5 kg processor held Duties (MED) certificates, as required by regulation. The factory foreman had about 4 years of fishing experience on board the Katsheshuk II. The 5 kg processor was on his second trip on the Katsheshuk II, and had also fished 2 seasons on a crab fishing vessel.
Environmental information
The weather conditions at the time of the occurrence were estimated by the ship's crew to be winds from the northwest at 30 knots with a swell of 1 to 2 m.
Hydraulic lever for shutter doors
The opening and closing of the shutter doors was controlled by hydraulically-driven levers, which were mounted in an inverted position on the deckhead. Factory workers used these levers to adjust the size of each holding tank opening, thus controlling the amount of shrimp running onto the conveyor belt for processing. Pushing the lever forward caused the shutter door to open, while pulling it back caused the shutter door to close incrementally. The hydraulic system could be isolated by closing the return line, which would render the shutter doors inoperable. The emergency stop for the hydraulics was located on the port bulkhead, aft, in the factory. The levers did not have external guards to prevent inadvertent activation, nor were the levers labelled.

The Transportation Safety Board (TSB) investigation examined the hydraulic lever Footnote 3 (photo 3) that controlled the starboard shutter door. The lever was designed to automatically return to the neutral position after it had been activated in either the “open” or “close” direction. When the hydraulic lever was functioning as intended, the shutter door would incrementally drop about 5 cm each time the lever was activated and released. However, the action of the lever spring was compromised and it did not recoil; no force was generated to automatically return the lever to the neutral position when it was released, as it was designed to do. The TSB determined that the position of the nut on the threaded lever allowed the lever to protrude into the hub assembly and displace the coil spring laterally and upward.
As such, when the lever was activated in the “close” position and then released, it did not automatically return to the neutral position. In contrast, when the lever was activated in the “open” direction, it returned to the neutral position as designed. The normal reporting procedure for a defect like this was to verbally inform the immediate supervisor, who in turn would inform the engineering staff. The engineering staff would then either address the defects immediately or fill out a work order for shore-based support. The continuous malfunction of the lever was not reported to the engineering staff or shore management and therefore was not addressed either on board or ashore. Some of the crew had known of this problem for more than 6 months.
Familiarization
On 07 January 2012, prior to his initial trip on board the vessel, the 5 kg processor received a first time crew member orientation to the vessel. He also signed the new crew orientation checklist, which included the following:
- Qualifications
- MED, first aid, etc.
- Walk -around of vessel
- Firefighting systems, muster station, lifesaving appliances, housekeeping policies, location of SMS manual and occupational health and safety (OHS) bulletin board, etc.
- Specific job functions
- Duties, responsibilities, work schedule, personal protective equipment required for the new crew member's area, sanitation and hygiene rules for factory, introduction to machines the new crewmember may use, and explanation and demonstration of safe operating procedures for equipment or tools in the new crew member's work areas.
The 5 kg processor did not receive an orientation to machinery, systems, or safety procedures outside of his expected work area. The task of cleaning the holding tanks was only done once at the end of each trip. The 5 kg processer had never done this task before and was not given an orientation to the equipment involved, including the levers activating the shutter doors.
Previous factory occurrences
In 2004, a crew member was crushed to death while cleaning the shrimp cooker on the Nova Gale, another large freezer vessel operated by a different company. Under normal operations, the shrimp coming off the conveyor belt filled the cooker basket until it reached a certain level, detected by an electronic sensor, and was automatically dumped into the cooker. In this occurrence, the crew member was inside the cooker basket and was cleaning it when he inadvertently triggered the sensor and was crushed between the cooker basket and the side of the cooker.
In January 2006, a similar occurrence took place on the Katsheshuk II when a crew member inadvertently triggered a sensor while cleaning a similar cooker basket. The crew member was trapped briefly between the cooker basket and the side of the cooker, but the master was nearby and pushed the emergency stop, preventing serious injury.
In June 2010, a second similar occurrence took place on board the Katsheshuk II. Again, a crew member was in the cooker basket and inadvertently triggered the sensor. Again, a crew member was nearby and pushed the emergency stop in time to avoid serious injury.
In both cases on board the Katsheshuk II, accident reports were filled out. In the 2006 accident, the preventative measure to avoid similar occurrences was to ensure that, prior to person(s) entering the cooker, the emergency stop button was engaged to avoid inadvertent activation. However, this measure was applied inconsistently. In the 2010 incident, the preventative measure was to hold more in-depth training on cooker systems. In addition, the company installed a second emergency shut-off in the cooker for use in the event that the external shut-off was not engaged during cleaning or maintenance of the cookers.
Management of safety
Safety management systems
No operation is entirely free of risk, and fishing is no exception. There are numerous ways to deal with these risks; one internationally-recognized method Footnote 4 is via safety management systems (SMS). Although the benefits of SMS have long been recognized by the marine community, SMS is not required on all types of vessels. The Katsheshuk II, as a fishing vessel, is not subject to the International Convention on the Safety of Life at Sea (SOLAS) and thus the International Safety Management Code for the Safe Operation of Ships and for Pollution Prevention (ISM Code) does not apply to it.
Effective safety management provides a formal framework for identifying and mitigating risk. Ideally, a vessel operator would identify existing and potential risks, establish safety policies and procedures to mitigate the risks, and then provide a means to continuously gauge effectiveness so as to improve organizational safety where necessary. Internal and external audits are used to regularly validate the effectiveness of the SMS. The resulting documented, systematic approach helps to ensure that individuals at all levels of an organization have the knowledge and the tools needed, as well as the necessary information to make sound decisions in any operating condition, including both routine and emergency operations.
An effective SMS may not identify all risks in advance, but when one is identified—in advance or as the result of an accident—it should be assessed, and any necessary mitigating measures incorporated for the future.
International standards for safety management systems
The ISM Code governs almost all of the international shipping community. It provides an international standard for the safe management and operation of ships and for pollution prevention. The functional requirements of an SMS, according to the ISM Code, are as follows:
- a safety and environmental-protection policy;
- instructions and procedures to ensure safe operation of ships and protection of the environment in compliance with relevant international and flag state legislation;
- defined levels of authority and lines of communication between, and amongst, shore and shipboard personnel;
- procedures for reporting accidents and non-conformities with the provisions of this Code;
- procedures to prepare for and respond to emergency situations; and
- procedures for internal audits and management reviews.Footnote 5
In addition to the above, key safety management principles advocated by the ISM Code include a commitment from management, recognition of the importance of attitudes and motivation of individuals at all levels, and the appointment of a designated person ashore (DPA) to serve as the link between the ship's staff and shore staff and to verify the SMS implementation.
Provincial safety initiatives
In the province of Newfoundland and Labrador, the Workplace Health, Safety and Compensation Commission (WHSCC) is a mandatory employer-funded insurance system that promotes safe and healthy workplaces, and provides return-to-work programs and compensation to injured workers and their dependents.Footnote 6 The WHSCC's Prevention and Return-to-Work Insurance Management for Employers/Employees (PRIME) initiative Footnote 7 is aimed at providing insurance-premium rebates for those companies that meet specific safety requirements. PRIME uses 2 incentives: refunds for employers that meet health and safety and return-to-work practices, and potential refunds based on a comparison of the employer's workplace injuries against a set range. To be eligible for PRIME, an employer must meet certain requirements, and the onus is on the employer to demonstrate compliance with these requirements during the PRIME audit process. These audits may, but are not required to, include a workplace visit.
Components of eligibility for PRIME include the following:
- having a written OHS and return-to-work policy statement
- providing orientations for workers
- conducting workplace inspections
- conducting accident/incident investigations
- holding OHS committee meetings
- holding tool box meetings Footnote 8
- evaluating and recognizing workplace hazards
In 2007, the WHSCC first verified that the Katsheshuk II qualified for the PRIME program and subsequently audited the vessel annually. In 2010, a similar verification was also carried out and the Katsheshuk II re-qualified. At no point did a WHSCC representative make a physical visit to the Katsheshuk II, nor was one required. In addition, the WHSCC advisors had limited knowledge of these types of fishing vessels.
Unlike the provincial body, Service Newfoundland and Labrador OHS, WHSCC did not have a mandate to conduct workplace inspections or assess hazards in the workplace. In some cases, OHS requirements may be greater than the WHSCC requirements noted under PRIME.
Service Newfoundland and Labrador, Occupational Health and Safety Division
The OHS division of Service Newfoundland and Labrador (Service NL) is supported by staff (including inspections officers, industrial hygienists, engineers, and radiation specialists) who perform various activities such as
- investigating workplace accidents and compiling statistics;
- conducting compliance inspections and detailed audits of workplaces;
- assessing hygiene of various physical, chemical, biological and ergonomic agents in the workplace in order to protect worker health;
- evaluating and inspecting radiation control measures in workplaces; and,
- enforcing OHS legislation.
Service NL had not inspected or audited the Katsheshuk II prior to the accident.
Transport Canada, marine safety
TC conducts periodic inspections of large fishing vessels like the Katsheshuk II. When equipment installations on ships affect the operation of the vessel with respect to navigation or shipping, the inspection of the equipment is always under federal jurisdiction. These inspections, however, do not cover elements of the vessel that relate to the business of fishing, such as factory operations.
Safety management system on the Katsheshuk II
The Katsheshuk II had a SMS in place, despite not being required by regulation to have one. The intent of the SMS, which was designed as an OHS program Footnote 9 in 2005 by a consultant in conjunction with Katsheshuk Fisheries, was to nurture on-board safety, prepare for PRIME, and comply with provincial OHS legislation. The SMS was also to take into consideration the applicable provincial and federal legislation while referencing the SOLAS regulations.
Initiatives established by the vessel's SMS ensured, among other things, that:
- safety meetings took place;
- new crew received vessel orientations;
- pre-trip safety inspection checklists were completed;
- accident investigations were carried out;
- hazardous materials programs took place; and,
- some safe work procedures were documented.
The TSB investigation revealed the following:
- The Katsheshuk II safety policy statement found in the vessel's SMS manual and posted on the OHS bulletin board was signed by the Katsheshuk Fisheries operations manager, rather than by senior management.
- The policy statement called for management to “co-operate with the OH&S Committee and crew members to create a healthy and safe work [sic] and provide the necessary awareness and training to allow our employees to work safely.”
- Senior officers were absent from nearly all safety meetings, despite the master and the first mate being members of the safety committee.
- Neither management, nor the ship's officers, nor the crew were provided with training in effective safety management.
- There were no documented risk assessments for workplace operations.
- There was no on-board or shore-based system to follow up on accident reports or safety deficiencies that were identified during safety meetings.
- Although documented safe work procedures existed, they were broad in scope and pertained mostly to the deck, with few procedures for the factory.
- Although there were some ad hoc procedures in place for some of the hazardous work in the factory, such as cleaning the cooker, these were not consistently followed.
- In 2008, the second officer had taken over the duties of safety committee designate. These duties include chairing safety committee meetings, conducting pre-departure vessel inspections, conducting new crew orientations, and being responsible for providing information to and addressing safety concerns of all crew members.
Hazard assessment
A key component of an effective SMS is the identification and assessment of workplace hazards.
During verification of Katsheshuk II's 2008 PRIME documentation, the WHSCC accepted several completed “Report of Unsafe Condition or Hazard” forms. WHSCC suggested, however, that assessments be developed for all hazards, and that these be ranked by “severity, probability, etc.” A total of 8 more “Report of Unsafe Condition or Hazard” forms were subsequently filled out by crew before new procedures were added to the vessel's new draft SMS manual.
Although risk assessments were subsequently added to the forms, the majority of the completed forms were related to fishing operations; only 1 related to factory operations. Footnote 10 None were associated with shipboard operation. Hazards associated with accessing the holding tanks via the vertical hatches were never identified, nor were they brought up at any meeting. The 2 previous on-board accidents involving the shrimp cooker were identified at tool box meetings, but hazards associated with this activity were not officially documented.
Tool box meetings
Tool box meetings were informal discussions among crew members Footnote 11 aimed at correcting unsafe acts or conditions, relaying safety-related rules or policies, or discussing recent accidents. These meetings were held approximately once a trip for each watch. In 2010, procedures to safely clean the cooker were discussed at 3 meetings of the factory crew: 2 of these discussions took place prior to the previously-noted incident involving a crew member in the cooker basket, and 1 took place afterward.
The procedures discussed at tool box meetings included:
- ensuring the emergency stop was engaged;
- turning off the hydraulics;
- setting the control to manual, and;
- ensuring another crew was standing by.
The same topic was brought up on 6 occasions in 2011.
Occupational health and safety committee meetings
As stated in the vessel's SMS manual, the OHS committee “shall include the master, first mate and two (2) or more selected crew members from that particular trip.” The company appointed the second mate as safety officer on board the vessel and determined that he was to chair safety meetings rather than the master. This was intended to foster greater communication regarding safety issues, as it was felt that crew members would be less open to discuss some issues in the presence of the master. Meetings were held on board once per trip, generally when fishing was completed and the vessel was on its way home. Although most crew on watch attended, the master, the chief mate, and the engineers did not usually attend, nor did other crew who were not on watch.
Discussion topics were usually taken directly from the SMS manual, which was read aloud verbatim. Subsequent discussion was generally limited, though crew members would occasionally voice safety concerns.
TSB watchlist
In 2012, the TSB released an updated edition of its 2010 Watchlist. This document identifies the 9 safety issues posing the greatest risk to Canadians and Canada's transportation system. One issue on the Watchlist is marine SMS. Specifically, the Board has pointed out that TC does not always provide effective oversight of marine transportation companies transitioning to SMS, nor are some companies even required to have one. The TSB has repeatedly emphasized the advantages of SMS in the marine industry, citing deficiencies in many occurrences over the last 14 years. Footnote 12
Analysis
After fishing operations were completed, the crew on board the Katsheshuk II began cleaning the vessel on the way home. The 5 kg processor was assigned to clean the shrimp holding tanks. As he was cleaning, he climbed in and out of the tanks several times through the 40 cm by 40 cm openings created by the hydraulic shutter doors. Once finished the job, he asked the factory foreman to inspect his work, and they both crawled through the starboard shutter door opening. After approving the job, the 5 kg processor crawled through the opening first and the factory foreman followed him. While the factory foreman was crawling out headfirst and face down, the hydraulic shutter door closed on his neck, killing him.
The investigation determined that the hydraulic shutter door was most likely triggered either when the 5 kg processor snagged the hydraulic lever with his clothing or bumped it with his head as he emerged from the tank and crawled over the conveyor belt.
Hydraulic lever
The hydraulic lever controlling the shutter door was designed to return to the neutral position after being activated in either the “open” or “close” direction and then released. However, the action of the lever spring was compromised when the lever was in the “close” position; the spring did not recoil, and no force was generated to return the lever to the neutral position when the hand lever was released, as it was designed to do.
It was determined that the hydraulic lever had stopped functioning as intended more than 6 months prior to the accident. The normal procedure for reporting defects in shipboard equipment was to verbally inform the immediate supervisor, who in turn would inform the engineering staff. The engineering staff would then fill out a work order to submit at the end of the trip for defects requiring shore-based support. Repairs not requiring shore-based support would be addressed immediately by the engineering staff. However, because the continuous malfunction of the hydraulic lever was not assessed and identified as a safety hazard and did not affect functionality during regular fishing operations, it was not reported or addressed either on board or ashore.
As the 5 kg processor was not aware of making contact with the lever, it could not be determined whether a properly functioning lever would have returned to the neutral position in time to prevent the accident. Furthermore, the speed at which the shutter door closes when activated would likely preclude any effective reaction by a crew member in the path of the closing door. In the absence of a properly working lever, the risks of injury to the factory foreman were increased. Knowingly or unknowingly using defective equipment, such as the hydraulic lever, may put crew members at risk.
Orientation
All new crew members must be provided with an orientation when they join a vessel. The purpose of this orientation is to provide crew with adequate basic safety training to effectively perform assigned duties and tasks in a safe manner. Orientations address general safety as well as safe working procedures associated with the tasks to be performed on board. When a crew member is assigned new tasks, it is necessary to provide him/her with a new orientation in order to mitigate any new hazards that might be encountered.
On his first trip on board the vessel, the 5 kg processor received an orientation. He was also briefed on the safe operating procedures for equipment he used for his day-to-day job. The holding tank shutter doors were not included in this orientation, as he was not expected to routinely work in this area. At the end of his second trip, the 5 kg processor was tasked to clean the holding tanks. Although he had not performed this task before, he received no new orientation, briefing, or training with respect to safe operating procedures or any associated hazards.
The 5 kg processor was therefore unaware of the purpose of the various levers in the area where he was assigned to work. He was also unaware that the activation of one of those levers would close the holding tank shutter door, and of the potential danger that this represented.
Climbing through the shutter door openings was an awkward process, which was compounded by having to crawl over the conveyor belt frame before being able to stand upright. The levers were in an exposed area above the conveyor belt frame, and no particular caution was exercised when the 5 kg processor was crawling over the conveyor belt frame as they represented no known danger to him.
In the absence of thorough workplace orientations, the hazards and risks associated with a workplace may remain unknown to crew members.
Safety management systems
An effective SMS requires organizations to recognize the risks involved in their operations and to competently manage those risks. International best practises for SMS involve a formal, documented, and systemic approach that includes a commitment from senior management, as well as a rigorous risk assessment process and a means to continuously gauge effectiveness so that improvements can be made where necessary. The resulting system helps ensure that individuals at all levels of an organization have the knowledge and tools to effectively manage risk, as well as the necessary information to make sound decisions in any operating condition.
The implementation of SMS aboard the Katsheshuk II was deficient in these key elements:
- Senior officers were absent from nearly all safety meetings, despite being members of the vessel's Occupational Health and Safety (OHS) committee.
- There was no formal SMS training given to crew members, ship's officers, or shore-side management or consultants.
- Although the vessel carried an SMS manual, safe work procedures were broad in scope and pertained mostly to the deck, with few procedures for the factory. Footnote 13 Moreover, procedures for work that had been identified as hazardous (such as cleaning the cooker) were ad hoc and were followed inconsistently.
- There were no documented risk assessments for workplace operations. None of the completed “Report of Unsafe Condition or Hazard” forms were associated with shipboard operations. Moreover, the previous on-board accidents with the shrimp cooker had not been documented as a hazard or identified in the safe work practices, despite being discussed at tool box meetings. The shutter door openings had not been identified as a potential hazard.
- There was no on-board or shore-based system to follow up on accident reports or safety deficiencies identified during safety meetings, nor for any problems—such as the malfunctioning lever—that were identified elsewhere (and about which some crew members had known for months).
As for compliance, with the province's Prevention and Return-to-Work Insurance Management for Employers/Employees (PRIME) initiative, this process was essentially a paper audit; advisors assigned by the Workplace Health, Safety and Compensation Commission (WHSCC) had limited knowledge of these types of fishing vessels, and it was not part of their mandate to visit and inspect actual conditions on board. It is clear, therefore, that the SMS aboard the Katsheshuk II, although voluntary, was not effective at identifying the risks and unsafe practices associated with the operation of the shutter doors. Moreover, although even the most rigorous SMS may not identify all hazards in advance, this one did not thoroughly incorporate mitigating measures even for those hazards that had been previously identified. The crew did not understand the principles of hazard assessments, nor had they received any training. Thus, a more rigorous procedure to identify risks throughout the vessel was not implemented despite advice from WHSCC. Crews working in such environments face the risk that other unsafe conditions or acts may remain unidentified and unaddressed.
The proposed amendments to Transport Canada's Safety Management Regulations (which apply to a segment of the non-pleasure fleet) would include vessels of the Katsheshuk II's size (under 500 gross tonnes) and would require it to have a SMS that is certified and audited.
Effectiveness of the vessel's SMS
A major component of an effective SMS is the auditing process. The International Association of Classification Societies (IACS) defines the audit process as:
A systematic and independent examination to determine whether the SMS activities and related results comply with planned arrangements and whether these arrangements are implemented effectively and are suitable to achieve objectives. Footnote 14
In 2007, the WHSCC first verified that the Katsheshuk II possessed all the documentation required to be accepted into the PRIME program. In 2010, a similar verification was also carried out. This process, however, covered only the documents, meeting minutes, and various forms that were filled out, making it essentially a paper audit for the sole purpose of qualifying for PRIME. Consequently, although the paperwork was filled out correctly and WHSCC suggested that hazard assessments be further developed, no new procedures were implemented and many components remained missing from the vessel's SMS.
The consultant hired by Katsheshuk Fisheries in 2005 was tasked with gathering the paperwork and improving on the vessel's SMS while meeting all the targets of the province's PRIME initiative. The consultant relied on crew members to define hazards and help develop safe work procedures. Most of these newly developed safe work procedures, some of which appeared in the newer draft SMS manual, involved fishing operations on deck. PRIME policies state that only a sample of safe work practices must be available for the health and safety advisor to review. Very few, if any, safe work procedures existed for factory operations, and no mention was made of the various pieces of machinery and hydraulics in the factory. The vessel's senior officers did not attend safety meetings, safe work practices in the factory were unaddressed, and orientation for new crew did not include safe work practices in the factory.
There was no system in place to assess whether the vessel's SMS activities and related results were effectively implemented or suitable for achieving the objectives of an SMS.
Without internal and external audits on board and ashore to verify whether safety and pollution prevention activities comply with the SMS, there is a risk that a company's SMS may not be effective.
Findings
Findings as to causes and contributing factors
- The company’s safety management system (SMS) did not identify the hazards associated with accessing the holding tanks via the shutter doors.
- The company provided no procedures for the safe use of the shutter doors as a means of access for cleaning the holding tanks.
- The 5 kg processor did not receive any familiarization or briefing on the hazards present in the after part of the factory and was unaware of the risks involved with the hydraulic lever.
- The factory foreman lost his life while exiting the holding tank when the hydraulic lever for the shutter door was inadvertently activated.
- The spring in the hydraulic lever was compromised and would not automatically return the lever to the neutral position.
Findings as to risk
- Defective equipment that is not reported or repaired in a timely fashion may put crew members at risk.
- Without an effective SMS, unsafe conditions or acts may not be identified and addressed, thereby putting the crew at risk.
- Without internal and external audits on board and ashore to verify whether safety and pollution prevention activities comply with SMS, there is a risk that a company’s SMS may not be effective.
Safety action
Safety action taken
Following the occurrence, the company replaced the defective hydraulic lever and, by order of the Occupational Health and Safety (OHS) division of Service Newfoundland and Labrador, the company:
- installed watertight access doors on both sides of the holding tank;
- provided confined space entry training for those crew members expected to enter confined spaces;
- relocated the overhead hydraulic levers and installed guards; and,
- installed locking pins on the main deck hatches as a safeguard for crew members entering the holding tanks from the main deck.
The company also:
- repaired the hydraulic lever in question and installed new locking pins, warning signage, locking isolation valves, and protective steel bars around the hydraulic levers, as well as an additional emergency shut-off switch to the hatch doors;
- installed a holding tank hatch door for access from the main deck for cleaning;
- investigated its other vessels and made modifications to its other shrimp trawler to ensure safety measures were in place in respect of the holding tank door system; and,
- completed a detailed hazard assessment in response to the incident that was particularly focused on the task of cleaning the shrimp holding tank and associated areas and functions on board the vessel.
On 22 February 2012, the company held a tool box meeting addressing various safety issues related to the incident, noting suggestions for certain policy and permit revisions and rescue procedures. Subsequent to the occurrence, the following safe working procedures were adopted for these factory activities:
- crossing over the Japanese chemical soak/dumper; Footnote 15
- using the kilo machine and strapping machine;
- cleaning the port and starboard receiving bins;
- cleaning the port and starboard tunnel freezers;
- cleaning and maintaining the cooker;
- working in the hold; and,
- safely loading and stacking product in the hold.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on . It was officially released on .