Main-track train derailment
Hudson Bay Railway
Freight train 995-15
Mile 99.59, Wekusko Subdivision
Ponton, Manitoba
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Executive summary
On 15 September 2018, at about 1632 Central Daylight Time, Hudson Bay Railway (HBR) freight train 995 was proceeding northward on the Wekusko Subdivision at 25 mph. At Mile 99.59, near Ponton, Manitoba, the train encountered a void in the roadbed surface ahead. Although the rails and ties were in place, they were actually unsupported and hanging over a washout that was about 50 feet long and 15 feet deep. The train travelled over the unsupported section of track, which collapsed under the weight of the locomotives. The 3 head-end locomotives and the first 4 cars derailed. All 3 locomotives were destroyed, and the crew was trapped in the cab of the head-end locomotive. The conductor died of his injuries on site about 8.5 hours later. The locomotive engineer was extricated nearly 10 hours after the accident and airlifted to a hospital in Thompson, Manitoba, in critical condition. The locomotive fuel tanks were ruptured and released about 6800 litres of diesel fuel.
Track infrastructure maintenance and vulnerability to washouts
Portions of the HBR rail network, like many sections of Canadian railways, were built on fills in locations that may be occasionally exposed to unusual water events that can lead to a washout. Such water events include
- high levels of precipitation,
- rapid melt of heavy snow pack,
- excessive natural water collection throughout a drainage basin,
- drainage disruption that results in excessive water buildup, which can occur due to beaver dams or blocked culverts, or
- any combination of the above.
In the spring of 2017, severe flooding occurred that resulted in a total of 23 washouts and severe track damage between Gillam and Churchill, which essentially shut down that portion of the HBR rail line. From the spring of 2017 to the summer of 2018, OmniTRAX, which owned HBR during this period, had not made any significant capital investment in the track infrastructure, despite several areas requiring work. One of these areas included the area of the derailment.
In the summer of 2018, in the area of the derailment, the precipitation was 380.8 mm, which was 60% greater than the historical average. This heavy precipitation contributed to the accumulation of water immediately east of and adjacent to the raised roadbed at Mile 99.59.
In the weeks preceding the derailment, HBR engineering personnel had been monitoring the high water levels in several areas along the Wekusko Subdivision, including the area of the washout that led to the derailment. The last inspection of the water levels at the occurrence location occurred 2 days before the derailment. Sometime between this last inspection and the arrival of the occurrence train, elevated water levels along the right of way had surged above the top of the culverts. Water flowed through the saturated grade, dislodging and destroying the wood box culverts under the rail bed; water flow was at least 12 feet above the post-washout creek bed. During the washout, the force of the water carried the culvert timbers as far as 1000 feet downstream from their original location. These box culverts were deteriorated and had been identified for replacement; however, culvert replacement alone was not a specific regulatory requirement, and the accident occurred before the work was undertaken.
There was significant beaver activity both upstream and in the vicinity of the derailment. HBR had a beaver control program in place, but this program was reduced in 2017, leaving the track infrastructure vulnerable to a washout event, particularly in situations when a beaver dam is breached. Upstream and east of the rail line, several beaver dams had been breached, likely due to the higher amount of precipitation that summer. These breaches further increased the flow and volume of water accumulating just east of, and immediately adjacent to, the roadbed at Mile 99.59. The additional accumulation of water increased the hydraulic pressure on the raised sand-based fill of the subgrade and contributed to its failure.
Emergency response
In this occurrence, a number of challenging circumstances delayed access to the accident site and complicated the emergency response. The remote location and difficult terrain delayed access to the site, while the release of diesel fuel, the potential of a liquefied petroleum gas release, and the need for a hazmat assessment to ensure that any dangerous goods present were within acceptable levels, all contributed to extending the time required for the response.
The On Board Trains Occupational Health and Safety Regulations require railways to have emergency response plans in place. Although the HBR emergency response plan had guidance for specific types of threats or events, the guidance regarding emergency response to a train derailment was limited to providing a reporting structure and a general safety message. There was no record of HBR conducting emergency response exercises or reviews of any actual responses. As a result, HBR personnel had not been sufficiently trained to respond to significant derailments that may involve dangerous goodss or employee or passenger injuries or fatalities. Furthermore, without proactive monitoring by Transport Canada of HBR’s emergency response plan, the gaps in the plan relating to managing train derailment events and setting up an incident command structure were not identified and addressed.
Dark territory
The derailment occurred while the crew were operating in what is known as dark territory. Train crews communicate by radio with a rail traffic controller (RTC) who issues clearances to facilitate train movement and to keep a safe distance between trains. In some cases, these clearances are issued for the entire subdivision, and the train crews do not encounter any other trains or track personnel. Although train crews maintain radio communication with the RTC, the RTC has no way of detecting where on the subdivision the train is located or what is occurring in the field.
HBR did not have specific company guidance that required a train crew or track maintenance personnel to check in by radio at designated intervals, nor is there any regulatory requirement to do so.
In this occurrence, the derailment was discovered by a civilian helicopter pilot who happened to be flying over the area and contacted the Royal Canadian Mounted Police (RCMP) to initiate the response. Had the pilot not discovered the derailment and returned to assist, it could have gone undetected and unattended for several more hours.
If the occupancy control system is used as the method of train control in remote areas and there is no specific company guidance for personnel to check in with the RTC while en route, there is an increased risk that emergency situations, including derailments, will go undetected for some time, particularly if the personnel are incapacitated.
1.0 Factual information
1.1 The accident
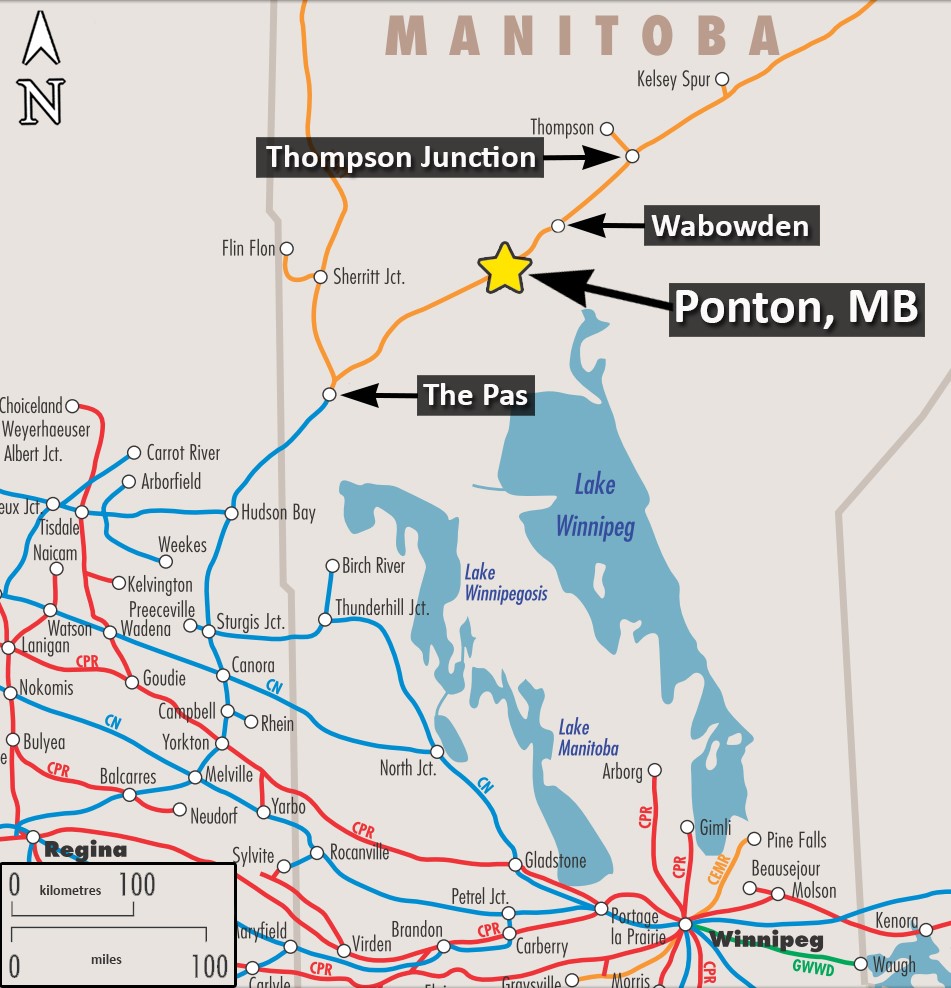
On 15 September 2018, Hudson Bay Railway (HBR) train 995 was ordered for 1100Footnote 1 in The Pas, Manitoba,Footnote 2 and was destined for Thompson, Manitoba (Figure 1).
The train was composed of 3 head-end locomotives, 4 empty cars, and 23 loaded cars. Eight of the loaded cars were tank cars loaded with dangerous goods (DG): 4 of these were loaded with liquefied petroleum gas (LPG, UN 1075) and 4 were loaded with gasoline (UN1203). The train weighed 3233 tons and was 1601 feet long. The crew consisted of a locomotive engineer (LE) and a conductor. Both crew members were qualified for their respective positions, were familiar with the territory, and met fitness and rest requirements.
The locomotives received a pre-departure inspection on 10 September 2018 at The Pas. All safety systems, including locomotive satellite radios,Footnote 3 were functioning as intended.
Before departure, the train received a full mechanical inspection, and a No. 1 air brake test was performed. No anomalies were noted.
Behind the 3 head-end locomotives, the train was sequentially marshalled as follows:
- 2 empty gondola air dump ballast cars
- 3 tank cars loaded with LPG
- 4 tank cars loaded with gasoline
- 1 tank car loaded with LPG
- 4 open-top hopper cars loaded with ballast
- 1 empty open-top hopper car
- 11 open-top hopper cars loaded with ballast
- 1 empty open-top hopper car
At 1155 on 15 September, the train was issued occupancy control system (OCS) clearance 209, authorizing movement in both directions to perform work along the Wekusko Subdivision between Mile 6.0 and Mile 133.0 (Wabowden South).
At 1200, the train departed The Pas (Mile 0.0) on the Wekusko Subdivision.Footnote 4
At 1445, upon passing Dyce siding (Mile 61.9), the crew provided a location report to the rail traffic controller (RTC), confirming the train’s location. Other than the end of the subdivision at Wabowden (Mile 136.4), this was the only place on the subdivision where a location report to the RTC was required. Although location reports could be provided at other places, it was not the regular practice to do so.
On the day of the occurrence, a meet had been planned with a southbound VIA Rail Canada Inc. (VIA) passenger train at Wabowden, where the 2 trains could pass each other and the VIA train could proceed south. The northbound freight train had been scheduled to arrive at Wabowden at 1810, before the VIA train’s scheduled arrival at 1900.
At 1632, as the train was proceeding northward at 25 mph on a raised portion of track, the train crew observed a void in the roadbed surface ahead at Mile 99.59. The rails appeared to be in place, so it was not immediately apparent that there was a significant washout.Footnote 5 Consequently, the train entered the washout location without the crew initiating an emergency brake application. The train proceeded on to the unsupported section of track, the track collapsed, and the head end of the train struck the opposite side of the washout. The 3 head-end locomotives, 2 empty gondola air dump ballast cars, and 2 tank cars loaded with LPG derailed (Figure 2).

All 3 head-end locomotives were heavily damaged. The lead locomotive impacted the opposite side of the washout about 12 feet below the rail and the trailing locomotives and cars ran into the lead locomotive and came to an abrupt stop in just over 400 feet. The lead locomotive had “folded” to an approximate 45-degree angle at its midpoint. The main generator and electrical cabinet in the lead locomotive were pushed forward into the cab, pinning the train crew inside. Both crew members were seriously injured; the conductor died of his injuries before he could be extracted.
The trailing locomotives (the 2nd and 3rd locomotives) came to rest on their sides. All 3 locomotives released diesel fuel from the fuel tanks and oil from the engines.
At the time of the accident, there were scattered clouds, good visibility, and a light westerly wind. The temperature was 9 °C, and the humidity was 43%.
1.2 Emergency response
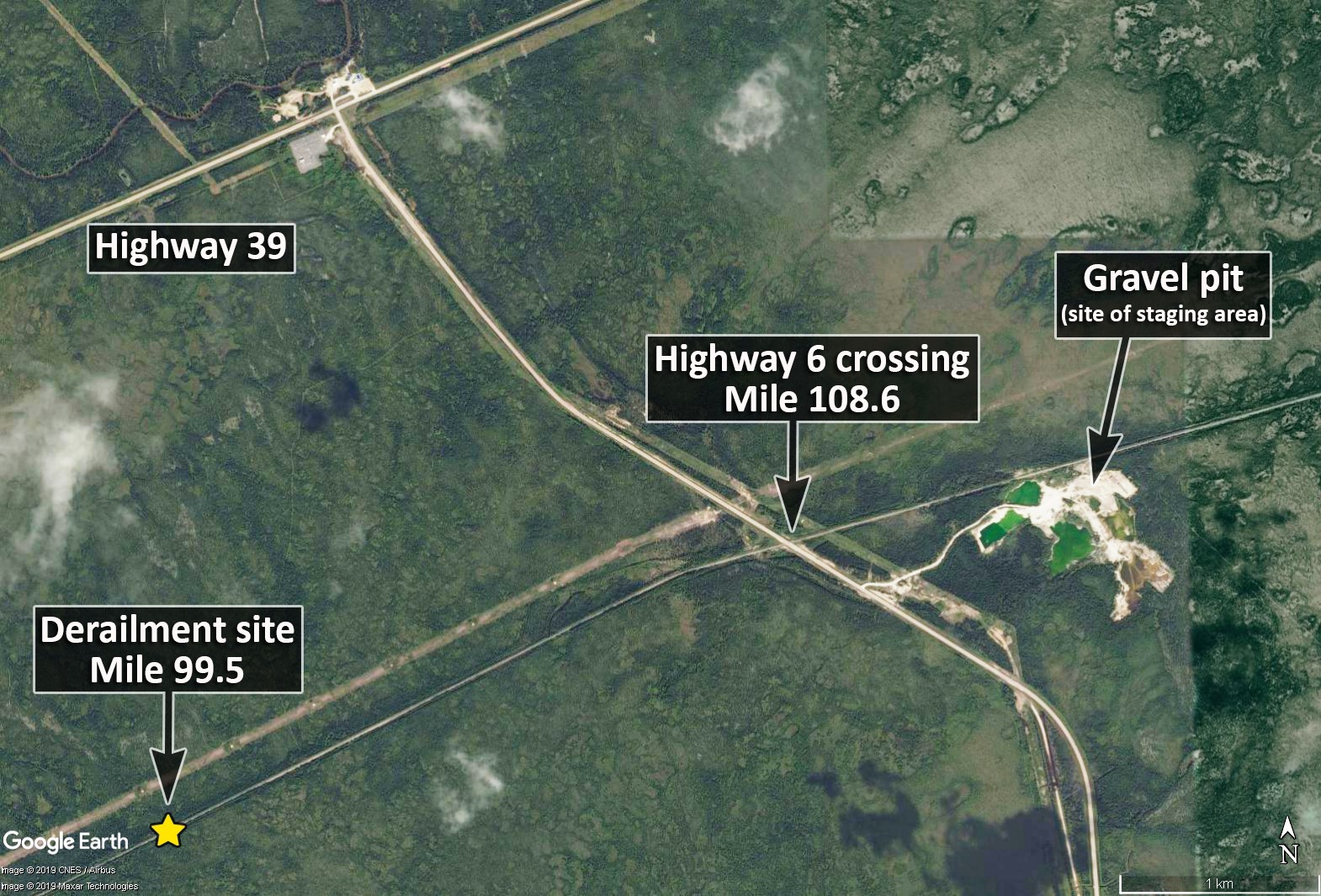
The derailment occurred in a remote area of northern Manitoba which is accessible only by air or rail. The accident site was about 9.1 miles (15 km) south of the Manitoba Provincial Trunk Highway 6 grade crossing at Ponton, which is located at Mile 108.6 of the Wekusko Subdivision (Figure 3). Ponton is 239 km northeast of The Pas and 156 km southwest of Thompson.
1.2.1 15 September 2018
At 1715, the crew of a helicopter (comprised of the pilot and the co-owner of the helicopter) that was en route to pick up surveyors in the area noticed the derailed train. After they picked up the surveyors, they learned that the surveyors had heard the derailment occur. The helicopter crew and surveyors flew back over the derailment site and saw a hand waving from a locomotive cab window.
At 1735, the helicopter landed on a nearby sandbar, and the helicopter crew and the surveyors went to the derailment site on foot. The surveyors approached the site and attended to the trapped crew members. The co-owner of the helicopter was able to call 911 while standing on top of a tank car. However, the 911 operator was unable to determine the location of the accident.
The co-owner then called a member of the Snow Lake Royal Canadian Mounted Police (RCMP) detachment and reported the derailment location and the current situation. This information was relayed to the RCMP control centre, which then called the pilot back for more details on the derailment site and to find out what equipment might be required to rescue the train crew.
At 1807, the RCMP notified the RTC of the accident. At 1818, the RCMP informed Thompson Fire and Emergency Services (TFES) of the train derailment, but did not initially tell them that the crew members were pinned inside the locomotive cab and that some of the derailed cars were transporting DG. TFES dispatched an emergency medical services (EMS) team, consisting of 2 paramedics and an ambulance, to Ponton.
At 1823, the RTC notified an HBR supervisor that there had been a rail accident on the Wekusko Subdivision, south of Ponton, and that the RCMP was on the scene. The RTC also told the supervisor that the crew members were pinned inside the locomotive cab. HBR management was informed, and they responded from The Pas. The road repair truck and hazardous materials (hazmat)–trained personnel were put on standby. An engineering employee was dispatched to the occurrence site in a hi-rail vehicle.
At 1830, the RCMP control centre called the pilot again to ask the pilot to fly the surveyors’ helicopter back to Ponton and pick up 2 RCMP officers who had arrived at the grade crossing. The pilot agreed and returned to Ponton with the helicopter.
At 1853, the TFES received additional information, including photographs, indicating that 2 people were injured and trapped in the cab of the lead locomotive and that DG were present. A general alarm was issued, paging all members of TFES. The photographs and additional information were not relayed to HBR.
At 1855, the pilot arrived back at the site with the RCMP officers, who said that TFES would respond. The pilot then flew the helicopter back to Ponton to transport any TFES personnel or supplies that might aid in the response. However, TFES did not send in any equipment.
At 1900, once on site, the RCMP reported that there was a smell of diesel fuel and possibly propane. The RCMP then informed the TFES that diesel fuel was leaking and the train had been carrying DG tank cars containing LPG, which might also be leaking.
At 1905, even though a helicopter had accessed the site, considering the risk of a DG release involving diesel fuel and LPG, the TFES decided, in accordance with established emergency response protocol, to keep all first responders away from the accident site until its hazmat team had conducted an assessment of the DG hazards. As a result, EMS personnel were informed that they could not access the site using the surveyors’ helicopter until the site assessment was complete.
TFES knew that 2 RCMP officers and first aid supplies had been flown in by helicopter and had told the RCMP officers to keep 300 to 500 m away from the derailed tank car containing propane. Nonetheless, the RCMP officers decided to stay with the injured crew members.
At 1912, a TFES rescue team, with the hazmat trailer and related equipment, departed Thompson for Ponton. While en route, TFES requested a Shock Trauma Air Rescue Service (STARS) air ambulance from Winnipeg. TFES was told that the air ambulance would not be able to depart, due to poor weather conditions in Winnipeg, but that another helicopter and pilot were staged at Island Lake, about 250 km east of the derailment site, and would attend the scene later that night.
Meanwhile, shipping documents were obtained from HBR, the Office of the Fire Commission of Manitoba, and CANUTEC were informed; and additional TFES personnel and equipment were dispatched from Thompson.
At 1940, the EMS team that had been dispatched from Thompson arrived at Ponton. The pilot of the surveyors’ helicopter told the EMS at Ponton that the injured train crew required first aid and pain medication. EMS replied that the TFES had ordered them not to enter the derailment site until the hazmat team had conducted a site assessment.
At 2000, the pilot of the surveyors’ helicopter flew back to the derailment site to pick up the co-owner and the surveyors, then returned to Ponton to deliver an RCMP vehicle key and pick up blankets and heating pads. The 2 RCMP officers remained at the site with the injured crew members. The surveyors’ helicopter made one last trip to the site to deliver the blankets and heating pads.
At 2030, the surveyors’ helicopter departed the accident site just before darkness. The helicopter was not equipped to be flown after dark.
At 2050, the TFES arrived at Ponton, and the TFES captain, who was fully trained in incident command structure, assumed command of the response. This was the first time the TFES had encountered a train accident of this scale, and TFES personnel expected a larger railway response. Because HBR personnel, who were travelling a greater distance, had not yet arrived, TFES established incident command and a staging area in a gravel pit near the Provincial Trunk Highway 6 grade crossing.
At 2120, an HBR supervisor and a superintendent arrived at the Provincial Trunk Highway 6 grade crossing and went to the staging area. None of the responding railway personnel had been formally trained in emergency response or incident command. This was the first time that HBR personnel had to respond to an accident of this scale. At the site, the HBR company officers worked in support of the TFES and RCMP.
By 2145, all TFES personnel and equipment had reached Ponton, including the Thompson Fire Chief, who assumed command of the response. Additional emergency services responded from Snow Lake (EMS), and Wabowden (RCMP, fire, and EMS).
At 2146, the TFES and EMS response group made a first attempt to access the derailment site to perform a site assessment and begin rescue activities. This attempt included
- 2 all-terrain vehicles (ATVs),
- a rescue boggan,
- 2 qualified hazmat technicians,
- 2 firefighter/paramedics (wearing full turnout gear), and
- various equipment, including gas monitoring/sampling meters, lighting, tools, medical equipment, and self-contained breathing apparatus (SCBA) for all responders.
Travel to the derailment site along the rail bed was difficult for the ATVs. At 2155, after travelling about 2 km, both ATVs got flat tires. The decision was then made to use hi-rail vehicles to travel the 15 km from the Provincial Trunk Highway 6 grade crossing at Ponton into the derailment site.
At 2200, an HBR track foreman in a truck equipped with a hi-rail arrived at the Ponton staging area with a rail saw and hydraulic tools. The foreman was instructed to put the truck on the rails and to pick up the TFES members who were with their ATVs. However, as the foreman had not been told the location of the accident site, he inadvertently travelled northward toward Wabowden, instead of southward. After travelling several miles without encountering the ATVs, the foreman turned the hi-rail vehicle, proceeded back to the staging area, and continued south until he located the TFES and EMS responders and transported them to the site. This confusion regarding the direction of travel and the flat tires on the ATVs delayed the arrival of the first group of TFES and EMS emergency responders on site by about an hour and a half.
At 2346, the first group of responders reached the site and conducted an initial site assessment. At 2347, after determining that no LPGFootnote 6 had been released and that the site was safe, the response team began attending to the injured crew members.
1.2.2 16 September 2018
At 0012, a second group of responders arrived on site by hi-rail with more lighting and hydraulic extrication equipment.
Extricating the injured train crew members proved extremely difficult. The effectiveness of the response team’s extrication equipment was limited by the size and thickness of the locomotive steel components that were pinning the crew members inside the locomotive cab. The emergency response teams initially focused on rescuing and extricating the LE, but after a short time, shifted their attention to the conductor.
At 0053, despite the emergency responders’ best efforts, they were unable to extricate the conductor; he died of his injuries while they were attending to him.
The families of the train crew members were first informed of the accident at about 0100. They were not informed of the accident when it occurred, nor were they provided with timely, accurate information, including the status of the crew members, as the response unfolded..
Following the death of the conductor, extrication efforts continued as the emergency responders attempted to free the LE from the locomotive cab. At 0230, the LE was extricated and transported by hi-rail to the staging area (about 15 km away) where a helicopter was waiting.
At 0330, the helicopter departed for Thompson General Hospital with the LE in critical condition.
At about 0400, due to the hazardous conditions remaining at the accident site, all emergency responders were recalled to the staging area. After numerous discussions about the situation, it was determined that recovering the conductor’s body would require assistance from additional agencies with more advanced rescue equipment. At about 0700, incident command at the site was transferred to the RCMP.
1.2.3 Between 16 September 2018 and 17 September 2018
On the morning of 16 September, after further discussions among the emergency responders, it was determined that the Urban Search and Rescue (USAR) team at the Manitoba Office of the Fire Commissioner (OFC) would extract the conductor’s body from the cab. The USAR team, located in Brandon, MB, had the necessary specialized equipment and the expertise to do so.
On 17 September, the USAR team travelled from Brandon to Ponton (approximately 700 km) in preparation for the extraction. It was not until 1455 that the family was told that the conductor’s body was to be extracted the following day.
With respect to environmental clean-up at the occurrence site, starting on 16 September, adsorbent booms were placed downstream in the creek to reduce the environmental impact of the locomotive diesel fuel and lube oil that had been released.
1.2.4 18 September 2018
At 1000 on 18 September, the OFC and the USAR team accessed the accident site. With their specialized rescue training and specialized equipment, the team began the extraction. At about 1530, the conductor’s body was recovered. Upon completing the recovery, the site was turned back over to HBR, and site remediation was then started.
1.2.5 Sequence of events relating to the emergency response
Tables 1 and 2 present a summary of the sequence of events relating to the emergency response.
| Time | Time since the accident | Event |
|---|---|---|
| 1632 | 00:00 | The train proceeded on to the unsupported section of track, the track collapsed, and the head end of the train struck the opposite side of the washout. |
| 1715 | 00:43 | The crew of a helicopter flying overhead noticed the derailed train. |
| 1735 | 01:03 | The helicopter returned to the accident site and landed on a nearby sandbar. |
| 1735 | 01:03 | The co-owner of the helicopter called 911 to report the accident. |
| 1745 | 01:13 | The co-owner called the RCMP detachment in Snow Lake to report the accident. |
| 1807 | 01:35 | The RCMP notified the RTC of the accident. |
| 1818 | 01:46 | The RCMP informed Thompson Fire and Emergency Services (TFES) of the accident. TFES dispatched the first EMS team. |
| 1823 | 01:51 | The RTC notified an HBR supervisor of the accident. |
| 1826 | 01:54 | HBR management was informed of the accident. |
| 1830 | 01:58 | The helicopter departed the site to pick up RCMP personnel in Ponton. |
| 1845 | 02:13 | An HBR engineering employee was dispatched from The Pas to the occurrence site in a hi-rail vehicle. |
| 1853 | 02:21 | TFES received additional information, indicating that 2 people were trapped in the locomotive cab. |
| 1855 | 02:23 | The helicopter arrived at the accident site to drop off 2 RCMP officers. The helicopter then returned to Ponton to be available to transport other personnel and supplies as necessary. |
| 1900 | 02:28 | The RCMP officers on site informed TFES that they could smell diesel fuel and possibly propane. They also indicated that diesel fuel was leaking and that the train had been carrying DG tank cars containing LPG, which might also be leaking. |
| 1905 | 02:33 | In accordance with established emergency response protocol, the TFES made the decision to keep all first responders away from the accident site until its hazmat team had conducted a hazard assessment at the site. |
| 1912 | 02:40 | A second TFES Rescue team (EMS) departed Thompson to travel to Ponton. |
| 1940 | 03:08 | The first EMS team that had been dispatched by TFES arrived at Ponton. |
| 2010 | 03:38 | TFES’s hazmat truck and trailer was dispatched from Thompson to travel to Ponton. |
| 2030 | 03:58 | The helicopter arrived back at the accident site with hot pads, blankets, and other supplies, and then departed. |
| 2050 | 04:18 | The TFES captain arrived in Ponton and assumed command of the emergency response. |
| 2100 (approx.) | 04:28 | The staging area was established in a gravel pit near the Highway 6 grade crossing. |
| 2120 | 04:48 | The HBR supervisor and superintendent arrived at the staging area. |
| 2145 | 05:13 | All TFES personnel and equipment had reached Ponton and were at the staging area. |
| 2146 | 05:14 | EMS personnel departed the staging area using 2 ATVs to travel to the accident site. |
| 2155 | 05:23 | En route to the accident site, both ATVs got flat tires while travelling on the track. |
| 2200 | 05:28 | An HBR track foreman in a hi-rail vehicle arrived at the staging area and was asked to pick up the EMS personnel and transport them to the accident site. However, the hi-rail vehicle departed northward toward Wabowden, instead of southward. |
| 2346 | 07:14 | After having turned the hi-rail vehicle to travel southward and then picking up the EMS personnel, the track foreman reached the accident site. |
| 2347 | 07:15 | Once a a hazmat assessment had been conducted, the accident site was cleared for continued emergency response with no restrictions. EMS personnel began attending to the injured crew members. |
| Time | Time since the accident | Event |
|---|---|---|
| 0012 | 07:40 | A second group of EMS responders arrived at the accident site by hi-rail with the hydraulic extrication equipment and additional lighting equipment. |
| 0015 (approx.) | 07:43 | The EMS responders began the task of extricating the injured train crew members. |
| 0053 (approx.) | 08:21 | The conductor died of his injuries while EMS responders were attending to him. |
| 0055 (approx.) | 08:23 | The EMS responders continued their extrication efforts to free the LE from the locomotive cab. |
| 0230 | 09:58 | The LE was successfully extricated from the locomotive cab. He was then transported by hi-rail to the staging area. |
| 0330 | 10:58 | The LE was transported by helicopter to Thompson Hospital. |
| 0700 (approx.) | 14:28 | Incident command at the site was transferred to the RCMP. |
1.2.6 Site remediation
Manitoba Sustainable Development responded immediately to the accident and placed absorbent booms in the creek to mitigate the environmental impacts downstream.
HBR engaged Tervita and GFL Environmental to remediate the site. They arrived shortly after the accident and placed additional rubber and absorbent booms in close proximity to the accident site to further mitigate potential environmental impacts.
The site remediation also included transloading the LPG product from the derailed tank cars and removing the damaged rolling stock. New metal culverts were installed and the river banks of the creek were reinforced after which the roadbed and track were restored.
GFL removed all remaining locomotive fuel, coolant, oil, batteries and miscellaneous environmental contaminants.
HBR engaged the services of Clifton Engineers to provide services including testing, remediation expertise, and monitoring of the environment at this location.
Manitoba Sustainable Development followed up with the railway before freeze-up in 2018 to ensure the site was left clean and free of contaminants and debris before winter.
1.3 Characteristics of liquefied petroleum gas and precautions to take in the event of a release
LPG is a compressed odourless, flammable gas. Ethyl mercaptan, an odorant, is often added to LPG so that released gas can be easily detected.
1.3.1 2016 Emergency Response Guidebook – Guide 115
Guide 115 of the 2016 Emergency Response GuidebookFootnote 7 identifies the potential hazards of various flammable gases, including LPG, and provides guidance for emergency response and public safety. In addition, the guide outlines potential hazards and safety precautions to consider when dealing with flammable gases.
Potential hazards associated with flammable gases include fire or explosion.
- EXTREMELY FLAMMABLE.
- Will be easily ignited by heat, sparks or flames.
- Will form explosive mixtures with air.
- Vapors from liquefied gas are initially heavier than air and spread along ground.
[…]
- Vapors may travel to source of ignition and flash back.
- Cylinders exposed to fire may vent and release flammable gas through pressure relief devices.
- Containers may explode when heated.
- Ruptured cylinders may rocket.
Health hazards associated with flammable gases include asphyxiation, respiratory irritation, burns and frostbite. The guide also states that
- Vapors may cause dizziness or asphyxiation without warning.
- Some may be irritating if inhaled at high concentrations.
- Contact with gas or liquefied gas may cause burns, severe injury and/or frostbite.
- Fire may produce irritating and/or toxic gases.
1.4 National Fire Protection Association standard NFPA 472: Standard for Competence of Responders to Hazardous Materials/Weapons of Mass Destruction Incidents
National Fire Protection Association (NFPA) standard NFPA 472: Standard for Competence of Responders to Hazardous Materials/Weapons of Mass Destruction Incidents (NFPA 472) is the standard applied for response agencies throughout North America. NFPA 472 specifies the minimum level of competencies required by responders to emergencies involving hazardous materials Footnote 8 (hazmat) and weapons of mass destruction, which are necessary for a risk-based response to these types of incidents. The standard covers competencies for
- awareness level personnel;
- operations level responder;
- hazmat technicians;
- incident commanders;
- hazmat safety officers; and
- other specialist employees. Footnote 9
Competencies for hazmat technicians and incident commanders are similar and include the ability to
- Analyze a hazmat/weapons of mass destruction incident to determine the complexity of the problem and potential outcomes.
- Plan a response within the capabilities of available personnel.
- Implement the planned response consistent with the standard operating procedures and the site safety and control plan.
- Evaluate the progress of the planned response and modify the plan if necessary.
- Terminate the incident by assisting in an incident debriefing and critique. Footnote 10
In addition, incident commanders for responding agencies are required to conduct an incident debriefing and a multi-agency critique as well as to submit a report of the incident to the authority having jurisdiction. Footnote 11 The purpose of the critique is to learn what went right, what went wrong, and what needs to be improved to make responses safer in the future.
Following the accident, the TFES held an internal debrief of the occurrence and no issues were identified. HBR did not hold a debrief meeting nor were they invited to participate in the TFES debrief.
1.5 Emergency response involving dangerous goods
When dealing with DG in an emergency response situation, industry best practice requires that a formalized incident command structure be established to manage the response. When multiple agencies respond with mutual aid, each agency should establish its own incident command and then work under an integrated unified command structure. In this occurrence, only the TFES established an incident command.
Incident command is a response management system developed to organize people, equipment, and resources to respond to any emergency situation, including incidents that involve fire and DGs. It has been used extensively by the military, firefighters, police services, and hazmat emergency response teams, and has been incorporated into law in the United States since March 1990.Footnote 12 In Canada, when incident command is established for fire and hazmat incidents, the local fire chief or provincial official is often recognized as the authority having jurisdiction and assumes the role of incident commander. The senior railway company officer on site will usually implement a company incident command that is integrated into the unified command structure, and coordinate railway site intervention and/or remediation activities.
For any railway occurrence involving DG, including LPG, the initial source of information is usually the train crew. In the event that a crew becomes incapacitated or is unable to provide site information, the task of collecting and assessing the initial source of information falls to qualified emergency responders. These usually include trained railway personnel and trained fire department personnel.
An emergency response involving DG will typically include the following activities:
- An incident command is implemented, and a staging area is selected.
- Emergency responders gather initial information from a safe distance.
- Emergency responders assess the initial information and develop a site entry plan and a safe work plan. These plans will typically include the method of entering the site, site monitoring, identifying potential sources of ignition, and the use of appropriate personal protective equipment (PPE).
- Responders enter the site with appropriate PPE, including, if necessary, positive-pressure SCBA. Responders normally carry devices for air-quality monitoring and product detection, as well as intrinsically safeFootnote 13 radios, cameras, and/or cellphones. Electronic devices that are not intrinsically safe can be a source of ignition.
- Once the site assessment is complete and the area is deemed to be safe, EMS and other response personnel enter the site to begin rescue operations and other site activities, as necessary.
1.5.1 Decision making during emergency response
Research on how individuals and teams make decisions in high-stress situations highlights the need for clear, well-practised procedures for dealing with emergency situations. Specifically, it has been shown that, when teams begin a new task in extreme conditions, they tend to be conservative in their approach and focus on rules or formalized procedures.Footnote 14 This behaviour has been explained as follows:
individuals undergoing stress, anxiety and psychological arousal tend to increase their reliance on internal hypotheses and focus on dominant cues to emit well-learnt responses. In other words, the potential decision response to a crisis situation is to go by the book, based on learned responses.Footnote 15
Research has underscored the importance of clear lines of responsibility in dealing with emergencies.Footnote 16
1.6 Hudson Bay Railway emergency response plan
The HBR emergency response plan states the following:
1.0 EMERGENCY RESPONSE PLANS
1.1 General Plans
The Hudson Bay Railway strives to conduct its operations in a manner that ensures the safety of its employees and the public, and in full compliance with all applicable regulations.
In the event of an incident, the Hudson Bay Railway will take prompt and appropriate action in accordance with this plan, using emergency responders trained to protect life, health, property and the environment, while maintaining full cooperation with regulatory agencies, public agencies and the media.
Our response capability is maintained through local emergency response personnel. The Emergency Response Plan is tested through exercises and systematic reviews of all actual responses.
The other sections of the HBR emergency response plan deals with specific types of threats or events: bomb threats, non-accidental explosions, hijacking of a train, hostage taking, and blockades of tracks.
The HBR emergency response plan did not set forth any processes or procedures for an emergency response to a train derailment in a remote location involving DG and life-threatening injuries to a train crew. The only relevant information for this type of emergency was a reporting structure and a general safety message.
There were no records of HBR conducting any emergency response exercises involving other responding agencies or of any systematic reviews of previous responses.
1.7 Site examination
1.7.1 Derailed freight cars
Both empty gondola air dump ballast cars came to rest in various positions within the washout.
The first derailed tank car (PROX 35275) came to rest perpendicular to the track. This car remained upright with the A-end laying down the embankment into the creek bed and displayed a wheel burn on one side of the tank jacket.
The second derailed tank car (GATX 209551) came to rest upright, adjacent and parallel to the track along the right-of-way. The car exhibited extensive damage to the A-end car body bolster, but there was no visible tank damage.
No product had been released from any of the derailed tank cars.
1.7.2 Track
A subgrade failure and washout measuring about 50 feet long and 15 feet deep had left the rails and ties unsupported and hanging.
Before the derailment, drainage for the creek at this location consisted of 2 wood box culverts, each measuring 40 inches high, 48 inches wide, and 42 feet long, with the top of the culvert located approximately 12 feet below the rail bed. The culverts were inspected on 13 September 2018. Records indicate that there was high water, but both culverts were flowing.
The washout had occurred suddenly, with a significant release and flow of water downstream, as the water levels dropped over 12 feet.
There were indications of significant beaver activity both upstream and east of the rail line; several beaver dams had been breached.
Culvert timbers and flattened streambed plants were observed as far as 1000 feet downstream, north of the washout (Figure 4).

1.8 Weather conditions during the preceding spring and summer
The occurrence area had experienced a wet spring and summer in 2018, with heavy rainfall occurring frequently since May.
Environment Canada’s closest monitoring station was located at Cross Lake Jenpeg, about 100 km east of the derailment site. However, data recorded at that site did not include precipitation totals.
The Environment Canada monitoring station at Thompson, approximately 160 km north of the derailment site, had recorded 380.8 mm of precipitation in the summer of 2018. The average precipitation during the summer for this area was 237.0 mm.
1.9 Hudson Bay Railway
The HBR was built in the early 1900s by Canadian Northern Railway. It was then taken over by the Government of Canada and completed in 1929. The line extends from The Pas to Churchill, with a branch line to Flin Flon and an operating agreement with Keewatin Railway Company to Lynn Lake.
HBR business focused primarily on resource-based sectors hauling ores, lumber, grain, and petroleum products along with equipment, food, and other basic provisions for people in the remote north.
1.9.1 Track ownership and capital investment
In 1997, OmniTRAX Canada (OmniTRAX) acquired the HBR, the Port of Churchill, and all associated assets and began operating it as HBR. Both before and after the OmniTRAX acquisition, the line between The Pas and Churchill was maintained and operated as Class 3Footnote 17 track that permits a maximum track speed of 40 mph for freight trains.
In 2014, with traffic volumes declining and sale of the line being contemplated, HBR, under OmniTRAX, began to reduce investment in maintenance staff and capital projects on the line.
In 2015, the Canadian Wheat Board was dissolved, grain traffic to the Port of Churchill declined significantly, and further staff and capital reductions took place. Subsequently, OmniTRAX began the process to sell off the railway and port.
In the spring of 2017, severe flooding occurred, resulting in a total of 23 track washouts and severe track damage between Gillam and Churchill. This portion of the HBR rail line was essentially closed, cutting off rail service to Churchill and the Port of Churchill. HBR did not undertake repairs to fix the flood-damaged line due to the significant costs. And because the rail line was for sale, much of the other infrastructure maintenance was also being deferred. In general, HBR, under OmniTRAX, performed only a minimum amount of maintenance to keep the remaining portion of the rail line open while remaining in regulatory compliance.
With a reduced engineering force, the track infrastructure began to deteriorate. On 25 October 2017, HBR issued a General Bulletin Order downgrading the track to Class 2, which restricted speed on the entire Wekusko Subdivision to 25 mph for freight trains and 30 mph for passenger trains.
From 2017 until HBR was sold in 2018, OmniTRAX made no capital investment in HBR, nor was it required to, despite several areas needing work. The replacement of the box culverts at Mile 99.59 due to the deterioration and settling had been identified because the track needed to be lifted in that area, but culvert replacement alone is not a specific regulatory requirement. However, the Transport Canada (TC)– approved Rules Respecting Track Safety, otherwise known as the Track Safety Rules, state that
each drainage or other water carrying facility under or immediately adjacent to the roadbed must be maintained and kept free of obstruction, to accommodate expected water flow for the area concerned.Footnote 18
On 31 August 2018, Arctic Gateway Group LP (a consortium of owners) purchased the HBR, the Port of Churchill, and all associated assets and liabilities from OmniTRAX. Rail operations continued as the HBR under the ownership of Arctic Gateway Group. The new company inherited all aspects of the operations. This included HBR operating policies and procedures in place while under the ownership of OmniTRAX, including the HBR emergency response plan.
1.10 Subdivision information
The Wekusko Subdivision runs from The Pas (Mile 0.0) and extends north to Wabowden (Mile 133.0). Much of the subdivision is in a remote location, with limited cellphone coverage.
The Wekusko Subdivision is a low-density rail traffic line. Train traffic includes 4 VIA passenger trains and 2 HBR freight trains each week.
Movements on the subdivision operate under OCS, as authorized under the Canadian Rail Operating Rules (CROR), and are supervised by a RailTerm RTC located in Montréal, Quebec. In the vicinity of the accident, the maximum authorized speed was 25 mph for freight trains and 30 mph for passenger trains.
The OCS method of train control is also referred to as operating in dark territory. In dark territory, there are no trackside signals for a train crew to respond to in the field. Instead, train crews communicate by radio with an RTC who issues them clearances to facilitate train movement. The RTC is responsible for coordinating train movements and maintaining a safe distance between trains.
Trains are typically issued clearances for the entire subdivision and will often traverse the area without meeting any other trains or track personnel. Although train crews communicate by radio with the RTC, the RTC has no way of remotely detecting where the train is located on the subdivision or what might be occurring in the field. There is no company guidance that requires a train crew to check in by radio at designated intervals, nor is there any regulatory requirement to do so.
1.11 Track information
In the vicinity of the derailment, the track was tangent with a slight descending grade northward towards the creek. The rail was 100-pound head-contact jointed rail manufactured by Algoma Steel in 1950 and laid in 1955. The rails were 78 feet long and fastened together with 4-hole joint bars secured with 1-inch bolts. The rail was laid on 12-inch double-shoulder tie plates with 2 spikes per plate anchored at every 2nd tie. The ties were softwood with 55 ties per 100 feet. The ballast was a mix of pit run gravel and 3-inch minus crushed rock with the cribs full and ballast extending slightly beyond the ties to form full shoulders.
The roadbed was about 12 feet above the local terrain. At the derailment site, the subgrade was mainly sand (Figure 5).

A trestle bridge had previously traversed the creek at this location and provided drainage to the local area. At some point, the bridge was replaced with 2 wood box culverts and sand fill. The subgrade had been compacted over the years by the passage of trains. However, it remained susceptible to water infiltration, particularly during periods of high water in the local area.
1.12 Drainage in the area of the derailment
The HBR passes through vast areas of boreal forest wetlands, which are home to a large population of beavers. The land area east of the derailment site encompassed approximately 10 square miles of boreal forest.
Natural drainage of the creek flowed primarily in a northwest direction. In the vicinity of the accident, drainage was provided by culverts under the rail line located at Mile 96.45, Mile 99.59, Mile 99.79, and Mile 99.91. Under conditions of normal water flow, each of these culverts functioned independently.
At Mile 99.59, water passed through the wood box culverts installed 12 feet below the rail. However, as a result of the high water volumes, the water had been backing up and forming a large pool of water east (upstream) of the rail line. Aerial examination following the derailment showed the recent high-water levels east of the rail line, as visible shoreline water markings were present (Figure 6).

1.13 Beaver control
The Track Safety Rules require the roadbed to be maintained and kept free of obstructions to accommodate expected water flow for the area concerned. When the expected water flow has been or may be affected by beaver activity, the railway is responsible for controlling water levels that can affect safe railway operations.
When the Canadian National Railway Company (CN) operated the line, a beaver activity hazard assessment (BAHA) program was in place. This program required hazard assessments to be conducted on the portions of the rail network where the beaver population was significant and where beaver activity could impact the safe movement of trains. Sites were identified and ranked by numerical score (BAHA hazard score) based on how severe the problem was. The BAHA hazard score rating system took into account the potential and nature of the hazard, the characteristics of the drainage basin, topography, level of beaver activity, and existing infrastructure.
The BAHA hazard score was intended to quantify conditions and circumstances that increase the likelihood or severity of failure of the railway embankment resulting from a sudden release of water and debris. Events that can trigger an embankment failure include
- periods of intense precipitation
- rapid snowmelt
- beaver activity
- insufficient intervention to remove beaver dams
In areas with high BAHA hazard scores, one of the primary defences in managing water flow related to beaver activity is the destruction and control of beaver populations and the removal of beaver dams. This program was used extensively before the railway was acquired by OmniTRAX in 1997.
HBR, under OmniTRAX, continued a beaver control program run by a contractor who was a beaver control specialist. In 2015, the contractor had removed 813 beaver dams. In 2016, HBR began removing beaver dams on an ad hoc basis, primarily focusing on what was observed from the track. This work was supplemented by an explosives contractor. This work continued during the spring, summer, and fall, resulting in the removal of 82 beaver dams.
The contractor removed 55 beaver dams during the summer of 2017. However, in the fall of that year, the company decided to end the arrangement with the explosives contractor, and the beaver dam removal program was discontinued. From the summer of 2017 onward, beaver dams were removed by HBR work crews, either by hand or by machine, when the dams were accessible from the track.
In August 2018, a contractor was hired for 4 days before HBR was sold to Arctic Gateway. The contractor removed 41 dams.
1.14 Hudson Bay Railway track and culvert inspections
During the summer of 2018, the railway’s engineering personnel was primarily focused on ensuring proper drainage along the right of way and on performing any maintenance required to keep the line open.
In the vicinity of the derailment, the following inspections were conducted:
- The track was visually inspected in accordance with the Track Safety Rules. The most recent visual track inspection was conducted on 10 September 2018, with no track defects noted.
- The most recent track geometry test was performed on 22 August 2018, with no defects noted.
- The most recent rail flaw detection (ultrasonic) test was performed on 15 August 2017, with no defects noted.
1.14.1 Hudson Bay Railway high water and geotechnical inspections
In the week before the accident, the Wekusko Subdivision track was patrolled on 3 occasions to monitor for high water.
On Monday 10 September 2018, high water was noted at several locations, including Mile 99.59, where the water level was 6 inches above the culvert but still flowing freely. The culverts at Mile 99.79 and Mile 99.91 were blocked and required clearing. It was also noted that additional ballast was needed to lift both rails at Mile 99.59.
On Wednesday 12 September 2018, the track was patrolled in the vicinity of the derailment: high water was again observed. A stake was placed at the water’s edge to monitor the height of the water. The grade was inspected, and there was no visible water seepage from the grade at that time. Ballast was delivered and on hand for the planned track lift at Mile 99.59.
At 1545 on Thursday 13 September 2018, the track was again patrolled. It was noted that the water had dropped by 1 foot at Mile 99.59 from the previous day, and the track lift and surface had been completed. This was the last track inspection before the derailment. No further actions were deemed necessary to protect the track in advance of the next trains scheduled for 15 September 2018.
At the time of the inspection on 13 September, HBR track inspectors and supervisors were not fully aware of the susceptibility of the site to water saturation, the significance and potential consequences of uneven ponding against the roadbed, and how this could affect soil stability. HBR, under the ownership of OmniTRAX, did not provide any geotechnical training to track inspectors or supervisors before the derailment, nor had these employees received any geotechnical training before OmniTRAX acquired HBR in 1997.
1.14.2 Geotechnical training for other railways
Following a significant derailment in 1997 involving a subgrade failure near Conrad, British Columbia,Footnote 19 CN and Canadian Pacific Railway (CP) jointly developed a subgrade hazard training program for maintenance‑of‑way employees entitled Geotechnology for Railroaders. The program has since been delivered to CN and CP personnel across the country. This program includes components dealing with engineering spring preparedness and inspections, a drainage hazard reporting form, and safety measures for water control.
1.15 Regulatory oversight
TC is responsible for providing various forms of regulatory oversight of, and guidance to, the railway industry in Canada. This includes oversight related to the Railway Safety Act and its pursuant regulations, the Track Safety Rules and related infrastructure, as well as the Railway Safety Management System Regulations, 2015 (the 2015 SMS Regulations). TC also provides regulatory oversight and enforcement of the Canada Labour Code (CLC), Part II, and its pursuant regulations on behalf of the Minister of Labour for occurrences involving railway on-board employees.
1.15.1 Transport Canada guidance on culverts and drainage
In January 2012, TC published a Guideline for Culvert Safety Management Footnote 20 which was developed in consultation with the railway industry. The objective was to provide railway companies with a guide for the development of their Culvert Safety Management Program (CSMP) and to promote industry best practices. The guideline highlights the importance of effective inspection and maintenance of culverts, including hazards associated with beaver dams, high-water events, waterway adequacy, blocked culverts, and deferred work.
In January 2014, TC issued a Railway Safety Bulletin entitled “Bridges and Culverts - Mitigating Risk During and After Severe Weather.” Footnote 21 The bulletin was developed due to several unsafe conditions that developed at bridges and culverts as a result of flooding, heavy precipitation, or high-flow events in 2013. The bulletin provides recommended procedures and best practices to address the issue.
1.15.2 Investigation of hazardous occurrences involving railway on-board employees
Employment and Social Development Canada (ESDC) has a memorandum of understanding (MOU) with TC. Under the MOU, TC Rail Safety is responsible for investigating hazardous occurrences in the railway industry involving on-board employees, in accordance with the application and enforcement of the CLC, Part II.
Because this accident resulted in one employee being seriously injured and another being fatally injured, TC conducted a parallel investigation on behalf of ESDC.
1.15.3 On Board Trains Occupational Health and Safety Regulations
Pursuant to the CLC, the On Board Trains Occupational Health and Safety Regulations SOR/87-184 (the OBTOHS Regulations) were approved by the Minister of Labour and came into force on 02 April 1987.
Part XIII of the OBTOHS Regulations deals with “Safe Occupancy of the Work Place” and states in part:
Emergency Procedures
- 13.7 (1) An employer shall, after consulting with the work place committee or the health and safety representative, prepare emergency procedures to be implemented
- if any person commits or threatens to commit an act that is likely to be hazardous to the health or safety of the employer or any employees;
- where there is a possibility of an accumulation, spill or leak of a hazardous substance in a work place controlled by the employer, in the event of such an accumulation, spill or leak;
- in the event of an accident involving a train; and
- in the event of the failure of the lighting system of a train.
- (2) The emergency procedures referred to in subsection (1) shall contain
- a full description of the procedures to be followed, including the duties of his employees; and
- the location of the emergency equipment provided by the employer. Footnote 22
There were no records of any TC review of HBR’s emergency procedures or response plan before the accident.
1.15.4 Railway Safety Management System Regulations, 2015
On 01 April 2015, the 2015 SMS Regulations came into force, replacing the 2001 SMS Regulations. Many of the changes incorporated into the 2015 SMS Regulations responded to the recommendations from the 2007 Railway Safety Act reviewand from the 2008 study on rail safety by the Standing Committee on Transport, Infrastructure and Communities.
Under these regulations, federally regulated railway companies must develop and implement a safety management system (SMS), create an index of all required processes, keep records, notify the Minister of proposed changes to their operations, and file SMS documentation with the Minister when requested.
Section 5 of the SMS Regulations states that a railway company must develop and implement an SMS that includes (in part):
- a process for accountability;
- a process with respect to a safety policy;
- a process for ensuring compliance with regulations, rules and other instruments;
- a process for managing railway occurrences;
- a process for identifying safety concerns;
- a risk assessment process;
- a process for implementing and evaluating remedial action;
- a process for establishing targets and developing initiatives;
- a process for reporting contraventions and safety hazards;
Considering items (a), (c), (d), and (g), it would be reasonable to expect that a railway would have an emergency response plan that sets forth accountabilities and processes for managing railway occurrences, and for implementing and evaluating remedial action for such occurrences, including derailments.
1.16 Transport Canada regulatory activities involving Hudson Bay Railway since July 2016
On 08 July 2016, TC undertook an inspection under the Railway Safety Act. An issue relating to non-compliance was identified to HBR for not posting the CLC, Part II and not having the CLC Regulations readily available. HBR signed an Assurance of Voluntary Compliance to post the information within 14 days, and the matter was closed.
TC further conducted occupational health and safety inspections on 22 August 2016, 12 September 2017, 11 October 2017, and 12 October 2017. No contraventions were observed.
Between 22 August 2016 and 31 May 2018, TC performed 4 mechanical equipment inspections of HBR in The Pas. Each inspection identified areas of non-compliance with regard to freight car and locomotive equipment. Letters of non-compliance were issued to HBR detailing the nature of the required maintenance. In each case, HBR performed the required maintenance, which resolved the mechanical non-compliance issues.
In November 2016, TC undertook a 4-day audit of HBR’s SMS with regard to paragraphs 5(a) to 5(i) of the SMS Regulations. The audit identified 1 non-compliance and 4 deficiencies with respect to HBR processes. The non-compliance and deficiencies identified that the HBR processes for reporting were not being followed and that HBR did not fully collaborate with employees to identify safety hazards. The non-compliance and deficiencies were subsequently resolved, completing the audit.
Between 13 June 2017 and 16 June 2017, TC track inspectors undertook a review of the Wekusko Subdivision track maintenance. This included a review of HBR documentation from 14 May 2017 to 10 June 2017, including all associated maintenance performed on the subdivision, and a visual inspection and a track geometry inspection using TC’s track assessment vehicle. This inspection revealed several areas of cross-level deviation, none of which exceeded the maximum allowable for Class 3 track. The inspection also identified several areas with beaver dams and water management issues, but none of these areas were in the immediate vicinity of the derailment.
On 18 June 2017, TC issued a letter of non-compliance and concern highlighting issues identified during the track inspection.
On 07 July 2017, HBR replied to TC to indicate that corrective measures had been put in place to address the issues identified during the inspection. TC subsequently issued a letter of Sufficient Action, and the matter was closed.
On 11 October 2017, an operations inspection occurred that involved TC monitoring a train crew. A written authority was not copied or transmitted, resulting in a letter of non-compliance being issued. There was no follow-up on this letter.
Additional operation inspections were conducted on 05 July 2017, 10 October 2017, and 12 October 2017, which did not identify any non-compliances.
There were no further TC inspections or audits of HBR before the accident.
1.17 Previous occurrences involving collapse of subgrade
Since 1992, the TSB has investigated 10 other derailments involving subgrade collapse, some of which resulted in crew fatalities or serious injuries. In 4 occurrences, the subgrade collapse resulted from excessive water influenced by breached beaver dams (Appendix A). In the other 6 occurrences, the subgrade failures were attributable to water saturation and buildup of pore pressure in moisture-sensitive fills as a result of record-high precipitation and/or the blockage or failure of water-drainage systems (Appendix B).
The presence of moisture-sensitive deposits in railway subgrades is the consequence of the limitations of construction capabilities and the understanding of soil characteristics at the time the subgrades were initially constructed (circa 1900). At that time, the ability to compact the subgrade was limited, and the importance of doing so was not fully appreciated.
Many sections of Canadian railways built on fills in locations that are exposed to unusual water events—high levels of precipitation, rapid melt of heavy snow pack, excessive natural water collection throughout a drainage basin, or drainage disruption and associated buildup, such as beaver dams or blocked culverts—can become a safety risk.
1.18 Previous investigations involving dark territory where emergency response was affected by delays in notifying the rail traffic controller
Since 1995, the TSB has investigated 2 other main track derailments that occurred in dark territory where emergency response was affected by delays in notifying the RTC:
R03V0083 – On 14 May 2003, at approximately 1210 Pacific Daylight Time, CN freight train No. 356-51-14, travelling eastward from Prince George, British Columbia to Edmonton, Alberta, derailed 2 locomotives and 5 cars loaded with lumber on a bridge at Mile 7.9 of the Fraser Subdivision near McBride, British Columbia. The 2 crew members were fatally injured. Train movements on the Fraser Subdivision are governed by the occupancy control system, as authorized by the CROR and supervised by an RTC located in Edmonton. The RTC had not heard from the crew since approximately 1140. The RTC attempted to contact the train 12 times between 1323 and 1335, but received no response. At 1354, CN personnel were dispatched by road vehicle to locate the train. The investigation determined that
[h]ad the territory been equipped with a system that communicates the location of the train at frequent intervals, such as the Global Positioning System, or frequent calls been made between the train and the rail traffic controller, the train’s location and status could have been recognized earlier, prompting a quicker response.
R95V0017 – On 20 January 1995, at approximately 0721 Pacific Standard Time, CP westbound freight train No. 981-20, operating with 3 locomotives, 27 loaded cars and 22 empty cars approached the 10 degree left-hand curve at Mile 111.0 of the Nelson Subdivision. The train was travelling at approximately 25 mph when an emergency brake application was initiated. The train travelled a further 322 feet before striking fallen rock on the track. The 3 locomotives and the first 2 cars derailed and fell down the 125-foot rock cliff into Kootenay Lake. The locomotive engineer and a trainee were drowned. The conductor suffered minor injuries. Rail traffic on the subdivision was controlled by the occupancy control system and supervised by an RTC located in Revelstoke, British Columbia. The investigation noted that
[w]ith no means of radio communication, [the conductor] ran westward on the tracks meeting maintenance-of-way employees at Mile 114.0 [3 miles away]. The rail traffic controller (RTC) was immediately advised of the accident and emergency response forces were summoned.
1.19 TSB Watchlist
The TSB Watchlist identifies the key safety issues that need to be addressed to make Canada’s transportation system even safer.
ACTIONS REQUIRED Safety management and oversight will remain on the Watchlist until:
|
Safety management and oversight is a Watchlist 2018 issue. All transportation companies have a responsibility to manage safety risks in their operations.
While some companies consider safety to be adequate as long as they are in compliance with regulatory requirements, regulations alone cannot foresee all risks unique to a particular operation. That is why the TSB has repeatedly emphasized the advantages of SMS, an internationally recognized framework to allow companies to effectively manage risk and make operations safer.
In this occurrence, the railway’s emergency response plan, which had not been reviewed by the regulator, did not include detailed procedures or processes for responding to a derailment. In addition, supervisory personnel at the railway had not received any training relating to incident command.
2.0 Analysis
The train was operated in accordance with company and regulatory requirements. Neither the mechanical condition of the locomotives nor the rolling stock were contributing factors to this occurrence. The analysis will focus on drainage and beaver control, track maintenance, inspection and patrols, and emergency response and regulatory oversight.
2.1 The accident
At 1632 on 15 September 2018, the train was proceeding northward at 25 mph on a raised portion of track at Mile 99.59. The train crew observed what appeared to be a void in the roadbed surface ahead. The rails and ties appeared to be in place, but were actually unsupported and hanging over a washout that was about 50 feet long and 15 feet deep. The train crew did not initiate an emergency brake application before entering the washout, which may have lessened the severity of the impact.
The train travelled over the unsupported section of track, which collapsed under the weight of the locomotives. The head end of the lead locomotive dropped about 12 feet below the rail and impacted the opposite side of the washout. Then the other 2 locomotives, 2 empty gondola air dump ballast cars, and 2 tank cars loaded with liquefied petroleum gas (LPG) derailed.
The lead locomotive sustained catastrophic damage upon impact, as the train’s tonnage and momentum continued to push the equipment forward until it came to an abrupt stop in just over 400 feet. The lead locomotive had listed to its side and folded to an approximate 45-degree angle at its mid-point. The main generator and electrical cabinet were pushed forward, crushing the locomotive cab and pinning the train crew members inside the cab. Both crew members were seriously injured. The conductor died of his injuries before he could be extracted.
The derailment occurred when the train encountered an unsupported section of track due to a washout and subgrade failure that had occurred at Mile 99.59 before the train’s arrival.
2.2 Subgrade failure and track washout
In the weeks preceding the derailment, Hudson Bay Railway (HBR) engineering personnel had been monitoring the high water levels in several areas along the Wekusko Subdivision. In the week before the derailment, the area in the vicinity of the derailment had been inspected 3 times. During these inspections, water flow through the culverts at Mile 99.59 was at times below the tops of the culverts, and at other times above the tops of the culverts.
The last inspection of the water level at Mile 99.59 was conducted 2 days before the derailment. It was noted that the water had dropped by 1 foot from the previous day, water was flowing through the culvert at that time, and the planned track lift and surfacing had been completed. No further actions were deemed necessary to protect the track in advance of the next scheduled trains.
Sometime between the last inspection and the train’s arrival 2 days later, elevated water levels along the right of way had surged above the top of the culverts. Water flowed through the saturated grade, dislodging and destroying the wood box culverts. During the washout, the force of the water carried the culvert timbers as far as 1000 feet downstream from their original location. Indications at the site showed that the water flow had been at least 12 feet above the post-washout creek bed. The washout and subgrade failure occurred as a result of water saturation and pore pressure build-up in the moisture-sensitive sand fill, caused by the elevated water levels that had built up adjacent to the track.
2.3 Inspection and track patrols
The HBR track inspectors and supervisors were unaware of the susceptibility of the site to water saturation, the significance and potential consequences of uneven ponding against the roadbed, and how these could affect soil stability. Prior to the derailment, HBR, under OmniTrax, had not been providing any geotechnical training to track inspectors or track supervisors, nor had these employees received any such training before OmniTrax acquired HBR in 1997.
Although the requisite track inspections were conducted and the culverts were cleared, the HBR track inspectors did not fully understand the danger associated with uneven ponding of water against the grade.
2.4 Water flow management
Portions of the HBR rail network, like many sections of Canadian railways, were built on fills in locations that can be occasionally exposed to unusual water events that can lead to a washout. Such water events include
- high levels of precipitation,
- rapid melt of heavy snow pack,
- excessive natural water collection throughout a drainage basin,
- drainage disruption that results in excessive water buildup, which can occur due to beaver dams or blocked culverts, or
- any combination of the above.
2.4.1 Precipitation
In the vicinity of the derailment, the historical average summer precipitation was 237.0 mm. However, in 2018, the summer precipitation for this area was 380.8 mm, representing a 60% increase when compared to the average historical norm. Heavy precipitation that summer (about 60% greater than historical norms) contributed to the accumulation of water immediately east of and adjacent to the raised roadbed at Mile 99.59.
2.4.2 Beaver control program
The HBR passes through vast areas of boreal forest wetlands, which are home to a large population of beavers. Both before and after the sale of HBR to OmniTRAX in 1997, a beaver control specialist who was a licensed contractor had been hired to control beaver populations and remove their dams to help better manage water flow.
In 2014, rail traffic volumes were declining and OmniTRAX was contemplating selling the line. OmniTRAX began to reduce capital investment on the HBR. This involved a reduction in maintenance staff and capital projects.
In 2015, with HBR traffic volumes continuing to decline and track infrastructure maintenance activities declining, OmniTRAX began the process to sell off the railway and the Port of Churchill. The beaver control specialist recorded removing 813 beaver dams that year.
In 2016, HBR began using an explosives contractor along with track employees to remove beaver dams.
In the fall of 2017, HBR cancelled its use of the explosives contractor, likely as a cost-saving measure, without having a viable alternative strategy for beaver control. Any further removal of beaver dams by HBR from the summer of 2017 onward was performed by work crews when the dams were accessible from the tracks.
In August 2018, a contractor, hired before the sale of HBR, removed 41 dams in 4 days.
There was significant beaver activity both upstream and in the vicinity of the derailment. Upstream and east of the rail line, several beaver dams had been breached, likely due to the higher amount of precipitation that summer. These breaches further increased the flow and volume of water accumulating just east of, and immediately adjacent to, the roadbed at Mile 99.59. The additional accumulation of water increased the hydrostatic pressure on the raised sand-based fill of the subgrade and contributed to its failure. Therefore, the reduction of HBR’s beaver control program left the track infrastructure vulnerable to a washout event, particularly in situations when a beaver dam is breached.
2.4.3 Reduced track infrastructure maintenance
In the spring of 2017, severe flooding occurred that resulted in a total of 23 washouts and severe track damage between Gillam and Churchill, Manitoba, which essentially shut down that portion of the HBR rail line. Since that time, OmniTRAX had not made any significant capital investment in HBR, despite several areas requiring work. One of these areas included the area of the derailment. Although HBR engineering personnel had identified that the wood box culverts at Mile 99.59 had deteriorated and needed to be replaced, culvert replacement alone was not a specific regulatory requirement and the accident occurred before the work was undertaken.
In the vicinity of the derailment, there had been heavy rainfall throughout the summer. Several breached beaver dams further contributed to the high water levels.
The combination of water accumulation from the heavy precipitation that summer and the beaver dams that had breached upstream resulted in a significant amount of water pooling adjacent to the track. If railway drainage systems are not monitored and maintained in a timely manner, drainage system components might deteriorate and fail, increasing the risk of a subgrade failure leading to a derailment.
2.5 Emergency response
The derailment occurred at 1632 on 15 September 2018, in a remote area in northern Manitoba. The accident was first noticed at 1715, when the crew of a private helicopter flying overhead observed the derailed train. Upon landing the helicopter at the accident site, the crew made emergency calls to 911 and the Royal Canadian Mounted Police (RCMP). Thompson Fire and Emergency Services (TFES) and HBR were subsequently notified, and arrangements were made to travel to the accident site. At 1855, RCMP officers reached the accident site by helicopter. At 2345, the emergency medical services (EMS) team (from TFES) reached the accident site by rail using an HBR hi-rail vehicle.
At 0053 on 16 September, despite the EMS team’s best efforts to extricate the conductor, he died of his injuries. The locomotive engineer was successfully extricated at 0230, and arrangements were made to transport him by hi-rail to the staging area, and then by helicopter to hospital.
For this occurrence, the emergency responders had to deal with a number of logistical challenges to initially reach the accident site, and then with a number of other challenges at the site.
The logistical challenges to reach the accident site included the following:
- The accident occurred at a location that was accessible only by air or rail.
- The private helicopter that was being used to transport the emergency responders, equipment, and supplies to the accident site had to depart just before darkness, because it was not equipped to be flown after dark.
- When EMS personnel initially attempted to reach the accident site on ATVs, their ATVs got flat tires while travelling along the track.
- The emergency responders had to wait to be picked up by an HBR hi-rail vehicle, which itself was inadvertently delayed because it initially departed in the wrong direction.
The other challenges at the accident site included the following:
- In addition to the diesel fuel leak from the damaged locomotives, there was the possibility of an LPG leak from the damaged tank cars. Consequently, a hazardous materials (hazmat) assessment was required.
- The lead locomotive was heavily damaged during the derailment, with the main generator and the electrical cabinet pushed forward, pinning the crew members inside the cab.
- The equipment that was initially used to extricate the pinned crew members from the locomotive cab had limited effectiveness when cutting the heavier-gauge steel used in locomotive construction.
In this occurrence, a number of challenging circumstances delayed access to the accident site and complicated the emergency response. The remote location and difficult terrain delayed access to the site, while the release of diesel fuel, the potential of a LPG release, and the need for a hazmat assessment to ensure that any dangerous goods (DG) present were within acceptable levels all contributed to extending the time required for the response.
2.6 Emergency response plan and training
When dealing with an emergency response situation, industry best practice is based on establishing a formal incident command structure to manage the response. When multiple agencies respond, each agency establishes its own incident command and then works together under an integrated unified command structure.
Incident command is a response management system developed to organize people, equipment, and resources to respond to any emergency situation. In Canada, when incident command is established for fire and hazmat incidents, the local fire chief or provincial official is often recognized as the authority having jurisdiction, and assumes the role of incident commander.
For a railway accident, such as a derailment involving DG and/or employee fatalities, the railway will usually implement its emergency response plan and then work with other agencies under a unified command structure.
Railways will usually respond immediately with all available mechanical, engineering, and DG personnel and equipment, and then scale back the response later as required. In such circumstances, railways usually assume command, sometimes while en route to a site, and establish a company incident command structure and staging area to begin work. Railway personnel are usually trained and prepared to respond to a vast array of conditions.
2.6.1 Thompson Fire and Emergency Services
When TFES personnel arrived at Ponton, Manitoba, the TFES captain, who was fully trained in incident command structure, assumed command of the response. A staging area and incident command were established in a gravel pit near the Provincial Trunk Highway 6 grade crossing. This was the first time the TFES had encountered a train accident of this scale.
TFES personnel are trained to National Fire Protection Association (NFPA) standard NFPA 472: Standard for Competence of Responders to Hazardous Materials/Weapons of Mass Destruction Incidents (NFPA 472), which is the standard applied for response agencies throughout North America. NFPA 472 specifies the minimum level of competencies required by responders to emergencies involving hazardous materials. The competencies required for incident commanders include the ability to
- Analyze a hazmat/weapons of mass destruction incident to determine the complexity of the problem and potential outcomes.
- Plan a response within the capabilities of available personnel.
- Implement the planned response consistent with the standard operating procedures and the site safety and control plan.
- Evaluate the progress of the planned response and modify the plan if necessary.
- Terminate the incident by assisting in an incident debriefing and critique.
In addition to standard NFPA 472, TFES personnel are trained to refer to the Emergency Response Guidebook, which identifies the potential hazards of transportation incidents involving DG, such as flammable gases.
2.6.2 Hudson Bay Railway
Upon being notified of the accident, HBR put the road repair truck on standby, as well as hazmat-trained personnel, and deployed 2 supervisors to the site. At 2120, the HBR personnel arrived at the Ponton staging area. Although TFES had already established an incident command structure, HBR did not formally establish an incident command to manage its emergency response activities. The HBR personnel who had been deployed had limited previous experience in responding to an accident of this scale. In addition, they had not been formally trained in emergency response or in the establishment of an incident command structure.
Although the HBR emergency response plan had guidance for specific types of threats or events, there was no specific guidance on emergency response to a train derailment beyond providing a reporting structure and a general safety message. There was no record of HBR conducting emergency response exercises or reviews of any actual responses. As a result, HBR personnel had not been sufficiently trained to respond to significant derailments that may involve DGs or employee or passenger injuries or fatalities.
If a robust emergency response plan for significant derailments is not implemented by a railway, including training for railway personnel, the railway’s response to these events might not be consistent nor effective, increasing the risk of additional adverse outcomes.
2.6.3 Civilian assistance
The helicopter crew and surveyors, who discovered the derailment and initially attended to the injured train crew members, worked under difficult circumstances and played an important role in alerting authorities, providing aid and comfort to the trapped crew members, and assisting the RCMP with the initial response.
2.7 Risk associated with train operations in dark territory
Since 1995, the TSB has investigated 2 other main-track derailments that occurred in dark territory where emergency response was affected by delays in notifying the rail traffic controller (RTC).
The TSB’s investigation into the May 2003 main track derailment near McBride, British Columbia, Footnote 23 found that
[h]ad the territory been equipped with a system that communicates the location of the train at frequent intervals, such as the Global Positioning System, or frequent calls been made between the train and the RTC, the train’s location and status could have been recognized earlier, prompting a quicker response.
With respect to this occurrence, the Wekusko Subdivision is a low-density line averaging about 1 train per day. The method of train control is the occupancy control system, so trains operate in dark territory without the assistance of trackside signals that crews can respond to in the field. Much of the subdivision is in a remote location, with limited cell phone coverage.
While in dark territory, train crews communicate by radio with an RTC who issues them clearances to facilitate train movement. The RTC is responsible for coordinating train movements and keeping a safe distance between trains.
In some cases, trains are issued clearances for the entire subdivision: they traverse the area without meeting any other trains or track personnel. Although train crews maintain radio communication with the RTC, the RTC has no way of detecting where on the subdivision the train is located or what is occurring in the field. There is no specific company guidance that requires a train crew or track maintenance personnel to check in by radio at designated intervals, nor is there any regulatory requirement to do so.
In this occurrence, this derailment was discovered by a civilian helicopter pilot who was flying over the area and contacted the RCMP to initiate the response. Had the pilot not observed the derailment and returned to assist, the derailment could have gone undetected and unattended for several more hours.
If the occupancy control system is used as the method of train control in remote areas and there is no specific company guidance for personnel to check in with the RTC while en route, there is an increased risk that emergency situations, including derailments, will go undetected for some time, particularly if the personnel are incapacitated.
2.8 Transport Canada oversight of Hudson Bay Railway
2.8.1 Railway rules and regulations
Since 2016, Transport Canada (TC) has conducted a number of regulatory activities to monitor HBR’s compliance with regulations. The TC activities included the monitoring and review of HBR’s occupational health and safety program, mechanical equipment inspections, safety management system (SMS), track inspection, and operations and rules compliance.
When TC identified deficiencies in each of these areas, a letter of non-compliance was issued. HBR responded to the letters by providing details on its corrective actions. In each case, upon reviewing HBR’s response, TC indicated that the remedial action was sufficient. Given the scope of these activities, TC was regularly conducting regulatory inspections to ensure that HBR was compliant with rules and regulations.
2.8.2 Emergency response plans
Railways usually immediately respond to a derailment involving DG and/or employee fatalities with all available resources. However, the scale of the response can differ between major railways (Canadian National Railway Company [CN] and Canadian Pacific Railway [CP]) and shortline railways (such as HBR) due to the availability of resources and the sometimes more remote territory where some shortlines operate. In these situations, an effective emergency response plan that covers all contingencies is an important part of executing a successful emergency response.
The On Board Trains Occupational Health and Safety Regulations (the OBTOHS Regulations) require railways to have emergency response plans in place. Although HBR had an emergency response plan, it contained no guidance that covered responding to a train derailment. There was no record of HBR conducting any emergency response exercises or reviews of actual responses involving multiple agencies, which further suggests that HBR had not trained for the eventuality of a significant derailment. These factors also played a role in the delay associated with the emergency response.
Furthermore, in accordance with the Railway Safety Management System Regulations, 2015, it would be reasonable to expect that a railway would have an emergency response plan that sets forth accountabilities and processes for managing railway occurrences, complying with regulations, as well as implementing and evaluating remedial action for such occurrences, including derailments. Such a plan would be especially needed for derailments in a remote area that involve employee or passenger injuries or fatalities, or that may also involve DGs.
However, without proactive monitoring by TC of HBR’s emergency response plan, the gaps in the plan relating to managing train derailment events and setting up an incident command structure were not identified and addressed. A TC review of the HBR emergency response plan would have been an opportunity to identify gaps in the plan, and could have presented HBR with opportunities for improvement.
If regulatory oversight of a railway’s emergency response plan, particularly for shortline railways, is not conducted, potential gaps in the plan may not be identified and addressed, increasing the risk that emergency events will not be responded to in the most effective manner.
3.0 Findings
3.1 Findings as to causes and contributing factors
These are conditions, acts or safety deficiencies that were found to have caused or contributed to this occurrence.
- The derailment occurred when the train encountered an unsupported section of track due to a washout and subgrade failure that occurred at Mile 99.59 before the train’s arrival.
- The washout and subgrade failure occurred as a result of water saturation and pore pressure buildup in the moisture-sensitive sand fill, caused by the elevated water levels that had built up adjacent to the track.
- Although the requisite track inspections were conducted and the culverts were cleared, the Hudson Bay Railway track inspectors did not fully understand the danger associated with uneven ponding of water against the grade.
- Heavy precipitation that summer (about 60% greater than historical norms) contributed to the accumulation of water immediately east of and adjacent to the raised roadbed at Mile 99.59.
- The reduction of Hudson Bay Railway’s beaver control program left the track infrastructure vulnerable to a washout event, particularly in situations when a beaver dam is breached.
- The remote location and difficult terrain delayed access to the site, while the release of diesel fuel, the potential of a liquefied petroleum gas release, and the need for a hazardous material (hazmat) assessment to ensure that any dangerous goods present were within acceptable levels all contributed to extending the time required for the response.
- Without proactive monitoring by Transport Canada of Hudson Bay Railway’s emergency response plan, the gaps in the plan relating to managing train derailment events and setting up an incident command structure were not identified and addressed.
3.2 Findings as to risk
These are conditions, unsafe acts or safety deficiencies that were found not to be a factor in this occurrence but could have adverse consequences in future occurrences.
- If railway drainage systems are not monitored and maintained in a timely manner, drainage system components might deteriorate and fail, increasing the risk of a subgrade failure leading to a derailment.
- If a robust emergency response plan for significant derailments is not implemented by a railway, including training for railway personnel, the railway’s response to these events might not be consistent nor effective, increasing the risk of additional adverse outcomes.
- If the occupancy control system is used as the method of train control in remote areas and there is no specific company guidance for personnel to check in with the rail traffic controller while en route, there is an increased risk that emergency situations, including derailments, will go undetected for some time, particularly if the personnel are incapacitated.
- If regulatory oversight of a railway’s emergency response plan, particularly for shortline railways, is not conducted, potential gaps in the plan might not be identified and addressed, increasing the risk that emergency events will not be responded to in the most effective manner.
3.3 Other findings
These items could enhance safety, resolve an issue of controversy, or provide a data point for future safety studies.
- Although Hudson Bay Railway engineering personnel had identified that the wood box culverts at Mile 99.59 had deteriorated and needed to be replaced, culvert replacement alone was not a specific regulatory requirement and the accident occurred before the work was undertaken.
- The equipment that was initially used to extricate the pinned crew members from the locomotive cab had limited effectiveness when cutting the heavy-gauge steel used in locomotive construction.
- The helicopter crew and surveyors, who discovered the derailment and initially attended to the injured train crew members, worked under difficult circumstances and played an important role in alerting authorities, providing aid and comfort to the trapped crew members, and assisting the Royal Canadian Mounted Police with the initial response.
4.0 Safety action
4.1 Safety action taken
4.1.1 Transport Canada
On 05 February 2019, Transport Canada (TC) inspectors conducted a site profile and comprehensive inspection of Hudson Bay Railway (HBR). During this inspection, it was noted that, following the derailment on 15 September 2018, HBR had updated its security plan and emergency response plan to include measures to address derailments. It was also noted that HBR would purchase and upgrade its communication equipment.
Because this accident involved a fatality and a serious injury to on‑board employees, TC conducted a parallel investigation on behalf of Employment and Social Development Canada, in accordance with a memorandum of understanding between the 2 parties.
4.1.2 Hudson Bay Railway
Following the occurrence, HBR inspected all of the culverts on all of its subdivisions. HBR also reinstated its beaver control program, including additional new equipment, personnel, inspection protocols, and training to all track foremen on their track inspection guidelines. In addition, HBR hired a specialist in bridges, structures and culverts for all planned inspections. This specialist will attend all 3rd-party engineering inspections.
The company’s security plan and emergency response plan was updated to include a section on responding to a derailment. The plan was rolled out company-wide in April 2019.
The company’s communications policy with respect to operating in dark territory was modified to require crews to check in with the rail traffic controller (RTC) every hour. If the crew does not do so within 30 minutes, the RTC will immediately notify an HBR supervisor.
In April 2019, HBR updated its safety management system (SMS) to include updated reporting templates and procedures, as well as company targets and initiatives. Designated reporting stations were set up in appropriate booking-in locations with paperwork and procedural outlines. The new SMS also included quarterly and annual safety reporting and trend analysis.
HBR implemented a new hazard prevention program. As part of this program, in June 2019, HBR completed a task analysis with its health and safety committee.
HBR developed a pre-employment training program in collaboration with the University College of the North and Manitoba Education and Training for new track employees. The 4-week course includes training specific to rail and track safety.
HBR implemented an on-boarding program, and put a process in place to educate employees on company safety procedures. In addition, HBR implemented a process to coordinate additional rail specific training and track certification expiry dates.
The process for health and safety meetings was updated. A training program for committee members was implemented, including
- creating an electronic template for meeting minutes to ensure all reported concerns and ideas are dealt with;
- implementing a follow-up process to ensure that items are completed in a timely manner; and
- ensuring that all committee members take online training on the Canada Labour Code, Part II.
This report concludes the Transportation Safety Board of Canada’s investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .
Appendices
Appendix A – TSB investigations involving subgrade failure and beaver dams
TSB Railway Investigation Report R92T0183 – In July 1992, a Canadian National Railway Company (CN) freight train encountered a collapsed subgrade at Mile 135.0 of CN’s Caramat Subdivision near Nakina, Ontario. In this occurrence, the roadbed failure was caused by a sudden draw down of the water in a pond from a breached beaver dam. The train travelled onto the suspended portion of track. Two crew members were fatally injured, and a 3rd was seriously injured.
TSB Railway Investigation Report R97T0097 – On 07 April 1997, a Canadian Pacific Railway (CP) freight train plunged into a depression in the track at Mile 44.8, Parry Sound Subdivision, near Pointe au Baril, Ontario, resulting in the derailment of 4 locomotives and 14 cars. The subgrade failure was attributed to hydrostatic stresses from changes in water levels as a result of a beaver dam. One crew member sustained serious injuries, and 2 crew members had minor injuries. The loose state of the sand fill was viewed as a contributing factor in the subgrade failure. The track remained intact and suspended over the depression, allowing the Automatic Block Signal system to continue to function as the train approached the area of failure.
TSB Railway Investigation Report R97T0200 – On 18 July 1997, the roadbed collapsed at Mile 195.75 of CN’s Bala Subdivision. The collapse occurred at a location where a bridge had been replaced by a culvert and pit run fill. A large upstream beaver dam, not visible from the right of way, failed, releasing a large volume of water down towards the track. The water flowed through and washed out the grade and culvert, leaving the track hanging over the gap. No trains were involved, as the subgrade failure was detected by track maintenance personnel before any trains arrived.
TSB Railway Investigation Report R09H0006 – On 03 June 2009, an Ottawa Valley Railway freight train derailed 2 locomotives and 7 cars at Mile 60.1 of the North Bay Subdivision near Hodgson, Ontario. The locomotives overturned, resulting in minor injuries to the crew. The collapse was attributable to the record amount of rainfall in the previous week that resulted in increased ground water flow and accumulation. Rising water level in 3 upstream beaver ponds led to the failure of a 15-foot section of one of the dams, releasing a large volume of water. The water had a cascading effect when 2 additional dams failed as the water flowed downstream. A pond formed against the upstream bank of the track subgrade when the accumulated water exceeded the capacity of the culvert. The water level rose rapidly and flooded the track, washing out several sections of the track subgrade, leaving the track intact but unsupported.
Appendix B – Other TSB investigations involving subgrade failure
TSB Railway Investigation Report R94W0101 – In April 1994, a Canadian National Railway Company (CN) freight train encountered a washout depression at Mile 91.0 of the Kinghorn Subdivision, near Orient Bay, Ontario. Two crew members were seriously injured, and 1 sustained minor injuries. The roadbed failure was attributable to water infiltration and weakening of the glacial lacustrine silts and clays. The track had remained intact and suspended over the depression and did not affect the occupancy control system method of train control being employed.
TSB Railway Investigation Report R97V0063 – On 26 March 1997, a CN freight train encountered a large roadbed depression and derailed at Mile 106.15 of the Ashcroft Subdivision, near Conrad, British Columbia. Both crew members were fatally injured. The Board determined that an extraordinary volume of surface water runoff from melting heavy snow cover and high seasonal precipitation was not captured and carried away as intended by the drainage system above the adjacent Trans-Canada Highway. The water soaked into the ground, migrated through the highway fills, and infiltrated and destabilized the moisture-sensitive railway subgrade. The railway subgrade could not sustain the resultant high pore pressure and collapsed.
TSB Railway Investigation Report R13E0069 – On 28 April 2013, at 0355 Central Standard Time, a Canadian Pacific Railway (CP) freight train was proceeding westward from Wilkie, Saskatchewan, to Hardisty, Alberta, when 17 of its cars, loaded with potash, derailed at Mile 80.7 on the Hardisty Subdivision, near Provost, Alberta. Approximately 350 feet of track was destroyed. There were no injuries.
The derailment occurred when the train passed over a track irregularity due to a track subgrade failure. The roadbed was approximately 10 feet above the local terrain and had been constructed in the early 20th century using in situ sand, gravel, and clays. Although the subgrade had been compacted over the years by the passage of trains, it had remained susceptible to water infiltration. Due to the limited capacity of the drainage system and the southern exposure, the water level remained higher on the south side of the track relative to the north side, resulting in above-normal water-level infiltration and saturation of the track subgrade.
TSB Railway Investigation Report R13W0124 – On 28 April 2013, a VIA Rail Canada Inc. (VIA) northbound passenger train encountered a roadbed slump at Mile 83.55 of CN’s Togo Subdivision, near Togo, Saskatchewan. The 2 locomotives and the 2 leading cars derailed. The embankment collapse occurred due to water saturation and the buildup of pore pressure in moisture-sensitive fills, which resulted from a rapid snowmelt and inadequate water drainage due to the ice plug at the culvert outlet. The frozen culvert had blocked surface drainage and had caused ponding in the upslope ditch. This ponding resulted in excess hydraulic head forming in the culvert barrel and drop structure. The excess head on the leaking drop structure and culvert rivet holes resulted in an elevated piezometric surface condition in the embankment, making it more susceptible to failure.
TSB Railway Investigation Report R15H0092 – On 01 November 2015, a Huron Central Railway freight train was proceeding westward on the Webbwood Subdivision at 25 mph when a train-initiated emergency brake application occurred at Mile 72.08, near Spanish, Ontario. Two separate groups of equipment derailed: 3 locomotives and 8 cars on the head end and 5 cars near the middle of the train. Approximately 225 feet of roadbed was destroyed. No dangerous goods were involved. There were no injuries.
Water saturation within the embankment resulted in reduced cohesion and stability of the subgrade material, reducing the capacity of the track to support trains. Over time, the unstable roadbed, in conjunction with the impact loading of car wheels that was magnified by the non-staggered joints, had produced increased deflections at the rail joints, initiating fatigue cracks within the joint bars.
TSB Railway Investigation Report R18W0168 – On 05 July 2018, while travelling at 33 mph, a VIA passenger trainencountered a track washout in a remote location at Mile 23.60 of the CN Turnberry Subdivision. The 2 lead locomotives derailed and came to rest on their side. The crew then made an emergency radio broadcast and advised the rail traffic controller of the derailment and the need for assistance, as the site was inaccessible by road. The 2 operating crew members sustained minor injuries and were treated at the local hospital. There were no other injuries.
To provide drainage from the Pasquia Hills, 2 culverts, each measuring about 30 feet long by 8 feet in diameter, run from west to east under Highway 9 at roadway kilometre 37. Following heavy rains in the area in the week before the occurrence, the culverts under the highway began accumulating forest debris. This resulted in the accumulation of a significant amount of water along the west side of the highway. With the rising water levels and the associated rise in hydraulic pressure, the water flow eventually overwhelmed the culverts and washed out the highway and roadway culverts.
With the highway breached, the excess water flowed overland, flooding the railway right-of-way between 2 railway culvert locations (Mile 23.53 and Mile 24.23). The increased water volume eventually overwhelmed the railway culverts (3 of which measured 3 feet in diameter and 1 of which measured 2.5 feet in diameter) and started to flow through the track subgrade. Eventually, the trackbed washed out, leaving the track unsupported at the occurrence location, causing the derailment.