Runaway rolling stock
Canadian Pacific Railway
Runaway cut of cars
Mile 119.5, Winchester Subdivision
Smiths Falls, Ontario
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
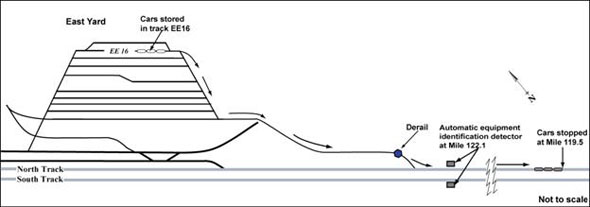
On 04 July 2007, at approximately 2220 eastern daylight time, eastward Canadian Pacific Railway train 220 travelling on the south track of Canadian Pacific Railway's Winchester Subdivision (near Smiths Falls, Ontario) reported that there were three unattended rail cars on the north track east of Smiths Falls Yard at approximately Mile 119.5. The three cars had rolled eastward, uncontrolled, for approximately 3.4 miles, from Smiths Falls Yard. Uncontrolled entry to the main track from different areas of the yard was protected by a number of derail installations, which are intended to derail runaway cars as they pass over them. The runaway cars were returned to the yard without further incident.
Ce rapport est également disponible en français.
Factual information
The cut of cars (SOO 5002, SOO 5010 and SOO 5017), flat cars that were being used to transport track ties, had been moved the previous day (03 July 2007) by Canadian Pacific Railway's (CPR) Engineering Services employees and stored in track EE16 in Smiths Falls Yard (see Figure 1).
The cut of cars was handled using a highway tractor truck that had been modified to operate on rails. This reconfigured truck is known as a Brandt hi-rail truck (see Photo 1). On 03 July 2007, the Brandt truck had an air system failure that affected its braking capability and its ability to recharge braking systems on rail cars.

On 04 July 2007, when the Brandt hi-rail truck was used again to move the cut of cars, there was insufficient air supply to recharge the braking systems of the rail cars. In addition, due to the lack of air, the normal practice of performing a push-pull testFootnote 1 on the parked cars and testing the effectiveness of the securement of the three cars could not be made.
The normal practice of the employees assigned to this work crew for leaving this cut of cars unattended was to have full air brakes applied and the only available hand brake applied. The cut of cars was reported as being secured, with only one hand brake applied and a partial application of air brakes.
Several hours later, the cut of cars was reported at a location on the main track approximately 3.4 miles east of its stored location. Railway personnel determined that the cars had rolled uncontrolled from their location in the yard (track EE16), over the derail installation at the east end of Smiths Falls Yard, and onto the main track. The derail had been set in its derailing position. The cars travelled on a slight ascending grade and ran through the main-track switch before passing a wayside monitoring device,Footnote 2 located just east of the main-track switch, which indicated that the cut of cars was travelling at 7.5 mph as it passed this location.
CPR's investigation into this occurrence determined that the cars may have proceeded over the derail at 9 mph. CPR's Standard Practice Circular (SPC) 22 recommends the use of a wheel crowder with the sliding derail if the anticipated speed of an uncontrolled movement is between 9 and 15 mph.
Modifications to the rail cars
Post-incident examination of the rail cars revealed that two of the original three operating hand brakes had been made inoperative by a custom modification. The two areas between the three rail cars had been covered by steel plates to enable continuous loading of ties for the length of the three coupled rail cars (see Photo 2).
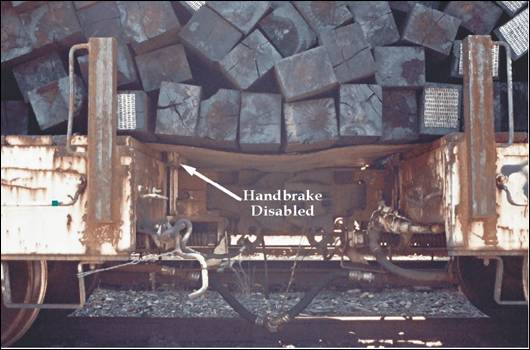
Because this type of rail car is equipped with a stem-type hand brake, the rail car modifications, implemented by the Engineering Services group, resulted in the disabling of two of the three hand brakes. CPR's Equipment Engineering group was not involved in the custom modification, and mechanical personnel had not inspected nor certified the rail cars after they were modified.
Canadian Pacific Railway's instructions for securing cars
CPR's General Operating Instructions Hand Brake Policy prescribes that "more than two cars ALWAYS require at least TWO handbrakes." It also prescribes that the hand brake effectiveness be tested to ensure that it is sufficient to prevent that cut of cars from moving. The Hand Brake Application Procedures prescribe that the hand brake be applied with the air brake released or the brake cylinder bled off.
CPR Timetable 71, Winchester Subdivision Footnotes, Item 12.3, prescribes that a minimum of three operative hand brakes be applied to a cut of cars when it is left unattended at the east end of Smiths Falls Yard.
Training of engineering services personnel for handling rolling stock
At CPR, a training course on handling rolling stock is delivered to Engineering Services employees who are required to handle rail cars using track machines such as the Brandt hi-rail truck. The purpose of this course is to prepare employees to handle rail cars in an Engineering Services work environment. The course prescribes the operating requirements with respect to applying hand brakes. The employees involved in this occurrence had taken the course.
The derail installation
The derail installed at the east end of Smiths Falls Yard was a No. 6 size. As specified in CPR Plan No. T-10-49-3, a No. 6 derail is to be used for a rail weight of 85 pounds. At Smiths Falls Yard, the track consists of 115-pound RE rail. For this size of rail, the Plan suggests a No. 7 derail. During post-incident examination, a similar No. 6 derail at a second location in Smiths Falls Yard was also found.
According to CPR's SPC 22, derails are to be sized by measuring the vertical distance in inches (that is rounded off to the nearest inch) from the top of the rail to the top of the surface on which the derail will be attached. This distance will be affected by the vertical wear of the rail, tie plate thickness, adzing under the tie or the derail, and whether shims have been used.
At Smiths Falls Yard, the rail had been upgraded from 85 pounds to 115 pounds without implementing the corresponding change in derail size. The date of the track upgrade and the date of the derail installations are not known.
During the course of the investigation, it was revealed that CPR Plan No. T-10-49-3 was not readily available as a reference and guidance document to the track forces at Smiths Falls. While the Plan should normally have been kept at the track maintenance forces (TMF) offices, it had been stored at another office at the opposite side of the yard. In addition, several of the employees responsible for adherence to the Plan were not aware of its requirements.
Laboratory Analysis of the Derail
The occurrence derail (see Photo 3) was sent to TSB's Engineering Laboratory for examination (LP 071/2007). The laboratory examination confirmed the following:
- The derail had been in the derailing position when the cut of cars passed over it.
- The sliding portion of the derail had dislodged from its functional location inside the derail casing.
- The derail casing had the end of one hold-down shelf broken away (refer to label "C" in Photo 3). This was old damage that had been painted over.
- The other hold-down shelf was bent with a broken weld (refer to label "D" in Photo 3). This was recent damage, likely from this incident.
- The crossties that supported the derail were not sound. Two of the securing spikesFootnote 3 were missing (refer to positions indicated in Photo 3 as "A" and "B").
- A cross-elevation of 11/16 inch was measured at the location of the derail, with the derail installed on the higher rail.

Additional observations from the laboratory analysis include those of the other No. 6 derail installed at Smiths Falls Yard. At this derail installation, the crossties were split at some spike locations and the fasteners were not fully seated. The derail box was not lying flat on the ties. There was a gap under the toe of the derail when it was set in the derailing position and the up and overlock was not fully engaged.
Annual yard inspection
In April 2007, CPR had conducted an annual yard inspection at Smiths Falls Yard. During this inspection, no defects were noted for the derail installation at the east end of Smiths Falls Yard. However, it was noted that the ties at the occurrence location were old and that the spike holes were deteriorated (see Photo 4). In addition, the inspection noted that the crossties at this location should be replaced. The crossties had not been replaced before the occurrence.

Regulatory requirements and regulatory inspections at Smiths Falls Yard
The Railway Track Safety Rules (TSR), as approved by Transport Canada, prescribe the minimum safety requirements for railway track that is part of the general system of transportation. In the TSR, there are two defect codes related to derails: T.E.2.3 (Improper derail size) and T.E.2.4 (Improperly installed derail).
Transport Canada inspectors had conducted yard inspections at Smiths Falls Yard in October 2002 and August 2003. During these inspections, no derail deficiencies had been noted.
Analysis
When unattended cars are not properly secured, railway employees, the general public and the environment are exposed to the potential consequences of an uncontrolled movement. In many rail yards, the final safety defence against an uncontrolled movement is the derail installation. When used properly, the derail will protect the main track from runaway cars. In this occurrence, the last line of defence failed to derail the uncontrolled movement.
The analysis will focus on the securement of unattended rail cars, modifications to equipment by non-equipment personnel, and the installation and inspection of derails.
The accident
The runaway rolling stock incident occurred when a three-car consist was not adequately secured. With only one hand brake applied and a partial application of air brakes, the cut of cars rolled away from its parked location. The cut of cars travelled over the derail installation at the east end of Smiths Falls Yard without derailing and entered the main track. The derail failed to function as intended because it was the wrong size and had not been properly installed and maintained.
In addition, examination of the cut of cars revealed that two of the three stem-type hand brakes had been made inoperative by a prior custom modification by non-equipment personnel. The two areas between the three rail cars had been covered with steel plates to enable continuous loading of ties for the entire length of the three coupled cars. The single remaining hand brake was designed to apply the brakes on one truck only.
Safe securement of this three-car consist had been dependent on using both the single hand brake and a full application of air brakes, which was an adaptive behaviour made as a result of the ineffective single hand brake. However, with the air system failure on the Brandt hi-rail truck, there was inadequate air supply to fully apply the brake system on the rail cars. The failure of the air system on the Brandt hi-rail truck also prevented the testing of the securement of the three cars. With the air in the brake system depleted and only one hand brake applied, the brakes were insufficient to hold the cut of cars, leading to the uncontrolled movement.
Modification to equipment by non-equipment personnel
The flat cars had steel sheeting bridging the two areas between the cars to facilitate the handling of a larger load of ties continuously over the three cars. This modification, implemented by the railway's Engineering Services group, resulted in covering over the hand brake wheel located on the end of and between the cars. With this modification, two of the three original hand brakes were rendered inoperative. When custom modifications affecting rail car braking systems are performed without involving the railway's Equipment Engineering group, the adequacy of the braking systems may be compromised, leading to an increased risk of uncontrolled movements.
Installation and maintenance of derails
The derails installed at Smiths Falls Yard were incorrectly sized and were anchored to deteriorated ties using only six of the available eight fastener holes. In this state, the derail's ability to function as intended was compromised because the impact forces from the uncontrolled movement pulled the derail from the ties. Before this occurrence, the ties at the derail installation had been identified as requiring renewal. However, this maintenance had not been completed.
A cross elevation of 11/16 inch was measured with the higher rail being that with the derail. This would tend to crowd the wheels toward the opposite low rail. Sound engineering practice suggests that the derail be on the lower rail.
Engineering Services personnel involved in inspecting the derails were not sufficiently aware of the technical requirements of derail installation to identify the incorrect size. Although SPC 22 was in the reference library for these employees, CPR Plan No. T-10-49-3, the detailed technical drawing, was not readily available. Without adequate knowledge of the technical requirements for derail installations or having reference documents immediately available, there is an increased risk that incorrectly installed derails and inadequately maintained derails will not be identified during yard inspections.
Findings
Findings as to causes and contributing factors
- The rolling stock ran away uncontrolled because the three-car consist was left unattended with only one hand brake and a partial application of air brakes.
- Only one hand brake remained operative in this cut of cars after a custom modification had been performed.
- The failure of the air system on the Brandt hi-rail truck prevented the testing of the securement of the cut of cars prior to it being left unattended.
- When the uncontrolled movement reached the derail installation at the east end of Smiths Falls Yard, the derail failed to function because it was the wrong size and had not been properly installed and maintained.
Findings as to risk
- When custom modifications affecting rail car braking systems are performed without involving the railway's Equipment Engineering group, the adequacy of the braking systems may be compromised, leading to an increased risk of uncontrolled movements.
- Without adequate knowledge of the technical requirements for derail installations or having reference documents immediately available, there is a risk that incorrectly installed derails and inadequately maintained derails will not be identified during yard inspections.
Safety action taken
Following this occurrence, the TSB sent Rail Safety Advisory (RSA) 07/07 to Transport Canada (TC) indicating that it might wish to review the railway industry's procedures for verifying the safety of rolling stock when it is modified for work service.
In addition, the TSB issued Rail Safety Information letter (RSI) 13/07 informing TC of the inadequate maintenance of derails at Smiths Falls Yard. The TSB also issued RSI 16/07 informing TC of the incorrectly sized derails at Smiths Falls Yard and the possibility that this situation could be present at other locations.
In response to this occurrence and TSB's RSA and RSIs, Canadian Pacific Railway (CPR) initiated the following safety action:
- Investigation of safety related occurrence protocol response
CPR initiated its Investigation of Safety Related Occurrence Protocol (ISROP) process and appointed a five-member team which conducted a re-enactment of the events. The team concluded that there were not sufficient hand brakes on the cars to secure them and that the employees involved did not have sufficient training from their "Handling Rolling Stock" training program to recognize that deficiency. - Educational bulletins
On 12 July 2007, a Safety Flash was issued to CPR employees describing this uncontrolled movement incident and the corrective measures taken.
On 28 September 2007, Safety Broadcast ES024_07 was issued as a Safety Alert to CPR's Engineering Services personnel describing the incident and the related derail deficiencies. The Safety Alert requested employees to review the requirements of applicable Standard Practice Circular (SPC) 22 with special attention to the sections on selection and sizing of derails; tie requirements under derails; general site requirements at derail locations; and maintenance and inspection of derails. - Employee training
CPR's ISROP process concluded that the Engineering Services group's "Handling Rolling Stock" training course did not adequately prepare the employees to understand the procedures, rules and safety practices concerning air brakes on rolling stock. CPR added a new hands-on training segment to the course to improve the employees' understanding of air brakes. - Use of rail cars by engineering services
CPR removed the three 80-ton steel deck flat cars (SOO 5002, SOO 5010, and SOO 5017) from this service and replaced them with rail cars having side sill–mounted hand brake levers that applied the brake shoes to all wheels. In addition, CPR issued internal instructions to its Engineering Services group that modifications to car equipment must first be approved by its Equipment Engineering group. - System-wide review of derails
CPR conducted a system-wide review of derail locations to verify the safe condition of all derails, including correct size and proper securement of derails. This system wide review and the appropriate corrective actions were completed by January 2008. CPR reported that corrective action was taken at 26 derail installations. At many of these installations, the condition of hold down fastenings was improved. In addition, at 10 of these installations, the derail was upgraded to meet the speed and gradient specifications as outlined in SPC 22. - Derails on private tracks
CPR inspected private tracks owned by its customers which had derails protecting CPR's tracks. Subsequent to these inspections, letters were sent to 10 customers with private sidings requiring them to address identified deficiencies. - Derails at Smiths Falls Yard
Subsequent to this occurrence, CPR changed out the two derails at Smiths Falls Yard. A switch point derail was installed at the occurrence location. At the second location, the previous No. 6 derail was replaced with a No. 8 derail. - Reference documents at Smiths Falls
CPR plans and related reference documents are now stored at the track maintenance forces (TMF) offices and are available to all employees.
In response to this occurrence, TC initiated the following safety action:
- Meeting with Canadian Pacific Railway
TC met with CPR. As a result, CPR issued internal instructions to its engineering forces that modifications to car equipment must first be approved by its Equipment Engineering group. - Conducting audits
During the months of December 2007 and January 2008, TC inspected flat cars at Guelph Junction and at CPR's Toronto Yard. As a result, several cars were shopped for hand brakes and other safety appliance defects. TC later verified with CPR that these cars had new hand brakes applied to them and have had their brakes adjusted and tested.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .