Grounding and subsequent sinking
Articulated tug-barge
Tug Nathan E. Stewart and tank barge DBL 55
Seaforth Channel, 10 nm west of
Bella Bella, British Columbia
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 13 October 2016, shortly after 0100 Pacific Daylight Time, the articulated tug-barge composed of the tug Nathan E. Stewart and the tank barge DBL 55 went aground on Edge Reef near Athlone Island, at the entrance to Seaforth Channel, approximately 10 nautical miles west of Bella Bella, British Columbia. The tug's hull was eventually breached and approximately 110 000 L of diesel oil were released into the environment. The tug subsequently sank and separated from the barge. The tug was removed from the environment 33 days after the occurrence. Seven 208 L drums of diesel oil–soiled absorbent pads were collected from the site.
Le présent rapport est également disponible en français.
1.0 Factual information
1.1 Particulars of the vessels
| Names of vessels | Nathan E. Stewart | DBL 55 |
| International Maritime Organization number | 8968210 | n/a |
| Official number | 1120997 | 1229343 |
| Port of registry | New York, NY | Portland, OR |
| Flag | United States | United States |
| Type | Tug | Tank barge |
| Gross tonnage | 302 | 4276 |
| Length | 29 m | 87.78 m |
| Built | 2001, Hope Services Incorporated, Dulac, LA, U.S. | 2010, Zidell Marine Corporation, Portland, OR, U.S. |
| Propulsion | 2 diesel engines × 1193 kW driven fixed-pitch propellers | none |
| Cargo | none | none |
| Crew | 7 | unmanned |
| Registered owner | Kirby Offshore Marine Operating LLC, Houston, TX, U.S.A. | Kirby Offshore Marine Pacific LLC, Houston, TX, U.S.A. |
1.2 Description of the tug and the tank barge
1.2.1 Tug
The Nathan E. Stewart was a conventional harbour and deep-sea towing tug of steel construction (Figure 1). It had an upper and lower wheelhouse for navigating. The upper wheelhouse could be accessed through an internal stairwell from the lower wheelhouse. It had an open layout, with windows that provided a nearly all-around, unobstructed view, and there was a chair in the middle of the space. The navigation of the tug was normally conducted from the upper wheelhouse.

The Nathan E. Stewart was owned by Kirby Offshore Marine Operating LLC (Kirby) and was equipped with an automatic identification system (AIS),Footnote 1 an autopilot, a global positioning system (GPS), an electronic charting system, paper charts, depth sounders, 2 radars, 2 very high frequency (VHF) radiotelephones, 1 portable VHF radiotelephone, and an internal vessel intercom system. The tug's depth sounders, GPS, radars, and electronic charting system contained both visual and audible navigational alarm functions for depth, cross-track error, waypoint arrivals, time countdown, and radar guard zone. The Nathan E. Stewart was not equipped with a bridge navigational watch alarm system (BNWAS).Footnote 2
Below the main deck was the fore peak, storage compartment, engine room, and steering compartment. The port and starboard pneumatically operated pins, which were used to connect the tug and barge, were located in the storage compartment. There were also 3 aft and 4 forward fuel tanks, as well as additional oil tanks for lubricant, gear oil, hydraulic oil, used oil, and bilge water (Appendix A).Footnote 3
1.2.2 Tank barge
The DBL 55 is a double-hulledFootnote 4 tank barge with 14 cargo tanks, and is certified to carry 52 000 barrelsFootnote 5 with a maximum displacement of approximately 11 000 long tons.Footnote 6 It is also certified to carry 116 long tons of deck cargo. On deck, the barge is equipped with 2 diesel oil service tanks, 2 holding tanks, and 300 m of pollution boom and absorbent pads. It has a raked bow designed for ease of movement in sea conditions and a 9.7 m deep V-shaped indent at the stern to accommodate the bow of a pushing tug (Figure 2).

When the Nathan E. Stewart is in pushing mode, the bow of the tug is secured to the V-shaped indent at the stern of the barge with pneumatically operated pins. These pins create a hinge between the tug and the barge that allows for their differing movements during transit. When the 2 vessels are connected in this manner, they become an articulated tug-barge (ATB).
1.3 History of the voyage
During the day on 11 October 2016, the Nathan E. Stewart and the DBL 55,operating as an ATB, arrived at Ketchikan, Alaska, where all cargo on board the DBL 55 was discharged. At 2230,Footnote 7 the ATB departed Ketchikan for Vancouver, British Columbia, with 7 crew members on board. The navigational watches were shared by the master, first mate, and second mate.
At 2300 on 12 October, the second mate went to the upper wheelhouse to take over the watch from the master. The second mate's watch readiness was not discussed. The master handed over the watch and went to bed. The second mate then prepared for the watch by adjusting the chair, window curtains, radio, and heaters; reviewing the logbook entries; and checking the ATB's position on the tug's electronic charting system. There was minimal vessel traffic as the ATB entered Milbanke Sound, British Columbia.
At 0000 on 13 October, the assistant tankerman began engine room rounds. At 0020, the second mate altered the vessel's course to port to pass 1 nautical mile (nm) off Ivory Island and enter Seaforth Channel. Just over 30 minutes later, the ATB passed the alteration waypoint off Ivory Island. At this time, the weather at Ivory Island consisted of light winds of 9 knots from the east, light rain, and a 0.3 m sea.
The assistant tankerman completed a check of the tug's engine room and called the second mate from the galley intercom radio at approximately 0100, with no response. The assistant tankerman made another call to the second mate, with no response. Just prior to the grounding, the assistant tankerman began making his way to the wheelhouse to check on the second mate.
At approximately 0106,Footnote 8 the ATB struck Edge Reef off Athlone Island, at the entrance to Seaforth Channel, approximately 10 nm west of Bella Bella, British Columbia, at 52°14.37′ N and 128°23.08′ W (Appendix B). Following the impact, the second mate reversed both engines and placed the rudders hard to port. The assistant tankerman, who had not yet reached the wheelhouse, felt the impact and radioed the second mate. The second mate informed the assistant tankerman that the ATB had hit the reef.
The noise of the engine in full reverse and/or the vibration of the tug when it struck the reef alerted the remaining crew. The master went to the upper wheelhouse, took over the watch, and instructed the second mate to ensure that the crew was awake and would survey the damage to the ATB. The tug's starboard engine was disabled, so the master attempted to reverse off the reef with the port engine while moving the rudder from hard over port to hard over starboard. The ATB pivoted around but did not move off the reef, and the tug made contact with the seabed several times.
At 0111, the master reported to Marine Communications and Traffic Services (MCTS) that the tug Nathan E. Stewart and the empty tank barge DBL 55 had grounded on Edge Reef in Seaforth Channel. The master requested assistance from the Canadian Coast Guard (CCG) and informed MCTS that the crew intended to stay on board and survey the damage. The crew proceeded to survey the damage and check for any ingress of water to both the tug and the barge.
MCTS relayed the details of the occurrence to the Joint Rescue Coordination Centre (JRCC) in Victoria, British Columbia, and notified CCG Regional Operations Centre, Pacific Region; Transport Canada (TC); and the CCG's Environmental Response.
At 0122, MCTS broadcast the ATB's state of urgency, and the search-and-rescue (SAR) lifeboat Cape St. James, stationed in Bella Bella, was tasked with the SAR mission. Shortly afterward, the master reported to MCTS that the tug was hard aground and grinding on the reef. The master directed the crew to move personal belongings, immersion suits, and lifesaving equipment from the tug to the barge. At this point, the master set the AIS to "vessel aground." The CCG ships John P. Tully and Bartlett were tasked to respond to the occurrence, with estimated times of arrival of 0730 and 0930, respectively.
At approximately 0200, the master notified Kirby's authorized representative of the situation. Shortly thereafter, the Cape St. James arrived on scene and offered the master a towline, which was not accepted. At this point, the extent of the damage was unknown, but the crew reported that the tug and the barge did not appear to be taking on water.
The crew set up fuel transfer hoses from the tug to the barge in preparation to transfer fuel, if needed. The engineers discovered that the keel coolers had been breached, and they shut down the port main engine. The crew continued to monitor for damage and ingress of water, and the Cape St. James surveyed the surrounding water and recorded the draft marks on the barge.
At approximately 0315, the second mate underwent drug and alcohol testing as per the United States Code of Federal Regulations.Footnote 9
At 0345, the Cape St. James reported that there were no signs of pollution. However, MCTS notified CCG Environmental Response that pollution could be released from the tug, and that, following the SAR mission, this could become a pollution-response incident.
As the tide continued to rise, the wave action increased to 2 to 3 m, which increased the tug's motion and contact with the seabed.
At approximately 0407, the Nathan E. Stewart's chief engineer reported that the tug's No. 1 port fuel tank level was decreasing. The crew began to transfer fuel from the tug to the barge. Shortly afterward, a crew member reported that the No. 1 centre fuel tank valve had failed, and that fuel was leaking into the bilge. The master advised MCTS that there was a smell of diesel coming off the sea, and provided MCTS with a contact number for the authorized representative.
At approximately 0520, the master reported to MCTS that the Nathan E. Stewart was taking on water and that diesel oil was leaking into the sea. The crews of the Cape St. James and the Nathan E. Stewart deployed the barge's containment boom around the tug. The crew also set up portable pumps to dewater the tug.
Following the master's report, CCG Environmental Response began coordinating the pollution response. They told the John P. Tully to stop in Shearwater, British Columbia, and pick up the CCG's pollution control equipment. At approximately 0630, the containment boom around the tug parted.
At approximately 0650, due to the ingress of water into the tug's engine room, the Nathan E. Stewart lost power and the fuel transfer pump stopped. The crew retrieved additional portable pumps from the barge and set them up in an effort to dewater the tug. By 0800, the additional pumps were no longer keeping up with the ingress of water.
By 0700, the Western Canada Marine Response Corporation (WCMRC)Footnote 10 had engaged local contractors from Shearwater to assist with the spill response, and British Columbia's emergency response program had been notified of the situation. A provincial regional emergency operations centre was activated, and a provincial Ministry of Environment and Climate Change Strategy environmental officer was briefed and deployed. By this time, the Heiltsuk First Nation, in Bella Bella, had been made aware of the grounding, and 3 of their vessels had arrived on scene.
At approximately 0815, the tug Haisea Guardian and the Bartlett's fast rescue craft arrived on scene to assist the Nathan E. Stewart and its crew. The fast rescue craft supplied the Nathan E. Stewart crew with additional pumps. A short time later, the Bartlett arrived, and the master of the Cape St. James handed over incident command to the master of the Bartlett.
At approximately 0900, in light of the Nathan E. Stewart's deteriorating situation, the master collected the logbooks and ordered the crew to prepare to abandon the tug. The fast rescue craft transported the Bartlett's chief officer to the Nathan E. Stewart,where the chief officer and the master discussed the situation.
Soon after, a wave flooded the back deck of the tug, washing 2 crew members overboard. One crew member climbed back on board the tug. The tug's stern sank, and it became suspended from the barge by the tug's pneumatic pins. The fast rescue craft retrieved the other overboard crew member and the tug's remaining crew, and the chief officer abandoned the tug onto the barge.
Around this time, the Royal Canadian Mounted Police vessel Inkster arrived on scene. By 0945, the entire crew of the Nathan E. Stewart had been transferred to the Bartlett.
1.4 Spill response and tug salvage
When a spill occurs, the responsible partyFootnote 11 is required to take all reasonable measures to contain and stop the release of pollution, and to notify the appropriate authorities of the incident.
As the day progressed, multiple agencies became involved in the spill response and began to operate within the incident command system (ICS).Footnote 12 Those agencies included the following:
- the responsible party, who is required to assume all costs related to the spill response and recovery of the affected environment
- the authorized representative, acting on behalf of the responsible party, who contracted a marine emergency response company and other companies who conduct clean-up operations (WCMRC), wildlife and shoreline assessments, environment sampling, and salvage/dive operations
- oversight and assistance agencies, namely CCG Environmental Response, Environment and Climate Change Canada (ECCC), various TC departments and programs, Fisheries and Oceans Canada (DFO), the British Columbia Ministry of Environment and Climate Change Strategy, and the Heiltsuk First Nation.
Throughout the day on 13 October, key personnel began to arrive in Bella Bella, including the authorized representative, an environmental officer from the CCG, and an environmental officer from British Columbia's Ministry of Environment and Climate Change Strategy (see Section 1.18 for more detail). These personnel, along with Heiltsuk First Nation representatives, formed a unified command (UC). The UC then established an incident command post at the offices of the Heiltsuk Tribal Council. The Bartlett continued to receive reports of pollution from the vessels in the vicinity of the occurrence, and several tugs that had been contracted by the authorized representative were deployed to assist with the situation.
At about 1000 on 13 October, the Cape St. James left the scene while several small Heiltsuk First Nation vessels and the fast rescue craft attempted to turn the ATB around to get a towline on it and stabilize its position. At about 1030, the attempts to get a line onto the ATB were successful and the Haisea Guardian was able to stabilize its position. The tide was close to high and the barge was floating free as the sunken stern of the Nathan E. Stewart anchored the barge. The first WCMRC vessel, the Clowhom Spirit 1, arrived on scene.
At 1135, the master of the Bartlett announced to those on scene that the authorized representative had contracted a marine emergency response company who would be responsible for overseeing the clean-up operations going forward. Around this time, there were 2 WCMRC vessels on scene, awaiting instructions from the marine emergency response company. Meanwhile, the pollution continued to spread and had entered Gale Passage. The Heiltsuk first responders requested that a boom be put in place to stop the diesel fuel from entering the passage.
At approximately 1300, the John P. Tully arrived on scene and transferred the CCG's pollution equipment to the Bartlett. The crews of both vessels, as well as some of the crew from the Nathan E. Stewart, replaced the towline connecting the ATB to the Haisea Guardian with a stronger line.
At 1530, the crew of the Nathan E. Stewart was taken by water taxito Shearwater Resort and Marina.
By 1600, the authorized representative had conducted an overflight of the area and Heiltsuk Tribal Council members were assisting WCMRC vessels in deploying booms and absorbent pads in Gale Passage. At approximately 1615, the Bartlett supplied booms, 2 anchors, and 1 of its crew members to a small Heiltsuk vessel, which already had 2 responders on board. The fast rescue craft accompanied the vessel as its crew deployed a boom between the shoreline and the barge. Because the tide was low, the rocks near the shoreline were exposed; there were also large swells. During the attempts to deploy the boom, it was decided that the sea conditions were too dangerous for the crew to continue working.
At approximately 1730, the WCMRC vessel Eagle Bay arrived on scene. The Bartlett,the fast rescue craft, and the John P. Tully were released for the evening. Shortly thereafter, a dive team arrived on scene with 2 crew members from the Nathan E. Stewart to assess the tug's underwater condition. At 1830, the Eagle Bay and its crew began deploying 300 m of boom in the Gale Passage area.
At approximately 1900, the Nathan E. Stewart's ATB pins failed and the barge broke free from the tug. The tug then completely filled with water and sank, and came to rest on the seabed. The tugs North Arm Diligent and Haisea Guardian towed the barge to Norman Morrison Bay, where the barge was then anchored.
At 1927, a CCG helicopter conducted an overflight, and its crew observed a large sheen of diesel oil on the water outside of the containment boom that was secured around the tug, as well as some recoverable product within the boom.
Clean-up and tug salvage operations continued for the next 40 days, until 22 November. That period included approximately 11 days on which operations were suspended due to weather concerns. Response personnel worked almost daily over the remaining days, performing the following tasks:
- WCMRC crews continued skimming Seaforth Channel to collect as much diesel oil as possible and continuously repositioned booms around the tug and areas of concern. Absorbent pads were continuously deployed, collected, and replaced.
- Salvage operations continued, including towing the DBL 55 from Norman Morrison Bay to North Vancouver, British Columbia. Salvage divers attempted to stop the diesel oil in the tug from leaking. Approximately 119 000 L of diesel oil and lubricants were also removed from the tug. Divers prepared the tug for repositioning and lifting, and removed the remaining debris from the ocean floor. On 14 November, various vessels and barges were used to reposition and lift the tug.
- TC's National Air Surveillance Program conducted overflights to assess pollution.
- The CCG's helicopter conducted overflights to monitor operations and transport crews.
- The Bartlett was positioned on scene to assist with communication and coordination among the various vessels at the occurrence location, as well as to monitor the situation, provide personal protective equipment, and track all vessel movements in order to ensure a safe working area.
- Contracted company personnel conducted shoreline assessments.
- Contracted company personnel conducted wildlife assessments and monitoring, and collected water and plant samples. Samples continued to be taken well after the tug was removed from the environment.
- Contracted Heiltsuk First Nation representatives participated in and supported operations by monitoring clean-up and salvage operations as well as shoreline and wildlife assessments, and contributing services, facilities, equipment, vehicles, and supplies.
On 22 November, the incident command post was stood down, dive operations were completed, and a notice to mariners was issued regarding the completion of the salvage operation.
1.4.1 Summary
Over the course of the spill response, the UC estimated that 45 vessels and over 200 people were involved in response activities, including 114 response personnel in the field.Footnote 13 The Nathan E. Stewart crew and response personnel removed about 119 000 L of diesel oil and lubricants from the tug prior to salvage. An estimated 110 000 L of pollutants were released into the environment before the tug was removed from the water. Some of the pollutants were collected with absorbent pads.Footnote 14
During the spill response, 168 samples of water, sediment, vegetation, and animal tissue were taken at 27 different locations. Shoreline Cleanup and Assessment Technique (SCAT) surveys covered approximately 350 km of shoreline.
1.5 Vessel certifications
1.5.1 Tug
On 19 March 2014, the tug underwent a United States Coast Guard (USCG) inspection. No deficiencies were noted.
On 31 July 2015, the USCG issued a Minimum Safe Manning Document requiring that the tug be manned by 7 personnel: a master, 2 licensed officers in charge of navigation watch, 2 able seamen,Footnote 15 a chief engineer, and a licensed engineer. At the time of the occurrence, the vessel was manned as per the requirements for safe manning.
1.5.2 Tank barge
On 18 February 2016, the DBL 55 was inspected by the USCG. No deficiencies were noted. The USCG conducted a stability assessment of the tank barge on 24 February 2011; its stability was assessed as satisfactory for operation in exposed waters.
1.6 Personnel certification and experience
1.6.1 Master
The master held a certificate valid for service on oceangoing towing vessels of 3000 gross tonnage (GT) or less. The master had successfully completed training on bridge resource management, voyage planning, situational awareness, and leadership and managerial skills.
The master had started working as a deckhand in 1999 and was promoted to master in 2012. Since 2013, he had worked as master of the Nathan E. Stewart operating as an ATB on the northwest coast of the U.S. and Canada. At the time of the occurrence, the master was the only officer on board who held a valid pilotage waiver (see Section 1.11).
1.6.2 Second mate
The second mate was certificated as an officer in charge of a navigational watch on uninspected towing vessels only. He had also had training in bridge teamwork, the use of automatic radar plotting aids, and electronic chart display information systems. While studying to gain additional mariner's credentials, he had worked as a deckhand for Kirby from October 2013 to June 2014; he obtained the additional credentials in January 2015. He had worked as a second mate on other company vessels since April 2015 and on the Nathan E. Stewart since 08 July 2016. This was the second mate's second roundtrip voyage on the tug.
1.6.3 First mate
The first mate held a master certificate valid for service on oceangoing towing vessels of 3000 GT or less. The first mate had been working in the towing industry since 2000, and had worked on the Nathan E. Stewart as first mate since 2001. At the time of the occurrence, the first mate held an expired pilotage waiver; a copy of his new certificate of competency had not been received by the Pacific Pilotage Authority Canada (PPA), as was required.
1.6.4 Assistant tankerman
The assistant tankerman had had training on safe tanker operations and was certified as an able-bodied seaman. The assistant tankerman had started working for Kirby in May 2015, and had worked as assistant tankerman on the Nathan E. Stewart since 09 October 2016. This was the assistant tankerman's first voyage on the tug.
1.7 Environmental conditions
In autumn and winter, the exposed portion of the British Columbia coast normally experiences strong southeast winds associated with frontal systems.Footnote 16
ECCC issued a storm warning for the central coast of British Columbia for the afternoon and evening of 12 October 2016, calling for southeasterly winds of 35 to 45 knots in the afternoon and 40 to 50 knots in the evening.
Similar weather observations were reported at the time of the occurrence by the masters of the Nathan E. Stewart and the Cape St. James: winds 10 knots from the southeast and 0.5 m waves from the northeast. The sky was overcast with rain and 8 nm visibility. The seawater temperature was 11 °C and the air temperature was 7.7 °C.
At the tidal station in Bella Bella, high water was at 2258 on 12 October and low water was at 0521 on 13 October, with a tidal range of 3 m.
1.8 Damage to the vessels
1.8.1 Tug
The Nathan E. Stewart's hull sustained damage below the waterline. In addition to numerous scrapes, keel fractures, deformations, and indentations to the hull, there were large puncture holes in the shell plating adjacent to the fuel oil tanks and engine room. Because most of the tug was submerged in seawater for over a month, the wheelhouse, accommodation, and engine room were damaged. The tug was declared a total constructive loss.
1.8.2 Tank barge
The DBL 55's outer hull sustained damage below the waterline. In addition to numerous scrapes, keel fractures, deformations, and indentations to the outer hull, there were large puncture holes in the outer hull's shell plating adjacent to the cargo tanks in the mid-section. The cargo tanks were not punctured. The tank barge was towed to Vancouver for repairs before it was put back into service.
1.9 Company operations
Kirby is one of the largest towing operators in the United States. It operates tugs and barges on the east coast of the U.S., on the Mississippi River, in Hawaii, and along the northwest coast of North America, including in Canadian waters. On the northwest coast, the company's tank barges carry petroleum products from refineries in British Columbia and Washington State to distribution centres in Alaska.
1.10 Inside Passage transits
The Inside PassageFootnote 17 is used by commercial traffic such as cruise ships, tugs, barges, tankers, and fishing vessels (Appendix C, route A). Vessel activity on the Inside Passage varies seasonally with an average of approximately 1100 vessels transiting portions of the passage each month.Footnote 18
Under the Pacific Pilotage Regulations,Footnote 19 the combined tonnage of all vessels in any arrangement of vessels, including ATB arrangements, is taken into consideration in determining whether the vessels are required to have a pilot on board or a pilotage waiver. Approximately 430 vessels and 250 barges have a pilotage waiver granted by the PPA for the compulsory pilotage waters of the Inside PassageFootnote 20 (Appendix C, red areas). The Inside Passage route is favoured by these vessels, either by the more direct route through Laredo Sound and Principe Channel (Appendix C, route B), or the longer but more protected route through Fitzhugh Channel and Grenville Channel (Appendix C, route A). The Nathan E. Stewart used the latter route.
1.11 Coastal pilotage
The PPA is a Crown corporation created in 1972 under the Pilotage Act. Its mandate is to provide safe, reliable, and efficient marine pilotage and related services in the coastal waters of British Columbia. Currently, vessels or vessel arrangements of more than 350 GT but less than 10 000 GTFootnote 21 (mainly tugs and barges) may apply for and be granted pilotage waivers if the operator meets certain conditions,Footnote 22 making these vessels exempt from compulsory pilotage.
In February 2016, the authorized representative for the Nathan E. Stewart had applied for a pilotage waiver from compulsory pilotage, which was then granted by the PPA. The waiver included 15 other tugs, 14 barges, and 69 personnel. The master and 2 mates on board the Nathan E. Stewart met the experience conditions needed for the granting of pilotage waivers. However, the first mate had not met the condition of supplying the PPA with a current certificate of competency, and the second mate had not requested a pilotage waiver. The morning of the occurrence, the authorized representative requested that the second mate be included in the approved pilotage waiver personnel list.
On 16 October, 3 days after the occurrence, the PPA informed the authorized representative that, effective immediately, all British Columbia coast pilotage waivers held by all Kirby vessels and marine officers were being revoked.
1.11.1 Pacific Pilotage Authority Canada risk assessment project
On 24 October, the PPA issued a letter explaining amendments to its waiver system to approximately 60 companiesFootnote 23 that held a pilotage waiver.
A risk assessment project was undertaken by the PPA to assess the interim amendments. As part of the project, a survey of approximately 95% of waiver holders was conducted. Nearly half of the respondents and the risk management team raised concerns about the following:
- extra manning required to maintain a 2-person bridge watch
- company's profitability in maintaining a 2-person bridge watch
- extra demands on masters, leading to fatigue
- interpretations of what a 2-person bridge watch means (i.e., 2 persons continuously on the bridge or 2 persons available on watch and on the bridge unless otherwise required)
On 23 May 2017, the PPA released the conditions under which the PPA would consent to granting waivers to qualified applicants from then on. In addition to the requirements that the PPA already had in place, the new conditions stated that all vessels operating under a waiver must
- be operating a BNWAS;
- be fitted with, and transmitting on, a Class A AIS;
- report to PPA by email upon entering and departing compulsory pilotage areas;
- have 2 persons on the bridgeFootnote 24 when operating in confined waters;Footnote 25 and
- not carry or push/tow oil cargo in designated "no-go" areas.Footnote 26
1.12 Bridge-manning requirements
1.12.1 Bridge resource management
Vessels must be navigated safely at all times, in compliance with the International Regulations for Preventing Collisions at Sea (COLREGs), and in a manner that will not harm the environment. Bridge resource management is the management and use of all resources, human and technical, to ensure the safe completion of the voyage. Effective bridge resource management mitigates the risk that an error on the part of 1 person, or a single point of failure,Footnote 27 will result in a dangerous situation.
1.12.2 Bridge procedures guide
The International Chamber of Shipping Bridge Procedures GuideFootnote 28 captures the best watchkeeping practices for commercial vessels and encompasses current standards and recommendations. It includes additional guidance on bridge resource management and the conduct of the bridge team, such as the use of passage planning, integrated electronic navigation systems, and the Global Maritime Distress and Safety System.
The guide emphasizes that the officer of the watch (OOW) may be the sole lookout in daylight conditions as per the Seafarers' Training, Certification and Watchkeeping (STCW) code. The guide suggests that if sole lookout is practised on any vessel, guidance on this practice should be provided in the shipboard operational procedures manual, supported by master's standing orders as appropriate, and should cover, at minimum
- under what circumstances sole-lookout watchkeeping can begin;
- how sole-lookout watchkeeping should be supported; and
- under what circumstances sole-lookout watchkeeping must be suspended.
The STCW code also recommends that before a 1-person bridge watch begins, the master should be satisfied that
- the OOW has had sufficient rest prior to beginning watch;
- in the opinion of the OOW, the anticipated workload is well within the bridge team's capabilities to maintain a proper lookout and remain in full control of the prevailing circumstances;
- back-up assistance to the OOW has been clearly designated;
- the OOW knows who will provide that back-up assistance, under what circumstances back-up must be called, and how to call it quickly;
- designated back-up personnel are aware of response times and any limitations on assisting the OOW, and are able to hear alarm or communication calls from the bridge; and
- all essential equipment and alarms on the bridge are fully functional.
The Nathan E. Stewart operated with a 1-person bridge watch, and it was not common practice to use the navigational alarms.Footnote 29
1.12.3 Canadian requirements
Pursuant to the Canada Shipping Act, 2001 (CSA 2001), the Marine Personnel Regulations (MPR) require the master of a vessel that is not securely anchored in port or securely moored to shore to ensure that a deck watch is maintained in accordance with parts 2, 3, and 3-1 of section A-VIII/2 of the STCW code.Footnote 30
These sections of the STCW code state, among other things, that a proper lookoutFootnote 31 shall be maintained at all times, that the lookout must be able to give full attention to the keeping of a proper lookout, and that the officer in charge of the navigational watch may be the sole lookout in daylight under specified conditions. The MPR are applicable to foreign vessels in Canadian waters.Footnote 32
Under the MPR, the Nathan E. Stewart was required to have 2 people on the bridge during hours of darkness.Footnote 33
1.12.4 United States Coast Guard requirements
When the Nathan E. Stewart transited U.S. waters, it was required to comply with the U.S. Code of Federal Regulations. While in U.S. waters, the Nathan E. Stewart's master and officer in charge of the navigational watch had to assess the requirement for a lookout. This assessment had to be consistent with the COLREGs.Footnote 34 In addition to the master or OOW, a lookout should be added when it is necessary to
- maintain a state of vigilance with regard to any significant change in the operational environment;
- assess the situation and the risk of collision/allision;
- anticipate stranding and other dangers to navigation; and
- detect any other potential hazards to safe navigation.Footnote 35
In determining the requirement for a lookout, the OOW must take all relevant factors into account, including but not limited to weather, visibility, traffic volume, proximity of dangers to navigation, and the attention necessary when navigating in areas of increased vessel traffic density.Footnote 36
Under the U.S. Code of Federal Regulations, it is not mandatory to have 2 people on the bridge during the hours of darkness, but it is the responsibility of the master and the OOW to assess the requirement for a lookout during the hours of darkness.
1.12.5 Company requirements
Kirby's Common Procedures ManualFootnote 37 provides guidance to assist the master in organizing the bridge team under varying conditions. Although Kirby recognizes that towing vessels have traditionally been designed to be manned and operated by 1 OOW serving as both the OOW and the lookout, it requires that additional people be assigned to the bridge watch, depending on the vessel's operational status and situation. The master is responsible for establishing and posting a watch rotation.
A TSB examination of the Nathan E. Stewart's upper wheelhouse determined that although it could accommodate 2 persons on bridge watch duty, the upper wheelhouse was set up for a 1-person bridge watch.
In addition to the guidance provided to the masters in organizing the bridge team when tugs are underway, Kirby requires that at least 1 licensed deck officer serve as OOW and that 1 additional watchkeeper be present at all times (i.e., 2-person bridge watch). On ATB units underway in pilotage waters, the additional watchkeeper is required to stand watch on the bridge except when making safety rounds,Footnote 38 answering alarms, or performing other tasks of short duration as authorized by the OOW.Footnote 39
The "Management System Audits" section of Kirby's Common Procedures ManualFootnote 40 provides direction for the conduct of audits that are designed to evaluate a crew member's knowledge and application of the manual. Company records indicate that the crew of the Nathan E. Stewart was audited on 16 June 2016.
The investigation determined that it is common practice for company tugs in this type of operation to operate with a single person on the bridge.
1.13 Fatigue
For sleep to be restorative, it should occur at night in a period of at least 7, and up to 9, continuous hoursFootnote 41 Footnote 42 so that all 5 stages of sleepFootnote 43 occur during each nightly sleep period. For a normal nighttime sleeper, deep sleep (stages 3 and 4) occurs early in the sleep period, while rapid eye movement (REM) sleep occurs in the second half.Footnote 44 ResearchFootnote 45 suggests that deep sleep may serve a physiologically restorative function,Footnote 46 and REM sleep is more likely to restore cognitive processes.
If a person's sleep is repeatedly disrupted during the first half of the normal sleep period, total deep-stage sleep will be decreased, increasing the risk of fatigue and disrupted physiological functioning. If a person's sleep in the second half of the sleep period is interrupted, REM sleep will be restricted, leading to impairments in cognitive functioning as well as increased fatigue.
Sleep disruption not only limits the total amount of sleep obtained, it also disrupts the quality of sleep. After each awakening, the sleep cycle normally restarts, rather than resumes the stage that was interrupted. Sleep that does not follow the natural, uninterrupted progression through all stages of sleep within repeated 90-minute cycles has a disrupted sleep "architecture," is of poor quality, and can result in fatigue during waking hours. The division of a rest period into a number of shorter segments can result in increased sleepiness and decreased performance.Footnote 47 Footnote 48 Footnote 49
Fatigue may result from 1 or more of 6 risk factors: acute sleep disruptions; chronic sleep disruptions; continuous wakefulness; circadian rhythm disruptions; sleep disorders or other medical and psychological conditions; and/or illnesses or drugs that affect sleep or sleepiness. Other factors that may influence a person's ability to obtain restorative sleep are individual factors (e.g., morningness/eveningness, ability to nap), the nature of the work (e.g., whether it is monotonous), and the individual's schedule type (e.g., split shiftsFootnote 50 ) (Appendix D).
1.13.1 Circadian rhythm
The time of day has a strong effect on an individual's alertness and performance due to changes in body physiology that are synchronized to a circadian (daily) rhythm. The body is physiologically ready for sleep at night, and the best quality and longest duration of sleep are obtained at night.Footnote 51 Likewise, due to the circadian rhythm, overall performance and cognitive functioning are at their worst during the nighttime period. This pattern can occur in the absence of fatigueFootnote 52 —that is, overall performance may be low during the circadian trough even if a person is not fatigued.
1.13.2 Work–rest requirements
TC's MPR are the regulatory means of addressing the risks of fatigue in the marine industry in Canada, and incorporate the requirements set out in the STCW code. The MPR require that crew members of foreign vessels in Canadian waters
- not work more than 14 hours in any 24-hour period, or more than 72 hours in any 7-day period; or
- have at least 10 hours of rest in every 24-hour period, and 77 hours of rest in every 7-day period.Footnote 53
Further, the daily hours of rest are to be divided into no more than 2 periods, one of which is at least 6 hours in length, and the interval between 2 consecutive rest periods must not exceed 14 hours. The shift-scheduling practices of the Nathan E. Stewart were in accordance with the applicable MPR provisions.
In the marine transportation industry, some operators may economize by, for example, limiting the size of the crew on board a vessel to the smallest complement permitted by regulations. However, having a smaller crew on board increases the risk of fatigue by requiring mariners to work longer, irregular hours across long periods of time, while at the same time providing them limited opportunities to obtain good quality, uninterrupted sleep. Poor sleeping conditions, rotating shift schedules, and high workload can also increase the risk of fatigue on board vessels.Footnote 54
For individuals whose work schedules require that sleep be obtained across multiple, non-consecutive segments, it can be challenging to obtain sufficient quantity and quality of restorative rest. Due to the circadian rhythm, rest periods that occur in daytime periods may be less restorative than those taken during the hours of darkness.Footnote 55 As well, meals, personal chores, crew shift changes, and unscheduled interruptions (such as emergency drills) prevent crew members from obtaining the necessary amount of sleep in the time available.
Recent research has demonstrated that mariners' compliance with regulatory work–rest scheduling requirements is generally poor.Footnote 56 Footnote 57 In addition, when shift schedules change intermittently, for example when a vessel is in port versus when it is at sea, there is an accommodation period during which an individual is more likely to be fatigued until he or she adjusts to the new schedule.
The shift-scheduling practice on board the Nathan E. Stewart was to assign watch duties while the tug was at sea according to a shift schedule where an individual would work for 4 consecutive hours and would then be off duty for 8 hours (i.e., a 4-on, 8-off schedule). When the tug was in port (and for the 12-hour period before and after arriving in, and departing from, port), the shift schedule would change to a 6-on, 6-off schedule, to allow the crew to perform additional duties such as voyage planning and unloading cargo. Each crew member's shifts typically ended at the same time of day.
International researchFootnote 58 Footnote 59 Footnote 60 on shift-scheduling practices for OOWs has found that, compared to other schedules, the 6-on, 6-off schedule is associated with less daily sleep, increased opportunity for poor-quality fragmented sleep, more frequent episodes of nodding off (micro-sleeps), and excessive sleepiness—especially during the early morning hours. Furthermore, watch handover times are considered suboptimal, in that "the toughest hours of the day for staying awake and alert (i.e., between midnight and 6:00) are entirely on the shoulders of the same watch team."Footnote 61 According to the USCG, these findings
Footnote 62Changing the 6-on, 6-off watch start and end times by 3 hours across bridge watch teams, such that nighttime hours are equally divided, has been found to shift the risk of sleepiness and of falling asleep so that it is more equally distributed across bridge watch teams.
In this occurrence, the grounding took place in the early morning hours of 13 October. The crew had been working a 6-on, 6-off shift schedule from 10 October until the morning of 12 October, while the tug was in port; it left port on 11 October at approximately 2230.
1.14 Second mate's work–rest schedule and risk of fatigue
The second mate had been on board the Nathan E. Stewart since 20 September (23 days). When in port (on a 6-on, 6-off schedule), the second mate was on watch from 2200 to 0400 and again from 1000 to 1600. The second mate rested in the shared cabin most afternoons during the off hours between 1700 and 2200, but rarely fell asleep. Thus, restorative sleep was primarily obtained during morning hours. The second mate slept, on average, 8 hours per day when not at sea.
The second mate's hours of work and restFootnote 63 in the 72-hour period prior to the occurrence were as follows:
- On 10 October, the second mate was on watch while at sea from 1200 to 1600, and again on 11 October from 2200 to 0400. The second mate had slept from 0500 to 1130 that morning. (Daily total sleep: 6.5 hours. The second mate had rested during the evening hours, but likely did not fall asleep.)
- On 11 October, the second mate performed voyage-planning and tug-loading duties while in port from 1000 to 1600. The ATB departed port at approximately 2230. The second mate was on watch from 2100 to 0400 on 12 October. The second mate had slept from 0430 to 0900 that morning. (Daily total sleep: 4.5 hours. The second mate had rested during the evening hours, but likely did not fall asleep.)
- On 12 October, the second mate was on duty performing other tasks from 1130 to 1700, which included a fire drill that all crew members attended. The second mate came back on watch at 2200. The second mate had slept from 0500 to 1120 that morning. (Daily total sleep: 6.3 hours. The second mate had rested during the evening hours, but likely did not fall asleep.)
As a result, at the time of the grounding, the second mate had been awake for up to 13 hours.
An assessment of the second mate's work schedule in the days preceding the occurrence was conducted using Fatigue Avoidance Scheduling ToolFootnote 64 software. This assessment estimated that the second mate's performance at the time of the grounding was equivalent to a normal nighttime sleeper who had missed 1 night of sleep.
The TSB investigation found that the following fatigue-inducing factors existed for the second mate at the time of the grounding:
- acute sleep disruption
- chronic sleep disruption
- circadian rhythm disruptions
- individual factors
- nature of the work
- schedule type
Continuous wakefulness, medical and psychological conditions, illnesses, drugs, and sleep disorders are additional fatigue risk factors that were not present for the second mate at the time of the grounding. The acute sleep disruption was present because of the second mate's shortened sleep (6.3, 4.5, and 6.5 hours of sleep, rather than 8 hours) on the 3 consecutive days preceding the accident. The chronic sleep disruption occurred because the second mate had been on the tug for 23 days and had worked a challenging shift schedule. This disruption was further compounded by an individual factor: the second mate's inability to nap on most days during the afternoon or early evening break.
According to Transport Canada's Fatigue Management Guide for Canadian Marine Pilots,
Footnote 65In this occurrence, the following conditions in the wheelhouse related to the nature of the work further increased the risk of the second mate's falling asleep:
- the monotonous nature of the watchkeeping tasks
- the steady drone of the tug's engines
- the warm temperature (2 electric wheelhouse heaters were on)
- the light music playing (the satellite radio was on)
- the dark environment (it was night and the curtains on the bridge were drawn)
- the lack of interaction and conversation with other crew members (the second mate was alone on the bridge)
- the calm sea conditions
- the sedentary nature of the navigational and chart plotting task (the second mate was relying exclusively on the electronic charting system to monitor the tug's position)
- the comfortable chair in which the second mate was seated
1.15 Fatigue risk mitigation strategies
ResearchFootnote 66 shows that a lack of sleep and inconsistent sleep times are the primary risk factors that contribute to fatigue in mariners. Fatigue risk management requires a proactive approach that includes not only compliance with regulations (which can only ever mandate hours of rest, not hours of sleep) but also mariner education and awareness. Only mariners themselves can control their sleep time. Training and educating mariners allows them to identify and take preventative measures that go beyond the regulations.
The prevention of fatigue in the workplace is a shared responsibility between an organization and its employees. An organization may contribute to preventing fatigue by
- educating employees at all levels on the causes and mitigation of fatigue;
- defining appropriate policies and procedures with respect to fatigue management;
- ensuring that the working environment minimizes fatigue as much as is practicable; and
- striving for continual improvement in reducing the risk of fatigue.
Employees may prevent fatigue by
- applying their knowledge of the prevention and effects of fatigue to take all reasonable steps to be well-rested for work;
- making effective use of fatigue countermeasures;
- recognizing the signs of fatigue in themselves and co-workers; and
- taking action to ensure that fatigue arising from activities inside or outside of work does not lead to performance issues.
1.15.1 Fatigue awareness training
In 2003, in response to TSB Recommendation M96-18, TC finalized a fatigue management and awareness training program for marine pilots, which was integrated within the broader training programs for apprentice pilots in Canada. The program includes a fatigue management guideFootnote 67 that presents information on sleep fundamentals, issues regarding the biological clock (circadian rhythms), the effects of irregular work schedules on fatigue, and various coping strategies that can be used to minimize the likelihood of experiencing fatigue while at work. It also includes situations that marine pilots can expect to encounter in their day-to-day work and identifies the signs of fatigue that pilots can use to self-diagnose, such as forgetting to communicate with crew, forgetting to monitor the vessel's position on a regular basis, or missing a point of reference.
The guide notes other factors that can exacerbate fatigue, including environmental conditions such as darkness, constant noise, and warm temperatures. Performing routine tasks under a low workload is noted as a factor that makes it especially difficult to fend off sleepiness, particularly for a person who is sleep-deprived. The guide also presents coping strategies that can temporarily minimize the effects of fatigue once it has occurred. These include the following:
- consuming caffeine
- turning on a bright light
- engaging in exercise
- strategic napping
- exposing oneself to intermittent loud noise
- getting fresh (cool) air
- receiving mental stimulation from conversationFootnote 68
TC has also provided the rail industry with a document entitled Fatigue Management Plans: Requirements and Assessment Guidelines, to help rail companies with the development of fatigue management plans (FMPs). Rail FMPs must be filed with TC in order to meet the industry's Work/Rest Rules for Railway Operating Employees.Footnote 69
In the civil aviation industry, there is no requirement for operators to have an FMP, but TC does provide guidance to those voluntarily adopting these programs.Footnote 70
1.15.2 Leadership training for seafarers
Annex A of the STCW code, as amended, provides standards for leadership, teamwork, and managerial skills at the operational and management levels. In response, TC developed a policy in July 2017 that addresses the mandatory requirements for leadership, teamwork, and managerial skills.
TC has stated that the amended MPR would require masters, chief officers, electro-technical officers, and officers in charge of the navigational watch on ships of 500 GT or more wishing to acquire a new or upgraded certificate of competency to provide a training certificate that includes a module on managing fatigue and stress. TC has indicated in a draft publication reviewed by the TSBFootnote 71 that the module should be at least 2 hours long and should cover the following subjects:
- causes and effects of stress and fatigue
- relationship between fatigue and stress
- identifying signs and symptoms of stress and fatigue
- stress and fatigue reduction strategies
- regulatory requirements
Given that the Nathan E. Stewart was a vessel of less than 500 GT, this new fatigue and stress training would not apply to its crew.
1.15.3 Crew endurance management systems
The expression "crew endurance" refers to a crew's ability to maintain performance within safety limits while enduring job-related physical, psychological, and environmental challenges. The Crew Endurance Management System (CEMS) is a concept developed by the USCGFootnote 72 for managing the risk factors that can lead to human error and performance degradation in maritime work environments.
1.15.4 Company management of fatigue risks
There is currently no requirement for marine companies to develop or implement FMPs or provide fatigue awareness training. Kirby did not have an FMP at the time of the occurrence, nor was it required to by regulation. The master, first mate, and second mate had not undergone training on fatigue awareness, fatigue management, or alertness strategies, nor were they required to have done so by regulation.
Although the company does not have a formal FMP, it was aware of CEMS. Kirby personnel are listed in a 2009 CEMS newsletter as providers of "CEMS Coaches Training."Footnote 73
Kirby's Common Procedures ManualFootnote 74 did set out requirements for hours of work and rest that were in accordance with the STCW code.Footnote 75 The master was responsible for ensuring that these requirements were met and that a report was periodically sent ashore.Footnote 76
1.16 Previous occurrences
1.16.1 One-person bridge operations
In each of the following previous occurrences reported to the TSB involving a tug-barge unit, 1 qualified person was alone on the bridge during transit within a compulsory pilotage area:
- In April 2002, the barge Pitts Carillon, pushed by the tug Progress, struck and knocked down Light 82 in the St. Lawrence Seaway.Footnote 77
- In April 2004, the tug Doug McKeil (with an upper and lower wheelhouse), while pushing the loaded barge Ocean Hauler, struck private docks and boathouses on the U.S. side of the St. Clair River.Footnote 78
- In July 2004, the tug Evans McKeil (with an upper and lower wheelhouse), while pushing the empty barge Ocean Hauler, struck and damaged private docks as well as a pleasure craft on the U.S. side of the St. Clair River. The tug subsequently ran aground.Footnote 79
- In September 2004, the barge A-397, pushed by the tug Karen Andrie (with an upper and lower wheelhouse), struck and knocked down Light Tower D33 in the lower Detroit River.Footnote 80
1.16.2 Fatigue
Since 1994, there have been 139 marine occurrences reported to the TSB in which fatigue was considered to be a factor. Of the 128 investigations undertaken by the TSB since 2002, fatigue was cited as a finding in 15 of them (12%). Appendix E lists 6 TSB marine investigation reports since 2006 that found risks related to fatigue and directly applicable to this occurrence.
1.17 Incident command system
The ICS allows response organizations to have a formalized structure for command, control, and coordination of the response at an emergency site (Appendix F). It is recognized worldwide as a scalable system that provides a common response framework for an event of any size.
During the day, the incident response in this occurrence was managed under the UC of federal and provincial authorities, the responsible party, and First Nations incident commanders. During night operations, the command was given to a CCG vessel in the vicinity. According to ICS guidelines, a UC "enable[s] agencies with different legal, geographic, and functional responsibilities to coordinate, plan, and interact effectively."Footnote 81 Under a UC, participating agencies can jointly manage an incident while retaining their authority and accountability by developing an incident action plan. This plan provides responders with common priorities, objectives, and strategies, with the goal of ensuring a safe and efficient response.
The intent of this type of command is to help incident commanders come to a consensus when making decisions. If the incident commanders within the UC do not agree, there are a number of factors to consider before the final authority is assigned to a specific incident commander.
1.18 Responsibilities and response
Canada's Marine Oil Spill Preparedness and Response Regime was designed to ensure that the industry has the capacity to clean up its own spills, under the leadership of TC and the oversight of the CCG.
In this occurrence, responders from several primary and secondary agencies with multiple jurisdictions were involved in the emergency response. These federal, provincial, local, First Nations, and private agencies worked together to manage the response. Approximately 30 secondary agencies participated in the incident command system during the course of the emergency response, including health authorities, marine contractors, consultants, First Nations groups, and environmental and wildlife service contractors.
The primary agencies' major responsibilities and actions taken during the response are detailed in the sections that follow.
1.18.1 Fisheries and Oceans Canada
DFO holds the lead federal role in managing Canada's fisheries and safeguarding its waters.Footnote 82 The Department's stated role is to support strong and sustainable economic growth and innovation, while contributing to a clean and healthy environment and sustainable aquatic ecosystems.Footnote 83 DFO actively participated in this occurrence on many levels, including SAR, oil spill response, and ecosystems and fisheries management.
1.18.1.1 Canadian Coast Guard
The CCG is a special operating agency of DFO. It owns and operates a fleet of vessels, air-cushion vehicles, and helicopters, and provides key maritime services to Canadians. Its responsibilities include maritime safety, protection of marine and freshwater environments, facilitation of maritime commerce and sustainable development, and support of marine scientific research. The CCG supports other government organizations by providing a civilian maritime fleet and broadly distributed shore-based infrastructure.Footnote 84
1.18.1.2 Marine Spills Contingency Plan
The Marine Spills Contingency Plan—National Chapter, issued in April 2011, defines the scope and framework within which the CCG operates when responding as the lead agency to marine pollution incidents in Canadian waters. The plan covers roles and responsibilities, preparedness, response, requests for CCG assistance, port response activities, plan maintenance, and program contacts. If the polluter responds to the incident and takes full responsibility for it, the CCG acts as the federal monitoring officer and monitors the polluter's response.Footnote 85 When the marine polluter is unknown, or is unwilling or unable to respond to the incident, or when the source of pollution (from land or sea) is unknown, the CCG assumes full responsibility for response management as the on-scene commander. In all cases, the CCG has the final authority to ensure an appropriate response.
The plan also includes the CCG's Environmental Response Levels of Service,Footnote 86 contingency planning, training, exercises, and resources. The Levels of Service are the services that CCG is expected to provide to Canadians: providing a preparedness capacity to respond to ship-source marine pollution incidents, and responding to cases of marine pollution. CCG resources are required to be activated within 6 hours of the completed assessment of a given case of pollution.
The Marine Spills Contingency Plan contains chapters on each of the 5 response regions (Pacific, Central and Arctic, Quebec, Maritimes, and Newfoundland and LabradorFootnote 87 ). Each region is responsible for developing and updating its chapter within the Plan. The Pacific region's chapter was last updated in 2001.
The Marine Spills Contingency Plan is required to be reviewed no less than every 5 years. The current plan was due for renewal in 2016, and has been updated but not made public. In the interim, in January 2017 (3 months after the occurrence), the CCG approved an Environmental Response Concept of Operations document, which states that the CCG will apply the ICS as its methodology for responding to marine pollution incidents. The CCG will be the federal incident commander and will work within a UC with the polluter and organizations that have jurisdiction over, or a mandate related to, the incident. According to the CCG, the principles in the Environmental Response Concept of Operations document were followed during the Nathan E. Stewart spill response.
1.18.1.3 Canadian Coast Guard search and rescue
As per the Oceans Act,Footnote 88 DFO and the CCG are responsible for providing federal maritime SAR operations. Of these 2 agencies, the CCG has primary responsibility. The CCG's SAR responsibilities include detecting marine incidents, coordinating and controlling SAR operations through the JRCC, and providing maritime resources to Canadians. CCG vessels may be tasked to provide assistance to a vessel aground with people on board, provided that the SAR operation does not endanger people or property and that "commercial assistance is not available or cannot be on scene in sufficient time."Footnote 89
In this occurrence, although some actions to address the pollution were taken prior to the tug's sinking, CCG procedures state that Environmental Response is not to be officially initiated until the SAR mission is completed. In total, the CCG tasked 3 vessels of various sizes with the SAR mission. The CCG's SAR mission was terminated when all crew members from the Nathan E. Stewart were on board the Bartlett. JRCC coordinators then initiated the transfer of control of the incident to CCG Environmental Response. At 1340 on 13 October, a handover message officially transferred control of the incident to CCG Environmental Response.
1.18.1.4 Canadian Coast Guard Environmental Response
The CCG is the lead federal response agency for all ship-source pollution incidents in waters under Canadian jurisdiction.Footnote 90 Under Part 8, section 180, of the CSA 2001, the Minister of Fisheries and Oceans (the minister responsible for the CCG) may take measures deemed necessary to address an incident where it is believed on reasonable grounds that a vessel is discharging, or likely to discharge, a pollutant. These measures include monitoring the response actions taken by the responsible party and, when it is considered necessary to do so, directing any person or vessel to take those same measures or to refrain from doing so.
The CCG Environmental Response program's overall mission is to "ensure an appropriate level of preparedness and response capability for all ship-source and mystery source pollution incidents in waters under Canadian jurisdiction."Footnote 91 The program's specific objectives are to minimize the impact of marine pollution incidents on public safety, the environmental impact of marine pollution incidents, and the economic impact of marine pollution incidents.
In this occurrence, the CCG Environmental Response duty officer was notified of the incident by MCTS. The duty officer collected information about the incident and assessed it. Initially, the primary objectives of the CCG vessels and crews were to stabilize and secure the ATB, conduct soundings around the incident location, transport personnel as needed, ensure the safety of the many small craft in the area, and assist those deploying booms. The Bartlett remained on scene and monitored all response activities.
Throughout the spill response, CCG personnel and vessels assisted with the spill response and salvage operations where needed, and provided on-site communications as well as situation reports to the incident command post every few hours. The CCG vessel on site was always the designated on-site commander, and provided accommodations to responders as needed. As the federal marine safety expert, the CCG was responsible for monitoring and controlling site safety (water, air, and shore operations). The CCG kept track of the various vessels and personnel entering and leaving the site, set up an exclusion zone around the tug, and provided a site-safety officer, who helped develop operational safety briefings with safety personnel committee members at the incident command post. CCG vessel personnel provided first-aid assistance, and their vessels were available for emergency response as needed.
The CCG owns and maintains pollution-response equipment in depot sites across the regions. In this occurrence, the CCG accessed and deployed this equipment with the help of other responders.
The CCG helicopter conducted several flights a day to transport personnel and cargo, provide site-viewing opportunities, monitor pollution and personnel activities, and rescue stranded personnel when necessary. CCG vessels provided trained personnel for helicopter cargo-slinging operations. Once the initial response vessels were operating under the direction of the UC, CCG personnel provided personal protective equipment and conducted approximately 16 safety inspections on spill response vessels.
In total, the CCG tasked 12 vessels, ranging from a medium-endurance multi-tasked vessel to a fast rescue craft. More than 100 CCG personnel were involved in SAR and Environmental Response operations on a daily basis.
1.18.1.5 Ecosystems and fisheries management
On 14 October 2016, DFO took precautionary action and issued the following fishery notice through its Ecosystems and Fisheries Management sector: "CHEMICAL Contamination Emergency Closure for Bivalve Shellfish in portion of Area 7."Footnote 92 DFO also issued a federal Species at Risk Act permit, which allowed the relocation of the endangered northern abalone during the tug salvage. DFO authorized the removal of the tug under the Fisheries Act,Footnote 93 which allowed the authorized representative to undertake tug-salvage operations despite the risk of harming marine life. DFO's Conservation and Protection office in Bella Bella provided on-water transportation to and from the incident site for ECCC enforcement officers. DFO biologists provided support to the Environmental Unit of the UC for issues under DFO's mandate.
1.18.2 Transport Canada
1.18.2.1 National Oil Spill Preparedness and Response Regime
TC is the lead government agency providing legislative and regulatory oversight for marine spills; the CCG assumes a lead operational role within the spill response itself. Through guidelines, policies, regulations, publications, and programs, TC works to prevent marine pollution and to prepare and respond to marine pollution incidents.
TC's environmental response system is responsible for the National Oil Spill Preparedness and Response Regime. In collaboration with the CCG, ECCC, other federal agencies and departments, and industry, the regime works to enable Canada to be ready to respond to marine oil spills of up to 10 000 tonnes per geographical area of response within prescribed time standards and operating environments. The regime applies the polluter-pay principle, which holds the polluter liable for all response costs.
TC also has an Environmental Prevention and Response National Preparedness PlanFootnote 94 that works in conjunction with its response regime. Under the plan, TC's responsibilities include the following:
- overseeing the regime implementation
- monitoring compliance with regulations and enforcement actions
- managing the National Aerial Surveillance Program
- reviewing oil-handling facility pollution prevention and response plans
- certifying response organizations and monitoring their activities during a spill response
- ensuring that prescribed vesselsFootnote 95 have the appropriate documentation
As a vessel of less than 400 GT, the Nathan E Stewart was not a prescribed vessel and was not required to be a member of, or voluntarily have arrangements in place with, a response organization. Therefore, TC's National Oil Spill Preparedness and Response Regime was not required to be implemented, and TC did not monitor the activities of the response organization during the spill response according to the Environmental Prevention and Response National Preparedness Plan. As a result, oversight of the spill response was the responsibility of the CCG.
1.18.2.2 Transport Canada Marine Safety and Security
Under the Environmental Prevention and Response National Preparedness Plan, Transport Canada Marine Safety and Security is responsible for operational compliance with the CSA 2001, and aims to ensure compliance by investigating ship-source pollution occurrences.
During the spill response, TC marine safety inspectors provided technical support to the incident command post by reviewing and approving towing and salvage plans.
In January 2017, TC implemented a planned concentrated inspection campaign focused on further assessing the compliance level of tugs and barges operating on the west coast. The campaign ran from January to March 2017, with marine safety inspectors assessing approximately 60 vessels, including some foreign vessels similar to the Nathan E. Stewart. At the time this report was prepared, the results of the campaign had not been made public.
1.18.3 Western Canada Marine Response Corporation
The WCMRC is the only TC-certified response organization on Canada's west coast and has nearly 2200 members. Under the CSA 2001, industries and vessels that are required to have an arrangement (prescribed vessels) with a response organization and that operate on the west coast must pay bulk oil cargo fees to cover the above-mentioned services and must be members of the WCMRC. In addition, industry is required to pay for all response costs associated with spill events.
Non-prescribed vessels may voluntarily become members of the WCMRC by signing a Ship Membership Agreement and Confirmation of Arrangement. Non-member vessels may also hire WCMRC as a third-party response organization.
According to the WCMRC's website,Footnote 96 it ensures a state of preparedness and
- responds within the prescribed time standards in the response organization standardsFootnote 97 (response time standards are based on spill location. For the Bella Bella region, the response time standard is 18 hours plus travel time);
- develops and works within a response plan;
- provides trained responders such as full-time and part-time staff, advisors, and contractors; and
- provides vessels and spill response equipment at strategic locations across the province.
In this occurrence, the WCMRC executed and coordinated the operational spill response by deploying equipment and personnel under the direction of the responsible party. The corporation worked within the ICS under the authority of the UC. The WCMRC posted on its website all of the incident action plans provided by the UC throughout the 42 days of the spill response.
During the spill response, the WCMRC was responsible for the on-water recovery operations under a third-party agreement with Kirby. The WCMRC's equipment, contractors, and personnel were deployed from different locations in British Columbia: Shearwater, Prince Rupert, and Vancouver Island. The WCMRC mobilized 70 personnel and 20 different types of on-water vessels, including barges, tugs, specialized spill response vessels, water taxis, landing crafts, and work boats. The WCMRC also provided safety officers with expertise regarding the safety of the spill response and helped conduct site assessments, safety briefings, response training, health and safety plans, and on-site air monitoring. In addition, the WCMRC allowed Heiltsuk First Nation and government agency observers to be present on board its vessels during recovery operations.
1.18.4 British Columbia Ministry of Environment and Climate Change Strategy
British Columbia's Ministry of Environment and Climate Change Strategy is the key provincial agency coordinating the Province's response to pollution incidents, such as marine oil spills, within its jurisdiction. The Ministry's Environmental Emergency Program provides procedures for responding to spills of hazardous materials and harmful substances. The program also develops and implements tools to prevent and prepare for spills, such as the Comprehensive Emergency Management Plan, which includes the Marine Oil Spill Response Plan.
Emergency Management BC is the emergency coordination centre that receives notification of marine spills. Once notification is received, environment emergency response officers assess the incident to determine the provincial role. The Province can monitor and/or augment the response, or take over the response as needed. According to British Columbia's Emergency Response Management System, the incident management team is organized using the ICS structure with local, federal, and industry representatives, responding agencies, and the responsible party as participants. These participants make decisions and devise strategies regarding the response and coastal resource identification, protection and treatment for intertidal shores and sea beds, wildlife protection, and oil waste handling.
In this occurrence, the Province assumed a monitoring role to ensure that the response met provincial expectations. This role included establishing public safety and environmental protection priorities. The Province also took on a sampling coordinator role by initiating and coordinating a sampling plan. Working with the Environmental Unit of the UC, the Province developed wildlife plans and submitted them to the UC for approval. The Province also used a websiteFootnote 98 to provide information about the response to the public.
1.18.5 Heiltsuk First Nation
The location of the Nathan E. Stewart's grounding was within the traditional territories of the Heiltsuk First Nation. Heiltsuk ancestral homeland includes a defining portion of what is now known as the central coast of British Columbia. It extends north from the southern tip of Calvert Island to Klekane Inlet, east to the head of Dean Channel, and to the offshore area west of Goose Island, Aristazabal Island, and Calvert Island, and includes the intervening inlets, channels, islands, and waterways.Footnote 99 Near the occurrence location, there are 9 salmon rivers, 56 clam beds, 18 cockle beds, and a northern abalone bed. The northern abalone is an endangered species protected under the Species at Risk Act.
The Heiltsuk First Nation is a self-governing nation with its own tribal council (the Heiltsuk Tribal Council), and exercises its rights to steward and harvest its resources throughout its traditional territories. The people of the Heiltsuk First Nation have stated that they depend on natural resources within their territories for food, health, traditional activities, their economy, and their cultural identity, and traditional harvesting remains integral to their distinctive culture. The Heiltsuk First Nation traditionally harvests at least 25 food species from the area affected by the spill, including salmon, halibut, ground fish, shellfish (i.e., crabs, prawn, shrimp, clams, and oysters), sea urchins, sea cucumbers, herring, herring spawn on kelp, eulachon, abalone, and seaweed.
In January 2010, the Heiltsuk Integrated Resource Management Department (HIRMD) was established to provide an integrated approach to stewardship and decision making in regard to land, water, and cultural resources within the Heiltsuk territories. The HIRMD provides technical advice to the Heiltsuk Tribal Council, including advice on land and marine-use planning, management of the land and fisheries programs, implementation of forestry initiatives, and protection of Heiltsuk culture and heritage.
Given the location of the occurrence site, vessels from the Heiltsuk First Nation were among the first on scene. The Heiltsuk First Nation was the lead local government organization involved in the UC.
On the morning of the occurrence, at approximately 0430, an emergency response officer from British Columbia's Ministry of Environment and Climate Change Strategy called and informed a HIRMD director of the incident. The director then informed other members of the community.
Early in the incident, approximately 7 Heiltsuk vessels were on scene to help, and the Heiltsuk First Nation provided vessels throughout the environmental response and salvage operations. They deployed booms, transported personnel, provided local knowledge and spill response equipment from their local fuel company, and fulfilled other logistical requirements. As the spill response continued, members of the Heiltsuk First Nation served as observers on board WCMRC vessels, and on board the SCAT and wildlife assessment team vessels.
As observers and members of the UC, the Heiltsuk First Nation provided traditional ecological, cultural, and marine knowledge and experience throughout the clean-up and tug-salvage operations. On 20 October, the First Nations Health Authority circulated a warning regarding the health hazards associated with diesel exposure.
The Heiltsuk First Nation maintains that Canada failed to consult with them on spill-response planning elements such as authority, capacity, funding, and equipment. Due to the spill, the Heiltsuk imposed a harvesting closure on the affected area. At the time this report was prepared, the Heiltsuk's closures were still in place, as was DFO's prohibition on the harvest of bivalve shellfish due to red tide contamination. The Heiltsuk First Nation is concerned that many marine species may have been contaminated, which would have a long-term impact on the Heiltsuk's commercial and traditional harvesting.
1.18.6 Environment and Climate Change Canada
ECCC is the federal authority responsible for providing environmental and scientific advice during an oil spill.
Several agencies supported the ECCC during this incident: the Emergencies Science and Technology Division, the Meteorological Service of Canada, and the Canadian Wildlife Service, all working within the National Environmental Emergencies Centre (NEEC). NEEC provided scientific and technical advice to the UC, including the following:
- weather forecasts and information on the physical operating environment
- spill movement and trajectory forecasts
- appropriate response strategies and clean-up techniques
- the location of sensitive areas
- the sampling program
- protection of sensitive ecosystems and wildlife such as migratory birds and fish
- guidance on the efforts of the UC's Environmental UnitFootnote 100
NEEC also provided a candidate to fill the new position of scientific support coordinator within the ICS. This role was to support the UC by providing on-demand environmental modelling of the pollutant, supplying weather forecasts, producing description sheets, and performing sensitivity mapping.
During SCAT operations, NEEC supplied technical specialists, who
- revised and commented on plans and reports;
- participated on site as SCAT members to offer regulatory oversight and monitor practices and clean-up methods;
- participated in the discussions in the selection of final cleaning points; and
- provided a sampling plan for long-term monitoring and the assessment of environmental impacts.
Canadian Wildlife Service technical specialists provided advice to the wildlife response and consulting company on issues regarding migratory bird protection.
ECCC's enforcement branch began an investigation of potential infractions of the environmental and wildlife acts and regulations from the operations of the ATB.
1.18.7 Nathan E. Stewart crew
The Nathan E. Stewart's Health, Safety, Quality, and Environmental Management System Policy Manual stipulates that the master has the overriding authority over the vessel and the responsibility to make decisions with respect to the safety of human life, property, and the environment.Footnote 101 Kirby has a spill response field guide that includes emergency procedures, a shipboard oil pollution emergency plan, and a shipboard marine pollution emergency plan. The guide contains specific emergency procedures for situations including grounding, containment, and oil spills.
In this occurrence, the Nathan E. Stewart's crew deployed the tank barge's pollution control equipment, assessed the damage to both vessels, monitored the fuel tank levels on both vessels, transferred fuel from the tug to the barge, and informed the relevant authorities of the incident. The master followed the company's emergency procedures for grounding in an attempt to remove the vessel from the reef. The master also ensured that the crew was ready to abandon the tug. After the vessel sank, the master and the crew assisted the CCG and salvage vessels with the barge's towline and with initial dive operations.
1.18.8 Responsible party
In this occurrence, Kirby, the company that owns the Nathan E. Stewart, was the responsible party, and the company's authorized representative acted on behalf of the responsible party. Kirby assumed responsibility for the incident, operated within the UC, and funded the spill response and salvage operations. The company also had contingency plans for marine occurrences, and had a salvage company on retainer and a response plan in place.
The authorized representative contacted the WCMRC in the early stages of the incident and requested assistance. The authorized representative signed a third-party, incident-specific agreement with the WCMRC shortly after the grounding. The same morning that the agreement was signed, another company representative arranged for and signed, with a WCMRC agent, a voluntary Ship Membership Agreement and Confirmation of Arrangement under subsection 167(1) of the CSA 2001, in an attempt to become a member of the WCMRC. The application was later reviewed and withdrawn; it was rendered unnecessary because a third-party agreement had been signed. As well, a WCMRC membership cannot be issued to a vessel during an active spill response.
On the evening of the occurrence, the authorized representative arranged for the personnel of the marine emergency response company to arrive on scene. The company's personnel were familiar with the ICS and provided internet access and necessary software to manage the documentation for the spill response and salvage. The company assisted in arranging accommodation and tracking for all responders involved in response activities.
Once the salvage company had been made aware of the incident, it deployed resources to the occurrence site. These included a dive team, several larger salvage tugs, and a heavy-lift crane.
The authorized representative also contracted a U.S. scientific advisory firm to conduct pre- and post-salvage SCAT surveys and recommend cleanup activities as necessary. Strategists and planners within the incident command post used this survey data to develop a shoreline clean-up plan. SCAT teams were involved throughout spill-response operations, conducting initial field surveys, inspections, and shoreline sign-offs, which indicate that no oil was observed on a specified shoreline.
In addition, the authorized representative contracted a wildlife response and consulting company to work with the Heiltsuk First Nation to minimize the impacts on wildlife.
The authorized representative had additional support from company personnel off-site. Kirby estimates that 28 personnel worked a total of 502 full-time days in all aspects of the spill-response and salvage operations.
1.19 Responders' after-action reviews
The CCG Marine Contingency Spills Plan states that post-incident reviews should be conducted to evaluate the CCG's response to a marine pollution incident. Not all federal agencies that responded to the spill in this occurrence conducted a post-incident review; however, some of the other responding agencies conducted reviews in the form of after-action reviews (AARs). These reviews identify lessons learned, operational and logistical problems, and safety issues, and make recommendations on how to address these issues.
The significant response issues identified in the AARs included limited communication, misunderstanding of responsibilities, lack of safety equipment, lack of training and practical exercises, and site safety.
1.19.1 Communications
The AARs indicated that communication among agencies was challenging in this occurrence. The remote location made for limited communication between the incident command post and the crews on board the vessels active in the response, the responders ashore, external agencies, and the site command. The limited VHF radiotelephone reception, satellite, and internet connections led to difficulties in establishing an effective method of communication. The incident command post's location also hindered the communication of daily action plans to spill responders who were being housed outside of Bella Bella.
1.19.2 Roles and responsibilities
Most of the AARs stated that there was confusion about the specific responsibilities of the various responding agencies, which created uncertainty for the spill responders. The lack of clearly defined responsibilities was reported within and between agencies. This confusion led to speculation about what could or should have been done during the response, as well as the reported lack of instructions and action plans in the first few days.
For example, when CCG vessels arrived on scene, there was initially an expectation on the part of the public and the Heiltsuk First Nation that the CCG would react to the spill and take direct action in the immediate spill response, rather than monitor the situation and ensure the safety of those on scene. This expectation created confusion and communication problems during the initial response to this occurrence.
1.19.3 Safety equipment
The AARs identified the lack of personal protective equipment and air-monitoring devices in the early stages of the spill response. It was noted that initial response vessel operators, acting independently of the UC, did not have adequate safety equipment—such as personal flotation devices, bailers, oars, and proper VHF radiotelephone installations—on board, and that they often operated alone. These vessel operators did not have environmental hazardous material suits, gloves, boots, eyewear, or masks in the early stages of the spill response.
1.19.4 Training and exercises
The AARs identified the need for additional training for personnel within the incident command post, spill responders, and CCG personnel. Several AARs recommended that the training be standardized and required for all future responders.Footnote 102 The ICS management structure for emergency responses was not familiar to some agencies within the UC, which led to confusion when action plans were being developed.
There was a lack of pollution response exercises and training for spill responders, who were not given any safety instructions or direction regarding how to use the oil spill response equipment before deploying it.
It was noted that the Heiltsuk First Nation's values and culture, as well as the magnitude of the spill's impact on the community, were generally not well understood by all agencies involved in the spill response. It was also noted that Indigenous cultural sensitivity training was required.
1.19.5 Site safety
Some AARs highlighted issues regarding site safety and identified unsafe conditions, such as the following:
- small vessels working close to shore in rough seas
- health concerns from spill responders working with oil products without adequate protection
- an inability to track vessels and spill responders
- the inaccuracy of the helicopter's passenger manifests
- observers on board responder vessels while those vessels were in operation
1.19.5 Operational spill response
The overall spill response was also reviewed in the AARs. Some of the operational topics reviewed were as follows:
- the accessibility, condition, and inventory of the CCG pollution equipment
- the set-up and operations of the incident command post and the UC
- the lack of TC oversight of the response organization's operations
- the response organization's capacity to respond to an additional spill in a different location
- the length and overall scale of the response
1.20 Oceans Protection Plan
Approximately 3 weeks after the occurrence, on 07 November 2016, the Government of Canada launched its national Oceans Protection Plan. The Plan aims to support safe and clean marine shipping initiatives, build partnerships with Indigenous and coastal communities, increase economic opportunities for Canadians, improve marine safety, and protect the marine environment. The overall objective is to achieve a world-leading marine safety system to prevent marine pollution incidents and to improve Canada's response to them. The plan for improved oil pollution response includes the following:
- tougher requirements for industry responses to incidents
- proactive on-water monitoring and response capacity
- enhanced sharing of marine traffic information with Indigenous and coastal communities
- developing comprehensive response systems for marine spills, such as the initiative for a regional response plan for the northern portion of British Columbia
- building greater capacity and standardization in training and exercising for CCG, Indigenous, and other responders
- improved Indigenous capacity in the design and delivery of marine safety
- the development of Indigenous community response teamsFootnote 103
1.21 Independent reviews of Canada's spill response regime
There have been several recent independent, third-party reviews of Canada's spill response regime that provide findings and recommendations.
1.21.1 Tanker safety expert panel report
In 2013, a tanker safety expert panel conducted a reviewFootnote 104 of Canada's oil spill response regime that included preparedness, the polluter-pays principle, leadership and stewardship, communication and engagement, and continuous improvement.Footnote 105
The report observations indicated the following:
- Government departments are working independently from each other. The report states, "many activities [are] being performed in silos, which hinders the cohesiveness of the federal management of spill preparedness and response."Footnote 106
- There is no nationwide framework for training and exercises. According to the report, "various government departments and stakeholders carry out their own programs, often independently from each other."Footnote 107
- There is confusion among federal agencies regarding the federal government's responsibility and leadership. The report states the following:
1.21.2 Marathassa incident review
In April 2015, the bulk carrier Marathassa discharged an unknown quantity of fuel oil into English Bay, British Columbia (TSB Marine Occurrence M15P0055). The Commissioner of the CCG initiated a reviewFootnote 109 of the incident, which was completed in July 2015. The review identified key facts, observations, and analysis in regard to the spill response, including
- confusion about the roles and responsibilities among the agencies involved;
- the lack of clarity with regard to roles and responsibilities, and who was in command and control; and
- the incident command post's lack of comprehensive multi-agency oil spill response plan, which would have aided decision making.
Following the review, 25 recommendations were made to the agencies involved in the spill response. The recommendations relevant to this occurrence included the following:
- Continue to implement the ICS and conduct exercises with all partners.
- Develop reference tools for incident command post staff regarding roles and responsibilities.
- Consider using a pre-established incident command post location.
- Assign roles and explain them to incident command post staff.
- Consider using an ICS coach.
According to the CCG's management action plan dashboard for the Marathassa environmental response operation,Footnote 110 these recommendations have been addressed.
1.21.3 Clear Seas Centre for Responsible Marine Shipping report
The Clear Seas Centre for Responsible Marine Shipping is an independent, not-for-profit research centre that provides information about marine shipping in Canada.Footnote 111 The centre's report, entitled Leading Systems for Oil Spill Response in Ports: Implications for Canada,Footnote 112 identifies issues that should be considered in an effort to improve Canada's readiness to respond effectively to spills. According to the report, the development of the Oceans Protection Plan reinforces the need for significant changes to the national Marine Spills Contingency Plan.
The report concludes with 15 implications for those responsible for Canadian's spill response regime, including the following:
- Adopt a UC as a part of the response policy.
- Improve the spill response exercise.
- Update response training for first responders.
- Review contingency plans every 3 or 5 years.
1.21.4 Research and Planning Group, LLC report
Nuka Research and Planning Group, LLC is an environmental consulting firm that specializes in international environmental projects.Footnote 113 The firm prepared a West Coast Spill Response Study for British Columbia's Ministry of Environment and Climate Change Strategy. The study consists of 3 volumes:
- Volume 1: Assessment of BC Marine Oil Spill Prevention and Response Regime
- Volume 2: Vessel Traffic Study
- Volume 3: Word Class Oil Spill Prevention, Preparedness, Response and Recovery System. An updated version of Volume 3, entitled "Marine Oil Spill Prevention, Preparedness, Response and Recovery: World Leading Approaches from Select Jurisdictions," was produced in 2015.
The objective of this study was to provide the Province with essential information to improve British Columbia's spill response regime.
Volume 3 assessed the features of a world-class response system, made recommendations, and highlighted opportunities to enhance British Columbia's response regime:
- In an effective spill response, planning is integrated across jurisdictions and sectors. A standing committee or structure consisting of government and non-government agencies should be implemented to improve planning and response management, and to minimize confusion.Footnote 114
- Incident reviews support continuous improvement: lessons learned from spills can be shared and incorporated into planning. In the event of a spill, TC and the CCG should conduct an independent incident review, using experts who did not participate directly in the spill response. This review should be made available to the public.Footnote 115
1.22 TSB laboratory reports
Various electronic components were recovered from the Nathan E. Stewart and sent to the TSB Engineering Laboratory for examination and data extraction. The components were dried, cleaned, and dismantled. Significant corrosion and salt build-up were found on the circuit boards. Most of the components did not contain any memory that would store user data.
Due to the extent of the damage, the components could not be powered up and data could not be extracted from the memory chips and hard drives. These particular components were outdated or too damaged, or did not contain any information relevant to the occurrence.
The TSB completed the following laboratory reports in support of this investigation:
- LP297/2016 – Data Extraction from Echo Sounder
- LP305/2016 – Data Retrieval from Electronics
2.0 Analysis
The TSB's investigation into the grounding of the articulated tug-barge (ATB) and subsequent sinking of the Nathan E. Stewart determined that the watchkeeper missed a crucial course alteration, which resulted in the ATB's running aground.
This analysis focuses on the risks of fatigue associated with the 6-on, 6-off watchkeeping shift schedule, as well as on the lack of fatigue-awareness and -management training, which amplifies these risks.
The analysis also examines the spill response and discusses the need for all responding agencies to work together to identify and address any deficiencies or unsafe conditions during the response. However, the report does not comment on the overall effectiveness of the spill response, the spill response equipment, or the impacts of the spill.
2.1 Factors leading to the grounding and subsequent sinking
On 13 October 2016 at approximately 0020, Marine Communications and Traffic Services recorded the ATB's last course alteration toward the entrance of Seaforth Channel, British Columbia. For the next 46 minutes, the ATB's course and speed remained constant until it grounded on Edge Reef, near Athlone Island, approximately 10 nautical miles (nm) west of Bella Bella, British Columbia.
The investigation determined that the second mate, who was working alone on the bridge and was fatigued, was asleep when the ATB passed approximately 1 nm abeam of Ivory Island at the entrance to Seaforth Channel, and did not make the planned course alteration into the channel. The ATB then struck and grounded on a reef.
The navigational alarms were not used and a bridge navigational watch alarm system (BNWAS) was not available. The use of these could have prevented the second mate from falling asleep and provided a warning to other crew members or an alert when the course alteration had been passed. The assistant tankerman, who was the second person on watch, was not stationed on the bridge. After contact with the second mate could not be made over the tug's intercom radio, the assistant tankerman did not reach the wheelhouse to check on the second mate before the ATB grounded.
Following the grounding, and after several hours of continuous interaction between the tug's hull and the reef, the hull breached and diesel oil was released into the environment. The tug filled with water and sank 8.5 hours after it first struck the reef. The pollution boom around the tug did not contain the diesel oil. Approximately 110 000 L of oil were not recoverable and were left in the environment; 119 000 L of oil were recovered from the tug.
2.2 Bridge-manning requirements
To ensure safe navigation, it is critical that there be sufficient personnel available to carry out safety-critical tasks such as monitoring the vessel's progress, steering, and performing lookout duties. It is therefore essential that adequate consideration be given to bridge watch composition and workload management.
The mandate of the Pacific Pilotage Authority Canada is to ensure safe navigation in the designated pilotage waters of British Columbia through the use of a pilot, or by issuing a pilotage waiver to vessels and their watchkeepers when specific conditions are met.
The Seafarers' Training, Certification and Watchkeeping(STCW) code sets the standard for bridge watch composition, and recommends that certain measures be in place before a 1-person bridge watch begins. These measures reduce the risk of a single point of failure.
In this occurrence, the Nathan E. Stewart was operating without an effective 2-person bridge-watch system while transiting through British Columbia's compulsory pilotage waters, contrary to the federal Marine Personnel Regulations (MPR). Although the tug had a 2-person watch system in place, the additional person on the watch was primarily occupied with conducting safety rounds and ship-husbandry duties, and was not stationed on the bridge. No one on the bridge-watch team was aware of Kirby Offshore Marine Operating LLC's (Kirby's) procedure that required an additional person on the bridge watch while transiting in pilotage waters, despite both internal and third-party routine audit programs designed to evaluate a crew member's knowledge and application of Kirby's Common Procedures Manual.
The 2-person watch system used by the Nathan E. Stewart and other U.S. tugs holding a pilotage waiver is deemed acceptable by the U.S. Code of Federal Regulations, which state that a 2-person bridge watch is not required even during hours of darkness if the master and/or officer of the watch does not identify a risk with a 1-person bridge watch.
The TSB investigation determined that, for many tugs, the normal practice was to have a 2-person watch (i.e., only 1 person stationed on the bridge), as opposed to a 2-person bridge watch.
Furthermore, it was common practice not to use the Nathan E. Stewart's navigational alarms. For example, the cross-track error or waypoint arrival alarm could have alerted the second mate to the fact that a course alteration was missed. The use of a radar guard zone could have warned the second mate of the proximity of Athlone Island, and the depth alarm may have provided a warning of the impending collision with the reef. If the available audible alarms had been used, the second mate could have been alerted to the missed course alteration and the proximity of land.
The tug was not equipped with a BNWAS. Although the use of a BNWAS does sound an audible alarm when the navigator does not acknowledge a visual warning after a predetermined period of time, it is not a substitute for an effective lookout.
Communication between the second mate and the assistant tankerman was never established. Consequently, the second mate was the single point of failure, with no other means, other than personal vigilance, of ensuring that there was an effective watch.
If a 1-person bridge watch is in use without mitigating measures, particularly during the hours of darkness, a single point of failure may occur, increasing the risk of an accident.
2.3 Fatigue
Fatigue has been recognized as a factor in many marine accidents.Footnote 116 Footnote 117 Certain vessel working conditions, such as working in isolation, having a poor sleep environment, and shift work, may increase the risk of fatigue‑related accidents. Although challenging shift schedules, such as a 6-on, 6-off schedule, are commonly used and are at times unavoidable in 24/7 marine transportation operations, companies can establish effective countermeasures to mitigate the risk of fatigue for crew members who work those shift schedules.
Based on the analysis of fatigue factors, and the fact that the second mate fell asleep approximately 15 minutes before the grounding, the investigation concluded that the second mate was fatigued. This fatigue impaired the second mate's ability to carry out his watchkeeping responsibilities, which resulted in the grounding.
2.3.1 6-on, 6-off shift schedule
To ensure that seafarers obtain sufficient sleep, the STCW code establishes the minimum hours of rest (off-duty hours) for seafarers internationally. Transport Canada's MPR provide the regulatory means by which the risks of fatigue are addressed in the marine industry in Canada, and incorporate the requirements set out in the STCW code.
In this occurrence, the crew had been working the 6-on, 6-off shift schedule for 58 of the 72 hours leading up to the grounding, including the morning prior to the occurrence. Although this system fulfills the provisions of the STCW code and the MPR, such that hours of rest are divided into no more than 2 periods, "one of which is at least 6 hours in length,"Footnote 118 this schedule has been called into question by various studies and experts internationally.Footnote 119 Footnote 120 Footnote 121 The investigation identified the following deficiencies with the 6-on, 6-off schedule:
- A continuous period of 6 hours of rest is impossible due to the time required for daily chores, personal hygiene, meals, shift-change briefings, and unscheduled interruptions.
- Having to meet daily sleep needs in 2 sleeping periods interrupts normal sleep patterns and disrupts sleep architecture.
- Sleep taken in the afternoon is more likely to be of poor quality, because it occurs at a time when people are physiologically prepared to be awake.
- Watchkeepers on watch during the night shift are at risk of falling asleep because people are physiologically prepared for sleeping at this time.
- If an individual finds it difficult to nap, and if the environment is not conducive to daytime napping, this kind of shift schedule presents an even higher risk of fatigue.
Because crews are not actually achieving 2 continuous 6-hour periods of rest, this shift schedule is inconsistent with the MPR and the STCW code.
On board the Nathan E. Stewart,although the second mate was consistently able to obtain at least 4 hours of good quality sleep during the morning hours, the second mate was generally unable to fall asleep in the afternoons and early evenings. Because deep sleep occurs primarily in the first half of the daily sleep period,Footnote 122 it is likely that the second mate was obtaining sufficient deep sleep, but insufficient rapid eye movement (REM) sleep. Chronic restriction of REM sleep is associated with impaired cognitive function and increased fatigue.Footnote 123
If a 6-on, 6-off shift schedule is used without fatigue-mitigating measures, there is a risk that crew members will be impaired by fatigue while on duty.
2.3.2 Fatigue awareness and management training
In this occurrence, the company that owned the Nathan E. Stewart did not provide training to the crew on fatigue awareness and/or management (including mitigation strategies), and none of the crew on board the Nathan E. Stewart had undergone fatigue awareness training prior to working for the owners of the tug. As a result, the symptoms of fatigue in the second mate were not identified, prevented, or mitigated, leading to the second mate's falling asleep while on bridge watch.
In the maritime industry, shift schedules alone do not normally present an unreasonable risk of crews' falling asleep when on bridge watch, if steps are also taken to mitigate the risks. In this occurrence, several characteristics of the bridge environment were sleep-inducing, increasing the likelihood that the second mate would fall asleep. The following mitigation strategies could have reduced that risk:
- having a second person on the bridge
- keeping the temperature in the wheelhouse cool
- keeping the light level as intense as possible without inhibiting night vision
- requiring the watchkeeper to stand up and move around rather than stay seated
- having the watchkeeper use non-automated methods to navigate
- using navigational alarms, including activating the audible component of these alarms
- the installation and use of a BNWAS
Although hours of work and rest requirements represent a layer of defence, they are not a guarantee that mariners will obtain adequate sleep. More is needed to effectively and reliably prevent fatigue among mariners. A fatigue management plan is a means of establishing more than minimum hours of rest and can address fatigue awareness training, use of alertness strategies, and fatigue-reporting mechanisms to monitor actual levels of operational fatigue. Shared night shifts, longer and more frequent breaks, increased use of the 4-on, 8-off shift schedule, and a limit of 9 working hours a day have also been proposed.Footnote 124
The United States Coast Guard has developed, and promotes deployment of, the Crew Endurance Management System for managing the risk factors that can lead to human error and performance degradation in maritime work environments. In Canada, the development of fatigue management plans is required in the rail industry but not in the marine industry, nor is there any requirement for fatigue-related training.
If there is no requirement for crews to receive fatigue-awareness or -management training, there is a continued risk that fatigue will not be identified, prevented, or mitigated.
2.4 Management of the emergency spill response
In this occurrence, a number of factors and dynamics influenced the spill response. Throughout its investigation, the TSB examined search-and-rescue operations, spill response, responder responsibilities, salvage operations, and after-action reviews, by reviewing
- the responsibilities and responses of the major agencies involved;
- applicable standards and regulations;
- communications and operational protocols;
- practices and procedures;
- applicable directives, plans, and concepts;
- the after-action reports completed by those involved; and
- independent studies of Canada's spill response regime.
2.4.1 Initial response
At the onset of most large-scale emergencies, people experience surprise, disbelief, and confusion, and encounter logistical and communication problems. In this occurrence, these reactions and problems were heightened due to the location of the incident. Site accessibility, environmental conditions, and the cultural, social, and economic importance of the area to the Heiltsuk First Nation had to be considered and addressed. Local vessel operators who initially responded were neither trained nor suitably equipped to deal with the hazardous conditions they faced.
Despite the logistical challenges, initial confusion, and issues with communication, within the first 6 hours of the incident the CCG search-and-rescue program was activated, followed by CCG Environmental Response, and the authorized representative (on behalf of the responsible party) took control of the spill response and salvage operations. The authorized representative contracted several marine spill experts and many other vessel resources.
All of the required personnel from the primary agencies involved were deployed and made their way to Bella Bella as available transportation allowed. There was no delay in the agencies' reaction to the incident and the oil spill response, and the recovery efforts of both the Western Canada Marine Response Corporation and the CCG met the prescribed time standards.
2.4.2 Incident command system
The key to the successful implementation of an incident command system (ICS) and unified command (UC) is planning and exercising, so that all agencies involved fully understand their roles and responsibilities. Priorities, objectives, and jurisdiction need to be defined, and the ICS's and UC's roles, responsibilities, resources, and capabilities need to be identified.
In this occurrence, the CCG Environmental Response did not manage the spill response in accordance with the 2011 Marine Spills Contingency Plan. Instead, within hours of the occurrence, an ICS and a UC were established, based on the CCG's Environment Response Concept of Operations document, which had yet to be operationalized, published, and exercised. Other responding agencies, and some CCG personnel, were not familiar with the ICS, which created confusion about the roles and responsibilities of all responding agencies and about who had final authority.
For example, with the adoption of an ICS and the different perspectives of UC participants comes the risk of disagreements. According to ICS guidelines, if participants in the UC cannot come to a consensus in their decision-making process, factors that are to be considered in determining who will have the final authority include
- the type, size, and location of the response;
- statutory authority enacted by legislation;
- lead jurisdiction (local, federal, and provincial authorities and Indigenous Peoples may all have a claim to primary jurisdiction); and
- the commitment level of personnel and resources.
In this occurrence, the federal incident commanders assumed that the CCG had final authority, and the other incident commanders were aware of this assumption. The CCG is considering clarifying that, in cases of ship‑source pollution where CCG is the lead federal agency and a UC is established, the CCG maintains final authority on behalf of Canada to overrule the UC.
A successful implementation of an ICS and a UC relies on a full understanding of the functionality of ICS, especially with regard to the roles and responsibilities of its participants and final authority; this information should be established and documented in all relevant emergency response plans well before an emergency occurs. Informed and coordinated responding agencies can therefore support each other more effectively.
2.4.3 Post-response evaluation
In contrast to other countries, Canada has had few large marine oil spills. Other countries' spill response and management regimes would provide Canada with models and lessons applicable to its own system. According to the Clear Seas Centre for Responsible Marine Shipping report, Canada's spill response plans can be improved.Footnote 125
Several of the independent reports that have evaluated Canada's current spill response regime have also commented on the need for a comprehensive incident review each time a spill occurs, to support the continuous improvement of the regime. These reports state that each review must be independent and conducted by experts who did not participate directly in the response; the results of each review must be shared publicly and incorporated into future planning.
The CCG's Marine Spills Contingency Plan is the only response plan that requires a spill response review. The impact of decisions and actions taken by other spill responders is not considered and, therefore, system-wide inefficiencies are not identified.
Other responding agencies conducted their own after-action reviews (AARs) of the spill response in this occurrence, independent of the CCG's review. The majority of the AARs were conducted without input from or consultation with other responding agencies. The investigation found that each AAR evaluated the internal aspects of its own agency's response, from that agency's perspective, and within the scope of its response responsibilities.
There is no requirement within Canadian regulations or agencies to conduct a coordinated and comprehensive evaluation or review of spill responses, in order to identify and address issues as if the emergency response body were 1 agency. Conversely, the U.S. Coast Guard does have a spill response policyFootnote 126 that requires an outside reviewer to conduct an Incident Specific Preparedness Review. Under this policy, the reviewer must have substantive expertise related to the event but cannot have been directly involved in the response. The reviewer's evaluation of the actions of the U.S. Coast Guard is done in conjunction with an examination of the national, regional, and local spill response.
A coordinated and comprehensive lessons-learned session or evaluation, with the participation of all agencies involved, may identify spill response deficiencies and inefficiencies more effectively than individual evaluations such as agency AARs, including issues with the ICS.
If a coordinated and comprehensive evaluation of the response to an environmental spill is not conducted, there is a risk that shortfalls will go unidentified by the response groups as a whole, resulting in a missed opportunity to improve Canada's overall spill response regime.
3.0 Findings
3.1 Findings as to causes and contributing factors
- The second mate, who was working alone on the bridge, was fatigued.
- The second mate fell asleep and did not make the planned course alteration, and the articulated tug-barge struck and grounded on a reef.
- The navigational alarms were not used and a bridge navigational watch alarm system was not available; the use of these could have prevented the second mate from falling asleep and provided a warning to other crew members.
- The other crew member on watch was not on the bridge and did not reach the wheelhouse prior to the grounding.
- Following the grounding, and after several hours of continuous interaction between the tug's hull and the reef, the hull breached and released diesel oil into the environment.
- The pollution boom around the tug did not contain the diesel oil; approximately 110 000 L of diesel oil were not recoverable and were left in the environment.
3.2 Findings as to risk
- If a 1-person bridge watch is in use without mitigating measures, particularly during the hours of darkness, a single point of failure may occur, increasing the risk of an accident.
- If a 6-on, 6-off shift schedule is used without fatigue-mitigating measures, there is a risk that crew members will be impaired by fatigue while on duty.
- If there is no requirement for crews to receive fatigue-awareness or -management training, there is a continued risk that fatigue will not be identified, prevented, or mitigated.
- If a coordinated and comprehensive evaluation of the response to an environmental spill is not conducted, there is a risk that shortfalls will go unidentified by the response groups as a whole, resulting in a missed opportunity to improve Canada's spill response regime.
3.3 Other findings
- There was no delay in the agencies' reaction to the incident and the oil spill response, and the recovery efforts of both the Western Canada Marine Response Corporation and the Canadian Coast Guard met the prescribed time standards.
- Other responding agencies, and some Canadian Coast Guard personnel, were not familiar with the incident command system, which created confusion about the roles and responsibilities of all responding agencies and about who had final authority.
4.0 Safety action
4.1 Safety action taken
4.1.1 Pacific Pilotage Authority Canada
On 16 October 2016, 3 days after the occurrence, the Pacific Pilotage Authority Canada (PPA) informed the authorized representative that, effective immediately, all British Columbia coast pilotage waivers held by all Kirby Offshore Marine Operating LLC vessels and marine officers were being revoked.
Following the occurrence, the PPA began to monitor vessel traffic entering the pilotage area. The traffic monitoring resulted in the identification of 17 companies operating in compulsory pilotage waters without a pilot or the required PPA pilotage waiver.
On 24 October, 11 days after the occurrence, the PPA issued a letter explaining amendments to its waiver system to companies that held a pilotage waiver. These amendments stated that all vessels must have 2 people on the bridge at all times while operating in confined waters, and that 1 of those must be the waiver holder. The amendments also indicated that vessels carrying petroleum products as cargo but not delivering fuel to local communities
- are no longer allowed to transit the northern section of the Inside Passage;
- are to follow a route between mainland British Columbia and Haida Gwaii; and
- in adverse weather conditions, and after clearance with vessel traffic, can proceed through Laredo Channel and Principe Channel by entering via Laredo Sound or Browning Entrance (Appendix C, route B).
These additional requirements were immediately implemented on an interim basis, until a full risk assessment was conducted.
From November 2016 to May 2017, a risk assessment project was undertaken to assess the interim amendments for their net impact on safety, identify any inherent safety gaps, and make recommendations for further improvements to the safety of vessels operating under pilotage waivers on British Columbia's northern coast. The project's risk management team was composed of the PPA, Transport Canada (TC), the Canadian Coast Guard (CCG), the United States Coast Guard, BC Coast Pilots, the Council of Marine Carriers, First Nations groups, and Canadian and U.S. company pilot waiver holders.
The project concluded that the interim measures implemented by the PPA in October 2016 were effective in reducing the navigational risk to pilotage-waiver traffic on the north coast of British Columbia. On 23 May 2017, the PPA released the project report, entitled A Risk Assessment of the Pacific Pilotage Authority's Process for Granting Waivers from Compulsory Pilotage of the BC Coast. The report recommendations are incorporated within the PPA's "Standard of Care" Implementation Guidelines.Footnote 127 Although these guidelines do not have the force of law, they include the conditions under which the PPA will consent to granting waivers to qualified applicants.
On 14 August 2017, after further consultation with TC, the PPA proposed amendments to its guidelines for granting future pilotage waivers, eliminating the option of a 1-person bridge watch during the hours of darkness, by clarifying "that the relaxation of the requirement for two persons on the bridge should only be considered available in conditions of daylight and good visibility."Footnote 128
4.1.2 Canadian Coast Guard
Within the first 48 hours of the spill response, it was noted that the initial response vessel operators did not have adequate safety equipment, environmental hazardous material suits, gloves, boots, eyewear, or masks on board, and that they often operated alone. The initial community-level response vessels and volunteers responded to local beaches and to the spill site independent of the unified command structure and its operations and safety branches. First responders outside of the unified command structure are generally not obligated to follow directions from the CCG. The CCG is not able to maintain an exclusion zone on the water, making enforcement of public safety challenging.
To address this, the CCG has implemented a training and engagement process with coastal and Indigenous communities that will outline personal safety issues, provide exposure to the incident command system, and offer equipment and training to assist with first response.
4.1.3 Transport Canada
On 26 September 2017, after consultations with the PPA on its amendments to the guidelines for granting future pilotage waivers, TC issued Ship Safety Bulletin No. 07/2017, "Deck Watch Requirements for all Canadian and Foreign Vessels, Including Tug Boats Operating in Waters Under Canadian Jurisdiction," which is intended to remind all foreign and Canadian vessel owners and operators of the deck watch requirements that are to be observed on their vessels, as stipulated by the Marine Personnel Regulations.
4.1.4 Kirby Offshore Marine Operating LLC
Kirby Offshore Marine Operating LLC has reported taking the following safety actions:
- installing a bridge navigational watch alarm system on all of its vessels
- ensuring that all of its tugs that transit British Columbia coastal waters have a Ship Membership Agreement and Confirmation of Arrangement with the Western Canada Marine Response Corporation
- requiring crew members to complete a 5-day navigation simulator training program before being promoted to officer of the watch
- implementing a "Wheelhouse Assessment Program" designed to provide a peer-led, onboard oversight of vessel watchkeeping practices
- revising its Watch Change Conference Checklist to include verification of watch readiness
- hiring 3 additional personnel dedicated to providing oversight of vessel crewing issues
- improving its mariner licensing and credential verification process, as follows:
- a crewing manager is tasked with overseeing compliance; and
- new software now tracks crew compliance with licensing and credential requirements, produces weekly reports, and notifies the crew manager when a licence or similar requirement is set to expire
- making amendments to its Common Procedures Manual to require
- the activation and use of electronic charting system software at all times
- boundary crossings and cross-track error alerts to be enabled at all times
- that, in addition to the officer of the watch, a lookout be posted in the wheelhouse at all times when a vessel is underway in pilotage waters (including "compulsory pilotage areas" as set out in the Pilotage Act)
4.2 Safety action required
Sleep is a fundamental biological need. Fatigue is the biological symptom of the unsatisfied need for sleep. Obtaining an insufficient quantity or quality of sleep results in fatigue, which impairs performance and, in the extreme, inevitably leads to falling asleep. These consequences of fatigue are significant risk factors and predictors of occupational accidents and injuries,Footnote 129 motor vehicle accidents,Footnote 130 and transportation occurrences.Footnote 131
A number of factors can increase a person's level of fatigue, including the nature of the work being undertaken, having a poor sleep environment, and working a 6-on, 6-off shift schedule. Individual factors such as the inability to nap can also influence a person's ability to obtain restorative sleep.
The use of the 6-on, 6-off shift schedule is a longstanding practice in the marine industry and was not designed according to principles of modern sleep science. Watchkeepers who work this schedule face challenges in achieving sufficient uninterrupted restorative sleep because of the needs presented by, for example, daily chores, meals, and shift-change briefings. Furthermore, total daily sleep needs on this schedule can only be met by sleeping in 2 separate periods, which creates a situation that presents other challenges; for example, any sleep taken during the daytime period may be of poor quality given that it occurs at a time when human beings are physiologically prepared to be awake.
Although the 6-on, 6-off shift schedule has been called into question by various studies and experts internationallyFootnote 132 Footnote 133 Footnote 134 Footnote 135 Footnote 136 it continues to be used throughout the marine industry. For example, in this occurrence, the watchkeepers of the Nathan E. Stewart had been working this schedule for over 2 days prior to the grounding. Opportunities to sleep were provided, but the second mate's inability to nap, combined with the sleep-inducing conditions on the bridge, led to increased fatigue and resulted in the second mate's falling asleep while on watch. Consequently, a planned course alteration was not made and the tug ran aground.
Given that accidents caused by fatigue still occur, there is a compelling need for seafarers to recognize and address the factors that contribute to fatigue.
Internationally, fatigue is recognized as a safety issue. Annex A of the Standards for Training, Certification and Watchkeeping Convention was amended in 2010 to include the requirement that seafarers undergo training on how to manage fatigue. As a basis for ensuring that seafarers obtain sufficient sleep, the Seafarers' Training, Certification and Watchkeeping (STCW) code also establishes minimum hours of rest. However, the Standards for Training, Certification and Watchkeeping Convention does not apply to non-convention vessels, such as small tugs and fishing vessels.
TC's Marine Personnel Regulations (MPR) provide the regulatory means by which risks of fatigue are addressed in the Canadian marine industry, and incorporate the STCW code. However, the MPR do not identify what fatigue is or its associated risk factors. This approach is limited because of the impossibility of regulating sleep, as opposed to rest periods. Regulations that specify hours of work and rest represent one layer of defence, but they do not guarantee that seafarers will obtain adequate sleep.
Currently, the MPR are being revised to include mandatory training on fatigue management for masters and officers on vessels of 500 gross tonnage or more who are seeking to acquire a new or upgraded certificate of competency. This means that all currently licensed watchkeepers working on larger vessels, and all watchkeepers on smaller, non-convention vessels such as the Nathan E. Stewart (i.e., the vast majority of watchkeepers), will not benefit from the same training requirements and, as a result, may not have the same level of awareness of fatigue and its risk factors.
Although fatigue is widely accepted as an unavoidable condition within the marine industry and is recognized as a contributing factor in many marine accidents,Footnote 137 there is a general lack of awareness of the factors that cause fatigue. If watchkeepers have an understanding of those factors and of the practical actions that can be taken to minimize their effects, there may be a significant reduction in the number of fatigue-related occurrences.
The Board therefore recommends that
the Department of Transport require that watchkeepers whose work and rest periods are regulated by the Marine Personnel Regulations receive practical fatigue education and awareness training in order to help identify and prevent the risks of fatigue.
Transportation Safety Recommendation M18-01
In addition to providing fatigue education and awareness training, all 24/7 transportation operations must effectively manage the risks associated with fatigue. Although training is one layer of defence, it is not enough to effectively and reliably prevent fatigue; a proactive, multifaceted approach is necessary.
The U.S. Coast Guard has developed, and promotes deployment of, the Crew Endurance Management System for managing the risk factors that can lead to human error and performance degradation in maritime work environments.
Fatigue in the Canadian rail industry has been studied and recognized as a risk since 1986. As a result, TC has provided the rail industry with a document entitled Fatigue Management Plans: Requirements and Assessment Guidelines to help rail companies develop fatigue management plans (FMPs). Rail FMPs must be filed in order to meet the industry's Work/Rest Rules for Railway Operating Employees.Footnote 138
The current Canadian regulatory regime for the aviation industry does not reflect scientific principles and knowledge of fatigue, regarding working at different times of the day, sleep hygiene and quality, and mitigating the effects of cumulative fatigue. Transport Canada Civil Aviation, in recognition of this gap, is in the process of changing flight crew hours of work and rest periods.Footnote 139 Transport Canada Civil Aviation is also proposing an exemption mechanism for all air transport services operating with an approved fatigue risk management system.Footnote 140
In response to TSB Marine Recommendation M96-18, TC developed and implemented fatigue-management and -awareness training materials for marine pilots. However, more is needed to effectively and reliably prevent fatigue among all seafarers.
An FMP is a proactive, multifaceted means of establishing more than just sufficient periods during which watchkeepers can achieve restorative sleep. It can address other important issues, such as fatigue awareness training; policies, procedures, and a working environment that mitigates factors that contribute to fatigue; and mechanisms that strive for continual improvement in fatigue management.
Implementing effective fatigue education and awareness for watchkeepers is one step that will assist the marine industry in going beyond the regulations to mitigate the risk of fatigue. Implementing comprehensive FMPs within the marine industry will bring it in line with approaches to fatigue management that have already been adopted by the rail and air transportation modes.
The Board therefore recommends that
the Department of Transport require vessel owners whose watchkeepers' work and rest periods are regulated by the Marine Personnel Regulations to implement a comprehensive fatigue management plan tailored specifically for their operation, to reduce the risk of fatigue.
Transportation Safety Recommendation M18-02
This report concludes the Transportation Safety Board of Canada's investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .
Appendices
Appendix A – General arrangement of the Nathan E. Stewart
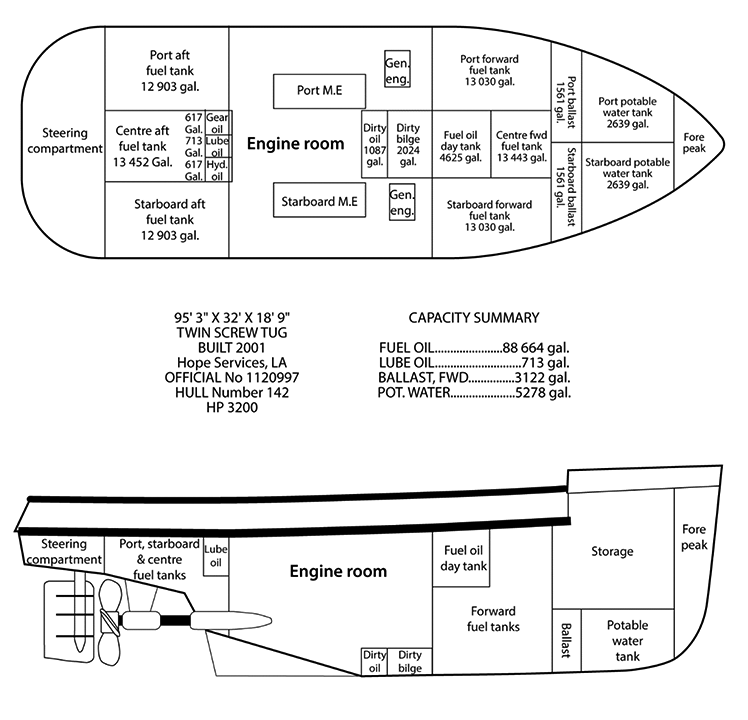
Appendix B – Area of the occurrence
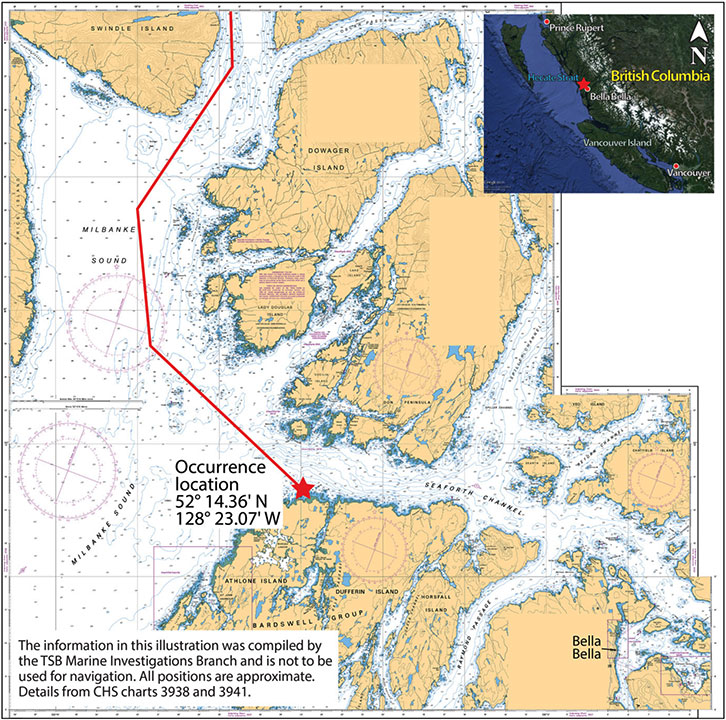
Appendix C – Compulsory pilotage waters and Inside Passage
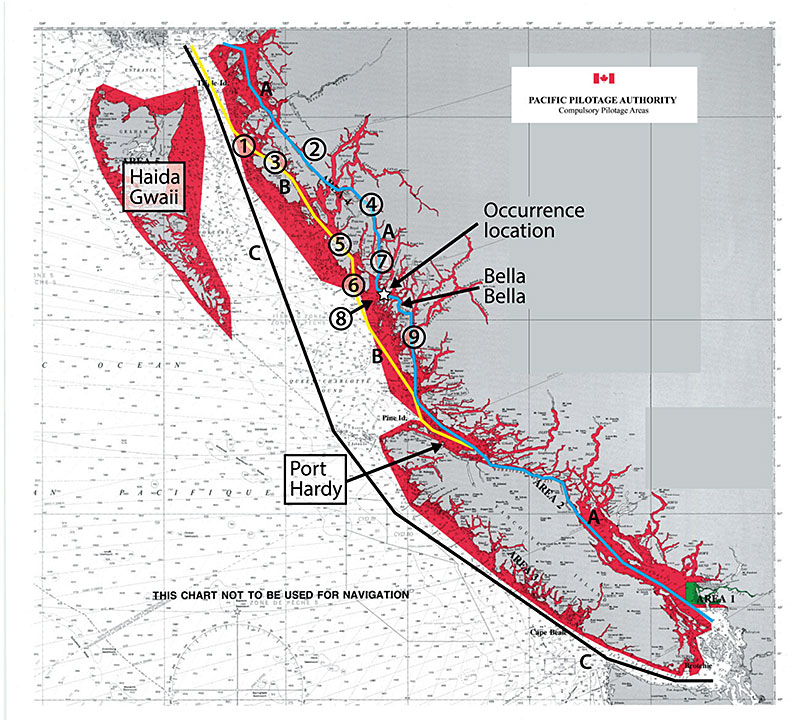
Source: Pacific Pilotage Authority Canada, with TSB annotations
Legend
- Inside Passage
- Weather route
- Non-compulsory pilotage waters
- Browning Entrance – route B
- Grenville Channel – route A
- Principe Channel – route B
- Princess Royal Channel – route A
- Laredo Channel – route B
- Laredo Sound – route B
- Finlayson Channel – route A
- Seaforth Channel – route A
- Fitzhugh Channel – route A
Appendix D – Definitions of fatigue risk factors
Acute sleep disruptions
Acute sleep disruptions are reductions in the quality or quantity of sleep that have occurred within the previous 3 days. Acute reductions in the quantity of sleep are normally considered remarkable when they are at least 30 minutes in duration and the amount of deep sleep or rapid eye movement (REM) sleep is curtailed.
Chronic sleep disruptions
Any disruptions to sleep quantity or quality that are sustained for periods longer than 3 consecutive days are considered chronic sleep disruptions. Comparing the amount of sleep obtained to the amount of sleep required for a given period of wakefulness can provide an estimate of a person's sleep debt. A sleep debt of more than 2 hours over a 7-day period may be indicative of chronic fatigue.
Although chronic sleep disruptions may be small, they can change an individual's sleep architecture. For example, the amount of deep sleep or REM sleep may be reduced without any reduction in total sleep time, resulting in fatigue. Disruptions in the quality of sleep for mariners include being at sea for extended periods, working shifts that divide sleep periods, and sleeping in environments with noisy crewmates, vessel engines, and rough seas, all of which can disrupt sleep quality without a person being aware of the change.
Circadian rhythm disruptions
There are numerous daily biological (circadian) rhythms in humans; some research indicates that there are hundreds.Footnote 141 Optimal human performance occurs when all the circadian rhythms are synchronized to each other as well as to external time cues. These time cues include the light–dark cycle, meal times, and socializing periods. People working shifts with irregular patterns usually have to adjust their sleep–wake patterns quickly to keep up with the changing shifts. Changing sleep–wake patterns too quickly can cause circadian rhythms to desynchronize.Footnote 142
Desynchronization occurs because each biological rhythm adapts to a new sleep–wake pattern at a different rate.Footnote 143 For those who work continuous night shifts, circadian patterns may change and adapt over time. However, for those who operate only occasional night shifts, circadian patterns will not adapt. In general, researchers have found that the adjustment of the human circadian system resulting from changes to the sleep–wake pattern occurs at a rate of 1 to 1.5 hours per day. Adjusting from being awake during the day to being awake at night, a 12-hour difference, could take between 12 and 18 days for complete adjustment to take place and optimum performance to return. Operating only a few night shifts, especially sporadically, will not result in optimum circadian adjustment and performance will continue to be affected by circadian lows.Footnote 144 Footnote 145
Desynchronization can cause fatigue, daytime sleepiness, psychomotor impairment,Footnote 146 impaired performance, insomnia,Footnote 147 other sleep disturbances, reduced cognitive skills, and muscle fatigue. Symptoms of desynchronization may also result in a further reduction in sleep time and quality. Employees working on shifts with variable start and finish times will constantly be susceptible to the development of desynchronization, regardless of the length of time they have worked variable shifts.Footnote 148 Fatigue is therefore known to increase as start time variability increases.Footnote 149
Timing
Performance and cognitive functioning are generally worst during the period when circadian rhythms dictate sleep, typically at night for diurnal workers and more specifically during a principal period of drowsiness that occurs between 0300 and 0500. Irrespective of motivation and circumstances, a person may have a hard time remaining alert during periods of maximum drowsiness. Performance on specific measurements such as reaction time,Footnote 150 arithmetic and signal detection,Footnote 151 and reaction to safety alarm alertsFootnote 152 have all been demonstrated to be worst during this period.Footnote 153 Footnote 154
Continuous wakefulness
The Transportation Safety Board of Canada defines continuous wakefulness as being awake for longer than 17 hours.
Appendix E – Recent marine occurrences in which fatigue was found to be a risk or causal factor
M12L0147 (Tundra) – On 28 November 2012, the bulk carrier Tundra ran aground off Sainte-Anne-de-Sorel, Quebec. The investigation found that fatigue was likely a factor in the pilot's diminished situational awareness and that "[i]f pilots are not trained in fatigue awareness, there is a risk that they may not be able to identify symptoms or signs related to sleep disorders that are not detectable through a regular medical exam."
M12N0017 (Beaumont Hamel) – On 30 May 2012, the passenger ferry Beaumont Hamel experienced an electrical failure that resulted in the loss of propulsion control and steering as it approached the wharf at Portugal Cove, Newfoundland and Labrador. The vessel then struck the wharf. The investigation found that "[f]atigue-management plans that do not provide sufficient opportunity for restorative sleep increase the risk of reduced crew performance on a routine basis."
M12F0011 (Viking Storm) – On 28 September 2012, the Canadian fishing vessel Viking Storm collided with the American fishing vessel Maverick, in thick fog, 30 nautical miles off La Push, Washington. The investigation found that the cognitive abilities of the mate were reduced due to fatigue. The investigation also found that "[i]f fishermen equate resting with sleeping in terms of its restorative capacity, there is a risk that they may underestimate the continuous hours of sleep necessary to restore their cognitive functions." As well, the investigation found that "[w]ithout a fatigue management plan that considers fishing operations and the need to ensure uninterrupted sleep, crew members may not be sufficiently rested to safely perform their duties."
M09W0064 (Velero IV) – On 08 April 2009, the U.S. fishing research vessel Velero IV collided with the U.S. fishing vessel Silver Challenger II east of the Numas Islands in Queen Charlotte Strait, British Columbia. The investigation found that "[w]ork/rest schedules that do not provide for sufficient restorative sleep are likely to lead to fatigue, performance degradation, and errors due to lack of attention, alertness, and vigilance."
M07L0158 (Nordik Express) – On 16 August 2007, the passenger vessel Nordik Express struck Entrée Island while approaching the entrance to Harrington Harbour, Quebec. The investigation found that "[i]n the absence of a fatigue management plan, the probability of fatigue-induced errors increases, thereby increasing the risk to vessels, crew, passengers, and the environment."
M06N0014 (Kometik) – On 08 April 2006, a welder and a crew member were performing welding repairs on the shuttle tanker Kometik when an explosive vapour mixture was ignited in the vessel's cargo tank in Conception Bay, Newfoundland and Labrador. The investigation found that a crew member was working while in a fatigued state. The investigation also found that "[t]he vessel's shipboard safety manual did not identify fatigue or workload as risk factors and did not incorporate procedures to mitigate them."
Appendix F – Incident command system organization chart
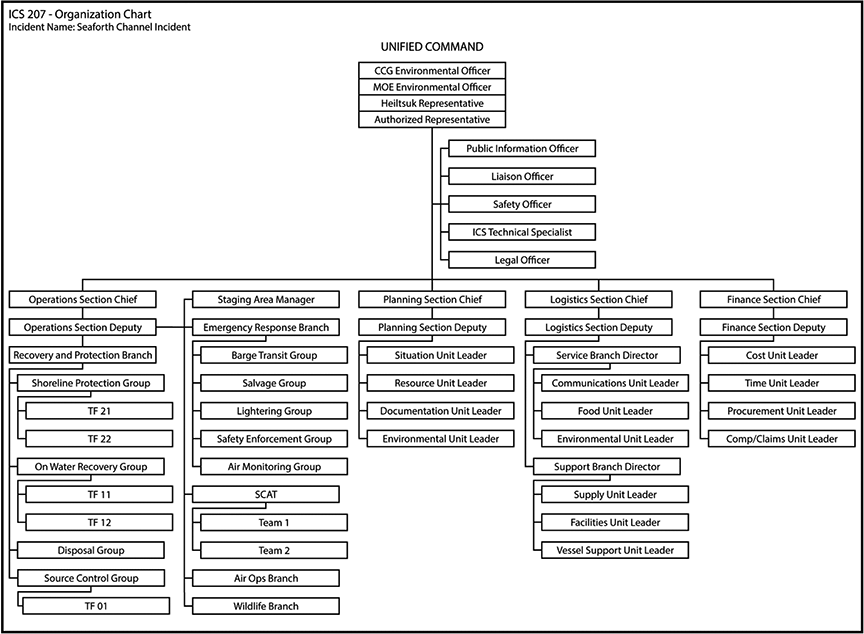
Appendix G – Glossary
- AAR
- after-action review
- AIS
- automatic identification system
- ATB
- articulated tug-barge
- BNWAS
- bridge navigational watch alarm system
- CCG
- Canadian Coast Guard
- CEMS
- Crew Endurance Management System
- COLREGs
- International Regulations for Preventing Collisions at Sea
- CSA 2001
- Canada Shipping Act, 2001
- DFO
- Fisheries and Oceans Canada
- ECCC
- Environment and Climate Change Canada
- FMP
- fatigue management plan
- GPS
- global positioning system
- GT
- gross tonnage
- HIRMD
- Heiltsuk Integrated Resource Management Department
- ICS
- incident command system
- JRCC
- Joint Rescue Coordination Centre
- MCTS
- Marine Communications and Traffic Services
- MPR
- Marine Personnel Regulations
- NEEC
- National Environmental Emergencies Centre
- nm
- nautical miles
- OOW
- officer of the watch
- PPA
- Pacific Pilotage Authority Canada
- REM
- rapid eye movement
- SAR
- search and rescue
- SCAT
- Shoreline Cleanup and Assessment Technique
- STCW code
- Seafarers' Training, Certification and Watchkeeping code
- TC
- Transport Canada
- TSB
- Transportation Safety Board of Canada
- UC
- unified command
- USCG
- United States Coast Guard
- VHF
- very high frequency
- WCMRC
- Western Canada Marine Response Corporation