Employee Fatality
Canadian Pacific Railway
Yard assignment FS23
Mile 46.9, Adirondack Subdivision
St-Luc Yard
Montréal, Quebec
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 08 November 2017, Canadian Pacific Railway yard assignment FS23 was performing switching operations in St-Luc Yard at Mile 46.9 of the Canadian Pacific Railway Adirondack Subdivision, in Montréal, Quebec. At about 0600 Eastern Standard Time, while reversing southward in the dark at approximately 10 mph, the yard assignment struck and fatally injured the yard helper.
1.0 Factual information
On 08 November 2017, Canadian Pacific Railway (CP) yard assignment FS23 (the assignment) was performing switching operations in St-Luc Yard at Mile 46.9 of CP's Adirondack Subdivision, in Montréal, Quebec (Figure 1).
The yard assignment consisted of a crew (a locomotive engineer, a yard foreman, and a yard helper) and a locomotive.
During typical switching operations in St-Luc Yard, the locomotive engineer remains in the locomotive while the yard foreman and yard helper are on the ground. The yard foreman and yard helper perform tasks such as lining switches, coupling and uncoupling cars, and applying hand brakes. Based on the instructions given by the yard foreman or yard helper, the locomotive engineer operates the locomotive forward and backward.
The trainmaster, positioned in the yard office tower in St-Luc Yard, prepares switch lists for the crews and supervises the switching operations. A typical switch list includes a list of cars to be picked up from a given track (in sequential order) and the destination track for each car.
1.1 The accident
On 07 November 2017 at 2230,Footnote 1 the assignment crew (the crew) began its tour of duty at St-Luc Yard. The crew was using 2 locomotives (CP 3061 and CP 4407) to switch cars from multiple tracks throughout the shift. The 3 crew members were qualified for their respective positions, met fitness and rest standards, and were familiar with the yard.
At approximately 0530 on 08 November 2017, the crew coupled the 2 locomotives to a cut of 12 cars in track DT29 and began switching the cars in accordance with the switch list (Table 1).
| Car No. | Equipment identification number | Empty (E) / Loaded (L) | Destination track |
|---|---|---|---|
| N/A | CP 3061 | Locomotive | S/O |
| N/A | CP 4407 | Locomotive | S/O |
| 12 | TILX 305560 | E | DT22 |
| 11 | CP 214449 | E | DT24 |
| 10 | CP 215592 | E | DT24 |
| 9 | TILX 650086 | E | DT23 |
| 8 | IANR 624466 | L | DT20 |
| 7 | SOO 601410 | E | DT03 |
| 6 | CP 215379 | E | DT24 |
| 5 | CP 214036 | E | DT24 |
| 4 | NOKL 570177 | L | DT20 |
| 3 | INEX 145 | L | DT04 |
| 2 | UTLX 958932 | L | DT07 |
| 1 | SOO 601534 | E | DT24 |
The yard assignment weighed approximately 1100 tons and measured about 900 feet in length. The yard foreman and yard helper were performing their various duties on the ground while the locomotive engineer was operating locomotive CP 3061, which was facing north. From this position, the locomotive engineer had a limited view of the yard foreman and yard helper and relied on radio communications for movement instructions.
The following car movements were performed by the yard assignment:
- The 1st car (SOO 601534) was placed and secured with its hand brake onto its assigned destination track (DT24).
- The 2nd and 3rd cars (UTLX 958932 and INEX 145) were temporarily placed and secured on the West Loop.Footnote 2
- The 4th car (NOKL 570177) was placed onto its assigned destination track (DT20).
See Table 2 for a more detailed sequence of events.
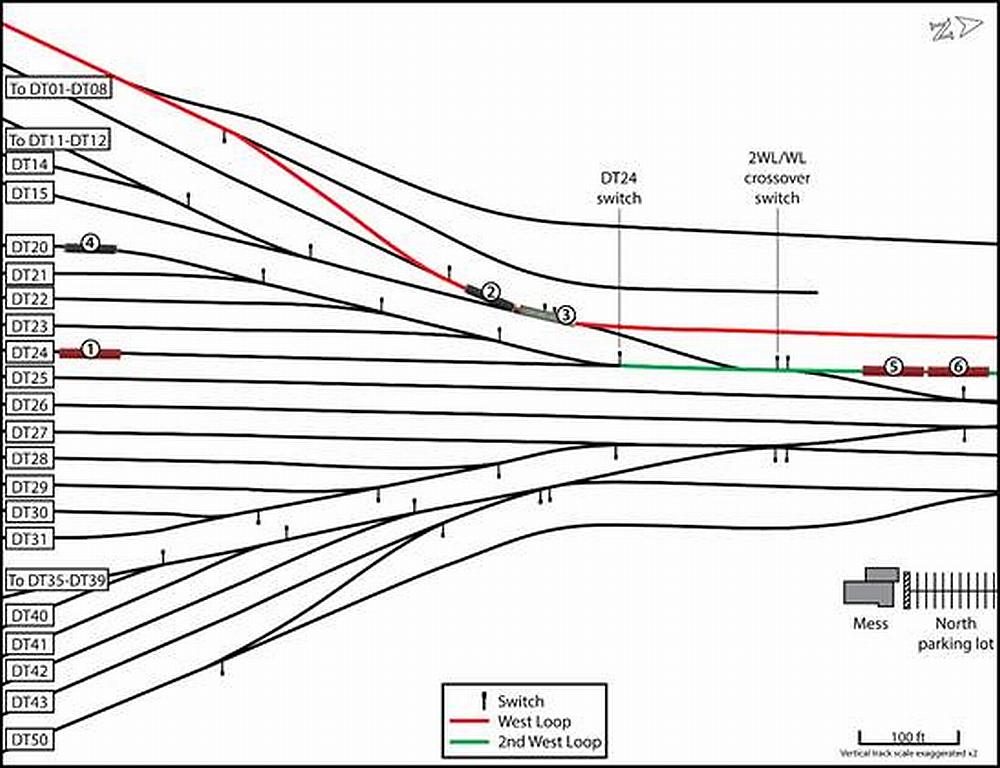
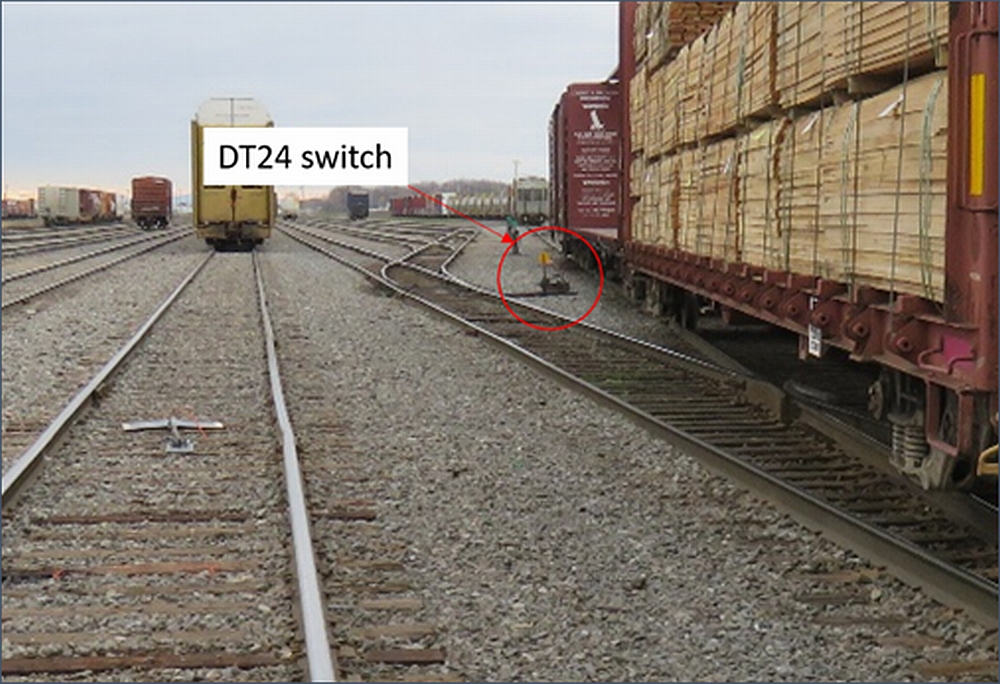
While the yard foreman was shoving the 4th car onto track DT20, the yard helper, who was posted near the switch for the crossover between the 2nd West Loop and the West Loop (the 2WL/WL crossover), left his location without informing his crew, headed east, and entered the mess buildingFootnote 3 approximately 155 feet away (Figure 2).
Shortly thereafter, the yard helper exited the mess building and returned to the 2WL/WL crossover switch. At that time, the yard assignment had completed the placement and securement of the 4th car (NOKL 570177) onto track DT20, and was proceeding northward out of that track on the 2nd West Loop.
In preparation for the next movement, where the 5th and 6th cars (CP 214036 and CP 215379) would be placed onto track DT24, the yard foreman headed toward that track while the yard helper instructed the locomotive engineer by radio to stop the yard assignment with the last car positioned approximately 100 feet north of the 2WL/WL crossover switch.
The yard helper placed the 2WL/WL crossover switch in reverse position (displaying a yellow target), then walked to the DT24 switch and also placed it in reverse position (displaying a yellow target).Footnote 4
The yard helper confirmed to the locomotive engineer that the yard assignment was lined for track DT24. He then instructed the locomotive engineer to move the assignment south by 15 car lengths.
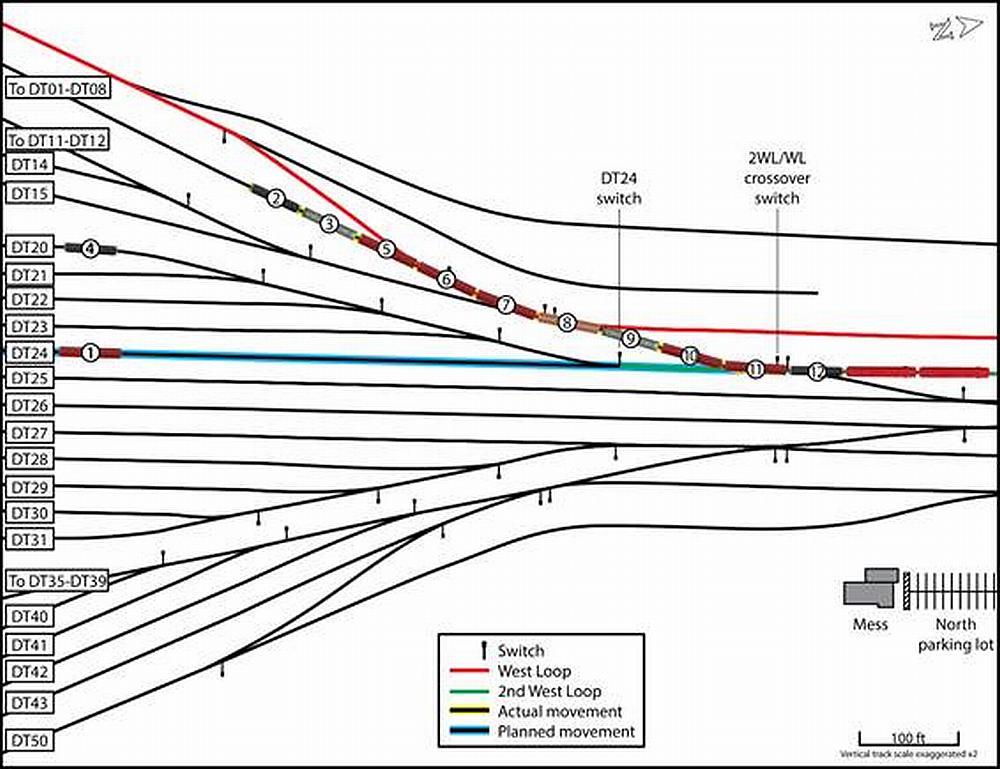
However, at the 2WL/WL crossover switch, the yard assignment diverted toward the West Loop and the 2 cars (INEX 145 and UTLX 958932) that had temporarily been placed there earlier. At approximately 0600, after having travelled 315 feet and reaching a speed of 10 mph, the yard assignment collided with car INEX 145. The locomotive engineer immediately applied the brakes to stop the movement (Figure 3).
Radio communication was established between the locomotive engineer and yard foreman. They determined that the yard assignment had not been routed toward track DT24 as intended. After repeated attempts to contact the yard helper by radio, the yard foreman walked up and began inspecting the yard assignment.
The yard helper was located under car CP 215379, having been struck and fatally injured by the yard assignment. The sequence of events (Table 2) was determined based on the review of the available information, including radio communication records, locomotive event recorder data, surveillance video recordings, and interviews.
| Time* | Event |
|---|---|
| 0530 (approx.) | The crew coupled the locomotives to the cars on track DT29, and the yard helper walked to the southern extremity of the cut of cars to release the hand brakes. |
| 0537:39 | The yard helper said that the rotation of cars was not the same as in the switch list, and that the yard foreman should verify this. |
| 0537:59 | The yard helper instructed the locomotive engineer to pull the yard assignment forward across the diamond, toward the 2nd West Loop. |
| 0541:38 | The yard helper, who was riding car SOO 601534, instructed the locomotive engineer to stop the yard assignment north of the crossover between track DT25 and the 2nd West Loop. |
| 0542 (approx.) | The yard foreman walked toward track DT24. |
| Between 0544:10 and approx. 0548 | The following steps were taken to place car SOO 601534 on track DT24:
|
| 0548:11 | The yard foreman secured car SOO 601534 on track DT24 and uncoupled it from the yard assignment. |
| 0548:45 | The yard assignment proceeded forward (north) toward the 2WL/WL crossover to prepare for the next movement. The yard foreman rode up with the yard assignment to perform a job briefing. |
| 0550:47 | The yard helper instructed the yard assignment to stop north of the 2WL/WL crossover. |
| 0551 (approx.) | The following steps were taken to temporarily place cars UTLX 958932 and INEX 145 on the West Loop, south of the 2WL/WL crossover:
|
| 0552:30 | The yard foreman secured cars UTLX 958932 and INEX 145 on the West Loop, just south of the 2WL/WL crossover, and uncoupled them from the yard assignment. |
| 0552:43 | The crew began to take the following steps to place car NOKL 570177 onto track DT20:
|
| 0554:03 | The yard assignment began reversing toward track DT20. |
| 0554:30 (approx.) | The yard helper momentarily entered the mess building. |
| 0556:41 | The yard foreman secured car NOKL 570177 onto track DT20 and uncoupled it from the yard assignment. |
| 0556:55 | The yard assignment began pulling out of track DT20. |
| 0557 (approx. based on available information) | While the yard assignment was pulling out of track DT20 and the locomotives were approaching the 2WL/WL crossover switch, the yard helper exited the mess building, had a brief conversation with a fellow employee in the north parking lot, and headed toward the 2WL/WL crossover switch. |
| 0557:40 | The yard helper informed the locomotive engineer that there were 8 car lengths left to clear the 2WL/WL crossover switch. |
| 0558:31 | The yard helper instructed the locomotive engineer to stop the yard assignment north of the 2WL/WL crossover switch. |
| Between approx. 0558:31 and 0600:20 | The yard foreman walked toward track DT24 to prepare for the next movement. The yard assignment stopped with the last car (CP 214036) approximately 100 feet north of the 2WL/WL crossover switch. Both the 2WL/WL crossover switch and the DT24 switch were in normal position (i.e., displaying a green target). The yard helper placed the 2WL/WL crossover switch in reverse position (i.e., displaying a yellow target). The yard helper placed the DT24 switch in reverse position (i.e., displaying a yellow target). |
| 0600:20 | The yard helper confirmed that the yard assignment was lined for track DT24 and instructed the locomotive engineer to start backing up 15 car lengths. The yard assignment reversed and reached a speed of 10 mph. |
| 0600:51 | After travelling approximately 315 feet, the yard assignment collided with the cars that had been left on the 2WL/WL crossover track. |
* Events that could not be verified with respect to time and/or exact circumstances are identified as “approx.” or “approx. based on available information.”
At the time of the accident, no other switching assignment was on duty at St-Luc Yard and no other track maintenance or mechanical employees were working near the area.
The temperature was approximately 1 °C, there was a southeasterly wind of 10 km/h, and sunrise was at 0643. On the night of the occurrence, there was no precipitation and no snow on the ground.
1.2 St-Luc diamond
The accident occurred in a section of the yard referred to as the “diamond.” The diamond is approximately 1000 feet long and has 6 parallel tracks and multiple crossovers, 2 of which are intersecting. The diamond is the intermediary between the north end of the departure yard and the northern part of St-Luc Yard. Most of the switching at St-Luc Yard is performed at this location. The departure yard consists of approximately 40 tracks of varying lengths used for switching activities and storing cars (Figure 4).
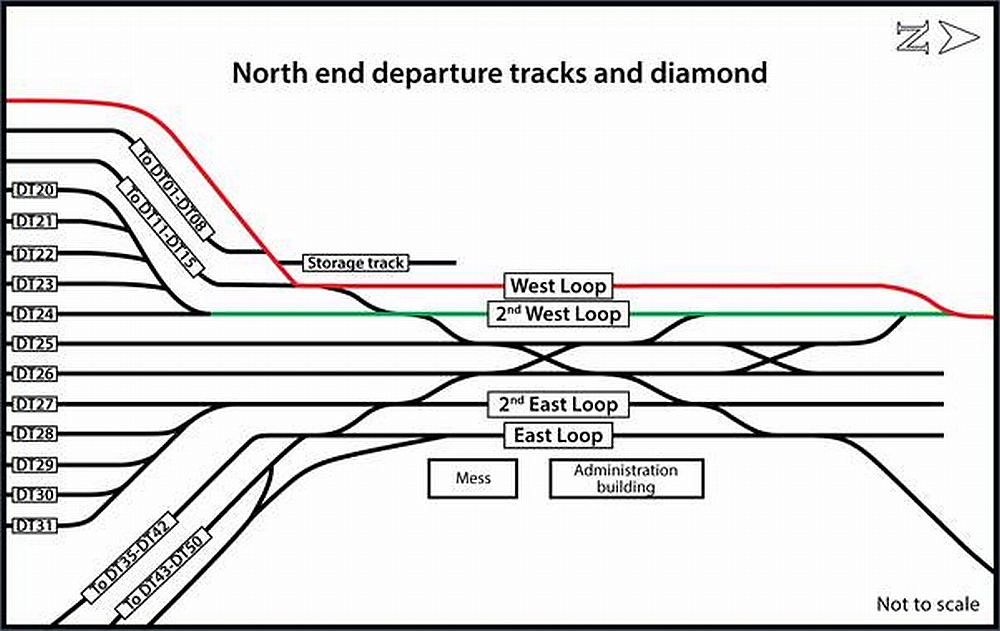
Tracks DT01 to DT24 are located on the west side of the yard and are accessible from the 2nd West Loop, while tracks DT27 to DT50 are on the east side of the yard and are accessible from the 2nd East Loop. Tracks DT25 and DT26 divide the yard into its east and west sides and are accessible from the intersecting crossovers. The switches at the north end of the departure tracks and the switches on the diamond are hand-operated.
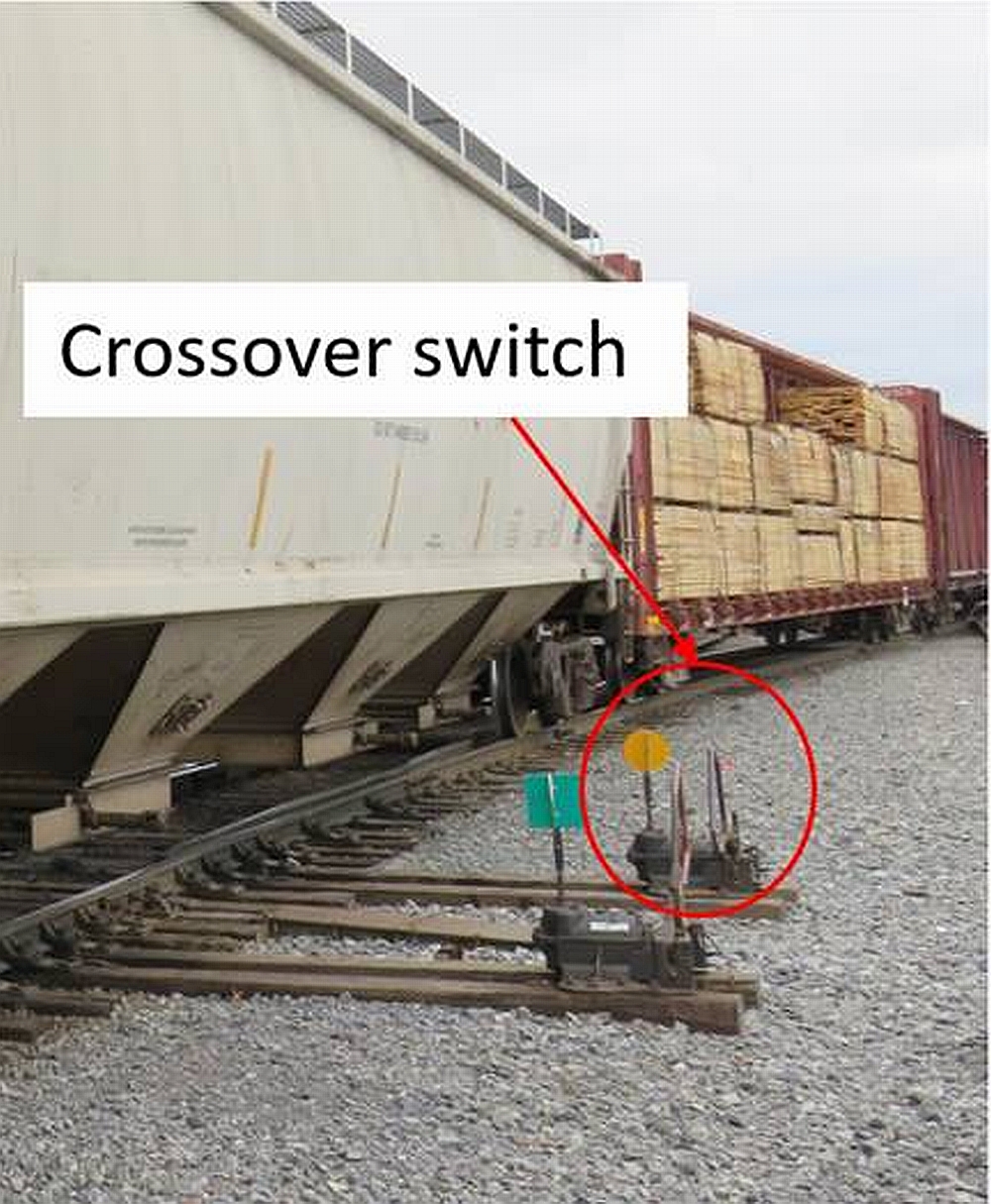
At the southern extremity of the 2nd West Loop, a crossover connects the 2nd West Loop to the West Loop (2WL/WL crossover). When the 2WL/WL crossover switch is in the reverse position (displaying a yellow target) (Figure 5), a yard assignment travelling southward is diverted onto the crossover and toward the West Loop (adjacent track). When the 2WL/WL crossover switch is in the normal position (displaying a green target), a yard assignment travelling southward is directed toward the lead of tracks DT20 to DT24.
The lead of tracks DT20 to DT24 has 4 switches, the first being for track DT24. When the switch for one of these tracks is in the reverse position (displaying a yellow target), a yard assignment is lined for that particular track.
To place cars on destination track DT24, the yard assignment would have to be placed on the 2nd West Loop, with the last car positioned north of the DT24 switch. The DT24 switch would then have to be placed in the reverse position to align the yard assignment toward track DT24.
1.3 Site examination
Following the accident, the 2WL/WL crossover switch was found in the reverse position, lined for the West Loop. No switch identification markings were present. The switch handle was secured with the foot lock, and its keeper was in the keeper hole. The switch points showed no signs of damage. The switch was inspected and tested; no exceptions were noted. The DT24 switch was found in the reverse position, lined for track DT24 (Figure 6).
The side of the DT24 switch had a non-reflective marking indicating the switch number.
The 2 locomotives were on the 2nd West Loop, adjacent to the yard office. Coupled to the locomotives were 10 cars, none of which were damaged or derailed. The brake pipe between locomotive CP 4407 and car TILX 305560 was not connected. The cars occupied part of the 2nd West Loop, the crossover toward the West Loop, and a portion of the West Loop. The hand brake on the last car (UTLX 958932) was found applied.
The yard helper's safety glasses, work gloves, switch list, and lantern were found on the west side of the yard assignment, adjacent to the DT24 switch. The lantern used by the yard helper was damaged during the accident, and examination of its functionality could not be performed.
1.4 Track information
St-Luc Yard is located at Mile 46.9 of CP's Adirondack Subdivision and is CP's major yard in the Montréal area. It integrates switching and marshalling of freight trains, some intermodal operations, repair shops, and a car compound.
St-Luc Yard is configured as follows:
- The tracks are primarily oriented in the north–south direction.
- The yard contains 44 miles of track and is equipped with about 260 switches.
- The yard has a maximum capacity of 1500 cars.
About 14 trains arrive and depart daily, transporting approximately 259 515 cars per year. Train movements within the yard are governed by Rule 105 of the Canadian Rail Operating Rules (CROR) and are limited to a maximum speed of 15 mph.
Since its construction, St-Luc Yard has undergone various modifications affecting the yard's operations. Among these changes was the conversion of the hump yard to a classification yard for flat switching. This change consisted of removing the automation associated with a hump yard,Footnote 5 reducing the grade used for switching, and removing half of the hump yard tracks. Following these modifications, the St-Luc classification yard was used primarily for switching blocks of cars with multiple destinations and requiring multiple switching operations. Blocks of cars with few destinations and requiring a small number of switching operations were moved directly to the departure tracks through the diamond.
Flat switching continued at the classification yard until late 2012, at which time the classification yard was closed. Switching at St-Luc Yard was then moved primarily to the diamond area.
1.5 Crew information
The locomotive engineer had 31 years of railway experience, which included 28 years as a locomotive engineer. The yard foreman was qualified as a yard helper, yard foreman, and locomotive engineer. He began working with the railway in 2004 and completed locomotive engineer training in 2010. The yard helper began working for the railway in 2011 and completed yard helper and yard foreman training in 2012.
Switching operations in CP's Montréal service area (MSA) work on a 24/7 schedule. The work is accomplished by means of regular bulletined assignments and spare employees who work on call and fill vacancies. Each week, employees in the MSA (locomotive engineers, yard foremen, and yard helpers) bid on and are placed on assignments (including spare lists) based on their preferences and seniority. The occurrence locomotive engineer, yard foreman, and yard helper were each familiar with the yard layout and the switching operations performed at St-Luc Yard.
On the night of the accident, the assignment's regular yard foreman had been asked to work as a locomotive engineer on a different assignment, creating a vacancy in the yard foreman position. When an assignment's yard foreman is absent, the assignment's yard helper is promoted to yard foreman and the yard helper position is filled using an employee from the yard's spare list. Because there were no employees available on the yard's spare list, the yard helper requested yard assignment FS23 at St-Luc Yard in lieu of his regular assignment that started at 2359 at another CP terminal within the Montréal service area. The yard helper received the call to work at St-Luc Yard on the assignment at approximately 2000 on 07 November 2017.
1.5.1 Work/rest history of yard helper
The yard helper had worked 7 of the previous 9 nights, typically with an on-duty time between 2230 and 2359 and finishing work between 0630 and 1010. The yard helper typically had a nap before going to work at night and normally slept well. His last shift at St-Luc Yard had been on 01 November 2017 at 2230 on assignment FS23. His last period of more than 24 hours of rest had started on the morning of 05 November 2017.
The yard helper's work and rest history is provided in Appendix A. The yard helper was working his 2nd consecutive night shift at the time of the accident. Following a night off work, the yard helper had reported for work at 2359 on 06 November 2017, completing his shift at 0810 on the morning of 07 November. On the night of the accident, the yard helper reported to the mess building for his shift at approximately 2200. The yard helper had 14 hours off duty between shifts during which he had the opportunity to sleep before receiving the call for this work assignment.
The yard helper had been working predominantly during night-time hours in the period leading up to the accident, leaving sleep opportunities during the day. It was not possible to obtain a full sleep history for the yard helper. However, based on cell phone records, periods where the yard helper was active and periods where the yard helper could have obtained sleep were identified. The yard helper had the opportunity for full nighttime sleep on the night of 05 to 06 November 2017 and 2 opportunities for afternoon naps on 06 November 2017 (i.e., one 4-hour period early in the afternoon and a 1-hour period just prior to being called in for the evening shift). It could not be determined whether the yard helper had used the available opportunities to sleep.
On 07 November, the yard helper stopped at the St-Luc Yard office after his shift was over at 0810 to submit paperwork related to the reimbursement of personal protective equipment purchases. The yard helper was also at the St-Luc Yard office around noon, when he was off duty. As a result, he had the opportunity for 3 hours of sleep before receiving his call for the work assignment in St-Luc Yard for that night. Thus, the yard helper could have had a maximum of only 4 hours of sleep out of the previous 38 hoursFootnote 6 prior to the accident.
1.5.2 Employee alertness
Fatigue has the potential to degrade human performance and must be managed effectively in 24/7 transportation operations. To identify the likelihood of fatigue being present at the time of an occurrence, the TSB examines 6 known fatigue risk factors: acute sleep disruption, chronic sleep disruption, continuous wakefulness, circadian rhythm effects, sleep disorders, and medical conditions that have the potential to disrupt sleep.
The human body has a circadian (daily) rhythm that controls the sleep-wake cycle. This cycle is “set” primarily by visual cues of light and darkness, and is synchronized to the 24-hour day. People who regularly work at night can have difficulty initiating and maintaining sleep on subsequent nights, and the sleep that is obtained will tend to be less restorative than for a normal nighttime sleeper.Footnote 7
The TSB used the Fatigue Avoidance Scheduling ToolFootnote 8 software to assess the yard helper's work schedule and rest opportunities in the days preceding the occurrence. This assessment was used to validate the effects of the yard helper's work/rest history on his overall performance at the time of the occurrence. It was estimated that the quantity and quality of sleep obtained in the preceding days likely would have made the yard helper less attentive to his environment.
1.6 Canadian Rail Operating Rules
CROR General Rule C sets out general standards for vigilance when working around trains. It states:
Employees must:
- be vigilant to avoid the risk of injury to themselves or others;
- expect a movement, track unit or equipment to move at any time, on any track, in either direction; […]Footnote 9
When operating switches, the following rule applies:
104. HAND OPERATED SWITCHES
General
- Operation of Switches - semi-automatic, spring, dual control or auto-normal switches operated by hand are considered hand operated switches, and all rules governing hand operated switches apply.
- Except while being turned, each switch must be secured with an approved device. When a switch has been turned, the points must be examined and the target, reflector or light, if any, observed to ensure that the switch is properly lined for the route to be used.Footnote 10
When radio communications are used to control switching, the following rule applies:
123.2 SWITCHING BY RADIO
When radio is used to control switching, and after positive identification has been established, the following procedures are required:
[…]
- when the movement has travelled one-half the distance required by the last instruction and no further communication is received, the movement must stop;
[…]
- when car lengths are used to communicate distance, unless otherwise arranged, the distance referred to is 50 feet per car length.Footnote 11
Before the accident, the locomotive engineer received confirmation by radio that the yard assignment was lined for track DT24. He was instructed to back up a distance of 15 car lengths (approximately 750 feet). According to CROR Rule 123.2, no radio communication was required until the yard assignment had travelled approximately 375 feet.
1.7 Switch locations
Most flat switching yards are designed so that the track laddersFootnote 12 (Figure 7) minimize the distance to clearance points and provide maximum yard capacity.

The American Railway Engineering and Maintenance-of-Way Association (AREMA) Manual for Railway Engineering (the AREMA Manual) includes guidance for the design, construction, and operation of yards and terminals used in railway service.Footnote 13 According to the AREMA Manual,
- Switch stands for hand-operated switches should be located on the outside of the ladder. This would allow employees to move from one switch to another and operate switches without having to cross or stand foul of any track.
- Inside switch stands should be used only when power switching is provided.
- Walking surfaces should consist of yard ballast suitable for footing and drainage.Footnote 14
At St-Luc Yard, most of the switches at the north end of the departure yard are located on the outside of the ladder. However, at the northern extremity of the departure yard, the ladders for tracks DT20-DT24, DT11-DT15, and DT01-DT08 are in close proximity to each other and are bordered by the West Loop (Figure 2). The close proximity of the tracks results in reduced clearance around some switches, which does not allow an employee to handle switches without moving foul of an adjacent track. For example, the DT24 switch is positioned approximately 2½ feet from the adjacent track (Figure 8).

Routine exposure to workplace hazards without negative consequences can desensitize an employee to the risk associated with those hazards.Footnote 15
1.8 Switch targets
Switch targets are used to indicate the route for which the switch has been lined. The CROR require that non–main-track hand-operated switches display targets as follows:
- Green switch targets are displayed when the non-main-track switch is in normal position.
- Yellow switch targets are displayed when the non-main-track switch is in the reverse position.
- Switch targets may be any shape, but must not be diamond shape.
The switch targets at St-Luc Yard met these requirements.
Many adaptations to switch targets are available to further help operators identify the direction of travel. These targets have been developed to provide additional information to the switch operator. An example is a switch cube direction indicator (Figure 9).

The switch cube direction indicator replaces a traditional switch target with a cube. Each side of the cube has a different colour and has arrows that indicate the resulting direction of the yard assignment based on the switch position. Unlike a traditional switch target, a switch cube direction indicator provides additional visual cues as to the track for which the switch is lined.
The switch targets in Figure 7 also have track identification on the reflective targets themselves. This practice provides the yard foreman or yard helper with another visual cue to more easily see the track for which the switch is lined.
1.8.1 Switch identification errors
About 1 week earlier, a trainmaster had conducted a routine footboard safety meeting with the occurrence yard helper to discuss the importance of ensuring that switches are lined in the intended direction. During this meeting, the yard helper had pointed out that some switches in the yard could not be relied on solely by observing their target colour or the location of the switch arm.Footnote 16 The yard helper had further noted that newcomers to the yard may require additional time to become acquainted with the switches and tracks.
The investigation determined that when any switching errors at St-Luc Yard were reported, local management would likely bring in the employee involved for a statement. A potential outcome from this process was disciplinary action.
Since 1999, the TSB has investigated 7 other occurrences where adverse consequences relating to misaligned switches occurred. These investigations are summarized in Appendix B.
1.9 Changes to switching job tasks
During switching, the tasks of a yard foreman and yard helper include operating switches, coupling and uncoupling cars, applying hand brakes, entraining and detraining moving equipment, riding equipment, and, depending on the yard's configuration, a significant amount of walking.
When the St-Luc classification yard was closed in 2012 and the switching operation was moved to the diamond area in the yard, the potential hazards associated with the switching tasks changed because of the diamond area's track layout.
Table 3 highlights the differences between some of the yard foreman and yard helper switching tasks associated with the St-Luc classification yard versus the diamond area.
| Task | Classification yard | Diamond area |
|---|---|---|
| Release zone* | Dedicated release zone with switching lead and 25 tracks. | No dedicated release zone; section of track north of the crossover switch on the 2nd West Loop used to release cars. |
| Switch positioning | Most of the switches are located on the outside of the tracks, adjacent to a roadway. | The switches are located either on the inside or the outside of the tracks. In some cases, employees are foul of the track while switching. |
| Lighting | On the northern extremity, there are 3 light towers, 1 of which is specifically placed to illuminate the release zone. | The closest light source to this location is next to the East Loop, approximately 90 feet away east of the DT24 switch. |
| Ballast | Yard ballast consisting of smaller grade crushed material. | Mainline railway ballast. |
| Tripping hazards | No other tracks, switches or tripping hazards in the release zone. | There are multiple tripping hazards such as switch stands and overlapping tracks. |
* An area in the yard where cuts of cars are separated from the movement and sent to destination tracks.
In the diamond area, the track is tangent and allows crews to switch between the 3 ladders on the west side of the St-Luc departure yard. On the west side of the diamond, the clearance between the tracks was limited, placing the yard foreman or yard helper foul of adjacent tracks during flat switching operations. When handling the DT24 switch, the yard foreman or yard helper will always be foul of the West Loop crossover track.
1.10 Lighting
The On Board Trains Occupational Health and Safety Regulations (Regulations) contain lighting provisions for operations personnel while working at night in rail yards.
According to the Regulations:
- In areas where employees are engaged in the flagging, switching, and marshalling of rolling stock, the required minimum level of lighting is 50 lux.
- The required minimum level of lighting is to be provided, where reasonably practicable, by a lighting system installed by the employer.
- Where it is not reasonably practicable to provide the required minimum level of lighting by way of a lighting system installed by the employer, employees are to be provided with portable lanterns that give the prescribed levels of lighting.Footnote 17
CP issues handheld lanterns to all yard employees. On the night of the occurrence, both the yard foreman and the yard helper were provided with a handheld lantern equipped with an incandescent signalling bulb and an LED spot bulb housed in a reflector assembly (Figure 10).

When necessary, yard employees use the lantern's signalling bulb and/or LED reflector to illuminate the ground, read switch lists, verify track switch points, and illuminate reflective targets on the switch stands to confirm switch positions.
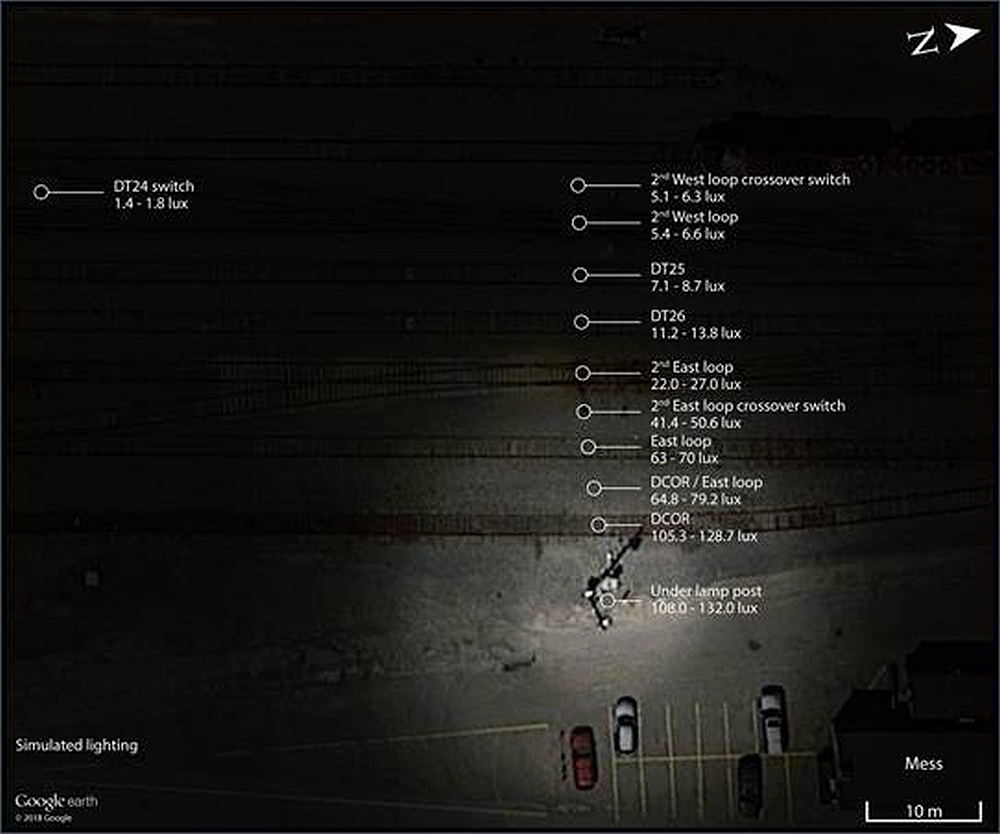
In the diamond area, there was one fixed lamp post located on the east side (east lamp post). The TSB measured the levels of lighting under different conditionsFootnote 18 at various task locations in the yard.Footnote 19 It was determined that with the area's fixed lighting system,
- The general average level of lighting for the area from the east lamp post to the 2WL/WL crossover switch was 48.2 lux.
- The average level of lighting for the 2WL/WL crossover switch task location was 5.7 lux.
- The average level of lighting for the DT24 switch task location was 1.6 lux (Figure 11).
With the use of a portable lantern with only the signalling bulb lit, the average level of lighting at the task locationsFootnote 20 was increased by 4 lux. As a result,
- The average level of lighting for the 2WL/WL crossover switch task location was 9.7 lux.
- The average level of lighting for the DT24 switch task location was 5.6 lux.
When the portable lantern was used with the LED spot bulb lit and aimed at a task location, the level of lighting was over 400 lux, exceeding the prescribed levels at a task location.
When rolling stock or a person was casting a shadow over a task location, the level of lighting at the task location within the shadowed area was consistently between 0 and 3 lux.
Since the change in yard operations in 2012, some employees had verbally expressed concerns to St-Luc Yard management about insufficient levels of lighting on the west side of the diamond and into the 3 ladders. However, there were no records that these concerns were formally or informally raised to the company's health and safety committee, and CP took no action to increase the lighting in St-Luc Yard.
1.11 Developing, maintaining, and regaining situational awareness
Mental models are internal structures that allow individuals to describe, explain, and predict events and situations in their environments.Footnote 21 Effective performance in operational environments requires operators to continually update the mental model of their current situation. Maintaining situational awareness is a 3-stage process in which operators take in information from their environment, understand its significance for the current situation, and project into the future to assist in planning.Footnote 22
The ability to recall information and maintain information in working memory represents a significant potential bottleneck in an individual's ability to maintain situational awareness.Footnote 23 Further, the limitations of working memory can become more acute when faced with normal operational stressors:
Stressors such as anxiety, time pressure, mental workload, uncertainty, noise or vibration, excessive heat or cold, poor lighting, physical fatigue, and working against one's circadian rhythms are unfortunately an unavoidable part of many work environments. These stressors can act to reduce SA [situational awareness] considerably by further reducing an already limited working memory and reducing the efficiency of information gathering. It has been found that people may pay less attention to peripheral information, become more disorganized in scanning information and are more likely to succumb to attentional tunneling when affected by these stressors. People are also more likely to arrive at a decision without taking account of all available information (premature closure).Footnote 24
1.11.1 Mental models during train operations
Mental models are developed based on several factors, including experience, knowledge, perception, and comprehension of external cues available in the work environment. Once a mental model is adopted, it is very resistant to change. For people to change their mental models, the existing model must be superseded by another one, with the new information being sufficiently compelling to result in an update of the mental model. The human working memory has a limited capacity, so not all the cues available in the work environment will be retained. This results in simple and incomplete mental models that are developed internally to understand and make sense of a dynamic and complex work environment.Footnote 25
1.12 Railway Safety Management System Regulations
The 2001 Railway Safety Management System Regulations (2001 SMS Regulations), in effect when the St-Luc classification yard was closed in 2012, required federally regulated railway companies to develop and implement a safety management system (SMS).
Section 2 of the 2001 SMS Regulations stated the following:
2. A railway company shall implement and maintain a safety management system that includes, at a minimum, the following components:
[…]
- a process for
- identifying safety issues and concerns, including those associated with human factors, third-parties and significant changes to railway operations, and
- evaluating and classifying risks by means of a risk assessment
- risk control strategies;
[…]
- consolidated documentation describing the systems for each component of the safety management system.Footnote 26
1.12.1 Canadian Pacific Railway's safety management system
CP's SMS includes a Hazard Prevention Program and a Risk Assessment Policy and Procedure, which are routinely updated and refined to support continuous improvement. With these two programs, hazards can be reported, assessed, and mitigated at any time.
CP's Risk Assessment Policy and Risk Assessment Procedures have evolved since 2012. CP currently requires a risk assessment to be conducted whenever
- A Safety Concern” (i.e., a hazard or condition that may present a direct safety risk to employees, or pose a threat to safe railway operations) is identified through analysis of safety data;
- A proposed change to CP Operations that could:
- introduce a new hazard to the workplace resulting in adverse effects;
- negatively impact or contravene any existing policy, procedure, rule or work practice used to meet regulatory compliance or any CP requirements or standards;
- create or increase a direct safety risk to employees, railway property, property transported by the railway, the public or property adjacent to the railway; and
- require authority by a regulatory agency to implement.Footnote 27
Because CP did not consider the closing of the St-Luc classification yard to be a significant change to railway operations at St-Luc, no risk assessment was performed in 2012.
Since 2015, the TSB has investigated 3 other occurrences in which CP had made changes to its operations. In these occurrences, CP had not considered some of the changes to be “significant,” and therefore no risk assessment was performed (Appendix C).
1.13 Safety culture
A recognized definition of an organization's “safety culture” is “shared values (what is important) and beliefs (how things work) that interact with an organization's structures and control systems to produce behavioural norms (the way we do things around here).”Footnote 28
The safety culture of an organization is the result of individual and group values, attitudes, perceptions, competencies, and patterns of behaviour that determine the commitment to, and the style and proficiency of, an organization's health and safety management system (SMS).
An effective safety culture includes proactive actions to identify and manage operational risk. It is
- an informed culture where people understand the hazards and risks involved in their own operation, and work continuously to identify and overcome threats to safety
- a just culture, where the workforce knows and agrees on what is acceptable and unacceptable
- a reporting culture, where safety concerns are reported and analyzed and where appropriate action is taken
- a learning culture, where safety is enhanced from lessons learnedFootnote 29
In April 2016, the TSB held a Transportation Safety Summit that brought together more than 70 senior executives and leaders representing operators, labour organizations, industry associations, and regulators from all modes of transportation. A broad consensus emerged from the discussions that, to improve safety effectively, SMS must clearly identify the systemic issues underlying the behaviour. Further, effective communication and collaboration were key elements in building the trust necessary to address safety issues at this level. However, the biggest challenge identified in terms of bringing about this type of “just” culture was the need to build trust and respect in organizations that may have a history of blame.Footnote 30
1.13.1 Canadian Pacific Railway's safety culture
In parallel with implementing an SMS, CP recognized the importance of building an effective safety culture. To help strengthen its safety culture, CP introduced the Home Safe initiative, which promotes both safety engagement and feedback: “By instilling […] the importance of [employees] taking responsibility for their own safety as well as the safety of their co-workers, [CP] can better ensure everyone goes home safe after each and every shift.”Footnote 31 Through CP's Home Safe initiative, employees are trained to offer and ask for help, warn co-workers if they believe they are putting themselves or others at risk, as well as identify, report, and remove hazards.
CP's 2015 Reporting Contraventions, Safety Hazards and Identifying Safety Concerns Procedure specifies that employees have a responsibility to report safety hazards and contraventions and outlines the steps to be followed to report and analyze contraventions and safety hazards. The procedure states that such reporting will not result in disciplinary action, provided that it is in good faith and does not involve criminal activity, malicious intent, or false or misleading information. The procedure also provides for multiple means of reporting hazards:
- verbally to a supervisor;
- in writing using a safety hazard report form if a supervisor is unavailable; or
- if an employee does not feel comfortable reporting directly to a supervisor, through “A‑line,” CP's anonymous, confidential, and independently maintained reporting process.
The procedure also outlines a follow-up process that specifies that hazards should be mitigated expeditiously (i.e., immediately, if possible) and according to the hierarchy of controls. This can include addressing the following:
- elimination of the hazard;
- substitution of other materials;
- processes or equipment;
- engineering controls;
- administrative controls; and
- provision of personal protective equipment (PPE).
Safety hazards involving a written report are to be reviewed by the respective workplace health and safety committee. Reported issues that cannot be resolved are expected to be escalated by following the applicable procedures for the respective workplace health and safety committee.
1.14 Confidential safety reporting systems
To encourage occurrence reporting, a number of jurisdictions internationally have set up confidential rail safety reporting systems that offer reporters confidentiality and protection from prosecution.
1.14.1 Federal Railroad Administration / National Aeronautics and Space Administration Close Call Reporting System
The U.S. Federal Railroad Administration (FRA) set up a program known as the Confidential Close Call Reporting System (C3RS)Footnote 32 in 2007. Following a pilot program involving 4 railroads, including CP, with each participating for 5 years, the program was opened to other operators. As of 2018, 8 railroads were participating in the program; however, participants consist of only passenger railroads.Footnote 33
Railroads participate under a memorandum of understanding (MOU). Specific provisions can vary, but generally include the following:
- An employee has a defined period to file a report with the C3RS for a close call. A close call is defined as “any condition or event that may have the potential for more serious safety consequences.”Footnote 34
- Reports are sent directly to the National Aeronautics and Space Administration (NASA) (as “honest broker”). Once the reports are reviewed, NASA may contact the submitter for additional information. Following this, reports are de-identified, and an identification strip on the report is sent back to the submitter as proof that a report has been filed.
- Filing a report protects the submitter from company and FRA disciplinary action in most circumstances (as set out in the MOU).
- De-identified reports are analyzed by a peer-review team that includes company and FRA representatives.
The C3RS is complementary to, and does not replace, other safety reporting programs such as those provided by a company's safety management structure. A review by the FRA of the C3RS program identified the following:
- The C3RS program has demonstrated bottom-line impacts in the reduction of derailments, injuries, discipline hearings, and equipment costs.
- Effective labour and management relations had a positive impact on safety culture.
- The improvement in safety culture was perceived to have increased the communication between supervisors and labour in the presence of C3RS, in particular when supervisors embrace the willingness to communicate and have productive, blame-free conversations about safety with their employees.
- Improved cooperation between labour and the organization helped achieve more systemic corrective actions.
- The review team had limited opportunities to collect additional safety data related to reported occurrences from the organizations. Therefore, it could not provide a greater understanding of all contributing causes and potential corrective actions.
- Railways can share knowledge about non-proprietary process improvements and corrective actions, increasing the overall benefit of C3RS in the industry.
- An increase was identified in the initiation of corrective actions following occurrences. However, a more robust tracking feature is needed to monitor the effectiveness of the corrective actions.Footnote 35
1.14.2 United Kingdom Confidential Incident Reporting and Analysis Service
The United Kingdom Confidential Incident Reporting and Analysis Service (CIRAS)Footnote 36 was established in 1996. It provides an independent, confidential safety reporting line for various transportation industries, including bus and rail.
The CIRAS is governed by the CIRAS Committee, consisting of representatives from the United Kingdom rail industry and other United Kingdom transportation modes. The committee also includes a number of trade union members and independent professionals with expertise in other industries and academia, such as oil and gas. The program shares lessons learned with all industries through newsletters and information on its website.
The CIRAS reporting and follow-up process is similar to the FRA's C3RS program, with CIRAS acting as an honest broker. Once a report is submitted (i.e., through the website, or by text, phone, or hard copy), the submitter is contacted outside of work to obtain additional information, and a report is prepared and submitted to the appropriate member organization. A response is then provided to the submitter outlining the action taken.Footnote 37
1.14.3 Transportation Safety Board of Canada confidential reporting program
The Transportation Safety Board of Canada (TSB) administers a program called SECURITAS that enables confidential reporting on concerns about safety in the marine, pipeline, rail, and air modes of transportation. The incidents and potentially unsafe acts or conditions submitted through SECURITAS are not always reported (or required to be) through other channels.
SECURITAS reports can lead to the TSB issuing safety communication letters to the Minister of Transport, to other government departments, or to industry organizations for action. These reports can also help the TSB identify widespread safety issues. By combining confidential report data with other accident and incident reports and studies, and by sharing safety information with other agencies in Canada and abroad, a greater insight is gained into national and global transportation safety issues. SECURITAS reports can also support TSB studies and analyses on safety-related matters such as operating procedures, training, human performance, and equipment.
1.15 TSB Watchlist
The TSB Watchlist identifies the key safety issues that need to be addressed to make Canada's transportation system even safer.
Safety management and oversight is a Watchlist 2018 issue. In this occurrence, there was no risk assessment performed as part of the decision to change the yard operations, and therefore there was no job hazard assessment of the operations being performed in the yard. Since no assessment was performed, no risk mitigation measures were identified or established that could have reduced the potential for switching accidents such as this one from occurring.
Actions required
Safety management and oversight will remain on the Watchlist until:
- Transport Canada implements regulations requiring all commercial operators in the air and marine industries to have formal safety management processes, and effectively oversees these processes.
- Transportation operators that do have an SMS demonstrate to Transport Canada that it is working—that hazards are being identified and effective risk-mitigation measures are being implemented.
- Transport Canada not only intervenes when operators are unable to manage safety effectively, but does so in a way that succeeds in changing unsafe operating practices.
Fatigue management in rail transportation is a Watchlist 2018 issue. As this occurrence demonstrates, fatigue continues to pose a risk to the safe operation of trains, including switching yards with a 24/7 operation.
1.16 TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP017/2018 – Radio Analysis
- LP066/2018 – Light Level Measurements
Actions required
Fatigue management in rail transportation will remain on the Watchlist until TC takes the following actions:
- Transport Canada develops a policy framework for the management of fatigue based on its review of fatigue management systems, fatigue science and best practices.
- Transport Canada works with industry and employee representatives and fatigue science specialists to develop a comprehensive approach to fatigue management in the rail sector.
- Transport Canada completes amendments to the Work/Rest Rules for Railway Operating Employees, 2011, based on fatigue science.
2.0 Analysis
Neither the condition of the track nor the rolling stock played a role in this occurrence. Yard assignment FS23 (the assignment) was the only train crew on the diamond, and there were no other railway personnel in the area at the time of the accident. Because there were no witnesses or surveillance cameras that provided a clear image of the events immediately before the accident, the possibility that the yard helper had fallen on the tracks or become incapacitated could not be excluded. However, using the information gathered, the investigation focused on the events that most likely occurred before the accident. The analysis will therefore focus on switching activities, the yard design, fatigue, situation awareness, and Canadian Pacific Railway's (CP) safety management system.
2.1 The accident
The accident occurred when the yard helper was struck and fatally injured by his own yard assignment, which was switching a cut of cars on the west side of the diamond at St-Luc Yard.
While the yard foreman was shoving a car on nearby track DT20, the yard helper, who was located north of the crossover switch between the 2nd West Loop and the West Loop (2WL/WL crossover switch), had left his position to enter the mess building. Shortly thereafter, upon returning to the yard, the yard helper needed to reorient himself with the activities in the yard to confirm the requirements for the next movement. This involved determining the routing and positioning of the yard assignment for the next movement, including the corresponding switches that would need to be lined. The yard helper's brief absence from the diamond area created a task interruption that shifted his focus away from his duties.
The yard assignment had completed its previous task and was proceeding out of track DT20 in preparation for the next task, which consisted of placing the 5th and 6th cars (CP 214036 and CP 215379) on track DT24. To place these cars on track DT24, the yard assignment needed to be positioned on the 2nd West Loop, north of the DT24 switch. This switch would then have to be placed in the reverse position to align the yard assignment toward track DT24.
However, the yard helper instructed the locomotive engineer to stop the assignment past the 2WL/WL crossover switch, which is located north of the DT24 switch on the 2nd West Loop, further than was necessary to complete the next move. This was where the yard helper had been positioned before entering the mess building.
When the yard assignment stopped clear of the 2WL/WL crossover switch, the yard helper reversed that switch, which incorrectly aligned the yard assignment toward the West Loop. The yard helper then reversed the DT24 switch with the intent of aligning the yard assignment toward track DT24 and instructed the locomotive engineer to move the yard assignment into that track. However, the incorrect alignment of the 2WL/WL crossover switch was not identified, which resulted in the yard assignment proceeding over the 2WL/WL crossover instead of the DT24 track.
After reversing the DT24 switch, the yard helper moved to a location west of track DT24 that was clear of the intended route of the yard assignment, but where he was foul of the 2WL/WL crossover track. From this position, the yard helper would have had visual contact with the yard assignment when giving instructions to the locomotive engineer by radio.
From his position, the locomotive engineer could not see the yard helper or the 2WL/WL crossover switch. Proceeding according to radio instructions, the locomotive engineer could not detect the incorrect routing of the yard assignment.
2.2 Employee alertness
An individual's ability to maintain situational awareness is reduced by environmental stressors including fatigue, long working hours, and working counter to one's circadian rhythm. These stressors can affect a person's working memory and attention, reducing the capacity to gather and process information effectively.Footnote 38
The yard helper had the opportunity to obtain a sufficient quantity of sleep during the 38 hours preceding the accident. However, based on other personal activities that day, the yard helper could have had a maximum of only 4 hours of rest during this period.Footnote 39 It could not be determined whether the yard helper had taken the available opportunities to sleep.
The yard helper had the opportunity for full nighttime sleep on the night of 05 to 06 November 2017. It is likely that the yard helper's circadian rhythm—entrained to sleep primarily during the day—acted to decrease the quality of any sleep obtained that night. Therefore, although the yard helper may have been rested when he began his night shift on 06 November 2017, it is likely that he was not as well rested as if he had been working day shifts regularly.
Toward the end of the night shift on 08 November 2018, the yard helper would have been experiencing fatigue due to disruption in the quantity and quality of sleep obtained in the preceding days. This would likely have made the yard helper less attentive to his environment and more prone to attentional narrowing and operational errors. It is likely that the yard helper's fatigue contributed to the incorrect alignment of the 2WL/WL crossover switch.
2.3 Yard lighting
During night operations on the diamond, the level of lighting varied from one area to another. In the vicinity of the occurrence area, there was one fixed lamp post, located on the east side of the diamond. The average level of lighting for the area from the lamp post to the 2WL/WL crossover switch was about 48.2 lux, close to the 50 lux minimum required by the regulations. However, on the west side of the diamond, close to the location of the accident, the level of lighting did not exceed approximately 9 lux. This level of lighting is insufficient to allow individuals working in those areas to be fully aware of their surroundings. A fixed system providing sufficient coverage in the yard would allow employees working in these areas to have adequate lines of sight between the departure tracks and the diamond area of the yard.
While both the yard foreman and the yard helper were using handheld lanterns on the night of the occurrence, as provided for in the regulations, this auxiliary lighting does not replace the illumination provided by a fixed system in the yard. Some railway employees had also identified the insufficient lighting in St-Luc Yard as a concern.
At the time of the occurrence, the existing levels of lighting in the diamond area of the yard made it more difficult for the yard foreman to visually determine the location of the yard helper and to distinguish the direction of travel of the yard assignment.
If railway yards are not adequately illuminated for night switching operations, the visibility of employees, yard tracks, and railway equipment can be compromised, increasing the risk of accidents.
2.4 Switching operations in the diamond area
When the classification yard was closed in 2012, most of the switching operations at St-Luc Yard were moved to the diamond area, which had a significantly different configuration than the classification yard.
Employees are required to remain vigilant while working on or around tracks at all times. However, the switches on the diamond are bordered by other tracks, which causes employees to place themselves foul of the tracks when handling switches. Routine exposure to working foul of an adjacent track can desensitize an employee to the hazards of rail yard operations.
The ground surface in the release zones on the diamond consists of mainline railway ballast, which is less conducive to walking than ballast typically found in a yard. There are also multiple tripping hazards, such as switch stands and overlapping tracks. The operational tasks of the yard foreman and the yard helper require constant walking, in particular between the tracks in the diamond area, where tripping hazards exist.
The ability to clearly identify the switch being handled and the direction for which the switch is lined is key to reducing switch alignment errors. Not all switches in St-Luc Yard have clear identifying marks. The 2WL/WL crossover switch was not labelled, and the DT24 switch was marked with a non-reflective marking on the side of the switch stand. During a footboard safety meeting the week before the accident, the yard helper had said that newcomers to the yard may require additional time to become acquainted with the switches and tracks. While employees familiar with the yard are generally aware of the specific switch locations and track alignment, if switches at St-Luc Yard are not clearly identified and the direction of movement is not clearly indicated, switch alignment errors can occur, increasing the risk of accidents.
2.5 Safety management systems
The Railway Safety Management System Regulations (SMS Regulations) in place when the change in St-Luc Yard was implemented required railway companies to implement and maintain a safety management system (SMS) that included a process to identify safety issues and concerns, including those associated with significant changes to railway operations. The SMS Regulations also required railway companies to have a process for evaluating and classifying risks through a risk assessment.
Although flat switching was already occurring on the diamond, closing the classification yard was a significant change to switching at St-Luc Yard. Therefore, given the differences between the configuration of the classification yard when compared to the diamond area, a task analysis of the yard helper and yard foreman roles would have been appropriate. A task analysis could have identified the differences between the release zones, the risk of being foul of the tracks when releasing cars or turning switches, the presence of tripping hazards, and a reduction in the level of ambient lighting. Thus, mitigating measures such as increased lighting, improved walking conditions, the identification of switches and their targets, and the modification of the switching leads and release zones could have been identified, reducing the risks to employees becoming foul of a track while performing switching operations. CP's SMS did not consider a risk assessment necessary, and therefore the opportunity to identify the new hazards created by the change to switching at St‑Luc Yard was missed.
Since 2015, the TSB has investigated 3 other occurrences where CP had made changes to its operations and did not consider some of the changes “significant.” Therefore, CP did not perform a risk assessment for these operational changes. If risk assessments are not completed when a change to railway operations occurs, new hazards might not be identified, increasing the risk of accidents.
2.5.1 Safety culture at Canadian Pacific Railway's St-Luc Yard
Effective safety management includes a need to continuously identify and mitigate hazards to manage risks. This is influenced by an organization's safety culture, which is characterized by shared values, attitudes, perceptions, competencies, and patterns of behaviour that interact toward enhancing safety.
CP has a procedure in place for the identification and reporting of safety hazards and regulatory contraventions or violations. The procedure specifies that employees have a responsibility to report safety hazards and contraventions and that such reporting will not result in disciplinary action. CP's procedure provides multiple means for employees to report such incidents, including an anonymous reporting process.
At St-Luc Yard, if switching error reports were received by local management, the follow-up would typically include having the employees involved in the incident make a statement. As this could result in disciplinary action, many incidents involving switching errors were not being reported at St-Luc Yard. As a result, management was unlikely to be informed of these types of errors, and leading indicator analysis would not necessarily identify safety issues to implement mitigation measures. CP's procedure for hazard reporting and identification was not implemented effectively at St-Luc Yard.
Other organizations have recognized the benefits of non-punitive incident-reporting policies. They have implemented successful confidential reporting and investigation programs. This provides the employees involved some level of protection from discipline. Without an effectively implemented non-punitive incident-reporting policy, data pertaining to incidents involving close calls may not be consistently collected. Therefore, the opportunity to perform leading indicator analysis and implement appropriate mitigation measures is lost. If a railway company's safety management system is not supported by a positive safety culture, its effectiveness at identifying and mitigating hazards is reduced, increasing the risk of accidents.
3.0 Findings
3.1 Findings as to causes and contributing factors
- The accident occurred when the yard helper was struck and fatally injured by his own yard assignment, which was switching a cut of cars on the west side of the diamond at St-Luc Yard.
- The yard helper left his position to enter the mess building. The yard helper's brief absence from the diamond area created a task interruption that shifted his focus away from his duties.
- The yard helper instructed the locomotive engineer to stop the assignment past the 2nd West Loop / West Loop (2WL/WL) crossover switch, which is located north of the DT24 switch on the 2nd West Loop, further than was necessary to complete the next move. This was where the yard helper had been positioned before entering the mess building.
- The yard helper reversed the 2WL/WL crossover switch, which incorrectly aligned the yard assignment toward the West Loop.
- It is likely that the yard helper's fatigue contributed to the incorrect alignment of the 2WL/WL crossover switch.
- The incorrect alignment of the 2WL/WL crossover switch was not identified, which resulted in the yard assignment proceeding over the 2WL/WL crossover instead of the DT24 track.
- The yard helper moved to a location west of track DT24 that was clear of the intended route of the yard assignment, but where he was foul of the 2WL/WL crossover track.
- Proceeding according to radio instructions, the locomotive engineer could not detect the incorrect routing of the yard assignment.
- Canadian Pacific Railway's safety management system did not consider a risk assessment necessary, and therefore the opportunity to identify the new hazards created by the change to switching at St-Luc Yard was missed.
3.2 Findings as to risk
- If railway yards are not adequately illuminated for night switching operations, the visibility of employees, yard tracks, and railway equipment can be compromised, increasing the risk of accidents.
- If switches at St-Luc Yard are not clearly identified and the direction of movement is not clearly indicated, switch alignment errors can occur, increasing the risk of accidents.
- If risk assessments are not completed when a change to railway operations occurs, new hazards might not be identified, increasing the risk of accidents.
- If a railway company's safety management system is not supported by a positive safety culture, its effectiveness at identifying and mitigating hazards is reduced, increasing the risk of accidents.
3.3 Other findings
- Routine exposure to working foul of an adjacent track can desensitize an employee to the hazards of rail yard operations.
- The operational tasks of the yard foreman and the yard helper require constant walking, in particular between the tracks in the diamond area at St-Luc Yard, where tripping hazards exist.
- Canadian Pacific Railway's procedure for hazard reporting and identification was not implemented effectively at St-Luc Yard.
4.0 Safety action
4.1 Safety action taken
4.1.1 Transport Canada
Through a memorandum of understanding with Employment and Social Development Canada, Transport Canada conducted an investigation into the yard helper's death, under Part II of the Canada Labour Code (the Code). The purpose of the investigation was to understand the circumstances surrounding his death so that recurrence can be prevented and to determine whether Part II of the Code was violated.
As a result of the investigation, a direction was issued to Canadian Pacific Railway regarding the levels of lighting at St-Luc Yard. CP has until May 2019 to address the items in the direction.
4.1.2 Canadian Pacific Railway
Canadian Pacific Railway (CP) took the following corrective actions:
- Conducted a system-wide campaign that focused on the hazards present when working on or about tracks, as well as the associated risk mitigation processes.
- Initiated a system-wide awareness campaign to review the rules and hazards associated with close/restricted clearances on the railway.
- Initiated a program called “Critical Safety Rules” to increase awareness of the dangers of working on or about tracks, as well as the required risk mitigation processes.
This report concludes the Transportation Safety Board of Canada's investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .
Appendices
Appendix A – Yard helper's work/rest history

* Data used to identify periods of being awake and opportunities for sleep for 05 to 08 November 2017 were derived from the yard helper’s cell phone records for these dates.
Appendix B – Occurrences involving misaligned switches
The following is a list of other occurrences involving misaligned switches that the TSB has investigated.
- R16D0073 – On 11 August 2016, at approximately 2119 Eastern Daylight Time, Canadian National Railway Company (CN) freight train M39421-11 was travelling eastward on the Sherbrooke Subdivision of the St. Lawrence & Atlantic Railroad (SLA). At Acton Vale, Quebec, at Mile 93.22, the crew noticed that the switch was lined for the siding. The train's emergency brakes were applied, but the train was unable to stop before reaching the switch. The train diverted into the siding and struck a derail, resulting in the derailment of the lead locomotive. The derail was destroyed and the track was slightly damaged. No one was injured. On the day of the accident, an SLA foreman was to handle switches 272 and 273 and the derail for the track leading to the quarry to allow 2 maintenance machines to reach the quarry. After the machines had passed, the foreman restored switch 273 to the normal position and locked it, but did not do so for switch 272. The foreman was preoccupied with the next task of placing the derail in the non-derailing position to allow the machines to continue to the quarry. Believing that switch 272 had also been restored to the normal position and locked, the foreman transmitted and wrote down this erroneous information before leaving the site.
- R13W0260 – On 18 November 2013, CN freight train L586 41-18 was switching into the Murphys interchange track at Mile 61.0 of CN's Tisdale Subdivision, near Tisdale, Saskatchewan. At about 1818 Central Standard Time, during the hours of darkness, while reversing westward at approximately 12 mph, the train struck and seriously injured a conductor trainee. The employee was transported by ambulance to hospital, but succumbed to injuries during transport. It was determined that the required switching tasks likely conflicted with the trainee's mental model. Instead of lining main track switch TS 22 to the normal position, the trainee inadvertently reversed the nearest main track switch (TS 23) and lined it into the interchange track where he was working. As the trainee reported the mainline switch as lined and locked in the normal position for the main track, the other crew members were unaware that the train was not following its intended route. The investigation determined that if a loss of situational awareness occurs, administrative defences, such as rules and procedures, may not always protect against switching errors, which increases the risk of an accident.
- R12Q0030 − On 09 August 2012, VIA Rail Canada Inc. passenger train P600-21-09 was proceeding southward at 24 mph on the CN Lac St-Jean Subdivision when it unexpectedly diverted into the siding at Hegadorn, Quebec, Mile 78.11. The north switch of the siding had been left in the reverse position by track maintenance employees. There was no derailment. A total of 59 passengers were on board, in addition to the train crew. No one was injured. It was determined that the switch was inadvertently locked in the reverse position after the maintenance crew handled it and left the site, and that the crew did not verify the exact position of the switch after it was last handled.
- R10E0096 – On 18 August 2010, at approximately 0330 Mountain Daylight Time, CN switching assignment L602-23-17 was shoving 50 loaded and 5 empty cars eastward into track VC-64 at Scotford Yard when the movement collided with a cut of 46 empty cars in the track. As a result of the collision, 43 cars derailed, including 21 cars of dangerous goods or residue. There was no release of product and there were no injuries. The foreman had mistakenly positioned himself at the VC-64 switch and did not confirm his location by reading the number on the switch target. The investigation determined that the collision and derailment occurred when 55 cars were shoved, unprotected, into track VC-64, where they contacted a cut of stationary cars. The intended move had been to shove the cars into track VC-63, which the crew knew was clear.
- R09Q0030 – On 17 July 2009, at approximately 1900 Eastern Daylight Time, CN remotely controlled yard assignment YLUS-30 derailed 5 tank cars at Limoilou Yard in Québec, Quebec. A turnout and about 180 feet of track were damaged. No one was injured, but there was a minor fuel leak. As turnout EL18 had a hand-operated switch stand, it was not designed to allow rolling stock to trail through it and was required to be set for the route being used. During the point movement, the assignment trailed through the switch. As the switch was not equipped with a semi-automatic switch stand, it was damaged and therefore no longer permitted reverse movement. Furthermore, as the helper usually saw the switch in its normal and locked position and his attention was likely focused on the activity at the crossings, he did not observe the switch target and did not realize that the assignment had trailed through and damaged the switch.
- R00T0179 − On 09 July 2000, VIA Rail Canada Inc. passenger train 683, travelling westward at 39 mph on the Goderich-Exeter Railway Guelph Subdivision, unintentionally diverted into the siding at Mile 41.37 in Rockwood, Ontario. The east switch of the siding had been left in the reverse position by employees carrying out work in the area. Upon entering the siding, the train collided with track machines. The collision resulted in the derailment of the locomotive and the following 2 coaches; however, all train equipment remained upright. Twelve passengers and 2 employees sustained minor injuries.
- R99H0007 − On 23 April 1999, VIA Rail Canada Inc. train 74, travelling eastward on the north main track of the CN Chatham Subdivision at Thamesville, Ontario, encountered a reversed switch, crossed over to the south main track and derailed at Mile 46.7. The derailed train collided with stationary rail cars on an adjacent yard track. The 2 members of the train crew who were in the locomotive cab were fatally injured. Four people were admitted to hospital with serious injuries. Seventy-seven of the 186 passengers and crew on board were treated in hospital. Numerous others received first aid on site. The investigation determined that the main track crossover switches at Thamesville likely were incorrectly lined and locked in the reverse position by the last authorized crew members.
Appendix C – Other TSB investigations related to Canadian Pacific Railway operational changes where no specific risk assessment was performed
- R16C0065 – On 03 September 2016, at about 0925 Mountain Daylight Time, Canadian Pacific Railway (CP) train 303-646, proceeding westward at approximately 22 mph at Mile 171.7 of the Brooks Subdivision, collided with the tail end of train 113-31, which was stopped on track PT01, near Alyth Yard in Calgary, Alberta. Two locomotives on the head end of train 303-646 derailed, as did 2 covered hopper cars behind the locomotives. The last car on train 113-31, a 3‑platform container car, also derailed. There were no injuries. No dangerous goods were released. In June 2013, following the collapse of the Bonnybrook Bridge, CP had changed the designation of track PT01 between Ogden and the begin/end interlocking limits at 12th Street East from main-track centralized traffic control (CTC) to non-main track. However, when rail traffic over the bridge resumed, CP did not put CTC back in service at this location. When it was decided to keep this section of track designated as non-main track, no risk assessment was conducted, nor was one required at that time. Without a risk assessment, the railway was not specifically aware of the hazards and safety concerns of train crews when operating through this location. Therefore, no specific action had been taken by the railway to mitigate the potential hazards. The investigation determined that, if risk assessments are not conducted for changes to railway operations, potential hazards associated with the operational change may not be identified and appropriately mitigated, increasing the risk of accidents.
- R16W0074 – On 27 March 2016, at about 0235 Central Standard Time, while switching in Sutherland Yard in Saskatoon, Saskatchewan, CP 2300 remote control locomotive system training yard assignment was shoving a cut of cars into track F6. As the assignment was brought to a stop, empty covered hopper car EFCX 604991 uncoupled from the train, unnoticed by the crew. The car rolled uncontrolled through the yard and onto the main track within cautionary limits of the Sutherland Subdivision. The car travelled about 1 mile and over 2 public automated crossings before coming to a stop on its own. There were no injuries and no derailment. No dangerous goods were involved. In early 2016, several operational changes were implemented by CP at Sutherland Yard. The operational changes prompted CP to complete a combined risk assessment in accordance with the SMS Regulations. The risk assessment covered remote control locomotive system (RCLS) operations and the introduction of a point protection zone. However, the risk assessment did not consider the impact of reducing the number of train crews or the change in local practice to primarily switching without air. The risk assessment did not specifically identify a potential hazard related to crew inexperience or the potential consequence of an uncontrolled movement. Therefore, remedial action to address a potential uncontrolled movement, such as the installation of a derail, was not considered or implemented to protect against uncontrolled movements while switching without air.
- R15V0046 – On 11 March 2015, at approximately 0130 Pacific Daylight Time, a rail traffic controller at CP stopped train 672-024 near Mile 102 on the Cranbrook Subdivision after the train had departed Cranbrook, British Columbia, and travelled east for 5 miles without authorization. There were no conflicting movements. The investigation determined that, although qualified for their respective positions, the management crew members were not familiar with the territory. As a follow-up to a meeting with Transport Canada who expressed concern about the increased use of management employees as train crew members, CP submitted its plan to TC, outlining the process for training management employee candidates from entry-level to qualified conductors or locomotive engineers. CP did not submit a risk assessment as part of its notification to TC because it did not consider the training for non-operational management employees to become qualified conductors and locomotive engineers as an operational change that required a risk assessment.