Capsizing and loss of life
Leviathan II
Clayoquot Sound, British Columbia
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 25 October 2015, at approximately 1500 Pacific Daylight Time, the passenger vessel Leviathan II was on a whale-watching excursion with 27 people on board when it capsized off Plover Reefs in Clayoquot Sound, British Columbia. The subsequent rescue operation recovered 21 survivors, which included 18 passengers and 3 crew members. There were 6 fatalities. As a result of the capsizing, approximately 2000 litres of fuel leaked into the water.
This report is also available in English.
1.0 Factual information
1.1 Particulars of the vessel
| Name of vessel | Leviathan II |
| Official number | 800190 |
| Port of registry | Vancouver |
| Flag | Canada |
| Type | Passenger |
| Gross tonnage | 32.58 |
| Length | 19.66 m |
| Draft (estimated at time of occurrence) | 0.60 m |
| Propulsion | Two diesel engines, providing 515 kW in total, driving twin-screw propellers |
| Built | 1981 (Rebuilt: 1996) |
| Maximum complement | Passengers: 46 Crew: 4 |
| On board at the time of the occurrence | Passengers: 24 Crew: 3 |
| Registered owner | Jamie's Whaling Station Ltd. |
1.2 Description of the vessel
The Leviathan II (Figure 1) was an aluminum vessel with a shallow vee-shaped hull. It was originally constructed in 1981 as a crew boat. It was purchased by its current owner in 1995, and, in the following year, it was rebuilt in a British Columbia shipyard to operate as a passenger vessel for whale watching. As part of the rebuild, the hull was lengthened by approximately 4.8 m at the stern. The top of the original cabin was also strengthened to provide a passenger seating area on the top deck and a flying bridge; navigation equipment was relocated from the wheelhouse to the flying bridge. As a result, the wheelhouse was no longer in active use.

The vessel had 3 passenger seating areas: the open top deck, the aft section of the main deck, and the enclosed lower cabin (Appendix A). The perimeter of the passenger seating area on the main deck had a railing around it, and there was an acrylic skylight above the seating area to protect passengers from the elements. A set of stairs on the main deck located amidships served as the main access point between the top deck and the lower cabin. The entrance to the lower cabin at the base of the stairs was fitted with a weathertight door.
The lower cabin, which was enclosed by windows, had 2 square-shaped viewing ports that extended downwards through the deck and allowed passengers to look at underwater features (Appendix A). The top and bottom of the viewing ports were fitted with laminated safety glass. A small galley area was also located in the lower cabin.
At the forward end of the lower cabin was a set of stairs that led up to the wheelhouse. The wheelhouse had 2 weathertight doors, 1 on each side, which opened onto the forward main deck. Although there was no door separating the wheelhouse from the passenger cabin, access to the wheelhouse was restricted to crew members only.
The hull consisted of a forepeak void space, which could be accessed through a sealed hatch in the wheelhouse, and 3 other void spaces, which could be accessed through sealed hatches in the lower cabin. The engine room, located aft of the No. 3 void space, was accessed through hatches on the main deck. There were port and starboard fuel tanks adjacent to the engine space; however, both had been decommissioned during the rebuild and were capped off. Aft of the engine room, there were 2 void spaces that housed the fuel tank, as well as 2 aft peak spaces.
The vessel was fitted with a bilge pump driven by the main engine. The bilge pump was connected to a manifold with shut-off valves for all compartments. The aft void spaces were additionally fitted with 12 volt direct current electric bilge pumps. The vessel was powered by twin diesel engines. Each of the 2 propeller shafts penetrated the hull through fittings on the transom and could be trimmed to adjust the degree at which its respective surface-piercing propeller was submerged. The vessel operated at a service speed of approximately 12 knots.
The vessel was fitted with a swim platform (Appendix A) that extended outwards from the stern by approximately 1 m to allow access to the water. The swim platform was the same width as the vessel.
The flying bridge had communications and navigation equipment that included a magnetic compass, a radar, a global positioning system (GPS), a depth sounder, a chart plotter, and 2 very high frequency (VHF) radiotelephones equipped with digital selective calling (DSC) capabilityFootnote 1 (1 of which was connected to the GPS). An alarm panel located in the wheelhouse provided warnings for low oil pressure, high water temperature, fire, and high bilge level. The vessel was not equipped with an emergency position-indicating radio beacon (EPIRB), nor was one required by regulation.
1.3 Company operations
The company has been conducting tours out of Tofino and Ucluelet, British Columbia, since 1982 and operates a fleet that, at the time of the occurrence, included 3 small passenger vessels and 6 rigid-hull inflatable boats (RHIBs). It offers whale-watching excursions seasonally from March to October, and approximately 25 000 passengers travel on these vessels each year. The vessel masters, in addition to performing regular duties and communicating on the radio with the front desk and other vessels, are responsible for providing passengers with tour information over the vessel's public address (PA) system during the voyage.
A typical whale-watching trip takes 2.5 to 3 hours, and the vessels travel various routes between the south end of Long Beach and Rafael Point on the coast of Flores Island, a distance of approximately 28 nautical miles. These routes change depending on weather conditions and the locations where whales and other marine wildlife, such as sea lions and otters, are most likely to be found at any given time. As part of the experience, in order to observe wildlife, it is not unusual for the vessels to pass close to land, and the vessels routinely travel near Plover Reefs.
Whale-watching excursions are weather-dependent, and trips are cancelled when conditions are likely to affect the comfort and safety of passengers. The company relies on the masters to determine when a trip must be cancelled because of poor conditions. A common practice was for company masters to cancel trips when the height of waves at the La Perouse Bank weather buoyFootnote 2 exceeded 4 m. In such situations, passengers are offered an inlet explorer tour, which stays in sheltered waters.
1.4 Description of Plover Reefs
Plover Reefs, the site of the occurrence, is located on the east side of Brabant Channel in Clayoquot Sound, British Columbia, in the vicinity of several inlets. The reef consists of several above-water rocks. The sea floor rises gradually up to the reef and, 500 m off the reef, the water depth is a maximum of approximately 30 m, and less in some places. Between March and October, the predominant direction of swell in the waters surrounding Plover Reefs is from the west. Plover Reefs is one of numerous reefs, rocks, and shoals that lie along the west coast of Vancouver Island, some of which are above water and others submerged. Tidal currents also flood and ebb in and out of sounds, straits, and inlets along the British Columbia coast.
1.5 History of the voyage
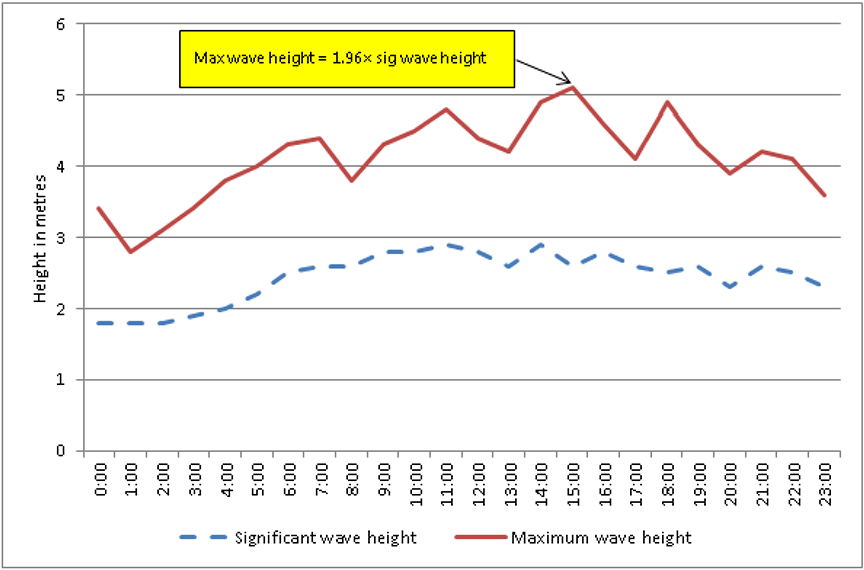
On 25 October 2015, 24 passengers arrived at the whaling station in Tofino for a whale-watching trip on board the Leviathan II. The master had checked the weather forecast on the Environment Canada website before the voyage, which was his first of the day. The forecast predicted southeast winds at 15 to 25 knots, becoming variable at 10 to 20 knots in the afternoon, and becoming northwest at 15 to 25 knots in the evening. The wave-height forecast predicted seas of 2 m, building to 3 to 4 m in the afternoon, and subsiding to 2 m near midnight.Footnote 3The master also checked the wave conditions recorded at the La Perouse Bank weather buoy. The significant wave heightFootnote 4 was between 2.6 m and 2.9 m, with a wave periodFootnote 5 of 9 to 10 seconds. The weather forecast was also available at the whaling station for the information of passengers.
While the passengers were checking in, the crew, which consisted of the master and 2 deckhands, prepared the vessel. The passengers boarded at approximately 1320Footnote 6 and were counted by the deckhands as they came aboard. The master then confirmed the number with the front desk staff over the radio. The passengers were permitted to move about freely among the 3 passenger seating areas during the voyage, and the door to the lower cabin was secured in the open position.
Upon departure, the master used the PA system to provide the passengers with general information about the vessel and the crew. He also briefed the passengers on the location of the lifejackets and the life rafts and on the need to follow crew instructions in an emergency. Finally, he requested their attention for a lifejacket demonstration, which was provided by one of the deckhands and involved showing passengers how to don a lifejacket properly.
The Leviathan II departed Tofino harbour at approximately 1330 and proceeded past Father Charles Rock and the La Croix Group, en route to Ahous Bay (Appendix B). As the vessel was proceeding, the master used the PA system to give passengers information about Tofino and the surrounding area. The master also cautioned passengers that the voyage might become rougher when the vessel exited the harbour, noting that they should remain seated, preferably at all times. If they did need to move around, they were to hold on and exercise caution when using the stairs.
Around 1405, the vessel arrived at Ahous Bay and the master checked in with the front desk staff. The vessel remained there for approximately 30 minutes while the passengers were whale watching. When the vessel left the area, the master checked in with the front desk again and stated that they were heading to Plover Reefs. While manoeuvring the vessel, the master also continued to give tour information over the PA system.
While the Leviathan II was proceeding to Plover Reefs so that the passengers could observe sea lions, there was a swell of approximately 2 m from the southeast. On approaching Plover Reefs, the master visually assessed the sea conditions and checked for the presence of breaking waves, in particular at a spot south of the reef that the company's masters commonly used to determine prevailing conditions. There were no signs of breaking waves or aerated water or foam in the surrounding area, other than on the edge of the reef itself.
The Leviathan II first proceeded along the south side of Plover Reefs and then made a 180° turn and returned to the southeast side of the reef, where the sea lions were located, to provide passengers on both sides of the vessel with an opportunity to view them (Appendix B). Shortly before 1500, the master was maintaining the vessel's position on a northerly heading approximately 100 m off the reef in water that was approximately 7 m deep while the passengers were watching the sea lions on the port side. As the vessel was departingFootnote 7 toward the north side of the reef, the master and one deckhand heard a noise and looked aft, at which time they saw a large breaking wave bearing down on the vessel's starboard quarter. The top of the wave was reported to be above the flying bridge. The master reached for the throttles in an attempt to turn the vessel to port so that the vessel would encounter the wave on the stern. However, at that moment, the wave struck the vessel's starboard quarter, causing the vessel to broachFootnote 8 and rapidly capsize. The vessel settled in an inverted position; its approximate location was 49°10.854' N, 126°04.938' W (Appendix B).
As the vessel capsized, one deckhand and most of the passengers fell into the water. The master and the other deckhand were initially trapped inside the flying bridge. Some of the passengers had been taking photographs on the top deck when the wave struck, and they slid down the deck as the vessel capsized, hitting railings, seats, and other objects before entering the water. Since they had not expected to enter the water, some passengers ingested sea water upon being submerged. The passengers were submerged for times varying from a few seconds up to 1 minute. Many struggled to expel the salt water they had ingested on entering the water, some had lost glasses (including the masterFootnote 9 and 1 of the deckhands), and some were weighed down by clothing and footwear.
The sea conditions, exacerbated by the wave action in the vicinity, made it difficult for the passengers to keep their heads and mouths above water. Some passengers found objects to hold onto to help keep them afloat, such as an anti-exposure suit, a canister, a paddle, and some seat covers. While afloat in the water, a number of the survivors encountered petroleum products that had spilled out from the overturned vessel.Footnote 10
The master and 1 deckhand successfully deployed one of the life rafts that had floated free from the vessel. They boarded the life raft and then assisted 3 passengers who were in the water nearby to also board the life raft. The other deckhand assisted a group of passengers in the water and later boarded the life raft. Concerned that the vessel would sink and drag the raft down, the crew cut the painter that was attaching the life raft to the vessel, and then attempted to manoeuvre the life raft toward the passengers.
Two of the passengers were in the lower cabin when the vessel capsized, and 2 other passengers found themselves in the lower cabin shortly after the capsizing. One of the passengers in the lower cabin made her way into the cabin from the main deck, and she and her husband both made their way out via the stairwell, surfacing near the life raft. The crew members then helped them board the life raft.
One of the other passengers in the lower cabin attempted to break the windows to escape, as the cabin was filling up with water. Having failed to break the windows, the 3 remaining passengers in the lower cabin eventually made their way into the wheelhouse, opened one of the doors, and escaped through it.Footnote 11 Once free of the vessel, 2 of the passengers held onto a child-sized lifejacket for flotation, while the third held onto the vessel.
Two additional passengers were able to swim to the life raft, while 8 passengers stayed afloat in the water with the assistance of a life ring. The crew found it difficult to paddle the life raft effectively in the prevailing conditions. They continued to encourage passengers in the water to swim towards the life raft. They also attempted to comfort the passengers in the life raft and distributed thermal protective aidsFootnote 12 to them. The crew managed to activate one of the hand flares that was contained in the emergency pack stowed within the raft.
Approximately 20 minutes after the capsizing, the deckhands spotted a rocket flare floating in the water in the vicinity of the life raft. They were able to retrieve it and activate it, attracting the attention of an Ahousaht First Nation fishing vessel that was hauling lines in the vicinity of Bartlett Island. After hauling their line, the fishermen proceeded toward the flare to investigate.
As they approached the area of the occurrence, the fishermen saw the Leviathan II's capsized hull and people in the water. They immediately requested assistance from other vessels in the area on VHF channel 68, which is the channel used by the Ahousaht First Nation. The Canadian Coast Guard (CCG) lifeboat station at Tofino was monitoring the channel and, when it heard the call, deployed a fast rescue craft, Tofino1.
A few minutes later, at 1546, the fishermen notified the CCG of the situation on VHF channel 16, which is used for distress communications. Marine Communications and Traffic Services (MCTS) Prince Rupert, which responded to the call, initially had difficulty identifying the occurrence location, as the clarity of the radio communications was poorFootnote 13 and MCTS staff were unfamiliar with the local nameFootnote 14 by which the fishermen referred to the location. The officer-in-charge on the Tofino1, who was familiar with the area, heard the confusion between MCTS and the fishermen on the radio and stopped his transit briefly to clarify the occurrence location for MCTS. At 1553, MCTS Prince Rupert broadcast a Mayday Relay.
The Joint Rescue Coordination Centre in Victoria tasked 2 search-and-rescue (SAR) aircraft and 4 CCG vessels to assist with the rescue. The Royal Canadian Mounted Police and several small craft also responded to the Mayday Relay. Twenty-one survivors were rescued and transferred to Tofino, where they were attended to by emergency health services. Some of the passengers suffered from hypothermia, ranging from mild to severe. Five bodies were recovered on the day of the occurrence and, at approximately 2335, the CCG lifeboat Cape Ann towed the partially submerged vessel and securely anchored it in sheltered waters north of Vargas Island. The body of one remaining passenger was found on 18 November 2015.
1.6 Vessel certification and inspections
The Leviathan II was certified, manned, and equipped in accordance with existing regulations. The vessel held 3 safe manning documents issued by Transport Canada (TC), allowing it to operate with different crew complements, depending on the number of passengers.
The vessel also held a valid TC inspection certificate and had been last inspected in February 2015. The certificate had the following conditions attached to it: the vessel must operate within 5 nautical miles from shore, in favourable weather, not shipping seas, and with passenger distribution in accordance with the stability document.
1.7 Personnel certification and experience
The master held a Limited Master 60, gross tonnage, certificate, first issued in 1999. The certificate was valid until April 2019 and was limited to vessels operated by Jamie's Whaling Station remaining within 25 nautical miles of the British Columbia coast. The master also held a Small Vessel Machinery Operator certificate, limited to passenger vessels with engine power less than 750 kW engaged on a limited, near-coastal class 2 or sheltered waters voyage. Additionally, the master held Marine Advanced First Aid and Marine Emergency Duties (MED) A1 and A2 certificates. The master had started his career in the marine industry in 1974, when he began working on fishing vessels, and had worked as master on whale-watching vessels since 1997. He was hired by Jamie's Whaling Station in 1998 and, between March and October each year since then, he had routinely conducted tours that included observing wildlife at Plover Reefs.
One of the deckhands had started working in the marine industry in 2003 and had been working as a deckhand on whale-watching vessels with Jamie's Whaling Station since 2012. This deckhand had obtained a Small Vessel Operator Proficiency certificate in 2014 and also held a Radiotelephone Restricted Operator's Certificate (Maritime), as well as Marine Basic First Aid and MED A3 certificates.
The other deckhand had started working with Jamie's Whaling Station on whale-watching vessels in 2014 and held a Marine Basic First Aid certificate, as well as MED A1 and MED A3 certificates.
1.8 Damage to the vessel
The vessel was raised to the surface on 29 October 2015. The machinery, fuel, piping systems, navigation equipment, electrical systems, and accommodation fittings had been contaminated by salt water. Structural damage also occurred during the recovery process, and the vessel was declared a total loss by the insurers.
1.9 Post-occurrence examination
Subsequent examination of the recovered vessel identified the following:
- The hull and fittings showed no sign of having permitted water ingress before the capsizing.
- Bilge-pumping systems were in place, and piping appeared undamaged.
- The fuel tank contained sea water with a light petroleum sheen on the surface.
- The seals and closing arrangements for the doors leading into the wheelhouse and cabin were intact.
- The safety glass for numerous portholes in the lower cabin and wheelhouse was shattered, as was the safety glass on the top of the viewing ports.
The chart plotter was disconnected by divers during the recovery of the vessel and was sent to the Transportation Safety Board of Canada (TSB) Engineering Laboratory in Ottawa, Ontario, where position and track information stored in the unit's memory was retrieved.
1.10 Damage to the environment
Approximately 2000 litres of diesel fuel and a small quantity of engine oil leaked into the water as a result of the capsizing. Most of the fuel dissipated with wave and wind action.
1.11 Fatalities and injuries
| Crew | Passengers | Total | |
|---|---|---|---|
| Fatalities | 0 | 6 | 6 |
| Serious injuries* | 0 | 4 | 4 |
| Minor / no injuries | 3 | 14 | 17 |
| Total | 3 | 24 | 27 |
* Under section 1 of the Transportation Safety Board Regulations, serious injuries include internal organ injuries; bone fractures (excluding simple fractures of nose, fingers, and toes); lacerations that cause severe hemorrhage or nerve, muscle, or tendon damage; or injuries that are likely to require hospitalization.
Of the passengers who died, 5 had been situated on the top deck at the time of the occurrence, and 1 had been situated on the main deck (Appendix C). It was reported that 5 were seen in an unresponsive state in the first few minutes following the capsizing, and the sixth passenger was seen within 20 to 30 minutes.
1.12 Environmental conditions
At the time and location of the occurrence, the wind was estimated to be 10 knots from the southeast, and wave conditions were a 2 m swell from the same direction. Conditions were overcast, the sea water temperature was 14 °C, and the tide was ebbing. The previous observedFootnote 15 high water was at 1131, with a water level of 3.86 m. The subsequent low water was at 1755, with an observed water level of 0.84 m.
Archived records of the significant wave height and maximum wave height recorded at the La Perouse Bank weather buoy are available from the Department of Fisheries and OceansFootnote 16 and are depicted in Figure 2. The Environment Canada wave-height forecastFootnote 17 includes the following warning:
1.13 Breaking waves
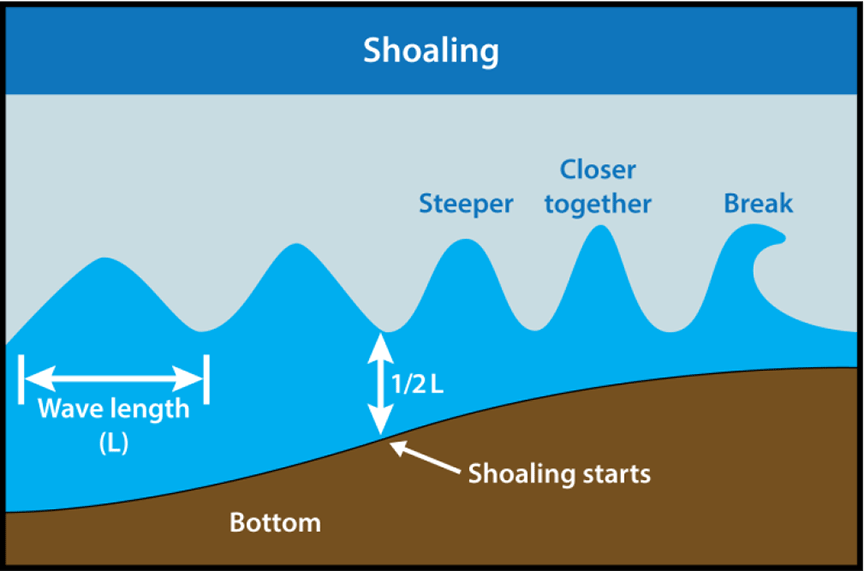
A breaking wave is a type of wave that rises up, pitches forward, and breaks into surf. Breaking waves can be caused by shoaling, which occurs when deep-water waves approach a shallow area or "shoal." In this situation, the waves slow down as they encounter water depths that are less than half their wave length (L) (Figure 3). As the waves slow down, their crests become closer together, and the waves become higher and steeper. When these waves are about as high as the water is deep, they pitch forward and break (Figure 3).
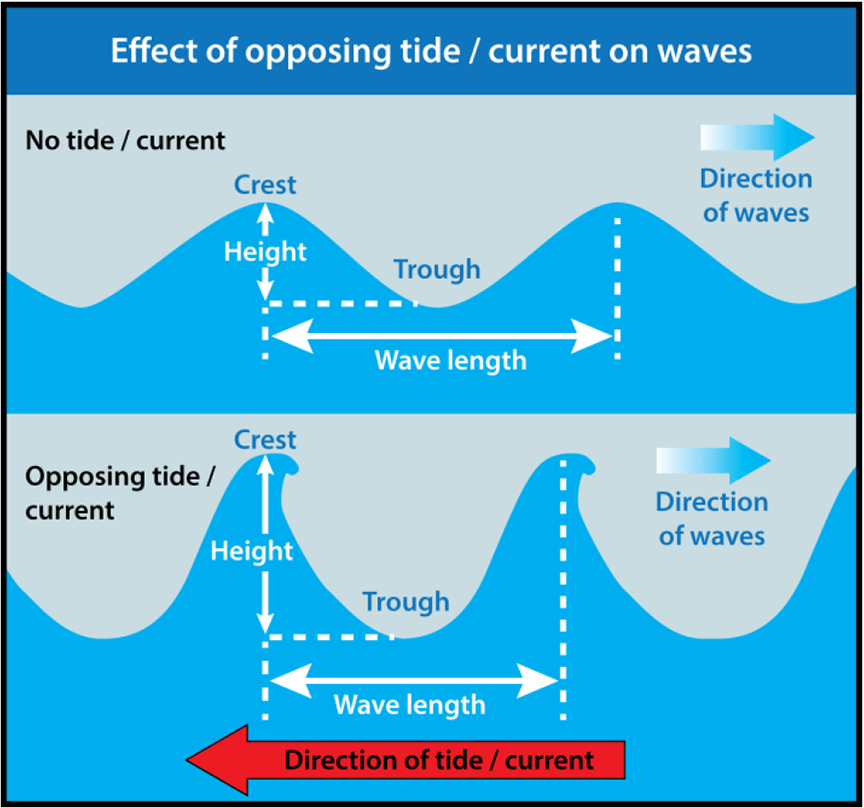
Opposing tides and currents flowing against waves are other factors that cause wave length to decrease and wave height to increase (Figure 4). In these conditions, waves rapidly become steeper, increasing the likelihood that they will break.
1.14 Lifesaving equipment
TC required the Leviathan II to carry lifesaving equipment for 50 people. At the time of the occurrence, the vessel was carrying all of the required equipment, including
- 52 adult lifejackets (for a body mass of greater than 40 kg)
- 12 child lifejackets (for a body mass of 40 kg or less)
- 4 life rings
- 2 life rafts with a 25-person capacity, each with an emergency pack
- 6 Type A rocket flaresFootnote 18
- 6 Type C hand flaresFootnote 19
- an aluminum skiff with an outboard motor
In addition to these items, the vessel carried 2 anti-exposure suits and 3 inflatable lifejackets for use by the crew.
The lifesaving equipment on the Leviathan II was distributed throughout the vessel in accordance with the lifesaving equipment plan (Appendix D). The lifejackets were stowed in lockers under the passenger seats on the main deck. Both life rafts had last undergone annual servicing on 06 February 2015, per the mandatory schedule. The forward life raft was resting in deep chocks and the aft life raft was strapped down in a cradle on the main deck. The aft life raft was fitted with a hydrostatic release unit, which is a pressure-activated release mechanism designed to operate when submerged to a depth of about 4 m.Footnote 20
The forward life raft had a Class B (Canadian) emergency pack, while the aft life raft was equipped with a Class B (Safety of Life at Sea [SOLAS]) emergency pack.Footnote 21 Among other things, these emergency packs contain distress-signalling equipment. The Canadian pack contains 6 Type C hand flares. The SOLAS pack contains 2 Type A rocket flares, 3 Type C hand flares, and a Type D buoyant smoke float,Footnote 22 in addition to a radar reflector.
The Canadian Life Saving Appliance Standard (TP14475), published by TC in 2010, no longer includes Canadian-specific emergency packs for life rafts on vessels such as the Leviathan II. The standard requires such vessels to be fitted with life rafts that are equipped with SOLAS emergency packs. However, life rafts approved before the standard was published continue to be accepted by TC until they are retired from service.
The vessel had a muster list posted in the galley that specified duties for crew in emergency situations and carried a first aid kit that was stowed in a locker in the wheelhouse.
1.15 Donning of flotation aids
There are currently no regulations within Canada regarding the donning of flotation aids or lifejackets for passengers while on board vessels greater than 15, gross tonnage, carrying more than 12 passengers. The LeviathanII is within this class of vessel. TC indicates that wearing a flotation aid while on an open deck of a small passenger vesselFootnote 23 is prudent but optional.Footnote 24 TC also cautions about wearing standard lifejackets inside enclosed spaces, as this could impede escape in case of an emergency.Footnote 25
By comparison, passenger vessels under 15, gross tonnage, carrying up to 12 passengers, when not equipped with a life raft and operating in water less than 15 °C (such as an RHIB engaged on a whale-watching tour) are required, under the Small Vessel Regulations, to carry equipment on board or establish procedures to protect all persons from the effects of hypothermia or cold shock resulting from swamping, capsizing, or falling overboard. For RHIBs used in whale watching, it is common for companies to require their passengers to wear an anti-exposure suit, and this was the practice as well at Jamie's Whaling Station.
In 2010, TC and the Canadian Red Cross Society published a report entitled Boating Immersion and Trauma Deaths in Canada: 16 Years of Research.Footnote 26 While the report focused mainly on recreational boating incidents, it included research data involving all deaths on boats in Canada. The report concluded that a vast majority of boating fatalities could be prevented, and identified mandatory wearing of appropriate flotation devices as the single most effective initiative for preventing boating fatalities. Death can occur rapidly if an individual has not donned a flotation device to keep the individual's head above water.Footnote 27
1.15.1 United States small passenger vessel regulations on personal flotation
In the United States, the 1996 amendmentsFootnote 28 to federal regulations that apply to small passenger vesselsFootnote 29 specify that the master must require passengers to wear personal flotation devices when possible hazards exist, including
- when transiting hazardous bars or inlets;
- during severe weather;
- in the event of flooding, fire, or other events that may call for evacuation; and
- when the vessel is being towed, except during the towing of a non–self-propelled vessel under normal operating conditions.
The amendments are based on recommendations from the National Transportation Safety Board following 3 occurrencesFootnote 30 involving charter fishing vessels that broached and/or capsized.
On 17 June 2003, the United States Coast Guard issued a safety alert regarding the wearing of flotation devices following the Taki-Too occurrence, in which a 32-foot charter fishing vessel capsized while crossing a bar, resulting in 9 people drowning and 2 going missing. The alert reiterated the regulations requiring the master of a vessel to require passengers to don flotation devices when possible hazardous conditions exist. The alert noted that wearing a flotation aid in such circumstances is "similar to wearing seatbelts during aircraft take-offs and landings and periods of turbulence" and that "the best time to don a life jacket is before it is needed—before people are in the water."
1.16 Cold-water immersion
Sudden, unexpected immersion in cold water causes the human body to react in 4 stages. The first stage, known as cold water shock, can last up to 2 minutes. Cold water shock consists of an immediate large gasp reflex, followed by hyperventilation and a massive increase in heart rate and blood pressure. The second stage, cold incapacitation, begins after 5 to 30 minutes in the water. At this stage, the individual begins to lose the ability to swim, as the limbs are subject to local muscle cooling and the muscles and joints become stiffer. The fine muscles of the hands may be the first to be affected, reducing the individual's ability to don or hold onto a flotation device within as little as 10 to 15 minutes.Footnote 31 Even strong swimmers can succumb to cold incapacitation.
After approximately 30 minutes in the water, the third stage, hypothermia, begins to set in, resulting in a reduction of blood flow to the hands, feet, and surface of the body; intense shivering in the early stages but a lack of shivering in the later stages; loss of consciousness; and eventually heart failure. A fourth stage, known as post-rescue collapse, may occur. When survivors are pulled from the water, the loss of hydrostatic pressure to the body causes a sudden drop in blood pressure, resulting in heart or brain failure. Further, as the body warms up, blood begins to flow more freely, which can result in fatal bleeding from internal or external injuries.Footnote 32
Water is often considered cold at temperatures lower than 15° C,Footnote 33Footnote 34Footnote 35 although some consider cold water as lower than 21° CFootnote 36 or even 25° C.Footnote 37 At the time of this occurrence, the water temperature was approximately 14° C. According to WorkSafeBC, "cold shock (stage 1) and swimming failure [cold incapacitation] (stage 2) are responsible for more drowning fatalities in British Columbia than hypothermia (stage 3) or post-rescue collapse (stage 4)."Footnote 38
1.17 Automatic distress alerting
An EPIRB is designed to transmit a distress signal to SAR authorities in an emergency. EPIRBs can be manually activated, or can float free and automatically transmit a signal and provide continuous position updates and homing-in capabilities when a vessel sinks. The Leviathan II was not equipped with an EPIRB, nor is one required by current regulations for this class of vessel.
On 22 March 1998, the whale-watching vessel Ocean Thunder, which was operated by the same company as the Leviathan II, was swamped and 2 lives were lost. The TSB investigation into this occurrence found that the absence of a requirement for an EPIRB may have precluded a timely SAR response and so adversely affected the success of the SAR mission.Footnote 39 The coroner also made a recommendation to TC that each operator carry EPIRBs. The company subsequently installed EPIRBs on all of its vessels. However, the EPIRBs were reported to have frequently transmitted false alerts and were removed from the vessels when the batteries came up for renewal.
Previous TSB investigations have identified that carrying an EPIRB can contribute to saving lives,Footnote 40 and the 2013 Spring Report of the Auditor General of Canada contained the following recommendation:
Footnote 41In response, TC has proposed to expand requirements to carry an EPIRB. At the national Canadian Marine Advisory Council meeting in April 2016, TC updated industry on the proposed Navigation Safety Regulations, which are expected to be completed in 2018. Under the revised regulations, which would consolidate the Ship Station (Radio) Regulations 1999, among others, vessels would be required to carry EPIRBs when operating outside of sheltered waters if the vessel is more than 8 m in length, is carrying more than 6 passengers, or is a tug/tow boat.
1.18 Vessel position monitoring
1.18.1 Company call-back system
The company had a call-back system in place to monitor vessels when they were operating offshore. The staff at the front desk was required to check in with vessels by VHF radiotelephone every 20 to 30 minutes and to record the vessels' position details in the radio log. A note on the radio log specified the procedure for sending out a DSC position request, which was to be initiated if there were 3 unsuccessful attempts to hail a vessel on the radio. Checking in with the vessels was one of a variety of tasks performed by front desk staff, who were also responsible for attending to customers, answering the telephone, and checking passengers in before a tour.
The company used a private VHF channel for communication between the front desk and company. The vessels also monitored channel 18, which is used by whale-watching fleets operating in the Tofino area, and channel 16, which is the distress calling channel. They also scanned other channels to gather local information to assist with the tours.
At times, vessels or front desk staff did not adhere strictly to the check-in frequency of 20 to 30 minutes. This was sometimes the case when masters were occupied with other duties, including manoeuvring the vessel, providing tour information, or communicating with other vessels and monitoring other channels on the radio. The staff at the front desk sometimes also missed scheduled calls while busy attending to passengers on the telephone or in person.
On the day of the occurrence, the last communication between the Leviathan II and the front desk was at about 1445, when the vessel departed Ahous Bay for Plover Reefs. After receiving no response from the vessel at 1530, the front desk transmitted a DSC position request to the vessel and attempted to contact the crew on their cell phones. After having no success, the front desk staff notified the operations and safety coordinator at approximately 1553. As they were doing so, they heard the Mayday Relay concerning the Leviathan II being broadcast by MCTS on VHF channel 16.
1.18.2 Vessel Traffic Services
One of the functions of MCTS is to provide Vessel Traffic Services (VTS) to vessels operating in Canadian waters. VTS provide a means of exchanging information between vessels and a shore-based centre. Participation is mandatory for most vessels greater than 20 m, but vessels less than 20 m may participate voluntarily. Participating vessels are required to report to MCTS when departing, when passing a designated calling-in point (CIP), and when arriving. Reports include the particulars of the vessel, routing, and the vessel's estimated time of arrival at the next CIP.
Vessels that participate are tracked by MCTS in the Vessel Traffic Management Information System using a combination of radar (when the vessel is operating within a radar zone) and automatic identification system (AIS),Footnote 42 where available.
If a signal is lost with a vessel that was previously being tracked, the MCTS officer attempts to establish communication with the vessel using all available means. If the vessel's signal has been lost for more than 15 minutes and attempts to contact the vessel fail, the situation is reported to the Joint Rescue Coordination Centre.
The Leviathan II was not participating in VTS and was not equipped with an AIS, nor were these required by regulation.
1.19 Modifications
After entering service in 1996, the Leviathan II underwent various structural and mechanical modifications and additions that included the following:
- The heat exchangers for the engine cooling system were replaced with an aluminum-channel keel-cooling system.
- A header tank for fresh water was installed on the starboard side of the main deck.
- An RHIB on the top deck was replaced with a 12-foot aluminum boat.
- A 25‑person inflatable life raft, which had been secured on the top deck, was removed from service.
- The flying bridge on the top deck was enclosed by an aluminum structure with glass windows to provide protection from the elements.
- A tank for fresh water was installed on the starboard side of the engine room, just below deck level, to service the marine head.
A declaration of modification history, submitted by the owners to TC in March 2011, did not mention any modifications.
1.20 Vessel stability
1.20.1 Leviathan II stability information
Following its rebuild in 1996, the Leviathan II was subjected to an inclining experiment to determine its lightship weightFootnote 43 and centre of gravity. Subsequently, a stability booklet was prepared according to TC requirements.Footnote 44
One of the introductory sections of the booklet was entitled "Good Seamanship" and included advice for the master on actions to take to address conditions that might affect vessel stability, such as properly stowing equipment to avoid shifting while at sea, and minimizing snow and ice accretion on exposed decks. Vessel operational limits and guidance with respect to environmental conditions were addressed by the following warning, which was taken directly from the TC standards:
Footnote 45In addition to a report of the inclining experiment, the booklet provided detailed stability calculations for various combinations of passenger and consumable loads, as well as assessments of those results against the TC standards.
The stability booklet for the Leviathan II was approved by TC on 12 December 1996, and a copy was stored on board the vessel.
1.20.2 TSB stability assessment
In order to assess the stability of the Leviathan II at the time of the occurrence and factors that may have affected it, the TSB developed a detailed computer model of the vessel and performed various stability calculations. The conclusions of this TSB stability assessmentFootnote 46 are as follows:
- The modifications that were made to the vessel since it entered service in 1996 resulted in a small change to the estimated lightship weight and centre of gravity and did not have a significant impact on the stability of the vessel.
- With consumables, passengers, and crew distributed as at the time of the occurrence, the vessel's stability met and exceeded TC stability standards for normal operating conditions.
- The results of the stability assessment with applied waves are consistent with the observed behaviour of the vessel at the time of the occurrence; that is, a rapid capsizing to port after having been struck on the starboard quarter by a large steep wave. The evaluation did not point to passenger load and distribution as being a likely factor affecting the outcome of the occurrence, nor were any other possible contributing factors identified, such as water ingress.
- The stability standards established by TC do not explicitly evaluate a vessel's risk when operating in a wave environment. Although compliance with the standards implies a measure of safety against capsizing in a seaway, the standards do not address exposure to extreme circumstances such as large breaking waves or surf-like conditions. In this regard, TC stability standards are consistent with international standards in warning vessel masters that operational measures must be taken to mitigate the risk of capsizing according to the prevailing circumstances.
- The results highlight the significance of encounter angle as a factor affecting the vessel's stability in waves. Specifically, the risk of capsizing is significantly reduced when the encounter angle is such that the vessel is meeting the wave head on.
- The risk associated with the absence of specific passenger controls for the Leviathan II in normal operating conditions was evaluated as low.
1.21 Management of safety
1.21.1 Safety management systems and risk assessment
The principal objective of a safety management system (SMS) on board a vessel is to ensure safety at sea, prevent human injury or loss of life, and avoid damage to property and the environment. Ideally, safety management involves individuals at all levels of an organization and fosters a systematic approach to the identification and mitigation of operational risks.
Elements of an effective SMS include
- operating procedures for the vessel and the use of checklists;
- maintenance procedures for the vessel and its associated equipment;
- documentation and record-keeping procedures;
- procedures for identifying hazards and managing risks;
- procedures to prepare for, and respond to, emergency situations; and
- drills, training, and familiarization for the vessel's crew.
Of these elements, the identification and mitigation of risk are central. According to the International Association of Classification Societies (IACS):
Footnote 47Another IACS documentFootnote 48 describes the characteristics of effective risk assessment methods:
- While methods may be more or less formal, they must be systematic to be effective. In other words, there must be an assessment process in place that can be consistently applied.
- The results of a risk assessment must be documented, so that there is evidence of the decision-making process being applied.
- Risk should be reduced to a level that is as low as reasonably practicable. This level is achieved when all reasonably practicable mitigating measures for identified hazards are in place.
- Those involved in the risk assessment should be those most familiar with the operation.
- Risk assessments must be updated as required, with new or infrequent activities being specific triggers for a risk assessment.
In Canada, passenger vessels carrying more than 12 passengers on an international voyage subject to the SOLAS Convention are required to develop a formal SMS.Footnote 49 This SMS must be certified and audited by a recognized organization. The Leviathan II did not operate under a certified SMS, nor was it required to by regulation.
1.21.2 TSB risk assessment
Risk assessment is the process of estimating and evaluating the level of risk associated with a hazard. The TSB uses a risk assessment methodology that involves determining risk by
- identifying the adverse consequence(s) associated with the hazard;
- assessing the probability of the adverse consequence(s);
- assessing the potential severity of the adverse consequence(s); and
- assigning the risk level using a risk matrix (Appendix E).
The TSB evaluated the risk associated with a passenger vessel capsizing in steep, breaking waves in coastal waters such as Plover Reefs by considering the probability and severity of this event over time—specifically, over the life of an individual vessel or fleet of similar vessels. Although a capsizing was deemed likely only on an "occasional" basis (over the past 25 years, this is the third capsizing in the area), the potential severity of the consequences was deemed "catastrophic." Applying these parameters to the risk matrix results in a qualitative risk assessment of "high" (Appendix E).
1.21.3 Company safety management
The company conducted health and safety meetings that were attended by department heads. The health and safety meetings covered operational and maintenance issues concerning the vessels, as well as the office buildings and property managed by the company. Additionally, driver and deckhand meetings were conducted once or twice per season, and crew members were required to attend. Topics of discussion included issues relating to the vessels such as maintenance, health and safety, log books, injury reports, and tours.
The company conducted biweekly safety drills on board the Leviathan II, during which the crew members practised drills to respond to various emergency scenarios such as fire, abandon ship, and man overboard. The crew would occasionally launch the skiff for practice as part of such drills. Records of drills conducted were maintained by the company. The company required masters to maintain a log book and report incidents and maintenance issues in a timely fashion.
The company also had a manual called Front Office Policies, primarily intended to instruct staff on shore in company procedures relating to administrative, sales, and other general duties and expectations. With respect to vessel operations, the "Radio Communications" section of the manual described the company call-back system, and the "Safety" section included some instructions for vessel crew, such as the requirements to give safety briefings to the passengers, to ensure that the passenger count on board was consistent with office records, and to be mindful of and correct any unsafe behaviours or conditions immediately. With respect to operational decisions, the "Safety" section of Front Office Policies included the following instructions:
Use common sense when deciding if a trip is doable.
[…]
Skippers will have the final say on whether a trip goes out in open waters or does an inlet explorer trip.
The manual also stated that the company had a risk assessment committee that met monthly and that the reports were available from these meetings. However, no formal risk assessments were provided to the TSB.
Jamie's Whaling Station Ltd. is also a founding member of the Pacific Rim Association of Tour Operators (PRATO). This is a group that meets informally once or twice a year to discuss operations, mainly focusing on the safety of the wildlife being viewed.
1.22 Medical examination of seafarers
Seafarers are required to undergo regular marine medical examinations to ensure that they are fit to perform duties on Canadian vessels. Examinations are conducted by marine medical examiners (MME), who are physicians designated by TC. MMEs are required to assess the seafarer's health against the standards set out by TC in Seafarer Medical Examinations: A Physician GuideFootnote 50 and to obtain any relevant documentation in order to make a proper assessment with regard to the examinee's medical condition and public safety.
Based on the examination, the MME deems the seafarer fit, fit with limitations, or unfit. If a seafarer is deemed fit or fit with limitations, the MME issues a provisional medical certificate that is valid for 6 months. During this time, the TC Marine Medical Unit independently reviews the file and, if the seafarer meets the standards, an official Marine Medical CertificateFootnote 51 is issued by the Minister of Transport. This certificate is valid for a maximum of 2 years.
During an examination, the MME can ask for information, perform standardized tests, and conduct a physical examination of the seafarer. MMEs also rely on the seafarer to self-report medication use and medical conditions. For this reason, the Canada Shipping Act, 2001Footnote 52 requires seafarers to be complete and accurate in reporting their medical conditions. Self-reporting enables the MME to ascertain whether a specialist is required for more in-depth examination to determine whether a seafarer meets certain medical standards. Since 2009, 3 TSB marine investigations have identified issues with respect to self-reporting of medical conditions.Footnote 53
1.22.1 Medical condition of the master
Before the occurrence, the master had last undergone a TC marine medical examination in 2014, when he had been assessed as fit for duty with corrective lenses required. For this examination and for each of his TC medical examinations dating back to 2003, the master's visual acuity and eye health was assessed as meeting the requirements. His unaided vision was assessed to be within but on the limit of 20/200, his visual acuity and visual fields were within limits, and there was no information documented concerning any progressive eye disease. The generic eye health questions that MMEs ask during marine medical examinations were all marked negative or no, and the master had signed all of the examination forms declaring that the information was complete and accurate. After his 2012 examination, TC had sent the master a letter indicating that his unaided vision was on the limit of the required standard.
The master had privately seen various eye specialists between 2009 and 2014, but none of the eye specialists' reports or the documentation from the master's personal physician referred to the master's certificate of competency. Following the occurrence, the TSB requested an independent ophthalmologist's review of the master's medical records. This review concluded that the master had an eye condition that would have made it difficult for him to acquire a normal visual image in all parts of his visual field. The review also concluded that there were discrepancies between the master's test results for unaided vision obtained during private eye examinations and those obtained during TC marine medical examinations.
1.23 TSB Watchlist
Safety management and oversight will remain on the TSB Watchlist until
- Transport Canada implements regulations requiring all commercial operators in the air and marine industries to have formal safety management processes and effectively oversees these processes;
- transportation companies that do have SMS demonstrate that it is working—that hazards are being identified and effective risk-mitigation measures are being implemented; and
- Transport Canada not only intervenes when companies are unable to manage safety effectively, but does so in a way that succeeds in changing unsafe operating practices.
The TSB Watchlist identifies the key safety issues that need to be addressed to make Canada's transportation system even safer.
Safety management and oversight is a 2016 Watchlist issue. As this occurrence demonstrates, some transportation companies are not effectively managing their safety risks, and TC oversight and intervention has not always proven effective at changing companies' unsafe operating practices.
1.24 Previous occurrences
On 02 April 1992, a small, open charter boatFootnote 54 rented out of Ucluelet, British Columbia, was on a whale-watching trip when the vessel was overturned by a very high breaking wave at the entrance to Barkley Sound. The occurrence resulted in 2 fatalities.
On 22 March 1998, a whale-watching passenger RHIB operated by Jamie's Whaling Station was swamped and heeled severely while off Plover Reefs, throwing all of the crew and passengers on board into the water. The occurrence resulted in 2 fatalities. The TSB investigation reportFootnote 55 concluded that a factor contributing to the occurrence was that the operator did not fully appreciate the conditions the vessel would encounter in turbulent waters in the vicinity of the reefs at the time of the accident. A report by the Coroners Serviceof British Columbia made several recommendations, including that operators have a periodic reporting schedule as well as carrying EPIRBs and/or pairing vessels in a buddy system.
On 02 August 2010, the sports fishing vessel QualicumRivers9 (C16465BC)Footnote 56 capsized in Quatsino Sound, British Columbia, resulting in 4 fatalities. Although the vessel was equipped with a sufficient number of lifejackets, none of the 4 occupants were wearing them at the time of the occurrence.
1.25 Outstanding recommendations
On 23 June 2002, following an occurrence in which the amphibious passenger vehicle LadyDuck took on water and sank in the Ottawa River and 4 passengers drowned,Footnote 57 the Board recommended that
The Department of Transport take steps to ensure that small passenger enterprises have a safety management system.
Transportation Safety Recommendation M04-01
This recommendation is currently assessed as Unsatisfactory.Footnote 58 The TSB has repeatedly identified the need for domestic vessels to have an effective SMS, an issue that has been on the TSB's Watchlist since 2010. The Board has noted that effective oversight of SMSes by TC is not always provided, and that an SMS is not required for some companies. To address this safety issue, the Board also noted the following:
Footnote 59The addition of this item to the Watchlist was the result of a number of investigationsFootnote 60 in which the Board found hazards and risks in the operation of a vessel that had either not been identified or not been addressed by the operator. Other investigationsFootnote 61 have also addressed shortcomings in the implementation of SMS, in which operators had not identified hazards associated with an operation, resulting in a lack of mitigation strategies for those hazards.
In 2014, TC updated industry on the proposed Safety Management Regulations, which would apply to 3 groups of vessels and the companies that manage them. Tier 1 would include SOLAS convention vessels, Tier 2 would include non-convention vessels over 500, gross tonnage, and Tier 3 would include non-convention vessels over 24 m in length and less than 500, gross tonnage. Vessels such as the Leviathan II would continue to remain outside the purview of these proposed regulations.
1.26 TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP252/2015 – Analysis of Contaminants
- LP255/2015 – NVM Downloads
- LP245/2015 – Laser Survey of Leviathan II
2.0 Analysis
2.1 Factors leading to the capsizing and loss of life
While the Leviathan II was at Plover Reefs to allow the passengers to view sea lions, the vessel maintained a position on the weather side of the reef, exposed to the incoming swell. As the vessel was leaving the area, a large wave approached the vessel from the starboard quarter. Moments before it struck the vessel, the master heard a noise that caused him to look aft and notice the wave. However, by this point, the wave was breaking and it was too late to realign the vessel in order to minimize the impact of the wave. The Transportation Safety Board of Canada (TSB) stability assessment supports the conclusion that the forces exerted on the vessel by this wave were sufficient to overcome the stability of the vessel and cause it to capsize; no other significant factors contributing to the capsizing were identified.
The rapid nature of the capsizing prevented the passengers and crew from donning flotation aids or thermal protective devices before entering the water. Given that the water temperature was 14° C, passengers and crew were immediately subjected to the effects of cold water immersion. Five of the 6 deceased passengers were reported to have been incapacitated within the first few minutes, and the 6th passenger within 20 to 30 minutes; these deaths likely occurred as a result of stage 1 (cold shock) and stage 2 (cold incapacitation) of cold water immersion.
The crew did not have time to transmit a distress signal before the capsizing, and the vessel was not fitted with a means to automatically signal distress. As a result, approximately 45 minutes elapsed before search-and-rescue (SAR) resources became aware of the capsizing. A nearby Ahousaht First Nation fishing vessel was instrumental in saving the lives of a number of survivors; if not for the fishing vessel's response, it is likely that more of the passengers in the water would have suffered hypothermia and/or died.
2.2 Risk assessment
The risk associated with company operations in the area around Plover Reefs is high. Providing passengers with a wildlife viewing experience in this area means that vessels may be operating in conditions that have the potential to generate hazardous waves. Although during the tourist season the predominant swell direction at Plover Reefs is from the west, effectively sheltering the area south of the reefs, it is uncertain that this will be the case on any given day. Given the tidal effects and water depths in the area around Plover Reefs, when the reefs are exposed to offshore swell, there is the potential for steep, breaking waves to form. The consequences of exposure to this type of wave could be catastrophic for small shallow-draft vessels, as was the case in this occurrence as well as the occurrence involving the Ocean Thunder in 1998. The nature of the sea and the processes that combine to form breaking waves in shallow areas are so unpredictable that it is not feasible to precisely forecast the height and steepness of waves coming from offshore at Plover Reefs. It is also not feasible to predict the response of a vessel to a breaking wave. Accordingly, it is necessary to implement operational measures to mitigate this risk.
When the Leviathan II arrived at Plover Reefs to view the sea lions, several conditions supporting the formation of breaking waves were present: the swell was coming from the southeast, travelling over the rising ocean floor, and meeting an opposing tide as it approached the rocks. Although the master was aware of these conditions, he did not observe any waves actually breaking in the area, other than those along the reef itself. Based on the conditions at the time, the master deemed it safe to operate the vessel on the weather side of the reef, and during these operations, the vessel took on a position and heading that exposed the vessel's starboard quarter to the incoming waves.
The company had not established guidelines addressing the potential formation of breaking waves when offshore swell was present to help its masters determine whether it was safe to operate on the weather side of Plover Reefs. Instead, it relied on each individual master's experience and judgment to mitigate this risk inherent in the company's operation. The masters had developed some informal practices, such as checking the significant wave height and period data at the La Perouse Bank weather buoy, communicating with other vessels in the area, and conducting an assessment of observed conditions during their approach.
Given the potential for breaking waves that could overcome the stability of shallow-draft vessels, other measures to mitigate the risk could be taken, such as
- approaching the reefs from the sheltered side or, if the conditions are not favourable, avoiding the area altogether;
- keeping a vigilant lookout and ensuring the vessel maintains a safe angle of encounter with any oncoming swell to minimize its effect on the vessel's stability; and
- ensuring that the vessel has a safe route away from the hazardous area.
Although the vessel's inspection certificate from Transport Canada (TC) included a limitation related to environmental conditions, this limitation was intended to ensure a measure of safety while transiting in open water and was not relevant to the specific hazard of exposure to extreme sea conditions such as breaking waves. Similarly, the warning in the stability book is of a general nature that is equally applicable to all vessels. As noted previously, the hazard posed by breaking waves is specific to an area of operation and must be managed consistently and effectively by the company, first, by implementing measures to ensure that the risk is identified on an ongoing basis and, then, by clarifying the actions to mitigate it.
In this occurrence, the measures taken by the company did not mitigate the risks associated with the hazard posed by sea conditions in the area of operation. There are approximately 9 whale-watching companies operating out of Tofino and Ucluelet, all of which operate in the same area as the LeviathanII and may be exposed to similar hazards. Beyond that, passenger vessels operating along the west coast of Vancouver Island may also be in areas that pose similar hazards, such as Barkley Sound and Quatsino Sound, which were the sites of previous occurrences involving fatalities.Footnote 62 Considering that there is no regulatory requirement for companies that operate domestic passenger vessels to develop formal safety management processes with associated risk assessment processes, there is the potential for other vessels and passengers to be exposed to hazardous environmental conditions without adequate mitigation measures being taken.
If companies that operate passenger vessels do not implement risk management processes to identify and address environmental hazards in their area of operation, such as the potential formation of breaking waves, then there is a risk of a similar capsizing and loss of life.
2.3 Donning of flotation aids
In the event of sudden and unexpected immersion in cold water, a flotation aid such as a lifejacket or personal flotation device (PFD) improves chances of survival by keeping a person's head above the water and reducing the need to swim. This is particularly critical if an individual is injured, unconscious, or incapacitated by the effects of cold water immersion. A flotation aid is most effective when it is worn before entering the water. Donning a flotation aid following an event such as capsizing or falling overboard becomes increasingly difficult, because a flotation aid may not be readily accessible or because the individual may be hindered by physical ability, injuries, and/or the mental confusion or shock that ensues after sudden and unexpected immersion. What was deemed a simple task on board may become an insurmountable challenge in cold water.
Although the Leviathan II was equipped with a sufficient number of lifejackets, the capsizing happened rapidly, and none of the passengers or crew had time to don the lifejackets before entering the water. The passengers were of varying ages and levels of physical ability, and some had sustained injuries during the capsizing. While most of the survivors were able to find objects in the water to keep them afloat, some of these makeshift flotation aids, which included a canister, paddle, seat covers, and a life ring, would have done little to keep the survivor's head above the water and reduce the need to swim in the way that a lifejacket or PFD is designed to do. Additionally, survivors were faced with the challenge of having to hold onto these objects, whereas a lifejacket or PFD would have kept them afloat even when the effects of cold water immersion rendered them no longer able to hold onto objects or unconscious.
The type of vessel, the nature of the operations, and the conditions encountered are all factors to be considered when assessing risks to passengers and safety precautions that should be taken to protect them during a voyage. On a rigid-hull inflatable boat (RHIB), for example, the risk of a passenger falling overboard is greater given the open style of the vessel. Therefore, operators are required, by regulation, to carry equipment on board or establish procedures to protect all persons from the effects of hypothermia or cold shock resulting from swamping, capsizing, or falling overboard. On a passenger vessel such as the Leviathan II, there are other factors to consider, such as the fact that some passengers may be on the open top deck while others are in the enclosed cabin during a voyage. Each location on the vessel poses different risks to the passengers; the passengers on the top deck may be more likely to fall overboard, whereas the passengers in the cabin may be at risk of entrapment if they are wearing a standard lifejacket at the time of a capsizing. The nature of the operations (sheltered water cruise versus whale-watching on the open ocean) must also be considered when assessing risk, along with the conditions encountered during the voyage (e.g., hazardous bars or inlets, severe weather).
There is currently no regulatory framework in Canada for small passenger vessels such as the Leviathan II with regard to donning flotation aids, nor is there a requirement for companies to assess their operations to identify under which conditions flotation aids should be worn during a voyage. As a consequence, it is uncommon for companies operating this class of vessel to require passengers to don flotation aids at any point during a voyage, even in conditions when passengers may be at increased risk (such as seated on an open deck while the vessel is operating in rough weather, navigating close to reefs, etc.).
If there is no requirement for companies to assess their operations to determine under which conditions flotation aids should be worn, there remains a risk that passengers on this class of vessel will be deprived of the benefits of a flotation aid in the event of sudden and unexpected immersion in cold water.
2.4 Distress alerting
In cold Canadian waters, the success of a SAR mission often depends upon prompt notification of SAR authorities about the vessel's position and other relevant information and upon the prompt tasking of SAR resources. Having the means to immediately alert authorities is therefore critical in enabling a quick response and increasing survival. Vessels in the area must also report sightings of flares or other distress signals to SAR authorities as soon as possible.
In this occurrence, the speed of the capsizing meant that the crew did not have time to transmit a distress call by the very high frequency (VHF) digital selective calling (DSC) radiotelephone. As well, once in the water, the crew had limited options to signal for help. The Leviathan II did not carry an emergency position-indicating radio beacon (EPIRB), nor was the vessel required to under existing regulations. However, carrying an EPIRB provides a means to immediately alert authorities of an emergency. A float-free EPIRB, which is designed to transmit a distress signal automatically when submerged, is especially useful in situations when crew are unable, or have insufficient time, to send out a distress call by other means, such as VHF/DSC radiotelephone or flares. Following the capsizing, approximately 20 minutes elapsed before a distress signal could be successfully transmitted, and approximately 45 minutes elapsed before SAR resources became aware of the emergency. During this time, a number of the survivors were in the cold water without proper flotation devices, hindering their chances of survival.
If vessels do not have effective means to promptly notify SAR authorities of an emergency, especially in a capsizing situation, there is a risk of a delay in SAR response that will hinder the survival chances of passengers and crew.
After the capsizing, the crew had attempted to signal for help using a hand flare from the Class B (Canadian) emergency pack in the life raft; however, hand flares have a limited range and are mainly used for drawing the attention of searching vessels when already in sight. They have limited effectiveness as an initial distress signal. Although the capsizing occurred less than 5 nautical miles from the shore, the crew was unable to attract the attention of vessels in the vicinity by discharging the hand flare.
The Leviathan II voluntarily carried a Class B (Safety of Life at Sea [SOLAS]) emergency pack in its other life raft; however, this life raft was not the one that the crew members managed to deploy during the occurrence. The Class B (SOLAS) emergency pack contained 2 parachute rockets and 1 buoyant smoke float, in addition to hand flares. Parachute rockets and buoyant smoke floats have a greater range of visibility and are therefore more effective for initially signalling distress. It was only after a parachute rocket was, by chance, recovered from the debris floating free of the vessel that the crew could successfully signal for assistance.
The vessel that first sighted the parachute rocket from the Leviathan II responded to the distress signal and was instrumental in saving the lives of a number of survivors. The first instinct for a vessel that sights a distress signal is often to proceed closer to investigate the source and to lend a hand if needed. A good practice is for vessels to report distress signal sightings to SAR resources immediately, as this can expedite SAR resources that are specially equipped to provide emergency assistance.
2.5 Collection and verification of seafarer medical data
Both the marine medical examiner (MME) and the seafarer have obligations in ensuring that a marine medical examination is comprehensive; the MME is responsible for collecting sufficient medical information to substantiate the outcome of the assessment, while the seafarer is obligated to disclose any medications or medical conditions that may be of relevance. TC also has a responsibility to review each MME assessment before issuing a marine medical certificate.
During the course of the investigation, the TSB examined the medical records of the crew members and identified that the master's personal medical records contained information about his eye health were not included in his records with TC. Additionally, the master's test results for unaided vision obtained during his private visits to eye specialists and optometrists differed from results obtained by TC during marine medical examinations.
The following factors contributed to TC being unaware of the master's eye condition:
- The master had not disclosed to the MME his specialist visits to optometrists and an ophthalmologist. This may be due partly to the master being unaware that his eye condition was of the type that needed to be disclosed. As well, seafarers may not disclose medical conditions out of concern that they will lose their medical certificates and, by extension, their employment.
- Certain eye conditions are difficult for MMEs to detect subjectively, and objective testing for specific vision conditions is not part of marine medical examinations. Without access to the master's personal medical records, the MME had limited means to detect the eye condition.
Because TC was not fully aware of the status of the master's vision, there was no opportunity for follow-up by the regulator to determine the extent to which it may have affected his fitness for duty. Furthermore, despite TC knowing that the master was on the limit of the TC standard for unaided vision, no further steps had been taken to monitor the status of the master's vision (such as increasing the frequency of testing or requiring a specialist assessment), thereby missing an opportunity to identify any decline in his vision.
If seafarers do not fully disclose medical information, and MMEs do not request supporting data, medical files may be incomplete, increasing the risk that seafarers will carry out their duties when not medically fit.
Furthermore, although the master's eyesight was not causal in the occurrence, there was a discrepancy between test results for unaided vision obtained privately and those obtained during TC medical examinations.
3.0 Findings
3.1 Findings as to causes and contributing factors
- While the Leviathan II was at Plover Reefs, the conditions were favourable for the formation of breaking waves.
- The vessel maintained position on the weather side of the reef, exposed to the incoming swell, to allow passengers to view wildlife. As the vessel was leaving the area, a large wave approached the vessel from the starboard quarter.
- Moments before the wave struck, the master became aware of it and attempted to realign the vessel to minimize its impact, but there was not enough time for his actions to be effective.
- The forces exerted on the vessel by this large breaking wave caused it to broach and rapidly capsize.
- The rapid capsizing resulted in the passengers and crew falling into the cold sea water without flotation aids or thermal protection, exposing them to the effects of cold water immersion.
- Approximately 45 minutes elapsed before search-and-rescue (SAR) resources became aware of the capsizing, as the crew did not have time to transmit a distress call before the capsizing, nor did the vessel have a means to automatically send a distress call.
- The crew members were able to discharge a parachute rocket, which alerted a nearby Ahousaht First Nation fishing vessel that was instrumental in saving the lives of a number of survivors.
3.2 Findings as to risk
- If companies that operate passenger vessels do not implement risk management processes to identify and address environmental hazards in their area of operation, such as the potential formation of breaking waves, then there is a risk of a similar capsizing and loss of life.
- If there is no requirement for companies to assess their operations to determine under which conditions flotation aids should be worn, there remains a risk that passengers on this class of vessel will be deprived of the benefits of a flotation aid in the event of sudden and unexpected immersion in cold water.
- If vessels do not have effective means to promptly notify SAR authorities of an emergency, especially in capsizing situations, there is a risk of a delay in SAR response that will hinder the survival chances of passengers and crew.
- If seafarers do not fully disclose medical information, and marine medical examiners do not request supporting data, medical files may be incomplete, increasing the risk that seafarers will carry out their duties when not medically fit.
3.3 Other findings
- The life raft deployed in the occurrence was fitted with a Class B (Canadian) emergency pack, which did not contain devices effective for initially signalling distress, such as a parachute rocket or buoyant smoke float.
- Although the master's eyesight was not causal in the occurrence, there was a discrepancy between test results for unaided vision obtained privately and those obtained during TC medical examinations.
4.0 Safety action
4.1 Safety action taken
4.1.1 Coastal Nations Search and Rescue Initiative
Following the occurrence, the Canadian Coast Guard (CCG) Search and Rescue (SAR) program increased the scope of outreach with remote First Nation communities on the British Columbia coast. Members of the Ahousaht and Tla-o-qui-aht First Nations participated in 2 days of SAR training led by the CCG at the Tofino Lifeboat Station. Representatives from the Tofino Royal Canadian Mounted Police, Parks Canada, Westcoast Inland SAR, and Royal Canadian Marine SAR Station 38 - Ucluelet also attended the training, which involved classroom theory and on-water exercises.
4.1.2 Transport Canada
In May 2016, the Transportation Safety Board of Canada sent Marine Safety Advisory Letter 01/16 to advise Transport Canada (TC) of observations made during the investigation concerning the medical condition of the master. TC subsequently reviewed the master's medical file and requested that the master provide TC with additional medical information related to his vision. The master was deemed fit by TC to hold a Marine Medical Certificate with the limitation "corrective lens required."
4.1.3 Jamie's Whaling Station
After receiving input from the managers and staff, the company established the following additional safety measures for the 2016 season:
- a simplified 30-minute call-in procedure with a timer fitted in the office;
- modifications to the vessels' storage lockers to permit lifejackets to float free in the event of a sudden capsizing;
- additional free-floating life rings and emergency position-indicating radio beacons on vessels;
- a requirement for passengers to don manually inflating personal flotation devices (other than on rigid-hull inflatable boats); and
- improvements to the launching capabilities of life rafts on 2 of the vessels.
Since the occurrence, the company has begun to formalize its safety management practices and to establish more formalized communication procedures regarding weather and sea-condition standards for tours among members of the Pacific Rim Association of Tour Operators.
4.2 Safety action required
4.2.1 Hazard identification, risk assessment, and risk mitigation (risk management)
4.2.1.1 Risk management of passenger vessel operations on the west coast of Vancouver Island
Although the predominant swell direction at Plover Reefs during the tourist season is from the west, effectively sheltering the area south of the reefs, there can be no certainty that this will be the case on any given day. Given the tidal effects and water depths of the area around Plover Reefs, when exposed to offshore swell, there is the potential for steep, breaking waves to form. The consequences of exposure to this type of wave could be catastrophic for small shallow-draft vessels, as they were in this occurrence as well as the occurrence involving the Ocean Thunder in 1998.
The nature of the sea and the processes that combine to form breaking waves in shallow areas are so unpredictable that it is not feasible to precisely forecast the height and steepness of waves coming from offshore at Plover Reefs. It is also not feasible to predict the response of a vessel to a breaking wave.
While vessels may encounter such hazardous waves only occasionally, the consequences could be catastrophic. Therefore, the level of risk associated with this hazard was determined to be high for the Leviathan II as well as for its passengers and crew. Accordingly, it is necessary to implement operational measures to mitigate this risk, such as by
- approaching the reefs from the sheltered side or, if the conditions are not favourable, avoiding the area altogether;
- keeping a vigilant lookout and ensuring the vessel maintains a safe angle of encounter with oncoming swell to minimize its effect on the vessel's stability; and
- ensure that the vessel has a safe route away from the hazardous area.
In this occurrence, the measures taken by the company did not mitigate the risks associated with the hazard posed by sea conditions in the area of operation.
There are approximately 9 whale-watching companies operating out of Tofino and Ucluelet, all of which operate in the same area as the Leviathan II and may be exposed to similar hazards. Two other passenger vessels, in addition to the LeviathanII, have been overcome by hazardous waves in the area of Clayoquot Sound and Barkley Sound since 1992, resulting in 10 fatalities. Beyond that, passenger vessels operating along the west coast of Vancouver Island may also be in areas that pose similar hazards.
The first vessel, a 5.8 m open recreational boat rented by a group of 4 people on a whale-watching trip, was overturned by a very high, breaking wave while off Mara Rock, Barkley Sound, British Columbia. All 4 occupants were thrown into the water, and there were 2 fatalities. The TSB investigationFootnote 63 determined that the vessel had capsized when overwhelmed by a high, breaking wave.
The second vessel, Ocean Thunder, departed Tofino, British Columbia, with 3 passengers and an operator (coxswain) on board for a 3-hour trip to watch marine life in the vicinity of Plover Reefs. While in that area, a large swell swamped and broached the vessel, throwing all of the occupants into the turbulent water and resulting in 2 fatalities. The TSB investigationFootnote 64 determined that one factor contributing to the occurrence was that the operator did not fully appreciate the dangerous conditions the vessel would meet at the time and location of the accident.
The formation of these hazardous waves depends on the combination of sea conditions and other factors, so the safety of operations in these areas must be managed systematically by the authorized representative in conjunction with the vessel's master. This management is achieved by continuously monitoring the conditions before and during the voyage, and by clarifying actions to mitigate the hazards of breaking waves in conditions favourable to the formation of these waves.
However, any encounter with such a hazardous wave has the potential for catastrophic outcome. Although measures to improve survivability must still be considered and implemented, the risk would be most effectively mitigated by reducing the likelihood of encountering the wave entirely.
Voyage planningFootnote 65 is one such mitigation process; it consists of taking into account elements such as weather, tides, and navigation dangers, and making a contingency plan and sail plan before setting off on a voyage. The degree of voyage planning necessary for small vessels depends on the size of the vessel, its crew, and the length of the voyage.
In this occurrence, the company had not established guidelines to address the potential formation of breaking waves. Instead, it relied on individual masters' experience and judgment to mitigate this inherent risk. If companies that operate passenger vessels off the west coast of Vancouver Island do not implement risk management processes to identify and address environmental hazards in their area of operation, such as the potential formation of breaking waves, then there is a risk of a similar capsizing and loss of life.
Therefore, the Board recommends that
The Department of Transport ensure that commercial passenger vessel operators on the west coast of Vancouver Island identify areas and conditions conducive to the formation of hazardous waves and adopt practical risk mitigation strategies to reduce the likelihood that a passenger vessel will encounter such conditions.
Transportation Safety Recommendation M17-01
4.2.1.2 Explicit requirements and guidance for implementation of risk management processes
In Canada, there are approximately 4000 registered passenger vessels. These vessels carry passengers on various types of voyages, ranging from ferry crossings and water-taxi transits to dinner cruises and whale-watching trips. Passengers on board these vessels may have varying ages, levels of ability, language needs, and even special needs such as impairments in hearing, sight, or mobility. As passengers are also likely to be unfamiliar with marine emergency procedures and survival techniques, they are especially vulnerable in a marine emergency.
Depending on the marine environment in which a passenger vessel is operating, it may be subject to any number of hazards. These hazards may result in marine emergencies such as fire, collision, person overboard, grounding, swamping, and capsizing. Although a marine emergency on a passenger vessel may be infrequent, encountering one could put the lives of passengers and crew at risk, with catastrophic results. This makes the risks associated with such operations high.
It is therefore essential that operators of passenger vessels be cognizant of the risks involved in their operations and proactively manage them through the effective implementation of risk management processes, by reducing risks to the lowest possible level. An effective risk management process will help vessel operators identify and evaluate hazards, establish safe operating procedures and policies to mitigate those identified risks, and provide a means to ensure that risks are assessed on an ongoing basis. A fully documented and systematic approach also helps to ensure that individuals at all levels of the organization, including the master, have the knowledge and tools to effectively manage risks, as well as the necessary information to make sound decisions in any operating condition.
Risk management is a key component of a safety management system (SMS). Following an occurrence in 2002, in which the amphibious passenger vehicle LadyDuck sank in the Ottawa River and 4 passengers drowned,Footnote 66 the Board recommended that
The Department of Transport take steps to ensure that small passenger enterprises have a safety management system.
Transportation Safety Recommendation M04-01
TC does not plan to require operators of small vessels (those less than 24 m in length and carrying fewer than 50 passengers) to adopt an SMS. According to TC, safety concerns for this class of vessels are addressed through existing regulations, inspections, and awareness initiatives, including the voluntary Small Vessel Compliance Programfor vessels under 15, gross tonnage.
The Board's assessment of TC's response is currently Unsatisfactory.Footnote 67
Since Recommendation M04-01 was made, the Board has found deficiencies regarding hazard identification and risk management in a number of other occurrencesFootnote 68 involving Canadian passenger vessels. The issue of safety management processes has been on the TSB WatchlistFootnote 69 since 2010. The Watchlist notes that
- there is a lack of a clear regulatory framework requiring all companies to implement formal safety management processes;
- there have been many investigations in which it was found that safety management processes were weak or not used; and
- TC oversight has not identified companies' ineffective processes or intervened when necessary; in addition, there is an imbalance between auditing processes and traditional inspections.
In the current Canadian regulatory framework, there are 2 provisions that address the need for an SMS and/or risk management process.Footnote 70 First, the Safety Management Regulations require those Canadian vessels to which chapter 9 of SOLASFootnote 71 applies to implement an SMS that is compliant with the ISM Code.Footnote 72 Second, the Canada Shipping Act, 2001 requires that procedures be developed for the safe operation of vessels and for dealing with emergencies.Footnote 73
However, these provisions have not been effective in ensuring that all Canadian passenger vessel operators implement risk assessment processes that effectively identify hazards and mitigate risk on an ongoing basis.
In the first case, the Safety Management Regulations refer to the ISM Code, under which the need for specific risk management processes is only implied. According to the Code, the "safety management objectives of the company should […] assess all identified risks to its ships, personnel and the environment and establish appropriate safeguards."Footnote 74 Although separate guidelines published by the International Association of Classification Societies (IACS) suggest that risk assessment is essential to ensure compliance with the Code, and that the method used must be systematic and documented,Footnote 75 the ISM Code itself does not provide any explicit requirements for risk management or elaborate any particular approach to the management of risk.
Furthermore, TSB investigations have found that, despite some vessel operators having an audited and certified SMS, they may not have structured and systematic risk assessment processes in place.
For example, the passenger ferry Jiimaan operated under an SMS that was certified and audited by a recognized classification society. The TSB investigation into the vessel's groundingFootnote 76 found that the absence of a risk assessment process within the company's SMS resulted in risks not being identified and mitigated. The investigation also found that the company's proposed risk assessment process (following an external audit of its SMS in 2011) did not reflect the principles for an effective risk assessment process as described by IACS. However, the vessel's proposed risk assessment process was found to be acceptable to the classification society when it conducted an ISM Code audit.
The passenger ferry Princess of Acadia also operated under a certified and audited SMS when it grounded on approach to the dock. The TSB investigationFootnote 77 found that the SMS did not provide guidance for the master to proactively identify risks and investigate hazardous occurrences, a factor increasing the risk in the vessel's operation.
To help small vessel operators comply with SMS requirements, Transport Canada has developed plain-language Safety Management Systems guidelines,Footnote 78 including sample SMS documentation.Footnote 79 These guidelines describe risk management in general terms, encouraging the use of a reporting process for the ongoing identification of hazards and a "risk register" to document the implementation and monitoring of risk controls. Although these guidelines go some way toward ensuring that all passenger vessel operators have implemented systematic processes to manage risks in their operations, there are some key shortcomings that limit their effectiveness:
- These guidelines are targeted to those vessel operators who may be implementing an SMS on a voluntary basis. Current regulatory requirements require mandatory SMS only for vessels operating on international voyages.
- Many of the "hazards" listed in the sample risk register are actually possible outcomes (such as collision/grounding, fire, environmental) or are general references to types of hazards (such as machinery spaces, water). Since the examples do not identify specific hazards that could contribute to these outcomes (such as high-traffic area on approach to dock, silting of navigable channel, or deterioration of insulation), targeted measures to reduce the likelihood of an occurrence are not identified.
In the second case, with respect to the Canada Shipping Act, 2001, paragraph 106(1)(b) concerns the requirement to develop procedures for the safe operation of vessels and for dealing with emergencies applies to all Canadian vessels, including those that are not required to implement an SMS, such as the Leviathan II. Although TC may consider risk management to be implicit in the requirement to "develop safe operating procedures," it is vague. There are no explanatory guidelines or standards concerning implementation of section 106 provided for either vessel operators or TC inspectors. Although TC inspectors may check that there are safe operating procedures on board a vessel, they do not evaluate the procedures themselves or the process by which the procedures were developed. The Leviathan II was inspected regularly but did not have any such procedures on board. Following this occurrence, it had not, at the time of publication of this report, incorporated formal risk management techniques to identify and mitigate hazards posed in the area of operation.
In TSB investigations that have identified issues with risk management on passenger vessels (including in this occurrence), there is clearly a fundamental difference between knowing about the existence of a hazard and having the capacity, as an organization, to fully "identify" it as such and then to systematically manage it. Furthermore, the IACS guidelines point to hazard identification as the first and most important step in risk assessment.Footnote 80
Other maritime administrations have taken steps to ensure that risk management processes are implemented in a meaningful way. For example, the Australian Maritime Safety Authority (AMSA) has regulations that explicitly require vessel owners and operators to implement a risk management process to ensure the operational safety of domestic commercial vessels, as part of an SMS. In addition, the AMSA has published detailed and thorough guidelinesFootnote 81 to accompany the regulations that provide guidance for implementing a risk management process. These guidelines
- are presented in a user-friendly format and written in clear language;
- describe the theory of hazard identification and risk assessment/mitigation;
- provide operators with useful information and tools to help them put the theory of risk management into practice on board their vessel;
- emphasize that the risk management process must be ongoing (addressing previously unanticipated hazards as they arise) and be kept up-to-date (regularly, or as circumstances change);
- highlight the benefits of conducting meaningful risk management exercises;
- make significant use of examples; and
- draw attention to the need to examine the specifics of all vessel operations, including normal and emergency situations.
In Canada, although TC provides guidance for SMS, the need for a comprehensive risk assessment process is not clearly stated, and guidance to the industry on how to implement such a process in their operations is minimal.
Risk management processes are considered a critical means of managing safety on board passenger vessels. As well, clear requirements and guidelines are needed to assist vessel operators and TC inspectors in the implementation and oversight of such processes.
Therefore, the Board recommends that
The Department of Transport require commercial passenger vessel operators to adopt explicit risk management processes, and develop comprehensive guidelines to be used by vessel operators and Transport Canada inspectors to assist them in the implementation and oversight of those processes.
Transportation Safety Recommendation M17-02
4.2.2 Automatic distress alerting
In an emergency situation in which a vessel rapidly capsizes or sinks, the survival of passengers and crew often depends on the successful transmission of a distress signal to search-and-rescue (SAR) resources. Although passenger vessels are required to carry distress-alerting equipment such as very high frequency (VHF) radio transceivers, VHF radiotelephones with digital selective calling, and pyrotechnics, this equipment relies on manual activation by a crew member to initiate the distress signal.
As previous investigations have shown, crew members may not be able to manually transmit a distress signal in an emergency situation for a number of reasons:
- they may not have enough time;
- they may be preoccupied with any number of urgent tasks and not transmit a signal when the opportunity exists; or
- they may find themselves unable to access the distress-alerting device when they are able to signal distress.
In recognition of these shortcomings, some vessels are required to carry an emergency position-indication radio beacon (EPIRB) that deploys automatically when immersed in water and emits a continuous signal to alert SAR resources. An EPIRB that is programmed and registered provides SAR resources with the vessel's position and an identifier that gives the SAR controller valuable information about the vessel and the owner. As SAR resources travel to the occurrence site, the EPIRB continues to transmit its position, allowing SAR resources to home in on the location, thus substantially reducing search time and improving the probability of survival. This is a critical feature that is not available with manually activated distress equipment, such as a VHF/digital selective calling radiotelephone, which could become inaccessible or non-operational if a vessel capsizes or sinks, making it impossible for the crew to provide ongoing position information to SAR resources.
Current Canadian regulations do not require all passenger vessels to be equipped with an EPIRB. A passenger vessel such as the Leviathan II, for example, which is limited to home trade, Class III voyages,Footnote 82 is not required to carry an EPIRB. Only those vessels engaged in voyages beyond home trade, Class III (those travelling more than 20 nautical miles from shore) are required to carry one.
The TSB has issued 2 previous recommendations following occurrences in which vessels carrying passengers were in an emergency situation but were unable to transmit a distress signal.
The first recommendation was issued as a result of an occurrence involving the charter boat 25K6527,Footnote 83 which was overturned by a large breaking wave near Barkley Sound, British Columbia, while on a whale-watching trip in April 1992. The occurrence resulted in 2 fatalities. There was no distress call from the vessel, and rescue efforts began only after the vessel was reported as overdue by the company. Following this occurrence, the Board recommended that
The Department of Transport encourage all charter vessel operators to equip their vessels with life-saving and emergency communication and/or signalling equipment suitable for the type of operation.
Transportation Safety Recommendation M94-03
The second recommendation was issued with regard to the passenger vessel True North II,Footnote 84 whichwas swamped by a series of waves while operating in inland waters on 16 June 2000. The vessel took on water, downflooded, and sank in Georgian Bay, Ontario, resulting in 2 fatalities. Although the vessel was equipped with a VHF radiotelephone, the speed with which the vessel sank prevented a distress transmission. The rescue effort began only when SAR authorities were informed of the accident by a passing vessel. Following this occurrence, the Board recommended that
The Department of Transport require small passenger vessels to provide pre-departure briefings, and to be equipped with a life raft that is readily deployable, lifesaving equipment that is easily accessible, and the means to immediately alert others of an emergency situation.
Transportation Safety Recommendation M01-03
TC subsequently amended regulations to require all passenger vessels to be equipped with a VHF radiotelephone and for those carrying more than 6 passengers operating beyond sheltered waters to carry a VHF radiotelephone equipped with digital selective calling. The assessment of the response to these recommendations is Fully Satisfactory.Footnote 85
The 2013 Spring Report of the Auditor General of Canada noted that emergency beacons help identify the location of a marine incident and reduce the time for SAR crews to find survivors. It therefore made the following recommendation:Footnote 86
Additionally, coroners have recommended that an EPIRB be carried following the fatalities that resulted after the swamping of the passenger vessel Ocean ThunderFootnote 87 and the fishing vessel Brier Mist.Footnote 88 Despite the coroner's recommendations, some passenger vessels (those travelling less than 20 nautical miles from shore) are still not required to carry EPIRBs.
In the case of the Leviathan II, it was largely due to fortunate circumstances that the crew were able to retrieve a flare from the water and use it as a distress signal, which was subsequently observed by a vessel fishing in the area; otherwise, the number of fatalities could have been greater.
In addition to the occurrence involving the Leviathan II, the TSB is aware of 11 other occurrencesFootnote 89 involving fatalities in which vessels were in distress within 20 nautical miles of shore and were unable to transmit a distress alert promptly. As a result, SAR efforts were delayed or not initiated.
At the national Canadian Marine Advisory Council meeting in April 2016, TC updated industry on the proposed Navigation Safety Regulations, which are expected to be completed by 2018. If put into effect, the revised regulations will consolidate the Ship Station (Radio) Regulations 1999, among others, and require that vessels carry EPIRBs when operating outside of sheltered waters if more than 8 m in length; when carrying more than 6 passengers; or if the vessel is a tug/tow boat.
In the meantime, passengers travelling on vessels not equipped with EPIRBs continue to be exposed to additional risk, even when the vessels operate close to the shore, and would benefit from the requirement for vessels to have a distress-alerting capability that does not rely on human intervention to be activated. Furthermore, in capsizing or sinking situations, passengers forced into the water or onto a survival craft should have the capability to continuously update SAR resources on their position, as the effects of the wind and current may cause them to drift. The proposed amendments by TC fall short of addressing the risk to passenger vessels less than 8 m carrying up to 6 passengers while operating beyond sheltered waters, as observed in the 2 occurrencesFootnote 90 in which no distress signal was received.
Therefore, the Board recommends that
The Department of Transport expedite the proposed changes to the Navigation Safety Regulations and expand its current emergency position-indicating radio beacon (EPIRB) carriage requirements to require that all commercial passenger vessels operating beyond sheltered waters carry an EPIRB, or other appropriate equipment that floats free, automatically activates, alerts search-and-rescue resources, and provides continuous position updates and homing-in capabilities.
Transportation Safety Recommendation M17-03
This report concludes the Transportation Safety Board's investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .
Correction
A sentence in the 10th paragraph of section 1.5 History of the voyage has been amended. The text in the initially released report read:
"The other deckhand assisted a group of passengers in the water, but was separated from the group when struck by another large wave; the deckhand then swam to the life raft and boarded it."
It now reads:
"The other deckhand assisted a group of passengers in the water and later boarded the life raft."
This correction was approved by the Board on ; the corrected version of the report was released on .
Appendices
Appendix A – General arrangement of the Leviathan II
DK = deck; ER = engine room; P = port; S = starboard.
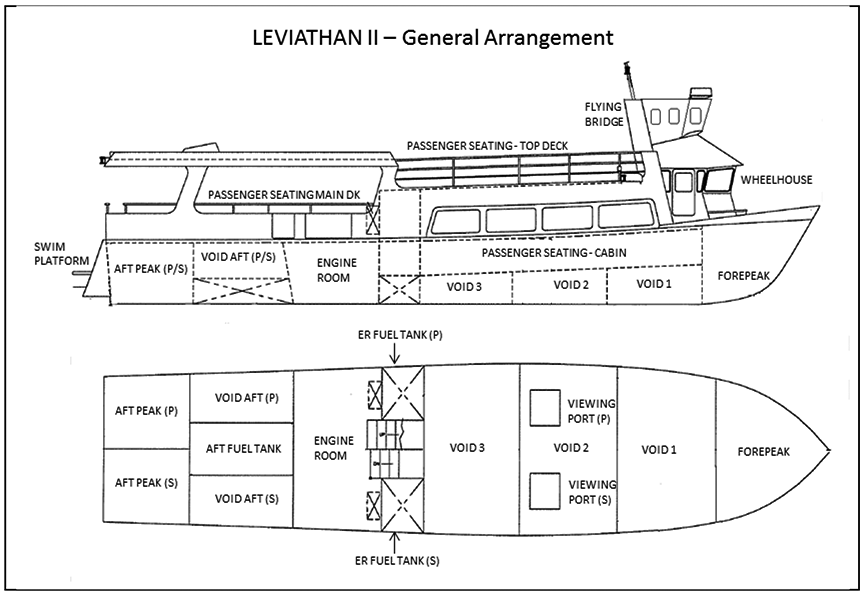
Appendix B – Area of the occurrence
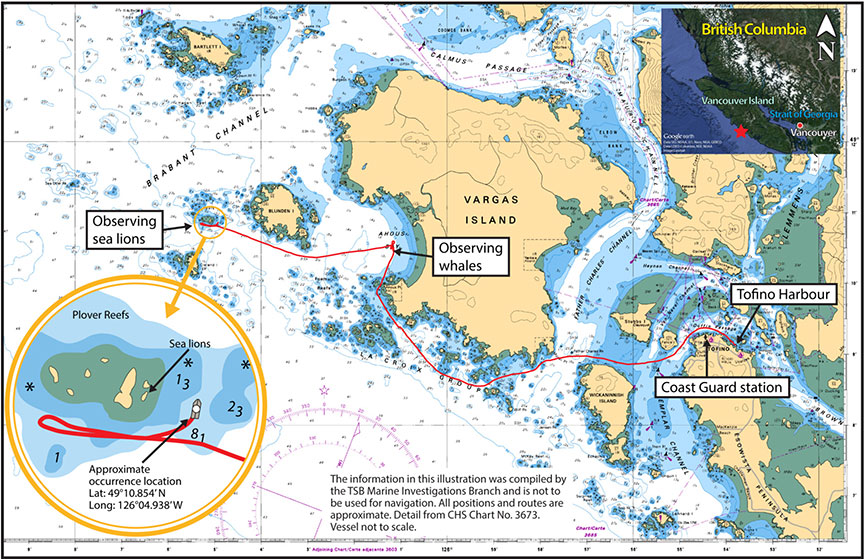
Appendix C – Approximate locations of passengers and crew before the capsizing
Source: Leviathan II stability booklet, with location of passengers and crew overlaid by TSB.
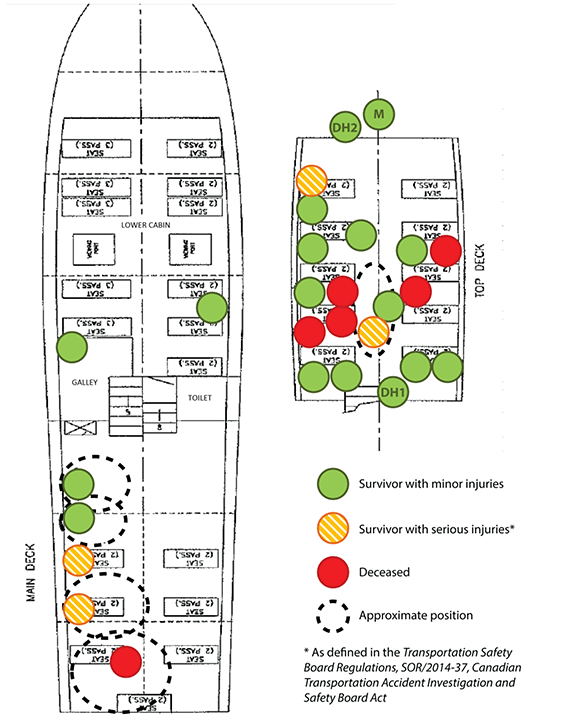
Appendix D – Lifesaving equipment plan
PAX = Passengers
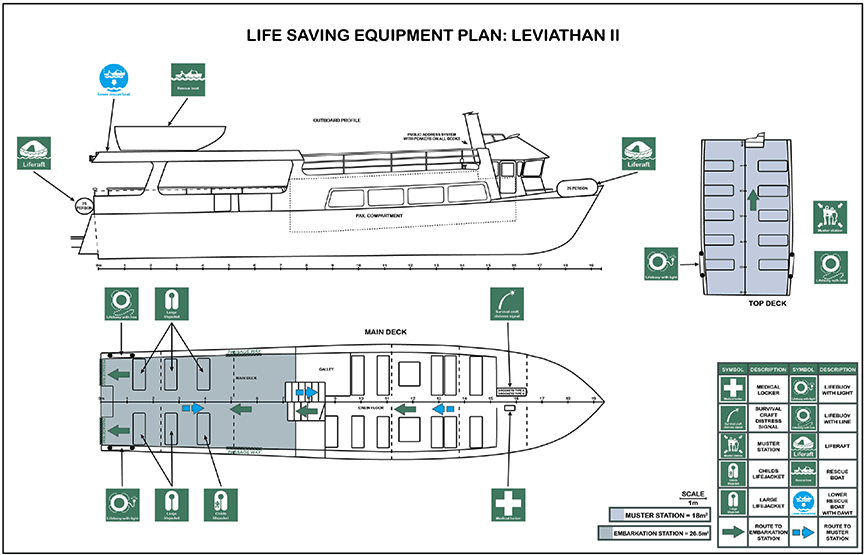
Appendix E – Risk matrix
| Severity of consequence | Probability of adverse consequences (over time) |
||||
|---|---|---|---|---|---|
| Frequent | Probable | Occasional | Unlikely | Most improbable | |
| Catastrophic | High | High | High | Medium | Medium-low |
| Major | High | High | High-medium | Medium | Low |
| Moderate | High | Medium | Medium | Medium-low | Low |
| Negligible | Low | Low | Low | Low | Low |
Definitions of probabilities of adverse consequence:
- Frequent: Likely to occur often during the life of an individual system, or occur very often in the operation of a large fleet of similar systems.
- Probable: Likely to occur several times during the life of an individual system, or occur often in the operation of a large fleet of similar systems.
- Occasional: Likely to occur sometimes in the life of an individual item or system, or will occur several times in the life of a large fleet, similar items, components, or systems.
- Unlikely: Unlikely but possible to occur sometime in the life of an individual item or system, or can reasonably be expected to occur in the life of a large fleet, similar items, components, or systems.
- Most improbable: So unlikely to occur in the life of an item or system that it may be assumed not to recur, or it may be possible but extremely unlikely to occur in the life of a large fleet, similar items, components, or systems.
Definitions of severity of adverse consequence:
- Catastrophic: Death or loss of system or plant, such that significant loss of production, significant public interest, or regulatory intervention occurs or reasonably could occur.
- Major: Severe injury, major system damage, or other event that causes some loss of production, that affects more than one department, or that could have resulted in catastrophic consequences under different circumstances.
- Moderate: Minor injury, minor system damage, or other event, generally confined to one department.
- Negligible: Less than the above.
Source: Transportation Safety Board of Canada (TSB), ISIM Reference Manual – Marine Mode (August 2014).
ISIM = Integrated Safety Investigation Methodology