Crossing accident and derailment
Canadian National
Train no M-306-31-05
Mile 178.67, Napadogan Subdivision
Drummond, New Brunswick
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 06 October 2001, at approximately 1630 Atlantic daylight time, Canadian National freight train no M-306-31-05, travelling eastward towards Moncton, New Brunswick, derailed 15 cars after striking an automobile on a farm crossing at Mile 178.67 of the Napadogan Subdivision, in the township of Drummond, New Brunswick. Seven of the derailed cars were tank cars carrying liquefied petroleum gas. One of the tank cars suffered damage to the top protective housing and fittings, causing a release of butane. Nine cars and approximately 1000 feet of track were destroyed. There were no injuries.
Ce rapport est également disponible en français.
1.0 Factual information
1.1 The accident
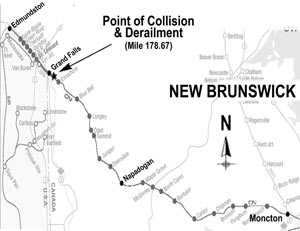
On 06 October 2001, at about 1530 Atlantic daylight timeFootnote 1, Canadian National (CN)Footnote 2 freight train no M-306-31-05 (train 306) departed Edmundston, New Brunswick, destined for Moncton, New Brunswick (see Figure 1). Train 306 consisted of 3 locomotives, 60 loaded cars, 52 empty cars, and 18 residue cars, was about 8700 feet long and weighed approximately 10 000 tons. There were two crew, a locomotive engineer and a conductor. They met fitness and rest standards, were qualified for their respective positions, and were familiar with the subdivision.
As train 306 approached a farm crossing at Mile 178.67, a southbound automobile moved onto the crossing and stopped. The locomotive engineer sounded the horn and then made an emergency brake application when it became evident that the automobile had stalled on the crossing. The crew sheltered themselves against the imminent collision. The lead locomotive struck the automobile and came to rest approximately 1070 feet from the crossing. The three occupants had abandoned the automobile prior to the collision and were not physically injured.
Information from the locomotive event recorder indicated that train 306 was travelling at a speed of 38 mph with the throttle in the no 8 position. At Mile 178.78, approximately 580 feet from the crossing, the locomotive horn was sounded and at Mile 178.68, approximately 70 feet from the crossing, train 306 was put into emergency from the controlling brake valve of the lead locomotive. The locomotive speed decreased from 38 mph to 27 mph in the first 14 seconds, remained constant for 6 seconds, and then decreased to 0 mph over the remaining 14 seconds. The emergency toggle switch, with which all Train Information and Braking system (TIBS)Footnote 3 are equipped, was not actuated.
1.2 Emergency response
The crew conducted the necessary emergency procedures and called the rail traffic controller to request immediate assistance. A CN supervisor and local firefighters responded immediately to the accident. The automobile occupants were transported to the local hospital where they were treated for post-incident stress trauma.
Two local police officers were dispatched to the site immediately after the accident. One officer approached the rear of train 306 in his police cruiser, smelled a strong gas odour, and withdrew from the site. The officer had basic dangerous goods awareness training. The safety equipment in his vehicle did not include any equipment for protection against dangerous goods.
In two previous railway accidents, a yard derailment in 2001 near Red Deer, Alberta (TSB Report R01E0009) and a main track derailment in 1999 near Britt, Ontario (TSB Report R99T0256), police officers approached the accident site without dangerous goods protective equipment and were exposed to anhydrous ammonia. In both of these occurrences, the officers had received basic dangerous goods awareness training.
As a result of the investigation on the derailment near Britt, the Board expressed concern that emergency response personnel in small communities may not be provided with the necessary tools, protective equipment and training to be fully aware of and prepared for the risks associated with the dangerous goods being transported through their community.
A security perimeter was established and the site was constantly monitored to ensure the safety of workers and nearby residents. A team from the Liquid Petroleum Gas Emergency Response Corporation arrived from Saint John, New Brunswick. Residents were advised to remain indoors, but no evacuation was required.
1.3 Occurrence site information
1.3.1 Derailed rolling stock
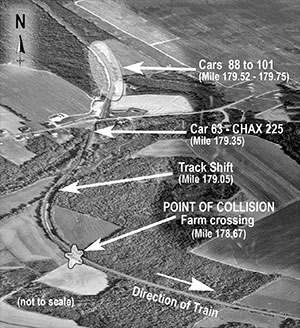
A subsequent inspection of train 306 determined that the 63rd car, and the 88th car to the 101st car from the head-end, derailed (see Photo 1). Fresh marks were visible on striker castings and coupler horns on many cars throughout the train.
1.3.2 Tank car CHAX 225
The 63rd car, CHAX 225, a class 111A tank car, buckled upwards and derailed the B-endFootnote 4 at Mile 179.35 (see Photo 2). The tank car was empty and located between loaded hopper cars. Samples from the car were sent to the TSB Engineering Laboratory for analysis (report LP 102/01); the examination did not reveal any significant reduction in the car's strength. According to Association of American Railroads (AAR) design standards, tank cars must withstand a minimum longitudinal force of 1 000 000 pounds.Footnote 5

The 88th car to the 101st car derailed in the entry spiral of a right-hand curve between Mile 179.75 and Mile 179.52. The 88th car remained upright. The 89th car to the 92nd car were rolled over south of the track. The 93rd car and 94th car, two long automobile carriers with end-of-car cushioning devices (EOCCD), jack-knifed, and six loaded pressure tank cars containing liquefied petroleum gas piled-up behind them. The derailed tank cars sustained damage to their head shields and stub sills.
1.3.3 Pressure Tank Cars Carrying Dangerous Goods
The 95th car, CITX 4240, a class 112 pressure tank car, came to rest on its side, striking the underframe of the 94th car. The protective housing was bent, damaging the liquid eduction valve (see Photo 3) and causing a release of butane.

Butane (UN 1075) is an extremely flammable, colourless gas. In gas and liquid forms, butane is an irritant that can cause eye injury, frostbite, or respiratory problems. It is an asphyxiant and may explode if subjected to an impact and/or static discharge. Special protective clothing and equipment are required when entering a leak or spill area.
Damage similar to that sustained by car CITX 4240 was observed on tank cars involved in the yard derailment at Red Deer, where damage to the top protective housing of an anhydrous ammonia car caused a product release that resulted in one fatality, the hospitalization of 34 people, and the evacuation of 1600 residents. Also, during a derailment on 26 November 1998 at MacMillan Yard, Concord, Ontario (TSB Report R98T0292), a tank car rolled over, damaging the protective housing and valve and causing a minor leak; the yard was evacuated and a major highway was blocked for several hours.
Safety action taken as a result of the Red Deer and Concord accidents involved the car owners, Transport Canada (TC), the Federal Railroad Association (FRA), and the AAR Tank Car Committee. It included stress analyses of tank car structure and manway areas, a review of top fitting protection requirements, and a review of accident data to determine the sturdiness of protective housing covers and clearances. In August 2002, the transportation of dangerous goods standards were issued.Footnote 6 The level of protection required for pressure tank car top fittings in the new standards has not been increased; however, TC has not ruled out the possibility of amending the standards once the industry review is completed.
1.3.4 Track
The Napadogan Subdivision consists of a single main track that extends from Pacific Junction, New Brunswick, (Mile 0.0) to Edmundston (Mile 219.4). Train movements were governed by the Centralized Traffic Control System in accordance with the Canadian Rail Operating Rules and were supervised by a rail traffic controller located in Montréal, Quebec.
In the area of the derailment, the maximum authorized timetable speed for freight trains was 45 mph. The track had an ascending grade varying from 0.2 to 0.4 per cent in the direction of train movement. The track structure consisted of continuous welded rail laid on double-shouldered tie plates and hardwood ties. On curves, the rail was 136 pounds and secured with six spikes per tie; on tangents, it was 132 pounds and secured with four spikes per tie. There were approximately 3120 hardwood ties per mile. The ballast consisted of crushed rock 1 ½ to 2 inches in diameter and 12 to 18 inches deep. The cribs were full and the shoulders were 18 inches wide.
The track met CN's Standard Practice Circulars and TC's Railway Track Safety Rules. The track geometry was recorded by a track geometry car on 13 July 2001; no exceptions were noted. The rails were tested by a rail flaw detection car on 05 September 2001; no internal defects were detected. The derailment area was last inspected by the assistant track supervisor in a Hi-rail vehicle on 04 October 2001; no defects were observed.
Examination of the derailment site revealed that at Mile 179.05, over a distance of about 30 feet along a curve, the track was shifted to the south, the ballast was disturbed and the spikes on the gauge side of the south rail were lifted two inches. At Mile 179.75, wheel flange marks were observed on the ties on the gauge side of the south rail, and on the web of the north rail. The north rail was rolled over to the field side.
1.3.5 The farm crossing
The farm crossing approach from the north side had a gravel surface level with the crossing planks. The planks were in good condition. The sight-line in the northwest quadrant was approximately 130 m (425 feet) for a driver stopped 6.5 m (20 feet) from the tracks. The sight-lines in the other quadrants met the 230 m (750 feet) draft minimum standards required for newly-constructed crossings.Footnote 7
1.4 Marshalling of train 306
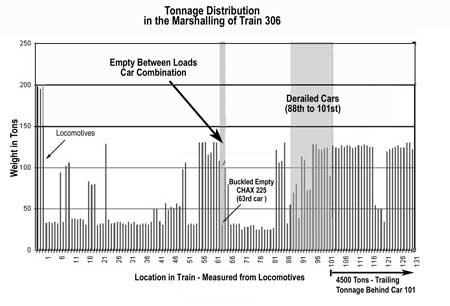
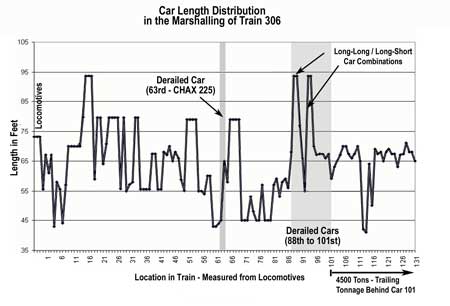
Most of the loaded cars on train 306 were located in the tail-end portion of the train (see Figure 2). There were several long-long and long-short car combinations in the consist (see Figure 3). Ten of the cars were equipped with EOCCDs. Train 306 passed by a wayside information system at Mile 200.5; no defects were noted.
1.4.1 CN train marshalling requirements
CNs train service planning is performed using a computerized system. This system, which also produces the train consists, tonnage profiles, and billing/dangerous goods information for individual trains, recognizes any train design that violates the CN General Operating Instructions(GOI) requirements for rolling stock restrictions and dangerous goods placement. The system is interfaced with wayside automated equipment identification systemsFootnote 8 which allow en route identification of marshalling violations. There are no GOI constraints on tonnage distribution along the train; as a result, weight distribution is not controlled when the train is marshalled.
The train journals for train 306, and other trains run to the same train service plan, show consistent sequential destination blocking.Footnote 9 They also show that the trains are generally marshalled with empty cars concentrated at the head-end, or placed between long blocks of loaded, heavy cars. Sequential destination blocking is commonly used by CN.
1.5 Emergency brake function
Trains with empties-ahead/loads-behind configurations are subjected to increased buff forces during emergency brake applications as shown by train dynamics studies.Footnote 10
The railways are implementing methods to control in-train forces during emergency braking. For instance, CN has issued a directive in timetable 78 requiring the application of the emergency brake from both the locomotive and the tail-end. This is achieved by placing the automatic brake valve in the emergency position, and actuating the emergency toggle switch on the locomotive stand (see Photo 4). Also, at thetime of this occurrence, CN was testing an end-of-train system that automatically initiates synchronous braking from both the locomotive and the tail-end during emergency and service applications. Some railways in the United States have already equipped their trains with such systems.Footnote 11 As of 01 November 2001, the AAR requires all new locomotives be equipped with automated end-of-train devicesFootnote 12 to comply with FRA Regulation 49 CFR 232.405, Design and Performance Standards for Two-Way End-of-Train Devices.Footnote 13 The FRA regulation requires all locomotives ordered on or after 01 August 2001, or first placed into service on or after 01 August 2003, to be designed to automatically initiate a simultaneous emergency brake application at the head and tail end of the train whenever the locomotive engineer places the train air brakes in emergency.

1.6 Other information
The Board investigated derailments that occurred after an emergency brake application on long trains that had an empties-ahead/loads-behind configuration similar to Train 306 (TSB Report R00Q0023 and Report R01T0006).
2.0 Analysis
2.1 The accident
Train 306 struck a stalled automobile at a farm crossing, and then derailed. When the locomotive horn was sounded, Train 306 was 580 feet from the crossing. At the speed at which train 306 was travelling, the automobile had sufficient time to clear the crossing; therefore, had the automobile not stalled, the collision would not have occurred. Even though there were no gates or signs at the crossing, and the sight-line in the northwest quadrant was less than the minimum standard, the condition of the crossing did not contribute to the collision.
The fresh marks on the coupler horns and striker castings, the type of damage to the derailed cars and the track structure, and the deceleration profile of the locomotive, are characteristic of an event involving high in-train buff forces. Therefore, the analysis will focus on the train dynamics, pressure tank car design and emergency response.
2.2 Emergency air brake operation
On trains equipped with conventional air brakes, an emergency brake application from the lead locomotive does not result in the simultaneous braking of all cars as the braking action takes time to propagate from the head-end of the train to the tail-end. The time of propagation results in the cars at the tail-end of the train receiving effective braking last. In longer trains, or trains containing cars with EOCCDs, the brake pipe length is increased, further delaying the onset of effective braking action in the tail-end-braking may be fully applied at the head end before any initiation of braking at the tail-end. Therefore, when the train is stretched, a run-in of train slack will occur and in-train buff forces will be generated.
2.3 Train marshalling
Train marshalling practices and length affect the magnitude of the in-train buff forces during emergency brake application from the locomotive. When trains are marshalled with light cars at the head-end and heavy cars at the tail-end, the head-end will decelerate sooner and faster than the tail-end. The heavy cars at the tail-end, with their greater momentum, will run into the slower moving cars at the head-end, generating high run-in buff forces. The amount of slack and the run-in buff forces are further increased on long trains, and on trains containing cars equipped with EOCCDs.
CN's marshalling GOIs and train planning systems have no constraints on tonnage distribution and train length; therefore, trains are not systematically configured to allow an effective control of the buff forces. On curved track, these buff forces, acting on long/long or long/short car combinations, generate a larger lateral force on the track structure, increasing the risk of derailment. Due to the inclination of the draw bars between empty and loaded cars, the buff forces will subject an empty car located between loaded cars to high compressive and lifting forces, which can derail or buckle the car.
For instance, train 306 was a long train marshalled with most of the weight in the tail-end. At the time of the accident, train 306 was negotiating an ascending grade, and was, therefore, fully-stretched; as the emergency brake was applied from the locomotive, a run-in occurred, and high buff forces were generated. Although the track met CN's Standard Practice Circulars and TC's Railway Track Safety Rules, the action of the buff forces on the 88th to the 101st cars, where several long/long, long/short car combinations were located on curved track, generated high lateral forces that exceeded the resistance of the track structure, causing gauge widening, rail rollover, and the derailment of the cars. Furthermore, the buff forces generated compressive stresses that exceeded the design specifications of the 63rd car, an empty tank car located between loaded cars, causing the tank car to derail and buckle.
2.4 Use of the emergency brake
The Board has investigated two other occurrences (TSB Report R00Q0023 and Report R01T0006) where the trains had a configuration similar to train 306. In both, there were issues relating to configuration and length and the generation of high in-train buff forces during emergency brake applications. Emergency brake applications are not uncommon. They are initiated when a collision is imminent or when there is a loss of air pressure due to air hose separation or kickers.Footnote 14 Therefore, since emergency brake applications are not uncommon and since CN marshalls trains with no constraints on tonnage distribution and train length, derailments caused by high in-train buff forces are more likely to occur.
Even though CN has a directive requiring locomotive engineers to initiate end-of-train braking in emergencies by actuating the toggle switch on the control stand in order to reduce in-train forces, the toggle switch was not actuated in this occurrence. During emergency brake activation, a locomotive engineer must quickly respond and perform a sequence of actions under pressure. To ensure that all motor components of the emergency procedure are reliably triggered, the response sequence must be overlearnedFootnote 15 (i.e., it becomes, through repetitive practice, an automatic process, thereby requiring less attention and making emergency responses more resistant to stress and interference by other tasks). If the emergency braking procedure is not overlearned, it is not performed consistently from both ends of the train, resulting in higher in-train buff forces and a greater risk of derailment.
The railways recognize that reliable actuation of end-of-train braking during an operator-initiated emergency brake application, either through on-going training or hardware automation, reduces the magnitude of in-train buff forces, and therefore, the risk of derailment. CN, in particular, has been very active in testing an end-of-train system that automatically initiates synchronous braking from both the locomotive and the tail-end during emergency and service applications. This safety initiative is a positive step towards reducing the risk of derailment during brake applications.
2.5 Pressurized tank car protection
In this occurrence, the liquid eduction valve was damaged, causing product to leak when tank car CITX 4240 overturned while train 306 was travelling at 27 mph. This type of damage also occurs in yard accidents where the speed is relatively low, as was observed on tank cars involved in the yard derailments at Macmillan Yard and Red Deer (TSB Report no R98T0292 and Report no R01E0009). Following these derailments, Transport Canada (TC) indicated that issues relating to design requirements applicable to top fitting protection would be examined when the standards were reviewed. In August 2002, new dangerous goods containment standards were issued; however, the requirement for rollover or skid protection for top fittings was not improved. Therefore, the shortcomings identified in the protection of top fittings remain unaddressed and will continue to present a risk to the public and the environment.
2.6 Emergency response
The local police officers dispatched to this occurrence were not experienced with large train derailments involving dangerous goods. They approached the accident without protective equipment for dangerous goods or information about the products involved in the derailment, even though they had received basic dangerous goods awareness training. This behaviour reinforces the safety concern expressed by the Board after the accident near Britt that, due to the low frequency of exposure to railway accidents, some first responders in small communities may not have the level of awareness to adequately assess the risks associated with railway accidents involving dangerous goods. Consequently, they continue to take inappropriate actions and expose themselves to dangerous goods in the performance of their duties.
3.0 Findings
3.1 Findings as to causes and contributing dactors
- The accident occurred when train 306 struck the stalled automobile on the crossing, and then derailed.
- Given the track profile and train configuration, the emergency brake application from the head-end caused excessive run-in, which generated high buff forces.
- Because of the curvature of the track, the high buff forces generated high lateral forces that exceeded the resistance of the track structure and derailed the 88th car to the 101st car.
- The 63rd car, an empty tank car located between loaded cars, was subjected to lifting forces and high compressive forces that exceeded its design specifications, causing the derailment and buckling of the car.
- When tank car CITX 4240 overturned, striking the adjoining car, the liquid eduction valve was damaged, causing a product leak.
3.2 Findings as to risk
- Marshalling General Operating Instructions and train planning systems, which have no constraints on tonnage distribution and train length, do not allow an effective control of the buff forces and increase the risk of derailment during an emergency brake application.
- Since the emergency braking procedure is not overlearned by the locomotive crews, the initiation of the emergency braking is not performed consistently from both ends of the train, resulting in higher in-train buff forces and a greater risk of derailment.
- As there is no requirement for rollover or skid protection for top fittings on pressure tank cars, damage to the top protective housing and fittings will continue to occur even in accidents where the speed is relatively low.
- Some first responders in small communities may not have the level of awareness to adequately assess the risks associated with railway accidents involving dangerous goods; consequently, they continue to take inappropriate actions and expose themselves to dangerous goods in the performance of their duties.
3.3 Other findings
- Even though there were no gates or signs at the farm crossing, and the sight-lines in the northwest quadrant were less than the minimum standard, the condition of the crossing was not a contributory factor in the collision.
4.0 Safety action
4.1 Action taken
4.1.1 Canadian National
Canadian National (CN) has initiated a program to equip its operating fleet of approximately 1600 road locomotives with an end-of-train system that automatically initiates synchronous braking from both the locomotive and the tail-end during emergency and service applications. As of April 2003, CN had equipped 98 locomotives and acquired 198 end-of-train devices for use in their Canadian operations.
The sight-lines of the crossing located at Mile 178.67 of the CN Napadogan Subdivision were improved in the north quadrant in 2002 to meet the minimum requirements of the proposed grade crossing standards.
As part of TransCAER (Transportation Community Awareness and Emergency Response Program), a North America-wide initiative sponsored by the railways and the chemical producers, CN has conducted 477 presentations to 16 325 first responders since 1993 in Canada, many of which take place in small communities. Visor cards describing precautions to take at a derailment site are supplied to first responders for display in their vehicles.
4.1.2 Transport Canada
Transport Canada (TC) revised the Railway Locomotive Inspection and Safety Rules in September 2002. Section 10.2 requires new locomotives to meet Association of American Railroads (AAR) standards for the automated and simultaneous activation of two-way end-of-train devices during an engineer-initiated emergency brake application.Footnote 16
On 27 May 2003, TC wrote the Railway Association of Canada to discuss development and implementation of train design specifications that take train tonnage and train length into consideration, and suggested that train-handling instructions be written to aid locomotive engineers with regards to weight distribution in order to avoid excessive braking forces whenever possible.
4.1.3 Industry
After the Red Deer occurrence, and other similar accidents, the AAR Tank Car Committee Task Force on Top Fitting Protection for pressure tank cars focussed on the issue more closely, in concert with the member railways, car builders, and regulatory agencies in Canada and the United States. Issues under review by the committee include:
- Ability for manway to withstand gentle rollover;
- Determination of loads on the manway generated from a slow rollover;
- Review of "Texas wedding ring" style construction manway strength as compared to other designs; and
- Appropriate vertical design loads for manways.
Engineering data from the Red Deer accident has been disseminated to help with the problem analysis. To date, no resolution has been put forward; the regulators in Canada and the United States continue to work on this issue, and to monitor the work in progress at the AAR.
4.1.4 Emergency response
Ensuring the safety of the public and police officers is of a paramount concern to the Royal Canadian Mounted Police (RCMP). Several courses of action have been taken to improve officer awareness with this type of event and the associated dangers. The police Cadet Training Program focuses on risk assessment at all stages of an investigation. Officer safety is stressed, with particular emphasis on knowing the environment surrounding any situation before entry. All members are provided with basic dangerous goods awareness training which includes identifying dangerous goods placards. On-line web tools containing the Code of Police Practice which is a guide for front-line officers when dealing with dangerous goods, bomb threats or explosions, and railway incidents are available to all force members. The site also contains links to the ">Transportation of Dangerous Goods Act and deals with the aspects of criminal offences under the Act.
As a result of the events of 11 September 2001, an Emergency Management Unit was Established within the RCMP's Critical Incident Program. One of the principal tasks of this new unit is to establish a standardized all-hazards emergency planning process and Emergency Operations Plan template for implementation by all RCMP divisions and their detachments. A draft copy of the Emergency Operations Plan will be forwarded to all RCMP Divisions for review and comment in the very near future. Within the Emergency Operations Plan are two annexes, "HAZMAT" and "Major Rail Event", which describe standardized emergency response policies and procedures for RCMP first responders as well as incident management with other response agencies.
A complete review of this accident will be conducted with the appropriate officers in New Brunswick, and in the future, it is expected that the implementation of the Emergency Operations Plan will assist in reducing risks to officers and other response agency personnel.
4.2 Action required
4.2.1 Safe train operation during emergency braking
Crossing accidents and other crisis situations occur almost daily, making the use of the emergency brake a relatively frequent event. The TSB occurrence database has shown that between 1998-2001, there were 1222 occurrences where there was an emergency brake application or a very high probability of the use of the emergency brakes. During the same period, there were 447 main track train derailments involving freight trains reported to the TSB. Among these, five occurrences, including the investigated occurrence, were identified as resulting from the use of an emergency brake application by the locomotive engineer.
TSB investigations have demonstrated that current defences do not always control in-train forces during emergency braking in a manner consistent with safe train operation. With the present marshalling of trains, with no constraints on tonnage distribution and train length, high in-train buff forces are more likely to take place, particularly during emergency brake applications initiated by the locomotive engineer or in the train itself. Depending on train make-up, the braking characteristics of the particular train, the track grade and curve profile, and the initial slack condition within the train, this could lead to an increase in the risk of derailment and an increase in derailment severity (as demonstrated in this occurrence or in Report no R00Q0023, where additional derailments occurred in the rear of the consist).
The issues related to the control of in-train forces on trains marshalled without constraints on tonnage distribution and train length have been included in the TSB Key Safety Issues List, which represent the issues presenting significant safety concerns.
While there have been only five occurrences from 1998 to 2001 where the train derailments resulted from an emergency brake application by the locomotive engineer, the consequences associated with those occurrences are of concern to the Board. There is a continuing trend towards the use of longer, heavier, trains. At the same time, the amount of chemical traffic on the railways is a continuing growth area in rail traffic. This situation indicates, all other things being equal, that the frequency of these accidents will increase and the outcome of future accidents, where the operator places the train in emergency, will be more severe than those which have happened in the last few years.
There are several remedial options to mitigate this situation. For example, on the administrative side, improved, intensive, training of locomotive engineers could develop in them a rote type of reaction, such that, when placing the train in emergency, they will automatically turn the toggle switch. Similarly, there could be a revision to the approach to marshalling long, heavy, trains such that in-train forces are more controllable. Finally, there is the possibility of technological approaches, such as a full application, including retrofitting of locomotives, of the mandatory system where a train placed in emergency would automatically initiate a head and tail-end emergency simultaneously. TC safety initiatives, which seek improvements in the railways' development of train-handling instructions, the implementation of train design specifications and rule revisions requiring new locomotives to meet new AAR standards for the automated and simultaneous activation of two-way end-of-train devices, will improve emergency brake performance in the long term.
CN has equipped six per cent of their locomotive fleet with an end-of-train system that automatically initiates synchronous braking from both the locomotive and the tail-end during emergency and service applications. However, CN and other Canadian railways have not committed to a program which would accelerate the replacement of existing systems with the newer technology. Therefore, the remaining existing locomotives will continue to use older end-of-train units until they reach the end of their service life. Given that Canadian railways are equipped with a relatively young locomotive fleet, and given the evolution of freight train operations to longer trains, the risks inherent to emergency situations on long freight trains will remain unaddressed. Therefore, the Board recommends that as a priority:
Transport Canada encourage the railway companies to implement technologies and/or methods of train control to assure that in-train forces generated during emergency braking are consistent with safe train operation.
Transportation Safety Recommendation R04-01
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .
Appendices
Appendix A - Glossary
- AAR
- Association of American Railroads
- CFR
- Code of Federal Regulations
- CN
- Canadian National
- EOCCD
- end-of-car cushioning devices
- FRA
- Federal Railway Association
- GOI
- General Operating Instructions
- m
- metre(s)
- mph
- mile(s) per hour
- RCMP
- Royal Canadian Mounted Police
- TC
- Transport Canada
- TIBS
- Train Information and Braking system
- TSB
- Transportation Safety Board of Canada