Bottom contact
Tanker Nanny
Deer Island, Chesterfield Inlet, Nunavut
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
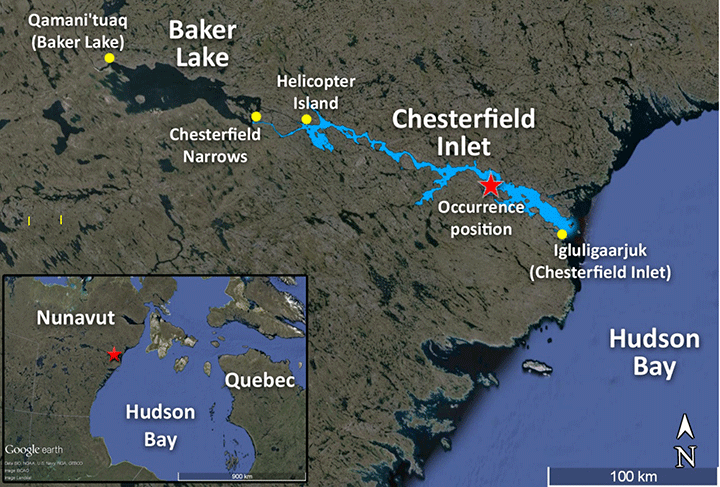
On 14 October 2014, at approximately 0630 Newfoundland Daylight Time, the tanker Nanny made bottom contact west of Deer Island in the Chesterfield Inlet, Nunavut. At the time, the Nanny had a partial cargo of diesel on board. No pollution or injuries were reported, but there was damage to the ballast tanks, including a crack that allowed water ingress. The vessel resumed its voyage following the occurrence, and later proceeded to St. John's, Newfoundland and Labrador, for repairs.
1.0 Factual information
1.1 Particulars of the vessel
| Name of vessel | Nanny |
|---|---|
| International Maritime Organization (IMO) number | 9051399 |
| Port of registry | St. John's, Newfoundland and Labrador |
| Flag | Canada |
| Type | Oil and chemical tanker |
| Gross tonnage | 6544 |
| Length | 110.6 m |
| Draft at time of occurrence | Forward: 6.1 m Aft: 6.9 m |
| Built | 1993, Hyundai Shipbuilding & Heavy Ind. Ltd., Ulsan, South Korea |
| Propulsion | 1 diesel engine (4050 kW) driving a controllable-pitch propeller |
| Cargo | Ultra-low sulphur diesel (6350 m³) |
| Crew | 14 |
| Registered owner and manager | Coastal Shipping Limited, Goose Bay, Newfoundland and Labrador |
1.2 Description of the vessel
The Nanny is a double-hulled oil and chemical tanker of steel construction with the navigation bridge, engine room, and accommodations located aft (Photo 1 and Appendix A). Propulsion is provided by a single diesel engine. The vessel has a single controllable-pitch propeller, a single spade rudder (with a maximum angle of 35° to either side), and 2 controllable-pitch tunnel thrusters of 450 kW each, 1 at the bow and 1 at the stern. The vessel's service speed is 14 knots.

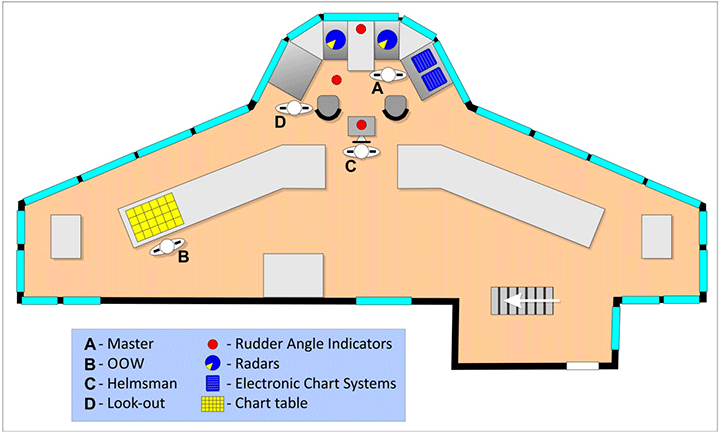
The bridge is equipped with all required navigational equipment. There are 2 radars, 1 located on either side of the centreline. Two electronic chart systems (ECS) are located on the starboard side of the centre console. The vessel has 2 global positioning systems (GPS), 1 located on the port side of the centre console, and the other located at the chart table on the port side of the bridge. The vessel is fitted with a simplified voyage data recorder (S-VDR).
The vessel is steered from a central helm station that is slightly aft of the centre console. There are 3 rudder angle indicators: 1 at the helm position, 1 on the centre console between the radars, and 1 mounted in the deckhead above and slightly aft of the port radar (Appendix B). The deckhead rudder angle indicator light was inoperative at the time of the occurrence.
1.3 Chesterfield Inlet navigation
Chesterfield Inlet is a 124-nautical mile (nm) navigational waterway joining Baker Lake, a freshwater lake, to Hudson Bay (Appendix C). The community of Baker Lake is 40 nm from the western entrance to Chesterfield Inlet. The inlet is subject to strong tidal streams of 3 to 5 knots that cause cross-currents in much of the waterway. Ebb tide flows of up to 8 knots have been reported in the Chesterfield Narrows, and tidal ripsFootnote 1 are frequent at Deer Island channel. The least depth along the inlet is 4.2 m in the Chesterfield Narrows.Footnote 2
The inlet is 1 nm wide or slightly narrower, except for 3 course legs where the channel broadens to 2 nm or more. On the approaches to Baker Lake, to the west of Helicopter Island, the navigable width of the inlet narrows to between 0.05 nm and 0.25 nm. Transiting the inlet on a vessel of the Nanny's size requires making over 50 course alterations, 12 of which are larger than 70°.
The landscape around the Chesterfield Inlet is low and sloping, with few distinguishing features. The shores are rocky and the radar images they produce correspond well with the charts. The Canadian Hydrographic Service (CHS) produces detailed paper charts of the inlet, but not electronic charts. These are, however, available from a private company.
Seventeen unlit leading beacon ranges mark the route through Chesterfield Inlet. Two of these ranges mark the outbound (easterly) route through Deer Island Channel. The shuttle tankers sometimes transit during darkness because they can only pass through Chesterfield Narrows during high tide, which occurs about every 12 hours.
1.4 History of the voyage
At 2330Footnote 3 on 12 October, the Nanny completed fueling operations in Baker Lake for the 2014 season and proceeded outbound to rendezvous with the tanker Travestern at Helicopter Island (Appendix C). At 0800 on 13 October, the Nanny secured alongside the Travestern and began taking on diesel fuel as cargo for 4 ports along the Labrador coast.
On 14 October at 0150, the Nanny departed from alongside the Travestern for the community of Chesterfield Inlet on Hudson Bay, a distance of approximately 107 nm. At that time, the bridge team consisted of the master, a second officer, a lookout, and a helmsman. At 0545, the helmsman and the lookout were relieved by a new watch. At 0600, the second officer plotted a position on the chart using a radar range and bearing, and was relieved by the third officer as officer of the watch (OOW).Footnote 4
The OOW monitored the vessel using the starboard radar and the ECS, and the master remained on the bridge. The vessel was full ahead and proceeding in darkness at speeds that at times exceeded 19 knots,Footnote 5 as a result of the ebb current. At 0615, the OOW recorded a position in the position log using 2 radar ranges which he cross-referenced with the GPS. The vessel was approximately 2.6 nm from the next course change of 071° true (T) through the Deer Island Channel which is 0.3 nm at its narrowest. The safest passage through the channel is marked by a set of unlit range beacons.
At 0622:42, the OOW, who was at the con for the first time in this area, requested that the master take over before the large alteration to port at Deer Island (Figure 1), approximately 0.7 nm before the next course change waypoint.Footnote 6 The master took over the con shortly afterwards, and the OOW went to the chart table and began preparing the next chart.Footnote 7 The helmsman was manually steering a course of about 140° gyrocompass (G) and the vessel was proceeding at a speed of 16.7 knots. The master was monitoring the vessel's progress on the starboard radar, where he had set up a parallel index to determine when to commence the port turn off Deer Island. A parallel index line was also set up on a course of 071° T to maintain a distance of 0.22 nm off the northernmost point of Deer Island.
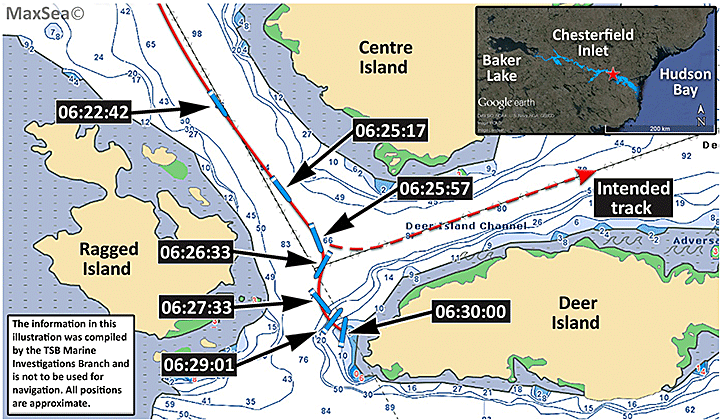
At 0625:17, the master ordered the helmsman to apply 10° port rudder to initiate the turn at the planned wheel-over position (Figure 1). The helmsman acknowledged the order by repeating it, but put the helm to 10° starboard. Within seconds, the master ordered the helmsman to apply 15°. The helmsman looked at the rudder angle indicator and repeated the order, but put the helm to 15° starboard.
At 0625:57, the master gave another port order while monitoring the vessel on the starboard radar. The helmsman asked for clarification about the direction of the order. The master ordered the helm be applied faster without indicating the direction. The helmsman then stated that the helm was at starboard 15°. The master ordered the helm hard to port. The helmsman acknowledged by repeating the order and applying maximum port helm (35°). At 0626:18, the course over the ground was 161°, the heading was 193°G, and the vessel was swinging to starboard at a rate of 93° per minute. The speed was 15.6 knots.
At 0626:33, the Nanny was at the alteration point for the next course (071°T) on a heading of 202°G (Figure 1). The speed was 13.4 knots. At 0626:41, the OOW moved from behind the chart table to stand just aft of the master. The OOW looked at the ECS on the starboard side and began stating various directions including: course over the ground, bearing to the missed alteration point and the heading without always indicating the parameter to which he was referring. The master continued to monitor the Nanny on the radar as the vessel began to swing to port. The lookout departed the bridge to standby the anchor. Over the next 3 minutes, the master continued to monitor the Nanny on the radar as it swung back to port while querying the information being provided by the OOW. At some point during these 3 minutes, the master applied astern propulsion.Footnote 8 At 0629:01, the heading was 046°G and the speed had decreased to 4 knots. By 06:29:47, the vessel's heading was 016°G and the speed was 0.2 knot. The course over the ground was 126°T.
At 0630, the Nanny made bottom contact 0.2 nm west of Deer Island in position 63°37.2′ N, 091°31.2′ W (Figure 1). The vessel's heading at this time was 012°G. The engines and the bow thrusters were used to manoeuvre the vessel back into the channel, and the Nanny continued its voyage while the crew sounded the tanks and checked for damage. They found a crack, approximately 0.6 m long, in way of No. 3 port water ballast tank that was allowing water ingress.
At approximately 1000, the Nanny arrived at anchor off Chesterfield Inlet and the OOW disembarked as scheduled. At this time, the master reported the occurrence to the company, which subsequently informed Transport Canada Marine Safety and Security (TCMSS) at 1230. At 1326, the master reported the occurrence to Northern Canada Regulation System (NORDREG). At approximately 2100, TCMSS ordered the Nanny to divert to Coral Harbour to facilitate communications while awaiting a condition of class.Footnote 9
On 15 October, based on the chief officer's damage report to the company, the classification society issued a condition of class. The Nanny was authorized to continue its voyage, discharge its cargo, and then proceed to the nearest port with suitable infrastructure to assess the damage and execute the required repair work. The Nanny discharged its cargo at 4 ports along the coast of Labrador and arrived in the port of St John's, Newfoundland and Labrador, on 28 October. The vessel was dry docked, a damage survey was performed, and repairs were made.
1.5 Damage to the vessel
An inspection following the occurrence found that the vessel had sustained damage to the tank plating and internal structures in way of the double-bottom water ballast tanks (Table 2). The vessel was out of service from 28 October to 29 November 2014 while the repairs were carried out in drydock.
| Tank # | Area of damage | Damage description |
|---|---|---|
| 1 | Starboard bottom | Plating and internal structure deformed |
| 2 | Starboard side | Plating and internal structure deformed, crack in plate |
| 3 | Starboard bottom | Plating and internal structure deformed |
| 3 | Port bottom | Plating and internal structure deformed, puncture in plate |
| 4 | Starboard bottom | Plating and internal structure deformed |
| 5 | Starboard bottom | Plating and internal structure deformed |
| 6 | Starboard bottom | Plating and internal structure deformed |
1.6 Vessel certification
The Nanny was certified and equipped in accordance with existing regulations. The vessel had a valid Safety Management Certificate that was issued by Det Norske Veritas (DNV) in 2013. Prior to that, in 2009, the Nanny held a Statement of Voluntary Compliance with the International Management Code for the Safe Operation of Ships and for Pollution Prevention (ISM Code) that was issued by DNV.
The vessel's Safe Manning Certificate indicated that the watch arrangement is a 2-watch system (6 hours on – 6 hours off). The company normally assigned an additional navigation officer to the Nanny in order to have 2 navigation officers on the bridge while conducting shuttle operations into Baker Lake. The third officer was the additional officer assigned for the duration of the shuttle runs in October 2014.
1.7 Personnel certification and experience
The master held a valid Master Mariner certificate issued in 2006. The master had been sailing in various capacities since 1972 and had served on tankers as a master since 1990 when he first started working with Coastal Shipping Limited. He had transited the Chesterfield Inlet numerous times, on board the Nanny and on other tankers. In 2014, the master had worked as master on the Nanny at various times, including a shift in June before rejoining the Nanny again on 06 October from the tanker Travestern. The master had completed a formal 30-hour bridge resource management (BRM) courseFootnote 11 in April 2008.
The OOW had worked on various vessels since 1982, and first obtained a Watchkeeping Mate certificate in 1986. He held a valid Watchkeeping Mate, Near Coastal issued in 2008. He had approximately 100 days of service as an OOW, having worked primarily as a deckhand/helmsman. The OOW first joined the Nanny on 28 September 2014 as third officer. The OOW had not completed BRM training, nor was he required to do so.
The helmsman held a valid Bridge Watch Rating certificate issued in 2013 and had first joined the Nanny on 01 August 2014. This was his first time working on a commercial vessel. The helmsman had approximately 8 years of previous experience on fishing vessels. The helmsman had not completed BRM training, nor was he required to do so.
1.8 Environmental conditions
At the time of the occurrence, the vessel was navigating in darkness. The visibility was clear, and the weather was overcast with variable wind under 5 knots. Low tide was predicted to be 0.4 m at 0952 at Norton Island,Footnote 12 and the ebb flow created a current that was calculated as being between 2 and 5 knots.
1.9 Baker Lake fueling operations
The Nanny is 1 of 2 shuttle tankers used to transfer fuel to shore tanks at Baker Lake. The shuttle tankers take on fuel from larger tankers that anchor near Helicopter Island, 32 nm from the entrance to Baker Lake. In general, fuel deliveries commence in July and continue until the shore tanks are full. They then resume towards the end of the season, in October, in order to top up the tanks before winter. In 2014, the shuttle tankers made 21 delivery transits into Baker Lake: 6 of these transits were in October.
The transit from Hudson Bay to Helicopter Island is 107 nm, at least 8 hours of navigation. Once at Helicopter Island, the shuttle tankers take on fuel for 12 to 24 hours then navigate the remaining 72 nm to the community of Baker Lake, at least 5 hours of navigation. It takes 12 to 24 hours to discharge cargo at the Baker Lake terminal, depending on the quantity to discharge, and then the shuttle tankers return to Helicopter Island. Thus, a round trip between Helicopter Island and Baker Lake takes a minimum of around 30 hours and must be timed so that the shuttle tankers pass through Chesterfield Narrows at high tide (Appendix C). The shuttle tankers make several transits to resupply the shore tanks, which can take up to a week.
1.10 Hours of work and rest
The International Maritime Organization (IMO) and the International Labour Organization (ILO) require maritime administrations to recognize the danger posed by fatigue, especially for those personnel whose duties involve the safe operation of a vessel. The International Convention on Standards of Training, Certification and Watchkeeping (STCW) and the Maritime Labour Convention (MLC) stipulate that seafarers who are assigned duty as officer in charge of a watch or as a rating forming part of a watch, and those whose duties involve designated safety, prevention of pollution, and security duties shall be provided with rest periods of
- not less than a minimum of 10 hours of rest in any 24-hour period,
- not less than 77 hours in any 7-day period,
and that,
- the daily hours of rest may be divided into no more than 2 periods,
- the interval between rest periods must not exceed 14 hours, and
- at least 1 of the rest periods must be at least 6 hours.
The STCW and MLC require that daily hours are maintained in a standardized form to allow for monitoring and verification of compliance.Footnote 13, Footnote 14
The company's safety management system (SMS) set out requirements for hours of rest that were in accordance with the STCW requirements.Footnote 15 It was the practice for each crew member to enter their hours of rest into a spreadsheet on the vessel's computer. The spreadsheet had 3 columns that automatically tabulated hours of work, hours of rest, and total hours of rest per 7 days. While the master had overarching responsibility for ensuring that these records were completed and periodically sent ashore, in practice, it was the chief officer who ensured that all records were completed monthly. These documents were filed ashore by the company and reviewed, if requested, in scheduled audits and reviews. There was no evidence that these hours had been reviewed.
The SMS explained that
[h]ours of rest are considered time when the crew members are not required to work. Since there are many things to be done during these off-hours, crew members are responsible to ensure they get adequate sleep during their hours of rest to avoid fatigue during their next work period. Short breaks are not considered rest hours and are to be recorded as work time.
The SMS also indicated that if a crew member was on call during a rest period then an adequate compensatory rest period must be provided if the normal period of rest was disturbed by call-outs to work.
The Transportation Safety Board of Canada (TSB) examined 7 of the crew members' work-rest schedules for the 2 weeks preceding the bottom contact. These included the schedules for the master, chief officer, second officer, third officer, bosun, and 2 deckhands. With the exception of the master and the OOW, none of the schedules were in compliance with the SMS. Specifically, 5 of the 7 crew members had worked longer than 14 hours at least once in the 2 weeks preceding the occurrence. One of the deckhands did not receive the daily minimum hours of rest on 7 of the 14 days that were examined, which meant there was also a non-compliance with the requirement for the weekly minimum hours of rest. There was 1 instance of a crew member being provided with a compensatory rest period. Twelve work-rest schedules from the Nanny crew were collected in a previous occurrence investigation.Footnote 16 Examination of these hours found that 5 schedules were in violation of the company SMS.
1.11 Fatigue
Fatigue refers to the body's response to sleep loss or sleep disruption and can cause individuals to suffer performance detriments that increase the risk of incidents and accidents.Footnote 17 Fatigue may result from one or more of the 6 risk factors: acute sleep disruptions, chronic sleep disruptions, continuous wakefulness, circadian rhythm disruptions, sleep disorders or other medical and psychological conditions, and/or illnesses or drugs that affect sleep or sleepiness.
Of the 128 marine investigations undertaken by the TSB since 2002, fatigue was cited as a finding in 14 of them (or 11%).Footnote 18 Five (or 36%) of these occurrences resulted in fatalities or missing persons.
In 2014, in light of several marine incidents where fatigue was considered to be a factor, a Concentrated Inspection Campaign (CIC) was conducted by various international port state control authorities. The CIC focused on compliance with STCW hours of rest. There were 4041 inspections in a 3-month period as part of a joint campaign between the Paris Memorandum of Understanding (MOU) and Tokyo MOU regions. The CIC found unsatisfactory compliance with required hours of rest. Analysis of the deficiencies showed that hours of rest were not being recorded correctly in 449 cases, (or 11%) and that watchkeeping personnel did not have sufficient rest in 203 cases (or 5%).Footnote 19
1.11.1 Fatigue risk factors
The TSB considers the 6 risk factors when determining if fatigue exists or not. These risk factors are established using crew members' hours of work-rest, actual hours of sleep obtained (when available), and specific sleep-related personal data. Appendices D and E provide further details about the hours of work and rest and definitions of the risk factors. The TSB used the established criteria for each of the 6 fatigue risk factors to determine whether or not fatigue risk factors were present for the 3 key bridge personnel in this occurrence.
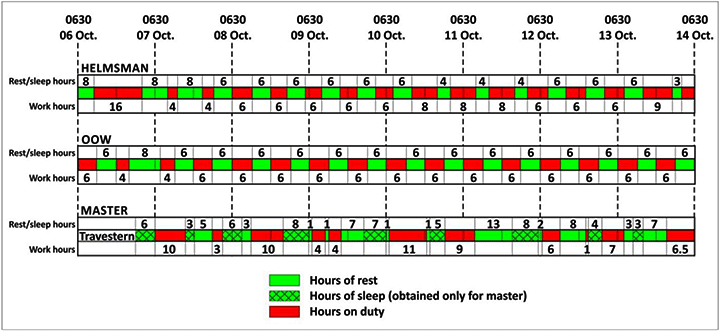
The work-rest schedules for the 3 key bridge personnel in this occurrence (the master, the OOW, and the helmsman) were analyzed for the 1-week period preceding the accident. During this period, the master was not assigned to a watch but was working whenever required. The OOW and helmsman were working a 6 hours on/6 hours off schedule, on duty from 0600-1200 and 1800-0000.
The master's hours of sleep showed that, before the occurrence, he had been awake for 13.5 hours, since 1700 on the previous day. In the 24 hours preceding the occurrence, he had a 3-hour nap and, in the 24 hours before that, he had one 4-hour nap following a period of continuous wakefulness of 17 hours. The day before that, he had a period of 22 hours of continuous wakefulness.
The hours of rest for the helmsman indicated that, over the 7 days leading up to the occurrence, he had worked 106 hours, with only 62 scheduled hours of rest. Three days before the occurrence, he received only 2 rest periods of 4 hours each. Before the occurrence, he had worked from 1800 until approximately 0300 and had expected to be called at 0800, but was called out for the 0600 watch instead.
The OOW was not required to work any extra hours outside his normal 6 on/6 off schedule in the week before the occurrence, although he had expected to start at 0800 on the morning of the occurrence, like the helmsman, but was called out for 0600 instead.
The TSB analysis found that 3 of 6 fatigue risk factors were present for the master and for the helmsman: acute sleep disruptions, chronic sleep disruptions, and desynchronization of the circadian rhythm. Additional fatigue risk factors may have been present for all 3 (Table 3).
| Fatigue risk factor | Master | Helmsman | OOW |
|---|---|---|---|
| Acute sleep disruption | Present | Present | May be present |
| Chronic sleep disruption | Present | Present | May be present |
| Circadian rhythm disruption – desynchronization | Present | Present | Not present |
| Circadian rhythm disruption – timing | May be present | May be present | May be present |
| Continuous wakefulness | May be present | Not present | Not present |
| Sleep disorders | Not present | Not present | Not present |
| Medical/psychological conditions | Not present | Not present | Not present |
1.11.2 Fatigue management plans
A fatigue management plan (FMP) is a recognized way to proactively manage operational fatigue. These plans may include appropriate shift and rest scheduling, fatigue awareness training, and use of alertness strategies and fatigue reporting mechanisms to monitor actual levels of operational fatigue. In the rail industry, Transport Canada (TC) has provided a document entitled Fatigue Management Plans: Requirements and Assessment Guidelines to help rail companies with the development of FMPs. Rail FMPs must be filed with TC in order to meet industry's Work/Rest Rules for Railway Operating Employees.Footnote 20 TC's document specifies that FMPs must consider, but not be limited to, the following: education and training, scheduling practices, dealing with emergencies, alertness strategies, rest environments, implementation policies, evaluation of FMPs, and crew management effectiveness.Footnote 21 Furthermore, according to the Railway Safety Management System Regulations (2015),Footnote 22 the railway company must apply the principles of fatigue science when scheduling the work of their employees.
In the civil aviation industry, there is no requirement for operators to have an FMP, but TC does provide guidance to those voluntarily adopting these programs.Footnote 23 There is no requirement for marine companies to implement FMPs, nor did the company that operates the Nanny have one.
While training about fatigue is not required, the vessel did carry a series of instructive safety videos on various topics including one on fatigue called Minimizing Fatigue, Maximizing Performance. These videos, which had been on board for about a year before the occurrence, were intended to be viewed by the crew during the regular occupational health and safety meetings. At the time of the occurrence, the crew had not watched the video on fatigue. None of the bridge team members had taken training on fatigue awareness, fatigue management, or alertness strategies, nor were they required to do so.
1.12 Medical hearing examinations
The IMO standard for the medical examinations of seafarers is set by the ILO. The ILO guidelinesFootnote 24 provide internationally recognized criteria for maritime administrations. Medical examinations ensure that
the seafarer demonstrates adequate hearing and speech to communicate effectively to detect audible alarms, [and] have no medical condition, disorder or impairment that prevents the effective and safe conduct of their routine and emergency duties on board. During the conduct of an exam the seafarer's intended position on board ship and, as far as practicable; the physical and mental demands of this work and the anticipated voyage pattern should be established.Footnote 25
For hearing examinations of seafarers, the ILO guidelines recommend using a
standardized method, such as a pure tone audiometer hearing test in the range of 500 to 3000 Hz. Alternative assessment methods using validated and standardized tests that measure impairment to speech recognition are also acceptable. Speech and whisper testing may be useful for rapid practical assessments. Hearing capacity for seafarers should be an average of at least 30 dB (unaided) in the better ear and an average of 40 dB (unaided) in the less good ear within the frequencies 500, 1000, 2000 and 3000 Hz (approximately equivalent to speech-hearing distances of 3 m and 2 m, respectively).Footnote 26
The ILO standard specifies the hearing performance requirements for those undertaking deck or bridge duties recommending that, in addition to passing the audiometer test, they be able to hear whispered speech at a distance of 3 m. Furthermore, “appropriate equipment should be used in the assessment of hearing capacity, visual acuity, colour vision and night blindness, particularly regarding those examinees who will be engaged in lookout duties.”Footnote 27
In Canada, TC designates physicians as marine medical examiners (MME) to perform medical examinations, including hearing tests, in accordance with the MPR.Footnote 28 The MPR stipulates that marine medical examinations follow the standards set by the ILO. To assist MMEs, TC also provides a guide, called Seafarer Medical Examinations: A Physicians Guide. The guide states that “[s]ubjective testing will be continued to be used to screen for hearing and the seafarer must demonstrate the ability to adequately hear conversation. Failing that, an audiogram must be provided.”Footnote 29
Prior to 2013, MMEs were required to administer a conversational test and a whisper test at 2 m. However, when the guide was last updated in 2013, it did not include the requirement to conduct the whisper test. The result is that the current version of the guidelines instructs MMEs to administer only a conversational test during a marine medical exam with no distinction for those with deck/bridge or lookout duties.
The master of the Nanny held a valid TC medical certificate and had consistently passed the subjective conversational and whisper tests at 2 m before 2013. In 2013, the master passed the subjective conversational test and a partial audiogram in at the lower ranges of 500 to 1000 Hz. In May 2015, the master passed the conversational test and was not given an audiogram test.
In August 2015, at the request of the TSB, the master underwent a hearing test administered by an independent physician; the test included an audiogram in the 500 to 8000 Hz range. The master passed the conversational test but failed the whisper test at a distance of 2 m and 3 m. Whispering occurs around 20 dB in the 2000 to 4000 Hz range (this is an approximation as speech sounds can vary according to intensity and pitch).Footnote 30 The master's audiogram indicated impairments from 1000 Hz to 8000 Hz. Specifically, the master had hearing loss ranging from mild to severe beyond 2500 Hz. The hearing loss was likely the result of noise-induced hearing loss and/or age-related hearing loss.
1.13 Navigational risk assessment
A navigational risk assessment involves identifying, analyzing, and mitigating hazards to vessels operating in a waterway with the goal of increasing navigational safety. In remote and challenging waterways such as Chesterfield Inlet, a navigational risk assessment is particularly important, given the complexity of navigating the inlet and the lack of lighted aids.
In 2006, the managing company of the Nanny organized a meeting with their senior masters to assess the navigational risks of providing a fuel delivery service to Baker Lake via Chesterfield Inlet. While the decisions made at the meeting were documented, the company was unable to provide the TSB with a record as the documents no longer existed.
However, some actions were taken to mitigate the risks such as:
- developing an entry into confined waters safety checklist,
- designating certain areas of Chesterfield Inlet as confined waters,
- ensuring a maximum draft of 4.6 m for Chesterfield Narrows,
- limiting passages to high tides at slack water in Chesterfield Narrows, and
- requiring the master or chief officer to be present with the OOW in confined waters.
1.13.1 Aids to navigation in Chesterfield Inlet
When the Canadian Coast Guard (CCG) designs or modifies an aid to navigation system, a level of service analysis is required to identify and mitigate risks in accordance with CCG's published levels of service. Due to the short summer season in the Arctic, the process of collecting information takes place over a number of years. The data gathered during the level of service analysis provides guidance in the appropriate selection of aids to ensure that the service being provided meets the availability as laid out in CCG Aids to Navigation program directives.
In 2010, the CCG received 30 requests for additional aids or modification to aids to navigation in the Arctic. These included requests to have the 2 sets of range beacons in Chesterfield Narrows lit and a buoy placed on Skua Reef. Chesterfield Narrows and Skua Reef are located approximately 85 nm and 45 nm west of the occurrence location, respectively. Several of the Arctic requests were deemed to be a high priority at the April 2011 meeting of the Arctic Marine Advisory Board sub-committee on charting and aids to navigation, co-chaired by the CCG and a member from the shipping industry.
In 2013, a CCG level of service analysis commenced for Chesterfield Inlet to identify traffic patterns and navigational hazards in the area. A geomatics survey of the fixed aids in Chesterfield Inlet (17 sets of unlit range beacons and 1 reference light) was conducted and the results have yet to be analyzed. In order to complete the analysis, more precise hydrographic information is required, and a hydrographic survey is scheduled to take place in the summer of 2016.
In its 2014 Fall Report of the Commissioner of the Environment and Sustainable Development, the commissioner noted
that despite repeated requests by the shipping industry for new or modified aids to navigation in 30 locations in the Arctic, reviews of only 2 of these locations were conducted by the Canadian Coast Guard. Industry stakeholders have expressed concern that there has been little progress in addressing their requests.Footnote 31
In May 2015, at the Prairie and Northern Region Canadian Marine Advisory Council, the company that operated the Nanny identified that their biggest issue in fuel deliveries to the Arctic communities is with the available infrastructure, including range lights. The CCG advised participants that the request for new/modified aids for Chesterfield Inlet remains a high priority.
1.14 Bridge resource management
BRM is the effective management and use of all resources, both human and technical, available to the bridge team to ensure the safe completion of the voyage. BRM incorporates concepts of communication, teamwork, problem solving, decision making, and situational awareness. In addition to performing their regular duties, navigating officers have a responsibility to work as a team to ensure a shared understanding of how the voyage will progress and to deal with emergencies as they arise. Specifically, bridge team members have a responsibility to maintain overall situational awareness as well as be responsible for their individual duties. They also have a duty to work as a team to help prevent single-point failure, which may occur when only 1 person is responsible for a safety-critical task and that person has no back-up to help identify possible errors. BRM entails communicating effectively, taking an active role in navigation and monitoring, and making use of all available navigational information to enable identification of equipment errors or human errors.
The master was trained in BRM; however, no one else on the bridge had taken BRM training.
1.14.1 Regulatory requirements for bridge resource management training
Currently, TC does not require bridge officers to complete BRM training to achieve or maintain their certificates of competency. However, TC does set standards for non-mandatory BRM training, which include training on situational awareness.Footnote 32 The company had provided the master with BRM training in 2012, but no other members of the bridge team had taken this training, nor were they required to do so.
TC has proposed amendments to the MPR requiring Simulated Electronic Navigation (SEN) training for issuance of new certificates, as well as for renewal of existing certificates. TC has also proposed changes that will introduce operational BRM competencies in level 1 (SEN 1) training courses and level 2 (SEN 11) training courses.Footnote 33
1.15 Passage planning
According to IMO guidelines,Footnote 34 all vessels should complete a voyage plan, also called a passage plan, from berth to berth to ensure the safe passage of the vessel on its intended voyage. A passage plan provides bridge team members with a shared model from which to work. Passage planning allows a bridge team to assess the safety of a voyage by identifying the risks, and thus having the opportunity to mitigate them. The IMO has further recognized that vessels operating in the Arctic and Antarctic are exposed to a number of unique risks including “poor weather conditions and that the relative lack of good charts, communication systems, and other navigational aids pose a challenge for mariners.”Footnote 35
The company SMS was consistent with IMO guidance regarding passage planning. The SMS indicated that passage planning includes the following 4 distinct stages:
- Appraisal of all the available information about the intended voyage, including a review of the charts and publications, prediction of the vessel's condition, assessment of the dangers expected, gathering of information about local tide conditions, etc.;
- Planning of the intended voyage, including courses, waypoints, distances, danger areas, parallel indexes on all conspicuous targets with 6 nm of the intended route, etc.;
- Execution of the passage plan, taking into account the prevailing conditions and abort points;
- Monitoring of the vessel's progress against the intended plan continuously throughout the voyage.
Specifically, the SMS indicated that the following must be included in the passage plan:
- no-go areas;
- the expected position fixing interval at a minimum of every 15 minutes in confined waters or more frequently if required and/or as stated in the master's standing orders;
- areas where the vessel must meet specific load or tide conditions; and
- the identification of confined waters.
The second officer developed the passage plan for the outbound voyage from Helicopter Island to Nain, Labrador. A portion of this voyage was in confined waters, as defined by the SMS. This portion was from Skua Rock to Deer Island in Chesterfield Inlet, a distance of approximately 42 nm. The bottom contact occurred during the last alteration before exiting the confined waters portion of Chesterfield Inlet, as defined by their SMS.
The passage plan was a template with standard written instructions and a route page with places for the navigating officer to add each waypoint, the course to steer, and distance to next waypoint. The passage plan developed by the second officer included a completed route page and referred to the navigation charts, where the courses as well as the parallel indexes were indicated. The passage plan was approved by the master. According to the SMS, all OOWs must review and sign the passage plan. The third officer, who was the OOW at the time of the occurrence, had not reviewed it, nor had he signed it.
The passage plan did not contain certain information required by the SMS, including no-go areas, specific information on tides, and speed restrictions. No additional instructions were provided by the master on expected position-fixing intervals, nor had he written any standing orders for this voyage.
1.16 Navigation procedures
To ensure effective monitoring of a vessel's progress in confined waters, navigators use a combination of visual aids to navigation and navigational equipment. This assists in maintaining situational awareness with respect to the vessel's progress and allows for cross-checking to identify potential equipment or human errors. “In port approaches or restricted waters, the vessel's position is best monitored through a combination of visual references such as leading lines, headmarks and buoy/beacons used together with radar parallel indexing, and by plotting the vessel's position.”Footnote 36
The vessel's SMS specified that monitoring is to be accomplished making full use of all available equipment and navigational aids, and that position monitoring and fixing occur in a manner that does not place sole reliance on a single method. Parallel indexing is to be used whenever indicated on the chart, the use of which gives instantaneous information regarding set and drift in relation to true course and provides a quick reference for confirming the vessel's position.
The checklist for confined waters required that either the master or chief officer be assigned to the bridge during the passage. The checklist had been completed for the occurrence voyage, and the on-board practice in Chesterfield Inlet was for the master or chief officer to be present on the bridge, along with the OOW. However, the roles and responsibilities for the officer who did not have the con were not defined. The STCW states that watches should be carried out based on certain BRM principles including establishing an understanding amongst watchkeeping personnel as to “their individual roles, responsibility, and team roles.”Footnote 37
1.17 Record of shipboard activities
Canadian regulations stipulate that information about shipboard activities be recorded in order to establish a complete record of the voyage.Footnote 38 The vessel's SMS required that specific shipboard activities be logged, including:
- On even hours: the complete row of the logbook, including course, compass, weather, and sea state information, and a vessel position;
- After each significant course change: an abbreviated row of the logbook including course and compass information, as well as a vessel position;
- During each watch: a note if the hand steering and radar tests were completed;
- Departures: the last line in or anchor aweigh time;
- Arrivals: the first line ashore or anchor let go time;
- Change of con: any changes outside of regular watch rotation.
In the 48 hours preceding the occurrence, with respect to the deck logbook entries:
- The complete row of the logbook had been filled out 6 times.
- No course changes were recorded.
- There was 1 entry noting that a steering test had been completed and the vessel had been steered in hand steering, and 1 entry noting that a radar test had been completed.
- No departures were recorded.
- No arrivals were recorded.
- No changes of con were recorded.
The vessel also had a position log, where the vessel's position was recorded more frequently, but the position information was not always recorded on even hours as stipulated in the SMS. As well, the Nanny bridge team maintained a rough log; however, the recording of shipboard activities was not being done in a manner that was consistent with the guidance in the SMS.
1.18 Previous occurrences
Since 2007, there have been 4 reports of vessel groundings in Chesterfield Inlet. Of these, 2 involved shuttle tankers owned by Coastal Shipping Limited: on 24 October 2012, the Dorsch grounded in the Regina NarrowsFootnote 39 and, on 25 October 2012, the Nanny grounded in the Chesterfield Narrows, damaging the forward section of the hull.Footnote 40
Below are some of the contributing factors that the Board found in the TSB investigation into the 2012 grounding of the Nanny in Chesterfield Inlet:
- The master and the OOW did not exchange navigational information throughout the voyage.
- There was insufficient monitoring of the vessel and ineffective BRM.
- Available navigation aids were not adequately cross-referenced.
In addition, the Board found that the availability of lit range beacons would enhance the ability to navigate safely in Chesterfield Narrows at night.
1.19 Outstanding recommendations
In 1995, the TSB published a report entitled A Safety Study of the Operational Relationship between Ship Masters/Watchkeeping Officers and Marine Pilots.Footnote 41 The objective of this study was to identify safety deficiencies associated with teamwork on the bridge. The report raised safety concerns related to the implementation of effective BRM by bridge teams and made the following recommendations:
The Department of Transport require that the initial training syllabus for all ship officers be modified to include demonstration of skills in Bridge Resource Management.
Transportation Safety Recommendation M95-09
The Department of Transport require that all ship officers demonstrate skills in Bridge Resource Management before being issued Continued Proficiency Certificates.
Transportation Safety Recommendation M95-10
In January 1996, TC stated, in its response to these recommendations, that it would promote the development and provision of BRM training courses and that there could be a requirement for prior completion of such a course once they were available in Canada. TC further indicated that such a requirement would be phased in depending on the certificate of competency held by the candidate. In December 2014, TC indicated that it was planning to amend the MPR so that part of the initial training for a Watchkeeping Mate certificate of competency would include BRM competencies. Additionally, the TC-approved STCW BRM training course would become mandatory to obtain an STCW certificate of competency as a master or as a chief mate. The responses to both recommendations have been assessed as Satisfactory Intent by the Board.Footnote 42
1.20 TSB Watchlist
The Watchlist is a list of issues posing the greatest risk to Canada's transportation system; the TSB publishes it to focus the attention of industry and regulators on the problems that need addressing today.
Safety management and oversight is a 2014 Watchlist issue. The solution will require all operators in the marine industry to have formal safety management processes. As well, TC must oversee companies' safety management processes, since some transportation companies are not effectively managing their safety risks, and TC oversight and intervention has not always proven effective at changing companies' unsafe operating practices.
2.0 Analysis
2.1 Events leading to the bottom contact
The vessel was underway in the confined waters of Chesterfield Inlet, Nunavut, at full ahead, in the same direction as the ebb tide, and in darkness. The vessel's speed was 16.7 knots when the master, who had just taken over the con, ordered a port alteration at the planned wheel-over position. The helmsman repeated the port order but put the helm to starboard. The master continued to monitor the vessel's progress on the radar. Within seconds of the initial port order, the master issued a larger port helm order because the vessel was not responding as he expected. The master then ordered port helm 2 more times, and the helmsman continued to apply starboard helm until, 51 seconds after the initial port order, the helmsman stated that the helm was to starboard and applied the correct port order, which stopped the vessel's rate of turn to starboard 28 seconds later.
Meanwhile, the officer of the watch (OOW) was not assisting the master to navigate, nor was he asked to do so following the change of con. Neither he nor the master noticed the error in the direction of the helm applied, nor did they acknowledge the helmsman when he stated that the helm had been to starboard. Over the next 3 minutes and 24 seconds, the master continued to issue orders for maximum port helm in an attempt to bring the vessel back to the original course despite the limited sea room available. He applied astern propulsion, but the strong tide and the vessel's speed did not allow enough time to prevent the Nanny from touching bottom at Deer Island, 4 minutes and 43 seconds after the initial course alteration order.
2.2 Fatigue
Normal healthy adults need between 6 and 9 hours of uninterrupted sleep each night in order to feel well rested and be able to maintain vigilance throughout the day. The average amount of sleep required is between 7 and 8 hours per night.Footnote 43 Disruptions to sleep cycles or sleeping patterns in personnel occupying safety-critical positions may cause performance decrements that increase the risk of incidents and accidents.
Analysis of the master, helmsman, and OOW's self-reported hours of work and rest all indicated disruptions to their sleep periods, especially the night before the occurrence, as follows:
- The master was subject to acute and chronic sleep disruption as well as circadian rhythm desynchronization. Additionally, the master may have been subject to fatigue risk factors related to continuous wakefulness and circadian rhythm timing.
- The helmsman was subject to acute and chronic sleep disruption as well as circadian rhythm desynchronization, and may also have been subject to fatigue risk factors related to circadian rhythm timing.
- The OOW may have been subject to fatigue risk factors related to acute and chronic sleep disruption and circadian rhythm timing.
The effects of fatigue on performance include slower reaction time, increased risk taking, and reduced ability to solve complex problems.Footnote 44 Fatigue more generally affects attention, vigilance, and cognitive functioning. Performance and cognitive functioning are generally the worst during the period when circadian rhythms dictate sleep, typically at night for daytime workers.
The disconnect, by the helmsman, of applying helm in the opposite direction to that ordered, despite acknowledging it correctly, is consistent with reduced attention and a resulting action slip.Footnote 45 Furthermore, despite monitoring the helm and the rudder angle indicator, there was a delay on his part in recognizing the error.
While the master detected a delay in the vessel's response to the helm order, he did not attribute this to an error in helm given that the helm order had been acknowledged correctly, his focus was on the radar, there were no visual cues due to the darkness, and there were no lighted aids.
Upon realizing the vessel was not turning to port, the master continued with the plan by repeatedly asking for port rudder without re-evaluating the situation to determine if this would be sufficient to turn the vessel in the diminishing sea room available. Astern propulsion was eventually applied, but not in sufficient time to prevent bottom contact. The difficulty of the master in assimilating the available information and developing accurate situation awareness is consistent with increased processing time, increased difficulty with problem solving, perseverance with a plan that was not working, and an increased time to react to an emergency.
At the time of the occurrence, the master and the helmsman were fatigued. Both were subject to significant fatigue risk factors and both exhibited performance decrements consistent with fatigue, contributing to the bottom contact.
2.3 Managing fatigue
2.3.1 On-board fatigue management
Preventing fatigue in the workplace requires that workers be provided with adequate rest periods between work shifts during which they are able to obtain sufficient sleep. Employers and employees must also be cognizant of the risks of fatigue to the extent that they manage their own sleep and rest effectively. This is of particular importance for those whose duties can have an impact on the personal safety of themselves or others. As a basis for ensuring that seafarers get sufficient sleep, international standards exist to establish minimum hours of rest (off-duty hours) for seafarers. This is the regulatory means by which the risks of fatigue are addressed in the marine industry.
The Nanny did not have a separate fatigue management plan (FMP), apart from the measures addressing fatigue included in the safety management system (SMS). However, the investigation found the following shortcomings with these measures:
- Although crew hours of rest and work were recorded, no one ashore or on the vessel was monitoring these records for compliance with the SMS and regulations; there were numerous instances where crew had worked extra hours and had not received the minimum prescribed hours of rest. A further examination of the crew members' rest periods from the previous grounding of the Nanny in Chesterfield Inlet in 2012 indicated a similar situation where minimum hours of rest were not being respected at all times.Footnote 46
- An instructional safety video on fatigue was on board; it had been provided by the company, but at the time of the occurrence the crew had not watched it.
On a vessel with a small complement such as the Nanny, the options to prevent fatigue amongst crew members who have worked extra hours are limited. Providing compensatory rest periods may be at the detriment to another crew member's rest. Stopping operations or delaying a departure represents a loss of efficiency with a cost to the company when vessels are fitted and crewed with the expectation that they be operational 24 hours a day, 7 days a week. However, when put in the context of this occurrence, a delay and a well-rested crew may have prevented an accident. The costs associated with such a delay outweigh the financial loss of the accident, which involved removing the vessel from service for dry dock and repairs. In this occurrence, ineffective fatigue management on board the vessel contributed to the master and helmsman being fatigued while on duty.
2.3.2 Fatigue management plans
Establishing minimum hours of rest is an element of fatigue management, but it is not an indicator that sleep is being obtained. As such, providing and monitoring the minimum hours of rest are limited as mitigation strategies for managing fatigue.
In this occurrence, the master's minimum hours of rest as recorded were in accordance with regulatory requirements; however, he was not obtaining sufficient sleep during rest periods. Managing fatigue poses a number of challenges because perception of fatigue is subjective, because the signs of fatigue are not always readily apparent, and because fatigue is difficult to measure. Testing for the existence of fatigue is complex, and both the magnitude and the number of fatigue risk factors must be considered. These challenges were highlighted by the results of the 2014 Concentrated Inspection Campaign (CIC) by Port State Control authorities which identified numerous cases where watchkeeping personnel were not even being afforded the minimum number of off-duty hours required by the regulations.
Given the challenges in managing fatigue, a multi-dimensional approach is required. An FMP is a means of establishing more than minimum hours of rest; it can address such things as fatigue awareness training, use of alertness strategies, and fatigue reporting mechanisms to monitor actual levels of operational fatigue. In Canada, the development of FMPs is a requirement in the rail industry. However, the marine industry does not have such a requirement, nor is there even a requirement for fatigue-related training.
If marine regulations do not require companies to develop comprehensive FMPs, performance decrements may occur in those who occupy safety-critical positions, increasing the risk of incidents and accidents.
2.4 Medical hearing examinations
Maintaining a proper lookout by visible and audible means at all times is an essential aspect of seafarers performing bridge duties. Bridge personnel, when working alone or as a team, are required to recognize occupationally related sounds in their specific environment as well as communicate effectively. This may involve detecting audible alarms, comprehending radio messages, and understanding bridge orders, all of which can have an impact on the safe operation of a vessel.
Seafarers who are holders of certificates of competency must undergo a hearing test as part of their regular medical examinations. The international standard for the medical examinations of seafarers is set by the International Labour Organization (ILO) and includes criteria for hearing ability. According to these standards, the hearing ability of deck personnel such as bridge watchkeepers should be greater than other crew to the extent that would be demonstrated by successfully hearing whispered speech at a distance of 3 m (equivalent to approximately 20 dB in the 2000 to 4000 Hz range).
However, the Transport Canada (TC) testing guidelines do not require those with deck or bridge duties to demonstrate an ability to hear at frequency ranges higher than those consistent with normal conversation; neither a subjective whisper test nor an audiometer test at ranges higher than 3000 Hz is required. In post-occurrence testing, the master of the Nanny passed the conversational hearing, but was unable to pass the whisper test at a distance of 2 m and 3 m. His audiogram indicated impairments from 1000 Hz and was considered abnormal from 2500 Hz with the impairments continuing until 8000 Hz.
This demonstrated that a seafarer may meet the TC guidelines for hearing but not meet the ILO guidelines for a seafarer undertaking deck or bridge duties. Given that TC guidelines for the hearing tests of those undertaking deck or bridge duties do not meet internationally accepted standards, there is a risk that Canadian bridge watchkeepers may have undetected hearing loss sufficient to impair their ability to safely conduct routine and emergency duties.
2.5 Navigation procedures
In confined waters, the task of the navigator becomes more challenging and involved, especially when frequent course changes are necessary. This high workload results in less time to take care of other required duties of the watch, such as position plotting, logbook keeping, radio communications, and monitoring of other bridge team members. It is not unusual, in these circumstances, to have the master or another officer present to share the responsibilities and to act as a back-up by monitoring the progress of the vessel, as there may be little time to react to an error in navigation or respond to an emergency.
In this occurrence, the master was on bridge with the OOW while navigating through confined waters, in accordance with their on-board practices. However, when the OOW came on watch that morning, there was no understanding or discussion about how their roles would be divided, nor did their navigation procedures delineate their roles and responsibilities related to the safe conduct of the vessel. This is contrary to principles described in the International Convention on Standards of Training, Certification and Watchkeeping (STCW) regarding bridge resource management (BRM).
The OOW, who had not reviewed the passage plan, asked the master to take the con before the turn at Deer Island which he perceived as difficult. Once he was relieved by the master, the OOW ceased participating in the monitoring of the vessel's progress. As such, when the error in helm was applied, the OOW was not in a position to readily detect the error and subsequently did not provide meaningful navigational information to assist.
The navigation procedures in use on board were not conducive to ensuring that the bridge team members responsible for monitoring the vessel were adequately vigilant considering the complexity of the navigation.
2.5.1 Bridge resource management
An ongoing exchange of information and the establishment of clear roles for bridge team members are key components of BRM to ensure the safe navigation of the vessel.
In this occurrence, the OOW had limited experience as an officer. He was not a contributing member of the bridge team in the period leading up to the occurrence; as a result, the master was the only one monitoring the vessel in confined waters. Once the helm error occurred, the OOW's assistance was not constructive, and the master did not provide him with clear direction as to how he could assist. Although the master had received BRM training, his performance with respect to BRM skills was likely impaired by his fatigue. The OOW, on the other hand, was less likely affected by fatigue, but he was not trained in BRM competencies.
As demonstrated by this occurrence and others, including the Nanny's 2012 grounding in Chesterfield Inlet,Footnote 47 shortcomings in the implementation of BRM principles have been a factor contributing to marine accidents. BRM training provides a bridge officer with practical skills and competencies to have the confidence required to exchange information with the bridge team. Although there is currently no regulatory requirement in Canada for bridge officers to complete training or demonstrate continued proficiency for BRM as a prerequisite to achieve or maintain certificates of competency, the planned TC amendments will include BRM competencies and knowledge as part of Simulated Electronic Navigation (SEN) training courses, for both new and renewed certificates.
Until such time as training and continued proficiency in the principles of BRM for all bridge officers are required, there is an increased risk that bridge team awareness and effectiveness will be impaired, thereby increasing the risk to the vessel, its complement, and the environment.
2.6 Safety management implementation and oversight
Ongoing management of safety by means of a documented SMS is intended to help organizations identify and mitigate risks in their operations. One of the objectives of an SMS is to assess all identified risk to vessels, personnel, and the environment and to establish appropriate safeguards. In addition, a vessel operator should carry out internal safety assessments to evaluate the effectiveness of the SMS and to verify whether all activities and operations comply with the SMS. One way to identify risks is by analyzing past accidents and hazardous situations. Once a risk has been identified, it can be mitigated by establishing standard operating procedures and by developing checklists.
In this occurrence, there were several factors relating to navigation practices and BRM that had also been identified in the Transportation Safety Board of Canada (TSB) investigation into the 2012 grounding of the Nanny. The investigation into the 2014 occurrence also found discrepancies between the requirements of the SMS and on-board practices, such as:
- logbook entries were not completed as required;
- the passage plan was missing relevant information and details that were required;
- requirements for minimum hours of rest were not always being met; and
- the OOW did not review or sign the passage plan.
The SMS did not have a process for verifying compliance with minimum hours of rest requirements and did not clearly define the roles and responsibilities of bridge team members when 2 navigators were present on the bridge. Despite having a certified and audited SMS since 2009, the investigation found several shortcomings in the implementation of the SMS on board, some of which are linked to the causal and contributing factors in this occurrence
3.0 Findings
3.1 Findings as to causes and contributing factors
- The helmsman incorrectly applied 2 helm orders to starboard during a large alteration to port, which caused the vessel to start swinging in the opposite direction of the intended course.
- Upon realizing the vessel was not turning to port, the master continued with the plan by repeatedly asking for port rudder without re-evaluating the situation. Astern propulsion was applied too late to prevent the Nanny from touching bottom given the vessel's speed and the limited sea room available.
- At the time of the occurrence, the master and the helmsman were fatigued. Both were subject to significant fatigue risk factors and both exhibited performance decrements consistent with fatigue, contributing to the bottom contact.
- Ineffective fatigue management on board the vessel contributed to the master and helmsman being fatigued while on duty.
- The officer of the watch ceased participating in the monitoring of the vessel's progress after the master took over the con so was not in a position to readily detect the helm error or to assist the master in responding to it.
- The navigation procedures used by the bridge team members were not adequate to effectively navigate the vessel.
3.2 Findings as to risk
- If marine regulations do not require companies to develop comprehensive fatigue management plans, performance decrements may occur in those who occupy safety-critical positions, increasing the risk of incidents and accidents.
- Until such time as training and continued proficiency in the principles of bridge resource management for all bridge officers are required, there is an increased risk that bridge team awareness and effectiveness will be impaired, thereby increasing the risk to the vessel, its complement, and the environment.
- Given that Transport Canada guidelines for the hearing tests of those undertaking deck or bridge duties do not meet internationally accepted standards, there is a risk that Canadian bridge watchkeepers may have undetected hearing loss sufficient to impair their ability to safely conduct their routine and emergency duties.
3.3 Other findings
- Despite having a certified and audited safety management system (SMS) since 2009, the investigation found several shortcomings in the implementation of the SMS on board, some of which are linked to the causal and contributing factors in this occurrence.
- The 2010 shipping industry request for new or modified aids to navigation in Chesterfield Inlet has not been resolved by the Canadian Coast Guard pending an analysis of all the aids to navigation in Chesterfield Inlet, which was commenced in 2013.
4.0 Safety action
4.1 Safety action taken
4.1.1 Det Norske Veritas – Germanischer Lloyd
Following the occurrence, Det Norske Veritas – Germanischer Lloyd (DNV-GL) indicated that they conducted a review of the safety management system (SMS) audit reports on the company and on the Nanny from January 2013. DNV-GL reported that the audits had been thoroughly conducted and had been carried out in close cooperation with the Flag Administration.
4.1.2 Coastal Shipping Limited
Following the occurrence, the operating company sent a memo to all vessels requiring the following to be implemented immediately:
- bridge officers to keep the deck log up-to-date (hourly);
- OOWs to remain vigilant and aware even when the master is on the bridge and has the con;
- all crew to adhere strictly to the rest hours;
- masters to submit the rest hours to the Human Resources (HR) department on a monthly basis;
- masters to request stoppage from the office to allow for crew rest if rest hour breach is present or anticipated;
- all crew to review the fatigue management video; and
- masters to forward the signed-off certificate for the review of the video to HR at the first opportunity.
The memo also alerted crew about upcoming changes to the confined waters checklist and noted that the above-indicated items would be incorporated in the SMS.
Additionally, the company acquired fatigue management software. The company indicated that the software was up and running on 1 of the vessels and will be installed on the other 4 vessels in the company fleet. The software is meant to “[r]educe crew fatigue while checking compliance with [the International Convention on Standards of Training, Certification and Watchkeeping] STCW 2010, the [International Labour Organization Maritime Labour Convention] ILO MLC, [the United States Oil Pollution Act of 1990] US OPA 90 and [the Oil Companies International Marine Forum] OCIMF recommendations.”
This report concludes the Transportation Safety Board's investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .
Appendices
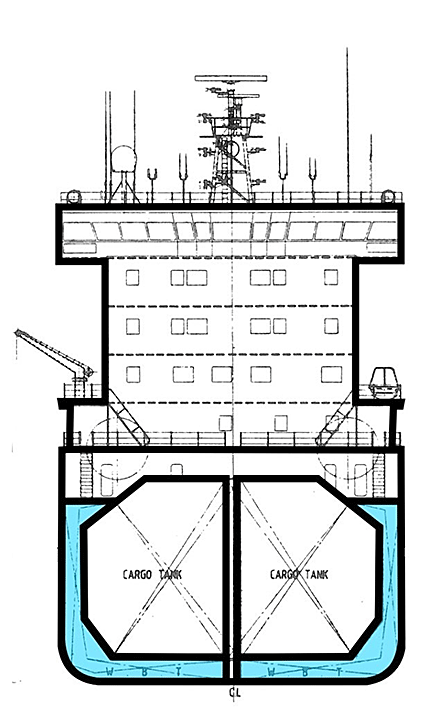
Appendix A – Nanny profile and cross-section (not to scale)
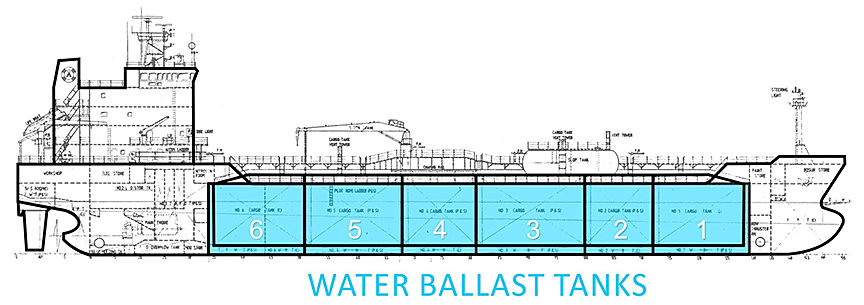
Note: Wing tanks (ballast) are shown as shaded (blue). Tanks 1, 3, and 5 are divided by a centreline bulkhead and tanks 2, 4, and 6 are continuous.
Damaged areas:
- Tank #1: starboard bottom
- Tank #2: starboard bottom
- Tank #3: port and starboard bottom
- Tank #4: starboard bottom
- Tank #5: starboard bottom
- Tank #6: starboard bottom
Appendix B – Nanny bridge layout
Appendix C – Area of the occurrence
Appendix D – Work-rest schedules
Work-rest schedules for the master, the helmsman, and the OOW for the period preceding the occurrence. Note that hours of rest for the master are subdivided into actual hours of sleep (hatched area). The master's hours also include 06 October, during which time the master was on the Travestern. The following day, the master joined the Nanny.
Appendix E – Definitions of fatigue risk factors
Acute sleep disruptions
Acute sleep disruptions are reductions in the quality or quantity of sleep that have occurred within the previous 3 days. Acute reductions in the quantity of sleep are normally considered remarkable when they are at least 30 minutes in duration and the amount of deep sleep or REM sleep is curtailed.
Chronic sleep disruptions
Any disruptions to sleep quantity or quality that are sustained for periods longer than 3 consecutive days are considered chronic sleep disruptions. Comparing the amount of sleep obtained to the amount of sleep required for a given period of wakefulness can provide an estimate of a person's sleep debt. A sleep debt of more than 2 hours over a 7-day period may be indicative of chronic fatigue. Although chronic sleep disruptions may be small, they can change an individual's sleep architecture. For example, the amount of deep sleep or REM sleep may be reduced without any reduction in total sleep time, resulting in fatigue. Disruptions in the quality of sleep for mariners include being at sea for extended periods, working shifts that divide sleep periods and sleeping in environments with noisy crewmates, vessel engines and rough seas, all of which can disrupt sleep quality without a person being aware of the change.
Circadian rhythm disruptions
Desynchronization: There are numerous daily biological (circadian) rhythms in humans; some research indicates that there are hundreds.Footnote 48 Optimal human performance occurs when all the circadian rhythms are synchronized to each other as well as to external time cues. These time cues include the light–dark cycle, meal times and socializing periods. People working shifts with irregular patterns usually have to adjust their sleep-wake patterns quickly to keep up with the changing shifts. Changing sleep-wake patterns too quickly can cause circadian rhythms to desynchronize.Footnote 49
Desynchronization occurs because each biological rhythm adapts to a new sleep-wake pattern at a different rate.Footnote 50 For those who work continuous night shifts, circadian patterns may change and adapt over time. However, for those who operate only occasional night shifts, circadian patterns will not adapt. In general, researchers have found that the adjustment of the human circadian system resulting from changes to the sleep-wake pattern occurs at a rate of 1 to 1.5 hours per day. Adjusting from being awake during the day to being awake at night, a 12-hour difference, could take between 12 and 18 days for complete adjustment to take place and optimum performance to return. Operating only a few night shifts, especially sporadically, will not result in optimum circadian adjustment and performance will continue to be affected by circadian lows.Footnote 51, Footnote 52
Desynchronization can cause fatigue, daytime sleepiness, psychomotor impairment,Footnote 53 impaired performance, insomnia,Footnote 54 other sleep disturbances, reduced cognitive skills, and muscle fatigue. Symptoms of desynchronization may also result in a further reduction in sleep time and quality. Employees working on shifts with variable start and finish times will constantly be susceptible to the development of desynchronization, regardless of the length of time one has worked variable shifts.Footnote 55 Fatigue is therefore known to increase as start time variability increases.Footnote 56
Timing: Performance and cognitive functioning are generally worst during the period when circadian rhythms dictate sleep, typically at night for diurnal workers and more specifically during a principal period of drowsiness that occurs between 0300 and 0500. Irrespective of motivation and circumstances, a person may have a hard time remaining alert during periods of maximum drowsiness. Performance on specific measurements such as reaction time,Footnote 57 arithmetic and signal detectionFootnote 58 and reaction to safety alarm alerts,Footnote 59 have all been demonstrated to be worst during this period.Footnote 60, Footnote 61
Continuous wakefulness
The Transportation Safety Board of Canada defines continuous wakefulness as being awake for longer than 17 hours.