Non main track collision
Canadian National
Switching assignment no. 602-23-17 and a stationary cut of cars
Track VC–64, Scotford Yard
Vegreville Subdivision
Fort Saskatchewan, Alberta
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 18 August 2010 at approximately 0330 Mountain Daylight Time, CN switching assignment L602-23-17 was shoving 50 loaded and 5 empty cars eastward into track VC-64 at Scotford Yard when the movement collided with a cut of 46 empty cars in the track. As a result of the collision, 43 cars derailed including 21 cars of dangerous goods or residue. There was no release of product and there were no injuries. The cars were intended for track VC-63.
Ce rapport est également disponible en français.
Factual information
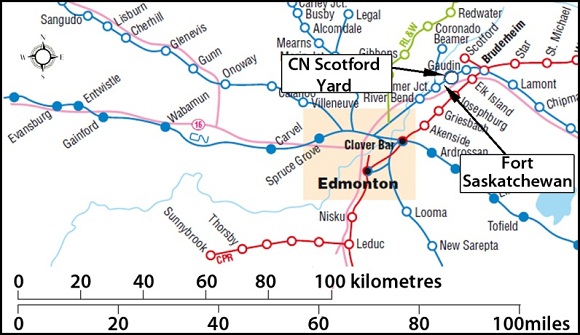
In the early morning hours of 18 August 2010, Canadian National (CN) switching assignment L602-23-17 (assignment 602) was performing routine switching operations on the west lead at Scotford Yard, just east of Fort Saskatchewan, Alberta (see Figure 1). The Locomotive Control System (LCS)Footnote 1 is not used in this yard.
Assignment 602 was in the process of building train 314. The movement was powered by 3 locomotives, weighed about 6613 tons and was 3498 feet long. The crew was requested to pull 55 cars (50 loads and 5 empties) from tracks VC-70 and VC-68 and to place them in track VC-63 (see Photo 1) for mechanical inspection and an air test.
The crew comprised a locomotive engineer, foreman,Footnote 2 helper and a trainee. The crew began its shift at 1800 on August 17, 2010. The trainee performed various switching duties under the direction of the foreman. After completing eight hours on duty, the trainee was permitted to depart. He was not present when the accident occurred.

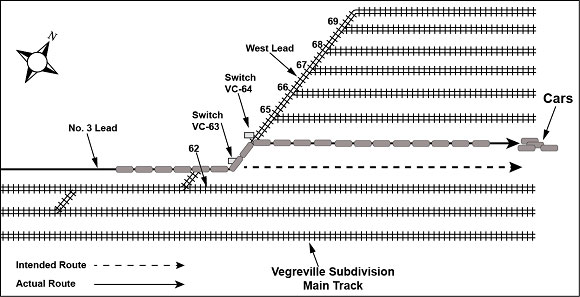
At approximately 0315Footnote 3, assignment 602 pulled westward onto the west lead track. The helper was situated on the front of the locomotive in order to line switches as the movement progressed. The crew had previously run light engine through track VC-63 and knew it to be clear. The foreman, riding one of the cars, counted the switches as the train progressed westward. He had planned to get off at the VC-63 switch, but mistakenly got off at the VC-64 switch. The track number is indicated on the switch target. The foreman stopped the movement after it cleared the VC-64 switch. He lined the switch and checked the points and switch target. Looking eastward down the track, he then radioed the locomotive engineer to begin shoving. The 55 cars were being shoved into track VC-64, instead of the intended track VC-63 (see Figure 2). During this move, no one was riding the point, nor was positioned on the ground to observe the progress of the movement. There were no yard personnel visually monitoring the progress of the movement from a remote location either by direct sight or camera.
Assignment 602 travelled approximately 12 car lengths into track VC-64 and at a speed of 9 mph struck a stationary cut of 46 empty cars (with the air brakes applied) that had been placed in the track about 2 ½ hours earlier. As a result of the collision, a total of 43 cars, 17 loads and 26 empties, derailed. The derailed cars included 8 cars from assignment 602, 8 stationary cars on track VC-64, 8 stationary cars on track VC-62, 9 stationary cars on track VC-65, 5 stationary cars on track VC-66 and 5 stationary cars on track VC-67 (see Photos 2 and 3). Eleven cars were destroyed. The dangerous goods cars involved included:
- 1 load of propane, UN1075;
- 4 loads of propylene, UN1077;
- 9 loads of diesel fuel, UN1202;
- 1 residue last contained propane, UN1075;
- 2 residue last contained flammable liquids, UN1993;
- 1 residue last contained carbon dioxide, UN2187;
- 1 residue last contained corrosive liquid, UN3267; and
- 2 residue last contained sulphuric acid, UN1830.


There were no dangerous goods released and there were no injuries. Over 400 feet of rail was rolled in track VC-62 and approximately 2000 feet of track was damaged in the adjacent tracks.
The sky was clear and the temperature was 10°C.
Incident response
The required initial notifications of the accident were carried out by the yardmaster and CN's Network Operations Centre. CN Operations, Mechanical and Engineering personnel along with CN Police Services responded to the occurrence. Municipal Police and Fire Services also responded. The response was coordinated by CN and the Municipal Fire Services.
Canadian Rail Operating Rules, Rule 115 Shoving equipment
Canadian Rail Operating Rules (CROR) Rule 115, Shoving Equipment, states (in part):
(a) When equipment is shoved by an engine or is headed by an unmanned remotely controlled engine, a crew member must be on the leading piece of equipment or on the ground, in a position to observe the track to be used and to give signals or instructions necessary to control the move.
EXCEPTION: A crew member need not be so positioned when the portion of the track to be used is known to be clear...
(b) Known to be clear is defined as seeing the portion of the track to be used as being clear and remaining clear of equipment and as having sufficient room to contain equipment being shoved. This determination must be made by a qualified employee who can observe the track and has radio contact with the employee controlling the movement. Where a track that has been seen to be clear and no access to that track is possible by another movement, the track may be considered as "known to be clear".
Note: When it can be determined that other movements are not on duty or will not be performing work in the track to be used, the requirement of known to be clear can be considered to be fulfilled continuously.
Effective 01 August 2009, CN Regional Special Instructions for CROR Rule 115 suspended the "KNOWN TO BE CLEAR" provision in order to ensure that the point is visually protected at all times. The exception to Rule 115(a) was also revised to state:
If a crew member is not on the leading piece of equipment or on the ground, in a position to observe the track to be used and to give signals or instructions necessary to control the move, duties of the crew member referred to in CROR Rule 115(a) “known to be clear” may be fulfilled by:
- Another CROR qualified person who is not a member of the immediate crew, (i.e. a yardmaster).
- Another qualified person, who is not a member of the crew, using a camera. The qualified person operating the camera must constantly observe the track to be used, and be able to give instructions necessary to control the movement.
The foreman was familiar with the revised requirements of CROR Rule 115.
Crew experience, training and work/rest schedule
The foreman on assignment 602 entered service in October 2009 and was qualified (as a foreman) in March 2010. He was initially scheduled as the helper on assignment 602 for the work shift. However, the regular foreman had booked off which resulted in him being assigned to work as foreman. This was his first shift working independently as a foreman in Scotford Yard. He had worked the required 45 shifts to qualify for promotion to foreman and had worked 82 of his 90 probationary shifts since. Prior to the accident, the foreman had worked 7 shifts at Scotford Yard, of which 4 were as a trainee and 3 were as a helper. For 12 of his 82 probationary shifts, he had been assigned a trainee.
The foreman had a full night sleep the night before and he had several hours of sleep in the afternoon prior to reporting for work at 1800. He had been off duty since August 15 (0700) when he finished working assignment 602 as a helper.
The helper on the occurrence train had been qualified as a foreman since March 2007. Although he had more experience than the foreman, due to collective agreement requirements he was called as the helper on the crew.
The locomotive engineer entered service in July 1983. He had worked in Scotford Yard since December 1995 when he qualified as a foreman.
Sleep/wake cycle
The sleep/wake cycle follows a 24-hour rhythm with approximately 1⁄3 of this time spent sleeping. Although individual rhythms vary, everyone's cycle has 2 distinct sets of alertnessFootnote 4 peaks and dips. The big dip, or the lowest point of alertness, is at night in the hours just before dawn between 3:00 am and 5:00 am.
Irregular work hour schedule
The circadian clock is perfectly synchronized to the traditional pattern of daytime wakefulness and night-time sleep. Irregular work hours, which include shifts at night, desynchronize the body's circadian rhythms. The body can adjust slowly to successive nights of shift work and daytime sleeping by an hour or two a day. It takes several days for the body to fully adjust to a new schedule of work hours. On the first 2 nights of shift work, there is a drop in alertness during the early morning hours. Within a few days, alertness is more easily sustained at night and daytime sleep improves. However, at the end of a period of night shifts or a few days off, the circadian clock would have to be reset.
Effects of alertness on performance
A lower level of alertness negatively affects task performance as it involves a lower attention to details and it impedes the cognitive process. Taking shortcuts, missing or misinterpreting cues, or miscommunications are examples of performance degradation as a result of a lower level of alertness.
Scotford Yard
Scotford Yard was originally built in the early 1980s. As demand grew, it has expanded to support the major petrochemical industry in the Scotford area. The commodities handled at this yard include fertilizer, phosphate rock, liquefied petroleum gas (LPG), sulphuric acid, sulphur dioxide and other dangerous goods.
The accident occurred near the centre of the yard. At the time of the accident, the yard lead tracks were lighted, but the centre of the yard was not. A yardmaster monitors the east and west ends of the yard with pole mounted video cameras. The centre of the yard has no camera coverage. Tracks VC-63 to VC-75 run east-west in a bowl configuration and the use of handbrakes is not required. When standing next to VC-63 and VC-64 during the day, it is possible to see if the tracks are clear to their east ends, approximately 4000 feet away. At the time of the accident, from the same locations, it was possible to see lighting along the east lead when the tracks were clear.
Prior to 2009, all cars moving into or out of the Greater Edmonton Terminal (GET) were put through the classification facility at Walker Yard. The closure of Walker Yard Hump in February 2009 resulted in a reduction of road switching assignments to and from outlying areas and increased the flat switching required at yards surrounding the Greater Edmonton Terminal, including at Scotford Yard. About 500 cars per day are flat switched at Scotford Yard. Prior to 2009, the number was approximately 300 cars per day. About 80% of the switching is performed at the west end of the yard. The maximum yard speed is 15 mph.
Scotford Yard switching and supervision
At the time of the occurrence, CN had 2 switching assignments that worked exclusively in Scotford Yard. Assignment 601 started at 0600 each day and assignment 602 started at 1800 each day. Both assignments worked 10 to 12 hours each day, 7 days a week, building trains.
At least 1 yardmaster is on duty in Scotford Yard at all times. Yardmasters are rules-qualified operations personnel who assign switching work to yard crews and coordinate yard activities including track usage. They can also provide camera point protection under CN Regional Special Instruction (RSI) to CROR Rule 115(a).
Track information
The tracks, leads and turnouts at Scotford Yard are constructed with 115-pound rail. Storage tracks at this yard are constructed with 100-pound rail. The turnouts are equipped with self guarded manganese (SGM) frogs. More than 50% of turnouts have Samson points on the diverging route. Ties on the east lead, west lead and at turnouts are hardwood. The ties are fully spiked with switch point guardsFootnote 5 on all west lead turnouts. At the time of the occurrence, there was a program in place to install switch point guards on the east lead turnouts.
Lead switches are controlled with semi-automatic 17B high mast switch stands that are pressure tested annually. These switches can be trailed through without damaging the connecting rod, but this is not an accepted practice in the yard. The standard high mast stands are being replaced with 36E ergonomic handle low stands. There are no automatic switches in the yard; all yard switches are operated by hand.
The east and west lead tracks and turnouts are ultrasonically tested once a year. They were last tested in May 2010. During this test, 2 defects were detected on each lead track and were repaired. Track geometry is normally tested once a year using CN's hyrail geometry vehicle. However, no track geometry test had been conducted at Scotford Yard in 2010 prior to the accident.
Analysis
There were no equipment or track defects present that were considered contributory to this occurrence. The analysis will focus on the application of CROR Rule 115, employee alertness and the actions of the foreman.
The accident
The intended move for assignment 602 was to shove 55 cars into track VC-63 which the crew knew was clear. However, the foreman mistakenly positioned himself at the VC-64 switch. Before instructing the assignment to shove eastward, he did not confirm his location by reading the number on the switch target. In addition, when looking eastward down track VC-64, had the track been clear he would have been able to see the east lead lighting. The absence of visible lighting at the far (east) end of the track was a visual cue that the track was occupied. However, the foreman either did not perceive this visual cue or did not interpret it correctly. The collision and derailment occurred when 55 cars were shoved, unprotected, into track VC-64 where they contacted a cut of stationary cars.
The foreman was aware that a revision to parts of CROR Rule 115 had suspended the “KNOWN TO BE CLEAR” provision in order to ensure that the point of the movement was visually protected at all times. However, based on his prior knowledge of the status of track VC-63 and the whereabouts of other yard movements, he considered this to be sufficient verification that the track was clear. Despite the requirement to visually protect the movement at all times, no visual point protection was provided during the move.
Employee alertness
The crew began their shift at 1800 the previous day and the accident occurred at 0315 the following morning. They had been on duty for about 9 1⁄2 hours. Late in the shift and in the early hours of the day, the body's circadian rhythm creates a lower level of alertness which can have a negative impact on worker performance. For example, lower levels of alertness can result in unintentional reduced motivation to perform well. This can translate into a willingness to take risks and a laxity in safety that would not normally be tolerated when alert.
In this occurrence, the foreman was working a night shift, which was his first shift following 2 days of rest. His circadian rhythm would not yet have been reset for a night shift. Although he had slept well on the Monday night and had napped on Tuesday afternoon prior to reporting to work, this kind of circadian disruption desynchronizes the body's rhythms and can cause reduced alertness, particularly in the early morning hours. A reduced level of alertness likely contributed to the foreman's actions, including his decision to bypass the requirement for visual point protection of the movement and his actions leading to misrouting assignment 602 into track VC-64.
Crew work experience
For a recently promoted foreman, job skills and knowledge are further developed through field experience. In addition it should be expected that mentoring by senior employees continues after an employee is promoted. Notably, both of the other crew members on assignment 602 had more operating experience than the foreman. However, with their operational responsibilities during the move, the other crew members were not in a position to correct the erroneous routing of the movement. While the foreman was trained and qualified for his position, he had limited experience as a foreman and was not fully familiar with operations at Scotford Yard.
Scotford Yard lighting
During daylight hours, the entire length of a clear track can be seen from both ends of Scotford Yard. Because most of the work is performed at the switches on the leads, yard lighting was provided along the leads at both ends of the yard to increase visibility, safety and productivity at night. During night operation at the time of the occurrence, it was not possible to fully observe the tracks from each end as the center of the yard was not illuminated. However, if the track was clear, some lighting from the opposite end of the track would have been visible and could have been seen reflecting off the rails.
When the foreman looked down track VC-64 it was dark, which likely led him to the mistaken conclusion that the track was clear. The absence of lights in the centre of the yard made it more difficult for the foreman to correctly perceive that track VC-64 was occupied. When railway yards are not adequately lighted for night switching operations, visibility along certain yard tracks can be compromised, making it more difficult to verify the status of the track and increasing the risk of a yard collision and derailment.
Findings
Findings as to causes and contributing factors
- The collision and derailment occurred when 55 cars were shoved, unprotected, into track VC-64 where they contacted a cut of stationary cars. The intended move had been to shove the cars into track VC-63 which the crew knew was clear.
- Despite the requirement to visually protect the movement at all times, no visual point protection was provided during the move.
- A reduced level of alertness contributed to the foreman's actions, including his decision to bypass the requirement for visual point protection of the movement and his actions leading to misrouting assignment 602 into track VC-64.
- While the foreman was trained and qualified for his position, he had limited experience as a foreman and was not fully familiar with operations at Scotford Yard.
Finding as to risk
- When railway yards are not adequately lighted for night switching operations, visibility along certain yard tracks can be compromised, making it more difficult to verify the status of the track and increasing the risk of a yard collision and derailment.
Safety action taken
In January 2011, TSB issued Rail Safety Advisory Letter 02/11 to highlight the number of recent switching accidents in Scotford Yard. The letter suggested that Transport Canada may wish to review CN's work procedures, safety measures and switching practices to ensure they are adequate and effective for safe operations.
Transport Canada's (TC) response stated that it was monitoring operations at Scotford Yard, as well as other CN rail yards in the Greater Edmonton Terminal (GET) area. TC identified rail operations in the GET area as a concern and has increased monitoring and inspections for the coming year. TC will continue with enhanced monitoring/inspection activities and will take appropriate action should a threat to safe rail operations develop.
In January 2011, CN installed additional lighting at Scotford Yard to increase visibility at the center of the yard during night switching operations.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .