Uncontrolled fall of rescue boat
Spirit of Vancouver Island rescue boat No. 3
Swartz Bay, Vancouver Island, British Columbia
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Description of the vessel
The Spirit of Vancouver Island is a roll-on/roll-off passenger ferry owned and operated by British Columbia Ferry Services Inc. The vessel has 4 rigid-hull inflatable type rescue boats located forward on deck 6 (2 on each side). The rescue boat involved in this occurrence, rescue boat No. 3 (hereafter referred to as “the rescue boat”), is located on the starboard side of the ferry (Figure 1).

The rescue boat is 6.83 m long and 1.99 m wide. It weighs 1108 kg and has a capacity of 6 persons. It was manufactured in March 2014 and was fitted on board the vessel in 2016, along with the davit used for raising and lowering the rescue boat (Figure 2).

The occurrence
On 19 June 2018, at about 1645,Footnote 1 an original-equipment manufacturer service technician for the davits on the Spirit of Vancouver Island boarded the ferry in Tsawwassen, British Columbia, to respond to a service call about intermittent jerking of the rescue boat davit.
While the vessel was docked, either at Tsawwassen or Swartz Bay in between sailings, the technician, positioned on deck 6, lowered and raised the rescue boat several times with assistance from crew members to test the intermittent jerking defect and determine its source.
During this time, the technician was unable to identify the source of the problem and decided to remain on the vessel after it shut down for the night to continue troubleshooting. A deckhand remained on board to assist the technician. In addition, 4 night-shift engineers and an engine room assistant were on board, performing duties in the engine room.
As troubleshooting continued, the technician explained to the deckhand that he planned to charge the hydraulic accumulator with nitrogen. To allow the technician to access the accumulator chamber, the deckhand lowered the rescue boat to the water and slackened the fall by approximately 75 cm to 100 cm, then raised the davit back to its maximum height. The uncrewed rescue boat remained floating in the water, with the fall slack and the lifting shackle and the hook resting on top of the fuel tank, while the technician charged the hydraulic accumulator with nitrogen. This process took approximately 20 minutes.
During this time, the sea state was calm without any swell. There was a northerly wind of 1 to 3 knots. The sky was clear, but it was dark.
At approximately 2340, after the technician had finished charging up the nitrogen, the first engineer came up to deck 6 at the technician’s request to witness the testing and acknowledge the completion of the defect repair. The deckhand began retrieving the rescue boat from the water using the davit while the first engineer and the technician stood by and observed.
From their positions on deck 6, the deckhand and the first engineer could see the rescue boat as it was being raised; however, they could not see how the hook and the lifting shackle were positioned.
The deckhand was able to raise the rescue boat smoothly. When it was approximately 25 cm below the davit’s limit switch, the deckhand changed the lifting speed from high to low as per normal operational practice to avoid activating the limit switch. The rescue boat jerked slightly due to this change in speed and then fell into the water, a drop of approximately 16 m. The impact from the fall resulted in 2 cracks to the rescue boat’s fuel tank and minor damage to the hull. An estimated 100 L of gasoline stored inside the boat’s fuel tank was released into the environment.
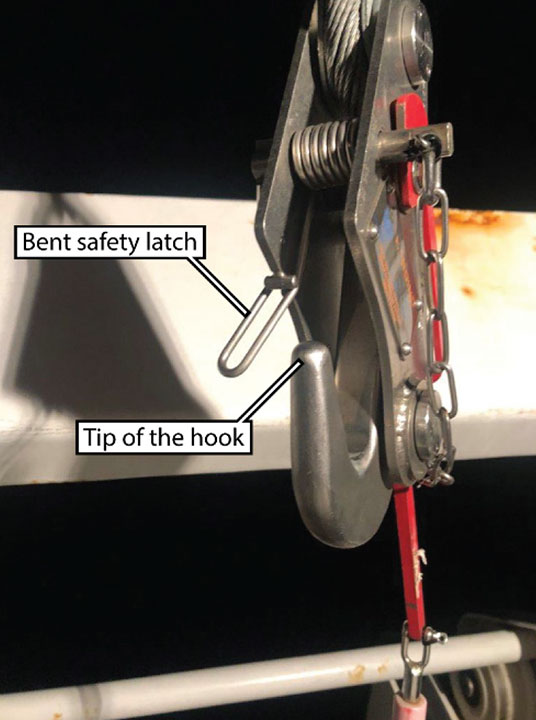
Following the occurrence, the first engineer, the deckhand, and the technician inspected the hook and observed that the spring-loaded safety latch on the hook was bent to the side, creating a gap between the latch and the tip of the hook (Figure 3). It could not be determined when or how the safety latch became bent.
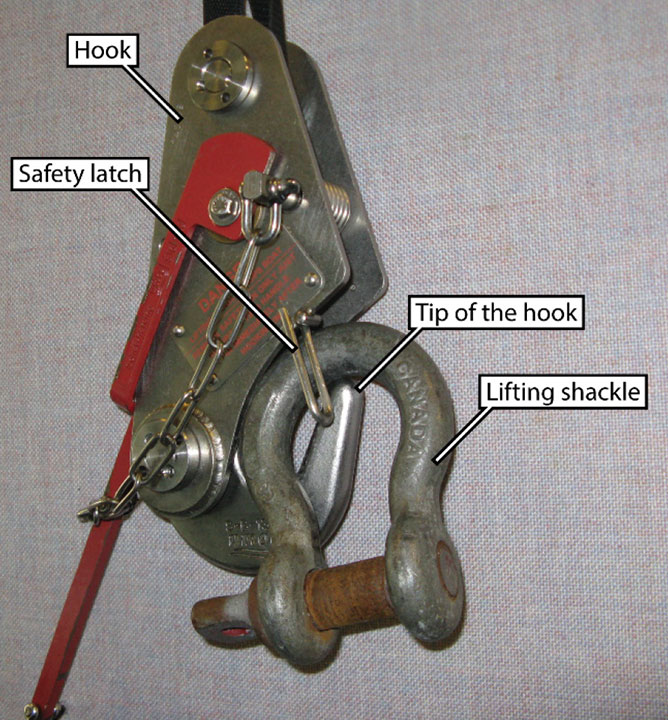
The investigation determined that the hook design is such that the lifting shackle can rest on the tip of the hook (Figure 4). When the falls were slack while the rescue boat was floating unmanned in the water, there may have been an opportunity for the lifting shackle to become positioned on the tip of the hook such that it could slip off the hook through the gap resulting from the bent safety latch.
Recent change to operating procedure
On 18 April 2018, British Columbia Ferry Services Inc. experienced an incident involving a rescue boat on another company vessel. In this incident, the rescue boat fell into the water during drills and 2 crew members in the boat were injured.Footnote 2
As a result, British Columbia Ferry Services Inc. imposed a temporary change to procedure so that, other than during an actual emergency, the raising and lowering of rescue boats was to be done unmanned. This temporary change was in place while the davits on all of the vessels in the fleet underwent inspection.
This temporary change was intended to reduce risk. However, it meant that, from the davit operating location and compounded by the darkness, there was no longer a way for the crew to verify that the lifting shackle was correctly positioned on the hook. The Canadian Centre for Occupational Health and Safety states that, before moving a load, the operator should ensure that the lifting device sits in the saddle of the hook.Footnote 3
In this occurrence, the rescue boat was lowered into the water and remained there for approximately 50 minutes with the fall slack and the hook and lifting shackle resting loose inside the rescue boat. During this time, the rescue boat was uncrewed and free to move about in the water, which may have created an opportunity for the lifting shackle to reposition itself on the tip of the hook. When the deckhand began raising the rescue boat, it was dark, and from his location on deck 6, he was unable to see the position of the lifting shackle on the hook.
Safety message
Any change to an operating procedure would benefit from a comprehensive risk assessment to help identify new risks that may have been introduced as a result of the change. In this case, the procedure was changed quickly following the previous incident involving crew injuries, and a comprehensive risk assessment was not conducted.
Safety action taken
Palfinger Marine
The service company instructed all of its technicians to conduct service or repairs only after confirming that the rescue boat has been removed from its davit fall.
British Columbia Ferry Services Inc.
Following this occurrence, the company carried out a risk assessment that resulted in rescinding the restriction on personnel in the rescue boats during non-emergencies.
This report concludes the Transportation Safety Board's investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .