Bottom contact
Tug Ocean Monarch
Princess Royal Channel, British Columbia
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 09 July 2017, at 0436 Pacific Daylight Time, the tug Ocean Monarch, with 3 crew members on board, made bottom contact while towing the loaded cement barge Evco No. 15 in the Princess Royal Channel, British Columbia. The tug’s hull and starboard propeller nozzle were damaged. No pollution was reported. There were no injuries. The tug continued on its voyage to Kitimat, British Columbia, using the port engine. The vessel then returned to the Fraser River and proceeded to a shipyard in Vancouver for repairs.
This report is also available in English.
1.0 Factual information
1.1 Particulars of the vessels
| Name of vessel | Ocean Monarch | Evco No. 15 |
|---|---|---|
| Official number | 815106 | 329605 |
| Port of registry | Vancouver, BC | New Westminster, BC |
| Flag | Canada | Canada |
| Type | Tug | Barge |
| Gross tonnage | 9.81* | 1538.98 |
| Length | 14.39 m | 57.91 m |
| Breadth | 5.94 m | 14.02 m |
| Depth | 2.47 m | 4.72 m |
| Built | 1991 | 1969 |
| Propulsion | Twin diesel engines (600 kW each) driving twin fixed‑pitch propellers | Non-propelled |
| Cargo | Not applicable | 1800 tons of cement |
| Crew | 3 | Uncrewed |
| Registered owners | Mercury Launch & Tug Ltd. | Lehigh Hanson Materials Ltd. |
* As recorded in the Transport Canada Register of Vessels.
1.2 Description of the Ocean Monarch
The Ocean Monarch is a twin-screw steel-hulled tug of closed constructionFootnote 1 (Figure 1). It has a plumb stemFootnote 2 and rounded transom stern.Footnote 3 The hull below the main deck is subdivided by 4 transverse watertight bulkheads that enclose 5 compartments (from forward): a void space, crew accommodations, engine room, fuel oil tanks, and lazarette (Appendix A).
The wheelhouse and a galley are located in the fore part of the tug. The wheelhouse is slightly raised up from the main deck, providing a clear view ahead and astern. The wheelhouse can be accessed via doors on the starboard and port sides as well as through a stairwell leading from the galley.

The wheelhouse is equipped with a magnetic compass, engine controls, an autopilot, radar, a global positioning system (GPS), an automatic identification system (AIS),Footnote 4 a very high frequency radiotelephone with digital selective calling (VHF/DSC), a chart plotter, and a foldable chart table with navigation charts. A second chart plotter on a laptop belonging to the mate interfaced with the tug's GPS, and both the master and mate used this chart plotter for navigation on the occurrence voyage. Both chart plotters have navigational alarms that can be configured to provide warnings if there are hazards near the vessel's track or if the vessel fails to make a planned course alteration.
A second conning position is located on top of the wheelhouse, where some lifesaving equipment, including an emergency position‑indicating radio beacon and a 4-person life raft, is stowed. This conning position is accessible via a fixed ladder on the aft side of the galley.
The galley is flush with the main deck and is accessed from the main deck by an aft-facing door. Inside the galley, there is a watertight hatch with a ladder leading down to the crew sleeping accommodations and the main lifesaving equipment storage area. There are 2 fuel oil tanks located forward, below the crew sleeping accommodations, and 2 fuel tanks located aft, between the engine room and the lazarette.
The engine room is accessed from the main deck level through a hatch with a coaming, located aft and starboard of the galley. Two diesel engines are located on the port and starboard sides of the engine room.
Since the tug came into operation in 1992, the engines had been replaced twice, once in 2003 and again in 2017. As well, the fuel oil tank configuration had been changed at some point since its initial installation; specifically, the rope store between the 2 aft fuel oil tanks had been partitioned and merged with the 2 existing fuel tanks.Footnote 5 The rope store access hatch was moved to the lazarette space on the port quarter.
The tug is fitted with a single-drum hydraulically driven towing winch and spooling gear.
1.3 History of the voyage
On 03 July 2017, at 1130,Footnote 6 a 3-person crew, consisting of a master, a mate, and a deckhand, boarded the Ocean Monarch for a 2-week work period. From 03 July to the early morning hours of 07 July, the crew performed 24-hour operations on the Fraser River in the Greater Vancouver area, during which the master performed or supervised most of the navigation and watch duties. During this period, the tug was stopped for 2 periods (7 hours 15 minutes on the morning of 04 July and 7 hours 45 minutes on the morning of 06 July), and the crew were signed off from work during these periods.
On 07 July, at 0200, the Ocean Monarch departed the Lehigh Construction Materials Terminal on the Fraser River to tow the barge Evco No. 15 to Kitimat via the Inside Passage (Appendix B). The time required for the voyage to Kitimat was estimated at approximately 2.5 days, with the tug in continuous operation. The master and mate took turns standing watch as the tug and tow proceeded continuously for the next 2 days. The deckhand tended to the barge, performed housekeeping duties, cooked, and kept a wheelhouse lookout watch, as directed by the master. As they passed mandatory calling-in points, the master and the mate reported the vessel's position via VHF/DSC radiotelephone to Marine Communications and Traffic Services (MCTS).
Sometime between 0336 and 0436 on 09 July, while the tug was transiting the Princess Royal Channel (Appendix B), the mate, who was on watch and seated alone in the wheelhouse, fell asleep. The master and the deckhand were asleep in the crew accommodation. At the time, the tug's course was being controlled by the autopilot, and the navigational alarms were disabled. There was no opposing traffic in the channel, and the lights for the navigation equipment were dimmed. The tug continued on a straight courseFootnote 7 in the channel, which has a gentle curve to the left. At 0436, the tug's stem and the starboard side of the hull made bottom contact with the starboard bank of the channel. The impact woke the mate as well as the master and the deckhand. As the master and the deckhand made their way up to the wheelhouse, the mate reversed the engines to back away from the shore and found that the starboard engine was inoperative.
Meanwhile, the Evco No. 15 continued to move forward, coming beside the tug and parallel with it, so that the tow wire was lying athwartships across the tug's deck as the barge slowed to a stop. The deckhand hauled in the tow wire, and the master used the port engine to manoeuvre the tug away from the shore and regain control of the barge.
Once the master had regained control of the barge, he instructed the mate and the deckhand to check the tug for damage. He also called the company and notified the owner of the situation. The mate and deckhand used a camera to try to see if there was any external damage under the tug, but the visibility was too poor to see anything. In the engine room, they found a steady drip of fuel oil in the bulkhead between the starboard forward fuel oil tank and the engine room. Over the next 6 hours, the mate and the deckhand drained fuel out of the starboard fuel oil tank into buckets and transferred it to the aft fuel oil tanks.
After assessing the damage, the master resumed the voyage to Kitimat at 0453, reporting to MCTS at subsequent calling-in points. At 1558 on 09 July, the tug and barge arrived in Kitimat.
The same day, at 1624, the Ocean Monarch began a return journey on 1 main engine to the Fraser River with an empty barge in tow. En route, it took a second empty barge in tow, arriving at the Fraser River on 13 July. On 14 July, the Ocean Monarch arrived at a Vancouver shipyard for repairs. No pollution was reported. There were no injuries.
1.4 Damage to the vessel
On 11 August, Transportation Safety Board of Canada (TSB) investigators were deployed to the shipyard.Footnote 8 The investigation found that the stem and the starboard side of the tug's steel hull had numerous scrapes, fractures, deformations, and indentations below the waterline. The starboard propeller and rotating nozzle had major damage and required replacement. The starboard forward fuel oil bulkhead had an internal crack.
1.5 Environmental conditions
In the early hours of 09 July, the weather was overcast with light rain, and the sea conditions were calm. Sunrise was at 0524; thus, at the time of the occurrence (0436), it was twilight.
The Princess Royal Channel is a narrow gorge less than 1 nautical mile (nm) wide. Where the tug contacted bottom, the channel was 0.7 nm wide and more than 100 m deep at its deepest point. At the time of the occurrence, an ebb tidal stream was flowing through the channel. The tidal stream in the Princess Royal Channel can reach speeds of up to 2.5 knots.Footnote 9
1.6 Personnel certification and experience
The master held a certificate of Master, Limited for a Vessel of less than 60 Gross Tonnage operating on the west coast of British Columbia. The master also held a Restricted Operator's Certificate – Marine Commercial (ROC-MC), and certificates for Marine Basic First Aid and Marine Emergency Duties (MED) A1, B1, B2, C, and D. The master began working for the company that operates the Ocean Monarch as a mate in September 2002 and as a master in September 2003. Before joining the company, he had worked as a deckhand and as a master on various tugs on the west coast since 1980.
The mate held a certificate of Chief Mate 150 Gross Tonnage, Domestic, engaged on a limited contiguous waters voyage. He also held certificates for ROC-MC, Marine Advanced First Aid, MED A1, A2, A3, D and International Convention on Standards of Training, Certification and Watchkeeping for Seafarers (STCW) Basic Safety. He had completed an electronic chart display and information systems course and a Simulated Electronic Navigation – Limited course. The mate began working for the company that operates the Ocean Monarch as a deckhand in 2015 and as a mate in May 2017. The occurrence voyage was his second voyage in charge of a navigation watch through the Inside Passage. Before joining the company, he had worked as a deckhand on various tugs on the west coast since 2008.
The deckhand began working for the company that operates the Ocean Monarch in 2012 and held certificates for Marine Basic First Aid and MED A1.
1.7 Vessel certification and inspection
The Ocean Monarch held a certificate of registry issued on 17 March 1992. Because the Ocean Monarch was registered as a tug of not more than 15 gross tonnage (GT),Footnote 10 the Ocean Monarch was not required to undergo inspections.Footnote 11
1.8 Regulatory oversight
Transport Canada (TC) is responsible for overseeing Canadian-flagged vessels to ensure that they are operating in accordance with the Canada Shipping Act, 2001 (CSA 2001). Under this legislation, an authorized representative (AR) is the individual responsible for acting with respect to all matters related to a vessel that are not otherwise assigned to any other person. For the Ocean Monarch, the AR is the owner.
Under the CSA 2001,Footnote 12 a vessel's AR is responsible for
- ensuring that the vessel and its machinery and equipment meet the requirements of regulations set out by the CSA 2001;
- developing procedures for the safe operation of the vessel and for dealing with emergencies; and
- ensuring that the crew receive safety training.
For regulatory oversight of tugs, TC uses the measurement of GT to draw a distinction in inspection, certification, and approval requirements between tugs of greater than 15 GT and those of not more than 15 GT. TC has developed 2 guidance documents to help with the safe operation of tugs. The Guidelines for the Construction, Inspection, Certification, and Operation of Tugs < 24 Metres in Length provide information on the requirements for tugs.Footnote 13 The Small Commercial Vessel Safety Guide provides information on the responsibilities of the AR and the safety requirements that apply to workboats, including tugs, of not more than 15 GT.Footnote 14
The differences in vessel inspection requirements for the 2 categories of tugs are summarized in the following 2 subsections.
1.8.1 Tugs of greater than 15 gross tonnage
TC inspects tugs of between 15 GT and 150 GT upon initial construction or registration and, subsequently, every 4 years. During the quadrennial inspection, a TC marine safety inspector is responsible for inspecting the vessel externally and internally and checking the vessel's structures and equipment (both routine and emergency), as well as on-board records and certificates, among other things.Footnote 15 The inspector is also responsible for checking for any changes or modifications to the vessel and changes in the vessel's use since the last inspection. Once identified deficiencies have been resolved to TC's satisfaction, TC issues an inspection certificate for the vessel that indicates the safe manning, limitations for voyages, weather conditions, and/or type of activity (e.g., towing) for which the vessel is used.
1.8.2 Tugs of not more than 15 gross tonnage
Tugs of not more than 15 GT are not certified under the current Hull Construction Regulations nor inspected by TC under the Hull Inspection Regulations. Under the CSA 2001, the AR is responsible for ensuring the vessel complies with all applicable regulations and is suitable for its intended operation and use. The AR must also keep appropriate records (e.g., a logbook, hours of work and rest) and make them available upon request to any person or organization authorized under the CSA 2001 to carry out inspections.Footnote 16 TC has the authority to conduct random monitoring inspections to verify compliance. There are no records to indicate random monitoring inspections; however, TC conducted a concentrated inspection campaign (an inspection campaign that targeted specific areas of safety concern on Canadian vessels) between January and March of 2017. As part of the campaign, TC inspected 30 tugs of not more than 15 GT and 30 tugs of greater than 15 GT. Based on an analysis of results from the campaign, TC concluded that tugs of not more than 15 GT had significantly more instances of regulatory non-compliance than tugs of greater than 15 GT.Footnote 17
1.9 Gross tonnage measurement for tugs
All vessels are required to undergo a GT measurement when they are registered. For a vessel of the Ocean Monarch's size and type, the GT is measured by an approved tonnage measurer in accordance with the CSA 2001,Footnote 18 and the GT is entered into the TC Canadian Register of Vessels. The Ocean Monarch's GT in the Register is 9.81, its initial measurement when it was first registered on 17 March 1992.
Following the occurrence, the TSB contracted an independent tonnage measurer to calculate the GT of the Ocean Monarch according to TC's current standard, as set out in the Standard for the Tonnage Measurement of Vessels.Footnote 19 This calculation found that the Ocean Monarch's tonnage measurement lengthFootnote 20 was 15.35 m, and the resulting GT was 63.6.
The significant difference between the Ocean Monarch's actual and registered GT arises from an issue that dates back a number of decades, when some tugs were designed and built with artificially raised engine-room floors to reduce the measured depth used in the initial GT calculation, and thereby reduce their overall measurement to less than 15 GT.Footnote 21 In some instances, the floors were just partitions and did not contribute to the vessel's structural integrity; they were fitted only for GT measurement purposes and were removed afterwards. A GT of less than 15 enabled the tugs to operate without undergoing inspections, being issued a safe manning document,Footnote 22 or being subject to voyage limitations or limitations on the type of activity for which the tug is used.
In 1991, owners of tugs with accurately registered GT measurements, the Canadian Merchant Service Guild,Footnote 23 and some employees on tugs with inaccurately registered GT measurements brought this issue to the attention of TC (which was responsible for the Canadian Coast Guard at the time). As an immediate corrective action to stop the use of artificially raised floors, TC informed tonnage measurers on 30 December 1991 that from 01 January 1992 onwards, TC would limit the height of open floors. To understand the magnitude of the issue, TC conducted a survey and identified at least 25 tugs registered as of less than 15 GT that were suspected to be of greater than 15 GT. After deliberations with industry, TC grandfathered these tugs. The Ocean Monarch was constructed around the time this decision came into force. Although TC did not grandfather the Ocean Monarch, following a dispute between TC and the owner, TC did allow the tug to be listed with a GT of 9.81, even though its actual GT was calculated as 31.18.
In 2003, when the Ocean Monarch underwent an engine replacement, the tug's high floors were removed, which changed the measurable depth of the engine room for the purposes of GT calculation. Consequently, TC requested that the owner recalculate the tug's GT. The owner contacted a naval architect but, after consultation with TC, it was agreed that the tug would remain listed under its original recorded GT.
Following this occurrence, the TSB obtained a sampling of tonnage measurement data for tugs measuring 12 to 15 m long and registered as of not more than 15 GT currently operating in BC. Using this data, the TSB conducted an analysis of 51 tugs' depth dimensions to determine whether they were realistic, given each tug's overall registered GT. The TSB assessed that 17 tugs did not have accurately registered GT measurements because of unrealistic depth dimensions (Appendix C). At the time of the occurrence, the Ocean Monarch's GT was estimated as 63.6.Footnote 24
1.10 Minimum safe manning
The CSA 2001 directs the master not to operate a vessel unless it is manned with sufficient and competent crew for the vessel's safe operation on its intended voyage and is so manned throughout the voyage.Footnote 25
For tugs of greater than 15 GT, TC provides a document with information on minimum safe manning for the vessel. The document is compiled on the basis of TC's assessment of the vessel's requirements during normal operations and emergency situations. It provides guidance on the number of crew members required to safely operate the vessel, their levels of certification, the areas where the vessel is permitted to trade, and a description of the voyages that the vessel is permitted to undertake. This document is valid for 5 years. Before it expires, the AR must contact TC to renew the document. A TC inspector then visits the vessel, verifies that its operating conditions have not changed, and renews the certificate.
As a tug registered as of not more than 15 GT, the Ocean Monarch was not required to have a safe manning document. Nevertheless, it was required to be sufficiently manned to comply with the requirements set out in the Marine Personnel Regulations (MPR). Accordingly, the MPR requires a minimum of 2 crew members for deck watchkeeping duties, one of whom holds a certificate of competency to perform such duties.
The MPR do include a provision that, during the daytime and in good visibility, the tug could proceed with only 1 crew member on deck watchkeeping duties, but only after an assessment of all relevant navigation factors (e.g., weather conditions, confined waters, other vessel traffic, dangers to navigation).Footnote 26 However, during the night, the MPR require 2 crew members for watchkeeping duties on the bridge.
Additionally, the Seafarers' Training, Certification, and Watchkeeping Code (the STCW Code) states that “the master of every ship is bound to ensure that watchkeeping arrangements are adequate for maintaining a safe navigational watch”Footnote 27 and elaborates that “a proper lookout shall be maintained at all times to serve the purpose of… fully appraising the situation and the risk of collision, stranding, and other dangers to navigation”.Footnote 28 It further states that “the lookout must be able to give full attention to the keeping of a proper lookout and no other duties shall be undertaken or assigned that could interfere with that task”;Footnote 29 and that “the duties of the lookout and the helmsperson are separate.”Footnote 30
Further, the STCW Code states that, in evaluating the manning required for a navigational watch, the master must take the following factors into consideration:
- Visibility, weather, and sea conditions
- Traffic density and other activities in the area where the vessel is navigating
- Additional workload caused by the nature of the vessel's operations and anticipated manoeuvres
- The fitness for duty of any crew members on call who are assigned as members of watch
- The professional competence of the vessel's officers and crew
- The experience of each officer of the navigational watch, and the familiarity of that officer with the vessel's equipment, procedures, and manoeuvring capability
- Any activities taking place on board the vessel at a particular time, including radio communication activities, and the availability of assistance to be summoned immediately to the bridge when necessaryFootnote 31
The Ocean Monarch was compliant with the MPR watchkeeping certification requirements because both the master and mate held the necessary certificates. However, in the hours leading up to the occurrence, there was only 1 watchkeeper responsible for the duties of lookout, helmsperson, and maintaining a navigation watch while the vessel was proceeding at night. As a result, the watchkeeping crewing was not compliant with the MPR, nor did it conform to the STCW Code.
1.11 Fatigue
Fatigue is recognized as being pervasive throughout modern society, and this has important implications for the highly safety-sensitive transportation industry. Disruptions to sleep or sleeping patterns in personnel occupying safety-critical positions can cause performance decrements that increase the risk of incidents and accidents. Fatigue has been shown to slow reaction time, increase risk taking, and reduce an individual's ability to solve complex problems. It more generally affects attention, vigilance, and general cognitive functioning. Fatigue also carries a risk of transportation staff falling asleep during safety-critical operations.
For sleep to be restorative, it should occur at night for a period of at least 7, and up to 9, continuous hoursFootnote 32,Footnote 33 so that all stages of sleepFootnote 34 occur during each nightly sleep period. For a normal nighttime sleeper, deep sleep occurs early in the sleep period, while rapid eye movement (REM) sleep occurs in the second half.Footnote 35 Deep sleep may serve a physiologically restorative function,Footnote 36,Footnote 37 whereas REM sleep is more likely to restore cognitive processes.
Fatigue may result from one or more of 6 risk factors: acute or chronic sleep disruptions, continuous wakefulness, circadian rhythm disruptions, sleep disorders or other medical and psychological conditions, and/or illnesses or drugs that affect sleep or sleepiness. Other factors that may influence a person's ability to obtain restorative sleep include individual factors (e.g., whether peak alertness is in the morning or evening, and/or an ability to nap), nature of the work (e.g., whether it is monotonous), and schedule type (e.g., split shifts).
1.11.1 Acute sleep disruptions
Acute sleep disruptions are reductions in the quantity or quality of sleep within the previous 3 days. Reductions of at least 30 minutes (quantity) or curtailed deep sleep or REM sleep (quality) are normally considered notable.
1.11.2 Chronic sleep disruptions
Any sleep quantity disruptions for periods longer than 3 consecutive days are considered chronic sleep disruptions. Comparing the amount of sleep obtained to that required for a given period of wakefulness can provide an estimate of a person's “sleep debt.” A sleep debt of more than 2 hours over a 7-day period may indicate chronic fatigue.
Chronic disruptions may be less notable than acute disruptions. Although the disruptions may be small, they can change “sleep architecture;” for example, reducing the amount of deep sleep or REM sleep without reducing total sleep time, resulting in fatigue and its associated impairments, such as slowed reaction times.
1.11.3 Continuous wakefulness
More than 22 hours of continuous wakefulness is typically considered the period after which fatigue causes almost all aspects of human performance to decline. Most individuals begin to experience uncontrollable brief episodes of sleep lasting 3 to 4 seconds, commonly known as “microsleeps,” and “state instability” (because wakefulness cannot be maintained) after this period of wakefulness.Footnote 38
1.11.4 Circadian rhythm
The time of day has a strong effect on an individual's alertness and performance owing to changes in body physiology that are synchronized to a circadian (daily) rhythm. The body is physiologically ready for sleep at night, when the best quality and longest duration of sleep is obtained.Footnote 39 Because of the circadian rhythm, overall performance and cognitive functioning are at their worst during the nighttime period between 0300 and 0500 (circadian trough). This pattern can occur in the absence of fatigue;Footnote 40 that is, overall performance may be low during the circadian trough even if a person is not fatigued.
If individuals' work schedules allow sleep only in multiple, non-consecutive segments, it can be challenging to obtain sufficient quantity and quality of restorative rest. Furthermore, if a rest period is during one's normal active daytime period (outside normal periods of circadian low), any sleep during that time will be less restorative than sleep during hours of darkness or during a circadian trough that occurs in the afternoon, when human physiology is naturally conducive to sleep.Footnote 41,Footnote 42,Footnote 43,Footnote 44 More generally, if individuals can sleep only in multiple shorter rest periods, they may be prevented from obtaining the required amount of sleep in the time available because of meals, personal chores, crew shift changes, and unscheduled interruptions.
Recent research has demonstrated that mariners' compliance with regulatory requirements for work/rest scheduling is generally poor.Footnote 45,Footnote 46 In addition, when shift schedules change intermittently—for instance, when a vessel is in port versus when it is at sea—there is an adjustment period during which crew members are more likely to be fatigued until they adapt to the new schedule.
1.11.5 Disorders, conditions, and medications
Sleep and/or quality of sleep may also be affected by certain disorders, conditions, and/or medications. These may include sleep disorders, physical injuries that prevent sleep, or medications that either make an individual drowsy or keep an individual awake.
1.11.6 Task monotony
Partial sleep deprivation may have less effect on individuals performing tasks involving a higher cognitive load, such as logical reasoning, problem solving, and decision making, than on individuals performing monotonous tasks.Footnote 47 This may be due, in part, to individuals' compensatory efforts to perform normally on complex, interesting, variable, or short tasks. In other words, people may become more engaged in tasks with a higher cognitive load than those that are monotonous, and exert more effort to perform them normally, thereby increasing physiological arousal levels and temporarily counteracting fatigue-related performance impairments. Conversely, task monotony has been shown to decrease alertness and increase drowsiness, which may lead to fatigue-impaired performance.Footnote 48
1.12 Regulations relating to fatigue
Some of the international, national, and local regulations in place to ensure the safe operation of vessels specify measures to reduce the probability of fatigue and/or to mitigate the effects of such fatigue.
As a Canadian vessel operating in both domestic and foreign waters, the Ocean Monarch was subject to different hours of work and hours of rest requirements, depending on the area of voyage. On the occurrence voyage, the Ocean Monarch was subject to the regulations governing hours of work and rest in Canadian waters.
1.12.1 Hours of work and rest—Canadian waters
Section 320 of the MPR species the hours of rest for masters and crew members of Canadian vessels operating in Canadian Near Coastal Voyage, Class 2 waters as follows:
- the master and every crew member [must] have
- at least 6 consecutive hours of rest in every 24-hour period, and
- at least 16 hours of rest in every 48-hour period; and
- not more than 18 hours but not less than 6 hours elapse between the end of a rest period and the beginning of the next rest period.Footnote 49
Additionally, the MPR require the master of a vessel to keep a record of every crew member's daily hours of work or of rest.Footnote 50
With respect to hours of work, when operating as a domestic vessel in Canadian Near Coastal Voyage, Class 2 waters, the Ocean Monarch was also subject to the West Coast Shipping Employees Hours of Work Regulations. These regulations permit an employee to work a maximum of 84 hours a week, plus 18 hours of overtime, over 7 consecutive days.Footnote 51
The enabling act for the West Coast Shipping Employees Hours of Work Regulations is the Canada Labour Code, Part III.Footnote 52 Section 172(2) the Canada Labour Code, Part III, regarding maximum hours of work, also applied to the Ocean Monarch crew. This section states that an employer may establish, modify, or cancel a work schedule under which the hours exceed the maximum set out in the West Coast Shipping Employees Hours of Work Regulations if the average hours of work for a period of 2 or more weeks does not exceed 48 hours a week.Footnote 53
In response to a complaint or when conducting an inspection, Employment and Social Development Canada (ESDC) has the authority to inspect, examine, and take extracts from the employee records related to hours of work or conditions of employment and wages, among other things. ESDC had never inspected the Ocean Monarch for compliance with the Canada Labour Code, Part III.
The Canada Labour Code, Part III requires the employer to make and keep records related to employees' hours of work, among other things,Footnote 54 for a period of 36 months, and make the records available for examination by an inspector.Footnote 55
1.12.2 Hours of work and rest—foreign waters
The following MPR requirements with respect to work and rest applied when the Ocean Monarch was operating in foreign Near Coastal Voyage, Class 2 waters:
321(1) The master […] shall ensure that the master and every crew member
- do not work more than 14 hours in any 24-hour period or more than 72 hours in any 7-day period; or
- have at least 10 hours of rest in every 24-hour period and 77 hours of rest in every 7-day period.
(2) The master shall ensure that
- the hours of rest are divided into no more than 2 periods, one of which is at least 6 hours in length; and
- the interval between 2 consecutive rest periods does not exceed 14 hours.Footnote 56
1.13 Fatigue risk-management strategies
Fatigue risk management requires a proactive approach that includes compliance with regulations—which can only mandate hours of rest, not hours of sleep—as well as mariner education and awareness. Only mariners themselves can control their sleep time. With training and education, both companies and mariners can identify and take preventive measures that go beyond the regulations.
Preventing fatigue in the workplace is a shared responsibility between a company and its employees. A company may contribute to preventing fatigue through various measures, including
- educating employees at all levels about the causes and mitigation of fatigue, including the need to get regular rest and the implications of being fatigued (both for themselves and others);
- defining appropriate policies and procedures for fatigue management, including detailed reporting requirements for hours of work and rest/sleep;
- ensuring a working environment that minimizes fatigue as much as is practicable and takes into account increased workload as a result of small crew numbers;
- creating an open-communication environment in which crew are encouraged to inform supervisors if they are fatigued or if they are experiencing factors that affect their sleep (e.g., stress, boredom, medication use, sleep-related disorders, relationship problems); and
- striving for continual improvement in reducing the risk of fatigue.
Masters may prevent fatigue using various means, including
- scheduling work and rest periods to minimize fatigue risk factors as much as possible (e.g., scheduling higher-risk tasks during daytime hours, having 2 crew on nighttime shifts, encouraging crew to sleep during rest periods, providing compensatory rest periods when sleep is interrupted);
- posting the crew's work schedule and examining the crew's hours of work and rest to determine whether they are sufficiently rested; and
- encouraging the crew to report when they feel fatigued and assessing crew members for signs of fatigue.
Crew may prevent fatigue by taking measures, including
- recording hours of work and rest/sleep;
- taking steps to ensure they are well rested for work by applying their knowledge of the prevention and effects of fatigue;
- making effective use of fatigue countermeasures;
- recognizing the signs of fatigue in themselves and co-workers; and
- taking action to ensure that fatigue caused by work or non-work activities does not lead to performance issues.
In 2003, in response to TSB recommendations M96-17, M96-18, M99-03, and M99-04, TC finalized a training program in fatigue management and awareness for marine pilots, which was integrated within the broader training programs for apprentice pilots in Canada. The program includes a Fatigue Management GuideFootnote 57 that presents information on sleep fundamentals, issues regarding the biological clock (circadian rhythms), the effects of irregular work schedules on fatigue, and various coping strategies to minimize the likelihood of experiencing fatigue while at work. It also draws on situations that marine pilots can expect to encounter in their day-to-day work and identifies the signs of fatigue that pilots can use to self-diagnose, such as forgetting to communicate with crew, forgetting to monitor the vessel's position regularly, or missing a point of reference.
The guide notes other factors that can exacerbate fatigue, including environmental conditions such as darkness, constant noise, and warm temperatures. The guide also notes that performing routine tasks under a low workload makes it especially difficult to fend off sleepiness, particularly if one is sleep-deprived. The guide presents coping strategies that can temporarily minimize the effects of fatigue when it occurs. These include
- consuming caffeine,
- turning on a bright light,
- exercising,
- strategic napping,
- exposing oneself to intermittent loud noise,
- getting fresh (cool) air, and
- receiving mental stimulation from conversation.Footnote 58
TC has also provided the rail industry with Fatigue Management Plans: Requirements and Assessment Guidelines, to help rail companies develop fatigue-management plans (FMPs). Rail FMPs must be filed with TC in order to meet the industry's Work/Rest Rules for Railway Operating Employees.Footnote 59, Footnote 60 In 2015, the Railway Safety Management System Regulations came into force, requiring that safety management systems include a “process with respect to scheduling” for the work of certain employeesFootnote 61 and that the process apply the principles of fatigue science.
The current Canadian regulatory regime for the aviation industry does not reflect scientific principles and knowledge of fatigue, either regarding working at different times of the day, ensuring sleep hygiene and quality, or mitigating the effects of cumulative fatigue. Recognizing this gap, TC Civil Aviation has amended the Canadian Aviation Regulations to change flight crew hours of work and rest periods and is proposing that air transport services with an approved fatigue risk-management system could be exempted from prescriptive regulations.Footnote 62
There is currently no requirement for Canadian marine companies to develop or implement FMPs or to provide fatigue awareness training. However, the International Maritime Organization (IMO) sets out some guidance for an effective FMP, which includes the following elements:
- Objective measurement of the causes and effects of fatigue, and
- Comprehensive programs that comprise
- training and education on fatigue and shiftwork for all watchkeepers;
- planning tools such as fatigue modelling or rosters (watchkeeping systems) and work arrangements; and
- impairment testing programs and audits of the results of previous initiatives.Footnote 63
TC has a representative on the IMO subcommittee working group on human element issues;Footnote 64 the working group is currently developing recommendations for the revision of the IMO Guidance on Fatigue Mitigation and Management. The working group met in February 2017 and is scheduled to meet again in 2018. TC considers human element issues to be significant and continues to participate, with the objectives of
- developing various types of tools (e.g., pamphlets, video training modules, seminars, and workshops) for disseminating the information provided in the IMO guidance; and
- incorporating the guidance when determining minimum safe manning levels for vessels and when developing regulations to mitigate the potential impact of fatigue.
The company that owns the Ocean Monarch did not have an FMP at the time of the occurrence, nor was an FMP required by regulation. The master, mate, and deckhand had not undergone training on fatigue awareness, fatigue management, or alertness strategies, nor were they required to do so by regulation.
1.14 Company management of fatigue
The company expected the master on the Ocean Monarch to manage hours of work and rest while carrying out 24-hour river and coastal operations with a 3-person crew. As well, the tug carried out voyages in foreign waters, where different hours of work and rest are permitted, and the master was responsible for adjusting the crew's schedule accordingly. It was assumed that crew members would report any fatigue. The company did not monitor the master's scheduling, only the total number of hours that the crew worked, for compensation purposes.
1.14.1 Hours of work and rest
The investigation found no indication that the crew had any medical or sleep issues that may have affected fatigue.
The crew's shift pattern was ad hoc, and their hours of work were subject to change based on operational requirements. The crew's shift schedule was not documented, although their total hours worked were, for compensation purposes. It was therefore not possible to ascertain detailed hours of work and rest for the crew in the days preceding the occurrence. However, based on work tasks, it was possible to ascertain when the crew had opportunities for rest.
All 3 crew members worked the first 2 weeks of June, followed by a 2-week rest period (18 June to 03 July).
Between 03 and 06 July, the crew returned from their rest period and performed river operations on a 24-hour schedule for the next 2.5 days, except for 2 periods when they were signed off from work. Except for these 2 periods, the work was mainly continuous, with the crew looking out for deadheads or shortening up the tow as required, and the master carrying out most of the navigating and watch duties. Over this time, the crew members did not take the opportunity to sleep in the accommodation bunks but did take short naps on the settee in the galley during transit from one location in the river to another. The engine exhausts are next to the galley, which make it a noisy area.
On 07 July, the crew switched from river operations to coastal operations, departing for Kitimat at 0200. MCTS records on call-in and course change indicate periods when either the master or mate were active (Table 2). The hours of work for the deckhand while on coastal operations could not be determined, although the deckhand was primarily working during the daytime and resting at night.
| Date | Crew member | 0000 to 0300 |
0300 to 0600 |
0600 to 0900 |
0900 to 1200 |
1200 to 1500 |
1500 to 1800 |
1800 to 2100 |
2100 to 0000 |
|---|---|---|---|---|---|---|---|---|---|
| 07 July | Master | 0200 (depart) | 0329 (call) | No activity recorded | No activity recorded | No activity recorded | 1628 (calls start) | On duty | 2216 (calls end) |
| 07 July | Mate | 0200 (depart) | On duty | 0808 (call) | Probably on duty | 1259 (call) | No activity recorded | No activity recorded | No activity recorded |
| 08 July | Master | No activity recorded | No activity recorded | No activity recorded | 1140 (call) | On duty | 1649 (call) | 1853 (call) | 2100 (sleeps) |
| 08 July | Mate | 0108 (calls start) | On duty | On duty | 0914 (calls stop) | No activity recorded | No activity recorded | 2037 (calls start) | On duty |
| 09 July | Master | Asleep | Vessel grounded at 0436 | - | - | - | - | - | - |
| 09 July | Mate | On duty, last call made 0149 | 0336 (course change) 0436 (grounding) | - | - | - | - | - | - |
These records suggest that the mate and the master took turns performing navigation and watchkeeping duties and that the mate took the night watch. The mate seemed to work from around 0100 to 1300, except just before the day of the occurrence, when the mate's calls started earlier, at 2037.
At the time of the grounding, the mate had been on duty for at least 8 hours.
1.15 Industry context
In the towing industry on the west coast of Canada, tugs are involved in berthing and unberthing operations for large vessels, coastal towing, log booming, and river towing and yarding operations. Each of these operations is unique and carries its own attendant risks. The nature of risk varies depending on the location and type of operations.
The type of work that a tug can undertake is largely determined by its size, engine power, and manoeuvring characteristics. Contracts for towing are normally assigned on a short- or long‑term basis through a tendering process. The industry is competitive and dynamic, and last-minute assignments or changes to assignments are commonplace. In addition to fuel, crewing is a major cost for operating a tug. While fuel cost and consumption are largely out of the control of the operator, crew costs, working hours, shift patterns are within their control.
It is difficult to obtain reliable data on the number of tugs operating on the west coast of Canada because the TC Register of Vessels contains some outdated information.Footnote 65 As of 14 March 2018, the register indicates that there are 1260 tugs operating in BC, of which approximately 1034 are not more than 15 GT.Footnote 66
1.16 Company operations
The company that owns and operates the Ocean Monarch has 6 tugs registered as of not more than 15 GT and a workboat of 17 GT. It operates 15 barges, ranging from 200 to 3000 GT. The company's tugs and barges operate in compulsory pilotage watersFootnote 67 off the west coast of Canada and in the northwestern states of the U.S. The company office is located in Vancouver, BC, where the owner/AR and 3 office staff work. The owner coordinates the work assignments and dispatches the tugs and barges by telephone. The company is a family business; the owner is actively involved in all aspects of the company operations, has a background in marine operations, and has experience operating tugs.
The tugs carry out operations involving the company's own barges as well as freight, bulk, roll-on/roll-off, and ramp barges owned by other companies. Operations range from providing short- and long-haul movement of barges within the Fraser River, assisting barges or log booms to transit railway bridges, shuttling barges from tie-ups to docks, and open-water towing within the Near Coastal 2 waters of BC.Footnote 68
The tugs are typically operated 24 hours per day, 7 days per week, with a 3-person crew on a loose 2-week shift schedule. This crewing method minimizes the need for crew changes and allows the tugs to work continuously. The company also uses the same tugs for both coastal towing and river towing assignments, which allows it to accept a variety of assignments from both customers and competitors.
The company compensates its masters to work up to 17 hours per day and its crew to work up to 16 hours per day.
The management of safety and operations on the tugs is left to the individual masters; the AR did not provide safe operating procedures, as required by the CSA 2001,Footnote 69 nor were fire and boat drillsFootnote 70 conducted on the Ocean Monarch.
1.17 Safety culture
Safety culture refers to the way that safety is perceived, valued, prioritized, and managed throughout all levels of a company. It encompasses a company's shared values (what is important) and beliefs (how things work), as well as how these interact with a company's structures and control systems to produce behavioural norms (“the way we do things around here”).Footnote 71
One of the most important factors affecting safety culture is the company management's degree of commitment to safety. It is vital that senior management or owner/operators actively demonstrate their commitment by providing leadership and resources to manage safety. In a smaller company with a leaner management structure, such as the one that operated the Ocean Monarch, management tends to have a large influence on the safety culture and sets the standard for its employees to follow.
To instill a strong safety culture, management should
- develop and actively share a safety vision;
- establish safety as a priority and actively incorporate it into all aspects of an operation;
- set out safety-related objectives and policies that the organization can use to conduct and control operations;
- encourage staff to participate in improving safety;
- support employees in ensuring safe operations and reporting of safety-related issues;
- set an example for others to follow; and
- provide the necessary time and money to implement safety-related actions.Footnote 72
An organization with a strong safety culture promotes a philosophy of continual improvement and communicates this philosophy to employees and stakeholders—both explicitly, through such things as values and mission statements, and implicitly, through day-to-day actions. This philosophy is formalized through policies that clearly communicate the importance of safety and recognize the contribution of each person in an organization to improving safety. Operating policies and procedures are also in keeping with the organization's safety philosophy.Footnote 73
A safety management system (SMS) is one method by which a company can strengthen its safety culture.
1.17.1 Safety management
The principal objectives of an SMS on board a vessel are to ensure safety at sea, prevent human injury or loss of life, and avoid damage to property and the environment. Effective safety management involves individuals at all levels of an organization and requires a systematic approach to identifying and mitigating operational risks.
Some elements of an effective SMS are
- clearly defined responsibilities, obligations, and authorities for the company and its masters;
- operating procedures for the vessel and the use of checklists;
- documentation and record-keeping procedures;
- procedures for identifying hazards and managing risks;
- procedures to prepare for and respond to emergency situations;
- drills, training, and familiarization for vessel crews; and
- a system for self-assessment and improvement.
At the time of the occurrence, the company did not have documented procedures for marine activities such as towing and yarding of barges, for managing hours of work and rest, for hiring and training employees, for operating vessels safely, or for dealing with emergencies.
In 2010, the Canadian Merchant Service Guild, the Council of Marine Carriers,Footnote 74 and TC started formal consultations on a regulatory proposal to introduce safety management regulations for Canadian non-convention vessels, including tugs not more than 15 GT. However, industry expressed concerns, primarily with regard to costs and feasibility, that the new regulations would be too onerous to implement for small companies that operate small vessels. In response to stakeholders' concerns, TC amended its regulatory proposal in 2012 to include only vessels greater than 24 m in length or carrying more than 50 passengers.
At the national Canadian Marine Advisory Council meeting in November 2014, TC updated the industry on the proposed safety management regulations.
These proposed changes would not apply to tugs the size of the Ocean Monarch.
1.18 Coastal pilotage waivers
The Pacific Pilotage Authority (PPA), a Crown corporation, was created in 1972 under the Pilotage Act. The PPA has a mandate to establish, operate, maintain, and administer safe and efficient pilotage services, as well as to operate on a financially self-sufficient basis.Footnote 75 Among other things, the PPA has the authority to
- establish compulsory pilotage areas;
- determine which vessels are subject to compulsory pilotage; and
- prescribe the circumstances under which compulsory pilotage may be waived.Footnote 76
The PPA has implemented a process through which some vessels, mainly tugs and barges,Footnote 77 may obtain pilotage waivers, making these vessels exempt from compulsory pilotage in designated pilotage areas (Appendix D) if the operators meet certain requirements.
Under these requirements, all persons in charge of a deck watch must
- hold certificates of competency of the proper class and category of voyage for the vessel that are required by Part 2 of the Marine Personnel Regulations;
- have served either 150 days of service in the preceding 18 months or 365 days of service in the preceding 60 months, of which 60 days must have been served in the preceding 24 months, at sea as a person in charge of the deck watch on 1 or more ships on voyages in the region or engaged in the coastal trade; and
- have served as persons in charge of the deck watch in the compulsory pilotage area for which the waiver is sought on 1 or more occasions during the preceding 24 months.Footnote 78
Before issuing a waiver, the PPA requests that the AR provide a signed statement of compliance for each watchkeeper's sea time. The PPA does not verify the information supplied by ARs.
An occurrence on 13 October 2016 involving the tug Nathan E. StewartFootnote 79 prompted the PPA to take a number of immediate actions concerning the waiver system. First, the PPA began monitoring vessel traffic entering the pilotage area using AIS, which identified 17 companies operating in compulsory pilotage waters without a pilot or the required PPA pilotage waiver.
The PPA also amended its waiver system to require all waivered vessels to have 2 people on the bridge at all times while operating in confined waters, and that 1 of those people must be the waiver holder. The amendments also indicated that vessels carrying petroleum products as cargo but not delivering fuel to local communities are not allowed in pre-defined no-go areas.Footnote 80 These amendments were explained in a letter sent to companies that held a pilotage waiver.
These interim measures were implemented while the PPA undertook a risk assessment to assess the impact of these measures on safety, to identify any inherent safety gaps, and to make recommendations for further improvements to the safety of vessels operating under pilotage waivers on British Columbia's coast.Footnote 81
On 23 May 2017, the PPA released the results of its risk assessment and, on 15 September 2017, released a final version of the “Standard of Care” implementation guidelines, which state that
[t]he provision of the waiver must be made with reasonable confidence that an acceptable “Standard of Care” is being maintained by the waivered company, vessel, and crew, such that the risk to life, property and the environment is not substantially greater than would be anticipated if the vessel were under a pilot's direction.
The “Standard of Care” lists conditions under which the PPA will grant waivers to qualified vessels (or companies that operate multiple vessels) in future. These conditions were added to the PPA's existing requirements, and include, among other things, that all vessels operating under a waiver must
- be operating a bridge navigational watch alarm system;Footnote 82
- be fitted with, and transmitting on, a Class A AIS; and
- have 2 persons on the bridge when operating in confined waters or in conditions of restricted visibility or in hours of darkness.Footnote 83
On 20 June 2018, the TSB followed up with the PPA to obtain an update on the status of the pilotage waiver system. The PPA indicated that it was monitoring all U.S. traffic equipped with AIS entering pilotage waters and verifying it against the waiver database. The PPA also has a list of Canadian companies providing towage services and monitors vessels from these companies using AIS. As at 20 June 2018, the PPA was monitoring 91 U.S. and Canadian companies. Currently, when the PPA identifies vessels that do not have a waiver entering a pilotage zone, the PPA contacts the ARs to inform them that either crew members must have a pilotage waiver or the vessel must have a pilot on board. The PPA also conducts random audits of crew documentation submitted during the waiver application process to check compliance with waiver requirements.
The PPA has recently published an article in a trade magazine aimed at making ARs and masters more aware of the pilotage waiver system and its requirements. Aside from monitoring vessel traffic in pilotage zones by AIS, the PPA indicates that it has limited resources to increase enforcement of the conditions of pilotage waivers in other ways (e.g., vessel spot checks). Additionally, not all vessels operating in pilotage zones have an AIS, which limits the PPA's ability to monitor using this method.
The company that operates the Ocean Monarch had applied for and was granted a pilotage waiver from the PPA in March 2017, as in previous years. The waiver covered all of the company's 6 tugs, as well as 8 of its barges and 23 personnel. The pilotage waiver request had been handled by an office employee, who sent the PPA a list of all company employees who might perform watchkeeping duties on a tug. Neither the company nor the PPA verified that the watchkeepers on the list had the experience required by the Pacific Pilotage Regulations.Footnote 84 The mate had been hired in May 2017 and, therefore, his name was not on the list that had been sent to the PPA about 2 months earlier. However, the master on board the Ocean Monarch was covered by the pilotage waiver.
The watchkeepers listed on the pilotage waiver application were not aware of the PPA regulations, the pilotage waiver that had been requested on their behalf, or the conditions of the waiver.
1.19 Mandatory occurrence reporting
The Shipping Casualties Reporting Regulations, the Vessel Traffic Services Zones Regulations, the Transportation Safety Board Regulations, and the Pacific Pilotage Authority Regulations all include requirements for vessels involved in marine occurrences in Canadian waters to report the occurrence in a timely manner.
The Shipping Casualties Reporting Regulations, issued under the CSA 2001, require
the master, any certificated officer, operator, member of the crew, pilot or person responsible for the ship, or the vessel being towed [to] report the incident without delay […] by radio communication to a Canadian radio ship reporting station […].Footnote 85
Among other things, the report should indicate
the identity of the ship from which the report is being made; the nature of the incident; […] the date, time and location of the incident; and […] whether the incident has caused or is likely to cause […] pollution of any waters.Footnote 86
The Vessel Traffic Services Zones Regulations require that a report be made to MCTS as soon as the vessel is involved in a collision, grounding, or striking, or the vessel sustains any defect in its main propulsion systems.
The Transportation Safety Board Regulations require marine occurrences to be reported either directly to the TSB or to a radio ship reporting station (e.g., a Canadian Coast Guard radio station or an MCTS centre). The Canadian Coast Guard emphasizes the need for timely reporting to MCTS to allow search and rescue resources to be alerted as soon as possible.
For a vessel that holds a pilotage waiver issued by the PPA and is involved in an occurrence in a compulsory pilotage area, the Pacific Pilotage Regulations require the master and the person who had the conduct of the vessel at the time of the occurrence to submit a full report to the PPA within 72 hours.Footnote 87
In this occurrence, the Ocean Monarch made bottom contact and sustained a failure of the starboard propulsion system. The master informed the company; however, although the tug continued to report in at all calling-in points before its arrival at Kitimat, the occurrence was not reported to MCTS, contravening the regulations. The Ocean Monarch also made a return journey on 1 main engine to the Fraser River with 2 empty barges in tow without having reported the occurrence to MCTS. As well, the occurrence was not reported to the PPA or the TSB in a timely manner.
1.20 Previous Board safety concern
Following an occurrence on 18 March 2015 involving the Syringa, a tug of less than 15 GT, that took on water and sank in the Strait of Georgia, BC, the Board issued a safety concern on the issue of regulatory oversight for tugs not more than 15 GT:
The Board is concerned that, without adequate oversight by the Department of Transport, shortcomings in the safety management and operations of tugs less than 15 GT may not be addressed. The Board will continue to monitor this situation with a view to assessing the need for further safety action on this issue.
1.21 Active TSB recommendations
Following an occurrence on 13 October 2016 involving the Nathan E. Stewart, a U.S.-registered articulated tug–barge unit that went aground after the second mate fell asleep while alone on watch at night, the Board made 2 recommendations, namely that
the Department of Transport require that watchkeepers whose work and rest periods are regulated by the Marine Personnel Regulations receive practical fatigue education and awareness training in order to help identify and prevent the risks of fatigue.
Transportation Safety Recommendation M18-01
the Department of Transport require vessel owners whose watchkeepers' work and rest periods are regulated by the Marine Personnel Regulations to implement a comprehensive fatigue management plan tailored specifically for their operation, to reduce the risk of fatigue.
Transportation Safety Recommendation M18-02
The report was issued on 31 May 2018.
In its response to the recommendations in August 2018, TC stated that it would continue collaborating with international partners on the Human Element, Training and Watchkeeping subcommittee of the IMO to address fatigue in the workplace by updating standards and applicable guidance material. TC also indicated that it required further research and industry engagement.
TC stated that it had started amending the MPR to implement the updated STCW by including mandatory training on fatigue management for masters and officers on vessels of 500 GT or more who are seeking to acquire a new or upgraded certificate of competency.
However, in the absence of any indication as to what changes will be made once the updated standards and guidance material have been reviewed by TC, it is unclear if and how the above-noted actions will address the intent of the recommendations. TC's response does not contain sufficient information to enable the Board to make a meaningful determination about whether the safety deficiency will be reduced.
Therefore, the response to Recommendations M18-01 and M18-02 are assessed as Unable to assess.
1.22 Previous occurrences
In 2011, the TSB investigated a fatigue-related occurrence involving a tug owned by the same company that operates the Ocean Monarch. On 28 June 2011, at 0410 Pacific Daylight Time, while being towed by the tug F.W. Wright, the loaded gravel barge Empire 40 struck the Queensborough Railway Bridge in the Fraser River.Footnote 88 The bridge centre swing span and protection pier suffered extensive damage. As a result, the bridge was inoperable for 2 months, causing major disruptions to railway and river traffic.
In that occurrence, the TSB investigation found that a third crew member (a mate) had joined the 2-person crew before a towing assignment. However, the master did not take advantage of the opportunity to rest and sleep after the mate joined the tug. As a result, the master had been awake for approximately 22 hours and was likely experiencing fatigue when he handed over the con to the mate and fell asleep at a critical stage in the passage. The mate had limited experience transiting the Queensborough Railway Bridge and, after having confirmed his approach to the bridge, attempted the transit on his own without seeking assistance from the master, leading to the barge striking the bridge. The investigation also determined that the company's operations were undocumented and informal, and it was left up to the masters and crew members to ensure that they obtained the appropriate amount of rest when needed. The TSB is not aware of any safety action taken by the company to address the fatigue-related issues raised during the investigation into the F.W. Wright accident.
Previous occurrences reported to the TSB have also identified issues similar to those raised in the Ocean Monarch occurrence with respect to fatigue (Appendix E) and 1-person bridge operations on tug–barge units (Appendix F).
1.23 TSB Watchlist
The TSB Watchlist identifies the key safety issues that need to be addressed to make Canada's transportation system even safer.
Safety management and oversight will remain on the TSB Watchlist until
- TC implements regulations requiring all commercial operators in the air and marine industries to have formal safety management processes and effectively oversees these processes;
- transportation companies that do have SMS demonstrate that it is working—that hazards are being identified and effective risk-mitigation measures are being implemented; and
- TC not only intervenes when companies are unable to manage safety effectively, but does so in a way that succeeds in changing unsafe operating practices.
Safety management and oversight is a Watchlist 2018 issue.
As this occurrence demonstrates, some transportation companies are not managing their safety risks effectively, and many are not required to have formal safety management processes in place. TC oversight and intervention have not always been effective at changing companies' unsafe operating practices. The solution will require all operators in the marine industry to have formal safety management processes, with oversight by TC. When companies are unable to effectively manage safety, TC must not only intervene, but also do so in a manner that succeeds in changing unsafe operating practices.
Fatigue management will remain on the TSB Watchlist until
- TC requires that watchkeepers whose work and rest periods are regulated by the MPR receive practical fatigue education and awareness training to help identify and prevent the risks of fatigue.
- Vessel owners are required to implement fatigue management plans, including education on the detrimental effects of fatigue and support to mariners in reporting, managing, and mitigating fatigue.
- TC reviews the domestic hours of work and rest provisions in the MPR in light of the most recent knowledge from fatigue science and, at a minimum, ensures consistency with the International Convention on Standards of Training, Certification and Watchkeeping for Seafarers.
Fatigue management in marine transportation is a Watchlist 2018 issue.
As this occurrence demonstrates, some transportation companies are not managing the risk of fatigue in their operations effectively, and many are not required to have FMPs in place. TC oversight and intervention have not always been effective at providing the training, education, and support necessary to mitigate fatigue among mariners. The solution will require TC to take actions to ensure that vessel owners are required to have FMPs, that mariners receive fatigue training, and that the domestic regulations around fatigue are, at a minimum, consistent with international standards.
1.24 TSB laboratory reports
The TSB completed the following laboratory report in support of this investigation:
- LP203/2017 – Chart Plotter Data Recovery
2.0 Analysis
The investigation determined that the watchkeeper, who was alone on watch in the wheelhouse at night, fell asleep while the tug and tow transited a narrow channel in the Inside Passage. The tug was on autopilot and proceeded until it made bottom contact. The investigation looked at the role of fatigue, the company's safety culture, and regulatory oversight for the Ocean Monarch and similar tugs.
2.1 Factors leading to the bottom contact
When the tug made bottom contact, the mate had been on duty for at least 8 hours and was alone on watch in confined waters. The master and deckhand were below deck asleep, and so the mate had no human interaction to help him remain awake. The tug was on autopilot, with all audible alarms disabled, and there were no strategies in place to mitigate crew fatigue.
Without records of the crew's actual hours of work and rest, it was not possible to assess the watchkeeper's level of fatigue. However, in the days leading up to the occurrence, the watchkeeper was subject to a number of fatigue risk factors, including acute fatigue, chronic sleep disruptions, circadian rhythm desynchronization, and nighttime working. On the night of the occurrence, the watchkeeper also experienced a low and monotonous workload in the wheelhouse.
The company did not have a fatigue-management plan (FMP), nor was one required by regulation. The master had received no guidance on fatigue management, and the crew had not received any training on conditions that contribute to fatigue. On the occurrence voyage, which was continuous over several days, the small crew complement of 3 made it challenging and, at times, impossible to have 2 watchkeepers at night while also ensuring the crew was sufficiently rested.
The tug was registered as less than 15 gross tonnage (GT) in 1992 and was permitted by TC to operate as a tug of this size, despite its estimated GT being greater than 15. As a consequence, it operated without regulatory inspections, safe manning guidance, or limitations on the type of voyage or activity it could undertake. The company and the master determined safe manning levels and the suitability of the tug for the voyages it was undertaking. The tug departed without enough crew to both manage operational requirements and remain sufficiently rested to operate safely on a continuous voyage of several days.
2.2 Presence of fatigue
The investigation was unable to ascertain the crew's hours of work or rest for the days preceding the occurrence, as this information was not recorded. It was therefore not possible to perform a quantitative analysis of data. However, it was possible to perform a qualitative analysis to establish the presence of fatigue. It was likely that acute fatigue, chronic sleep disruptions, and circadian rhythm desynchronization were fatigue risk factors for all of the crew members. In addition to these factors, the mate experienced additional risk factors—working during a circadian trough and task monotony—in the hours preceding the occurrence.
2.2.1 Acute fatigue
While on river operations from 03 to 06 July, the crew members worked on an as-needed basis throughout each 24-hour period, except for 2 work stoppages. Aside from these 2 periods, the work was mainly continuous and the crew did not rest in the accommodations but instead napped on the settee. Napping on the settee in the galley would have affected the crew's ability to achieve restorative sleep. Furthermore, there was no routine shift pattern and no compensation for interrupted rest periods. This type of operation would have reduced the crew's quantity and quality of sleep. Because this period was within the 3 days leading up to the occurrence on 09 July, acute fatigue was a risk factor for each crew member in the occurrence.
2.2.2 Circadian rhythm desynchronization
The crew had been off work for 2 weeks before their latest work period. While off work, they likely had normal nighttime rest. However, when returning to work for river operations in the days preceding the occurrence, the crew operated throughout the 24-hour period, across varying circadian rhythm highs and lows. Upon commencing coastal operations, the deckhand resumed a more regular daytime schedule and the master appeared to take more of the day/evening schedules. The mate, however, continued operating throughout the normal nighttime sleeping period, and his sleeping schedule continued to be variable.
Because the irregular hours started in the days preceding the occurrence, the crew had not had sufficient time or regular shift patterns to adapt to a new routine schedule. As a result, circadian rhythm desynchronization was a fatigue risk factor for each crew member, which would have exacerbated the effects of acute fatigue.
2.2.3 Chronic sleep disruptions
Any disruptions in sleep quantity that are sustained for periods longer than 3 consecutive days are considered chronic. It is unlikely the crew were fatigued before joining the vessel, as they had just completed a 2-week rest period. They would have started to become fatigued during the river operations that began on 03 July. However, once coastal operations began 2 to 3 days later, the crew resumed a more regular schedule. Although it is impossible to determine when each crew member actually slept, each one appeared to have about 12 hours available for rest (i.e., sleep became more achievable).
For this reason, it was unlikely that the crew continued to experience sleep deprivation once they started coastal operations. However, the crew likely would have experienced sleep disruptions as a result of the recent acute fatigue and circadian rhythm desynchronization, as well as the recent change in the quality of sleeping accommodations (tug accommodations rather than home).
2.2.4 Night operations
On the night of the occurrence, it was dark outside, the lights for the navigation equipment were dimmed, there was a low continuous vibration sound from the engine, the mate was seated, the sea conditions were calm, there was no opposing traffic, and the navigational alarms had been disabled. Performance and cognitive functioning are generally worst during a principal period of drowsiness between 0300 and 0500 (circadian trough). Any fatigue-inducing conditions exacerbate this vulnerability. Considering that the mate was likely already experiencing the effects of acute fatigue and circadian rhythm desynchronization, he would have been vulnerable to drowsiness during nighttime operations.
2.2.5 Task monotony
In the early hours of the morning, up to the time of occurrence, there was limited activity in the wheelhouse and the autopilot was engaged. The mate was more vulnerable to drowsiness as a result of the ambient conditions in the wheelhouse and a low and monotonous workload.
2.3 Management of fatigue
A lack of sleep and inconsistent sleep times are the primary risk factors that contribute to fatigue in mariners.Footnote 89 The Canadian Centre for Occupational Health and Safety cautions that “employers and supervisors should be concerned about the impact of fatigue in the workplace as it can be considered a form of impairment, making fatigue a workplace hazard.”Footnote 90 Regulations are the first line of defence to protect crews and operators from the risk of impairment due to fatigue.
The Ocean Monarch was required to abide by the minimum rest periods specified by the Marine Personnel Regulations (MPR) and the maximum work hours specified by the West Coast Shipping Employees Hours of Work Regulations and the Canada Labour Code, Part III. These require that the master ensures that crew members are not exposed to the risk of fatigue.
However, fatigue management must also be part of comprehensive and balanced safety management. Effective ways for a company to manage the overall risk of operational fatigue include compliance with regulations on hours of work and rest; implementation of an FMP or fatigue-related procedures, along with associated training; work–rest oversight; and fatigue reporting. External oversight must also be in place to ensure this process is working effectively.
2.3.1 Fatigue-management plans
An FMP is an effective tool to help companies ensure that fatigue is mitigated during operations. However, there is currently no requirement for Canadian marine companies to develop or implement FMPs. In this occurrence, an FMP may have helped the company to address some of the following shortcomings:
- Although it was the master's responsibility to manage the hours of rest for himself and his crew, the company had not provided the master and crew with fatigue awareness training.
- The master had no guidance or tools to assist him in managing hours of work and rest while also adjusting the crew members' schedules to accommodate shifts from river operations to coastal operations, domestic versus foreign voyages, and last-minute assignments.
- Without a defined work schedule and without documentation of the crew's hours of work and rest, the master and company had a limited ability to monitor the crew's activities to determine whether they were at risk of fatigue.
- The company did not have a formal method for fatigue reporting, and it was assumed that the crew would report fatigue. However,
- without training, the crew's ability to recognize fatigue in themselves and others was limited;
- mariners may be less likely to report feeling tired in an environment in which some or most of their co-workers are also likely to be fatigued;
- mariners may be less likely to report a personal issue such as fatigue directly to a manager or in a group setting; and
- mariners may be reluctant to report fatigue if it results in a reduction of working hours and thereby affects compensation.
- In order to operate with a single 3-person crew, the company allowed extended hours of work by compensating crew members for up to 16 to 17 hours per day.
The company therefore had no system in place to manage fatigue, to validate compliance with regulations governing hours of work and rest, or to monitor and track the crew's actual level of fatigue.
If a marine company does not have an FMP and there is no regulatory requirement for it to do so, there is a risk that crews will operate a vessel while fatigued, increasing the likelihood of an error that leads to an occurrence.
2.4 Management of safety
Effective management of safety requires a company to be actively involved in identifying and managing risks within its operations. While not all companies are required to have formal safety management systems (SMS) in place, it is nonetheless important that these companies work toward developing a strong safety culture.Footnote 91
A company with a strong safety culture strives to make safety a priority throughout all levels of the operation. It encourages employees to identify and report safety issues, and it provides the necessary support to manage these issues. A strong safety culture also guides a company toward regulatory compliance and helps it to establish an acceptable balance between management of safety and commercial pressures, in order to deliver efficient, cost-effective services.
If a company does not have a strong safety culture, commercial pressures can inadvertently lead to unsafe practices. The company may tend to operate at the minimum level of safety required by regulation or may not seek regulatory compliance at all. Over time, unsafe practices can become normalized as part of operations so that they are no longer considered risks. Masters are also placed in a challenging position if they receive little support to make operational decisions that prioritize safety. In such cases, it can be difficult for the crew to be the sole champions for safety.
Some of the safety issues and regulatory contraventions identified in the Ocean Monarch occurrence suggest shortcomings in the company's safety culture:
- There was only 1 watchkeeper in the wheelhouse at night, which was insufficient manning to ensure that all of the responsibilities associated with keeping a proper navigational watch were fulfilled and was also a contravention of both the MPR and the Seafarers' Training, Certification, and Watchkeeping Code.
- Given the nature of the tug's operations, it was not possible for the crew to remain sufficiently rested while maintaining a 2-person lookout with a crew of 3.
- Alarms to aid with safe navigation (e.g., to warn of hazards near the vessel's track or failure to make a planned course alteration) were not in use.
- There were no records maintained on the crew's hours of work (including overtime) and rest.
- Neither the master nor the company informed the appropriate authorities of the occurrence; they allowed the tug to operate in a damaged condition.
- The company had not provided its masters with comprehensive safe operating procedures.
- Fire and boat drills were not conducted on the Ocean Monarch.
- Although the mate was alone on watch, he was not covered by a pilotage waiver nor did he meet the experience requirements necessary to hold a waiver.
- The company had not informed TC after the tug's main engines were replaced in 2017; as a result, there was no follow-up to determine whether the modification had affected stability.
- TC was also not informed of the modification to the fuel oil tanks and the relocation of the access hatch for the lazarette space, both of which would affect the vessel's intact stability as assessed and approved.
- The company did not take safety action to address the fatigue-related issues raised by the TSB following a previous occurrence involving the company's tug F.W. Wright.
In the absence of a strong safety culture, an SMS, or documented operational procedures, the shortcomings in manning on the Ocean Monarch were not addressed to the company's management, nor did the company take an active role in identifying safety gaps and supporting masters in addressing them.
If companies do not establish a strong safety culture, there is a risk that commercial pressures and operational considerations will erode safety, leading to a hazardous operating environment for the crew.
2.5 Pilotage waiver compliance
The Pacific Pilotage Authority (PPA) has a mandate to provide safe, reliable, and efficient marine pilotage and related services in the coastal waters of British Columbia, including the Fraser River. While vessels operating in compulsory pilotage waters are required to have a pilot on board, some may be exempted under a waiver system. However, those exempted must still operate in a manner that ensures an equivalent level of safety such that the risk to life, property, and the environment is not substantially greater than would be anticipated if the vessel were under a pilot’s direction.
The investigation into the Ocean Monarch occurrence identified some issues with respect to the company’s compliance with the conditions of its pilotage waiver and with oversight of the pilotage waiver system in general:
- The PPA is currently tracking every vessel operating in pilotage zones using AIS, but not all vessels are fitted with AIS (e.g., tugs that do not hold waivers may not have an AIS).
- Some of the crew covered under pilotage waivers are unaware that they hold a waiver or of its conditions because the company that requests and obtains the waiver does not notify the crew.
- The PPA relies on authorized representatives to verify that crew members meet experience and certification requirements but has no independent process to verify the information provided other than conducting random audits.
Although the PPA has recently taken a number of proactive steps to improve awareness within the marine industry, some vessels are operating without fully complying with the associated requirements that ensure safe navigation.
If companies holding pilotage waivers do not operate in compliance with the conditions of the waiver and PPA oversight is not comprehensive enough to detect these non-compliances, there is a risk that vessels will not operate safely in pilotage waters.
2.6 Regulatory oversight
2.6.1 Tugs of not more than 15 gross tonnage
Vessel owners and operators have the primary responsibility to manage safety. However, it is vital that Transport Canada (TC) provide effective oversight and proactively intervene to ensure vessel owners and operators comply with regulations and can manage the safety of their operations effectively.
Currently, tugs of not more than 15 GT are not required to operate under a minimum safe manning document. This document specifies manning levels, taking into account the vessel's voyage classification, the number and certification of crew required for operations/maintenance, and emergency/abandon ship situations. Instead, the authorized representative and master for this class of vessels are responsible for determining manning levels in accordance with the MPR, and there is no oversight from TC to ensure manning levels are adequate. Unlike larger tugs, this particular class of smaller vessels is not required to be certified under the current Hull Construction Regulations and Hull Inspection Regulations. Consequently, these tugs are not subject to any geographical limitations on voyages, on the type of activity (e.g., towing) for which the vessel is used, or on the conditions (e.g., weather) in which the vessel is operating.
Although TC considers tugs of not more than 15 GT to be less of a risk and subjects them to less regulatory oversight, the consequences of not managing risks may be similar to tugs of greater than 15 GT. Although the recently conducted concentrated inspection campaign is not a substitute for effective oversight and, like all inspections, was reactive in nature, the results of the campaign show that a sampling of tugs of not more than 15 GT have more deficiencies than a sampling of those of greater than 15 GT. It is therefore important that tugs of not more than 15 GT are subject to a similar level of oversight as larger tugs to ensure that they are operated safely.
If tugs of not more than 15 GT are not subject to adequate regulatory oversight, there is a risk that shortcomings in operations will not be resolved, endangering the crew, the vessel, and the environment.
2.6.2 Tonnage measurement
While tugs of greater than 15 GT are subject to periodic inspections and accompanying manning and voyage restrictions, tugs of not more than 15 GT are not. They can therefore operate with fewer crew while carrying out any type of operation in any location, subject to the operator's judgment. Given the competitive nature of the towing industry, one in which contracts are usually allocated by a bidding system to the lowest-cost operators, tugs of not more than 15 GT have a commercial advantage over larger tugs. As a result, over the years, operators have employed various strategies to artificially reduce the registered GT of their tugs to under 15. While TC issued guidance in 1992 to stop this practice, the TSB analysis of tugs operating in BC identified that approximately 33% of the 51 vessels examined appear to have inaccurately registered GT measurements because of unrealistic depth dimensions.
Despite having an actual GT of 63.6, the Ocean Monarch was registered as a tug of not more than 15 GT and, since 1992, has been operating without being subject to the regulatory requirements for a tug of its size. For example, the Ocean Monarch did not have
- voyage restrictions,
- a minimum safe manning document,
- regular quadrennial inspections by TC, or
- a requirement for the master to hold a certificate valid for a vessel with a GT of up to 150.
Tugs of greater than 15 GT that were grandfathered and registered as tugs of not more than 15 GT are not subject to the regulatory requirements intended to ensure the vessel operates safely. In the absence of the intended regulatory oversight, safety issues may go unaddressed, especially those associated with insufficient manning and carrying out voyages for which the vessel is not suitable.
If tugs of greater than 15 GT are registered as tugs of not more than 15 GT, they will not be subject to oversight intended to ensure that they operate safely, and there is a risk that deficiencies will go unidentified and/or unaddressed, leading to accidents.
3.0 Findings
3.1 Findings as to causes and contributing factors
- The watchkeeper, who was alone on watch in the wheelhouse at night, fell asleep while the tug and tow transited the confined waters of the Inside Passage.
- The tug was on autopilot, with all audible navigational alarms disabled, and proceeded until it made bottom contact.
- When the tug made bottom contact, the mate had been on duty for at least 8 hours. The master and deckhand were below deck asleep, and so the mate had no human interaction to help him remain awake.
- It is likely that the acute fatigue, chronic sleep disruptions, circadian rhythm desynchronization, and nighttime working risk factors experienced by the mate in the days preceding the occurrence, combined with the low and monotonous workload in the wheelhouse, resulted in the mate falling asleep sometime between 0336 and 0436.
- There were no strategies in place to mitigate crew fatigue.
- Given the tug's 24 hours per day, 7 days per week operations, a crew complement of 3 made it challenging and, at times, impossible to have 2 watchkeepers at night while also ensuring the crew was sufficiently rested.
3.2 Findings as to risk
- If a marine company does not have a fatigue management plan and there is no regulatory requirement for it to do so, there is a risk that crews will operate a vessel while fatigued, increasing the likelihood of an error that leads to an occurrence.
- If companies do not establish a strong safety culture, there is a risk that commercial pressures and operational considerations will erode safety, leading to a hazardous operating environment for the crew.
- If companies holding pilotage waivers do not operate in compliance with the conditions of the waiver and Pacific Pilotage Authority oversight is not comprehensive enough to detect these non-compliances, there is a risk that vessels will not operate safely in pilotage waters.
- If tugs of not more than 15 gross tonnage are not subject to adequate regulatory oversight, there is a risk that shortcomings in operations will not be resolved, endangering the crew, the vessel, and the environment.
- If tugs of more than 15 gross tonnage are registered as tugs of not more than 15 gross tonnage, they will not be subject to oversight intended to ensure that they operate safely, and there is a risk that deficiencies will go unidentified and/or unaddressed, leading to accidents.
3.3 Other findings
- The Transport Canada Register of Vessels contains some outdated information for tugs, making it difficult to obtain reliable data on tugs operating on the west coast of Canada.
- While the master informed the company of the occurrence, it was not reported to Marine Communications and Traffic Services, the Pacific Pilotage Authority, or the TSB, as was required.
- At the time of the occurrence, although the Ocean Monarch's actual gross tonnage was 63.6, it was registered as a tug of not more than 15 gross tonnage and therefore was not subject to regulatory oversight (periodic inspections, a safe manning document, or any limitations on the type of voyages that it could undertake).
- A TSB analysis of a sampling of 51 tugs in British Columbia that measured 12 to 15 m long and were registered as of not more than 15 gross tonnage determined that, for 17 of these tugs, the depth recorded was significantly less than the typical depth of a tug of similar shape and size.
- The Pacific Pilotage Authority waiver process relies on operators to ensure accuracy of information submitted as part of a waiver request, and the Pacific Pilotage Authority has no process to verify the information other than random audits.
4.0 Safety action
4.1 Safety action taken
4.1.1 Mercury Launch & Tug Ltd.
Following the occurrence, the company installed a bridge navigational watch alarm system on the Ocean Monarch. New safe operating procedures were developed and implemented on the vessel. As well, the company informed all of its masters that navigation watch alarms are to be enabled and monitored at all times.
4.1.2 Canadian Coast Guard
The Canadian Coast Guard issued a contravention report to Transport Canada in regard to the company. The report indicated that the master did not ensure that a report was made to a marine traffic regulator following the bottom contact.
4.1.3 Transport Canada
Transport Canada launched a compliance inspection to identify regulatory infractions. The results of this inspection have not yet been released.
4.1.4 Pacific Pilotage Authority
Following the occurrence, the Pacific Pilotage Authority (PPA) revoked the pilotage waiver for the master and required the master to become informed of the waiver requirements before reinstating his waiver. The PPA also charged the company for applicable pilotage fees. The PPA published an article in a trade publication to increase awareness of the pilotage waiver system within the marine community. Additionally, the PPA sent an information package to authorized representatives of vessels that currently hold pilotage waivers. The information package is intended to inform masters of the conditions of a pilotage waiver.
This report concludes the Transportation Safety Board of Canada's investigation into this occurrence. the Board authorized the release of this report on . It was officially released on 10 January 2019.
Appendices
Appendix A – General arrangement of the Ocean Monarch (overhead and profile views)
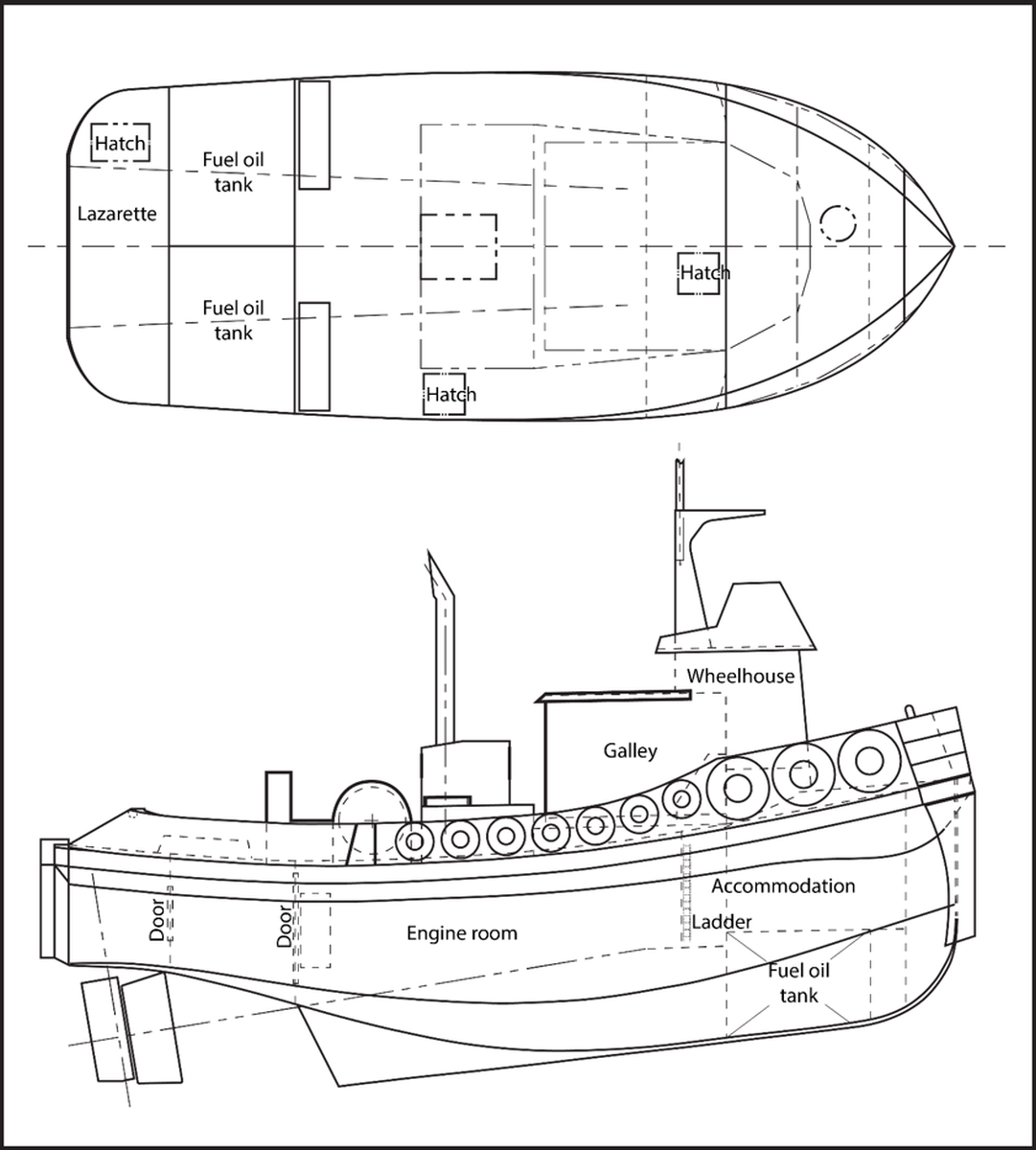
Appendix B – Area of the occurrence
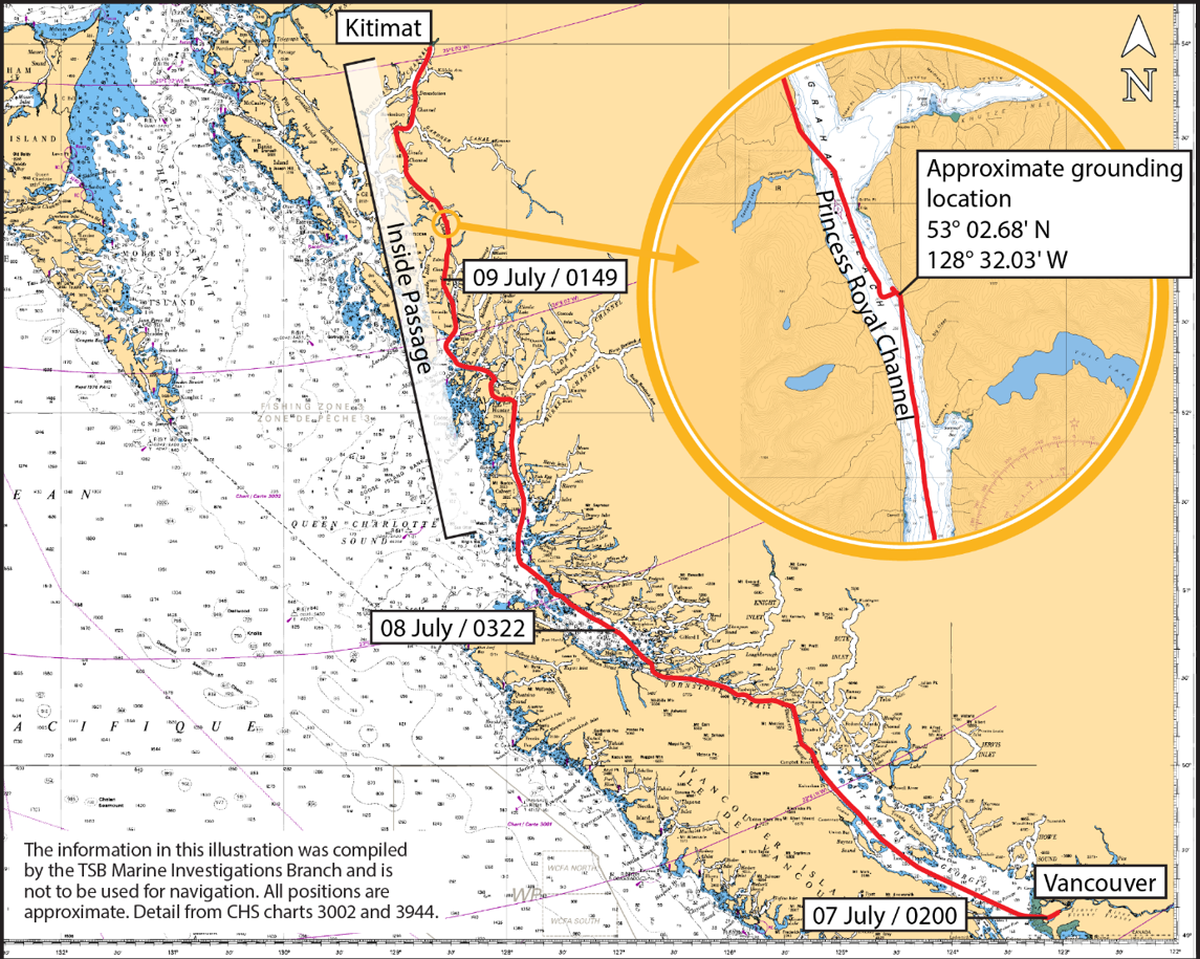
Appendix C – Analysis of tug gross tonnage measurements
The TSB analyzed the registered length, breadth, and depth measurements for a sampling of 51 tugs in British Columbia to identify whether the registered measurements are realistic, considering the tug's overall registered gross tonnage (GT). The analysis was prompted by instances in which the TSB identified incorrect registered tonnage measurements for 2 tugs, the Ocean Monarch and the Island Defender. The Island Defender was registered in 1990 with a GT of 14.66. The Department of National Defence purchased the tug in 1997, removed its high floors and recalculated its GT according to Transport Canada's Standard for the Tonnage Measurement of VesselsFootnote 92 as 64.83.Footnote 93
Because the TSB is aware that some tugs have historically been constructed with artificially raised floors, tugs of similar size were compared. The TSB assessed that 17 of the tugs from the sampling did not have accurate registered GT measurements because of unrealistic depth dimensions. For example, the Ocean Warlock has a maximum registered depth of 0.34 m, which includes an engine room space equipped with 2 × 600 kW engines. However, engines with that power rating have an average height of approximately 2 m.
Appendix D – Compulsory pilotage waters
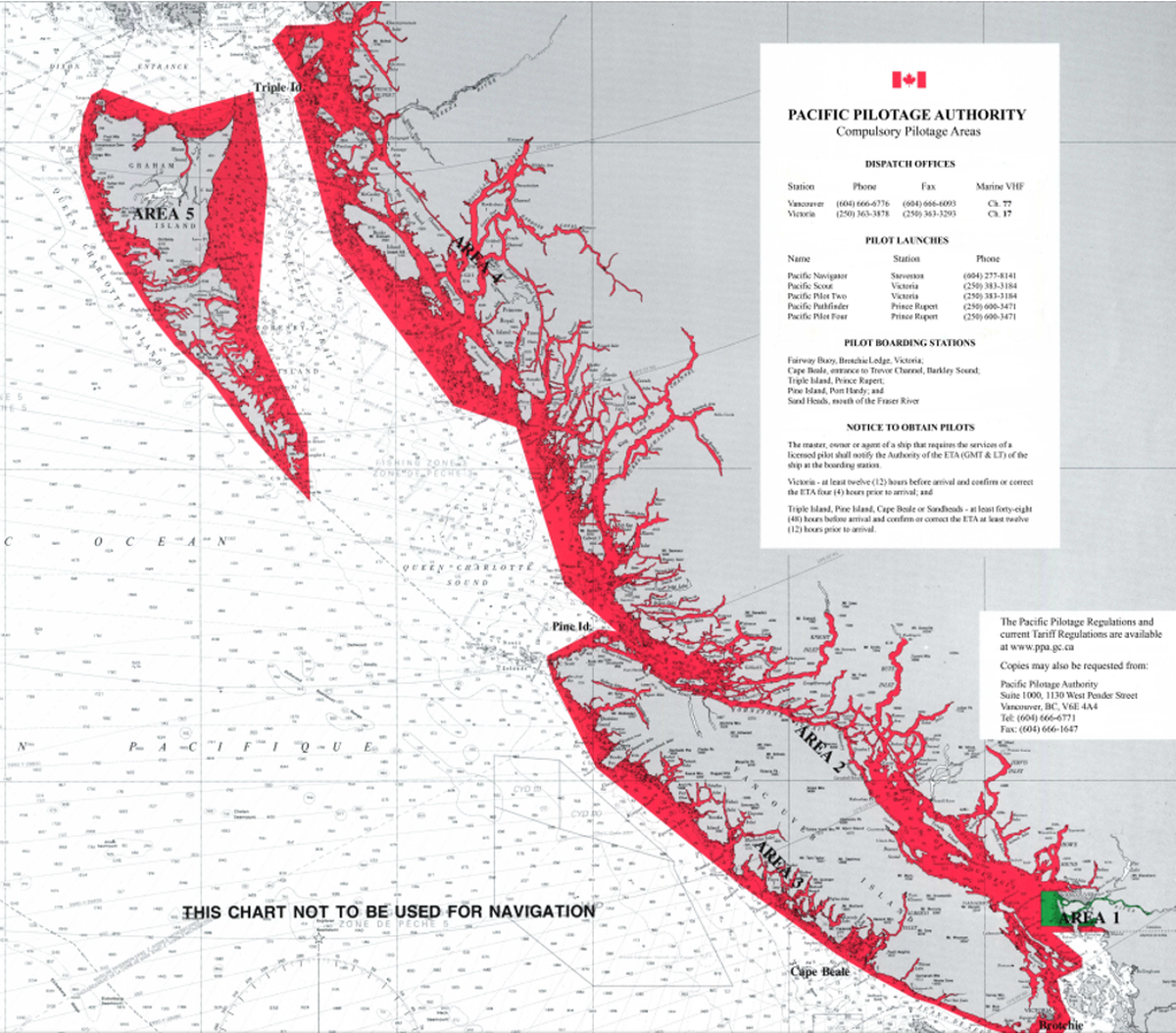
Appendix E – Previous occurrences involving fatigue
Since 1994, fatigue was a contributing factor in 139 marine occurrences reported to the TSB. Of the 128 marine investigations undertaken since 2002, fatigue was cited as a finding in 15 (12%). Six TSB investigation reports since 2006 found risks related to fatigue that are directly applicable to this occurrence.
M16P0378 (Nathan E. Stewart) – On 13 October 2016, shortly after 0100 Pacific Daylight Time, an articulated tug–barge, composed of the tug Nathan E. Stewart and the tank barge DBL 55, went aground on Edge Reef near Athlone Island, at the entrance to Seaforth Channel, approximately 10 nautical miles west of Bella Bella, British Columbia. The TSB investigation found that the second mate, who was working alone on the bridge, was fatigued. He fell asleep and did not make the planned course alteration. Available navigational alarms were not used, and a bridge navigational watch alarm system was not installed.
M12L0147 (Tundra) – On 28 November 2012, the bulk carrier Tundra ran aground off Sainte-Anne-de-Sorel, Quebec. The investigation found that fatigue was likely a factor in the pilot's diminished situational awareness and that “[i]f pilots are not trained in fatigue awareness, there is a risk that they may not be able to identify symptoms or signs related to sleep disorders, that are not detectable through a regular medical exam.”
M12F0011 (Viking Storm) – On 28 September 2012, the Canadian fishing vessel Viking Storm collided with the U.S. fishing vessel Maverick in thick fog, 30 nautical miles off La Push, Washington. The investigation found that the cognitive abilities of the mate were reduced owing to fatigue. The investigation also found that “[i]f fishermen equate resting with sleeping in terms of its restorative capacity, there is a risk that they may underestimate the continuous hours of sleep necessary to restore their cognitive functions.“ As well, the investigation found that “[w]ithout a fatigue management plan that considers fishing operations and the need to ensure uninterrupted sleep, crew members may not be sufficiently rested to safely perform their duties.”
M12N0017 (Beaumont Hamel) – On 30 May 2012, the passenger ferry Beaumont Hamel experienced an electrical failure that resulted in the loss of propulsion control and steering as it approached the wharf at Portugal Cove, Newfoundland and Labrador. Consequently, the vessel struck the wharf. The investigation found that “[f]atigue-management plans that do not provide sufficient opportunity for restorative sleep increase the risk of reduced crew performance on a routine basis.”
M09W0064 (Velero IV) – On 08 April 2009, the U.S. fishing research vessel Velero IV collided with the U.S. fishing vessel Silver Challenger II east of the Numas Islands in Queen Charlotte Strait, British Columbia. The investigation found that “[w]ork/rest schedules that do not provide for sufficient restorative sleep are likely to lead to fatigue, performance degradation, and errors due to lack of attention, alertness, and vigilance.”
M08W0193 (Kaien Pride) – On 13 September 2008, the tug Kaien Pride, towing 3 fish camp barges, ran aground on Garden Island, Prince Rupert, British Columbia. The tug refloated on its own with no apparent damage. The lone watchkeeper had fallen asleep at the wheel.
M07L0158 (Nordik Express) – On 16 August 2007, the passenger vessel Nordik Express struck Île de l'Entrée while approaching the entrance to Harrington Harbour, Quebec. The investigation found that “[i]n the absence of a fatigue management plan, the probability of fatigue-induced errors increases, thereby increasing the risk to vessels, crew, passengers, and the environment.”
M06N0014 (Kometik) – On 08 April 2006, a welder and a crew member were performing welding repairs on the shuttle tanker Kometik in Conception Bay, Newfoundland and Labrador, when an explosive vapour mixture was ignited in the vessel's cargo tank. The investigation found that a crew member was working while in a fatigued state. The investigation identified that “[t]he vessel's shipboard safety manual did not identify fatigue or workload as risk factors and did not incorporate procedures to mitigate them.”
Appendix F – Previous occurrences involving 1-person wheelhouse operations on tug–barge units
The following occurrences involving tug‑barge units were reported to the TSB. In each case, 1 qualified person was alone in the wheelhouse at night.
M16P0378 (Nathan E. Stewart) – On 13 October 2016, an articulated tug–barge, composed of the tug Nathan E. Stewart and the tank barge DBL 55, went aground on Edge Reef near Athlone Island, at the entrance to Seaforth Channel, approximately 10 nautical miles west of Bella Bella, British Columbia. The TSB investigation found that the second mate, who was working alone on the bridge, was fatigued. He fell asleep and did not make the planned course alteration. Available navigational alarms were not used, and a bridge navigational watch alarm system was not installed.
M16P0083 (Ocean Eagle) – On 15 March 2016, the tug Ocean Eagle towing the barge ZB 335 went aground in Johnstone Strait, British Columbia. The barge collided with the tug's stern and was damaged. There was no lookout posted, and the mate was alone in the wheelhouse during hours of darkness. The mate was busy with paperwork and missed the course alteration.
M07W0045 (Gulf Prince) – On 13 April 2007, the tug Gulf Prince, towing the empty barge MDM, grounded in the Gardner Canal, North Rix Island, British Columbia. There was one person in the wheelhouse at the time.
M04C0044 (Karen Andrie) – In September 2004, the barge A-397, pushed by the tug Karen Andrie (with an upper and lower wheelhouse), struck and knocked down Light Tower D33 in the lower Detroit River, Ontario.
M04F0016 (Evans McKeil) – In July 2004, the tug Evans McKeil (with an upper and lower wheelhouse), pushing the empty barge Ocean Hauler, struck and damaged private docks as well as a pleasure craft on the U.S. side of the St. Clair River. The tug subsequently ran aground.
M04F0010 (Doug McKeil) – In April 2004, the tug Doug McKeil (with an upper and lower wheelhouse), pushing the loaded barge Ocean Hauler, struck private docks and boathouses on the U.S. side of the St. Clair River.
M02C0011 (Progress/Pitts Carillon) – In April 2002, the barge Pitts Carillon, pushed by the tug Progress, struck and knocked down Light 82 in the St. Lawrence Seaway.